implant retention and removal after internal fixation of the symphysis pubis
TRANSCRIPT
Injury, Int. J. Care Injured (2005) 36, 827—831
www.elsevier.com/locate/injury
Implant retention and removal after internalfixation of the symphysis pubis
Raghu Raman a, Craig S. Roberts b, Hans-Christoph Pape c,Peter V. Giannoudis a,*
a St. James’s University Hospital, Beckett Street, Leeds, LS9 7TF, UKbUniversity of Louisville School of Medicine, Department of Orthopaedic Surgery,Louisville, Kentucky, USAcDepartment of Trauma, Hannover Medical School, Hannover, Germany
Accepted 23 November 2004
KEYWORDSSymphysis pubis;Plating;Failure;Infection;Dyspareunia;Pregnancy;Implant removal
* Corresponding author. Tel.: +44 11fax: +44 113 2065156.
E-mail address: [email protected]
0020–1383/$ — see front matter # 20doi:10.1016/j.injury.2004.11.012
Summary Although internal fixation of diastasis of the symphysis pubis is commonlyperformed, there are no clear guidelines regarding the indications for removal ofthese implants. The long-term physiologic effects of retaining these internal fixationdevices are not well described. We surveyed the literature to assess the currentthinking and recommendations regarding implant retention and removal. Twenty-fourcase series and two case reports were found, for a total of 482 cases. Complicationsarose as a result of implant retention in 7.5% of patients, with infection the mostcommon complication. There is no consensus in the literature regarding implantretention and removal after internal fixation of diastasis of the symphysis pubis.# 2004 Elsevier Ltd. All rights reserved.
Introduction
Pelvic ring injuries account for more than 10% of theinjuries to the human skeleton, with motor vehicleaccidents responsible for over 68% of the cases.7,18
Anterior pelvic disruptions are seen in more thanhalf of all pelvic ring injuries.7,18 Stabilisation of theanterior pelvic ring, particularly the pubic symphy-sis, is an essential part of the definitivemanagementof these injuries.
The preferred method of stabilisation of diastasisof the pubic symphysis is internal stabilisation which
3 2065084;
m (P.V. Giannoudis).
04 Elsevier Ltd. All rights rese
is rapidly replacing forms of external fixation as adefinitive procedure.34 Internal stabilisation of theanterior pelvic ring has been achieved using two-holed plates,36 four-holed plates (2.5—4.5 mm),20,26,29,34,37 curved plates,29,37 dynamic compressionplates,2,27,29,37 reconstruction plates,27,29,37 retro-grademedullary screws with wires,28,34 tension bandwiring31 and cord sutures.5,34 The techniques of sin-gle plating,27 double plating,17,27,34 biplanar fixa-tion27 and box fixation27 have also been described.
To our knowledge, there are no clear recommen-dations in the current literature databases (Med-line, CINAHL, Cochrane, Embase) regarding thelong-term effects of retaining these internal fixationdevices following bony union or the indications forimplant removal. The purpose of this study was to
rved.

828 R. Raman et al.
review the current literature on the subject in orderto identify the long-term physiologic effects (e.g.residual suprapubic pain, sexual disturbance, impo-tence) of implant retention, to review indicationsfor implant removal, to correlate any long-termeffects with implant failure and to examine theissue of implant removal in pregnant women.
Methods
We surveyed the literature using Medline, CINAHL,OVID, ADITUS search engines and Cochrane data-bases from 1966 to the present. The following keywords were used in the search: ‘symphysis rupture’,‘plate removal’, ‘symphysis plating’, ‘pubic plate’,‘effects of plate’, ‘sex and plate’, ‘pregnancy andplate’, ‘impotence and plate’, ‘pubic diastasis’,‘implant failure’ and ‘pelvic fracture’.
The inclusion criteria for references were thefollowing: references describing internal stabilisa-tion of the anterior pelvis, follow-up of at least 6months, case reports with a review of the literature,case series, prospective studies and retrospectivestudies. The exclusion criteria were: isolated casereports, cases with less than 6 months follow up andreferences, which did not fulfil at least one of theinclusion criteria.
Each reference was analysed. The following para-meters were recorded: the number of patients inthe study, type of injury, method of stabilisation ofthe anterior pelvic ring, complications, implant fail-ure, residual pain at latest follow-up, sexual dis-turbances and impotence, and the relationship ofpregnancy to implant removal.
Results
Based on these criteria, we found 24 case series and2 case reports included in the 26 references that weidentified.1,3,6,8—16,19—26,30,32,33,36—38 Twenty-onereferences reported on traumatic diastasis of thesymphysis while three articles described rupture ofsymphysis at labour.22,25,32 Two referencesdescribed stabilisation of the symphysis secondaryto osteitis.1,38 All patients in the selected studieshad the anterior ring internally stabilised. Stabilisa-tion by plate osteosynthesis was reported in 24articles, while one article described stabilisationusing tension band wires31 and another using Kirsch-ner wires, PDS suture material and PDS bands.13 Atotal of 482 cases were identified. The mean follow-up was 68 months (6—154 months).
Complications were described in all but onereference.14 Superficial infection was reported in
nine (2.2%) patients13,19,21,23,24,37 and deep infec-tion in six (1.6%).13,19,32 Implant failure wasdescribed in only 12 articles (46.1%).6,13,16,19,21—24,31,32,36,38 A total of 16 (5.7%) implant failureshave been described out of 277 cases in these 12articles. Residual pain (suprapubic pain) wasaddressed in 19 (73%) articles.3,6,8,11—13,16,19—25,31,33,36—38 There were 32 cases of residual painattributed to the anterior symphysis stabilisationdevice. Problems during sexual intercourse andimpotence were described in five references(21.2%).16,21,23,24,33 Twelve patients had sexual dys-function: five patients had deep dyspareunia andseven had erectile impotence.4 Of the 12 patientswith sexual problems, 9 patients had coexistentgenitourinary injuries.
Only two (7.6%) articles addressed the issue ofpregnancy in their patient groups.19,24 The platewas removed electively in one patient24 and twopatients had an uneventful ante and postnatal per-iod with the implant in situ.19,21
Plate removal was discussed in 15 studies(58%).3,8—10,12—15,19,21,23—25,32,33 Implants wereremoved in 17 patients.8,15,21,23—25 Fifteen of thesepatients had significant anterior pain. Implant failurewas reported in nine patients and infection in onepatient.21,24 Four patients had their implantsremoved electively (three females and onechild).8,15,24,25
Discussion
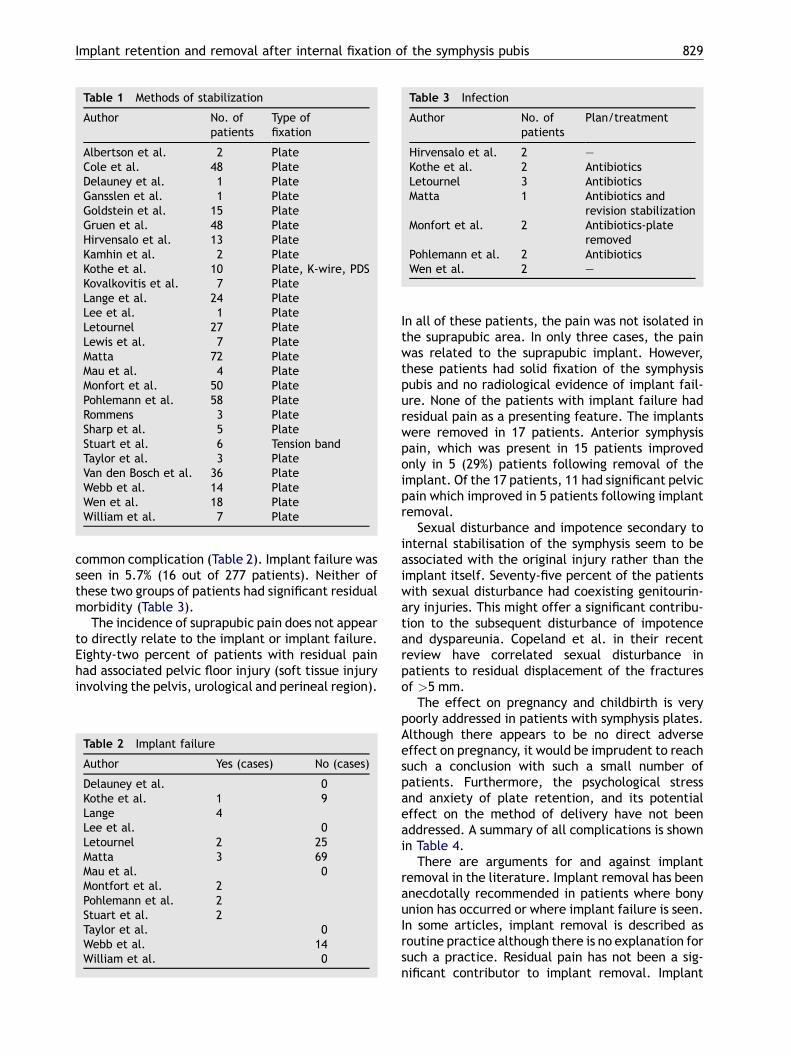
There is a plethora of information in the literatureon the biomechanics of the symphysis pubis andmethods of stabilisation of the symphysis. The beha-viour of various modes of fixation and their failureshas been extensively studied. For the stabilisation ofthe ruptured pubic symphysis, rigid forms of fixationsuch as plate osteosynthesis and flexible fixationssuch as wire loops or PDS banding have been recom-mended (Table 1).5,26,27,29—31,35—37
Long-term effects of implant retention and its rolein pregnant women have only been given cursoryattention in the current literature. Sharp havedescribed plate osteosynthesis of the symphysis dia-stasis as early as 1973.26However, subsequent studieshave failed to highlight the effects of plate retentionin patients with respect to pain, impotence andpregnancy. Four references were case series, withpatient numbers greater than 50.19,21,23,24 This pau-city of information in the current literature makes itdifficult to reach a definitive answer to the questionof implant removal following bony union.
Complications arose as a result of implant reten-tion in 7.5% of the patients, with infection the most
Implant retention and removal after internal fixation of the symphysis pubis 829
Table 1 Methods of stabilization
Author No. ofpatients
Type offixation
Albertson et al. 2 PlateCole et al. 48 PlateDelauney et al. 1 PlateGansslen et al. 1 PlateGoldstein et al. 15 PlateGruen et al. 48 PlateHirvensalo et al. 13 PlateKamhin et al. 2 PlateKothe et al. 10 Plate, K-wire, PDSKovalkovitis et al. 7 PlateLange et al. 24 PlateLee et al. 1 PlateLetournel 27 PlateLewis et al. 7 PlateMatta 72 PlateMau et al. 4 PlateMonfort et al. 50 PlatePohlemann et al. 58 PlateRommens 3 PlateSharp et al. 5 PlateStuart et al. 6 Tension bandTaylor et al. 3 PlateVan den Bosch et al. 36 PlateWebb et al. 14 PlateWen et al. 18 PlateWilliam et al. 7 Plate
Table 3 Infection
Author No. ofpatients
Plan/treatment
Hirvensalo et al. 2 —Kothe et al. 2 AntibioticsLetournel 3 AntibioticsMatta 1 Antibiotics and
revision stabilizationMonfort et al. 2 Antibiotics-plate
removedPohlemann et al. 2 AntibioticsWen et al. 2 —
common complication (Table 2). Implant failure wasseen in 5.7% (16 out of 277 patients). Neither ofthese two groups of patients had significant residualmorbidity (Table 3).
The incidence of suprapubic pain does not appearto directly relate to the implant or implant failure.Eighty-two percent of patients with residual painhad associated pelvic floor injury (soft tissue injuryinvolving the pelvis, urological and perineal region).
Table 2 Implant failure
Author Yes (cases) No (cases)
Delauney et al. 0Kothe et al. 1 9Lange 4Lee et al. 0Letournel 2 25Matta 3 69Mau et al. 0Montfort et al. 2Pohlemann et al. 2Stuart et al. 2Taylor et al. 0Webb et al. 14William et al. 0
In all of these patients, the pain was not isolated inthe suprapubic area. In only three cases, the painwas related to the suprapubic implant. However,these patients had solid fixation of the symphysispubis and no radiological evidence of implant fail-ure. None of the patients with implant failure hadresidual pain as a presenting feature. The implantswere removed in 17 patients. Anterior symphysispain, which was present in 15 patients improvedonly in 5 (29%) patients following removal of theimplant. Of the 17 patients, 11 had significant pelvicpain which improved in 5 patients following implantremoval.
Sexual disturbance and impotence secondary tointernal stabilisation of the symphysis seem to beassociated with the original injury rather than theimplant itself. Seventy-five percent of the patientswith sexual disturbance had coexisting genitourin-ary injuries. This might offer a significant contribu-tion to the subsequent disturbance of impotenceand dyspareunia. Copeland et al. in their recentreview have correlated sexual disturbance inpatients to residual displacement of the fracturesof >5 mm.
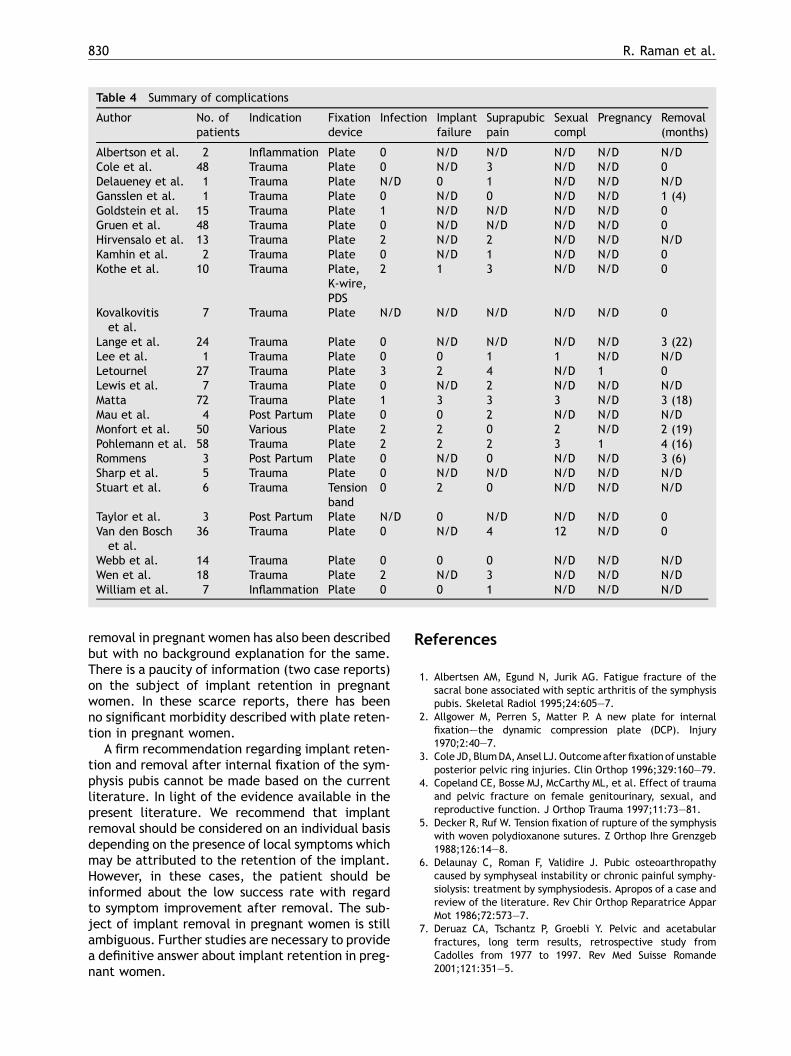
The effect on pregnancy and childbirth is verypoorly addressed in patients with symphysis plates.Although there appears to be no direct adverseeffect on pregnancy, it would be imprudent to reachsuch a conclusion with such a small number ofpatients. Furthermore, the psychological stressand anxiety of plate retention, and its potentialeffect on the method of delivery have not beenaddressed. A summary of all complications is shownin Table 4.
There are arguments for and against implantremoval in the literature. Implant removal has beenanecdotally recommended in patients where bonyunion has occurred or where implant failure is seen.In some articles, implant removal is described asroutine practice although there is no explanation forsuch a practice. Residual pain has not been a sig-nificant contributor to implant removal. Implant
830 R. Raman et al.
Table 4 Summary of complications
Author No. ofpatients
Indication Fixationdevice
Infection Implantfailure
Suprapubicpain
Sexualcompl
Pregnancy Removal(months)
Albertson et al. 2 Inflammation Plate 0 N/D N/D N/D N/D N/DCole et al. 48 Trauma Plate 0 N/D 3 N/D N/D 0Delaueney et al. 1 Trauma Plate N/D 0 1 N/D N/D N/DGansslen et al. 1 Trauma Plate 0 N/D 0 N/D N/D 1 (4)Goldstein et al. 15 Trauma Plate 1 N/D N/D N/D N/D 0Gruen et al. 48 Trauma Plate 0 N/D N/D N/D N/D 0Hirvensalo et al. 13 Trauma Plate 2 N/D 2 N/D N/D N/DKamhin et al. 2 Trauma Plate 0 N/D 1 N/D N/D 0Kothe et al. 10 Trauma Plate,
K-wire,PDS
2 1 3 N/D N/D 0
Kovalkovitiset al.
7 Trauma Plate N/D N/D N/D N/D N/D 0
Lange et al. 24 Trauma Plate 0 N/D N/D N/D N/D 3 (22)Lee et al. 1 Trauma Plate 0 0 1 1 N/D N/DLetournel 27 Trauma Plate 3 2 4 N/D 1 0Lewis et al. 7 Trauma Plate 0 N/D 2 N/D N/D N/DMatta 72 Trauma Plate 1 3 3 3 N/D 3 (18)Mau et al. 4 Post Partum Plate 0 0 2 N/D N/D N/DMonfort et al. 50 Various Plate 2 2 0 2 N/D 2 (19)Pohlemann et al. 58 Trauma Plate 2 2 2 3 1 4 (16)Rommens 3 Post Partum Plate 0 N/D 0 N/D N/D 3 (6)Sharp et al. 5 Trauma Plate 0 N/D N/D N/D N/D N/DStuart et al. 6 Trauma Tension
band0 2 0 N/D N/D N/D
Taylor et al. 3 Post Partum Plate N/D 0 N/D N/D N/D 0Van den Bosch
et al.36 Trauma Plate 0 N/D 4 12 N/D 0
Webb et al. 14 Trauma Plate 0 0 0 N/D N/D N/DWen et al. 18 Trauma Plate 2 N/D 3 N/D N/D N/DWilliam et al. 7 Inflammation Plate 0 0 1 N/D N/D N/D
removal in pregnant women has also been describedbut with no background explanation for the same.There is a paucity of information (two case reports)on the subject of implant retention in pregnantwomen. In these scarce reports, there has beenno significant morbidity described with plate reten-tion in pregnant women.
A firm recommendation regarding implant reten-tion and removal after internal fixation of the sym-physis pubis cannot be made based on the currentliterature. In light of the evidence available in thepresent literature. We recommend that implantremoval should be considered on an individual basisdepending on the presence of local symptoms whichmay be attributed to the retention of the implant.However, in these cases, the patient should beinformed about the low success rate with regardto symptom improvement after removal. The sub-ject of implant removal in pregnant women is stillambiguous. Further studies are necessary to providea definitive answer about implant retention in preg-nant women.
References
1. Albertsen AM, Egund N, Jurik AG. Fatigue fracture of thesacral bone associated with septic arthritis of the symphysispubis. Skeletal Radiol 1995;24:605—7.
2. Allgower M, Perren S, Matter P. A new plate for internalfixation–—the dynamic compression plate (DCP). Injury1970;2:40—7.
3. Cole JD, BlumDA,Ansel LJ.Outcomeafterfixationof unstableposterior pelvic ring injuries. Clin Orthop 1996;329:160—79.
4. Copeland CE, Bosse MJ, McCarthy ML, et al. Effect of traumaand pelvic fracture on female genitourinary, sexual, andreproductive function. J Orthop Trauma 1997;11:73—81.
5. Decker R, Ruf W. Tension fixation of rupture of the symphysiswith woven polydioxanone sutures. Z Orthop Ihre Grenzgeb1988;126:14—8.
6. Delaunay C, Roman F, Validire J. Pubic osteoarthropathycaused by symphyseal instability or chronic painful symphy-siolysis: treatment by symphysiodesis. Apropos of a case andreview of the literature. Rev Chir Orthop Reparatrice ApparMot 1986;72:573—7.
7. Deruaz CA, Tschantz P, Groebli Y. Pelvic and acetabularfractures, long term results, retrospective study fromCadolles from 1977 to 1997. Rev Med Suisse Romande2001;121:351—5.
Implant retention and removal after internal fixation of the symphysis pubis 831
8. Gansslen A, Pohlemann T, Hufner T, et al. Internal osteosynth-esis after unstable pelvic ring fracture in a 3-year-old child.Unfallchirurg 1998;101:570—3.
9. Goldstein A, Phillips T, Sclafani SJ, et al. Early open reductionand internal fixation of the disrupted pelvic ring. J Trauma1986;26:325—33.
10. Gruen GS, Leit ME, Gruen RJ, et al. Functional outcome ofpatients with unstable pelvic ring fractures stabilized withopen reduction and internal fixation. J Trauma 1995;39:838—44. discussion 844—5.
11. Hirvensalo E, Lindahl J, Bostman O. A new approach to theinternal fixation of unstable pelvic fractures. Clin Orthop1993;297:28—32.
12. Kamhin M, Ganel A, Salai M, Horoszowski H. Rigid fixation indiastasis of symphysis pubis. J Trauma 1980;20:523—5.
13. Kothe S, Keller HW, Heindel W, Rehm KE. Experience withsurgical treatment of ruptures of the symphysis pubis. Zen-tralbl Chir 1994;119:37—43.
14. Kovalkovitis I, Tozser K, Miksi G, Frey J. Rigid internal fixationof symphysiolysis. Magy Traumatol Orthop Helyreallito Seb1981;24:23—7.
15. Lange RH, Hansen Jr ST. Pelvic ring disruptions with symphysispubis diastasis. Indications, technique, and limitations ofanterior internal fixation. Clin Orthop 1985;201:130—7.
16. Lee J, Abrahamson BS, Harrington TG, et al. Urologic com-plications of diastasis of the public symphysis: a trauma casereport and review of world literature. J Trauma2000;48:133—6.
17. Leighton RK, Waddell JP, Bray TJ, et al. Biomechanical test-ing of new and old fixation devices for vertical shear fracturesof the pelvis. J Orthop Trauma 1991;5:313—7.
18. Leighton RL. Surgical treatment of some pelvic fractures. JAm Vet Med Assoc 1968;153:1739—41.
19. Letournel E. Surgical fixation of displaced pelvic fracturesand dislocations of the symphysis pubis (excluding acetabularfractures). Rev Chir Orthop Reparatrice Appar Mot1981;67:771—82.
20. Lewis MM, Mayer V. Pubic symphysis diastasis treated by openreduction and internal fixation. Clin Orthop 1977;123:37—9.
21. Matta JM. Indications for anterior fixation of pelvic fractures.Clin Orthop 1996;329:88—96.
22. Mau C, Ovesen J, Jensen J. Rupture of the symphysis afterspontaneous delivery surgical treatment of four cases.Ugeskr Laeger 2001;163:1442—3.
23. Monfort J, Le Neel JC, Leborgne J, et al. Recent disjunctionsof the pubic symphysis. Therapeutic indications apropos of 50cases. Ann Chir 1973;27:601—8.
24. Pohlemann T, Bosch U, Gansslen A, Tscherne H. The Hannoverexperience in management of pelvic fractures. Clin Orthop1994;305:69—80.
25. Rommens PM. Internal fixation in postpartum symphysis pubisrupture: report of three cases. J Orthop Trauma1997;11:273—6.
26. Sharp IK. Plate fixation of disrupted symphysis pubis preli-minary report. J Bone Joint Surg Br 1973;55:618—20.
27. Simonian PT, Routt Jr ML, Harrington RM, Tencer AF. Boxplate fixation of the symphysis pubis: biomechanicalevaluation of a new technique. J Orthop Trauma 1994;8:483—9.
28. Simonian PT, Routt Jr ML, Harrington RM, Tencer AF. Internalfixation of the unstable anterior pelvic ring: a biomechanicalcomparison of standard plating techniques and the retro-grade medullary superior pubic ramus screw. J OrthopTrauma 1994;8:476—82.
29. Simonian PT, Schwappach JR, Routt Jr ML, et al. Evaluation ofnew plate designs for symphysis pubis internal fixation. JTrauma 1996;41:498—502.
30. Stocks GW, Gabel GT, Noble PC, et al. Anterior and posteriorinternal fixation of vertical shear fractures of the pelvis. JOrthop Res 1991;9:237—45.
31. Stuart PR, Talbot D, Milne DD. Internal fixation of pubicsymphysis diastasis with a tension banding technique. Injury1990;21:223—4.
32. Taylor RN, Sonson RD. Separation of the pubic symphysis. Anunderrecognized peripartum complication. J Reprod Med1986;31:203—6.
33. Van den Bosch EW, Van der Kleyn R, Hogervorst M, Van VugtAB. Functional outcome of internal fixation for pelvic ringfractures. J Trauma 1999;47:365—71.
34. Varga E, Hearn T, Powell J, Tile M. Effects of method ofinternal fixation of symphyseal disruptions on stability of thepelvic ring. Injury 1995;26:75—80.
35. Waikakul S, Soparat K, Harnroongroj T. Anterior stabilizationin the pubic symphysis separation: a mechanical testing. JMed Assoc Thai 1999;82:72—9.
36. Webb LX, Gristina AG, Wilson JR, et al. Two-hole platefixation for traumatic symphysis pubis diastasis. J Trauma1988;28:813—7.
37. Wen Y, Liu X, Ge B, et al. A newer plate system for internalfixation of un-stable pelvic fractures. Int Surg 1998;83:88—90.
38. Williams PR, Thomas DP, Downes EM. Osteitis pubis andinstability of the pubic symphysis. When nonoperative mea-sures fail. Am J Sports Med 2000;28:350—5.