important telephone numbers - north · web viewthese particles are termed “quantum...
TRANSCRIPT

Research Service (151)
Laboratory Safety Manual
2015-2016
Note: The policies and procedures within this manual apply to laboratory research conducted in VA facilities. The University of Florida’s laboratory safety, radiation safety, and waste management policies differ. It is the responsibility of the investigators to be knowledgeable of the differences and adjust their behavior accordingly.

IMPORTANT TELEPHONE NUMBERS
EMERGENCY: EXT. 6911 FIRE: EXT. 6333 VA POLICE: EXT. 4901
EMERGENCY CALL ASSISTANT (AFTER HOURS):........................................................EXT. 6724ENGINEERING TROUBLE DESK:......................................................................................EXT. 6025ENVIRONMENT MANAGEMENT (EMS):........................................EXT. 6017, VA PAGER 32-1362GRAPHIC CONTROL (AFTER HOURS LAB EMERGENCY):...........................................EXT. 6616RESEARCH SERVICE OFFICE...........................................................................................EXT. 6069
Administrative Officer, Research Marie Johnson (352) 548-6476After Hours: (352) 262-3905
Email: [email protected]
Animal Care Services for NF/SG VHS Mike Riley CVT, LATG Tele: (352) 273-9242Facility Manager On-call Pager: 352-413-0824
After Hours: (352) 258-3287Email: [email protected]
Associate Chief of Staff, Research Dr. Stephen E. Nadeau, MD (352) 548-6069After Hours: (352) 514-5611
Email: [email protected]@ufl.edu
Associate Biosafety Officer Dr. Bhavna Bhardwaj Tele: 392-1591; UF EH&SEmail: [email protected]
Biosafety Officer, Alternate Karen Gillis Tele: 392-1591; UF EH&SEmail: [email protected]
Chemical Hygiene Officer, Research Dr. Kamal Mohammed Ext.: 7446; Room: D106-1After Hours: 352-256-2030
Email: [email protected]
Employee Health Office Gale Hockman, RN Ext.: 7359; Room: F110-1After Hours: (352) 473-9792
Email:[email protected]
Health Physicist, Nuclear Medicine David F. Watson Ext.: 6806; Room: A05-1Email: [email protected]
Institutional Animal Care & Use Committee (IACUC) Chair
Dr. Prodip Bose Ext. 5996
Email: [email protected]@ufl.edu
Institutional Animal Care & Use Committee (IACUC) Coordinator
Christopher Johnston (352) 548-6481
After Hours: (352) 870-1756Email: [email protected]
Key Control Coordinator & Research PIV Sponsor for WOC
Wanda Thomas Ext:. 4204 (Cisco phone)
Email: [email protected] Control Officer Daniel Zwickel , Physical Security Specialist/Police Service
Office: 352-745-8869 Cell: 352-745-8869 Email: [email protected]
Research PIV Sponsor Charisma Brown Ext: 6960 email: [email protected]
Laboratory Safety Officer Dr. Shen-Ling Xia Ext.: 6581After Hours: (352) 413-6679
Email: xiasl@ ufl.edu or [email protected]

IMPORTANT TELEPHONE NUMBERS, continued
Radiation Safety Officer Dr. Shailendra Shukla Ext.: 6514/6059, Room: T3-09VA Pager: 32-1747
After Hours (352) 331-8350 Email: [email protected]
Industrial Hygienist Bruce M. Carlberg Ext.: 4309/6025; Room: EB-59i-1After Hours Pager: 32-4840; Nights/Weekends/ Holidays,
call, Graphic Control at Ext. 6616, ask that Mr. Carlberg be contacted.Email: [email protected]
Safety Officer/Safety & Occupational Health Specialist
Darrell F. Crimmins Ext.: 6560; Room: EB100-1Cell: 352-260-7435
Email: [email protected] on Research Safety (SRS) Chair
Dr. Kamal Mohammed Ext.: 7446; Room: D106-1
After Hours: 352-256-2030Email: [email protected]
Subcommittee on Research Safety (SRS) Coordinator
Christopher Johnston (352) 548-6481
After Hours: (352) 870-1756Email: [email protected]
SRS – Research Service Liaison(SRS Forms and Documents)
TBA Ext.:TBA; Room: TBA
Email: TBAVMU Staff Anthony Mejia Ext.: 6495; Room: VMU
Email: [email protected]
WOC Coordinator Wanda Thomas Ext.: 4204 (Cisco phone)Email: [email protected]
Research Services: Laboratory Safety Manual Page iii

RESEARCH SERVICE SAFETY POLICIES AND PROCEDURES
Table of Contents
IMPORTANT TELEPHONE NUMBERS IVFOLLOW-UP RESPONSIBILITY FOR THE LABORATORY SAFETY MANUAL VIII
SECTION I. INTRODUCTION 1
PURPOSE OF RESEARCH SAFETY 1ADMINISTRATIVE 3LABORATORY SAFETY CONSENT FORM 4GUIDELINES FOR SAFETY TRAINING 5BIOSAFETY QUIZ 7
SECTION II. SAFETY PROCEDURES 13
PERSONAL SAFETY AND HEALTH PRACTICES 13BLOODBOURNE PATHOGENS 15USE AND HANDLING OF INFECTIOUS/POTENTIALLY INFECTIOUS MATERIALS 16INFECTION CONTROL 17SAFETY POLICY FOR WORKING WITH NANOMATERIALS 19HAZARDOUS CHEMICALS 31HAZARDOUS AGENTS REPORTING 33LABORATORY EQUIPMENT OPERATIONS 35CHEMICAL WASTE DISPOSAL 36BIOLOGICAL HAZARD DISPOSAL 36RADIOISOTOPES 37IN VIVO ANIMAL PROCEDURES WITH USE OF RADIOISOTOPES 39LIQUID NITROGEN (LN2) SAFETY PLAN 40
SECTION III. CHEMICAL HYGIENE PLAN (CHP) 47
TABLE OF CONTENTS 47I. GENERAL PRINCIPLES 49II. RESPONSIBILITIES 50III. THE RESEARCH SERVICE FACILITY 51IV. COMPONENTS OF THE CHEMICAL HYGIENE PLAN 52V. GENERAL PROCEDURES FOR WORKING WITH CHEMICALS AND HAZARDOUS AGENTS 64VI. SAFETY RECOMMENDATIONS 70VII. TECHNICAL GUIDANCE 72REFERENCES 72OSHA WEB SITE 73CHEMICAL HYGIENE PLAN – SIGNATURE SHEET 75
75APPENDIX A. HAZARDOUS MATERIALS DATA: INFORMATION AND RECOMMENDED FORM 77
SECTION. IV. ANIMAL SAFETY PROCEDURES 81
Research Services: Laboratory Safety Manual Page iv

ANIMAL FACILITY SAFETY 81CARE OF ANIMALS DURING EMERGENCIES 82ANIMAL BIOSAFETY LEVELS 83VMU PERSONNEL HEALTH ASSESSMENT 88INJURIES CAUSED BY RESEARCH ANIMALS 89TRAINING FOR ANIMAL USE AND CARE 91REFERENCES 91CONTACTS 91
SECTION V. SECURITY PROCEDURES 93
RESEARCH LAB AND ANIMAL FACILITY SECURITY 93BIOHAZARDS MATERIAL TRANSPORTATION AND SHIPPING 94RESEARCH VISITOR POLICY 95SOP FOR RESEARCH KEY CONTROL 96
SECTION VI. MEDICAL RESEARCH SUPPLEMENTAL DISASTER PLAN 99
A. GENERAL SUPPLEMENT 99B. SPECIFIC SUPPLEMENT 100
SECTION VII. COMMON RESOURCE EQUIPMENT 105
COMMON RESOURCE EQUIPMENT PROCEDURES 105LIST OF COMMON RESOURCE EQUIPMENT 106
SECTION VIII. SUBCOMMITTEE ON RESEARCH SAFETY STANDARD OPERATING PROCEDURES 109
PURPOSE 109BACKGROUND 109DEFINITIONS AND ACRONYMS 110RESPONSIBILITIES IN REGARD TO SAFETY OF PERSONNEL ENGAGED IN RESEARCH 113SRS MEMBERSHIP 116SRS AGENDA AND MINUTES 117TRAINING 118PROCESS FOR RESEARCH PROTOCOL SAFETY EVALUATIONS 119PROCESS FOR RESEARCH PROTOCOL SAFETY EVALUATIONS TABLES AND DECISION TABLES 123REFERENCES 129FOLLOW-UP RESPONSIBILITY 129
SECTION IX. MEMORANDUM OF UNDERSTANDING BETWEEN NF/SG VHS AND UF CONCERNING THE USE OF UF INSTITUTIONAL BIOSAFETY COMMITTEE 131
SECTION X. NF/SG VHS SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETY 135
SECTION XI. ACRONYMS 145
Research Services: Laboratory Safety Manual Page v

FOLLOW-UP RESPONSIBILITY FOR THE LABORATORY SAFETY MANUAL
The Subcommittee on Research Safety and the Laboratory Safety Officer are responsible for the annual review and revision of the Laboratory Safety Manual as needed.
Review/Revision: 10/24/2008 Review/Revision: 11/25/2009 Review/Revision: 05/24/2010 Review/Revision: 01/28/2011Review/Revision: 02/27/2012Review/Revision: 04/01/2013Review/Updated: 12/18/2014Review/Updated: 04/23/2015Review/Updated: 06/25/2015
Research Services: Laboratory Safety Manual Page vi
Research Services: Laboratory Safety Manual Page vii
SECTION I. INTRODUCTION
PURPOSE OF RESEARCH SAFETY
VHA Handbook 1200.8, issued March 6, 2009, mandates that VA Research Services must maintain a Research Safety Program that is consistent with VA Policies, Federal, State and Local Statues; and Regulations from Occupational Safety and Health Administration, the Environmental Protection Agency, and the Nuclear Regulatory Commission.
In compliance with this mandate, a service-wide Safety Manual must be developed, updated, reviewed and approved annually by the Subcommittee on Research Safety and forwarded to the Research & Development Committee for approval.
This Research Laboratory manual serves as a resource and reference to assist in the minimization of risk associated with the VA Research Service employees’ daily responsibilities.
References: VHA Handbook 1200.06, “Control of Hazardous Agents in VA Research Laboratories,”
October 21, 2005-October 31, 2010. Biosafety in Microbiological and Biomedical Laboratories (BMBL), Section VI, 5 th Edition,
December 2009. VHA Handbook 1200.8, “Safety of Personnel Engaged in Research,” March 6, 2009-
March 31, 2010.
This document has been designed to provide you with basic elements of laboratory safety and the policies and procedures that govern this facility. All laboratory-associated personnel must be familiar with the Laboratory Safety Manual. A copy of the Laboratory Safety manual must be kept in each laboratory. The most effective safety precaution is the use of common sense. Ask questions if you are unsure of something. Your well-being and that of your fellow laboratory workers are of the utmost importance to Research and Medical Center Management. It is your responsibility to read, understand and adhere to the practices and procedures in this manual. Failure to comply with the following practices and procedures may result in suspension and/or termination of research activity per VHA Handbook 1058.01, titled, “Research Compliance Reporting Requirements (Nov. 15, 2011).”
All laboratory personnel (including VA paid, paid through UF, WOCs, students, volunteers, etc.) must sign the Laboratory Safety Consent Form (page 4), the supervisor must sign it, and submit the signed and dated form to the Research Safety Coordinator, Research Office (125B-14).
All personnel (including VA paid, paid through UF, WOCs, students, volunteers, etc.) must attend the annual Mandatory Review. This is also available online. In addition, Research Service may sponsor other safety training and retraining sessions throughout the year. All employees must attend these sessions when offered. It is important to know about hazardous and toxic substances present in your work site, and you must be trained in their safe use by your supervisor, and you must take the online biosafety training on the CITI Research Services: Laboratory Safety Manual Page 1

Website (http://www.citiprogram.org). This is a mandatory one time online training that must be taken by all VA-paid and WOC employees who work in VA research labs, work with hazardous agents including select agents or toxins, work in BSL-2 labs, and all employees that have administrative duties associated with labs. See pages 5 and 6 for more information on the required safety training (Guidelines for Safety Training).Copies of the NF/SG VHS Research Service Laboratory Safety Manual can be found in the Research Safety/IACUC Coordinator’s Office in Room 125B-14. The manual consists of the following Sections that are either written specifically for the Research Service or adopted from Environment of Care (EOC) Manual, NF/SG Veterans Health Care System:
I. Introduction
II. Safety Procedures
III. Chemical Hygiene Plan (CHP)
IV. Animal Safety Procedures
V. Security Procedures
VI. Medical Research Supplemental Disaster Plan
VII. Common Resource Equipment
VIII. Subcommittee on Research Safety - SOP
XI. Memorandum of Understanding Between the NF/SG VHS and UF for the Use of the UF Institutional Biosafety Committee (IBC)
X. NF/SG VHS SRS Laboratory Inspection Checklist for Research Safety
XI. Acronyms
Research Services: Laboratory Safety Manual Page 2

ADMINISTRATIVEA. All new lab personnel must be either a paid VA employee or a WOC with the Research
Office prior to beginning any duties.
B. Key Cards to the Research lab area are only issued to personnel approved by the Research Service Office. Personnel who are not VA employees must have an approved WOC (WithOut Compensation) appointment set up before they can be issued key cards. See WOC Coordinator, Wanda Thomas, Room 122-14, for the WOC Application Forms.
C. All personnel are responsible for the key cards issued to them. Key cards are not to be loaned to other individuals.
D. Lost or stolen key cards must immediately be reported to Wanda Thomas – Key Control Officer, WOC Coordinator, Ext. 4204, Email: [email protected].
E. Key cards must be returned on your last day to Wanda Thomas (Room 122-14; Ext. 4204) or Chris Johnston (Room 125B-14; Ext. 6481).
F. Make sure you give your e-mail address to the WOC Coordinator or Research Service HR Coordinator when you are first hired. Please read your VA email on a regular basis. Most announcements from the VA Research Administrative Office are sent out via VA Email.
G. Wear your VA Identification badge at all times.
H. It is required for your VA badge to be valid for one year from the date of issue. Your key card to the Research lab area will be programmed to deactivate 11 days after your badge expiration date. When your badge is about to expire, please see Wanda Thomas to renew your badge and your key card.
I. There are some common refrigerators and microwaves available for your use for food in Room B065-1 (Basement), Room EB79-1 (Basement) AND Room E594-1 (5 th Floor), if you do not have an office space or your office does not have them. Remember: NO food or drink is allowed in the lab.
J. Children age 18 and below are NOT permitted in the laboratory areas. PI’s must obtain prior approval from Research Service for minor volunteers (students) seeking to work in their laboratory.
K. Unauthorized personnel are not permitted in the laboratory areas.
Research Services: Laboratory Safety Manual Page 3

RESEARCH SERVICE (151)
LABORATORY SAFETY CONSENT FORM
I have read the Research Service Laboratory Procedures Manual and have discussed its contents with my supervisor. I understand that the procedures and safety measures must be performed as described and that failure to comply may result in suspension of research activity in my laboratory at the NF/SG Veterans Health System, Gainesville VAMC, Research Service.
I agree to return all keys/access cards and ID Badges issued to me at the end of my employment.
Date:
Employee Signature:
Employee Name (Print):
Employee E-mail Address:
Supervisor Signature:
Supervisor Name (Print):
Lab Room Number:
NOTE: Each laboratory employee must complete this page and submit it to the SRS Coordinator (Room E554-1, Research Service) no later than one month after receiving the revised Lab Safety Manual. Keep the rest of the Manual in your Lab as a reference.
Research Services: Laboratory Safety Manual Page 4

GUIDELINES FOR SAFETY TRAININGNF/SGVHS Subcommittee on Research SafetyAPPROVED BY THE SUBCOMMITTEE ON RESEARCH SAFETY ON MARCH 28, 2013
REQUIRED FOR FREQUENCY TRAINING TITLE METHOD
TRAINING REQUIRED WHEN FIRST HIRED OR STARTING A NEW POSITIONAll VA-Paid and WOC employees who work in VA biological research labs*, work with hazardous agents including select agents or toxins, work in BSL-2 labs, and all employees that have administrative duties associated with such labs.
Initially** andOnly One Time
(within 30 daysof hire)
VA ORD BioSecurity Training, Basic Course
CITIhttp://www.citiprogram.org
All VA-Paid and WOC employees who are responsible for shipping (sending) bio-hazardous materials in VA labs
Initially(within 30 days
of hire)
VA Biohazard Shipping Training
CITIhttp://www.citiprogram.org
All VA-Paid and WOC employees who work with human or non-human primate blood, body fluids, organs, tissues, cell lines or cell clones and/or animals exposed to such materials in VA labs
Initially(within 30 days
of hire)
VA Bloodborne Pathogens,Basic Course
CITIhttp://www.citiprogram.org
All VA-Paid or WOC employees who work with nanotechnology in VA labs
Initially(within 30 days
of hire)
VA Understanding Nanotechnology and Its
Implications
CITIhttp://www.citiprogram.org
All VA-Paid and WOC employees who work in a VA lab. Initially(within 30 days
of hire)
Review and training on the Lab’s Chemical Hygiene Plan
Provided by theLab’s PI
All VA-Paid and WOC employees who work in a VA lab with liquid nitrogen present.
Initially(within 30 days
of hire)Liquid Nitrogen Training Provided by the
Lab’s PI
All VA-Paid and WOC employees who work in a VA lab and deal with radiation. Initially
(within 30 daysof hire)
Radiation Safety Training
Provided by theRadiation Safety Officer(Dr. S. Shukla, Ext. 6514,
[email protected]) *NOTE: VA labs = VA biological research laboratories that may include work with bio-hazardous materials, bloodborne pathogens, radiation,
chemicals, and other potentially hazardous materials**NOTE: Definition of “initially” = training must be taken within 30 days of the employee’s hire date.

GUIDELINES FOR SAFETY TRAINING - Continued
REQUIRED FOR FREQUENCY TRAINING TITLE METHOD
TRAINING REQUIRED ANNUALLYAll VA-Paid and WOC employees who are responsible for shipping (sending) bio-hazardous materials in VA labs
Every 2 Years(within 730 daysof last training
VA Biohazard Shipping Training
CITIhttp://www.citiprogram.org
All VA-Paid and WOC employees who work with human or non-human primate blood, body fluids, organs, tissues, cell lines or cell clones and/or animals exposed to such materials in VA labs
Annually(within 365 daysof last training
VA Bloodborne Pathogens, Basic Course
CITIhttp://www.citiprogram.org
All VA-Paid or WOC employees who work with nanotechnology in VA labs
Annually(within 365 daysof last training
VA Understanding Nanotechnology and Its
Implications
CITIhttp://www.citiprogram.org
All VA-Paid and WOC employees who work in a VA lab. Annually(within 365 daysof last training
Review and training on the Lab’s Chemical Hygiene Plan Provided by the Lab’s PI
All VA-Paid and WOC employees who work in a VA lab and deal with radiation. Annually
(within 365 daysof last training
Radiation Safety Training
Provided by theRadiation Safety Officer(Dr. S. Shukla, Ext. 6514,
REFERENCES: VHA Handbook 1200.06 VHA Handbook 1200.08 Title 29 CFR 1910.1030 CDC-NIH Biosafety in Microbiological and Biomedical Laboratories, 5 th Edition
NOTE: Training Certificates must be provided as proof of completing initial and annual training when protocols and Safety
Evaluations (initial, annual, 3-year ACORP and amendments) are submitted for SRS review.

BIOSAFETY QUIZ
Name: ___________________________
Date: ____________________________
NOTE: All new laboratory personnel (VA-Paid and WOCs) must take the Biosafety Quiz after reading the Laboratory Safety Manual and receiving required training from the laboratory Principal Investigator. PI should retain a copy of all tests.
1. Personal protective equipment (PPE) for each task is:A. Used at the discretion of the
employeeB. Designated by the supervisor and
specified by the exposure control plan (ECP) and / or by any site-specific standard operating procedures (SOPs)
C. Not necessary unless the task is labeled as “high risk”
D. Not required for students
2. Which of the following statements about Personal Protective Equipment (PPE) are correct?A. PPE must be worn and stored only
inside the laboratoryB. PPE must be chosen based upon
the work being completedC. Employees utilizing PPE must be
properly trainedD. All of the above
3. The main purpose of a laboratory coat is to:A. Keep your clothes from being ruinedB. Help assess the cleanliness of the
laboratoryC. Identify you as a trained professionalD. Keep contamination off your clothingE. Give you access to several pockets
at once
4. Laboratory coats must be taken home to be bleached and cleaned on a regular basisA. True B. False
5. It is okay to wear sandals in the lab as long as you also wear socksA. TrueB. False
6. Valid method(s) of compliance is / are:A. Eating, drinking, smoking or applying
cosmetics in the work areaB. Pipetting by mouthC. Washing hands before leaving the
work areaD. Wearing the appropriate personal
protective equipment (PPE)E. C and D above
7. An ideal container for biomedical waste would:A. Be hard-sidedB. Have a foot operated lidC. Be easily decontaminatedD. All of the above
8. The following material may be disposed of in the regular trash:A. Animal tissue, blood, dander or
droppings B. Human blood, tissue, or body fluidsC. Broken glass D. None of the above
9. How should biological materials that need to be transported from the lab to another location be handled?A. Wear a lab coat and transport
materials in your pocketB. Wear gloves and carry the material
in your handsC. Seal materials in a sturdy, leak-proof
secondary container
Research Services: Laboratory Safety Manual Page 7

D. Cells in cell culture flasks and /or dishes are fine for transport
10. You cannot use a gloved hand to open hallway doors and press elevator knobs.A. TrueB. False
11. Which type of disposable glove provides the greatest tear and puncture resistance?A. NitrileB. LatexC. Vinyl
12. If gloves are worn when handling viable, potentially infectious material, there should be no need for hand washing.A. TrueB. False
13. Alcohol-based hand sanitizers are just as effective as hand washing for removal of a broad-spectrum of infectious organisms.A. TrueB. False
14. If you notice that a sharps container is getting full, you should:A. Empty the sharps container into
biohazard bagB. Obtain a new one, close the lid on
the full one and arrange to have it safely transported for proper disposal
C. Empty the sharps container into a properly lined, leak proof, puncture proof container
D. Recap the needles and throw them in the regular trash
15. Remove the needle from the syringe before you put it in the sharps container. A. TrueB. False
16. Safe Sharps practices refers to:A. Plastic ware substituted for
glasswareB. Needle designs engineered to
minimize needle stick injuriesC. Discouraging the practice of
recapping needles D. All of the above
17. Which of the following materials require compliance with federal regulations for commercial carrier / air transport of dangerous goods:A. Dry iceB. Pathogenic culturesC. Chemical preservativesD. All of the above
18. Biohazard labels or stickers are required
on:A. Storage and transport
containers/equipment used for blood or OPIM
B. Biomedical waste containersC. Contaminated linen/laundry binsD. All of the above
19. A Biosafety Level 2 (BSL-2) lab works with agents that may be described as:A. Not associated with disease in
healthy adult humansB. Associated with human disease
which is rarely serious and for which preventive or therapeutic interventions are often available
C. Associated with serious or lethal human disease for which preventive or therapeutic interventions may not be available but are not readily transmissible to others (high individual risk but low community risk)
Research Services: Laboratory Safety Manual Page 8

20. You should alert your supervisor and reassess health risks involved with BSL-1 and BSL-2 material that you are working with when:A. You have a cold or the fluB. You are pregnantC. You have been diagnosed with or
suspect that you may have an immune disorder
D. All of the above
21. Site-specific standard operating procedures (SOPs) as well as an exposure control plan (ECP):A. Outline in detail all measures that
will be taken to eliminate or minimize employee exposure to hazards
B. Must be workplace-specificC. Must be readily accessible to
employeesD. All of the above
22. If an exposure incident occurs, the exposed employee should: A. Wash the exposed skin with soap
and water, flush other exposed areas with water, and inform their supervisor / administration
B. Seek medical treatment at the location identified in your exposure control plan
C. A or B, as appropriateD. Go on as if nothing happened
23. Which one of the following procedures could generate aerosols?A. Sonicating tissue culture cellsB. Intranasal / intratracheal inoculation
of animalsC. Vortexing / homogenizing solutionsD. All of the above
24. Which one of the following practices best prevents worker exposure to infectious aerosols?A. Balancing the safety cups prior to
placing them in the centrifugeB. Opening the centrifuge safety cups
only in the biological safety cabinetC. Using a splash shield to open
rubber-stoppered tubes D. Wearing a surgical mask while
performing work
25. Ethanol or isopropyl alcohol solutions are not a preferred disinfectant, because:A. They require a long contact time and
have a fast evaporation rateB. They do not have broad spectrum
disinfectant capabilityC. All of the above
26. Fabric chairs are allowed at lab benches and microscopes according to both the 5th edition (2009) of the CDC/NIH publication, “Biosafety in Microbiological and Biomedical Laboratories (BMBL) and the NIH Guidelines for Research Involving Recombinant DNA Molecules or Synthetic Nucleic Acid Molecules (March 2013). A. TrueB. False
27. NIH Guidelines for Research Involving Recombinant DNA Molecules or Synthetic Nucleic Acid Molecules (March 2013) consider which of the following when conducting a risk assessment:A. GeneB. VectorC. Intended / Unintended hostsD. Training / Safe practicesE. All of the above
Research Services: Laboratory Safety Manual Page 9

28. Biological Safety Cabinets used for infectious / potentially infectious material must be certified at least:A. DailyB. MonthlyC. YearlyD. Once
29. Which of the following protects both the user and the material that is being handled: A. Fume hoodB. Clean benchC. Biological Safety Cabinet (BSC)D. All of the above
30. In a Class II, Type A2 biological safety cabinet (typical unit found in most labs):A. Downward laminar flow splits 2-6
inches above work surface between front and rear grills
B. HEPA-filtered air from the cabinet is re-circulated in the unit and also exhausts to the room
C. It is safe to work with substantial amounts of chemicals and radiolabeled nucleotides
D. A and B only
31. Open flames are not allowed in a biological safety cabinet becauseA. They disrupt airflow patterns that
protect user and productB. They can damage HEPA filtersC. They pose a fire hazardD. All of the above
32. Acceptable alternatives to Bunsen burner use in the biological safety cabinet (BSC) include:A. Disposable loops, spreaders, or
glass beadsB. BacticineratorC. Wrist-operated Touch-O-Matic
burner
D. All of the above
33. It’s okay to store pipette tips and microcentrifuge tubes in the biological safety cabinet as long as they are pushed up against the back wall of the cabinet.A. TrueB. False
34. Which of the following practices should be utilized when working in a biological safety cabinet?A. Disinfect all surfaces of the BSC
before and after workB. Disinfect all items which go into and
come out of the BSCC. Allow the BSC to operate before
work begins and after work ceasesD. All of the above
35. If a spill should occur within a Biological Safety Cabinet (BSC), what steps would immediately be taken?A. Turn off the BSC, grab the biological
spill kit, and immediately wipe up the spill with a dry, absorbent towel
B. Turn off the BSC and pour a germicidal agent on the spill
C. Turn off the BSC, evacuate the laboratory, and notify company safety authorities
D. Leave the BSC on, grab the biological spill kit, add absorbent material and germicidal agent, wipe up the spill once contact time has permitted inactivation, and remove corrosive residue with 70% ethanol.
E. Leave the BSC on, grab the biological spill kit and wipe up the spill with a dry, absorbent towel
36. Disinfectants decontaminate soiled and clean surfaces equally well.A. TrueB. False
Research Services: Laboratory Safety Manual Page 10

37. Household bleach solutions used for surface disinfection should be prepared:A. Once a dayB. Once a weekC. Once a monthD. When the bottle is empty
38. In order to avoid wearing gloves outside the laboratory, you should:A. Not work with infectious agentsB. Use a disinfected, leak-proof
secondary container for transportC. Open doors for someone else who is
using gloves to transport your materials
D. Take gloves off and leave them on the bench so that you can put them back on when you get back
39. The vaccine that must be offered to personnel working with human blood cells is:A. hepatitis A virusB. hepatitis B virusC. tetanusD. malaria
40. Blood-borne pathogens may be transmitted with contact to:A. EyesB. Mucous membranesC. Broken skinD. All of the above
41. A surgical mask alone provides mucous membrane protectionA. TrueB. False
42. Surgical masks and N-95 respirators provide the same level of protection against aerosols.A. TrueB. False
43. The primary strategy for Hepatitis C prevention is:A. ImmunizationB. Universal precautionsC. Post exposure treatmentD. A and B only
44. Which of the following is true regarding Hepatitis B:A. The virus is only viable for a few
minutes once outside the bodyB. Three vaccinations are required for
protection, each given one week apart
C. Is only transmitted by a stick with a contaminated needle
D. Infections have dropped by about 95% since the introduction of the vaccine
45. Which of the following is true regarding the most common BBP diseases:A. Hepatitis B is more transmissible
than Hepatitis CB. HIV is more transmissible than
Hepatitis B
46. Which of the following is NOT a good control to use against infection/exposure to BBP diseases?A. Safety equipment (engineering
controls)B. Safe work practicesC. Personal protective equipmentD. Your immune system
Research Services: Laboratory Safety Manual Page 11

BIOSAFETY QUIZ – ANSWER KEY
1. B
2. D
3. D
4. B – A commercial laundry service is required. If contaminated or potentially contaminated with infectious materials, lab coats must be bleached / autoclaved before they leave the facility.
5. B – Foot cover must appropriately shield feet from exposure to percutaneous injury, corrosives, or biologicals
6. E
7. D
8. D
9. C
10.A
11.A
12.B – Always wash hands after removing gloves. Glove integrity may be unknowingly compromised.
13.B – Hand washing is superior, but sanitizers are allowable if a sink is not immediately available. Hands must still be washed as soon as possible.
14.B
15.B – Remember to minimize handling of sharps!
16.D
17.D
18.D
19.B
20.D
21.D
22.C
23.D
24.B (answers a and c will help prevent exposure, but b is the best answer)
25.C
26.B
27.E
28.C
29.C
30.D
31.D
32.D
33.B – blocking the rear plenum (grates) will disrupt the airflow and could compromise containment / protection
34.D
35.D
36.B
37.A
38.B
39.B
40.D
41.B – A surgical mask protects the user’s mouth from splashes, but eyes have mucous membranes, too!
42.B – N95 respirators offer superior protection. However, they are tight-fitting (have two straps and seal to the face) and require fit testing for effectiveness assurance.
43.B
44.D
45.A
46.D
Research Services: Laboratory Safety Manual Page 12

SECTION II. SAFETY PROCEDURES
PERSONAL SAFETY AND HEALTH PRACTICES
Prior to working with human pathogens see the Research Infection Control Plan (in this Section) and consult an Employee Health Physician to identify any medical issues that may place you at higher risk for infection.
A. All personnel must be familiar with symptoms of disease or illness associated with materials they handle. Personnel must know what constitutes a potential exposure or release. Such incidents are to be reported to the PI or Lab Supervisor immediately (who may then report particulars to medical care providers, as appropriate, and complete appropriate VA report forms).
B. Know ahead of time the location and operation of emergency equipment, such as the eyewash and safety showers, first aid kit, chemical and biological spill kits, emergency numbers, fire extinguishers, and emergency exits.
C. Mouth pipetting under any circumstance is forbidden.
D. FOOD and DRINK are strictly forbidden in the laboratories.E. Application of cosmetics, unprofessional conduct (i.e., nail clipping, etc.) use of
tobacco products and gum chewing are not permitted in the laboratory.
F. Contact lenses must not be worn in the laboratory. If they must be worn, eye protection, such as tight fitting goggles, must be worn.
G. Wear ANSI approved protective goggles when performing any activity with a splash hazard (e.g., working with corrosive chemicals, retrieving vials from liquid nitrogen, breaking up pieces of dry ice, etc.)
H. Should eyes become contaminated, wash extensively (15 minutes) at the eye wash station. Eye-wash stations are located at each sink in each lab. All eye injuries should be evaluated by a physician. Report the incident to your supervisor immediately and report to Employee Health Office F110-1.
I. All injuries (i.e., needle sticks, cuts, abrasions, etc.) and accidents or work-related illnesses are to be reported to your supervisor immediately and if necessary, report to Employee Health Office F110-1. In case of accidents, the immediate supervisor or PI must take the employee to the Employee Health Office. The Employee Health Nurse will initiate and accident report (in ASISTS), and both the employee and supervisor are required to go online and complete their part of the report.
J. Wash hands after removing gloves and before leaving the laboratory.
K. Personal Protective Equipment (PPE), including lab coats that are worn in the laboratory, may not be worn elsewhere in the hospital especially the cafeteria and may not be taken home to wash.
Research Services: Laboratory Safety Manual Page 13

L. Each lab must have appropriate gloves for removing hot items from the autoclave and cold items from freezers or liquid nitrogen containers and for handling strong acids, bases, solvents or dry ice.
M. OPEN-TOED SHOES/SANDALS ARE PROHIBITED in the laboratory and in the VMU.
N. When handling items from ultra-low freezers or from liquid nitrogen, personnel must use cryogenic gloves, face shields, protective clothing and impervious foot wear.
O. Gloves are not to be worn outside the laboratory areas. Opening cabinet doors or exit doors with gloves on is prohibited.
P. Potentially infectious material must be transported in a leak-proof, decontaminated secondary container. A transportation cart should be used to transport biohazard containers. Carrying biohazard containers by hand is strongly discouraged. If you are transporting outside of the laboratory you should not wear gloves. Only if necessary/essential for the protection of personnel transporting infectious materials, one hand may be gloved, but the other hand must not be gloved. Opening doors or operating elevators, etc. must be carried out using the hand without the glove.
Q. For your personal safety and the safety of others, dried, cracked, and broken skin on hands MUST be covered with gloves at all times.
R. Wash all potentially contaminated body areas as well as arms, face, and hands. Locate nearest shower or drench hose and use if necessary.
S. Fire regulations do not permit storage of any materials within 18” from the ceiling.T. All containers (i.e., bottles, tubes, flasks, etc.) in labs must be clearly labeled as to
content. If abbreviations are used to label any items, a list of abbreviations used and the respective full names must be posted in a convenient place that is visible to all personnel.
U. All compressed gas tanks must be properly secured at all times.V. At the end of each day, clean up and disinfect the entire work area to ensure good
housekeeping and proper storage of all laboratory items used. Bench covers must be changed daily, if used, and may not be taped to the bench top in any area of the laboratory.
W. If you hear the fire alarm bells, check to see if the fire is in your area. If not in your area, be alert for further information. DO NOT USE THE ELEVATORS.
X. I f you discover a fire in your lab/area, remember RACE:1. Rescue all persons from the immediate area of the fire.2. Activate the Alarm via manual pull stations which are located at all stairwells or
call 6333 and give specific information about the fire. Notify the staff in the immediate area of the fire to leave the lab area.
3. Confine the fire by closing all doors in the immediate area.4. Evacuate/Extinguish the fire if it is small and you feel comfortable doing so.
Y. In an emergency situation: Notify other lab personnel in case they do not hear the alarm announcement and leave the area.
Research Services: Laboratory Safety Manual Page 14
BLOODBOURNE PATHOGENS
A. All personnel must undergo annual bloodborne pathogen training.B. All personnel must follow universal precautions while handling biohazard material
including blood or body fluids.C. All personnel must avoid direct contact with all visible blood, body fluids, mucus
membranes and non-intact skin.D. All personnel must wear gloves, gowns and masks necessary to avoid blood/body
fluid contacts.E. Must wear gloves for all invasive procedures, and while working with specimens.F. Must wear gloves, gowns, and goggles when splash of body fluids or infectious
material is likely.G. Protect yourself at all times; do not assume that any blood or body fluids are safe.
Wash hands after the procedure.H. Must properly dispose the biohazard specimens or waste in biohazard-marked bags
which are available from Environmental Management Service.I. Do not use red biohazard-marked bags for disposal of non-biohazardous waste.
Research Services: Laboratory Safety Manual Page 15

USE AND HANDLING OF INFECTIOUS/POTENTIALLY INFECTIOUS MATERIALS
A. When using a Biological Safety Cabinet (BSC) work at least 6” back inside the front intake so you do not disrupt the “air curtain.” Do not cover the back plenum of the BSC with equipment or other materials as it disrupts the air flow.
B. Avoid the use of needles whenever possible. Substitute plastic for glassware whenever possible.
C. All human specimens are considered to be potentially infected with hazardous agents. Direct handling of these substances is to be avoided. Gloves, forceps, or other protective equipment must be used as appropriate.
D. Spilled material must be contained with paper toweling and immediately covered with a solution of freshly prepared (within 24 hours) 10% bleach in water for 30 minutes. Discard paper towels in a biohazard waste bag. The area must then be thoroughly cleaned with 70% ethanol in water. Report the spill to your supervisor.
E. Minimize puncture of biomedical waste containers by placing plastic pipettes or other items that have been contaminated with microorganisms in a rigid, leak-proof container (properly labeled with a biohazard symbol) prior to disposal.
F. UV light may only be activated when there is proper shielding and when there is no danger of excessive exposure to laboratory personnel. Wear protective eye wear when using UV light. Protect skin from exposure by wearing gloves. Do NOT rely on the UV source in the BSC to decontaminate surfaces.
G. Clean the BSC at the end of each procedure and do not use it for storage. Use a solution of freshly-prepared (within 24 hours) 10% bleach, Amphyl or Wescodyne followed by 70% ethanol in water to remove corrosive residue. The VMU uses MB-10 and is stable for seven days.
H. BSCs (Type II) must be NSF/ANSI Standard 49 certified by qualified engineers or contractors at least annually. Chemical fume hoods must have the ventilation checked by qualified engineers or contractors annually.
Research Services: Laboratory Safety Manual Page 16

INFECTION CONTROL
Principal Investigators are responsible for establishing procedures for handling and disposing of specific biohazards used in their laboratories that are not covered by the hospital memoranda. The investigators must receive approval from University of Florida EH&S (Division of Environmental Health and Safety) Biosafety Office, and obtain approval from VA SRS prior to starting work with recombinant DNA or infectious pathogens in the laboratories at the NF/SGVHS, Gainesville, FL.
A. General Instructions1. Autoclave all items containing infectious/potential infectious materials or
recombinant DNA prior to disposal.2. Follow approved biohazard statement (rDNA/pathogen registration from
University of Florida).3. If using animals, consult the IACUC-approved ACORP.
B. Additional Information1. Route of Infection
Infections may be spread by several routes. The actual occurrence of an infection is dependent on both the virulence of the infecting agent and the susceptibility of the host.a. Air borne: Droplets and aerosols may be formed by simply removing caps or
cotton plugs or swabs from tubes. Ejecting liquids for needles too rapidly may also create an aerosol. Breakages in centrifuges are serious accidents.
b. Ingestion: May occur through mouth pipetting, failure to wash hands after handling specimens or cultures, and by handling of cigarettes.
c. Direct Inoculation: Scratches, needles, broken glass or animal bites may permit direct inoculation.
d. Skin Contact: Some very virulent organisms and others not so virulent can enter through small cuts or scratches, or through conjunctiva of the eye.
e. Vectors: Mosquitoes, ticks, fleas, and other ectoparasites may be potential sources of infection in the laboratory; especially if animal work is performed (all windows must be closed in the laboratory).
2. Handling Specimensa. Wash hands frequently even when using gloves (but remove gloves to
wash hands).b. Centrifuge: If specimens must be centrifuged, they must be covered by a
sealed cap to prevent aerosol formation.c. Bio-safety cabinet: Specimens classified as BSL-2 must be handled in a
biosafety cabinet. Do not obstruct the air-flow and handle samples at least 6
Research Services: Laboratory Safety Manual Page 17

inches inside from the front intake. Specimens for fungus cultures must be handled in the biosafety cabinet.
3. Processing Specimensa. All blood specimens are considered as biohazardous material and must be
handled as potential biohazard materialb. All specimens are potentially contaminated therefore investigators must use
careful techniques at all times.c. All cultures are potential pathogens therefore investigators must use careful
techniques at all times.d. Large numbers of plates must be handled in baskets. Test tube racks or
trays are required for tubed cultures (DO NOT place tubes in glasses or paper cups).
e. Tuberculosis and fungus specimens and cultures will be handled and processed in the biological safety cabinets.
f. Needles and loops must be sterilized so as not to cause spattering of material on heating.
g. Work benches must be disinfected with freshly prepared 10% chlorine bleach followed by 70% ethanol after completion of every procedure.
4. Disposal of Biohazardous Materiala. Waste from microbiological specimens (e.g., culture plates, flasks, etc.) must
be placed into plastic autoclavable bags. Autoclave at least 60-90 minutes, at 121C/250F, 15PSI, prior to discarding in biohazard (red) bags for disposal by Environmental Management Service (EMS)..
b. Liquid waste must be decontaminated with appropriate disinfectant. Recommended method is to use a final concentration of 1:10 bleach, allow a minimum of 30 minutes contact time, and pour it down the sink. Autoclave the disposal containers (as described above) before discarding in red biohazard bags.
c. Contaminated reusable containers (e.g., glass test tubes, conical flasks, beakers, etc.) must be autoclaved as described in a. above prior to cleaning. Place them in a sealed and clearly labeled container to minimize any hazard to others prior to sterilization.
d. Any breakage of bags or leakage of contaminated material must be reported to the supervisors for instructions on procedures for safe clean up.
e. All blood specimens/other human body fluids are considered biohazardous material. Inactivate the blood (as described above for liquid waste). Empty glass tubes can be placed inside a sharps container, in a sturdy cardboard box, autoclaved (as described above), and placed inside the red biohazard bags for final disposal by the EMS. Needles, scalpel blades, lancets, etc., should be discarded in a sharps contained. Sharps containers can also be used to discard ‘non-sharps’ objects, such as used pipette tips, glass Pasteur pipettes, razor blades, slides, and cover slips. If the discards contents are
Research Services: Laboratory Safety Manual Page 18
infectious/potentially infectious Autoclave the sharps container (as described above). Sharps containers must be replaced when they are ¾ full.
5. Needle and Syringe Handling Proceduresa. DO NOT destroy, bend, or clip the used needles. The preferred practice is to
NOT replace the needle cap on a used needle (many needle sticks are caused in this manner).
b. Used needles must be placed in red plastic containers (Biohazard sharps disposal box) available from Building Management Services.
c. Never leave needles lying on the work bench.d. If injured, report immediately to employee health or the emergency room and
then notify the research office (ext. 6069).
SAFETY POLICY FOR WORKING WITH NANOMATERIALS
A. ObjectiveThis policy is intended to provide guidelines for individuals working at the NF/SG VHS who may use, handle or be exposed to nano-sized materials during the course of their employment.
B. AuthorityGuidelines set forth by the National Institute for Occupational Safety and Health (NIOSH) 29 CFR 1910.1200 Hazard communication and NIOSH publication “Approaches to Safe Nanotechnology” 2009
C. PolicyThis policy applies to all employees engaged in any activity at the NF/SG VHS Research Service wherein they may become exposed to nano-sized particles of any material during the performance of their duties as employees of NF/SG VHS Research Service.
D. DefinitionNanoparticles (NPs) are engineered materials or other particles being studied in research projects that have at least one dimension between 1-100 nanometers. Nanoparticles can be spheres, rods, tubes, flakes and other geometric shapes. The small particles may be bound to surfaces or substrates, put into solution or suspension, attached to a polymer or handled as a dry powder.
E. BackgroundNanoparticles have always been present in our natural environment. They may be naturally occurring such as in volcanic ash or from forest fires. They may be unintentional byproducts of our society such as in auto and factory emissions. Over the past several years they have been intentionally created or engineered to be used in therapeutics. These very small particles often exhibit properties different from
Research Services: Laboratory Safety Manual Page 19

larger particles of the same composition, making them of interest to researchers and of potential benefit to society. Only limited information is currently available on the toxicity of a few types of nanoparticles. It is believed that some engineered nanoparticles may present harmful health effects following exposure. This policy focuses on practices employees should follow to protect themselves from the potential hazards of engineered nanoparticles.
Laboratory research most commonly involves handling nanoparticles in liquid solutions or other forms that do not become easily airborne. Even free formed nanoparticles tend to agglomerate to a larger size. Recent research of nanoparticles handling in fume hoods have shown that it is safer to use as small a quantity as possible when handling dry powder forms of the materials. Larger quantities, more than 15 grams, resulted in some airborne material detected in the breathing space of the technicians, (Tsai et. al., J. Nanopart Res (2009) 11:147-161).
When research involves work with engineered nanoparticles for which no toxicity data is yet available, it is prudent to assume the nanoparticles may be toxic, and to handle them with caution using the laboratory safety techniques outlined below in the guidelines for handling nanoparticles. Also, spills of nanoparticles should be quickly and properly cleaned up, as detailed below.
Nanoparticles are classified based on their morphology and the main categories to date include the following (Aitken, 2004):
1. Fullerenes. Discovered in the 1980s, these are comprised entirely of carbon and take the form of hollow spheres or tubes. These are similar in structure to graphite, forming a sheet of hexagonal carbon rings, but also contain pentagonal and heptagonal rings that allow the formation of three-dimensional structures. The smallest fullerene, a 60 carbon molecule termed buckminsterfullerene (familiarly referred to as “buckyballs”), is the most familiar and recognizable from of NP addressed in common and scientific literature. Fullerenes are produced naturally in small amounts through burning of carbon-containing fuels and can be manufactured in commercial quantities through arching and combustion of graphite, coal, and various other hydrocarbons.
2. Nanotubes. This class of NP is actually comprised of fullerene-like (carbon) particles that are elongated to form tubular structures having a diameter of 1 to 2 nanometers. Carbon nanotubes have significant tensile strength, strength equaling or exceeding 100 times that of steel have been reported. In addition to great tensile strength, nanotubes also have the advantage of much lower weight in comparison to steel and most other commonly used structural materials: Other highly useful properties exhibited by nanotubes includes capacity for high conductivity, high molecular absorption, and other unique electrical properties.
3. Nanowires. These are essentially tiny interconnecting wires of a single crystalline structure that are constructed using approaches similar to semiconductor fabrication – template disposition.
Research Services: Laboratory Safety Manual Page 20

4. Quantum Dots. Sometimes referred to as artificial atoms, quantum dots are assemblies of materials between two to ten nanometers. They can be composed of metals, metal oxides, or semiconductor materials and typically exhibit unconventional electronic, magnetic, optical, or catalytic properties. These are constructed through chemical-colloidal disposition: a growth process that can be tuned to alter the structure’s final characteristics. These particles are termed “quantum dots” because their final size (alone) can control their physical properties; irradiated fluorescent quantum dots for example, will emit different wavelengths of light depending on particle size.
F. Occupational Exposure HazardsPrimary routes of occupational exposure to nanoparticles include: inhalation, trans-dermal absorption, and ingestion (Borm et al., 2006). Epidemiological data is limited for occupational exposure to nanoparticles. The available data suggests humans and laboratory animals exposed to nanoparticles may experience adverse health effects associated with chronic exposure. The observed effects are dependent on the route of exposure and the particular nanoparticle to which the individual has been exposed. The following observations have been recorded following chronic exposure to nanoparticles.
1. Carcinogenicity. Carcinogenicity data on nanoparticles is limited. Studies have shown that certain nanoparticles cause lung tumor development in experimental animals following a lung particle overload (Lee et al., 1985; Heinrich et al., 1995). In particular, carbon nanotubes (CNTs) exhibit a direct relationship between length and particle deposition and their effects on lung irritation, chronic lung inflammations, exacerbation of asthma, and the formation of granulomas consisting of macrophage-like multinucleated cells (Borm et al., 2006; Rehn et al., 2003).
2. Genotoxicity. Radicals may form on the surface of some nanoparticles that may have toxicological consequences resulting in the formation of reactive oxygen species (Albrecht et al., 2006). Reactive oxygen species have been shown to interact with DNA (Dung et al., 2006) resulting in DNA damage that causes fibrosis and lung cancer (Albrecht et al., 2006). In addition, molecular components of the nanoparticles are likely to have aromatic ring systems which have the size and shape to interact with DNA, and thus have potential to promote DNA damage or cancer (Freites, 2003). Many of the genotoxic effects associated with nanoparticles may be directly related to the characteristics of the nanoparticle surface: functionality, charge, and induced charge (Oberdöster et al., 2005). These characteristics create unique properties that may result in genotoxic interactions.
3. Cytotoxicity. Cytotoxicity depends upon the geometric shapes of the carbon nanomaterial (Jia et al., 2005). Carbon nanotubes (CNTs) have been studied for their cytotoxic properties and have been shown to cause a time- and dose-dependent relationship resulting in apoptosis of various human cell lines (Massimo et al., 2005; Cui et al., 2005; Monerio-Riviere et al., 2005). The CNTs are thought to cause cellular toxicity by a non-specific association with hydrophobic regions of the cell surface and internalization by endocytosis, and
Research Services: Laboratory Safety Manual Page 21

accumulation in the cytoplasm of the cell. DNA then wraps around the CNTs resulting in cell death (Hoet et al., 2004).
4. Toxicity. There is limited toxicological data in relation to nanoparticles. Most of the experimental work has involved a limited set of more common NPs, such as carbon black, titanium dioxide, iron oxide, and amorphous silica. Inhaled nanoparticles have the potential to aggravate existing respiratory condition, such as asthma or bronchitis (Oberdöster, 2001), and cause lung inflammation or tumors (Borm et al., 2006). Inhaled nanoparticles have been show to translocate from the lungs toward other organs within 24 hours after exposure (Hoet et al., 2004). Specific consequences of the translocation are largely unknown. However, preliminary results indicated that affected organ systems may show inflammation, altered heart rate and functions, and oxidative stress (Brown et al., 2004; Stone et al., 1994; Campen et al., 2003; Campbell et al., 2005). Ingested nanoparticles may be absorbed through the intestinal lining and translocate into the blood stream where they undergo first pass metabolism in the liver (Jani et al., 1994; Bockmann et al., 2000). Again, the effects of this translocation are largely unknown. Dermal uptake is limited and does not appear to produce systemic effects (Borm et al., 2006).
G. Potential Routes of Exposure for Research PersonnelThere are four possible routes of workplace exposure to nanoparticles: inhalation, ingestion, injection, and skin absorption.
1. Inhalation. Respiratory absorption of airborne nanoparticles may occur through the mucosal lining of the trachea or bronchioles or the alveoli of the lungs. Because of their tiny size, certain nanoparticles appear to penetrate deep into the lungs and may translocate to other organs following pathways not demonstrated in studies with larger particles. Thus, whenever possible, nanoparticles are to be handled in a form that is not easily made airborne, such as in solution or on a substrate.
2. Ingestion. As with any contaminant, ingestion can occur if good hygiene practices are not followed. Once ingested, some types of nanoparticles might be absorbed and transported within the body by the circulatory system. To prevent ingestion, eating and drinking are not allowed in laboratories outside of clearly designated areas.
3. Injection. Exposure by accidental injection (skin puncture) is also a potential route of exposure, especially when working with animals or needles. To prevent this, wear double gloves and lab coats, and apply the standard practices for working with sharps.
4. Skin Absorption. Is the most controversial route of exposure to nanoparticles. In some studies nanoparticles have been shown to migrate through intact skin and be circulated in the body. Skin contact can occur during the handling of liquid suspensions of nanoparticles or dry powders. Skin absorption is much less likely for solid bound or matrixed nanomaterials. Researchers should double glove to
Research Services: Laboratory Safety Manual Page 22

protect themselves from skin absorption and to protect their research materials from being contaminated. Outer gloves should be removed inside a fume hood or vented HEPA filtered biosafety cabinet and placed into a sealed bag. This will prevent the particles from becoming airborne in the lab.
H. Responsibilities
1. Subcommittee on Research Safety (SRS)SRS is responsible for the development and periodic review and updating of this policy. SRS will remain current with the literature that addresses environmental health and safety issues for research laboratories and regulatory agency requirements for research with nanoparticles including experiments involving animals. SRS will assure the latest safety information is incorporated into this policy as it becomes available. SRS will ensure that controls for nanotechnology research are based upon the most recent regulations, directives, guidance, and/or other applicable information.
2. Principal Investigators/SupervisorsPrincipal investigators and or supervisors are responsible for writing specific safety protocols, SOPs to be followed by all employees in their laboratories and the VMU personnel while working with nanoparticles or nanoparticles exposed animals. They will provide safety training to their employees who may be exposed to nanoparticles as a part of their employment. The principal investigator will also provide the required personal protective equipment and necessary training to use to employees and see to it that it is used properly.
3. EmployeesEmployees are responsible for complying with the safety procedures outlined in the working with nanoparticles policy as well as with written safety procedures specific to the task they perform in the course of their work with nanoparticles. Employees must maintain an awareness of nanoparticle safety issues pertaining to the materials they work with and report safety concerns immediately. Employees are responsible for attending appropriate safety training and for wearing the appropriate personal protective equipment (PPE) when working with nanoparticles.
I. SAFE WORK METHODSThe list of potential nanoparticle-related health hazards identified above necessitates the need for principal investigators to conduct thorough risk assessments individually for all nanoparticles and processes involved, and to prepare protocols which include measures for minimizing staff exposure potential. No governmental regulations currently exist regarding nanotechnology use. In lieu of available regulatory guidance, VCU and OEHS recommend that the course for principal investigators to follow is to either eliminate or reduce exposure potential as much as feasible through implementation of the safe work methods listed below.
1. Administrative Controlsa. Management considerations for nanoparticles and other potentially hazardous
chemicals must be included in the laboratory Chemical Hygiene Plan.
Research Services: Laboratory Safety Manual Page 23

b. Protocols involving the in vivo use of nanoparticles must include completion of ACORP Test substances page under Appendix-3 and approval through the Institutional Animal Care and Use Committee and the SRS.
c. Principal investigators will develop and implement standard operating procedures (SOPs) by which laboratory staff will prepare/administer nanoparticles with minimal exposure.
d. All tasks having potential for occupational exposure to nanoparticles will only be conducted by competent staff who have received appropriate training (OSHA: “Worker Right to Know”) regarding the specific nanoparticle-related health and safety risks, SOPs, and procedures to be followed in event of an exposure incident.
e. Laboratory personnel using nanoparticles in any procedure are required to complete applicable training on Nanoparticles modules under Biosafety Course on Collaborative Institutional Training Initiative (CITI) website.
f. Laboratory personnel must be instructed to use extreme caution when performing injections involving nanoparticles since accidental needle stick presents an exposure threat.
g. Exposures involving nanoparticles or any other acutely hazardous material should be reported to Employee Health as soon as possible.
2. Personal Protective Equipment Nanoparticle exposure may often be attributable to the wearing of inadequate PPE. Staff involved in any tasks where potential exposure to nanoparticles exposure exists must don the following PPE:a. Examination gloves: One particular type of glove will not always provide
adequate protection and glove selections is best determined by the risk assessment and the chemicals used for the procedure. Nitrile or rubber examination gloves which cover hands and wrists completely through overlapping sleeve of lab coat when working with nanoparticles may provide adequate protection. Wearing of two sets of gloves (“double gloving”) is advised whenever performing tasks involving nanoparticles and other hazardous substances. Laboratory personnel should thoroughly wash hands with soap and water before and immediately upon removal of examination gloves.
b. Safety glasses or safety goggles (ANSI Z-87 approved) are considered the minimum appropriate level of eye protection. SRS recommends donning of full-face shield when conducting tasks posing potential for any generation of aerosol or droplets.
c. Lab coats or disposable coveralls that provide complete coverage of skin not otherwise protected by PPE and/or attire. Laboratory personnel whose clothing has been contaminated by nanoparticles should change into clean clothing promptly. Do not take contaminated work clothes home – contaminated clothing should be disposed of as hazardous waste consulting Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
d. Appropriate laboratory attire: laboratory personnel handling nanoparticles should don attire which when worn in combination with lab coat and other PPE provides entire coverage of the body. Short pants/dresses and open-toed shoes are not appropriate laboratory attire.
Research Services: Laboratory Safety Manual Page 24

e. If an aerosol exposure threat exists, all procedures should be conducted in an approved chemical fume hood whenever possible (see Engineering Controls below). If an approved chemical fume hood cannot be utilized, an appropriate air-purifying respirator must be utilized for all procedures where exposure potential is present. A respiratory protection program that meets OSHA's 29 CFR 1910.134 and ANSI Z88.2 requirements must be followed whenever workplace conditions warrant a respirator's use. Prior to instituting respiratory protection to personnel, the laboratory personnel must participate in the University Respiratory Protection Program. The VA investigators must register with Employee Health (Gale Hockman at Ext. 7359).
3. Work Practicesa. Procedures with the potential for producing nanoparticle aerosols should be
conducted within an approved chemical fume hood whenever possible.b. Needles used for nanoparticle injection will be disposed of in approved sharps
containers immediately following use.c. Needles used for nanoparticle injection should never be bent, sheared, or
recapped. d. Bench paper utilized during preparation of nanoparticle stock should be lined
with an impervious backing to limit potential for contamination of work surfaces in the event of a minor spills.
e. Areas where nanoparticles are prepared and/or administered should be cleaned and decontaminated immediately following each task. Bench tops, BSC interiors, equipment, and laboratory surfaces with potential for nanoparticles contamination should be routinely cleaned.
f. Do not eat, smoke, or drink where nanoparticles are handled, processed, or stored, since exposure may occur via ingestion. Wash hands carefully before eating, drinking, applying cosmetics, smoking, or using the restroom.
4. Engineering Controlsa. To minimize airborne release of engineered nanoparticles to the environment
nanoscale materials should be handled with engineering controls such as a HEPA-filtered local capture hood, bio-safety cabinet. If none of these are available, work should be performed inside a laboratory fume hood. Use of a chemical fume hood is recommended for potential of aerosolizing nanoparticles. In all cases where engineering controls alone do not sufficiently reduce exposure potential, provision of appropriate PPE for suitably minimizing hazard will be required.
b. Syringes used for nanoparticles injection must be safety engineered (self-sheathing syringes, luer-lock syringes, etc.). Exceptions will be considered by the IBC on a case-by-case basis.
c. Animals should be appropriately restrained and/or sedated prior to administering injections and other dosing methods.
d. Laboratories and other spaces where handling of nanoparticles occurs must be equipped with an eyewash station that meets American National Standards Institute (ANSI) and OSHA requirements.
5. Waste Disposal
Research Services: Laboratory Safety Manual Page 25
a. Nanoparticles are potentially hazardous materials, surplus stocks and other waste materials containing greater than trace contamination must be disposed of through the VA hazardous waste disposal program.
b. Metabolism and excretion of nanoparticles are dependent upon the route of absorption and the particle surface properties. Inorganic nanoparticles, such as titanium dioxide, are unlikely to be altered. However any chemical group added to the inorganic particle’s surface could be modified enzymatically or non-enzymatically within the body (Borm et al., 2006). Polymers of nanoparticles will most likely undergo enzymatic alteration but will be based on the chemical composition and specific properties of the polymer. Some carbonaceous nanoparticles have been metabolized in aquatic systems and it is therefore assumed that those with branched side chains or hydrophilic groups are targets for normal human metabolic machinery which is driven by oxidative enzymes (Sayers et al., 2004). It has been shown in animal models that certain polymer based nanoparticles are excreted via urine (Nigavkar et al., 2004). Radiolabeled nanoparticles administered to laboratory animals were found to be secreted in bile. Therefore it can be implied, depending upon the properties of the nanoparticle, that the feces of contaminated individuals will contain nanoparticles or nanoparticle metabolites (Nefzger et al., 1984). The metabolism and potential risks associated with nanoparticle use requires that all potential contaminated carcasses, bedding, and other materials be disposed of through incineration.
c. All contaminated sharps waste materials must be placed in proper sharps container and disposed of as regulated medical waste (RMW).
6. Spills Laboratory personnel must use appropriate PPE prior to attempting to manage any spill involving NPs agents. NF/SG VHS SRS policy for addressing spills involving nanoparticles is provided below:a. Small spills (typically involving less than 5 mg of material) of nanoparticle-
containing powder should be wet-wiped with cloth/gauze that is dampened with soapy water. Affected surfaces should be thoroughly wet-wiped three times over with appropriate cleaning agent determined by the laboratory risk assessment – with clean damp cloth used for each wipe down. Following completion all cloth and other materials utilized during spill clean-up with potential for nanoparticles contamination must be disposed of as hazardous waste.
b. Small spills (typically involving less 5 ml of material) of nanoparticle-containing solutions should be covered/absorbed with absorbent material. Areas affected by liquid spills should be triple cleaned with soap and water following removal of absorbent paper.
c. For larger spills of nanoparticles, contact Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
J. Safety Guidelines for Handling NanoparticlesThe practices for safely working with nanoparticles are essentially the same as one would use when working with any chemical of unknown toxicity.
Research Services: Laboratory Safety Manual Page 26
1. Write a Safety Operating Procedure (SOP) to outline the safety procedures to be followed in the handling of nanoparticles in your lab protocols. Use good general laboratory safety practices as stated in your Chemical Hygiene Plan (CHP). For example; wear double gloves that are specific for the chemical or material, safety glasses or goggles, and appropriate protective clothing.
2. All personnel participating in research involving nanoscale materials need to be trained concerning the potential hazards, as well as on proper techniques for handling nanoparticles. As with all safety training, documentation in the CHP needs to be maintained to indicate who has been trained in the safe use of the nanoscale material.
3. No eating and drinking are allowed in labs areas where chemicals or nanoparticles are used.
4. When purchasing commercially available nanoscale materials, be sure to obtain the Material Safety Data Sheet (MSDS) and to review the information in the MSDS with all persons who will be working with the material. (Note that given the lack of toxicological data on the effects of nanoparticles, the information on an MSDS may be more applicable to the properties of the bulk material.)
5. In some cases, the making of nanoparticles involves the use of chemicals that are known to be hazardous or toxic. Be sure to consider the hazards of the pre-cursor materials when evaluating the process hazard or final product. Users of any chemicals should make themselves familiar with the known chemical hazards by reading the MSDS or other hazard literature.
6. To minimize airborne release of engineered nanoparticles to the environment, nanoparticles are to be handled in solutions, or attached to substrates so that dry material is not released. Where this is not possible, nanoscale materials should be handled with engineering controls such as a HEPA-filtered local capture hood, bio-safety cabinet. If none of these are available, work should be performed inside a laboratory fume hood. HEPA-filtered local capture systems should be located as close to the source of nanoparticles as possible, and the installation must be properly engineered to maintain adequate capture ventilation. Contact physical plant division for guidance, and UF EH&S for any required permits and Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025..
7. Use fume hoods to expel any nanoparticles from tube furnaces or chemical reaction vessels. Do not exhaust aerosols containing engineered nanoparticles inside buildings.
8. Never work outside of a ventilated area with nanomaterials that could become airborne. If a research protocol requires work to be done outside of a ventilated area, contact the EH&S Laboratory Safety Program at 392-1591 and Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025 prior to proceeding; a respirator may be required.
Research Services: Laboratory Safety Manual Page 27

9. Lab equipment and exhaust systems used with nanoscale materials should be wet wiped (10% bleach in water) and HEPA vacuumed prior to repair, disposal or reuse. Construction/maintenance crews should contact Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025 for assistance.
10. Spills of engineered nanoparticles are to be cleaned up right away. The person or persons cleaning up should wear appropriate PPE, including double gloves to prevent contamination with the spilled material. Depending on the size of the spill and the material involved the spill area can be either vacuumed with a HEPA filtered vacuum and/or wet wipe the area with towels, or a combination of the two. For spills that might result in airborne nanoparticles, proper respiratory protection should be worn (see item 8 above). Do not brush or sweep spilled/dried nanoparticles. Place a Tacky-Mat at the exit to reduce the likelihood of spreading nanoparticles on footwear. For assistance with clean up of large chemical spills or those of toxic or unknown content contact Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
11. Many engineered nanoparticles are not visible to the naked eye and surface contamination may not be obvious. Work surfaces should be wet-wiped regularly – daily is recommended. Alternatively, disposable bench paper can be used. Wet wipes or bench paper must be placed in a plastic bag and secured before removal from the work area. It will then need to be placed into a second bag for disposal as hazardous waste.
12. All waste engineered nanoparticles should be treated as hazardous materials unless they are specifically known to be non-hazardous. Dispose of and transport waste nanoparticles in solution according to hazardous waste procedures for the solvent. Information on how to dispose of a specific nanoparticle waste, can obtained by contacting Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
K. Animal StudiesIt is currently unknown how animals dosed with nanoparticles will excrete them. Metabolism and excretion of nanoparticles are dependent upon the route of absorption and the particle surface properties. Inorganic nanoparticles, such as titanium dioxide, are unlikely to be altered. However any chemical group added to the inorganic particle’s surface could be modified enzymatically or non-enzymatically within the body (Borm et al., 2006). Polymers of nanoparticles will most likely undergo enzymatic alteration but will be based on the chemical composition and specific properties of the polymer. Some carbonaceous nanoparticles have been metabolized in aquatic systems and it is therefore assumed that those with branched side chains or hydrophilic groups are targets for normal metabolic processes driven by oxidative enzymes (Sayers et al., 2004). It has been shown in animal models that certain polymer based nanoparticles are excreted via urine (Nigavkar et al., 2004). Radiolabeled nanoparticles administered to laboratory animals were found to be secreted in bile. Therefore it can be implied, depending upon the properties of the nanoparticle, that the feces of contaminated animals will contain nanoparticles or nanoparticle metabolites (Nefzger et al., 1984). The metabolism and potential risks
Research Services: Laboratory Safety Manual Page 28

associated with nanoparticle use requires that all potential contaminated carcasses, bedding, and other materials be disposed of in accordance with current regulations.
Dosing and necropsies shall be conducted within an exhausted hood, preferably one with HEPA filtration if available. Additionally, the composition of the nanoparticles will vary amongst animal study ACORP protocols, e.g. chemical composition, radiolabelled nanoparticles, nanoparticle structure, etc., so potential toxicity and safety control measures may also vary with each IACUC proposal. When ACORP reviewers have specific concerns about IACUC proposal’s involving nanoparticles in animals, SRS will address those concerns to make sure safety controls are included based on the Research Service Chemical Hygiene Plan (CHP) and or Biological Safety Program.
The following recommendations, useful for animal care personnel, address animal housing, waste and bedding. The method in which the animals are dosed with nano-particles will determine how animals should be housed. If the animals are subjected to an aerosol containing nanoparticles then they should be housed in “environmentally controlled cages” preferably in room with a negative pressure. If the animals are dosed with nanoparticles via ingestion or injection then they can be housed in conventional housing. Staff that care for the animals in either condition should wear appropriate PPE to prevent exposure to airborne materials or materials on surfaces from urine, feces etc. Workers who are disposing of contaminated bedding should also wear the appropriate PPE, including but not be limited to; protective eye wear, disposable gloves, dust mask, closed front disposable gown, hair cover and shoe covers. The bedding should be disposed off as biohazard material in red bags.
L. Registration of Nanoparticle Research
The use of nanopartiles at NF/SG VHS requires approval of nanoparticle research projects by the SRS.
M. Further Reading
Aitken, RJ et al. Manufacture and use of nanomaterials: current status in the UK and global trends. (In-depth review) Occupational Medicine 2006; 56: 300-306.
International Council on Nanotechnology http://icon.rice.edu/ National Institute for Occupational Safety and Health Nanotechnology Topic Pagewww.cdc.gov/niosh/topics/nanotech . The National Nanotechnology Initiative in the United States www.nano.gov .
N. References
1. RJ Aitken, KS Creely, CL Tran (2004). Nanoparticles: An occupational hygiene review. Institute of Occupational Medicine. Health and Safety Executive, Research Report 274. Retrieved October 6, 2006, from http://www.hse.gov.uk/research/rrpdf/rr274.pdf
2. Albrecht MA, Evans CW, and Raston CL. Green Chemistry and the Health Implications of Nanoparticles. Green Chemistry 2006; 8: 417-432.
Research Services: Laboratory Safety Manual Page 29

3. Bockmann J, Lahl H, Eckert T, and Unterhalt B: [Titanium blood levels of dialysis patients compared to healthy volunteers]. Pharmazie. 2000; 55: 468.
4. Borm PJA, Robbins D , Haubold S , Kuhlbusch T, Fissan H, Donaldson K, Schins RPF, Stone V, Kreyling W, Lademann J, Krutmann J, Warheit D, and Oberdorster E. The potential risks of nanomaterials: a review carried out for ECETOC. Particle and Fibre Toxicology 2006; 3:11.
5. Brown DM, Donaldson K, Borm PJ, Schins RP, Dehnhardt M, Gilmour P, et al. Calcium and ROS-mediated activation of transcription factors and TNF-alpha cytokine gene expression in macrophages exposed to ultrafine particles. Am J Physiol Lung Cell Mol Physiol 2004; 286:L344-L353.
6. Campbell A, Oldham M, Becaria A, Bondy SC, Meacher D, Sioutas C, et al.: Particulate matter in polluted air may increase biomarkers of inflammation in mouse brain. Neurotoxicology. 2005; 26: 133-140.
7. Campen MJ, McDonald JD, Gigliotti AP, Seilkop SK, Reed MD, and Benson JM: Cardiovascular effects of inhaled diesel exhaust in spontaneously hypertensive rats. Cardiovasc Toxic.l 2003; 3: 353-361.
8. Cui DX, Tian FR, Ozkan CS, Wang M, and Gao HJ. Effect of single wall carbon nanotubes on human HEK293 cells. Toxicol Lett. 2005; 155: 73-85.
9. Dung CH, Wu SC, and Yen SC. Genotoxicity0 and oxidative stress of mutagenic compounds found in fumes of heated soybean oil, sunflower oil and lard. Toxico. In Vitro. 2006; 20: 439-437.
10.Freites RA. Nanomedicine, vol IIA: Biocapatibility, Landes Bioscience, 2003 11.Heinrich U, Fuhst R, Ritteinghausen S, et al. Chronic inhalation exposure of
wistar rats and 2 different strains of mice to diesel-engine exhaust, carbon black, and titanium-dioxide. Inhalation Toxicology, 1995; 7:533-556.
12.Hoet PHM, Druske-holdeld I, and Salata OV. Nanoparticles – known and unknown health risks. J. Nanobiotechnol., 2004; 2: 12.
13.Jani PU, McCarthy DE, and Florence AT: Titanium dioxide (rutile) particles uptake from the rat GI tract and translocation to systemic organs after oral administration. J Pharm. 1994; 105 : 157-168.
14.Jia, G., H. Wang, et al. Cytotoxicity of carbon nanomaterials: single-wall nanotube, multi-wall nanotube, and fullerene. Environ Sci Technol, 2005; 5: 1378-83.
15.Kirchner C, Liedl T, Kudera S, Pellegrino T, Javier AM, Gaub HE, Stolzle S, Fertig N, and Parak WJ. Cytotoxicity of colloidal CdSe and CdSe/ZnS nanoparticles. Nano lett. 2005; 5:331-338.
16.Lee KP, Trochimowicz HJ, and Reinhardt CF. Pulmonary response of rats exposed to titanium dioxide by inhalation for two years. Toxicol Apply Pharmacol., 1985; 79:179-192.
17.Massimo B, Buckner S, Konstantina N, et al. Multi-walled carbon nanotubes induced T lymphocyte apoptosis. Toxicol. Lett. 2006; 160: 121-126.
18.Monteiro-Riviere NA, Nemanich RJ, Inman AO, Wang YY, Riviere JE. Multi-walled carbon nanotube interactions with human epidermal keratinocytes. Toxicol Lett. 2005; 3: 377-84.
19.Nefzger M, Kreuter J, Voges R, Liehl E, Czok R. Distribution and elimination of polymethyl methacrylate nanoparticles after peroral administration to rats. J Pharm Sci. 1984; 73: 1309-1311.
Research Services: Laboratory Safety Manual Page 30

20.Nigavekar SS, Sung LY, Llanes M, El Jawahri A, Lawrence TS, Becker CW, et al: 3H dendrimer nanoparticle organ/tumor distribution. Pharm Res. 2004; 21: 476-483.
21.Oberdorster G. Pulmonary effects of inhaled ultrafine particles. Int Arch Occup Environ Health. 2001; 1:1-8.
22.Oberdorster G, Oberdorster E, and Oberdorster J. Nanotoxicology: An emerging discipline evolving from studies of ultrafine particles. Environ. Health Perspect 2005; 113: 823-839.
23.Rehn B, Seiler F, Rehn S, Bruch J, and Maier M. Investigations on the inflammatory and genotoxic lung effects of two types of titanium dioxide: untreated and surface treated. Toxicology and Applied Pharmacology, 2003; 189:84-95.
24.Sayes CM, Fortner JD, Guo W, Lyon D, and Colvin VL. The differential cytotoxicity of water-soluble fullerenes. Nano Letters. 2004; 4: 1881-1887.
25.Stone V, Johnson GD, Wilton JC, Coleman R, and Chipman JK. Effect of oxidative stress and disruption of Ca2+ homeostasis on hepatocyte canalicular function in vitro. Biochem Pharmacol. 1994; 47: 625-632.
FOLLOW-UP RESPONSIBILITYThe Subcommittee on Research Safety is responsible for the annual review and revisions of this SOP as needed.
HAZARDOUS CHEMICALSA. Obtain and read Material Safety Data Sheets (MSDS) sheets before using any
chemicals.
B. Mercaptoethanol and other volatile reagents will be opened, aliquoted, etc., only in a fume hood.
C. Protect yourself from chemical exposures. Be sure to use appropriate personal protective equipment (lab coats, gloves, face shields, masks, goggles, etc.) when working with hazardous chemicals.
D. All flammable substances, bases and acids must be kept in their respective cabinets. Low flashpoint reagents requiring refrigeration will be kept in the explosion proof refrigerators in Room E354-1, and D119-1.
E. A suitable spill kit must be available in each laboratory that uses chemicals.
F. Chemical storage areas must be periodically examined to determine whether the containers and the chemicals in them are still safe, i.e., within a specified expiration date and with no visible corrosion.
G. Please become familiar with the proper waste procedures for the chemicals you use. Questions about chemical waste disposal can be directed to Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
H. If you have any chemicals for disposal (old, no longer used or past expiration date), please notify the Industrial Hygienist and use the appropriate form.
I. A container for disposal of old batteries (alkaline, NiCad, etc.) is located in E584-1.
Research Services: Laboratory Safety Manual Page 31

J. Hazardous chemicals MUST NOT be stored in chemical fume hood work areas.
K. After completion of daily work procedures, all hazardous chemicals MUST be returned to their proper storage locations.
L. If you plan to work with either perchloric acid or ethyl ether (or other peroxide formers) consult the policies in the R&D Safety Policies and Procedures Manual. Since these are highly hazardous chemicals all protocols involving the use of these chemicals require prior approval of the Subcommittee on Research Safety (SRS). If you are unclear about the safety procedures and/or proper disposal procedures for handling chemical substances, speak to your supervisor.
M. Date chemicals upon receipt and read labels carefully before using.
N. Mercury spills are cleaned by Environmental Management Services (EMS). Contact EMS at Ext. 6017 or Pager 32-1362 following a spill.
Research Services: Laboratory Safety Manual Page 32

HAZARDOUS AGENTS REPORTINGA. The Centers of Disease Control and Prevention (CDC), has identified certain
biological, chemical and radioactive materials or agents as having potential for use as weapons of mass destruction. Improper use and/or containment of these materials or agents pose a risk to national security because of their: (A) ease of dissemination or transmittal between individuals; (B) potential for high mortality rates and major public health impact; (C) potential for causing public panic and social disruption; and (D) risk for public health preparedness.
B. Storage and/or use of these materials or agents in any quantity in a Department of Veterans Affairs (VA) research laboratory requires special consideration for physical security, personnel access, inventory control, and emergency preparedness. The investigators who intend to work on the following hazardous agents must notify and obtain necessary approvals before beginning the research work. The investigators must promptly report to Deputy ACOS-R/ACOS-R, and Biosafety Officer on hazardous agent inventory level in their possession. The Biosafety Officer will inspect the laboratory at least semiannually for inventory and physical security measures.
1. Biological Select Agents and Toxins (This list is NOT comprehensive) :AbrinBacillus anthracis*Botulinum neurotoxins*Brucella abortus, Brucella melitensis, Brucella suisBurkholderia (Pseudomonas) mallei*Burkholderia (Pseudomonas) pseudomallei*Clostridium Botulinum*ConotoxinsCoxiella burnetiiCrimean-Congo hemorrhagic fever virusDiacetoxyscirpenolEastern Equine Encephalitis virusEbola virus*Foot and mouth disease virus*
Francisella tularensis*Lassa fever virusMarburg virus*Mycoplasma capricolumMycoplasma mycoidesNipah virus Reconstructed 1918 influenza virusRicinRickettsia prowazekiiRift Valley Fever virusSaxitoxin
Research Services: Laboratory Safety Manual Page 33

South America Hemorrhagic Fever viruses (Chapare, Junin, Machupo, Sabia, Guanarito)
Staphylococcal enterotoxins A, b, C, D, E subtypesT-2 ToxinTetrodotoxinTick-borne Encephalitis viruses (Far Eastern virus, Siberian type, Kyasanur Forest
disease virus, Omsk Hemorrhagic Fever virus)Variola major virus (Smallpox virus)*Venezuelan Equine Encephalitis virusYersinia pestis
*Denotes Tier 1 Agents, for more information refer to http://www.selectagents.gov/.
2. Chemical Agents :3-quinuclidinyl bezilate (BZ)Chlorine gasCyanogen chloride (CK)CyclosarinDiphosgeneHydrogen cyanide (AC)Lewisite (L) – note there are 3 individual chemicals included in this categoryLysergic acid dietylamide (LSD)Nitrogen mustard (HN-1, NH-2, or HN-3)Phogene (CG) – also known as carbonyl chloridePhosgene oxime (CX)Sarin (GB)Soman (GD)Sulphur mustard (H, or HD, or HT), also called mustard gas or mustard agentsTabun (GA)VX is both the name and symbol)
C. Radioactive Materials and/or Radiation Sources:1. The special considerations required for radioactive materials and/or radiation
sources should be based on the specific radionuclide, the half-life, and the quantity present. For a “radiation low-risk” situation, basic security measures should be followed.
2. “Radiation high-risk” is a single location or room where the total activity of a single radionuclide with a half-life of more than 3 days is greater than one Curie and the radionuclide is received, stored, or used. “Radiation high-risk” location and where radioactive materials and/or radiation sources are received, stored, or used.
3. As additional agents or materials are identified by the CDC, those agents or materials will be considered by VA as hazardous agents, and will be subject to the same security requirements as those agents or materials identified above in paragraph B.
Research Services: Laboratory Safety Manual Page 34

LABORATORY EQUIPMENT OPERATIONSA. Be sure operating procedures are posted or readily available for all equipment.
B. Never attempt to operate equipment without prior instruction from someone who knows how to use it correctly.
C. Do not leave heating elements (i.e., hot plates, Bunsen burners, etc.) operating and unattended in the lab.
D. Electrophoresis equipment may be left unattended, but it must be double checked before it is left to run overnight.
E. Use of Extension cords are prohibited except for temporary use (less than 90 days) if approved by Engineering Services (Electrical Shop). Any other exceptions must be approved in writing by the Facility Safety Officer. Extension cords shall mean any UL approved flexible electrical cord used solely for the purpose of extending power from an electrical source to electrically powered equipment. UL approved power strips or a uninterruptible power supply (UPS), may be used only for sensitive /critical electronic equipment (computer, printer, analytical instruments) where electrical surge protection or EMI/RFI filters are required or recommended by the equipment manufacture or Engineering Services (Electrical Shop). Power strips shall mean a UL approved electrical apparatus consisting of an enclosed strip containing one or more receptacles protected by a circuit breaker or fuse incorporated into its design, and powered by a flexible cord. A UPS shall mean an electrical apparatus that provides emergency power to a load when the input power source fails.
F. Frayed or damaged electrical cords must be reported to Engineering (Ext. 6025); initiate a work order so that the cord may be repaired or replaced.
G. Old or broken VA equipment that is no longer needed must be turned in to Research Service. Responsible laboratory must submit VA Form 90-2237 to Dr. Shen-Ling Xia who will handle the “turn-in” process. DO NOT dispose of VA equipment yourself – it is government property!
Research Services: Laboratory Safety Manual Page 35
CHEMICAL WASTE DISPOSAL
The key concern in chemical waste disposal is environmental responsibility. The disposal practices for all chemical wastes are articulated in the Hazardous Materials Management Manual issued by NF/SG VHS Memorandum No. 138-7. Before discarding any type of chemical wastes, check the appropriate Material Safety Data Sheet (MSDS) or consult with the Industrial Hygienist Bruce Carlberg. You will be instructed on what to do or the substance will be disposed for you. If you use any particular chemical substance regularly, the Industrial Hygienist can arrange scheduled pick-ups of hazardous wastes. Contact Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025.
A. Each laboratory is responsible for supplying their own glass disposal boxes (EMS only provides red bags for biohazard trash).
B. Disposed of all broken glass in a small white trash can lined with a standard (non-biohazard) plastic bag labeled, “Glass for Disposal”. When the box is 75% full, close it securely with tape, label it as “Glass for Disposal”, and place it on the laboratory floor for pick-up (DO NOT leave the trash can in the hallway). Also dispose of empty glass containers that are not broken, but need to be thrown out, in the white trash cans. These white trash cans must only contain glass that is not biohazardous.
C. Chemically contaminated glass items must be properly placed in a plastic container, and the container must be labeled and must be deposited with Industrial Hygienist for safe disposal. Note: Chemically contaminated glass must not be mixed with other waste, contact Mr. Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025 and for further instructions.
BIOLOGICAL HAZARD DISPOSAL
A. Biohazardous or potentially biohazardous trash (including but not limited to: tissue culture flasks, syringes without needles, tissue culture dishes/plates, plastic tubes and gloves) must be placed in biohazard bags (with red color).
B. Sharps (needles, glass and plastic pipettes, razor blades, etc.), whether contaminated or not, are to be disposed of in puncture proof “sharps” containers. When the container is 75% full, dispose of by labeling the container as ‘TRASH” in a red biohazard waste bag.
C. Furthermore, any biohazardous waste that contains glass must be disposed of in a puncture resistant Sharps container. This includes blood vials, glass vials, glass pipettes, Pasteur pipettes, etc.
D. For radioactive waste, see next two sections.
Research Services: Laboratory Safety Manual Page 36
RADIOISOTOPES
Principal Investigators must obtain prior approval from the NF/SG VHS Radiation Safety Committee/Radiation Safety Officer before initiating any new study involving radioisotopes. All personnel using radioisotopes must follow general laboratory safety guidelines. In addition they need to follow guidelines specific to radioisotopes for both safety, as well as, regulatory reasons. The following are only basic guidelines for working with radioisotopes. A copy of the full Radiation Safety Guide must be available in each laboratory using radioisotopes. All questions concerning radiation safety must be directed to the Radiation Safety Officer (RSO), Dr. Shailendra Shukla at ext. 6514/6059 or VA pager 1747 in room T3-09. Radiation Safety documents and forms are also available in NF/SG intranet homepage under Services / Nuclear Medicine / Radiation Safety.
A. All procedures using radioisotopes must comply with the Nuclear Regulatory Commission’s regulations, VA’s National Health Physics Programs guidelines, and our license conditions. A copy of our license is available in the above mentioned web-site.
B. Do not use radioisotopes unless you have undergone training from your supervisor and studied this document (See pages 5-6 for information on training). New laboratory personnel are not allowed to work with radioactive material until they are approved by the RSO. The NF/SG System’s RSO also provides periodic radiation safety training and all employees must attend at least one of these in each calendar year. New employees must attend first such available training.
C. Personnel radiation monitoring dosimeters are required for workers likely to receive greater than 10% of Federal radiation exposure limits. When working with radioisotopes, always wear a lab coat, radiation badge and gloves. Badges will be exchanged quarterly, and distributed to the laboratories by a designated Research Service representative. Do not take badges out of the building, and when not being worn always store them away from sources of radiation.
D. All purchase requests for radioactive material to be used at the NFSGVHS shall be pre-approved (submit a paper copy or e-mail request to the RSO: [email protected]) by the VA RSO or his designated representative.
E. Radioactive material must be stored in a locked cabinet, freezer or refrigerator that is clearly labeled "Caution Radioactive Material”.
F. Volatile forms of I-125 or I-131 must be opened in a fume hood. The designated iodination hood is in Research Common Resource Room E354-1. Consult with the RSO before initiating any iodination study.
G. Any room where radioactive work will be performed must be labeled "Caution Radioactive Material".
H. Never allow the radioisotope container to be uncapped any longer than necessary.
I. Place a double layer of bench cover in the designated area where you plan to work. DO NOT tape the bench cover to the bench top.
J. A radioisotope logbook must be maintained in each laboratory. The log must include:
Research Services: Laboratory Safety Manual Page 37

1. A log sheet for each vial of isotope recording the date received, lot number, amount used, and date;
2. A record of the amount of waste generated and its location; and
3. Weekly (or right after an experiment, if working with radioisotopes only occasionally) wipe test must be done for beta and gamma work areas. Wipe tests must be conducted for all areas where radioactive work has been performed. Counts per Minute (CPM) will be converted to Disintegrations per Minute (DPM) by dividing CPM’s by the counting efficiency of the counter. Any wipe test results greater than 200 DPM above background DPM must be decontaminated and retested. In any week in which radioisotopes are not used, and wipe tests are not necessary, a statement as such must be made in the log book. The Radiation Safety Officer will conduct periodic inspections of all radioactive work areas and log books.
K. Use a radiation survey meter when working with gamma emitters (such as 125I, 51Cr, and 35S) and high energy beta emitter (e.g., 32P). Be careful not to contaminate the probe. When taking a break, leaving the laboratory or at the end of a procedure, the work area and personnel involved must be monitored for contamination. The Survey meters must be calibrated at least once a year. Contact the RSO for arranging the calibration.
L. All containers, equipment and work areas, to be used during a procedure, must be properly labeled with radioactive tape.
M. Any spill must be contained with paper towels, and then cleaned with detergent until counts register at background level. All toweling, gloves, bench cover, etc., must be disposed of in the appropriate radioactive waste container. Skin contamination must be removed by washing with mild soap in tepid water flushing with large volumes of water. Care must be taken not to abrade the skin. Do not leave the immediate area without monitoring hands, lab coat and shoes when finished. If there is a major spill (i.e. involving more than 1 mCi) you must also report immediately to the RSO.
N. All radioactive waste containers must be kept in an area separate from where regular trash is stored. Radioactive waste containers must also have clearly visible labels for “Radioactive Waste” and “DO NOT REMOVE”.
O. Liquid radioactive waste containing non-hazardous chemicals and radioisotopes with a half-life of less than 120 days must (e.g. P-32) be stored in the laboratory until the radioactivity decays to background level. Upon verification by the RSO, such liquid must be disposed in the sink. Liquid waste containing hazardous chemicals (e.g. scintillation cocktails) or radioisotopes with half-lives of greater than 120 days (e.g. C-14, H-3) must be brought to NFSG VHS radioactive waste storage building. Make arrangement to bring the waste with the Assistant Health Physicist, Dave Watson (Ext. 6806, [email protected]) or with the RSO. The complete radioactive waste disposal policy is described in the Radiation Safety Guide.
P. The same rules applies to solid waste, i.e., waste containing or contaminated with radioisotopes with half-lives less than 120 days must be stored in the laboratory until the RSO verifies that the radiation level has decreased to background level. At that point, all radioactive labels must be defaced and the waste must be treated like regular
Research Services: Laboratory Safety Manual Page 38

trash. Waste containing or contaminated with radioisotopes with half-lives greater than 120 days must be brought to the radioactive waste storage building.
Q. Refer to the Radiation Safety Guide and consult with the RSO for the proper planning of any study involving radioactivity in animals.
R. All waste (solid or liquid) brought to the radioactive waste storage building must be bagged and clearly labeled. DO NOT mix isotopes together. Dry and liquid waste must be separate. Please leave scintillation vials in their cardboard trays.
S. The label must include:1. Isotope2. Date sealed3. Estimated activity (mCi)4. Laboratory Room Number5. Principal Investigator
IN VIVO ANIMAL PROCEDURES WITH USE OF RADIOISOTOPES
A. Prior approval is required of all animal protocols involving radioisotopes and must be granted by the NF/SG VHS Radiation Safety Committee, Research Subcommittee on Research Safety and IACUC.
B. Investigators wishing to work with radioisotopes in animals must review the procedure with the Facility Director and Chief Veterinary Medical Officer, prior to the initiation of the study. He/she will ensure that there is appropriate space and equipment.
C. A room housing studies with radioisotopes in animals must be clearly identified with appropriate signage on the door.
D. It is the Investigator’s responsibility to first consult with the Research Safety Officer (Bruce Carlberg, Industrial Hygienist at Ext. 4309/6025, [email protected]) and Radiation Safety Officer (Shailendra Shukla, Ext 6514, [email protected]). Correctly dispose of radioactive carcasses and other materials as directed by the Officers.
Research Services: Laboratory Safety Manual Page 39

LIQUID NITROGEN (LN2) SAFETY PLAN
(Major portions of this document were adapted from the Safety Precautions and Regulations for Dispensing Liquid Nitrogen at the Department of Physics & Astronomy, UNC-Chapel Hill, the Argonne National Laboratory Physics Division Cryogenic Safety Manual, and Environmental Health and Safety Office Liquid Nitrogen Safety, University of Hawaii John A. Burns School of Medicine).
The purpose of this document is to highlight general cryogenic safety practices and detail the process of dispensing liquid nitrogen (LN2) from the VA Common Resource Room D113-1. Lab and system-specific cryogenic safety training should be completed by the lab PI or other qualified personnel.
A. Overview of Cryogenic Safety HazardsCryogenic liquids (e.g., liquid helium, nitrogen, oxygen, carbon, or nitrous oxide) are liquefied gases that are kept in their liquid state at extremely low temperatures. LN2 is colorless, odorless and tasteless. It is non-flammable, physiologically inert and non-toxic. It is an extremely cold liquid with a boiling point of -196ºC = -320ºF.
There are many applications of LN2 in a biomedical research facility, one of the most common being cryopreservation. The storage of cells at temperatures below -130 ºC, is essential in order to preserve biological material unaltered.
The safety hazards associated with the use of cryogenic liquids can be categorized as follows:
1. Cold Contact BurnsLiquid or low-temperature gas from any of the specified cryogenic substances will produce effects on the skin similar to a burn.
2. AsphyxiationDegrees of asphyxia will occur when the oxygen content of the working environment is less than 20.9% by volume. Effects from oxygen deficiency become noticeable at levels below ~18% and sudden death may occur at ~6% oxygen content by volume. This decrease in oxygen content can be caused by a failure/leak of the cryogenic vessel or transfer line and subsequent vaporization of the cryogen.
3. Explosion – PressureHeat flux into the cryogen from the environment will vaporize the liquid and potentially cause pressure buildup in cryogenic containment vessels and transfer lines. Adequate pressure relief must be provided to all parts of a system to permit this routine out-gassing and prevent explosion.
4. Explosion - ChemicalCryogenic fluids with a boiling point below that of liquid oxygen are able to condense oxygen from the atmosphere. Repeated replenishment of the system can thereby cause oxygen to accumulate as an unwanted contaminant. Similar oxygen enrichment may occur where condensed air accumulates on the exterior of cryogenic piping. Violent reactions, e.g. rapid combustion or explosion, may occur if the materials which make contact with the oxygen are combustible.
Research Services: Laboratory Safety Manual Page 40

B. Training for Handling Cryogenic LiquidsIt is the Principal Investigator’s or Supervisor’s responsibility to ensure that staff handling liquefied gases are instructed and trained as to the nature and the safe handling of LN2. All VA paid and WOC employees who work in a VA lab with liquid nitrogen present must be initially instructed by the laboratory Principal Investigator on the handling of the gas (See pages 5-6 for information on training). This training must be in compliance with this LN2 Safety Plan.
All personnel working with cryogenic fluids must be thoroughly familiar with the hazards involved. They must also be familiar with all emergency measures that might be required in the event of an accident. Employees who have not worked with cryogenic fluids and systems must be trained on the job by Principal Investigator/ Supervisor/experienced employees until thoroughly familiar with safe methods of operation. PI must maintain training certificates of Personnel and a copy must be forwarded to SRS Coordinator.
The training must address:
The physical, chemical and physiological hazards associated with cryogenic fluids
The proper handling procedures for cryogens and cryogenic containers
The emergency procedures required in case of an accident
The reporting procedures in case of an accident
Additionally, each employee must receive training by the responsible scientist on the specific cryogenic equipment or system s/he is expected to use. This should cover:
Description of the equipment
Operating procedures
Maintenance schedule and procedures
Specific hazards
Reporting of incidents
The training shall be documented. The documentation shall include: 1) content of training, 2) date, 3) name of trainer, 4) a dated training attendance list showing names of the trainees (typed or printed) and their signatures. Send a copy of the training attendance document to the SRS Coordinator.
C. Cryogen HandlingThe hazards associated with the handling of cryogenic fluids include:
1. Cold contact burns and freezing (contact with cold liquid, gas or surface)
The potential for freezing by contact with the extreme cold of cryogens necessitates varying degrees of eye, hand and body protection. When a cryogenic fluid is spilled on a person, a thin gaseous layer apparently forms next to the skin. This layer protects tissue from freezing, provided the contact with the cryogen involves small quantities of liquid and brief exposures to dry skin.
Research Services: Laboratory Safety Manual Page 41
However, having moist skin, exposure to moving cryogens, or extended periods of time, can freeze tissue.
The most likely cause of frostbite to the hands and body is contact with cold metal surfaces. Since there is no protective layer of gas formed, frostbite will occur almost instantaneously, especially when the skin is moist. The damage from this freezing (frostbite) occurs as the tissue thaws. Intense hypothermia (abnormal accumulation of blood) usually takes place.
Additionally, a blood clot may form along with the accumulation of body fluids, which decreases the local circulation of blood.
Adequate protection and clothing is required at all times when handling, transferring or operating near cryogenic fluids. Should a burn occur, immerse the injured tissue in tepid water but do not rub or scratch the area.
2. Asphyxiation (displacement of oxygen by inert gas)
When liquid cryogens are expelled into the atmosphere at room temperature, they evaporate and expand on the order of 700 to 800 times their liquid volume. Even small amounts of liquid can displace large amounts of oxygen gas and decrease the oxygen content of the atmosphere below a safe level with a possibility of asphyxiation.
Whenever possible, handling of cryogenic fluids where release into the atmosphere is possible should be done in open, well-ventilated areas.
When there is the possibility of an oxygen deficiency hazard (ODH), oxygen monitors should be installed. If such a monitor triggers an ODH alarm, personnel are to leave the area immediately.
3. Explosion (excessive buildup of pressure in container of cryogenic fluid)
Heat flux into the cryogen is unavoidable regardless of the quality of the insulation provided. Since cryogenic fluids have small latent heats and expand 700 to 800 times to room temperature, even a small heat input can create large pressure increases.
Dewars must be moved carefully. Sloshing liquid into warmer regions of thecontainer can cause sharp pressure rises.
Pressure relief devices must be provided on each and every part of a cryogenic system. Satisfactory operation of these devices must be checked periodically and may not be defeated or modified at any time.
Vents must be protected against icing and plugging. When all vents are closed, enough gas can boil off in a short time to cause an explosion. Vents must be maintained open at all times.
Some materials may become brittle at low temperature and fail in the case of overpressure or mechanical shock. Only suitable materials may be used to store or transfer liquid cryogens.
Research Services: Laboratory Safety Manual Page 42
D. Personal Protective Equipment (PPE) is required when handling LN2Whenever handling or transfer of cryogenic fluids might result in exposure to the cold liquid, boil-off gas, or surface, protective clothing shall be worn.
1. Face shield required. LN2 can splatter, possibly onto face and eyes. Safety glasses (even with side shields) or goggles are not sufficient to protect the face.
2. Insulated gloves required (gloves should be loose fitting, so they can be quickly removed if liquid pours into them, or they should be elastic cuff insulated gloves). Inspect the gloves for damage before use.
3. A splash resistant lab coat is required to minimize skin contact. A floor length splash resistant apron may also be worn.
4. REQUIRED: Closed toe shoes that cover the top of the foot or boots with cuff-less trouser legs extended over the top of the boots to prevent LN2 from spilling into them.
5. Prior to use inspect all PPE for damage. If any PPE is damaged or missing, DO NOT PROCEED until items are replaced.
E. Dispensing of LN21. Under no circumstances should you leave the area while filling a dewar.
2. Open the lock on the gate. See Research Office if you don’t have a key.
3. Put on protective clothing as described in 2.2.
4. Look for any warning signs or indications that the LN2 tank should not be used (i.e., metal fill hose connections are leaking).
5. If necessary, attach the metal fill hose to the LN2 tank (you will need at least one wrench). Be careful not to cross thread the fittings when attaching the hose - hold up the metal fill hose when attaching to threaded connector on LN2 tank so that both connections are in a straight line when the connections are screwed together.
6. Open the venting valve on your dewar, if applicable.
7. Open the valve on the top of the LN2 tank (turn the valve handle counterclockwise). Hold onto the metal fill hose when opening the top valve on LN2 tank so that the hose doesn’t move when the pressure and LN2 flow increases into the hose. DO NOT HAVE YOUR FACE DIRECTLY OVER THE OPENING OF THE DEWAR WHEN FILLING!
8. When the LN2 is initially filling/cooling the metal hose and the dewar, there will be a whistling sound as they cool – this should last only for a minute or two. After the metal fill hose has covered over with frost the whistling sound should decrease, if still whistling then open the top valve on the LN2 tank further (the valve on the LN2 tank must be opened up by at least one full turn and that should stop the whistling). If the whistling persists, then (1) the LN2 tank is near empty or (2) the carrier gas for LN2 in the tank has been blown off and LN2 cannot be transferred from the tank – change over to a full LN2 tank. It is important to open
Research Services: Laboratory Safety Manual Page 43

up the top valve on the LN2 tank when filling otherwise just the carrier gas is escaping- not liquid nitrogen.
9. As the dewar is filling, watch and listen for indications that it is nearly full.
10.Close the valve and check the level to avoid overspill.
11.When finished, close the valve (turn the valve handle clockwise) and remove the hose from the dewar.
12.Move your dewar from the filling area and lock the gate.
F. Emergency ProceduresIf problems occur with the filling valve, the main valve of the tank can be used to shut off the flow. It is located on the top of the LN2 tank – turn clockwise (to the right).
In case of emergency, e.g. explosion of a dewar, leave the area immediately - dial 911.
If LN2 comes in contact with eyes or immerses skin, seek immediate medical attention.
Report all emergencies and accidents to your PI, Research Office, and Industrial Hygiene Officer.
G. Restrictions1. LN2 is to be used only for legitimate research needs in the VA research facilities.
Use for off-VA activities should be approved in advance by VA Research Service administrators. Any other use is considered theft and is prohibited.
2. LN2 is to be obtained only by those who have been appropriately trained to do so.
3. When transporting LN2, vessels need to have a secure lid - all transportation vessels need to be rated for cryogenic use. DO NOT TRANSPORT LN2 IN SYTROFOAM BOXES.
4. Failure to wear appropriate protective clothing will result in suspension of privileges.
H. TipsThere is no need to open or close the top LN2 tank valve with tools. It should be closed firmly, but does not require white knuckled torque - this can damage the valve.
When filling a wide-mouth dewar, a meter stick can be used as a dipstick. Dunk it into the dewar for a few seconds and when removed, the frost line will indicate the height of the liquid.
A cold dewar fills much more efficiently than a warm dewar. As with your car, do not wait until yours is completely empty to fill it back up.
(Updated on 04/01/2013)
Research Services: Laboratory Safety Manual Page 44
Research Service
CHEMICAL HYGIENE
PLAN
U.S Department of Veterans AffairsNorth Florida/South Georgia Veterans Health System
Malcom Randall Division1601 SW Archer RoadGainesville, FL 32608
Research Services: Laboratory Safety Manual Page 45

Research Services: Laboratory Safety Manual Page 46

Research Service
SECTION III. CHEMICAL HYGIENE PLAN (CHP)
TABLE OF CONTENTS Page
I. GENERAL PRINCIPLES 49A. Minimize All Chemical Exposures 49B. Provide Adequate Ventilation 49C. Institute a Chemical Hygiene Plan 49D. Observe the PELs and TLVs 49
II. RESPONSIBILITIES 50A. ACOS for Research 50B. Administrative Officer 50C. Principal Investigators 50D. Chemical Hygiene Officer 51E. Employees 51
III. THE RESEARCH FACILITY 51A. Design 51B. Maintenance 51C. Usage 51D. Ventilation 52
IV. COMPONENTS OF THE CHEMICAL HYGIENE PLAN 52A. Environment of Care (EOC) Manual 52B. Laboratory Safety Manual 52C. Biosafety Manual 52D. Hazardous Materials Management Manual 52E. Chemical Procurement and Storage 52
1. Procurement2. Storage
a. Flammablesb. Incompatible Chemicals
F. Exposure Monitoring 54G. Housekeeping, Maintenance and Inspections 55
1. Housekeeping2. Maintenance3. Inspections4. Passageways
H. Medical Program 561. Routine Surveillance2. Emergency First Aid Procedures
a. Eyeb. Cuts, Punctures and Needle sticksc. Chemical Burns
I. Protective Apparel and Equipment 571. Personal Protective Equipment 57
Research Services: Laboratory Safety Manual Page 47

2. Laboratory Responsibilities and PPE 573. Types of Personal Protection Equipment 57
a. Eye Protection b. Glovesc. Other Personal Protective Equipment
J. Recordkeeping 581. Accident Reporting2. Medical Recordkeeping3. Chemical Inventory
K. Signs and Labels 591. Types2. Chemical Labeling
L. Spills and Accidents 601. Mercury Spills2. Acid-Base Spills3. Large Mixed Spills4. Biological Spills5. Spill Evaluation
M. Employee Information and Training 61N. Disposal of Hazardous Wastes 62
1. Liquid Wastes2. Liquid Hazardous Wastes3. Biohazardous Wastes4. Batteries
V. GENERAL PROCEDURES FOR WORKING WITH CHEMICAL AND 64
HAZARDOUS AGENTSA. General Requirements 64B. Special Research Procedures 65
1. Compressed Gasses2. Radioactive Substances3. Caustic Materials4. Formaldehyde5. Xylene6. Carcinogens7. Perchloric Acid8. Use and Exposure to Biological, Chemical and Physical Agents
VI. SAFETY RECOMMENDATIONS 70A. Electrical Safety 70B. Fire Safety 70C. Control of Fires 71
VII. TECHNICAL GUIDANCE 72REFERENCES 72OSHA WEB SITE 73SIGNATURE SHEET 75APPENDIX A 77
Hazardous Materials Data: Information and Recommended Form
Research Services: Laboratory Safety Manual Page 48

RESEARCH SERVICE CHEMICAL HYGIENE PLAN (CHP)
I. GENERAL PRINCIPLESThe following principles govern the Research Service Chemical Hygiene Program for this Medical Center:
A. MINIMIZE ALL CHEMICAL EXPOSURE
Because few chemicals used in Research Service are without hazards, general precautions for handling all laboratory chemicals should be adopted, rather than specific guidelines for each particular chemical. Skin contact with chemicals should be avoided as a cardinal rule.
Even for substances of no known significant hazard, exposure should be minimized. For work with substances which present special hazards, special precautions should always be taken. One should assume that any mixture will be more toxic than its most toxic component and that all substances of unknown toxicity are toxic.
B. PROVIDE ADEQUATE VENTILATION
The best way to prevent exposure to airborne substances is to prevent their escape into the working atmosphere by the use of hoods and other ventilation devices.
C. INSTITUTE A CHEMICAL HYGIENE PROGRAM
A mandatory chemical hygiene program designed to minimize exposures is needed. It should be a regular, continuing effort, not merely a standby or short-term activity. Its recommendations are expected to be followed in teaching laboratories as well as by full-time laboratory workers. This document fulfills the need for a chemical hygiene plan.
D. OBSERVE THE PELs AND THE TLVs
The Permissible Exposure Limits (PELs) established by the Occupational Safety and Health Administration (OSHA) of the U.S. Department of Labor and the Threshold Limit Values (TLVs) established by the American Conference of Governmental Industrial Hygienists (ACGIH) should not be exceeded. (OSHA Standards available at www.OSHA.gov, and in the office of the Safety Officer, Mr. Ray Kerr, Room EB100-1, Ext. 6560, [email protected] .)
Research Services: Laboratory Safety Manual Page 49

II. RESPONSIBILITIESA. ACOS for RESEARCH
1. Oversees all phases of the Research Chemical Hygiene Plan.
2. Appoints the Chemical Hygiene Officer and members of the Subcommittee for Research Service (SRS).
B. ADMINISTRATIVE OFFICER
1. Investigates incidents or unsafe conditions concerning hazardous chemicals and assures prompt action is taken to prevent reoccurrence.
2. Ensures the development of procedures to properly use, store and dispose of hazardous chemicals utilized in Research Service.
3. Ensures training of employees on safe handling and disposal of hazardous materials, utilizing the resources of the Subcommittee for Research Service (SRS) and the Medical Center Industrial Hygienists and Safety Specialists.
4. Actively participates in the Research Service Safety Subcommittee and solicits the assistance of all members in the performance of workplace inspections and training of laboratory personnel on elements of the Chemical Hygiene Plan.
5. Ensures that each research laboratory maintains an inventory of hazardous materials that is accurate and complete; copies will provided to the Medical Center Industrial Hygienist upon request. The inventory of hazardous chemicals is required to be updated semi-annually.
6. Ensures that appropriate employees are trained on the safe handling and disposal of hazardous chemicals.
C. PRINCIPAL INVESTIGATORS
1. Ensures the development of procedures to properly use, store and dispose of hazardous materials utilized in Research Service laboratories as investigational activities are performed.
2. Ensures that anyone who works or otherwise performs educational or research activities in VA owned or operated research laboratories (whether paid or unpaid) are trained on topics related to handling and disposal of hazardous materials, means of safe egress from the building, and other actions designed to preserve occupational health and property.
3. Ensures that less hazardous chemicals are substituted where possible for dangerous substances in order to minimize potential exposure and reduce the volume of regulated waste generated.
4. Ensures that all activities performed in research laboratories are performed in accordance with the practices described in this plan.
5. Ensures that all staff in each laboratory are apprised of the location of this plan in the workplace and its contents as it relates to activities performed by workers.
Research Services: Laboratory Safety Manual Page 50

D. CHEMICAL HYGIENE OFFICER
1. Knowledgeable of all facets of the Chemical Hygiene Plan including the regulatory requirements surrounding its administration (see: www.OSHA.gov ) and its implementation.
2. Ensures that hazardous chemicals are stored, used and disposed of in compliance with Federal, State and local regulations.
3. Assists the Program Coordinator in investigation of incidents or unsafe conditions concerning hazardous chemicals and assures prompt corrective action is taken to prevent reoccurrence.
4. Performs periodic inspections of Research Service laboratories in order to assure compliance with the requirements of the Medical Center Safety, Occupational Health and Fire Protection Manual and all applicable medical center memorandums.
E. EMPLOYEES
1. Read and conduct each laboratory task in accordance with the requirements established by the Chemical Hygiene Plan.
2. Promptly report all unsafe conditions or unsafe use of hazardous chemicals to their immediate supervisors.
3. Develop good personal chemical hygiene habits.
III. THE RESEARCH SERVICE FACILITYA. DESIGN
The Research Service facility should have:
1. An appropriate general ventilation system with air intakes and exhausts located so as to avoid the intake of contaminated air.
2. Adequate, well-ventilated stockrooms and storerooms.
3. Laboratory hoods, where necessary, and sinks in each laboratory.
4. Other safety equipment including eyewash fountains and fire extinguishers.
5. Arrangements for safe and legal waste disposal.
B. MAINTENANCE
Chemical hygiene related equipment (hoods, exhaust fans, etc.) will undergo continuing preventive maintenance and be modified if inadequate.
C. USAGE
The work conducted and its scale must be appropriate to the physical facilities and especially to the quality of ventilation.
D. VENTILATION
Research Services: Laboratory Safety Manual Page 51

The system should:
1. Provide a source of air for breathing and for input to local ventilation devices.
2. It should not be solely relied upon for protection from toxic substances released into the laboratory.
3. Ensure that laboratory air is continually exchanged thereby preventing increase of air concentrations of toxic substances during the working day.
4. Ensure that direct airflow into the laboratory is from non-laboratory areas to the extent that air will be forced out to the exterior of the building.
5. Quality and quantity of ventilation should be evaluated on installation and regularly monitored annually by Facilities Management.
IV. COMPONENTS OF THE CHEMICAL HYGIENE PLANA. ENVIRONMENT OF CARE (EOC) MANUAL
All procedures contained in the EOC manual are included by reference into this Chemical Hygiene Plan.
B. LABORATORY SAFETY MANUAL (Bound with this manual)
Specific procedures also outlined in the laboratory safety manual are included by reference into this Chemical Hygiene Plan.
C. BIOSAFETY MANUAL (Bound with this manual)
All procedures contained in the Biosafety Manual are incorporated into this Chemical Hygiene Plan.
D. HAZARDOUS MATERIALS MANAGEMENT MANUAL (Issued by NFSGVHS Memorandum No.138-7)
Various procedures as applicable that are contained in the Hazardous Materials Management Manual (HMMM) are incorporated by reference into this Chemical Hygiene Plan.
E. CHEMICAL PROCUREMENT AND STORAGE
1. Procurement
a. All chemicals received and utilized in Research Service laboratories must have a Material Safety Data Sheet (MSDS), obtainable from the respective manufacturers.
b. When ordering hazardous materials, research personnel must request that the manufacturer provide an MSDS for the product using the procedures outlined in NFSGVHS Memorandum No. 138-14, “Hazard Communication Program”.
c. When possible, less hazardous substitutes should be found for more dangerous chemicals.
2. Storage
Research Services: Laboratory Safety Manual Page 52

a. Flammables
1) Quantities of 2 gallons or more must be stored in a safety can or approved flammable storage cabinet.
2) Small quantities (working amounts) can be stored on open shelves. Bulk storage that is 5 gallons or more must be stored in an approved flammable storage cabinet or designated room.
3) Chemicals such as ether must not be stored in a closed area such as a refrigerator. Ether should not be kept in storage for more than one year unless it contains inhibitors known to prevent the formation of peroxides. Opened containers of ether should be discarded within six months of the date the chemical was first opened. Ether should not be discarded via the drain. Empty containers should be placed in a fume hood overnight before discarding.
4) Flammables must be stored in laboratory safe refrigerators only, if they must be kept cool.
5) Any refrigerator to be used for the storage of flammables must be labeled in red letters or white lettering with a red background.
6) The transfer of flammables from one metal container to another should be preceded by electrical bonding in order to avoid creation of a static spark that may result from pouring the solvent.
b. Incompatible ChemicalsIncompatible chemicals requiring separate storage areas are noted as follows:
CHEMICAL INCOMPATIBLE SUBSTANCESAlkali metals (calcium, potassium, sodium)
Water, carbon dioxide, carbon tetrachloride
Acetic Acid Chromic acid, nitric acid, ethylene glycol, perchloric acid
Acetylene Copper, fluorine, bromine, chlorine, iodine, silver, mercury and their compounds
Acetone Concentrated sulfuric and nitric acids
Ammonia (anhydrous) Mercury, halogens, calcium, hypochlorite, hydrogen fluoride
Ammonium nitrate Acids, metal powders, flammable liquids, chlorates, nitrates, sulfur and finely divided metals
Aniline Nitric acid, hydrogen peroxide
Bromine Ammonia, acetylene, butadiene, butane, hydrogen, sodium carbide and finely divided metals
Chlorates Ammonium salts, acids, metal powders, sulfur, finely divided organics or combustibles, carbon
Chromic acid Acetic acid, naphthalene, camphor, alcohol, glycerin, turpentine and other flammables
Chlorine Ammonia, acetylene, butadiene, benzene, and other petroleum fractions, sodium carbides, turpentine, and finely divided powdered metals
Cyanides Acids
Research Services: Laboratory Safety Manual Page 53

CHEMICAL INCOMPATIBLE SUBSTANCESHydrogen peroxide Copper, chromium, iron, most metals or their respective salts, flammables, aniline,
nitromethane
Hydrocarbons Nitric acid, oxidizing gases
Iodine Acetylene, ammonia
Mercury Acetylene, formic acid, ammonia
Nitric acid Acetic, chromic and hydrocyanic acids, aniline, carbon, hydrogen sulfide, flammables, readily nitrated substances
Oxygen Oils, grease, hydrogen, flammables
Oxalic acid Silver, mercury
Perchloric acid Acetic anhydride, bismuth and its alloys, alcohol, paper, wood and other organic materials
Phosphorus pentoxide Water
Potassium permanganate
Glycerin, ethylene, glycol, benzaldehyde and sulfuric acid
Sodium Any oxidizable substance, i.e., methanol, glacial acetic acid, carbon disulfide, benzaldehyde, ethylene glycol, ethyl acetate, etc.
Sulfuric acid Chlorates, perchlorates, permanganates
Flammable liquids Ammonium nitrate, chromic acid, hydrogen peroxide, nitric acid, sodium peroxide, the halogens
F. EXPOSURE MONITORING
The Industrial Hygienist is responsible for evaluating exposure to hazardous materials as explained in NFSGVHS Memorandum 138-15, “Industrial Hygiene Program." Therefore, the uses of hazardous materials are expected to afford the Industrial Hygienist the opportunity to perform personal monitoring to determine exposure concentrations of various substances for which standards have been developed. A list of substances for which the Occupational Safety and Health Administration (OSHA) of the U.S. Department of Labor has established regulatory limits (OSHA Standards available at www.OSHA.gov, and in the office of the Industrial Hygienist, Bruce Carlberg, Room EB100-1, Ext. 4309, [email protected].)
1. The following list of substances may be evaluated by the Industrial Hygienist:
a. Formaldehydeb. Xylenec. Toluened. Mercurye. Ethanolf. Methanolg. Others as deemed necessary
Research Services: Laboratory Safety Manual Page 54

3. The Subcommittee on Research Safety (SRS) can request the Industrial Hygienist to conduct an evaluation of any workplace exposure if conditions warrant it.
4. All Research Service employees are responsible for notifying their immediate supervisor of any potential exposures to chemical hazards. Contact the Industrial Hygienist to ascertain the degree of hazard posed by chemical hazards.
G. HOUSEKEEPING, MAINTENANCE AND INSPECTIONS
1. Housekeeping
a. Housekeepers employed by Environmental Management Program (137) are responsible for routinely cleaning all floors and emptying designated trash cans in Research Service laboratories.
b. Research Service personnel are responsible for daily cleaning of all bench tops and other work areas such as fume hoods and laminar flow hoods.
c. All computer keyboard covers, when used, should be routinely replaced.
d. All telephones in laboratories using infectious agents will be routinely disinfected.
2. Maintenance
a. The Research Service Biomedical Engineering Technician is responsible for all routine maintenance on laboratory equipment with exception of those items specifically designated for preventive maintenance by Facilities Management Service.
b. All laminar flow hoods and fume hoods and biological safety cabinets will be inspected, cleaned and certified by a commercial vendor at least on an annual basis. Staff will not use hoods lacking certification or where certification has expired.
c. Eyewash Stations and Showers
1) Facilities Management Service will inspect all eyewash stations and showers located in research laboratories at an appropriate interval.
2) Research Service personnel are responsible for promptly reporting problems with eyewash units to Engineering Service.
d. Fire Extinguishers
The Medical Center Safety Specialist will inspect all fire extinguishers located in Research Service laboratories on a periodic basis. Accessibility will be maintained at all times to fire extinguishers. The use and maintenance of these units will be governed in accordance, with procedures contained in the EOC Manual. Fire extinguishers will remain unobstructed and not be used to prop open doors.
3. Inspections
Members of the Subcommittee on Research Safety (SRS) will perform formal inspections of laboratories on a periodic basis in order to ensure strict
Research Services: Laboratory Safety Manual Page 55

adherence to all safety practices. Inspections performed by a joint team of VA and representatives of the University of Florida Environmental Health and Safety (EHS) office via a Memorandum of Understanding (MOU) may also be performed in lieu of an SRS-designated team.
4. Passageways
a. Stairwells and hallways will not be used as storage areas.b. Access to emergency exits, emergency equipment and utilities controls
must not be blocked.
c. Emergency exit routes will be clearly posted.
H. MEDICAL SURVEILLANCE PROGRAM
Medical surveillance activities will be conducted in accordance with NFSGVHS Memorandum No. 05-16, "Employee Health Services."
1. Routine SurveillanceThe Employee Health Service administered by Human Resources Management Service (HRMS) oversees the medical surveillance program, as outlined in the above-noted memorandum for all VA Employees who are exposed to hazardous materials above permissible exposure levels.
2. Emergency First Aid Proceduresa. Eye
1) In the event of a chemical splash to the eyes, laboratory employees may ask co-workers to assist in washing the eyes. Eyelids must be lifted to avoid pooling of chemicals under them. They must be flushed with water for at least 15 minutes.
2) Medical attention must be sought immediately through the Employee Health Service.
3) The accident must be reported to the immediate supervisor as soon as possible.
4) Supervisors will fill out the automated Form 2162, "Report of an Accident," and CA-1 as specified by NF/SGVHS Memorandum No. 05-23, “Employee On-The-Job Injury/Occupational Illness or Disease” to the Research Service Office who will forward it within six (6) days to the Safety Specialist (138) and worker compensation specialist (05) respectively.
b. Cuts, Punctures, Needle sticks and Animal Bites1) All injuries such as cuts, punctures, needle sticks and animal bites
should be treated by employee health personnel immediately.
2) Reports as noted above must be properly filled out and submitted to the proper official.
c. Chemical Burns
Research Services: Laboratory Safety Manual Page 56

1) Corrosives can cause second or third degree burns. These chemicals include alkalis such as sodium hydroxide and common acids such as hydrochloric, sulfuric and nitric.
2) Chemicals should be diluted and washed off with copious amounts of water. Minor splashes and spills can be flooded in a sink. Larger splashes and spills require the use of the emergency showers. Ask co-worker for help. Material Safety Data Sheets (MSDSs) often contain the most complete information on the medical treatment options when exposed to hazardous materials. Some chemical powders should be brushed off the skin before flooding with water to avoid further skin and tissue damage. Always consult the MSDS for proper handling procedures when using hazardous materials. All chemical burns should be treated promptly by employee health personnel. Supervisors must complete all reports as noted in Paragraph a. above.
I. PROTECTIVE APPAREL AND EQUIPMENT
1. Personal protective equipment includes gloves, goggles, face shields, aprons, gowns and masks. Although the use of such equipment is generally the least desirable way to control workplace hazards because it places the burden of protection on the worker, the equipment must be available for situations when an unexpected exposure to chemical substances, physical agents or biological materials could have serious consequences. Safety Data Sheets (SDSs) should be consulted to determine the proper personal protective equipment requirements.
2. Each laboratory is responsible for procuring personal protective equipment from its project funds. Before the purchase or use of any personal protective equipment, the Medical Center Industrial Hygienist or Safety Specialist must be consulted to determine whether the equipment is acceptable.
3. Types of Personal Protection Equipment
a. Eye Protection
1) Chemical splash goggles and/or face shields, rather than safety glass should be used when pouring any hazardous chemicals or hazardous waste as they provide the best protection against splashes.
2) Protective eyewear must be available in all areas where hazardous substances are utilized.
3) Protective eyewear should be easy to clean and maintain. It must be clean and in good condition.
4) For those employees who wear glasses, goggles must fit over the glasses. Shoes must be worn at all times in the laboratory. Substantial shoes must be worn in areas where chemicals are in use or mechanical work is being done. As used in this policy, the term "substantial shoes" means shoes that do not provide protection against spilled liquids or semi-liquids such as chemicals, culture media, etc. Clogs, perforated shoes, sandals and cloth shoes are examples of shoes that do not meet this requirement. The use of shoe coverings
Research Services: Laboratory Safety Manual Page 57

may be appropriate in some cases, but their use should be limited as other hazards may be imposed by the use of these items (e.g., wet floors may become more slippery when walking on them with shoe covers). The procurement of such items is considered to be personal protective equipment and should be purchased by each research laboratory's operating funds.
b. Gloves
1) The need to use gloves for hand protection must be determined by each Principal Investigator. Should such protection be necessary, it is the responsibility of each research laboratory to purchase such items using appropriate grant monies.
2) Employees must wear gloves when handling all blood and body fluids and similar fluids from contaminated animals.
3) Special acid-resistant gloves may be necessary when handling acids.
4) Gloves should be used whenever substantial hand contact with solvents is possible.
5) Special gloves must be used when handling containers of cryogenic materials.
c. Other Personal Protective Equipment
1) Acid-resistant aprons must be worn when pouring such chemicals.
2) Respirators will be provided in areas where exposure to hazardous substances exceeds permissible concentrations. Only the Industrial Hygienist is allowed to prescribe the use of such devices. This action will be conducted in accordance with NFSGVHS Memorandum No. 138-12, "Respiratory Protection Program."
J. RECORDKEEPING
1. Accident Reporting
a. Procedures for completing an electronic "Report of an Accident," will be followed as described in NFSGVHS Memorandum No. 05-23, “Employee On-The-Job Injury/Occupational Illness or Disease”. This includes the completion of an electronic accident report by the immediate supervisor on behalf of the injured employee within 2 working days of the incident.
b. The Research Office will cooperate with Occupational Health personnel to ensure that the employees’ rights are preserved throughout the accident reporting and (if necessary) medical treatment process.
2. Medical Record Keeping
Medical records will be retained in accordance with NFSGVHS Memorandum No. 138-21, "Employee Access to Medical and Exposure Records."
3. Chemical Inventory
Research Services: Laboratory Safety Manual Page 58

a. An inventory of all hazardous chemicals will be compiled by the occupants of each research laboratory and used as a table of contents for the SDS collection.
b. A copy of the chemical inventory will be sent to the Medical Center Industrial Hygienist upon request.
c. The inventory of hazardous chemicals should contain the following information:
1) Name (as it appears on the label)
2) Manufacturer/supplier
3) Material Safety Data Sheet, if available
4) Method of disposal
5) Container size
6) Manufacturer/supplier stock or catalog numberd. Inventories will be updated twice a year to ensure that each chemical
found in the laboratory has an MSDS available for employees' use. Should a hazardous substance no longer be used in the workplace, the MSDS will be removed from this binder and sent to the Industrial Hygienist so stating that fact.
e. It is encouraged that the Hazardous Materials Data Form in Appendix A below be used to document the bi-annual laboratory chemical inventory for each VA laboratory.
K. SIGNS AND LABELS
1. TypesProminent signs and labels of the following types will be posted. This activity will meet the requirements of the VA Signage Manual that is maintained by Building Management Service (137).a. Telephone numbers of emergency personnel and supervisors should be
kept posted in each laboratory, preferably on each telephone handset. Stickers are available from the Safety Officer (Ext. 6050).
b. Location signs for eyewash stations, fire extinguishers, spill kits and other safety and first aid equipment.
b. Location of emergency exits.
c. Warning at areas where unusual hazards exist such as radioactive materials, lasers, biohazardous agents in use, etc. The Industrial Hygienist will maintain warning signs on “Notice” boards on doors to research laboratories in accordance with procedures described in the Environment of Care (EOC) Manual.
2. Chemical Labelinga. Original labels on containers of chemicals will not be defaced or removed.
Labels (either placed on containers by manufacturers or added by laboratory personnel) must include:
Research Services: Laboratory Safety Manual Page 59

1) Chemical identity
2) Appropriate hazard (i.e., caustic, corrosive, poison, irritant, flammable, carcinogen, etc., if noted on label)
3) Target organ effects (if any) as described in the appropriate MSDS.
b. Upon receipt, lab staff will annotate all chemical containers with the following information:
1) Date received
2) Expiration date, if any
3) Date opened
4) Storage requirements
c. Container labeling requirements contained in NFSGVHS Memorandum No. 14, “Hazard Communication Program” and the Hazardous Materials Manual will be followed.
L. SPILLS AND ACCIDENTS
This medical facility’s chemical spill response plan (in simplified terms) is (1) tell others in the general area about the spill, (2) clean the spill yourself if you can do so safely (based on your subjected knowledge of the spilled material and the factors at play); otherwise (3) Contact the Industrial Hygienist immediately at Ext. 4309/6534/6025. For nights and weekends, call Graphic Control at extension 6616, state that a chemical spill has occurred and ask for the Industrial Hygienist to be contacted. All large spills must be reported in writing to the Subcommittee on Research Safety. All spills will be handled in accordance with the procedures outlined in Chapter 3, Section 6 of the Medical Center's Disaster Manual. Spill control kits must be available in each laboratory and be suitable for the substances in use. Each researcher is responsible for providing suitable kits. Commercial kits are available from a variety of sources. Each laboratory supervisor must instruct all employees that spill kits located in laboratories can only be used by the Industrial Hygienist or under his direct supervision.
1. Mercury spills will be handled in accordance with NFSGVHS Memorandum No. 17, "Mercury Management Policy." Briefly, spill procedures are as follows:
a. Turn off any supplemental ventilation devices, if any, in the area,
b. Evacuate personnel from the area of the spill, and
b. Immediately notify Environmental Management (extension 6017/6531, or pager #1362) or the Industrial Hygienist (Ext. 4309/6534/6025).
c. After normal working hours, the caller should page 1362 and state that a mercury spill has occurred. The Environmental Management supervisor on duty will dispatch a trained responder to clean the spill.
Research Services: Laboratory Safety Manual Page 60

2. Acid-Base Spills that are small (i.e., a few drops) may:
a. Be absorbed or neutralized at once by using spill kits available in each laboratory.
b. Require the use of special protective equipment such as goggles, gloves, masks, fluid impervious gowns or aprons should be used for cleanup.
b. Require, in the event of a large spill, ventilation of the area, evacuate the area and notify the Industrial Hygienist.
3. Large Spills may necessitate...
a. Turning off any supplementation ventilation (such as fans) located in the area.
b. Evacuation of the area at once.
c. Following the instructions outlined in Chapter 3, Para. 6 of the Emergency Management Plan found in the reference section of the NFSGVHS website.
d. Never attempting to clean up a spill larger than can be contained or accommodated by the spill kits.
4. For Medical Spills that may be cleaned by lab personnel...
a. Spills of certain chemicals may cause the generation of aerosolized droplets that may require...
1) Evacuation of the area immediately.
2) Notification of the Industrial Hygienist immediately.
b. Small spills with aerosol formation may require...
1) Placement of paper towels over spill.
2) Flooding the area of a spill of a biological agent with a phenolic disinfecting agent or 5% sodium hypochlorite (bleach) and letting it set for at least 10 minutes.
3) Wearing gloves to pick up contaminated materials and dispose of materials in biohazard-labeled bags.
5. Spill Evaluation
a. Spills may be investigated by the Subcommittee on Research Safety (SRS) and the Industrial Hygienist.
b. Following analysis, information may be provided to all research personnel to prevent further incidents.
M. EMPLOYEE INFORMATION AND TRAINING
1. A copy of the Research Chemical Hygiene Plan (CHP) shall be kept in each Research Service laboratory and be available for all employees and students to read. A copy of the CHP will also be kept in the Research Service Office.
Research Services: Laboratory Safety Manual Page 61

2. Research Service personnel and students will be educated on the safe handling practices to avoid exposure to chemicals including the permissible exposure limits of OSHA regulated substances. This activity will be documented in accordance with the procedures outlined in NFSGVHS Memorandum No. 11-39, “Training Education Management Program (TEMPO)." Principal Investigators are responsible for ensuring that employees under their control receive this training.
3. Research Service personnel will receive initial fire, safety, and safety training upon initial employment in the individual research laboratory. Additional training in the following areas will be provided during HRMS Mandatory Training held in the Auditorium:
a. Fire Safety
b. Infection Control
c. Hazardous Materials and Wastes
d. Others
e. Safety Procedures
4. Mode of training
a. In-service will be conducted as soon as possible after initiation of employment and no later than one month after beginning employment.
b. Lab meetings held by individual Principal Investigators can be held at any time.
c. Handout materials, audio visual aids and computerized formats are encouraged when holding training sessions.
d. Medical Center, Environment of Care and Disaster Preparedness Manuals are excellent training sources.
e. Special sessions arranged by the Research Service and conducted by the Industrial Hygienist and/or the Safety Specialist may be arranged by appointment.
f. Topics presented in the HRMS Mandatory Training noted above may be available on VA computers for authorized personnel.
N. DISPOSAL OF HAZARDOUS WASTES
NOTE: Chemical users should consult SDS for manufacturer's recommended disposal methods. All methods must be in conformance with the procedures outlined in Chapter 6 of the Hazardous Materials Management Manual issued by NF/SGVHS Memorandum No. 8, “Hazardous Materials Management Program." Briefly, some (but not all) procedures for disposing of certain wastes generated in research laboratories include:
Research Services: Laboratory Safety Manual Page 62

1. Liquid Wastes
a. Some liquids may be flushed into the sewer system with copious amounts of water provided chemical volume is minimal as noted in the aforementioned manual.
b. Disposal of chemicals through the sewer system must comply with all Federal, state and local regulations and ordinances and Chapter 6 of the reference noted above.
c. The Industrial Hygienist may be consulted when in doubt as to whether a chemical can be disposed of via the sewer system. The Industrial Hygienist can be contacted at Ext. 4309/6534/6025.
2. Liquid Hazardous Wastes
NOTE: Chapter 1 of the Hazardous Materials Manual describes what wastes are hazardous, as regulated by the US Environmental Protection Agency. Hazardous chemical wastes will be disposed of as noted in Chapter 6 of the aforementioned manual.
3. Biomedical Wastes
a. Biomedical wastes will be disposed in accordance with the procedures described in NFSGVHS Memorandum No. 138-4, "Biomedical Waste Management".
b. Sharps will be placed in impervious containers for disposal. The acquisition of sharps containers is the responsibility of each individual investigator. Other materials capable of tearing trash bags or cutting personnel who must handle them such as broken glass and pipettes (both plastic and metal composition), glass sheets, etc.) must be placed in a container that will not rupture during transport to the incinerator. A suitable method of containing such wastes is to use either a commercially available cardboard box especially designed to hold such items (available from laboratory supply companies) or a sturdy cardboard box that has the proper configuration.
4. Batteries of all kinds (i.e., alkaline, carbon-zinc, lead-acid, nickel-cadmium, etc.) will be collected in plastic boxes furnished by Environmental Management (137) that may be obtained by calling ext. 6531, or pager 1362. These items will be disposed in a method that protects human health and the environment. The facility Industrial Hygienist should be contacted for information on how to dispose of other types of batteries.
Research Services: Laboratory Safety Manual Page 63
V. GENERAL PROCEDURES FOR WORKING WITH CHEMICALS AND HAZARDOUS AGENTSThe basic rules and regulations for working with chemicals and hazardous agents are applicable to all sections of the service and are listed for quick reference by employees.
A. GENERAL REQUIREMENTS 1. Smoking is prohibited in all medical center interior locations and is only
permitted in designated external smoking areas in accordance with Medical Center Memorandum No. 138-1, "Smoking Policy".
2. Food and beverages are not permitted in the technical work areas of research laboratories.
3. It is advised that Research Service personnel wear splash goggles when handling specimens and substances likely to cause eye irritation if accidentally splashed.
4. Hands must be washed before leaving the laboratory technical areas.5. Mouth pipetting is prohibited.6. Use of a fume hood, face shields or eye goggles must be used for protection
when handling caustic or corrosive materials.7. Hair shall be secured back and off the shoulders to prevent contact with
hazardous chemicals and contaminated materials.8. Any behavior that might confuse, startle or distract other laboratory personnel
must be avoided.9. Work areas must be kept clean and uncluttered.
10. Chemicals and equipment must be properly labeled and stored so that contents are legible.11. Work areas must be cleaned on the completion of each task or at least at the
end of each day.12. All broken or chipped glassware must be discarded in proper impervious
receptacles. Large pieces of broken glass should be removed with brooms and disposed of in the proper receptacle. Small pieces can be removed with tongs or forceps. Glass should never be removed with fingers. Receptacles must be puncture proof.
13. Consult MSDS when performing new procedures with unfamiliar chemicals for appropriate personal protective procedures.
14. Assure that all hazardous chemicals used in laboratory procedures have an MSDS on file in the appropriate binder.
15. Cover all specimens to be centrifuged.16. Needles and other sharp objects should be disposed of promptly and in
impervious containers. Needles should not be clipped or recapped by hand.17. Care should be taken not to create aerosols of biological fluids.18. Occupants must wear closed toe shoes and long pants or a lab coat sufficient
to cover exposed skin at all times while in the research laboratory. This
Research Services: Laboratory Safety Manual Page 64

requirement applies to all visitors. Open toed shoes are prohibited in the laboratory.
B. SPECIAL LABORATORY PROCEDURES
1. General Requirements for Compressed Gases
a. Cylinders must be secured at all times so they cannot fall.
b. Valve safety covers should be left on until pressure regulators are attached.
c. Containers must be labeled clearly with the contents and hazards of the gas.
d. Hand trucks or dollies with a securing device installed must be used when moving cylinders.
e. The use of oil, grease or lubricants on valves is prohibited.
f. Do not attempt to repair or force damaged or frozen cylinder valves.
g. No more than two cylinders should be manifolded together. Several instruments or outlets are allowed for a single cylinder.
h. When more than one cylinder of a highly flammable gas is to be used in one room, specific approval of the Medical Center Safety Specialist should be obtained beforehand.
i. Valves on all flammable gases cylinders shall be shut off when the unit is unattended.
2. Radioactive Substances
Procedures for using these substances are outlined in the "Radiation Control Guide Policies and Procedures" manual authored by the Radiation Safety Officer.
3. Caustic Materials
a. If quantities of acids or alkalies greater than 500ml are being used, a shield or barrier of some sort should be used so that breaks and spills can be controlled.
b. Lab coats/aprons, gloves and eye protection must be worn when handling highly corrosive materials as recommended on the MSDSs.
c. Mouth pipetting is prohibited.
d. Reagents must not be identified by sniffing contents.
e. Dilution: Add reagents slowly. Always add acid to water. Allow acid to run down the side of the container and mix slowly by gentle rotation. Avoid overheating.
f. Acids and bases must be transferred using bottle carriers.
4. Formaldehyde
Formaldehyde will be acquired, handled, used and disposed of in accordance with NF/SGVHS Memorandum No. 138-22, "Formaldehyde Management Policy."
Research Services: Laboratory Safety Manual Page 65

5. Xylene
a. Exposure to xylene must not exceed 100 ppm calculated as an 8 hour time weighted average (TWA).
b. Exposure must not exceed 150 ppm per 15 minute short term exposure limit (STEL).
c. Employees at risk of exposure will be monitored by the Industrial Hygienist during baseline surveys of Research Service laboratories or as part of a special request.
d. After review of results by the Industrial Hygienist consultation will be held with the Chief of Research Service and corrective action taken to reduce exposure concentrations to below the TWA and/or STEL should these levels be exceeded.
e. In the event of over exposure, the affected employees will be notified in writing within 15 days.
6. Carcinogens
Use of carcinogens as defined by OSHA in 29 CFR 1910.1200 (c) and Chapter 4 of the Hazardous Materials Management Manual will be conducted in accordance with the Manual, which requires the following:
a. Designation of specific work areas with restricted access.
b. Listing of personnel authorized to work in the area.
c. Inventory of types and quantities of such substances on hand.
d. Special training for affected personnel on safe handling procedures for the carcinogen chemical.
e. Maintenance of exposure monitoring records as defined by NF/SGVHS Memorandum No. 138-21, "Employee Access to Medical and Exposure Records."
7. Perchloric Acid
Consultation with the Industrial Hygienist is necessary before this substance is to be introduced into research laboratories.
8. Use and Exposure to Biological, Chemical and Physical Agents
a. Biological Agents -- Blood and Body Fluids
Use/Exposure: Contact with blood and body fluids may occur as a result of medical and surgical procedures, phlebotomy, specimen handling and test performance. (The chapter of the Infection Control Manual titled “Bloodborne Pathogens” articulates the program designed to prevent exposure to human blood and body fluids. It is found in the “References” section of the NF/SGVHS website.) For other biological agents, the following principles apply regarding the potential for harm:
Research Services: Laboratory Safety Manual Page 66

Health Effects:
1) Acute: the severity of the infection depends on:
i. the number of pathogens encountered;
ii. the worker's resistance which is affected by such things as: state of health, predisposing diseases, age, sex and hereditary factors;
iii. portal of entry (via inhalation, ingestion, mucous membrane of skin contact or direct inoculation); and the
iv. virulence of the organism.
2) Chronic: reproductive consequences ranging from congenital anomalies to death of the fetus and other chronic disease, such as cirrhosis of the liver and primary live cancer may result from some viruses including Hepatitis B, Rubella, Cytomegalovirus, Herpes and Human Immunodeficiency Virus (HIV).
b. Chemical Agents
1) Formaldehyde
Use/Exposure: Used as a fixative and is commonly found in research laboratories.
Health Effects:
i. Acute: Eye and respiratory irritation from the liquid and vapor forms. Severe abdominal pains, nausea, vomiting and possible loss of consciousness could occur, if ingested in large amounts.
ii. Chronic: High concentration of vapor inhaled for long periods can cause laryngitis, bronchitis or bronchial pneumonia. Prolonged exposure may cause conjunctivitis. Nasal tumors have been reported in animals. Suspect carcinogen.
2) Toluene/Xylene
Use/Exposure: Solvents used to fix tissue specimens and rinse stains. They are primarily found in histology, hematology, microbiology and cytology applications.
i. Acute: Eye and mucous membrane irritation from vapor and liquid forms. Dizziness, headache and mental confusion from the inhalation of vapor. Ingestion or absorption through the skin can cause poisoning. There is a potential for thermal burns as toluene/xylene are extremely flammable.
ii. Chronic: If the xylene or toluene contains benzene as an impurity, repeated breathing of the vapor over long periods may cause
Research Services: Laboratory Safety Manual Page 67

leukemia. Prolonged skin contact may cause dermatitis. Toluene has been implicated in reproductive disorders.
3) Acrylamide
Use/Exposure: The resin is used to make gels for biochemical separations.
i. Acute: Eye and skin irritation.
ii. Chronic: Central nervous system disorders, i.e., polyneuropathy. Suspected carcinogen. Mutagen.
c. Physical Agents
1) Ionizing Radiation
Use/Exposure: Kits containing radioactive isotopes or specimens and excreta of humans and animals who have received radionuclides may pose a hazard. Exposure may result from the handling of radioactive spills.
NOTE: Effects of radiation exposure are somatic (body) and/or genetic in nature.
i. Acute: Erythema and dermatitis. Large whole body exposures cause nausea, vomiting, diarrhea, weakness and death.
ii. Chronic: Skin cancer and bone marrow suppression. Genetic defects may lead to congenital defects in the employee's offspring.
2) Electrical Hazards
Use/Exposure: Exposure may occur when there is lack of maintenance to any electrical equipment, abuse and lack of understanding of the equipment and/or its controls. Oxygen enriched atmospheres and water may contribute to hazardous conditions.
i. Acute: Painful shocks, respiratory inhibition, deep burns (electrical and thermal), heart rate irregularities, death.
ii. Chronic: No documented effects.
3) Ultraviolet Radiation
Use/Exposure: Ultraviolet lamps are sometimes used in a biosafety cabinet.
i. Acute: Skin burns, damage to the eye (photokeratitis or conjunctivitis).
ii. Chronic: No documented effects other than cataracts.
Research Services: Laboratory Safety Manual Page 68

4) Compressed GasesUse/Exposure: Compressed gases are used in many clinical laboratories. They are found in varying sizes and in pure or mixed states. Examples: ammonia, carbon dioxide and nitrogen.
NOTE: Compressed gases can be toxic, radioactive, flammable and explosive. These effects arise from the compression of the gas and the health effects of the chemical itself.
5) Glass
Use/Exposure: Glassware is used as bottles, beakers, flasks, test tubes, pipettes and tubing. Chipped, cracked, badly etched glassware and sharp edges present hazards as well as broken glass.
NOTE: Cuts, scratches, abrasions are potential locations for infection.
Research Services: Laboratory Safety Manual Page 69

VI. SAFETY RECOMMENDATIONSThe following practices have been added to this chemical hygiene plan as a prevention of physical injury which can have the secondary effect of toxic exposure or injury.
A. ELECTRICAL SAFETY
1. GroundingAll laboratory instrumentation must be grounded and initially checked by Engineering personnel in accordance with Engineering SOP No. 5, “Equipment Management Program and New Equipment Testing”. If the equipment is intended for use on human subjects, Biomedical Engineering Technicians will need to perform safety tests and properly certify that the devices are safe for this purpose. The use of personally owned electrical devices in the medical center is governed by the procedures contained in NF/SGVHS Memorandum No. 90-10, “Personally Owned Property Placed In Official Use”.
2. ShocksAll shocks of any magnitude must be reported immediately to the Biomedical Engineering Technician for Research.
3. Corrective Action in Case of Shock
Shut off the current and/or unplug the instrument. Do not use the instrument that is causing shock. Report the incident immediately to the Safety Officer and Biomedical Engineering.
4. Repairsa. Repairs on the electrical system are not to be performed by laboratory
personnel. The Biomedical Engineering Technician must be consulted at ext. 6501 for assistance.
b. Any work performed on switches, outlets, circuit boxes or equipment must be referred to the Biomedical Engineering Technician for Research at ext. 6501 or Facilities Management Service at extension 6025.
5. Extension Cord Usage
a. Multiple outlet plugs are prohibited from use on all equipment.
b. When permitted, extension cords, power strips and UPS equipment must be UL approved, and in original condition. They can only be used in a manner so as not to create other hazards or be subject to damage (i.e., trip hazards, exposed to flammable atmospheres, run through doorways).
B. FIRE SAFETY
1. Be aware of ignition sources such as open flames, heating elements, and spark gaps.
2. Do not use flammable liquids in the presence of ignition sources.
3. Flammable liquids give off vapors which may also ignite or explode. Be sure flammable liquids are properly stored in approved flame cabinets.
Research Services: Laboratory Safety Manual Page 70
a. Quantities of less than 2 gallons may be stored in well ventilated areas.
b. Quantities of greater than one pint should be stored in safety cans.
c. Bulks of five gallons or more should be stored in approved storage cabinet or approved storage rooms.
d. The bulk storage in a safety cabinet should be less than 60 gallons per 5,000 square feet of laboratory area.
e. DO NOT store any flammable liquid in areas exposed to direct sunlight or heat.
C. CONTROL OF FIRES
1. Evaluation
a. Evaluate the type and extent of the fire. Control measures should only be undertaken for small fires if it can be done so safely, such as, shutting off gas sources, closing doors, removing oxidizers, etc.
b. Evaluate the type of material burning (wood, flammable liquids, electrical or gases).
c. Follow the prescribed procedures:
Rescue - All individuals in the immediate area should be evacuated.
Alarm - Pull the alarm box nearest to you.
Confine - Close all doors and openings.
Evacuate/Extinguish - Leave the premises and wait for the fire department. Fire extinguishers may be used if desired. No one is under obligation to do so, however.
2. Solid Combustibles
a. Small objects may be handled with heat resistant gloves and extinguished with water or CO2.
b. CO2 or dry chemical extinguisher may be needed for larger fires.
3. Flammable Liquids
Dry chemical extinguishers are usually needed for safe and effective control of burning liquids.
4. Electrical Equipment
a. Only use extinguishers provided in the labs.
b. Shut down circuit if possible.
5. Gas
a. Shut off source if possible.
b. Extinguish flame with CO2 only after gas has been shut off.
c. Keep flames away from gas cylinders.
Research Services: Laboratory Safety Manual Page 71
6. Fire Safety Equipment
a. Sand or absorbent material is to be used to contain the spread of liquids that have not been ignited.
b. Fire extinguishers are of the dry chemical type.
c. The use of fire resistant lab coats is encouraged.
d. Heat resistant gloves may be used to move or handle small burning objects, to handle hot vessels and to turn off hot valves or handles.
VII. TECHNICAL GUIDANCE
Technical guidance on any part of this Chemical Hygiene Plan can be obtained from either the GEMS Coordinator, at Ext. 4309, the Industrial Hygienist (Ext. 4309/6534/6025), or the Safety Officer (Ext. 6560). These specialists maintain an extension library of technical publications, pertinent regulations, and federal laws that address safety, occupational health, waste management and fire protection issues. In addition, they are available for consultation in any aspect of these issues.
REFERENCESThe policies referenced in the text of this Chemical Hygiene Plan are available on the NF/SGVHS website, with exception of Engineering SOP No. 5, which is available from Engineering in Room EB87-1 at the Gainesville Division. Because they are subject to change at any time, a central repository for the NF/SGVHS memoranda may be maintained in the Research Service Office and are available for review during normal business hours. All employees are encouraged to become familiar with these documents as they outline policies that apply to Research Service Personnel. Other references include:
NF/SGVHS Environment of Care (EOC) Manual. NF/SGVHS Emergency Preparedness Plan. (Available on-line at the NFSGVHS
website)
Hazardous Materials Management Manual , issued by NF/SGVHS Memorandum No. 7.
Infection Control Manual. (Available on-line at the NF/SGVHS website)
National Research Council, Prudent Practices in the Laboratory Handling and Disposal of Chemicals, National Academy Press, 1995.
The three references listed below govern safety, occupational health and fire protection activities applicable to the Research Service setting. The first document has been issued in order to meet certain requirements imposed solely on federal agencies by Executive Order 12196 signed by the President in 1978. All three of these documents represent the Department’s official policies on various
Research Services: Laboratory Safety Manual Page 72

occupational safety and health matters (including program administration). Consequently, adherence with the procedures contained in these publications is considered to be mandatory.
VA Directive 7700, “Occupational Safety and Health”, February 11, 2009.
VA Directive 7701.1, “Occupational Safety and Health Procedures”, August 24, 2010.
Information Letter IL 142-91-002. "OSHA... Final Rule for Occupational Exposures to Hazardous Chemicals in Laboratories (29CFR, Part 1910)," January 28, 1991.
The following federal regulations govern many of the activities contained in this plan. There are many other regulations that specifically address activities or practices that may be conducted in biomedical research laboratories. They may be consulted in the offices of the safety and health technical contacts listed above, or they may be accessed at no charge at www.osha.gov.
29CFR, Part 1910 et. seq.
29CFR, Part 1910.1450
29CFR, Part 1960 et. seq.
40CFR, Part 260 et. seq.
OSHA WEB SITE
NOTE: To access the latest standards of the U.S. Department of Labor, Occupational Safety and Health Administration (OSHA), go to www.OSHA.gov and click on “Regulations”.
The OSHA standards are also available in the Industrial Hygeinist’s office (Bruce Carlberg, Room EB100-1, Ext. 4309).
Research Services: Laboratory Safety Manual Page 73

APPENDIX A. HAZARDOUS MATERIALS DATA: INFORMATION AND RECOMMENDED FORM
Information on the Chemical Inventory Form
From: NF/SGVHS Safety Officer, Tuesday, October 25, 2011
Potential Hazards: Under “Potential Hazards”, does the hazardous material represent a potential hazard to employees under normal conditions or use or case of an uncontrolled release (i.e., a spill)? For example, Inh = Inhalation; Abs = Absorption; Ing = Ingestion as used in the workplace or if spilled on the floor.
Disposal Method (Application, In Process, RCRA Waste, etc.) : For all listed hazardous materials
For example, Disposal Method for all listed hazardous materials is: Application. This means that the materials are applied to either the skin or to a surface.
The purpose of this column is to list how the chemical is disposed. In Application case, all of these chemicals are applied to some kind of surface, and there’s no liquid waste being generated. Other methods of disposal appropriate for this column, in addition to Application, are:
In Process = The substance is either chemically altered to yield either an entirely new chemical or co-mingled with another substance to a form mixture that must be further evaluated as to whether it is an EPA-regulated hazardous waste that requires special disposal. Many substances become chemically changed (acids, for example, when they are neutralized) or co-mingled (various solvents or water that have impurities in them as the result of undergoing some process).
RCRA Waste = A waste that is indeed an EPA-regulated hazardous waste (RCRA stands for Resource Conservation and Recovery Act of 1976, the law that governs the identification, management, and disposal of such wastes) such as alcohols that are used in tissue fixation that are still flammable when ready for discarding. Collodion and ethyl acetate are sometimes used in instances where electrodes are applied to the body, and these highly flammable substances may yield a RCRA waste if there are any liquid residues, soaked towels, or rags.
Sanitary Sewer = The waste does not the meet the definition of an EPA-regulated hazardous waste, is soluble in water, and contains no ingredients that will interfere with wastewater treatment plant operations.
Solid Waste = A catch-all term for a material that is suitable for discarding in the garbage similar to ordinary trash, like certain gels that have solidified and contain no flammable constituents or toxic components
Some materials used are very benign and do not fall into the latter four (4) categories.
Research Services: Laboratory Safety Manual Page 74
NSN or MIL/FED:
Ignore the column titled NSN or MIL/FED Spec as this refers to items that are stocked in our warehouse that have a National Stock Number associated with them or are purchased according to a Military or Federal Specification. Hazardous materials such as these are purchased directly from GSA and have a 7-digit federal stick number listed on them (as XXXX-XX-XXX-XXXX). These are rarely found in research laboratory applications. Mil Specs are rarely found outside military procurement operations but are included here as historically there have been some products brought into the hospital for building construction applications.
This whole scheme is called waste characterization and is required by EPA. More than you wanted to know.
Contact:
Bruce CarlbergIndustrial Hygienist & GEMS CoordinatorNorth Florida/South Georgia Veterans Health SystemGainesville Division1601 SW Archer Rd.Gainesville, Florida 32608-1135TEL: 352-376-1611, Ext. 4309/6534/6025FAX: 352-374-6028
NOTE: Hazardous Materials Data Form (Chemical Inventory)The NF/SGVHS Committee on Research Safety has approved the plan that no later than September 30, 2013, all Research laboratories’ Chemical Inventories will be transferred to the to the Web based (SDS)/Chemical Inventory Service, run by the VHA Center for Engineering and Occupational Safety and Health (CEOSH) (Web site: http://vaww.ceosh.med.va.gov/ceosh/MSDS.shtml ).
To transfer your Chemical Inventory into the SDS system: Contact Marie Johnson ([email protected], 352-548-6476), provide the
name and VA email addresses of the PI and staff member(s) you have assigned to input the information.
The PI and designated staff member will be sent passwords to access the System.
Input all you laboratory chemical information into the System. Send an email to Marie Johnson ([email protected] ) confirming that
your Inventory has been put into the SDS System. Training on the SDS System will be provided in 2013 on the System.
Research Services: Laboratory Safety Manual Page 75
HAZARDOUS MATERIALS DATA FORMWorkplace Identifier
573-Facility
NF/SG VHS MCWorkplace PI Name Service
ResearchBldg. No./Location
Main - GainesvilleRoom/Area Date
MATERIAL NOMENCLATURE MANUFACTURER
NSN or MIL/FED
Spec
MSDS ON FILE
(Y or N)
QUANTITY USED
(per day, wk, mo, yr)
DISPOSAL METHOD (Application, In Process,
RCRA Waste, etc.)
POTENTIAL HAZARD (Y or N)
Inh Abs Ing Contact (Eye/Skin)
Research Services: Laboratory Safety Manual Page 76
Workplace Identifier
573-Facility
NF/SG VHS MCWorkplace PI Name Service
ResearchBldg. No./Location
Main - GainesvilleRoom/Area Date
MATERIAL NOMENCLATURE MANUFACTURER
NSN or MIL/FED
Spec
MSDS ON FILE
(Y or N)
QUANTITY USED
(per day, wk, mo, yr)
DISPOSAL METHOD (Application, In Process,
RCRA Waste, etc.)
POTENTIAL HAZARD (Y or N)
Inh Abs Ing Contact (Eye/Skin)
Research Services: Laboratory Safety Manual Page 77

SECTION. IV. ANIMAL SAFETY PROCEDURES
ANIMAL FACILITY SAFETY
Animals in Research
Veterinary Medical Unit (VMU):......................................................................Building II
Animal Caretaker:................................................................Mike Riley, Tele: 273-9242
Veterinary Medical Officer (VMO):.....................Dr. Karl Andrutis, DVM, 352-392-2978
VMO Designee:............................................Dr. Harvey Ramirez, DVM, 352-392-4481
IACUC Chairperson:.................................................Prodip Bose, MD, PhD, Ext. 5996
IACUC Coordinator:...................................................... Chris Johnston, 352-548-6481
Only persons listed on the Institutional Animal Care and Use Committee (IACUC) approved Animal Component of Research Protocol (ACORP) may enter the VMU unaccompanied. All persons working in the animal facility must have a current VA or WOC appointment to enter the facility. All other persons are considered visitors and must either report to the VMU Supervisor (i.e., vendors, contractors, etc.) or must get prior approval by completing a Visitor Request Form. The VMU Visitor Policy and Request Form can be found on the Research Service webpage (http://www.northflorida.va.gov/northflorida/research/VMU.asp).
Animal Biohazards
Animal studies present many different kinds of physical, environmental and biological hazards. These hazards may be unique according to the species involved and the nature of the research. Attention must be focused on the animal facility’s potential for increased exposure to both human pathogens and to zoonotic agents. The animals themselves can introduce new biological hazards to the facility. Special consideration must be given to field-captured animals or animals coming from unscreened herds, where latent infections are most common. Animals that shed virus through respiratory dissemination or dissemination in urine or feces are far more hazardous than those that do not. Animal handlers in research facilities working on infectious agents have a greater risk of exposure from the animals’ aerosols, bites, and scratches.
Research Services: Laboratory Safety Manual Page 79

CARE OF ANIMALS DURING EMERGENCIES
In case of emergency, that may include, but is not limited to, equipment failures, personnel absences, space shortages, and other disasters, the “Emergency Section” of the Memorandum of Understanding regarding the Care and Use of Animal Subjects between the University of Florida and the Malcom Randall VA Medical Center (Nov. 23. 2009) will be followed. The MOU is intended to help facilitate the resolution of such emergencies rather than to be restrictive. Responsible parties are the Supervisors, Managers, Directors and veterinary staffs of the institutional animal facilities at the VA and UF.
Research Services: Laboratory Safety Manual Page 80
ANIMAL BIOSAFETY LEVELS
This section describes the practices and facilities applicable to work on animals infected with agents assigned to corresponding Biosafety Levels 1-2. This facility does not accommodate Biosafety Level 3 or higher. Animal Biosafety Levels (ABSL) 1-2, provide increasing levels of protection to personnel and to the environment, and specify minimal standards for activities involving infected laboratory animals. Investigators inexperienced in conducting these types of experiments must seek help in designing their experiments from individuals who are experienced in this special work.
A. Animal Biosafety Level 1 (ABSL-1)All animals housed in the VMU are designated at a minimum of ABSL-1. ABSL-1 is suitable for work involving well characterized agents that are not known to cause disease in healthy adult humans, and that are of minimal potential hazard to laboratory personnel and the environment.
1. Standard Practices a. The VMU Supervisor along with the VMO, the IACUC and SRS establishes
policies, procedures, and Standard Operating Procedures (SOPs) for emergency situations.
b. Each project is subject to approval by the Institutional Animal Care and Use Committee (IACUC) and the Subcommittee on Research Safety and the R&D Committee. Any special practices are approved at this time.
c. Except for authorized VA/ACS staff, only persons listed on the Institutional Animal Care and Use Committee (IACUC) approved Animal Component of Research Protocol (ACORP) may enter the VMU unaccompanied. Refer to the VMU Visitor Policy posted on Research Service webpage for more details. Before entering, persons are advised of the potential biohazards and are instructed on the appropriate safeguards.
d. An appropriate medical surveillance program is in place.e. A Research Laboratory Safety Manual is prepared. SOPs are in place to
cover pertinent information. Personnel are advised of special hazards, and are required to read and follow instructions on practices and procedures.
f. Eating, drinking, smoking, handling contact lenses, applying cosmetics, and storing food for human use must only be done in designated areas and are not permitted in animal or procedure rooms.
g. All procedures are carefully performed to minimize the creation of aerosols or splatters.
h. Work surfaces are decontaminated after use or after any spill of viable materials.
i. All wastes from the animal room (including animal tissues, carcasses, and contaminated bedding) are transported from the animal room in leak-proof, covered containers for appropriate disposal in compliance with applicable institutional or local requirements. Incineration is recommended.
j. Policies for the safe handling of sharps are instituted.k. Personnel will wash their hands after handling cultures, animals, after
removing gloves, and before leaving the animal facility.l. A biohazard sign must be posted on the entrance to the animal room
Research Services: Laboratory Safety Manual Page 81

whenever infectious agents are present. The hazard warning sign identifies the infectious agent(s) in use, lists the name and telephone number of the responsible person(s), and indicates the special requirements for entering the animal room (e.g., the need for immunizations and respirators).
m. An insect and rodent control program is in effect.
2. Special Practices: None.
3. Safety Equipment (Primary Barriers): a. The wearing of laboratory coats, gowns, and/or uniforms in the facility is
required. b. Gowns and uniforms are not worn outside the facility.
4. Facilities (Secondary Barriers): a. The animal facility is separated from areas that are open to unrestricted
personnel traffic within the building.b. External facility doors are self-closing and self-locking.c. Doors to animal rooms open inward, are self-closing, and are kept closed
when experimental animals are present.d. The animal facility is designed, constructed, and maintained to facilitate
cleaning and housekeeping. The interior surfaces (walls, floors, and ceilings) are water-resistant.
e. Internal facility features such as light fixtures, air ducts, and utility pipes, are arranged to minimize horizontal surface areas.
f. If floor drains are provided, the traps are always filled with water and/or an appropriate disinfectant.
g. Ventilation must be provided in accordance with the Guide for Care and Use of Laboratory Animals, latest edition.
h. No recirculation of exhaust air must occur. Depending on type of housing (conventional housing, SPF animals or BSL2 housing), It may be recommended that animal rooms maintain negative pressure compared to adjoining hallways.
i. Each animal room and procedure area has a hand washing sink.j. Cages are washed in a cage washer. The mechanical cage washer has a
final rinse temperature of at least 180°F.k. Illumination is adequate for all activities, avoiding reflections and glare that
could impede vision. Foot candles are measured annually and maintained according to the Guide for the Care and Use of Laboratory Animals.
B. Animal Biosafety Level 2 (ABSL-2)Animal Biosafety Level 2 involves practices for work with those agents associated with human disease. It addresses hazards from ingestion as well as from percutaneous and mucous membrane exposure. ABSL-2 builds upon the practices, procedures, containment equipment, and facility requirements of ABSL-1.
1. Standard Practices Aside from the standard policies, procedures, and protocols for emergency situations established by the VMO and the VMU Supervisor, appropriate special
Research Services: Laboratory Safety Manual Page 82

policies and procedures must be developed as needed and approved by the Institutional Animal Care and Use Committee (IACUC) and the Subcommittee on Research Safety.a. Access to the animal room is limited to the fewest number of individuals
possible. Personnel who must enter the room for program or service purposes when work is in progress are advised of the potential hazard.
b. An appropriate medical surveillance program is in place.c. All personnel receive appropriate immunizations or tests for the agents
handled or potentially present (e.g., hepatitis B vaccine, TB skin testing). When appropriate, a serum surveillance system must be implemented.
d. Personnel are advised of special hazards, and are required to read and follow instructions on practices and procedures.
e. Eating, drinking, smoking, handling contact lenses, applying cosmetics, and storing food for human use must only be done in designated areas and are not permitted in animal or procedure rooms.
f. All procedures are carefully performed to minimize the creation of aerosols or splatters.
g. Equipment and work surfaces in the room are routinely decontaminated with an effective disinfectant (Chlorine Dioxide) after work with the infectious agent, and especially after overt spills, splashes, or other contamination by infectious materials. Refer to the VMU SOP on Bio-Safety Level 2 for detailed information.
h. All infectious samples are collected, labeled, transported, and processed in a manner that contains and prevents transmission of the agent(s). All wastes from the animal room (including animal tissues, carcasses, contaminated bedding, unused feed, sharps, and other refuse) are transported from the animal room in securely closed containers for appropriate disposal in compliance with applicable institutional or local requirements. The outer surface of the containers is disinfected prior to moving the material. Autoclaving of the contents prior to incineration is recommended.
i. Policies for the safe handling of sharps are institutedj. Needles and syringes or other sharp instruments are restricted for use in the
animal facility only when there is no alternative, such as for parenteral injection, blood collection, or aspiration of fluids from laboratory animals and diaphragm bottles.
k. Syringes that re-sheathe the needle, needle-less systems, and other safe devices must be used when appropriate.
l. Plastic ware must be substituted for glassware whenever possible.m. Personnel must wash their hands after handling cultures and animals, after
removing gloves, and before leaving the animal facility.n. A biohazard sign must be posted on the entrance to the animal room
whenever infectious agents are present. The hazard warning sign identifies the infectious agent(s) in use, lists the name and telephone number of the responsible person(s), and indicates the special requirements (e.g., the need for immunizations and respirators) for entering the animal room.
o. An insect and rodent control program is in effect
Research Services: Laboratory Safety Manual Page 83
2. Special Practices a. Animal care laboratory and support personnel receive appropriate training on
the potential hazards associated with the work involved, the necessary precautions to prevent exposures, and the exposure evaluation procedures.
b. Personnel receive annual updates or additional training as necessary for procedural or policy changes.
c. Records of all training provided are maintained.d. In general, persons who may be at increased risk of acquiring infection, or for
whom infection might be unusually hazardous, are not allowed in the animal facility unless special procedures can eliminate the extra risk.
e. Only animals used for the experiment(s) are allowed in the room.f. All equipment must be appropriately decontaminated prior to removal from
the room.g. Spills and accidents which result in overt exposures to infectious materials
must be immediately reported to the VMU Supervisor. Medical evaluation, surveillance, and treatment are provided as appropriate and written records are maintained.
3. Safety Equipment (Primary Barriers) a. Gowns are worn over uniforms/scrubs. Laboratory coats are not worn while
in the animal room. Masks, head covers and shoe covers are also worn. Before leaving the animal room gowns shoe covers, masks and head covers are removed as one exits the animal room. Remove scrubs before leaving the animal facility.
b. Gloves are worn when handling infected animals and when skin contact with infectious materials is unavoidable.
c. Personal protective equipment is used based on risk assessment determinations.
d. Biological safety cabinets, other physical containment devices, and/or personal protective equipment (e.g., respirators, face shields) are used whenever conducting procedures with a high potential for creating aerosols. These include necropsy of infected animals, harvesting of tissues or fluids from infected animals or eggs, or intranasal inoculation of animals.
e. When needed, animals are housed in primary bio-safety containment equipment appropriate for the animal species. Filter top cages are always handled in properly designed and operating animal biocontainment cabinets recommended for rodents.
4. Facilities (Secondary Barriers) a. Access to the facility is limited by secure locked doors.b. External doors are self-closing and self-locking. Doors to animal rooms open
inward, are self-closing, and are kept closed when experimental animals are present
c. The animal facility is designed, constructed, and maintained to facilitate cleaning and housekeeping. The interior surfaces (walls, floors, and ceilings) are water-resistant.
d. Internal facility appurtenances, such as light fixtures, air ducts, and utility pipes, are arranged to minimize horizontal surface areas.
Research Services: Laboratory Safety Manual Page 84

e. If floor drains are provided, the traps are always filled with an appropriate disinfectant.
f. Exhaust air is discharged to the outside without being re-circulated to other rooms. Ventilation must be provided in accordance with criteria from Guide for Care and Use of Laboratory Animals, latest edition. Except for SPF rooms, the direction of airflow in the animal facility is inward; animal rooms must maintain negative pressure compared to adjoining hallways.
g. Cages are washed manually or in an appropriate cage washer. The mechanical cage washer must have a final rinse temperature of at least 180°F.
h. An autoclave is available in the animal facility to decontaminate infectious waste.
i. A hand washing sink is in the animal room where infected animals are housed, as well as elsewhere in the facility.
j. Illumination is adequate for all activities, avoiding reflections and glare that could impede vision.
C. Animal Biosafety Level 3 (ABSL-3)Animal Biosafety Level 3 involves practices suitable for work with animals infected with indigenous or exotic agents that present the potential of aerosol transmission and of causing serious or potentially lethal disease. BSL-3/ABSL-3 facilities are not available at the Malcom Randall VAMC.
D. Animal Biosafety Level 4 (ABSL-4)Animal Biosafety Level 4 involves practices suitable for addressing dangerous or exotic agents that pose high risk of life threatening disease, aerosol transmission, or related agents with unknown risk of transmission. ABSL-4 facilities are not available at the Malcom Randall VAMC nor are they available at any VA facility nationwide.
E. ZoonosisAnimal routes of transmission must be considered in the risk assessment of research projects. There are over a hundred disease-causing agents that may be transmitted between animals and humans (zoonosis). The method of transfer of these agents varies considerably and may include direct contact, handling contaminated inanimate objects (like cages and water bottles), or transmission by vectors, such as flies, ticks, lice, mosquitoes, and fleas.
A few of the more common and/or recently reported zoonotic diseases or infections include:1. DOGS: Staphylococcus, Streptococcus, Brucella, visceral larva migrans
(toxocara), creeping eruption (Ancylostoma), ringworm (Microsporum), sarcoptic mange, leptospirosis, and rabies.
2. CATS: Cat-scratch disease, toxoplasmosis, ringworm (Microsporum, trichophyton), staphylococcus, streptococcus, pasteurella, rabies.
3. RATS, MICE, HAMSTERS: Pasteurella, staphylococcus, streptococcus, pseudomonas, bordetella, ringworm, salmonella, yersinia, lymphocytic choriomeningitis (LCM).
Research Services: Laboratory Safety Manual Page 85

VMU PERSONNEL HEALTH ASSESSMENT
A. Initial AssessmentAll new Veterinary Medical Unit employees must undergo a medical assessment to determine fitness for work prior to employment. The pre-employment medical assessment will be performed by Employee Health Service and will include:1. Medical history (to include a record of allergies, immunizations,
immunosuppressive diseases or the use of immunosuppressive medications, and physical limitations).
2. Physical examination 3. Skin-testing for tuberculosis (not for BCG vaccinates within the last 10 years or
known positives).4. Chest x-ray if necessary.5. Rabies vaccination series (optional and if necessary). Facility currently does not
house any dogs or cats.6. Hepatitis B vaccination.7. Updated Tetanus vaccination.
Persons with the following medical conditions will not be considered suitable for employment in the Veterinary Medical Unit as they would be placing themselves in a potentially life-threatening condition: ASTHMA, ALLERGIES, IMMUNOCOMPROMISED.
B. Annual Health AssessmentAnnually thereafter, VMU employees will complete a health report questionnaire and forward it to the Employee Health Office where it will be kept on file.
On the basis of the completed questionnaire, the Employee Health Physician will determine if a physical examination is warranted.
In addition, the following are required annually: TB skin test, and updated vaccinations as needed.
Additional testing and/or vaccinations may be obtained as required.
C. Health Assessment of Non-VMU EmployeesNon-VMU employees who work with research animals must use the initial and annual health questionnaire programs described above for VMU employees.
Rabies vaccination is available for all Research Service personnel who handle animals as deemed necessary. Current work in the VMU does not pose a risk to rabies. A Tetanus booster is recommended every 10 years.
Women who work with animals in the laboratory MUST declare their pregnancy as early as possible, and are to be made aware of the potential risks in consultation with the Employee Health Physician and or the Medical Center Safety Officer.
Research Services: Laboratory Safety Manual Page 86
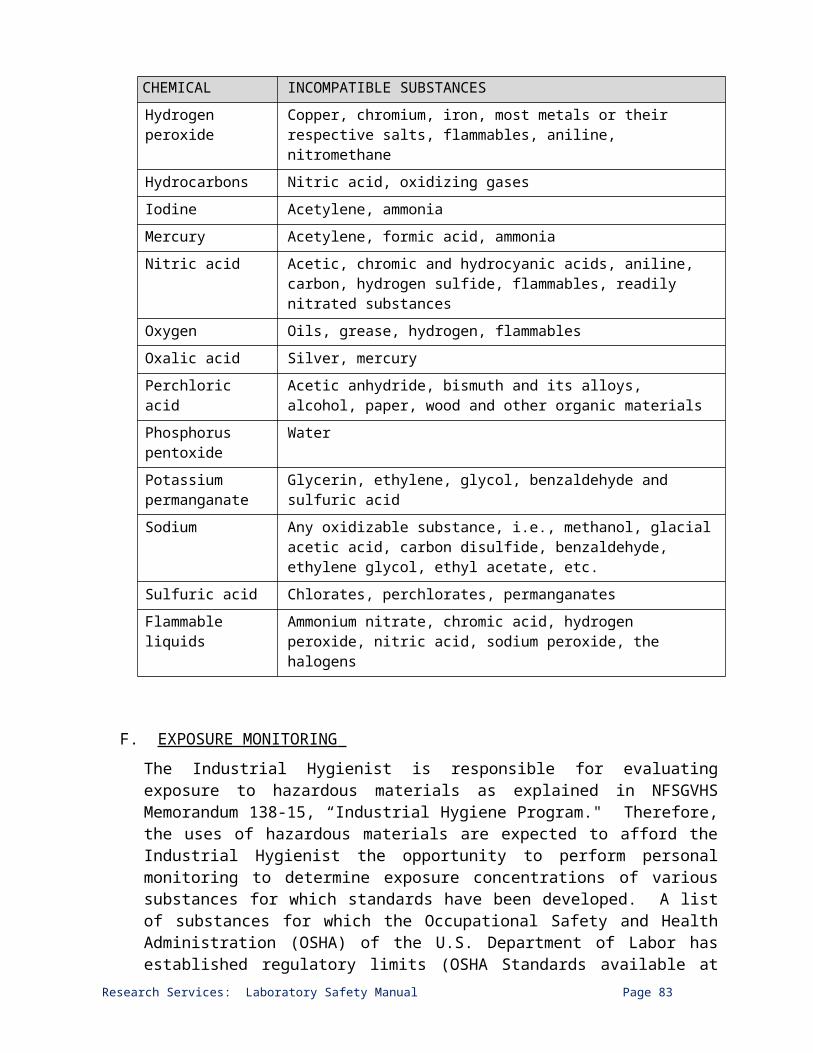
INJURIES CAUSED BY RESEARCH ANIMALS
A. Animal BitesImmediately after being bitten, thoroughly cleanse and irrigate the full depth of the wound with soap and running water. Allow at least 5 minutes contact of the soap solution with the wound.
Identify the biting animal and all animals associated with it. If possible, preserve the life of the biting animal for quarantining purposes. The animal shall not be destroyed until all questions as to the animal’s health can be addressed.
Report to the Employee Health Clinic for medical treatment (1st floor). If Employee Health Clinic is closed, employee will be evaluated by Emergency Room personnel.
All animal bites must be reported to the person’s immediate supervisor and to the VMU Supervisor.
Report injury and circumstances to your supervisor using "Report of Accident, Injury, Occupational Illness, or Fire," VA Form 2162.
B. Animal ScratchesScratches are not a mode of rabies transmission unless there is also contact with infected secretions.
Animals are not quarantined for inflicting scratches.
Such injuries are to be handled as indicated above under Animal Bites.
C. Animal Safety PracticesThe following practices may be applicable to use of research animals in the VMU and research labs.
1. PPE a. Protective clothing (lab coats, shoe covers) must be worn at all times when
working with animals in the VMU. These garments shall be removed prior to reentry to other sections of the building and upon leaving the animal facility.
b. Gloves must be worn when handling infected animals and/or infectious materials. Goggles, masks, and gowns must be worn if splattering of body fluids is likely.
2. Infection Control a. Work surfaces must be decontaminated after use or after any spill of viable
materials.b. Eating (includes chewing gum, sucking candy), drinking, smoking, and storing
food for human use is not permitted in the VMU animal rooms or research labs.
c. Personnel must wash their hands after handling animals and specimens.
Research Services: Laboratory Safety Manual Page 87

d. Bedding materials from animal cages are to be removed in such a manner as to minimize the creation of aerosols and disposed of in compliance with regulatory requirements.
e. If/when an infectious agent is in use in the VMU, the animal room may require special entry provisions (e.g. vaccination). A biohazard warning sign incorporating the universal biohazard symbol must be posted on the access door to the animal room. The hazard warning sign must:
f. Identify the infectious agent,g. List the name and telephone number of the animal facility supervisor or other
responsible person(s)h. Describe any special requirements for entering the animal room.i. Extraordinary care must be taken to avoid accidental wounds from sharp
instruments such as scalpel blades and needles. Needles must not be recapped or bent after use, but must be promptly placed into a puncture-resistant container used solely for such disposal.
j. Infectious waste is to be discarded into a "red" bagged container and autoclaved by VMU prior to disposal.
k. The steam autoclave in the VMU is tested with live bacterial spores (biological indicator) at least weekly.
l. Biological safety cabinets, other physical containment devices and/or personal protective devices (e.g. respirators, face shields) are to be used whenever procedures with a high potential for creating aerosols are conducted. These include:
m. Necropsy of infected animals. n. Harvesting infected tissues or fluids from animals or eggs.o. Intranasal inoculation of animals.p. Manipulations of high concentrations or larger volumes of infectious materials.
3. Animal Containment a. Doors to animal rooms in the VMU open inward, are self-closing, and kept
closed when experimental animals are present.b. Rodents are allowed to go to VA laboratories and then returned to the animal
facility. c. Animals going to UF labs may not be returned to the VMU after removal
except with the specific permission of the IACUC.
4. Animal Waste a. Carcasses and/or body parts must NEVER be disposed of in regular trash.
They are placed in red bags and stored in the common resource freezer Room D119-1. All animal carcasses and surgically excised tissues will be disposed of by VMU personnel via incineration.
b. Radioactive animals comprise a special category, and must be disposed of in consultation with Radiation Safety. Radioactive carcasses and tissues will be removed by vendors authorized to do so by the Radiation Safety Committee and the Medical Center's Radiation Safety Officer as indicated.
Research Services: Laboratory Safety Manual Page 88
TRAINING FOR ANIMAL USE AND CARE
All research personnel must complete all applicable training as outlined in the Institutional Animal Care and Use Committee Standard Operating Procedures. Training may be accessed at the www.citiprogram.org or AALAS Learning Library websites prior to working with research animals.
This training must be species-specific and a copy provided to the IACUC Coordinator.
Additional training can be provided by the VMO or the VMU Supervisor.
REFERENCES
Investigators using research animals are responsible for adhering to the contents of the following: PHS, NIH OPRR’s Policy on Humane Care and Use of Laboratory Animals. PHS, NIH Publication 86-23, "The Guide for the Care and Use of Laboratory
Animals." NRC, National Academy Press, Occupational Health and Safety in the Care and Use
of Research Animals. PHS, CDC Publication 93-8395, Biosafety in Microbiological and Biomedical
Laboratories. U.S. Department of Labor, Occupational Safety and Health Administration: Blood-
borne Pathogen Standard. AAALAC Accreditation Standards. VMU Standard Operating Procedures
CONTACTS
Please contact the VMU Supervisor/Representative: Sherry Scruggs (Tele: 273-8322) for additional information regarding the safe use of laboratory animals.
Research Services: Laboratory Safety Manual Page 89

Research Services: Laboratory Safety Manual Page 90

SECTION V. SECURITY PROCEDURES
RESEARCH LAB AND ANIMAL FACILITY SECURITY
A. The Research security system generates an alarm every time you have forgotten to swipe your key card and then try to swipe again. Please make every effort to correctly swipe your key card to enter lab doors. It will take a few seconds for the system to recognize your swipe and unlock the door. (SWIPE ONLY ONE TIME for each entry/exit or your access will be denied the next time .) DO NOT SWIPE UNAUTHORIZED DOORS you are not authorized to access. Call Wanda Thomas at Ext. 4204 to reset your Key Card.
B. The University ID badges that were distributed in 2006 will interfere with your electronic access so be sure to keep your electronic key separate from your University badge.
C. DO NOT hold any Research perimeter doors open. Proceed through the door quickly after swiping your access card. The door will be unlocked for 5 seconds. You have 30 seconds for the door to close before an alarm will sound in the Police Office. DO NOT HOLD DOORS OPEN.
D. Anyone who does not have an electronic swipe card is considered a visitor and must be signed in as a visitor in the Research Office. NO EXCEPTIONS. Visitors must be escorted at all times. VIOLATION OF THIS WILL RESULT IN LOSS OF PRIVILEGES TO ACCESS THE RESEARCH LABS.
E. Wear your VA ID Badge at all times. Your electronic access will be disabled if your WOC ID Badge has expired. See Wanda Thomas, Ext. 4204, at the Research Office to renew your badge.
F. If you are swiping your card after another person has just gone through, make sure to wait until the card reader light is red again before you swipe your electronic card.
G. Some office doors will be unlocked during normal working hours. At all other times the doors will be locked. Staff with permission to enter these offices will have to swipe their key cards to enter. These are the only areas where you can push the green button to exit.
Research Services: Laboratory Safety Manual Page 91
BIOHAZARDS MATERIAL TRANSPORTATION AND SHIPPING
A. Transportation of Infectious Materials:1. Transportation within BSL2 Laboratories:
a. All potential infectious materials are enclosed in durable, sealed containers (flasks, centrifuge tubes, freezer vials etc.) which are appropriate for the expected use.
b. When moving a flask from the incubator, the lid is closed tightly while the flask is still in the incubator and is then transported.
c. A cart is used whenever transporting more than one infectious item.d. A secondary container must be used to prevent any spills.
2. Transportation within VA Medical Center:a. This is done during a time when fewer people are present; i.e., before 8:00
AM or after 6:00 PM on weekdays, but preferably on the weekend.b. All potentially infectious materials are enclosed in durable sealed containers
(flasks, centrifuge tubes, freezer vials etc.) which are appropriate for the expected use. Before transferring, these containers are capped tightly and sprayed thoroughly with 70% ethanol. These containers are then placed in plastic biohazard bags, which are also sealed with rubber band.
c. These bags are placed in sturdy plastic (Rubbermaid) or cardboard or a Styrofoam box with appropriate padding (paper towels, absorbent paper, etc.) to minimize breakage.
d. The exterior of the box is clearly labeled “BIOHAZARD”.e. These boxes are placed on a cart for transportation within the VA Medical
Center.f. Only laboratory personnel specifically trained in handling pathogenic agents
are allowed to transport these materials. At least two laboratory personnel must accompany the transported material. Personnel must also take along spray bottles of 70% ethanol, 10% bleach (or appropriate disinfectant) absorbent paper, doubled bio-hazard bags, also appropriate personnel protective equipment for use in case of accident.
g. Service elevators are used for transportation between floors, a map may be drawn showing the expected route through the medical center.
B. Biohazardous Material Shipping:All VA-paid and WOC employees who are responsible for shipping (sending or receiving) biohazardous materials (blood, body fluids, infectious material, etc.) in VA laboratories must complete the VA Biohazard Shipping Training in CITI (hppt://www.citiprogram.org). The training is valid for 2 years. A copy of the training certificate must be immediately sent to the SRS Coordinator.
Research Services: Laboratory Safety Manual Page 92

RESEARCH VISITOR POLICY
A. All visitors must sign in on Research Service Visitors Logbook kept in the Research Service office and be escorted into and through the laboratory areas. Visitors are expected to follow all NF/SFVHS safety and security policies at all times. The VMU has its own separate visitor’s policy, to which its visitors must adhere.
B. A valid personnel identification containing a photograph of the individual must be provided prior to being admitted to laboratory areas.
C. Access to all approved visitors and students, is limited to regular working hours (7:30 AM to 4:00 PM), or when authorized employees are present Monday through Friday. Visitors are NOT allowed in the NF/SF VHS research laboratories during Weekends and Federal holidays.
D. Visitors must be accompanied at all times by an authorized VA employee when entering the laboratory area. This employee is responsible for serving as the visitor’s escort during their visit to the laboratory areas, activities and conduct, ensuring that the escorted visitor exits the area at the appropriate time.
E. Vendors must be restricted from all laboratory areas. If a PI or employee would like to meet with a vendor, s/he must schedule an appointment with the PI or employee in the Research Service Conference room (Contact Chris Johnston, 352-548-6481, or Helen Vaillancourt, Ext. 4971, to schedule the room). Contractors who need to render any kind of service in a laboratory must be cleared through VA Police Service with a background check; this must be completed prior to the vendor entering the Research areas. Once cleared and on the day the service will be rendered, the contactor(s) must first come to the Research Administration Office where they will sign the Contractors Log Book and receive and ID access card.
F. The contractor will render their service only during regular work hours: 7:30 AM to 4:00 PM, Monday through Friday. Before leaving Research areas, contractors must return to the Research Administration Office and return any ID and Access Cards and Sign-out.
Research Services: Laboratory Safety Manual Page 93

SOP FOR RESEARCH KEY CONTROL
A. Purpose: To establish policy, responsibility, and procedures for the request, issuance, and accountability of key cards for use in research areas.
B. Policy: Maximum security will be provided through appropriate control of issuance and accountability of key access to Research space
C. Procedure: Upon issuance of PIV Badge, individuals will be required to request key access to specific room(s) per initial written approval by their PI through the Key Control Coordinator. After verification of employee’s appointment, the Request for Key Access Form is approved by the ACOS or AO for Research. The Key Control Coordinator will forward the request to the Key Control Officer, assigned to Police Services as a Physical Security Specialist. The requestor is then assigned access through their PIV or Non-PIV Badge (electronic key cards are no longer used). Several key personnel may be assigned inclusive access to Research space by the Service Chief as needed; however, use of this level key access will be kept to the minimum. Research Service inclusive access will operate all door locks within the Research Service.1. Room access will be authorized on an as needed basis. Normally, the Director;
Associate Director; Chief of Staff; Chief, Facilities Management Service; Chief, Police Service, Associate Chief of Staff for Research (ACOS/R), Administrative Officer for Research (AO/R) and Deputy ACOS/Research will possess Research Service Master Keys.
2. Special area access will be issued for Service areas that require restricted access or special protection due to unusual vulnerability factors. All special access requires prior approval of the Core Director of that area, i.e., Veterinary Medical Unit Supervisor prior to the ACOS/Research or designee approval.
3. In emergency situations (ex: fire, chemical spill, leaks), a police officer shall provide access. The police officer will prepare a written report, through the ACOS/Research to the Associate Director, setting forth the circumstances requiring access (Memorandum No. 138-9).
4. In other than emergency situations (during duty hours), the Research Key Control Official may provide access in routine situations, e.g., locked PIV card in the office, left card home, etc.
5. Loss or Theft of Keys6. PIV users whose badges are lost or damaged must complete a Report of Survey
(Logistics) and a Police report (Police Service).All room access will be terminated immediately by the KeyControl Officer.The Research PIV Sponsor will receive notification from Police Service that the badge has been damaged or lost before an order for re-issuance can be completed. The Key Control Officer and Coordinator should also be notified.
Research Services: Laboratory Safety Manual Page 94

To protect your credentials/personal information, an application for replacement of PIV Badge and Room access should be submitted as soon as possible to the PIV Sponsor and the Key Control Coordinator.
7. Clearance from Duty All employees must personally turn in PIV Cards to Police Service when clearing station. The Key Control Officer should be notified to terminate room access upon clearing station. Staff outside of Research Service such as Housekeeping, Engineering, Police who signed for the key card from their Service Chief or designee must return those key cards to the perspective Service Chief or designee.
D. Responsibility:1. All individuals requiring a key card must initiate a Research Service Key Request
Form.2. Key Card Request Form must be signed by the PI or Service Chief, if not a
Research Service employee. The request must include individual room numbers of the authorized access areas.
3. The request will be forwarded to the ACOS/Research or his/her designee for approval.
4. Key access inventory will be conducted on an annual basis.5. Employees with Temporary, Term or other Time Limited Appointments will only
have access for the term of their appointment.6. If an employee is non-compliant with Research, e.g., Animal Studies or Human
Research Protection Program training, lapsed WOC renewal, etc., the ACOS/Research has the authority to cancel key accessaccess to Research Services space until compliance is met.
E. References: Research Service Key Request FormMemorandum No. 138-9, Change 4, dated September 6, 2012.
Research Services: Laboratory Safety Manual Page 95

SECTION VI. MEDICAL RESEARCH SUPPLEMENTAL DISASTER PLAN
A.GENERAL SUPPLEMENT
1. Definition of Functional Responsibilities
a. The Office of the Associate Chief of Staff for Research (ACOS/R) is designated to initiate and implement the Research Service supplemental disaster plan. The Chief of Staff (COS) Office notifies ACOS/R Office via the Research Service front desk, located off-site at the Commerce building, that the Medical Center Disaster Plan has been activated.
b. The employees of the Office of the Associate Chief of Staff for Research will assist the ACOS-R and Administrative Officer for Research (AO/R) in activating and carrying out the Research Service disaster plan.
2. Notification System
a. The ACOS/R and AO are notified in accordance with Attachment 1A, Chapter 1, Station Disaster Plan, and he/she in turn will notify the Deputy ACOS/R and AO/R to activate the supplemental plan.
b. Through the Office of the ACOS/R, all Research Service personnel located at the VA Hospital and Commerce Building, will be notified the Disaster Plan has been activated. In order to facilitate the notification of Research Service personnel the following will be maintained:
1) Emergency procedure instructions will be located in each laboratory area to supplement the notification procedures.
2) The ACOS/R Office will establish and maintain a current address and telephone number file on all Research Service employees.
3) The ACOS/R Office will establish and maintain a current emergency cascade calling list.
4. All employees, upon being notified of disaster plan activation, will report to their regularly assigned posts of duty and secure all laboratories and offices, taking care to shut off all non-essential electrical equipment and gas sources. Those employees regularly assigned to premises outside the VA will report to the AO/R Office.
5. Employees will then be notified of further assignments (e.g., to manpower pool in the auditorium, to aid in removing patients from the area, to secure office and laboratories, etc.).
Research Services: Laboratory Safety Manual Page 96

6. Assignment of Responsibility and Plan of Action
a. The ACOS/R and AO/R office staff will provide assistance, as needed, during activation of the disaster plan.
b. The ACOS/R and AO/R office staff will assist in the primary assessment of damages and casualties, and will make a written report to the ACOS/R and AO/R.
c. The ACOS/R and AO/R will be responsible for reporting to the COS and Medical Director’s Office, as requested.
B.SPECIFIC SUPPLEMENT1. Mass Casualty Plan
Research Office will implement Disaster Alerting Procedures as stated in Master Plan. As a supplement to phone notification, a runner will be used in all disasters. Research Service personnel in must report to the auditorium to serve in the manpower pool, etc.
2. Internal Disastera. Research Service Office will implement Disaster Alerting Procedures as
stated in the Master Plan.b. If necessary, Research Service Office will evacuate essential records. This is
the responsibility of the Administrative Specialist/Manager and Program Support Assistants as the alternates (IACUC, SRS, and HRPP coordinators, WOC coordinator).
3. Disaster Located Inside Research Service Areaa. Non-Radioactive Disaster
i. The employee must report the disaster by activating the nearest operating fire alarm.
ii. The reporting employee must request the assistance of a fellow employee to stay by the alarm system and direct emergency crew to the location of the disaster.
iii. The reporting employee must return to the disaster area and: if possible, carefully remove any injured employee in immediate
danger; fight the fire, if possible; and evacuate others in the adjacent area.
b. Radioactive Disaster i. The Research Service employee involved must contact VA radiation
Safety Officer Dr. Shailendra Shukla at Ext.6514/6069 and must notify the Chemical Hygiene Officer, Dr. Kamal Mohammed at Ext 7446.
ii. Confine the contamination to protect other personnel in the area.
Research Services: Laboratory Safety Manual Page 97
4. Disaster Located Outside Research Service Area
If the disaster is not in the Research Service area, all Medical Research employees will report to the auditorium for the manpower pool, etc.
5. Fire Disastera. When the fire alarm sounds, each Section Chief and/or Supervisor and/or
employee will be responsible to promptly horizontally evacuating the area, including shutting all doors. All personnel will meet by the main elevators of the floor on which they are and wait for first responders. Once the situation has been assessed by the first responders, research employees will be directed as to what actions they need to take.
b. If a fire originates in one of the research laboratories, remember: R: RESCUE A: ALARM C: CONFINE E: EVACUATE/EXTINGUISHAll personnel are expected to avoid exposing themselves to unnecessary risk to save material items.
6. Civil Disturbance Preparedness
a. Research Service Office will implement Disaster Alerting Procedures as stated in Master Plan.
b. All employees will report to the auditorium for assignment.
7. Hurricane Instructions
a. The Research Service Office will implement Disaster Alerting Procedures as stated in Master Plan.
b. When a hurricane/high winds WARNING is issued, all departments shall:1) Unplug all unnecessary electrical equipment and appliances.2) Store all equipment in safe areas away from windows.3) Assure that all equipment and supplies are removed from hallways.4) Assist where needed or as may become necessary.
c. All personnel must follow established procedures, as well as any instructions that may be issued.
d. All employees not considered essential for immediate operations or manning the manpower pool may be administratively excused by the Medical Center Director when an imminent storm warning is issued.
e. The manpower pool in the auditorium will be activated by the Assistant Personnel Officer when notified by the Command Center that winds have reached destructive force.
Research Services: Laboratory Safety Manual Page 98

8. Inspection of the Facilitya. All personnel MUST BE ALERT to unusual conditions during the storm. Be
alert for:1) Small leaks in the ceiling.2) Seepage of moisture in the ceiling or around windows3) Anything that seems abnormal.
b. Personnel must report these conditions immediately, as they are a strong indication that this is a danger area.
c. Personnel must move all patients from this area immediately.
9. Civil Defense Take Shelter Plan
a. Research Service Office will implement Disaster Alerting Procedures as stated in Master Plan.
b. The ACOS/R and AO/R will alert Research Service personnel of need for their area for shelter. Request they stop their ongoing work and require them to extinguish open flames and put away chemicals that could create a problem.
10. Bomb Threat Plan
a. Research Service Office will implement Disaster Alerting Procedures as stated in Master Plan.
b. The ACOS/R or AO/R will activate search teams to inspect Research Service areas. Lab personnel will be requested to examine their lab carefully for packages, etc.1) If a package container is found, personnel must contact the Bomb Alert
Command Post, ext. 6649. Do not move or disturb the package!2) If a package is not found, personnel must tape a piece of white paper on
their lab door indicating the area has been inspected, lock the door and evacuate the building.
11. Hazardous materials
a. Most laboratories contain chemicals and/or radioisotopes. Police, fire, and other emergency responders will be informed as to the types of biological, radioactive and chemical materials in use in each laboratory area. Additional notification information for emergency responders is referenced in the next bullet.
b. All laboratories must have posted at all times the Hazardous Chemical Inventory List. This list must be updated every six months and with the addition of any new chemicals. Updated copies must be submitted to the Facility’s Industrial Hygienist (Mr. Bruce Carlberg, Ext.4309).
Research Services: Laboratory Safety Manual Page 99

c. Radioactive signs must be posted on the doors where radioactive material is used and stored at all times.
d. Laboratory extinguishers are marked on walls and hallways.
e. Any major hazardous (chemical or biological) spill in the lab is to be contained by calling the Facility’s Industrial Hygienist and Research Chemical Hygiene Officer, shutting doors, and prohibiting entrance by unauthorized personnel.
f. MSDS must be on file in the laboratory.
12. Utility Failure-Electrical
a. Utilities affected:1) Electrical 8) Oxygen2) Emergency electrical 9) Gas3) Heat 10) Vacuum4) Water 11) Telephone5) Steam 12) Deionized water6) Air condition 13) Elevators7) Cold room and Freezer units
b. Proceduresa) Cascade notification system will be utilized so that the ACOS/R and
AO/RR/ACOS-R or Biological Safety Officer (or designee) are notified.b) Depending on the utility failure or scheduled outage, the Office of Research
Service or Laboratory Safety Officer (Dr. Shen-Ling Xia) notifies the individual laboratories affected by phone or by placing an appropriate notice on the door of each lab affected stating the type of failure and duration of failure or planned outage.
c) The affected laboratories then put their own backup plans into use (i.e., use other sources of deionized water, delay in ongoing experiments, place frozen material in other freezer or ultralow freezer, etc.). In the case of electrical failure, personnel in the building must monitor each laboratory for equipment failure and switch to emergency power if available.
13. HVAC Failure
In case of ventilation failure, personnel must stop any work being performed in a chemical fume hood or a biological cabinet. If personnel were exposed to any hazard due to the failure must report the incident to the Occupational Health immediately.
Research Services: Laboratory Safety Manual Page 100

SECTION VII. COMMON RESOURCE EQUIPMENT
COMMON RESOURCE EQUIPMENT PROCEDURES
A. Sign the log book if one is present.
B. Follow posted rules and, if necessary, read the instruction manual before using the equipment. For certain equipment items (e.g., confocal microscopy, fluorescence ration imaging), you must take a training class before using them.
C. Biohazardous or radioactive materials are approved for use in only certain pieces of equipment. Check before use. Clean up/decontaminate any waste you generate in the work area.
D. Equipment must be decontaminated per instructions after the use of any biohazardous material.
E. If your sample contains an isotope you must wipe test the equipment when finished. If counts are above background, decontaminate and do wipe tests until counts are at background level.
F. If you have any questions or are unsure about any aspect of common equipment contact the Laboratory Safety Officer (Dr. Shen-Ling Xia).
G. Notify Laboratory Safety Officer (Dr. Shen-Ling Xia) if you find any common resource equipment not in working order.
H. Emergency Safety Showers and Eyewash Stations.
ATTENTION: Emergency safety showers and eyewash stations are located in the following laboratories or Common Resource Rooms:
Basement Floor: D103-1 (To use call Ext. 7446 to make an appointment)
Basement Floor: D122-1 (Common Resource Room)
Third Flood: E354-1 (Common Resource Room)
Forth Floor: E459-1 (To use, call Ext. 6245 to make an appointment)
Fifth Floor: E585-2 (To use, call Ext. 6951 to make an appointment)
Handling and transfer of all corrosives should be performed in one of these locations.
See List of Common Resource Equipment below.
Research Services: Laboratory Safety Manual Page 101

LIST OF COMMON RESOURCE EQUIPMENT
NOTE: Do Not use any Common Equipment until you are properly trained in its use via the Contact Person. Sign the Log Book if there is one. Report all broken equipment to Dr. Shen-Ling Xia (Ext. 6581; [email protected]).
COMMON RESOURCE EQUIPMENT (RESEARCH)EQUIPMENT ROOM CONTACT PERSON, EXT.Animal Unit Bldg.11 Tony Mejia, 6495
Autoclaves (Steris 3021 Gravity Steam Sterilizer) D122-1Bert Herrera, 6797
Shen-Ling Xia, 6581
Autoclaves (Steris 3021 Gravity Steam Sterilizer) E364-1Bert Herrera, 6797
Shen-Ling Xia, 6581Break Room with microwave, refrigerator E594-1 Christopher Johnston, 6481
Centrifuges (Beckman L-90K) E354-1Bert Herrera, 6797
Shen-Ling Xia, 6581
Centrifuges (Beckman L-70K) D096-1Bert Herrera, 6797
Shen-Ling Xia, 6581
Centrifuges (Beckman Avanti J-E High Speed) E354-1Bert Herrera, 6797
Shen-Ling Xia, 6581
Centrifuges (Beckman Avanti J-E High Speed) D096-1Bert Herrera, 6797
Shen-Ling Xia, 6581
Centrifuges (Beckman Optima TLX 120,000 RPM) E354-1Bert Herrera, 6797
Shen-Ling Xia, 6581Centrifuge (IEC Centra MP4) E525-1 Elena Yarmola, 4305Clothes Washer/Dryer D113-1 Christopher Johnston, 6481
Cold Rooms with Freezer E463-1/E464-1Christopher Johnston, 6481
Shen-Ling Xia, 6581
Cold Rooms without FreezerBasement
EB81-1 Bert Herrera, 6797
Cold Rooms without Freezer E358-1Christopher Johnston, 6481
Shen-Ling Xia, 6581Cold Rooms without Freezer E569-1 Jeanette Lynch, 6914Conference/Break Room with microwave, refrigerator EB79-1 Christopher Johnston, 6481Conference Room E526-1 Christopher Johnston, 6481Confocal Microscopy -1P (Zeiss LSM 510 UV) D118A Shen-Ling Xia, 6581Confocal Microscopy -2P (Zeiss LSM 510 META) E313-1 Shen-Ling Xia, 6581Confocal Microscopy Imaging Workstation D119-1 Shen-Ling Xia, 6581
Autoclaves (2 units) D122-1 Bert Herrera, 6797
Autoclaves (2 units) E364-1 Bert Herrera, 6797
Research Services: Laboratory Safety Manual Page 102

COMMON RESOURCE EQUIPMENT (RESEARCH)EQUIPMENT ROOM CONTACT PERSON, EXT.Biological safety cabinet (for BSL II) E371-1 Kamal Mohammed, 7466Cryostat (Leica CM 1850) E525-1 Steve Borst, 5033Deionized & Distilled Water 18 MED OHM D122-1 Bert Herrera, 6797Deionized & Distilled Water 12 MED OHM E364-1 To be assignedFax Machine (352.374.6170) E584-1 Christopher Johnston, 6481Fax Machine (352.379.4145) E599-1 Christopher Johnston, 6481Film Developer (AGFA CP1000) D119-1 Bert Herrera, 6797
Flammable Storage Room E377-1Christopher Johnston, 6481
Shen-Ling Xia, 6581
Flammable Storage Room E470-1Christopher Johnston, 6481
Shen-Ling Xia, 6581Fluorescent Digital Microscopy (Nikon TE1200) E525-1 Shen-Ling Xia, 6581Fluorescent & X-Ray Image Station (Kodak 4000 MM) E525-1 Elena Yarmola, 4305Freezers, Ultralow -80C (6 units) EB81-1 Shen-Ling Xia, 6581Freezer, -20C, Flammable Material Storage (Thermo) E525-1 Shen-Ling Xia, 6581HPLC System (Prominence) E354-1 Shen-Ling Xia, 6581Ice Machine (Scotsman) D113-1 Bert Herrera, 6797Ice Machines E354-1 To be assignedIncubator, Low Temperature (Precision Scientific 815) E354-1 Shen-Ling Xia, 6581Isotope Counting (Beckman LS6500) D096-1 Bert Herrera, 6797
Isotope Counting (Beckman LS6500) E354-1Jeanette Lynch, 6914
Mary Handlogten, 4162Laser Microdissection (Zeiss PALM) E525-1 Shen-Ling Xia, 6581Liquid Nitrogen Tanks D113-1 Christine Conover, 6917
Micro-CT ex vivo (Bruker Skyscan 1172) E311-1 Joshua Yarrow, 6477Microinjection System (Eppendorf FemtoJet) E525-1 Shen-Ling Xia, 6581
MRI-rodent (7T, portable) E359-1 Perdip Bose, 5995Plate Reader (UV 160) E354-1 Steve Borst., 5033
Plate Reader (MD Spectra Max M5) E525-1Jeanette Lynch, 6914Shen-Ling Xia, 6581
Ratio Imaging Analyzer (Intracellular Imaging & Nikon) E525-1 Shen-Ling Xia, 6581Realtime PCR (AB 7500) E525-1 Elena Yarmola, 4305
Refrigerator for flammable material D122-1 Bert Herrera, 6797Shaker, Incubator, Floor Model (NBS Series 25) E371-1 To be assignedSpectrophotometer, Shimadzu E364-1 Bert Herrera, 6797Ultrasound Biomicroscopy (Vevo 2100) Bldg.11 Shen-Ling Xia, 6581Xerox Machine E584-1 Chris Johnston, 6481
Research Services: Laboratory Safety Manual Page 103

COMMON RESOURCE EQUIPMENT (RORC)EQUIPMENT ROOM CONTACT PERSON, Ext.Fax Machine Reception Liddy Cope, 4946LCD projector Conference Liddy Cope, 4946Photocopiers (2) Supply Liddy Cope, 4946
Printers (1 color, 2 B&W)Common Cubicle Liddy Cope, 4946
TV Conference Liddy Cope, 4946
TypewriterCommon Cubicle Liddy Cope, 4946
VCR Conference Liddy Cope, 4946
Updated 04/16/15
Research Services: Laboratory Safety Manual Page 104

NORTH FLORIDA/SOUTH GEORGIA VETERANS HEALTH SYSTEMRESEARCH SERVICE
SECTION VIII. SUBCOMMITTEE ON RESEARCH SAFETY STANDARD
OPERATING PROCEDURESApril 1, 2013
PURPOSEThese are the Standard Operating Procedures for the North Florida/South Georgia Veterans Health System (NF/SGVHS) Subcommittee on Research Safety (SRS). They are based on the Department of Veterans Affairs, Veterans Health Administration (VA-VHA) regulations and other applicable federal regulations governing the conduct of local research programs involving the use of potential hazards encountered in research settings, including, but not limited to biohazards, such as pathogens and etiologic agents corresponding to Biosafety Levels (BSL) 1-2, chemical, physical, and radiation hazards. NF/SGVHS does not currently have the capability to accommodate BSL-3 Research.
The primary purpose of the SRS is to ensure the safety of all NF/SG VHS personnel involved in research activities. The SRS is responsible for the oversight of research activities and studies involving biological, chemical, physical, and radiation hazards, including assuring that studies are reviewed and in compliance with all applicable regulations, policies, and guidelines prior to approval by the NF/SG VHS Research and Development Committee (R&DC); reviewing, prior to submission, studies for VA R&D funding; conducting annual review and oversight of all studies with potential safety hazards; and conducting an annual program of review and coordination of all safety-related activities in research laboratories including mandatory and non-mandatory training, safety inspections, chemical inventory updates, accident reporting, and liaison activities with all facility safety committees and officials as required in VHA Handbooks 1200.08 and 1200.06.
BACKGROUNDPer VHA Handbook 1200.08 Safety of Personnel Engaged in Research, Research offices must maintain a Research Safety Program that is consistent with VA policies, Federal statutes and regulations from Occupational Safety and Health Administration (OSHA), the Environmental Protection Agency (EPA), the Nuclear Regulatory Commission (NRC), National Institutes of Health (NIH) and Centers for Disease Control and Prevention (CDC), etc., and any applicable State and local requirements.
Research Services: Laboratory Safety Manual Page 105
DEFINITIONS AND ACRONYMS
A. Animal . The term “animal” is defined in VHA Handbook 1200.07, as any live vertebrate animal used or intended for use in research, research training, experimentation, or biological testing, or for a related purpose (Public Health Service (PHS) Policy on Humane Care and Use of Animals, Sec. III). An animal for purposes of compliance with the Animal Welfare Act Regulations (Sec. 1.1) means any live dog, cat, non-human primate, guinea pig, hamster, rabbit, or any other warm-blooded animal which is being used, or is intended for use in research, teaching, testing, or experimentation, exhibitions purposes, or as a pet. The term excludes birds, rats of the genus Rattus and mice of the genus Mus bred for use in research, and horses not used for research purposes and other farm animals, such as, but not limited to livestock or poultry, used or intended for use as food or fiber, or livestock or poultry used or intended for use in improving animal nutrition, breeding, management, or production efficiency, or for improving the quality of food or fiber.
B. Animal Component of Research Protocol (ACORP) . The ACORP, the official VA animal protocol form, is a set of questions that must be considered during a review of animal protocols. It must be used by VA Institutional Animal Care and Use Committee (IACUC) when a project involving animal research is submitted for consideration of VA funding.
C. Biohazards . Biohazards include, but are not limited to, the following:1. Pathogens and etiologic agents, human and non-human primate tissues
including blood and body secretions, and human cell lines corresponding to BSL 1-4;
2. Toxins produced by microbial organisms;3. Poisonous, toxic, parasitic, and venomous animals or plants;4. Recombinant DNA molecules;5. Select agents, as specified in Title 42 Code of Federal Regulations (CFR) Part
73; 7 CFR 331; and 9 CFR 121; and6. Animals experimentally or naturally exposed to any of the preceding.
D. University of Florida Institutional BioSafety Committee (IBC) . The NF/SGVHS does not have its own BioSafety Committee; therefore the Research Service uses the University of Florida Institutional BioSafety Committee, established by a Memorandum of Understanding (February 22, 2012). Under the MOU, the UF IBC shall review and approve or disapprove, as appropriate, all requests to perform research using recombinant DNA (rDNA) at NF/SG VHS, whether funded or unfunded and without regard to funding agency. While the UF IBC reviews research protocols for biosafety matters beyond biohazards, the scope of the UF IBC authority under the MOU extends only to rDNA. The NF/SGVHS SRS reviews and approves or disapproves, as appropriate, VA research using rDNA after the review and approval by the UF IBC. In addition, NF/SGVHS permits the UF IBC to inspect VA laboratories in which rDNA research is, or is proposed to be, conducted. (NF/SGVHS recognizes that UF is authorized to conduct inspections jointly with VA Safety staff of VA labs in which UF funded research is conducted.)University of Florida Institutional BioSafety Committee Web site: http://www.ehs.ufl.edu/Bio/default.asp.
Research Services: Laboratory Safety Manual Page 106

E. Chemical Hazards. Chemical hazards include any substance or mixture of substances with properties capable of producing adverse effects on the health and safety of humans. Chemical hazard categories include, but are not limited to, the following:1. Corrosives;2. Toxic substances (poisons, irritants, asphyxiates);3. Sensitizers;4. Carcinogens, mutagens, and teratogens;5. Flammables; and6. Explosives.
F. Grants Administrative Core (GAC) . The Grants Administrative Core is a work team within the Research Service Office consisting of staff and administrators that are charged to administer all VA grant activities, and human, animal, laboratory and safety compliance. The GAC members also act as R&D committee coordinators and liaisons. Contact information is available on the Research Service Web page: http://www.northflorida.va.gov/NORTHFLORIDA/Research/indexResearchers.asp .
G. Human Subject . As defined in VHA Handbook 1200.05 and Title 38 CFR Part 16 defines a human subject as a living individual about whom an investigator (whether professional or student) conducting research obtains either: 1) data through intervention or interaction with the individual; interaction includes communication or interpersonal contact between the researchers and the subject; or identifiable private information. This definition of human subject includes investigators, technicians, and others assisting investigators, when they serve in a "subject” role by being observed, manipulated, or sampled.
For research covered by Food and Drug Administration (FDA) regulations, human subjects means as individual who is or becomes a participant in a clinical investigation, either as a recipient of the test article or as a control. For research covered by FDA device regulations, subject means a human who participates in an investigation, either as an individual on whom or on whose specimen an investigational device is used or as a control. A subject may be in normal health or may have a medical condition or disease.
H. Human Subject Research Protocol . A human subject research protocol clearly and plainly provides an overview of a proposed study in order to satisfy the VA organization’s guidelines for protecting the safety of human subjects who might be impacted by the research study.
I. Laboratory Safety Manual . The Laboratory Safety Manual is designed to provide basic elements of laboratory safety, and the policies and procedures that govern this facility. All personnel associated with VA laboratories must be familiar with the Laboratory Safety Manual. A copy of the Laboratory Safety manual must be kept in each laboratory, and the Research Service Office, SRS Coordinator’s office. This manual serves as a resource and reference to assist in the minimization of risk associated with the VA Research Service employees’ daily responsibilities.
Research Services: Laboratory Safety Manual Page 107

J. Office of Research and Development (ORD) . ORD is the office within VA Central Office responsible for the overall policy, planning, coordination, and direction of research activities within VHA. The ORD serves as the primary VHA component to advise the Undersecretary of Health on all matters pertaining to compliance and assurance of the protection of human and animal, as well as, research information which also includes impropriety and research misconduct.
K. Physical Hazards . Physical hazards include, but are not limited to, the following:1. Ionizing and non-ionizing radiation,2. Noise,3. Vibration,4. Extremes of temperature and pressure,5. Explosive hazards,6. Electrical hazards, and7. Mechanical hazards.
L. Principal Investigator (PI) . Within the VA, a PI is a qualified individual who is a VA Investigator designated by NF/SG VHS to direct a research project or program, and who usually writes the grant application and protocol. The PI oversees scientific, technical, and day-to-day management of the research, and is considered to be the responsible leader of the research team.
M. Protocol for Research Safety . A protocol, whether an ACORP or a human subject research protocol, is part of the submission packet to the Subcommittee on Research Safety. The protocol, Research Protocol Safety Evaluation (VA Form 10-0398), and other required documents, are used to determine a study’s safety with regard to biological, chemical, physical, and radiation hazards and to determine compliance with all applicable regulations, policies, and guidelines prior to approval by the NF/SG VHS Research and Development Committee (R&DC),
N. Quorum . A quorum is defined as a majority of the voting members. At meetings of the R&D Committee and its subcommittees, including the SRS, a quorum must be established and maintained throughout the entire meeting in order for business to be conducted. A member with a conflict of interest cannot 1) contribute to a quorum, 2) be present for the discussion of the issue for which they are conflicted, except to answer questions from the committee or 3) be present for the vote on the issue (VHA Handbook 1200.05).
O. VA-Approved Research . VA-approved research is research that has been granted final approval by the NF/SG VHS R&D Committee (VHA Handbook 1200.08).
P. Without Compensation (WOC) . A WOC appointment is a VA appointment for a person who performs duties without any direct monetary compensation from the VA (VHA Directive 1200).
Research Services: Laboratory Safety Manual Page 108

RESPONSIBILITIES IN REGARD TO SAFETY OF PERSONNEL ENGAGED IN RESEARCH
A. NF/SG VHS Medical Center Director . The NF/SG VHS Medical Center Director is responsible for: 1) ensuring that the research safety program is staffed adequately and that resources are available to maintain full compliance with all applicable regulations and standards of safety; 2) ensuring that all Research personnel are included in the facility Occupational Safety and Health program and that research space is included in annual workplace inspections; 3) ensuring the resolution of any facilities-related deficiencies identified in inspections, 4) providing engineering support in conducting ventilation maintenance and validation of required specifications; 5) providing the technical assistance of facility safety and health professional, as needed; 6) in cooperation with the Associate Chief of Staff (ACOS) for Research ensuring that measures for the security of the research laboratories and surrounding space are developed; and 7) providing adequate administrative support for the SRS, including: a) space sufficient to provide privacy for conducting sensitive duties related to biosafety, b) the personnel to support the review and record-keeping functions of SRS, and c) support for the timely preparation of investigator correspondence and other documents.
B. Associate Chief of Staff for Research . The NF/SG VHS Associate Chief of Staff for Research (ACOS/R) is responsible for: 1) ensuring that safety related communications from the Chief Research and Development Officer (CRADO) are disseminated to appropriate personnel on time after receipt; 2) ensuring the responses to safety “holds”; 3) ensuring that research activities cease until a particular “hold” is lifted; and 4) ensuring continuous development and evaluation of performance standards of the Research Safety and Security Program.
C. Research and Development Committee . The NF/SG VHS R&D Committee is responsible for: 1) establishing the SRS committee, including assuring that the SRS meets the requirements of the VHA Handbook 1200.08, Appendix B, and approving the SRS Chair (who acts as the Research Safety Coordinator) and SRS members; 2) ensuring that the SRS reviews all study protocols for funding that involve safety hazards to personnel and the environment, and ensuring that the Safety Officer has bi-annually reviewed and approved a complete list of chemicals (identified as hazardous by OSHA or EPA) and is maintained; 3) acting upon SRS recommendations for approval or non-approval of reviewed proposals to be submitted to ORD for funding consideration; reviewing and acting upon SRS minutes; 4) ensuring the development and implementation of the laboratory Chemical Hygiene Plan; 5) appointing the Chemical Hygiene Officer; 6) overseeing compliance with VHA Handbook 1200.08 by all NF/SG VHS Principle Investigators; 7) ensuring the development and implementation of safety protocols by all PIs for all their research studies, and granting final R&D approval to all protocols (VA Form 10-0398, Research Protocol Safety Survey) prior to the initiation of research; 8) ensuring support to the SRS to assist in their functions; 9) ensuring the SRS meeting minutes are documented correctly and maintained by the Research Service Office; 10) providing the ACOS/R, Medical Center Director, and VISN 8 safety officials with adequate information to evaluated the performance of the R&D safety program; 11)
Research Services: Laboratory Safety Manual Page 109

ensuring coordination with all other NF/SG VHS and applicable UF regulatory committees; 12) reviewing accident and injury trends reported by the SRS and recommending and ensuring the implementation of corrective actions; and 13) ensuring that updates to the safety program provided by regulatory agencies are promptly acted on.
D. Subcommittee on Research Safety . The Subcommittee on Research Safety is responsible for:1. Reviewing all research activities involving biological, chemical, physical, and
radiation hazards for compliance with all applicable regulations, policies, and guidelines prior to submission for R&D funding. This includes a review of all research applications that will be conducted at the VA facility or by VA personnel with VA funding located off-site;
2. Reviewing VA Form 10-0398, Research Protocol Safety Evaluation includes a risk assessment of the facilities, level of containment, laboratory procedures, practices, training and expertise of personnel involved in the specific research conducted including recombinant DNA (rDNA) research;
3. Approving all research projects, with a majority of members, involving biological, chemical, physical, and radiation hazards, and forwarding the SRS decision to the R&DC for review and approval prior to the commencement of the study, this is done via a written set of minutes or a written list of approved protocols forwarded to the R&DC;
4. Annually reviewing all active research protocols involving biological, chemical, physical, and radiation hazards, regardless of funding status or source. All protocol changes must be documented, reviewed and approved.
5. Ensuring that the SRS reviews all study protocols for funding that involve safety hazards to personnel and the environment, and ensuring that the Safety Officer has reviewed and approved a complete list of chemicals (identified as hazardous by OSHA or EPA) and is maintained;
6. Coordinating all safety-related activities in research laboratories including mandatory and non-mandatory training, safety inspections, bi-annual chemical inventory up-dates, accident reporting, and liaison activities with all NF/SG VHS subcommittees and applicable UF committees (IBC and IRB), and including follow-up evaluations and correction of deficiencies, and ensuring coordination with other regulatory facility committees and R&DC subcommittees, the Radiation Safety Officer and IRB, and the Safety Officer;
7. Identifying the need for health surveillance of personnel involved in research projects and advising the R&DC and Employee Health, if needed;
8. Maintaining adequate documentation of all SRS activities and forwarding the SRS minutes to the Research Service Office.
9. Ensuring that all laboratory personnel receive/review annual and specific research safety training;
10.Holding the SRS meeting at least monthly, with a minimum of 11 meetings within the annual year, publishing the SRS meeting schedule on the Research Service Web site: http://www.northflorida.va.gov/NORTHFLORIDA/Research/indexResearchers.asp ;
11.Annually evaluate and correct, if needed, the effectiveness of the laboratories’ Chemical Hygiene Plan;
Research Services: Laboratory Safety Manual Page 110

12.Ensure the review of all injury reports, adverse environmental reports, injury and illness trends, and investigating, if needed (Ad Hoc committees may be used), providing corrective plans, and ensuring corrections; and reporting to the R&DC and ACOS/R
13.Ensuring there are policies and procedures in place to protect employee health, working with the facility staff to review quantity and type of hazardous waste; monitor environmental factors, as needed, and maintain records; and provide technical assistance where applicable.
E. Principal Investigators . All NF/SG VHS Principal Investigators are responsible for:1. Providing a complete and signed Research Protocol Safety Evaluation form (VA
Form 10-0398), Coversheet – Safety, abstract, protocol, complete list of “hazardous” chemicals, training records, radiation safety approval letter (if required, and other required documentation) to the SRS Coordinator before the published submission deadline for the next SRS meeting;
2. Reporting problems and concerns about operation and containment practices and procedures as applicable to the Research Laboratory Safety Officer, Veterinary Medical Officer (VMO), Radiation Safety Officer, etc.
3. Ensuring that all accidents are reported to the Employee Health Office and the Facility Safety Officer.
4. Securing approval of the R&D Committee through the SRS for any significant changes made in the approved original research plan (documented using the Research Protocol Safety Amendment Form).
5. Securing annual and 3-year ACORP continuing safety reviews through the SRS (documented using the Request for Annual Continuing Safety Review Form).
6. Coordinating with appropriate safety staff (Laboratory Safety Officer, Industrial Hygienist, Radiation Safety Officer, Chemical Hygiene Officer) for the removal or disposal of all chemicals, biological agents, radioisotopes, and waste generated by these materials.
7. Notifying all pertinent personnel prior to departure from the laboratory, as well as, notifying all pertinent personnel prior to relocating the research laboratory space.
8. Ensuring that a copy of the laboratory’s Chemical Hygiene Plan is readily available to all employees in the work area, that employees have been trained in the contents of the Plan, and that all provisions of the Plan are implemented in all laboratories under the PI’s supervision.
9. Maintaining an up-to-date inventory of all hazardous chemicals located in the laboratory.
10.Ensuring that all laboratory personnel know the location of this inventory.11. Investigating the deficiencies cited during all inspections of work areas.12.Submitting a written abatement plan for all deficiencies cited during inspections
to SRS within the specified time limits.
F. SRS Coordinator . The SRS Coordinator is responsible for assuring the Coversheet – Safety, Research Protocol Safety Evaluation form (VA Form 10-0398), Research Protocol Safety Amendment Form, and Request for Annual Continuing Safety Review Form are accurately processed, proper guidelines are followed, minutes are
Research Services: Laboratory Safety Manual Page 111
accurate, annual renewals are accomplished, files are maintained appropriately and securely, and that all work is conducted in a timely manner, and the SRS minutes are forwarded to the R&D Committee.
G. Research Laboratory Safety Officer . The Research Laboratory Safety Officer is responsible for review of laboratory safety and for updating the Research Laboratory Safety Manual annually and presenting it to the SRS for approval.
H. Chemical Hygiene Officer . The Chemical Hygiene Officer is appointed by the ACOS/R and oversees and updates the Chemical Hygiene Plan for the Research Service. This individual also presents chemical safety orientation to all new personnel working in the Research labs.
SRS MEMBERSHIP
A. The NF/SH VHS Subcommittee on Research Safety (SRS) will include the following member roles: 1. SRS Chair (voting)2. SRS Vice Chair (UF Affiliated, voting)3. Member of the Research and Development Committee, and R&DC Liaison (SRS
Chair, voting)4. Chemical Hygiene Officer (Ex Officio voting)5. Biological Safety Officer (UF Affiliated, voting)6. Alternate Biological Safety Officer (UF Affiliated, voting)7. Safety Officer (Facility Safety Officer, voting)8. Alternate Safety Officer (Assistant Facilities Safety Officer, voting)9. Radiation Safety Officer (voting)10.Laboratory Safety Officer (voting)11.VA Representative on UF IBC (voting)12.3 VA Scientists/Principal Investigators (voting)13.1 VA Clinician/Principal Investigator (voting)14.3 UF Affiliated Scientists/Principal Investigators (voting)15.Administrative Officer for Research Service (Research Service Liaison, Ex
Official Member R&DC) (Ex Officio, non-voting)16.NF/SG VHS Union Representative (Ex Officio, non-voting)17.Research Service Liaison (Ex Officio, non-voting)18.2 Research Compliance Officers (Consultants, non-voting)19.SRS Coordinator (non-voting)
B. The SRS maintains at least five voting members, exclusive of ex-officio members at all times. Routinely the SRS has from 10 to 15 voting members, each person representing more than one role listed above. A minimum of one UF affiliated member must attend each SRS meeting. The expertise of the SRS membership is diverse and represents expertise in the local facility, and various safety and research areas such as:1. Etiologic agents, including bloodborne and airborne pathogens2. Chemical carcinogens and other chemical hazards
Research Services: Laboratory Safety Manual Page 112

3. Physical and radiation hazards4. Specific occupational safety and health, environmental5. Research operations
C. Appointment of Members. SRS and R&DC members may forward the names of nominees for membership to the Research Service Office. The R&DC votes on the appointment of all SRS members and the Medical Center Director officially appoints members and the Chair in writing. The length of the appointments are: 1. The SRS Chair in appointed for the term of 1 year. The SRS Chair may be re-
appointed without any lapse in time; however, the SRS Chair may not simultaneously chair the R&D Committee or another research subcommittee.
2. Members may be appointed for up to three consecutive years and may be reappointed without any break in membership.
SRS AGENDA AND MINUTES
The SRS provides an agenda with attachments to the SRS members prior to the SRS meeting. It provides for the approval of the last set of minutes, unfinished business, new business, reoccurring reports, and other needed discussion of pertinent issues.
The SRS minutes document the discussion of the SRS meeting and includes the place, date, and time (start and end) of the meeting, attendance record including a lists of guests, the signature of the SRS Chair, an indication of quorum on all votes, a record of all discussions (including conclusions, recommendations, follow-up needed, and actions).
A recommendation is not to be carried for more than two meetings awaiting a resolution unless there is clear documentation that a plan of action is being followed and an anticipated date of resolution is noted in the minutes.
In addition, the SRS must review, at its next convened meeting, any report involving an incident or event as described in Handbook 1058.01, Section 9. Requirements Related to Research Safety.
Emergency sessions of the SRS may be convened if an incident is a significant risk to the safety of research personnel or the environment.
If the significance of a reported event is not clear, the SRS Chair, or designee, must consult the ORO RO and the ORO Associate Director for Research Safety and Animal Welfare.
Following the requirements of Handbook 1058.01, Section 9. Requirements Related to Research Safety, the SRS Chair must send a written report on reportable incidents to the Medical Center (MC) Director within 5 business days, and copy the ACOS/R and R&DC Chair.
The SRS must reach a determination that a reportable event did (or did not) occur within 30-45 days after receiving a relevant report. Remedial actions involving a specific study or research team must be completed within 90-120 days of the SRS’s determination, unless remediation required substantial renovation, fiscal expenditure, legal negotiation, etc. The determination will be discussed with the R&DC Chair and ACOS/R, and reported to the MC Director.
Research Services: Laboratory Safety Manual Page 113

Minutes are written and published within 3 weeks of the meeting date, reviewed and approved at the next meeting. The minutes are signed by the SRS Chair and distributed to:
PDF copy to R&D Secretary PDF copy to Safety Committee Members File Original in Committee Meeting Minutes Binder
TRAINING
Training requirements for all personnel are specified in the Guidelines for Safety Training, located in the Research Service Safety Policies and Procedures. Both initial and annual trainings are specified in the Guidelines.
Training certificates must be provided at the time of submission with these documents: Coversheet – Safety, Research Protocol Safety Evaluation Form (VA Form 10-0398), Research Protocol Safety Amendment Form, and Request for Annual Continuing Safety Review Form.
Research Services: Laboratory Safety Manual Page 114

PROCESS FOR RESEARCH PROTOCOL SAFETY EVALUATIONS
A. Safety Protocol Review Guidelines1. All study protocols (human, animal and laboratory) must have an initial Safety
evaluation.1. Bench studies (non human/non animal – does not go through IACUC or IRB)
i. Should the study require an initial SRS Full Board Safety Review (because there is a lab involved and there are safety issues), the IACUC Coordinator will monitor this study and will receive the annual safety renewal through the Safety Committee.
ii. Should the study have an initial SRS Chair Safety Review (there are no safety issues), this study will be treated as a non-human study and does not require any further action by the SRS, and will be processed through the HRPP Office.
2. The review of the Research Protocol Safety Evaluation (VA Form 10-0398), for each protocol, must include a risk assessment of the facilities, level of containment, laboratory procedures, practices, training and expertise of personnel involved in the specific research conducted including recombinant DNA research.
3. All studies that receive an initial Full Board SRS evaluation must complete the annual Renewal/Continuing Review by the anniversary SRS approval date (365 days after the initial or last SRS approval date – Committee meeting date). All IACUC studies must also annually submit an ACORP 3rd Year Safety Renewal for a Full Board SRS evaluation.
4. Notice is sent to the PI of the study, at least 90 to 60 days before the end date of the initial or last safety review, by the HRPP, IACUC or SRS Coordinator, that the annual Renewal/ Continuing Review is required.
5. Safety protocol reviews will be performed at the same time IRB and IACUC reviews are being performed.
6. No study may be given initial approval by the R&DC unless the Safety evaluation has been reviewed and approved by the SRS, and the SRS Chair has signed the Safety evaluation form.
7. Under no circumstances may a study (human, animal or laboratory) start without the final R&DC approval of the initial protocol.
8. Consideration of pending items for a protocol in review by the SRS may not be carried for more than two SRS meetings awaiting a resolution unless there is a clearly documented plan of action and an anticipated date of resolution is noted.
9. Should a study under review pass its last date of SRS approval, remedial actions will occur, based on the requirements of Handbook 1058.01, Section 9- Requirements Related to Research Safety. Remedial actions involving a specific study or research team must be completed within 90-120 days of the SRS’s determination, unless remediation requires substantial renovation, fiscal expenditure, legal negotiation, etc. The determination will be discussed with the R&DC Chair and ACOS/R, and reported to the MC Director.
11.The Study Start Date is: The date the study is initially approved by the R&DC (Committee meeting date).
Research Services: Laboratory Safety Manual Page 115

12.The SRS Expiration Date is: No longer than 1 year (365 days) from date of the SRS (Committee meeting date) initial or annual approval.
B. Initial Safety Protocol Review1. The SRS Coordinator obtains a complete and signed original Research Protocol
Safety Evaluation (VA Form 10-0398), along with the Coversheet-Safety, protocol, abstract, approval letters and training certificates, if required, from the Principal Investigator.
2. The SRS Coordinator reviews the forms and documents to determine if the study protocol is appropriate for a Chair Review or a Full Board Review.
3. SRS Chair Review a. If the study protocol is appropriate for a Chair Review, the Evaluation Form is
given to the SRS Chair for review and signature. No other signatures are required from the Safety Committee.
b. This study is added to the next SRS Agenda, as an informational item. The Evaluation Form and documents are scanned and distributed to the SRS members for their information and may be discussed during the SRS meeting.
c. After the SRS meeting, the SRS Coordinator notifies the HRPP Coordinator by email that the original and signed (by the SRS Chair) Evaluation Form is available for pickup and R&D approval.
d. The HRPP Coordinator adds the SRS approval to their HRPP study packet. e. For HRPP:
1) Once the HRPP Office is satisfied that the study packet is in full compliance, the study is placed on the R&DC agenda (i.e., HRPP Summary study list) for final approval.
2) The HRPP Coordinator generates the R&DC Initial Approval Letter and is responsible for attaining the R&DC Chair and ACOS/R signatures. In addition, the R&DC Chair signs the Research Protocol Safety Evaluation (VA Form 10-0398).
f. For IACUC: Animal studies may not go through SRS Chair Review. All animal studies must go through the SRS Full Board review and approval process (see below).
g. The HRPP Coordinator emails the final copy of the Evaluation Form and original R&DC Initial Approval Letter to the PI, and forwards the signed original copy of the Evaluation Form and a copy of the R&DC Initial Approval Letter to the SRS Coordinator for filing.
h. The original Evaluation Form, supporting documents and R&DC Initial Approval Letter are put into the SRS Study file (filed by PI last name and title).
i. The HRPP Coordinator updates the Master Study Spreadsheet and ePromise to show that full Safety approval has been granted.
4. SRS Full-Board Review a. If the study protocol is appropriate for a Full Board Review, the Evaluation is
made available to the SRS Chair and all SRS members for review, and is placed on the next SRS meeting agenda as an item for discussion.
Research Services: Laboratory Safety Manual Page 116
b. The study’s Evaluation Form and all documents are discussed at the next SRS meeting.
c. The SRS members review and discuss each study and may vote to Approve, Approve Pending Modifications, or Table the study.
d. If modifications are required, the SRS Coordinator notifies the PI of the SRS required corrections/concerns, provides the dates for the next SRS meeting to the PI, if needed, and follows up on all corrections/concerns.
e. Once all the revised documents are received the Coordinator confirms all corrections/concerns have been addressed, and consults with the SRS Chair, as needed. He/she then obtains all required SRS signatures on the Evaluation Form (may include Radiation Safety Officer (RSO)), Industrial Hygienist, and SRS Chair.
f. For HRPP: 1) Once the HRPP Office is satisfied that the study packet is in full
compliance, the study is placed on the R&DC agenda (i.e., HRPP Summary study list) for final approval.
2) The HRPP Coordinator generates the R&DC Initial Approval Letter and is responsible for attaining the R&DC Chair and ACOS/R signatures. In addition, the R&DC Chair signs the Research Protocol Safety Evaluation (VA Form 10-0398).
g. For IACUC: 1) Once the IACUC Office is satisfied that the study packet is in full
compliance and approved by the IACUC, the study is placed on the R&DC agenda (i.e., IACUC Minutes or IACUC Summary study list) for final approval.
2) The IACUC Coordinator generates the R&DC Initial Approval Letter and is responsible for attaining the R&DC Chair and ACOS/R signatures. In addition, the R&DC Chair signs the Research Protocol Safety Evaluation (VA Form 10-0398).
h. The HRPP or IACUC Coordinator emails the final copy of the Evaluation Form and original R&DC Initial Approval Letter to the PI, and forwards the signed original copy of the Evaluation Form and a copy of the R&DC Initial Approval Letter to the SRS Coordinator for filing.
i. The original Evaluation Form, supporting documents and R&DC Approval Letter are put into the SRS Study file (filed by PI last name and title).
j. The HRPP or IACUC Coordinator updates the Master Study Spreadsheet and ePromise to show that full Safety approval has been granted.
C. Amendments for Safety Protocols1. The SRS Coordinator obtains a complete and signed original Research Protocol
Safety Amendment Form, along with the Coversheet-Safety, protocol, abstract, approval letters and training certificates, if required, from the Principal Investigator.a. If the HRPP or IACUC Coordinators receive a HRPP or IACUC protocol with
amendments, they will ask the PI if there are also Safety Protocol changes. If there are Safety Protocol changes that impact safety, the Coordinator will make sure the PI knows to complete and submit a Research Protocol Safety
Research Services: Laboratory Safety Manual Page 117
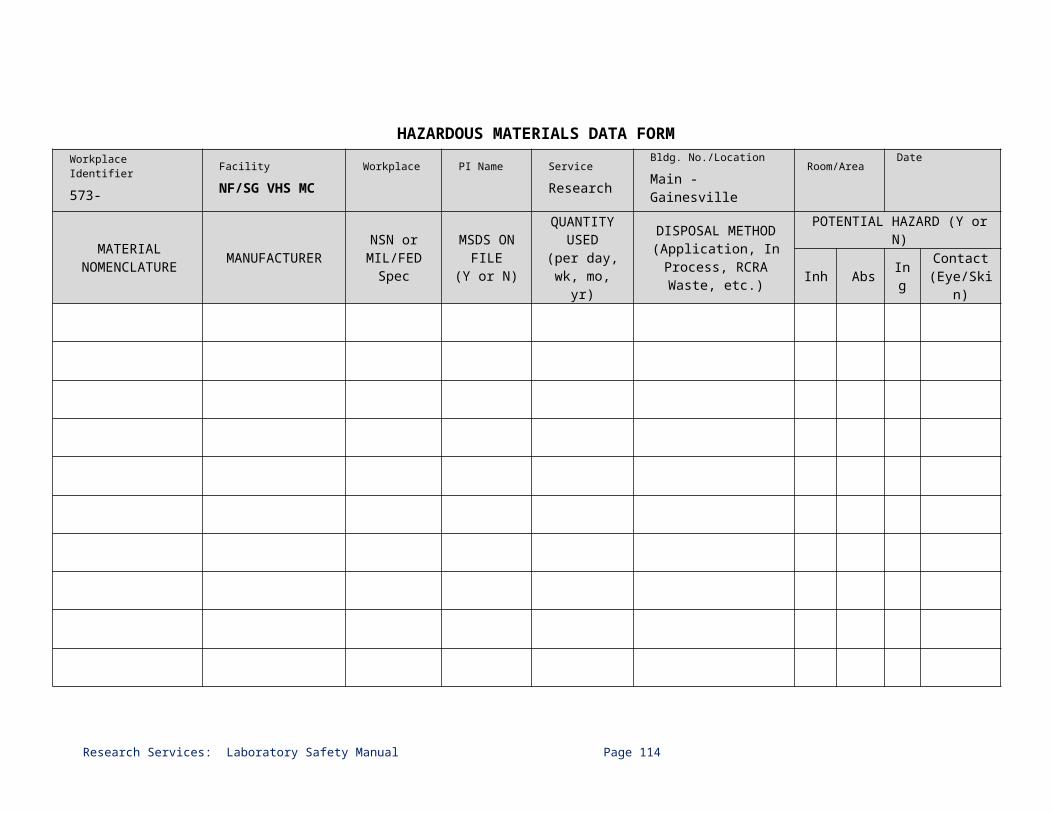
Amendment Form, Coversheet-Safety, and supporting documents, to be submitted to the SRS Coordinator.
b. A change in location/lab, research activity, use of chemicals, radiation, rDNA, PI, or the addition of personnel/staff requires Full-Board SRS Review.
c. Removal of personnel/staff only requires a Chair Review.2. The SRS Coordinator reviews the forms and documents to determine if the
Safety protocol is complete and appropriate for the SRS Full Board Review, and then places the Safety Protocol Amendment on the next SRS meeting agenda as an item for discussion.
3. Steps B.4. SRS Full-Board Review, c through j, are followed with the following exception:a. The HRPP or IACUC Coordinator emails the PI (cc: SRS Coordinator) that
the amendments have been approved, including the Amendments for the Safety Protocols.
b. The R&DC Chair’s signature is not required on the Research Protocol Safety Amendment Form. The Safety Amendment Form, signed by the SRS Chair, and other relevant documents, are attached to the email.
c. The study as part of the SRS minutes is placed on the R&DC agenda for informational purposes.
D. Annual Renewal/Continuing Review for Safety Protocols1. All Safety protocols/studies that originally received SRS Full-Board Reviews
require annual SRS continuing safety renewal (and for animal studies: 3 year renewals).
2. The HRPP and IACUC Coordinators notify the PI that the Request for Annual Continuing Safety Review, Coversheet-Safety and supporting documents must be submitted 90 days prior to the anniversary of the SRS approval date.
3. If there have been no changes to the protocol, only a signed original of the Coversheet – Safety and the Request for Annual Continuing Safety Review are required. The Chair or a designee will review and approve such protocol renewals.
4. For Safety protocols with minor to extensive changes within the past renewal period, SRS Full-Board Reviews are required.
5. The annual Safety Evaluation Renewals for IACUC and HRPP protocols are due before the SRS protocol approval anniversary (365 days after prior SRS approval date).
4. Steps B.4. SRS Full-Board Review, c through j, are followed with the following exception:a. The HRPP or IACUC Coordinator generates the ACOS/R Annual Renewal
Approval Letter and is responsible for attaining the ACOS/R signature. In addition, the R&DC Chair signs the Research Protocol Safety Amendment Form.
b. The study is placed on the R&DC agenda (For HRPP: HRPP Summary Study List; For IACUC: IACUC Minutes or IACUC Summary Study List) for informational purposes.
Research Services: Laboratory Safety Manual Page 118
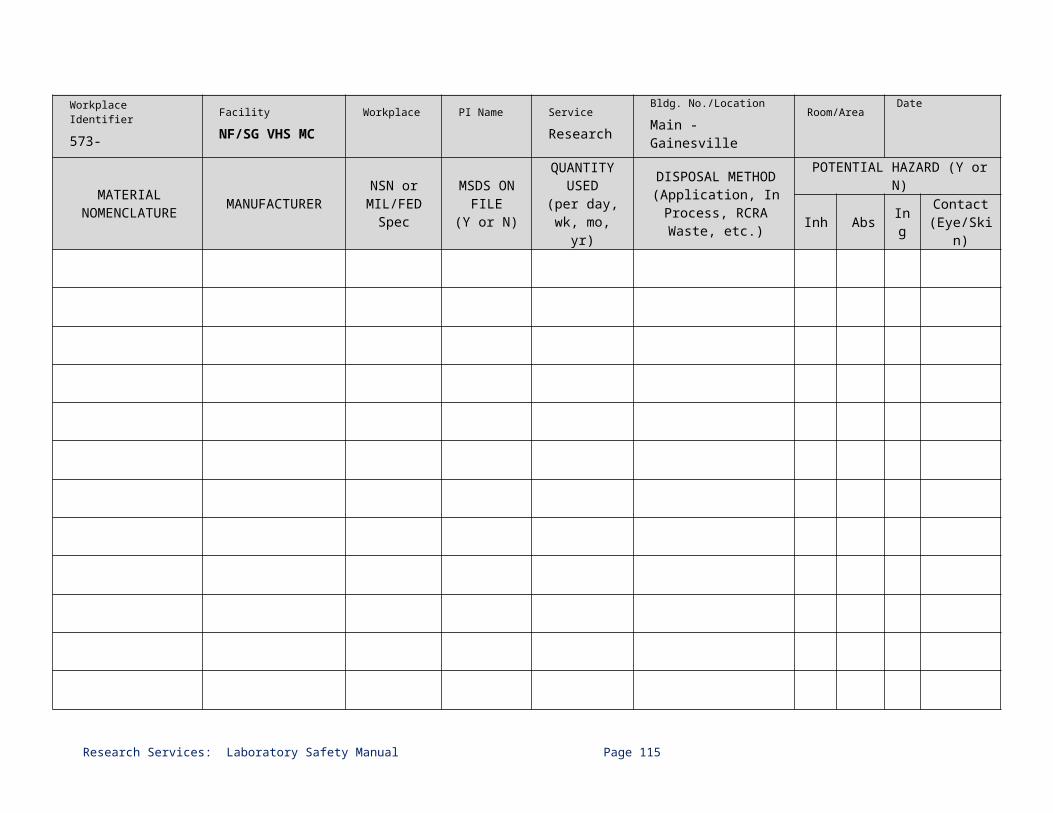
Grants Administration Core
PROCESS FOR RESEARCH PROTOCOL SAFETY EVALUATIONS TABLES AND DECISION TABLES
Initial Safety Protocol ReviewsSRS Chair Review Full-Board Review
Why and when is the initial Safety Protocol Review completed?
It is completed when the PI has a new study and submits it to the HRPP or IACUC for review.
The SRS Safety Protocol Review is done at the same time as the HRPP and IACUC review.
Forms Used Research Protocol Safety Evaluation (VA Form 10-0398) Coversheet-Safety
Human studies will have this type of review. Yes Yes
Animal studies will have this type of review. No Yes
Who signs the Research Protocol Safety Evaluation (10-0398)?
Principal Investigator SRS Chair R&DC Chair
Principal Investigator Chemicals: Safety Officer Radiation: Radiation Safety
Office SRS Chair R&DC Chair
When is this Evaluation signed by the SRS Chair and R&DC Chair?
SRS Chair signs: After he/she completes the SRS Chair Review
R&DC Chair signs: After the IRB, HRPP and SRS approvals are completed; and the HRPP Study List, (with the study listed) is approved by the R&DC.
SRS Chair signs: After the SRS Committee approves the initial protocol.
R&DC Chair signs: After the IRB and HRPP, or
IACUC, and SRS approvals are completed;
and HRPP Summary (with the study listed) is approved by the R&DC;
or the IACUC Summary or Minutes (with the study listed) approved by R&DC
Who signs the R&DC Initial Approval Letter?
R&DC Chair ACOS/R
R&DC Chair ACOS/R
When is the R&DC Approval Letter signed?
R&DC Chair and ACOS/R sign:
Right after the R&DC meeting approving the study has concluded.
R&DC Chair and ACOS/R sign: Right after the R&DC meeting
approving the study has concluded.
Who gets what copies?
SRS Coordinator: Original: Research Protocol Safety Evaluation (VA Form 10-
0398) Original: Coversheet-Safety Copy: R&DC Approval LetterPrincipal Investigator: Copy: Research Protocol Safety Evaluation (VA Form 10-
0398) Copy: Coversheet-Safety Original: R&DC Approval Letter
INITIAL SAFETY PROTOCOL EVALUATION
Research Services: Laboratory Safety Manual Page 119

Research Services: Laboratory Safety Manual Page 120
ChairDecision
NoYes
YesYes
No
Yes
No
* Start Safety
Evaluation Form Submitted
Is this an Animal Subject Study?
Is this a Human Subject Study?
Is this a Laboratory/ Bench (Non-Human/Non
Animal) Study
Study HAS1) Biological,2) Chemical,
3) Physical, and/orRadiological Hazards.
All animal subject studies must go through
the SRS Full Board review and approval
process.
** Full Board reviews the study evaluation.
Place on the SRS agenda as the Full Board – reviewed the initial evaluation.
** Full Board reviews the study evaluation.
Place on the SRS agenda as the Full Board – reviewed the initial evaluation.
*** Chair reviews the study evaluation.
Place on the SRS agenda as the Chair - reviewed initial evaluation.
NOTE: * Start: SRS Coordinator performs a pre-review and contacts PI on needed clerical changes/additions. ** Required submission: Cover Sheet-Safety, Research Protocol Safety Evaluation Form (VA Form 10-0398), Research Safety Protocol and abstract, chemical list, training forms, and other attachments *** Required submission: Cover Sheet-Safety, Research Protocol Safety Evaluation Form (VA Form 10-0398), abstract and protocol.NOTE: Chair Reviews performed weekly. Full Board Reviews performed at the monthly SRS meetings.
Animal Study: SRS Office communicates approvals with the PI, IACUC and R&DC
Human Study: SRS Office communicates approval with the PI and HRPP Office; HRPP notifies R&DC
Lab/Bench Study: SRS Office communicates approvals with the PI & IACUC Office; IACUC Office notifies R&DC
Human Study: SRS Office communicates approval with the PI and HRPP Office; HRPP notifies R&DC
Lab/Bench Study: SRS Office communicates approval with the PI and HRPP Office; HRPP Office notifies R&DC

Safety Protocol Amendment ReviewsSRS Chair Review Full-Board Review
Why and when is the Amendment for Safety Protocol Review completed?
It is completed when the PI makes amendments to his/her study that impact the study’s safety.
The SRS Safety Amendment Protocol Review is done at the same time as the HRPP and IACUC review.
Forms Used Research Protocol Safety Amendment Form Coversheet-Safety
Human studies will have this type of review. No YES Yes
Animal studies will have this type of review.
No for most
protocols
YESONLY if the change is
removing staff.
Yes
Who signs the Research Protocol Safety Amendment?
Principal Investigator Chemicals: Safety Officer Radiation: Radiation Safety Office SRS Chair
When is this Evaluation signed?
SRS Chair: After the SRS Committee approves the amendment.
Who signs the Approval Letter?
No letter is generated, PI receives email of approval and copy of SRS Amendment Form.
When is the email sent? After the HRPP or IACUC Office determines all
approvals have been completed, including the SRS approval, for the amendment.
How is the R&DC notified of the Amendments?
R&DC is informed at their next meeting: Amendments, as informational items, are
placed on the SRS Minutes (with the study listed)
Who gets what copies?
SRS Coordinator: Original: Research Protocol Safety Amendment Form Original: Coversheet-Safety Cc: on approval email from HRPP or IACUC CoordinatorPrincipal Investigator: Copy: Research Protocol Safety Amendment Form Copy: Coversheet-Safety Original: email from HRPP or IACUC Coordinator
Research Services: Laboratory Safety Manual Page 121
SAFETY PROTOCOL AMENDMENT REVIEWS
Research Services: Laboratory Safety Manual Page 122
StartAmendment
Form Submitted
Amendment Form submitted from a Study originally reviewed by SRS Chair.
Amendment Form submitted from a Study originally reviewed by
Full Board.
*** Changes are made to the study protocol that DO NOT impact safety (e.g., change in PI or staff, additional data/ analysis).
** Changes are made to the study protocol that DO impact safety (e.g., addition of chemicals, blood draws, etc.), MUST be reviewed by the Full Board.
*** Changes are made to the study protocol that DO NOT impact safety (e.g., removal of staff);
MUST be reviewed by the Chair.
** Every other type of an amendment (e.g., change in PI, added staff, chemicals, blood draw, data/analysis),
MUST be reviewed by the Full Board.
Full Board reviews the study amendment.
Place on the SRS agenda as a Full Board - amendment review.
Full Board reviews the study amendment.
Place on the SRS agenda as a Full Board - amendment review.
Chair reviews the study amendment.
Place on the SRS agenda as a Chair Review - Informational.
DO NOT submit an amendment to SRS.
NOTE: * Start: SRS Coordinator performs a pre-review and contacts PI on needed clerical changes/additions. ** Required submission: Cover Sheet-Safety, Research Protocol Safety Amendment Form, Research Safety Protocol and abstract, chemical list, training forms, and other attachments *** Required submission: Cover Sheet-Safety, Research Protocol Safety Amendment Form, protocol and abstract.NOTE: Chair Reviews performed weekly. Full Board Reviews performed at the monthly SRS meetings.
Safety Protocol Annual Renewal/Continuing ReviewsSRS Chair Review Full-Board Review
Why and when is the Annual Renewal for Safety Protocol Review completed?
All Safety Protocols that initially (or had a safety concern added to the protocol in a prior review) went through a SRS Full-Board Review require annual renewals; in addition animal protocols also require IACUC third annual reviews that include a revised protocol.
It is completed no later than 365 days since the initial or last SRS approval date.
The SRS Safety Annual Renewal Review is done at the same time as the HRPP and IACUC review.
Forms Used Request for Annual Continuing Safety Review Form Coversheet-Safety
Human studies will have this type of review.
Yes: Only if there are no changes to the safety protocol over the prior year.
Yes
Animal studies will have this type of review.
Yes: Only if there are no changes to the safety protocol over the prior year.
Yes
Who signs the Request for Annual Continuing Safety Review?
Principal Investigator SRS Chair R&DC Chair
Principal Investigator Chemicals: Safety Officer Radiation: Radiation
Safety Office SRS Chair R&DC Chair
When is this Annual Continuing Safety Review Form signed by the SRS Chair and R&DC Chair?
SRS Chair signs: After the SRS Committee approves the initial protocol
R&DC Chair signs: After all necessary Subcommittee reviews and
approvals are completedWho signs the ACOS/R Approval Letter? ACOS/R
When is the ACOS/R Approval Letter signed?
ACOS/R signs: After all necessary Subcommittee reviews and approvals
are completedHow is the R&DC notified of the Annual Renewals/ Continuing Reviews?
R&DC is informed at their next meeting: Amendments, as informational items, are placed on the
SRS Minutes, and HRPP Summary, or the IACUC Summary or Minutes (with the study listed)
Who gets what copies?
SRS Coordinator: Original: Request for Annual Continuing Safety Review
Form Original: Coversheet-Safety Copy: ACOS/R Approval LetterPrincipal Investigator: Copy: Request for Annual Continuing Safety Review Form Copy: Coversheet-Safety Original: ACOS/R Approval Letter
Research Services: Laboratory Safety Manual Page 123

SAFETY ANNUAL RENEWAL/CONTINUING REVIEW
Research Services: Laboratory Safety Manual Page 124
Yes
No NoYes
Yes
YesYes
No
No
Yes
Yes
1) Are there major changes to the safety protocol?OR2) Is this the IACUC 3rd annual review?
StartAnnual Continuing
Safety Review Form Submitted
Is this an Animal Subject Study?
Study must go through the SRS Full Board review and approval process.
** Full Board reviews the annual/3rd Year review.
Place on the SRS agenda as the Full Board – reviewed annual/3rd Year review.
Study must go through the SRS Chair review and approval process.
*** Chair reviews the annual review.
Place on the SRS agenda as the Chair - reviewed annual review.
No
Yes
NoIs this a Human Subject Study?
Is this a Laboratory/ Bench
(Non-Human/Non Animal) Study
Did this study have an Initial Full Board Review or a Full Board review last annual review?
There are changes to the safety protocol?
Are there major changes to the safety protocol since the last review or amendment?
Did this study have an Initial Chair Review?
Study must go through the SRS Full Board review and approval process.
** Full Board reviews the annual review.
Place on the SRS agenda as the Full Board – reviewed annual review.
Study must go through the SRS Chair review and approval process.
*** Chair reviews the annual review.
Place on the SRS agenda as the Chair - reviewed annual review.
This study does not require an Annual Review.
Animal Studies: SRS Office communicates approvals with the PI, IACUC and R&DCHuman Studies: SRS communicates approval with the PI and HRPP Office; HRPP notifies the R&DCLab/Bench Studies reviewed by Full Board: SRS Office communicates approvals with the PI, and R&DCLab/Bench Studies reviewed by Chair: SRS Office communicates approval with the PI and HRPP Office; HRPP notifies R&DC
NOTE: * Start: SRS Coordinator performs a pre-review and contacts PI on needed clerical changes/additions. ** Required submission: Cover Sheet-Safety, Request for Annual Continuing Safety Review Form, Research Safety Protocol (For IACUC: fully revised Protocol required for 3rd Year review), and abstract, chemical list, training forms, and other attachments *** Required submission: Cover Sheet-Safety, Request for Annual Continuing Safety Review Form, Research Safety Protocol (For IACUC: fully revised Protocol required for 3rd Year review), and abstract NOTE: Chair Reviews performed weekly. Full Board Reviews performed at the monthly SRS meetings.

REFERENCESVHA Handbook 1200.08, Safety of Personnel Engaged in Research, March 6, 2009VHA Handbook 1200.1, Research and Development (R&D) Committee, June 16, 2009
FOLLOW-UP RESPONSIBILITYThe Subcommittee on Research Safety is responsible for the annual review and revisions of this SOP as needed.
Initial Approval: 09/23/2009Review/Revision: 10/22/2010 Review/Revision: 01/20/2011Review/Revision: 02/27/2012Review/Revision: 04/01/2013Review/ 12/18/2014Review/ 04/16/2015
Research Services: Laboratory Safety Manual Page 125

SECTION IX. MEMORANDUM OF UNDERSTANDING BETWEEN NF/SG
VHS AND UF CONCERNING THE USE OF UF INSTITUTIONAL BIOSAFETY
COMMITTEE
Research Services: Laboratory Safety Manual Page 126
Research Services: Laboratory Safety Manual Page 127

Research Services: Laboratory Safety Manual Page 128

Research Services: Laboratory Safety Manual Page 129

Research Services: Laboratory Safety Manual Page 130

SECTION X. NF/SG VHS SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETY
GENERAL INSTRUCTIONS:The following checklist has been prepared as an assessment tool for the evaluation of VHA Research Safety Laboratories. The checklist is comprehensive and intended to provide guidance for developing and monitoring research safety program compliance (Appendix A explains acronyms used in the Checklist).
Return the completed, signed and dated form to Research Service Office, within 7 working days of the inspection date.
You may drop off the form in the Research Service GAC document safe, VAMC, Room E584-1. Place form in envelope.
SRS Assistant:
Location: Commerce Building, 2nd Floor
Tele. Ext.: 6069
Email:
Principal Investigator’s name and lab information:
PI’s Name:
Lab Coordinator(s) Name:
Ext: Email:
Date of Lab Inspection: List all Laboratory RoomNumbers that were Inspected:
Inspector’s information: Print, sign and date the form:
Print Name:
Ext: Email:
Date:
Signature:
NF/SG VHS SRS Laboratory Inspection Checklist (Version: April 1, 2013)
NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYResearch Services: Laboratory Safety Manual Page 131

Determine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Yes No Partial N/A Comments
A. LABORATORY SAFETY - GENERAL If this form reports on more than one room, note room number when reporting findings.
1. The work area is free of unnecessary clutter. Fume hoods and BSC are not used for general storage and have vents/ductwork unobstructed.
2. Carpets and/or rugs are not used in labs or work areas where biological or chemical materials are handled.
3. For rooms equipped with sprinklers, all items on shelves have a minimum vertical clearance of 18-inches from sprinkler heads, heating pipes, and lighting fixtures.
4. Functional fire extinguishers, appropriate for the hazard(s) present, are readily available and unobstructed.
5. Personnel have access to emergency first aid services or kits.
6. Safety showers and eyewashes are located wherever hazardous agents are used.
7. Eyewash and safety showers are tested and results are documented in accordance with facility policy.
8. An occupational noise monitoring program is implemented when potentially hazardous noise exists.
9. Personnel who are required to use respirators have undergone medical evaluations and have been properly trained and fitted for their use. Personnel who are permitted to voluntarily use respirators are provided a copy of 29 CFR 1910.134 Appendix D
10. Use of extension cords is approved by RSC and minimized.
11. Ground fault interrupter (GFI) electrical outlets are used in wet or high risk areas.
12. Compressed gas cylinders are transported on cylinder carts and secured with chains or straps and capped when not in use.
Research Services: Laboratory Safety Manual Page 132

NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
CommentsYes No Partial N/A If this form reports on more than one room, note room
number when reporting findings.13. Hazardous chemical storage is:
a. In properly identified and compatible containers and in a non-flammable storage room OR non-flammable cabinets;
b. Below eye level, but not on the floor;c. Segregated according to compatibility
(flammables separate from oxidizers, acids separate from bases, etc.);
d. Appropriate for flammable liquids (safety cans for volumes greater than 4-L and cabinets for volumes greater than 10-L);
e. Within appropriate cabinetry if flammable or corrosive;
f. In explosion-proof refrigerators when flammable cold storage is required;
g. Monitored for disposal prior to expiration – particularly for peroxide-forming reagents;
h. Examined periodically (at least annually) for replacement, deterioration, and container integrity.
14. All chemical and biological/medical lab wastes are collected and stored in compatible containers. Waste accumulation is minimized and limited to the lab area. Waste disposal is in accordance with federal and state regulations.
15. Spill control programs are in place and may include spill kits.Training is provided when spill kits are available.
16. Controlled substances are properly secured and inventoried.
17. Select carcinogens, reproductive toxins, and substances with a high degree of acute toxicity are handled in designated areas.
Research Services: Laboratory Safety Manual Page 133

NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Yes No Partial N/A Comments18. Eating, drinking, smoking, handling contact
lenses, and/or applying cosmetics are prohibited in all labs and/or areas where chemicals are used.
19. A personal protective equipment (PPE) hazard assessment must be conducted for each lab. (Form available on the Safety Web Page: http://www.northflorida.va.gov/northflorida/research/SafetyCom.asp) A copy of the certified hazard assessment must be maintained in each laboratory. All employees working in the lab must be trained in the PPE required for use in the lab.
20. PPE must be provided, used, and maintained in accordance with OSHA requirements and facility policies, (i.e., removal prior to leaving work area, cleaning and laundering, training, maintenance & care).
B. BIOSAFETY (BSL) 1 AND ANIMAL BIOSAFETY LEVEL (ABSL) 1 LABORATORIES
Standard Microbiological Practices If this form reports on more than one room, note room number when reporting findings.
1. The Lab or Animal Facility Director (PI if nonexempt rDNA) controls access to labs or facilities in accordance with local institutional policies.
2. Personnel are trained to follow safe work practices such as:
a. Hands are washed after work with cultures, glove removal, & before exiting the lab area.
b. Eating, drinking, smoking, handling contact lenses, and/or applying cosmetics are prohibited in all labs.
c. Mouth pipeting is prohibited and mechanical devices are used.
d. Procedures minimize potential splashes or aerosols.
e. Policies for the safe handling of sharps are enforced.
Research Services: Laboratory Safety Manual Page 134

NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Comments
Yes No Partial N/A If this form reports on more than one room, note room number when reporting findings.
f. Lab equipment and work surfaces are decontaminated at the end of the day and after any spill or splash.
g. Laboratory cold storage is not used to store food items for personnel.
3. Insect and rodent control programs are in place.
Safety Equipment (Primary Barriers)4. 5. Lab coats, gowns, or uniforms are worn to
minimize contamination of street clothes. No open-toed shoes or sandals are permitted.
5. Disposable gloves are available - specific types based on risk assessment.Reusable gloves (utility, autoclave, cryogenic, etc.) may be needed and must be maintained in a clean and sanitary condition.
6. Eye protection is provided and used for work that may involve splashes of hazardous materials.
Facilities (Secondary Barriers)7. Labs have doors.
8. Labs/facilities have a sink available for hand-washing.
Research Services: Laboratory Safety Manual Page 135
NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Yes No Partial N/A Comments
C. BIOSAFETY LEVEL (BSL) 2 AND ANIMAL BIOSAFETY LEVEL (ABSL) 2 LABORATORIESAll standard microbiological practices, safety equipment, and facility requirements for BSL/ABSL-1 apply in addition to the following:
Standard Microbiological Practices If this form reports on more than one room, note room number when reporting findings.
1. Lab Director ensures personnel receive initial training on the potential hazards of specific agent(s) and annual updates or additional training as needed.
2. The Lab Director ensures lab personnel are proficient in applicable biosafety procedures.
3. Contaminated materials are placed in properly labeled containers that prevent leakage during collection, handling, processing, storage, transport, disposal, and shipping.
4. Potentially contaminated waste is decontaminated by an approved method before disposal.
Safety Equipment (Primary Barriers)5. BSCs are properly maintained and used for
lab procedures involving:a. Aerosols and/or splashes; orb. High concentrations and/or large volumes of infectious agents. Note: Current certification is a maintenance indicator.
6. Appropriate personal protective equipment (PPE), as determined by risk assessment, is used and left in the laboratory area before exiting.
Research Services: Laboratory Safety Manual Page 136

NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Yes No Partial N/A Comments
Facilities (Secondary Barriers) If this form reports on more than one room, note room number when reporting findings.
7. When appropriate, biohazard signs are posted with the following information:a. Agent(s) in Useb. Biosafety Levelc. PPE and Immunization requirementsd. PI and Lab Supervisor’s Name with
contact informatione. Entry and Exit procedures
8. Lab doors are self-closing with locks that conform to local institutional policies.
9. Lab is constructed and equipped to facilitate cleaning and decontamination.
10. BSCs are located away from doors, windows that open, and heavily traveled areas.
11. Adequate illumination is provided to minimize reflections and glare that impede vision.
12. Bench tops are impervious to water and resistant to damage by moderate heat and/or chemicals.
13. Lab furniture is covered with a non-fabric material that can easily be decontaminated.
Research Services: Laboratory Safety Manual Page 137

NF/SG VHS-SRS LABORATORY INSPECTION CHECKLIST FOR RESEARCH SAFETYDetermine whether the following items are appropriately and sufficiently implemented in the laboratory and mark either “Yes,” “No,” “Partial,” or “Not Applicable.” Use the final column for your comments/suggestions if any to improve laboratory safety.
Yes No Partial N/A Comments
Lab Specific Practices If this form reports on more than one room, note room number when reporting findings.
14. Lab Director (PI if nonexempt rDNA) is responsible for assessing lab-associated risk(s) and establishing entry/exit requirements for personnel.
15. Lab Director incorporates biosafety procedures into lab SOPs or utilizes a lab-specific research biosafety manual.
16. Lab personnel receive appropriate immunizations and/or clinical testing for agents of concern.Note: Medical surveillance program is based on risk assessment.
17. Baseline serum samples are collected and stored for all at-risk personnel, as appropriate.
18. The lab and lab equipment are routinely decontaminated in accordance with applicable local, state and/or federal regulations and articles are contained or decontaminated prior to removal from the facility.
19. Incidents involving infectious materials are:a. Reported immediately to the Lab Director;b. Followed by medical monitoring and
appropriate care of personnel at risk; andc. Documented by a written report or record.
20. Animals and plants not involved in research cannot enter the laboratory.
Research Services: Laboratory Safety Manual Page 138

APPENDIX-AABSL Animal Biosafety Level NEC National Electrical CodeACOS/R&D Associate Chief of Staff – Research and Development NFPA National Fire Prevention AssociationAGA American Gas Association NHPP Nuclear Health Physics ProgramAPHIS Animal and Plant Health Inspection Service (USDA) NIH National Institutes of Health (DHHS)ASISTS Automated Safety Incident Surveillance and Tracking System NSF National Sanitation FoundationAWE Annual Workplace Evaluation NRC U.S. Nuclear Regulatory CommissionBMBL Biosafety in Microbiological and Biomedical Laboratories, 5th
EditionOIG Office of Inspector General
BSC Biological Safety Cabinet ORD Office of Research and DevelopmentBSL Biosafety Level OSH Occupational Safety and HealthBSO Biosafety Officer OSHA Occupational Safety and Health AdministrationCFR Code of Federal Regulations OSHP Occupational Safety and Health ProgramCHO Chemical Hygiene Officer PI Principal InvestigatorCDC Centers for Disease Control and Prevention (DHHS) PPE Personal Protective EquipmentCRADO Chief of Research and Development Officer RadSC Radiation Safety CommitteeDHHS U.S. Department of Health and Human Services R&D Research and Development CommitteeDOT U.S. Department of Transportation rDNA recombinant DNA (deoxyribonucleic acid)EPA U.S. Environmental Protection Agency RSC Research Safety CoordinatorEPRP Emergency Preparedness and Response Plan RSO Radiation Safety OfficerGFI ground fault interrupter RSP Research Safety ProgramHEPA High Efficiency Particulate Air SAFE Safety Automated Facility EvaluationIBC Institutional Biosafety Committee SOPs Standard Operating ProceduresL Liter SRS Subcommittee on Research SafetyMCD Medical Center Director VA U.S. Department of Veterans’ AffairsMOU Memorandum of Understanding VHA Veterans Health AdministrationNHPP Nuclear Health Physics Program VISN Veterans Integrated Service NetworkMSDS Material Safety Data Sheets USDA U.S. Department of Agriculture
Research Services: Laboratory Safety Manual Page 139

Research Services: Laboratory Safety Manual Page 140
SECTION XI. ACRONYMS
ACGIH – American Conference of Governmental Industrial Hygienists ACORP – Animal Component of Research Protocol ACOS/R – Associate Chief of Staff for Research AO – Administrative Officer BSC – Biological Safety Cabinet BSL – Biosafety Level CDC – Centers for Disease Control and Prevention CHP – Chemical Hygiene Plan COS – Chief of Staff CPM – Counts per Minute DNA – Deoxyribonucleic Acid DPM – Disintegrations per Minute EH&S – Environmental Health and Safety, Division of, UF ECP – Exposure Control Plan EMS – Environmental Management Services, VA EOC – Environment of Care HRMS – Human Resources Management Service, VA HRPP – Human Research Protection Program IACUC – Institutional Animal Care and Use Committee IBC – Institutional Biosafety Committee, UF LN – Liquid Nitrogen MOU – Memorandum of Understanding MSDS – Material Safety Data Sheets NF/SG VHS – North Florida/South Georgia Veterans Health System NIH – National Institutes of Health OSHA – Occupational Safety and Health Administration PELS – Permissible Exposure Limits PPE – Personal Protection Equipment RACE – Rescue-Alarm-Confine-Evacuate/Extinguish RS – Research Service, VA RSO – Radiation Safety Officer rDNA – Recombinant Deoxyribonucleic Acid SOP – Standard Operating Procedures SRS – Subcommittee on Research Safety TLVs – Threshold Limit Values TWA – Time Weighted Average UF – University of Florida VA – Veterans Affairs VAMC – Veterans Affairs Medical Center VHA – Veterans Health Administration VMO – Veterinary Medical Officer VMU – Veterinary Medical Unit WOC – Without Compensation
Research Services: Laboratory Safety Manual Page 141

Inside – Back Cover

Laboratory Safety Manual Published by:
North Florida/South Georgia Veterans Health SystemResearch Service Office1601 SW Archer Road (151)Gainesville, Florida 32608-1197Tele: 352-376-1611, Ext. 6069Manual Available at: http://www.northflorida.va.gov/northflorida/research/SafetyCom.asp