implications of c. difficile diagnostic testing
DESCRIPTION
Implications of C. difficile diagnostic testing. Not seeing the wood for the trees Warren Lowman Pathlink / Vermaak & Partners Pathologists Wits Donald Gordon Medical Centre Clinical Microbiology & Infectious Diseases, University of the Witwatersrand. Pubmed & C. difficile. 9298 hits - PowerPoint PPT PresentationTRANSCRIPT

Implications of C. difficile diagnostic testing
Not seeing the wood for the trees
Warren LowmanPathlink/ Vermaak & Partners Pathologists
Wits Donald Gordon Medical CentreClinical Microbiology & Infectious Diseases, University of the
Witwatersrand
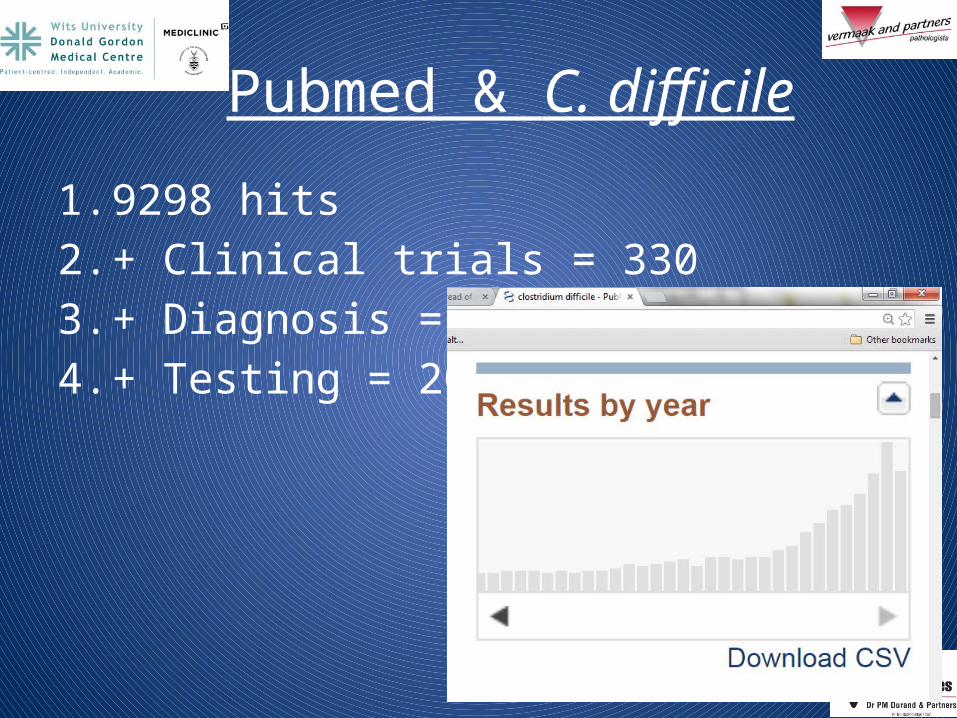
Pubmed & C. difficile
1. 9298 hits2. + Clinical trials = 3303. + Diagnosis = 1694. + Testing = 20
Clinical relevance…
2 key issues that are largely ignored:–Pre-test probability–PPV

ICU HC Surgical Medical Oncology0
20
40
60
80
100
120
C. diff pos+C. diff requestsN
o.
Are we selecting accurately?
67.1 tests/ 10 000 pt bed days (range, 29 – 153)

C. difficile diagnostics…
1. We are floundering- survey of UK labs indicate >25 different algorithms
2. Multitude of different assays3. Impacts on our understanding of the
epidemiology of CDI.
Jan Feb Mar AprMay Jun Jul AugSeptOct Nov Dec0
2
4
6
8
10
12
C. diff Rate/ 10 000 patient days
Rate (/10 000 pt days)2013 Cumulative rate
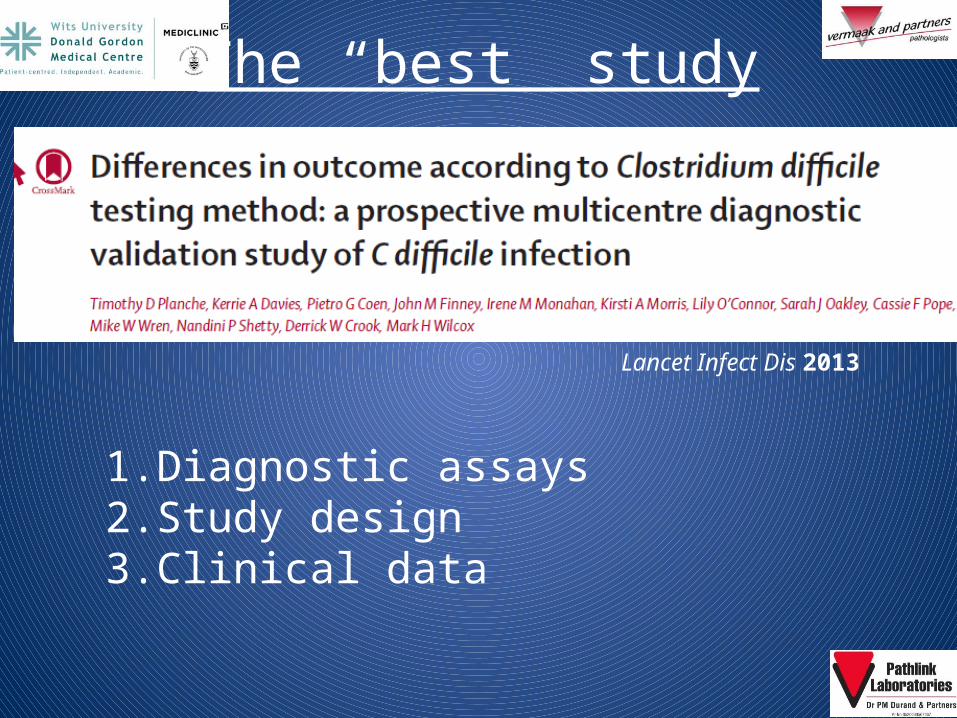
The “best” study
Lancet Infect Dis 2013
1.Diagnostic assays2.Study design3.Clinical data

Salient points
1. Tested all faecal samples irrespective of request
2. Wide scope of practice3. Detection of 3 targets: bacterium; toxin; gene4. Predefined groups: diagnostic; severity5. Statistically very “sound”6. Diagnostic performance assessed in training
phase

Clinical relevance by assay
1. Data for 6522 inpatient episodes
Variable Grp1 vs Grp2 Grp1 vs Grp3
Mean WCC 0.0004 <0.0001
Died 0.022 <0.0001
Death rate 0.0195 0.0033

…clinical relevance by assay1. Same comparison using PCR as surrogate for
cytotoxigenic culture
Variable Grp1 vs Grp2 Grp1 vs Grp3
Mean WCC <0.0001 <0.0001
Died 0.004 <0.0001
Death rate 0.0317 0.0018

The point…clinically

So what do we do about diagnosis?

What’s best?
Performance GDH + EIA NAAT + EIA
Sensitivity 81.8% 82.9%
Specificity 99.5% 99.6%
PPV 91.6% 92.1%
NPV 98.9% 98.9%
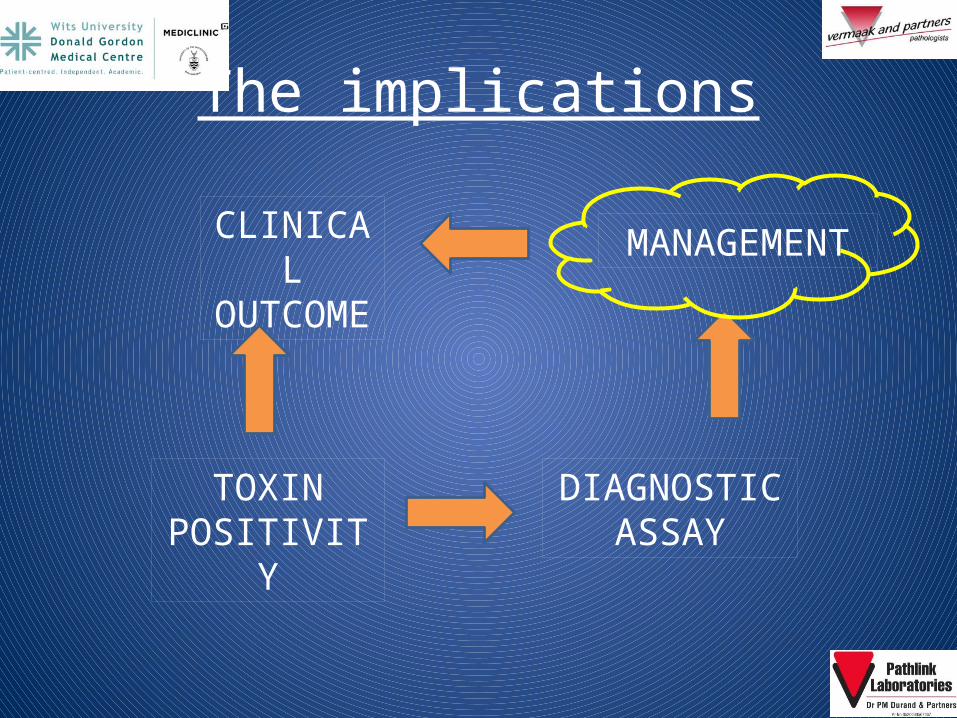
The implications
TOXIN POSITIVITY
DIAGNOSTIC ASSAY
CLINICAL OUTCOME
MANAGEMENT

C. difficile excretors…an issue?
Overtreatment…excessive antibiotic use!Cost…this all adds up
GDH EIA Toxin PCR
POSITIVE 14 7 14
NEGATIVE 11 18 11

3-stage algorithmGDH
EIA Toxin
Not CDAD
CDAD
NAAT
C. difficile excretor
Not CDAD8%

Thank you!