improved funding for disability support services … funding for disability support services ......
TRANSCRIPT

1
Improved Funding for Disability Support Services and Disability Support Workers
A Report in Support of the Business Case to
the New Zealand Government December
2012
New Zealand Public Service Association
Te Pūkenga Here Tikanga Mahi
New Zealand Disability Support Network
2
Contents
Page
1. Introduction
2. Background
3. Funding
3.1 Funding challenges for providers
3.2 Ministry of Health funding
3.3 Funding and wages
4. The workforce
4.1 The evolution of the disability support workforce
4.2 The disability support workforce today
4.3 Working conditions
4.4 Staff satisfaction
4.5 Pay Rates
4.6 Skills and Qualifications
4.7 Turnover
4.8 New Zealand disability support workers – some comparisons
5. Future directions
5.1 Increasing demand
5.2 New Model for Supporting Disabled People
5.3 Implications for the workforce
6. The change that is needed
6.1 Recommendations
6.2 Costing pay parity
3
4
5
5
6
8
8
8
10
10
12
13
13
16
18
20
20
22
23
25
25
26

3
Improved Funding for Disability Support Services and Disability Support Workers: A Report in Support of the Business Case to the New Zealand Government
1. Introduction
This business case has its origins in objective 4.5(c) of the Disability Workforce Action Plan:
Prepare business cases to increase funding for the disability support workforce using objective
evidence such as studies commissioned by unions and provider groups as key sources of data1
There has been a growing concern over the last decade or so about the sustainability of the disability
support workforce, particularly the ‘unregulated workforce’ - disability support workers. This workforce
has been characterised as:
predominantly female
low paid
mainly unqualified
having limited access to suitable training
part time
susceptible to high turnover
a source of potential labour for other low-paid occupations
without career pathways2
This growing concern has also reflected wider issues about the provision of quality disability support
services, which culminated in the Social Services Select Committee initiating an inquiry into the quality
of care and services for people with disabilities. The select committee reported in 2008 and it included
recommendations about the workforce.
The action plan assigned priorities to workforce development for 2009-2014 that aligned with the New
Zealand Disability Strategy, which is a government-wide, long-term plan based on a vision of a society in
which people with disabilities are able to fully participate. Timing meant that the workforce action plan
became part of the response of the government to the report of the select committee.
This business case explores in some detail the challenges that call into question the sustainability of
disability support workforce. It outlines the background to how disability support services have evolved
and how we have ended up with the disability support workforce we have today. It sets out the current
funding and workforce issues and the future demands and policy directions that will shape the disability
workforce of the future.
The business case is aimed at services funded through the Disability Support Services (DSS) of the
Ministry of Health. Home support services (funded by District Health Boards (DHBs) and ACC) and
vocational services (funded by the Ministry of Social Development (MSD)) fall outside the scope of this
paper. The problems they face are of a similar magnitude to those addressed here but the many sources
1 Ministry of Health, Disability Support Services Workforce Action Plan, p.30
2 Ibid. p. 10

4
of funding and the unique features of those sectors make it too complex to adequately deal with their
needs in this paper.
This business case concludes that, while progress has been made, the fundamental characteristics of the
workforce as outlined in the Disability Workforce Action Plan, still remain. The action plan identified a
number of objectives that need more funding and this business case makes the case that we will not
achieve all that we want to achieve in disability support services, unless there is a commitment to a
substantial investment in the disability workforce and clear timeframe for achieving that.
2. Background
The 2006 national disability survey indicated that around 660,300 or 17% of New Zealanders report that
they have a disability3. In 2006, 82 percent of people with disability were adults living in households, 5
percent were adults living in residential facilities and 14 percent were children (under 15 years) living in
households. The percentage of people with disability increased with age, from 10 percent for children
aged less than 15 years to 45 percent for adults aged 65 years and over. Nearly all adults living in
residential facilities reported having a disability (99.7 percent) and most had multiple disabilities (94
percent) and high support needs (82 percent).4
Approximately 33,700 (5% of those with disabilities) reported an intellectual disability5, which is
comparable to the figure of 31,847 taken from the Ministry of Health’s databases for the Ministry’s 2011
study on the prevalence of illness among people with a disability. However, in 2006 IHC estimated that
there were over 50,000 people with an intellectual disability living in New Zealand6 and the 2011
Ministry of Health study, using the ‘capture–recapture’ statistical method, estimated that there were
actually an additional 14,817 people with intellectual disability in the study population, giving a total of
46,664 people. 90% of the Ministry of Health’s adult residential facilities were coded as intellectual
disability in 2008.7 This business case is about the funding of disability support workers working for
providers funded by the Disability Support Services of the Ministry of Health, who are mainly involved in
working in support of those with an intellectual disability.
3 Statistics New Zealand, (2007) “Hot off the press” 2006 Disability Survey Report – source for all the following data
4 Ministry of Health. (2011) Health Indicators for New Zealanders with Intellectual Disability. Wellington: Ministry of Health. P.8. Note that the definition of intellectual disability in this study is likely to be a little broader than that in the 2006 Disability Survey Report because of the data used.
5 http://wdmzpub01.stats.govt.nz/wds/TableViewer/tableView.aspx?ReportName=Disability/Adults with disability, by
disability type, age-group, sex and place of residence, 2006
6 IHC, (2008) cit. Bonardi, A. (2009), The Balance between Choice and Control: Risk Management in New Zealand
Intellectual Disability Services, Fulbright New Zealand
7 Conversation with Rob Gill, Ministry of Health (18 August 2009), reporting on discussions of funding allocations under
the Leadership Development Scheme in 2008.

5
In the 1990s the structure of disability support services as we now know it, was begun to be put in place
as part of the general move to de-institutionalisation and the overall reform of the health and disability
system along market lines. Funding for disability supports was shifted from the Department of Social
Welfare to the Ministry of Health. The Disabled Person’s Community Welfare Act had established a
statutory right to services and the health and disability reforms replaced this with a model in which
there was a limit on funds.
As a result, rationing, and prioritisation became very real features of the service model, and valid
methods of assessing need and support available became essential.8
This was reflected in the Disability Support Services Framework, which included a model in which needs
assessment and service co-ordination were separate from service provision.
A competitive environment was established in health and disability services and new providers were
encouraged to compete for service contracts from the Ministry of Health. The reforms promoted
greater consumer choice, which accorded with the aims of disability advocacy groups, while establishing
a means of managing costs and driving efficiencies.9
With the establishment of the District Health Boards in 2000, which was accompanied by the devolution
of funding of health services from central government to the DHBs, disability support services funding
(for those aged under 65) remained with the Ministry of Health. Other funders of disability services
include the Accident Compensation Corporation and the Ministry of Social Development.
In recent years a number of significant reports and strategies have had an influence on how services for
people with disabilities are delivered. Most important of these was the New Zealand Disability Strategy
2001 and To Have an Ordinary Life 10, which was produced by the National Health Committee in 2003.
3. Funding
3.1 Funding challenges for providers
Most providers supply services to a range of groups and in different settings. Home support for those
with life-long disabilities and over 65s; residential support for those with life-long disabilities and over
65s; and respite and day services for those with life-long disabilities and those aged over 65. This
means that they may receive funding from several different sources, particularly if they provide services
in different district health board areas. DHBs fund most home support services and services for over 65s.
8 Bonardi p, 12
9 Ibid p. 13
10 National Advisory Committee on Health and Disability (2003), To Have an ‘Ordinary’ Life: Community membership for
adults with intellectual disability. A report to the Minster of Health and the Minister of Disability Issues, Wellington,
National Health Committee

6
They also fund mental health services and some providers deliver services to people with mental health
issues as well as those with disabilities. Residential support and home support for those with life-long
disabilities are funded through the Ministry of Health Disability Services. Some providers are also
providing supported vocational services which are funded through the Ministry of Social Development.
The inconsistency in funding arrangements can be frustrating and can incur significant administrative
and compliance costs. The inconsistency can also be passed on to workers in variable pay and
conditions, depending upon the contract they are working under.
Within the overall Ministry budget, funding of providers has been ad hoc and inconsistent. There is as
yet no standard and consistent approach to funding disability support providers. Overall there is a
consistent set of service specifications (which sets out the service expectations) that applies to all
providers, but this operates in the historical context of funding to each provider.
One of the variables is the legacy from the previous Regional Health Authorities, which funded providers
on a different basis across the country, reflecting such regional variations as the different approach of
local authorities to charging for water. This has not yet worked out of the system.
In addition funding for the major providers has evolved in different ways. For example, IHC (the largest
provider in the country) has been operating under a form of transparent pricing implemented in 2003,
but it does not as yet apply to any other provider. In addition, individual providers facing particular
pressures (such as the likelihood of industrial action over wages) have been able to negotiate extra
funding to head off a crisis.
There are three ways that funding to a provider can increase: the first is when the budget allocates
additional funding - this comes through as a percentage increase in funding (although the percentage
might vary according to provider); the second is when the needs of a person with disabilities increases
and the provider asks for a reassessment to occur. The needs assessment agency (NASC) then
recommends an increase to meet these needs. Assessments are supposed to take place on a regular
basis. The third is when the numbers of people supported by the provider goes up.
There have been efforts to reform the process of funding through the establishment of a transparent
pricing model that would put all providers on the same basis, but so far it has proved too difficult to
achieve. One of the reasons is that the model has struggled to get consistency in application across the
various NASC agencies around the country. Assessors have to use their judgement and this inevitably
leads to variation.
3.2 Ministry of Health funding
The Ministry of Health has been allocated $1.028 billion dollars in the 2011/12 budget for disability
support services. This represented extra funding of around $32.5 million from 2010/11, representing an
underlying price increase of 1.5% for most services. However in some areas there was additional funding
to meet specific needs or rising costs. For example, as the table below indicates, the biggest increase
within Disability Services came in Environmental Support Services, largely because of the significant
increase in the price of equipment over recent years.

7
The budget allocation for 2011/12 is up from around $880 million in 2008/9, representing an increase of
around 16.8% over that period. This is comparable to DHB funding which increased by 16.22% over the
same period.
The main areas (and amounts) of funding provided through Disability Services from 2004/05 to and
2010/11 were11:
‘Residential services’ is the most significant budgetary item. Over the period in question the increase in
total DSS expenditure has been 66% compared to 63% for residential. These increases appear to have
occurred mainly prior to 2009 and tended to taper off since then. Since the budget additional funding
has been provided to meet the costs of the sleepover case. The unions had successfully pursued a case
through the Employment Court arguing that sleepover shifts constituted work and that they should be
remunerated at the minimum hourly wage rather than by way of an allowance. The government agreed
to pay $27.5m towards the costs of back pay claims (at 50% of the cost of claims) and to contribute up
to $90million over three years to support employers as they phase in the minimum wage for sleep over
shifts12.
While these increases over the period from 2004 appear to be reasonable, they have not addressed the
problem of underfunding in the sector:
they have tended to be absorbed by growing numbers or increasing complexity of need13, rather
than wages as reflected in the outcome of collective bargaining
11
Figures provided by the Ministry of Health, June 2012
12 http://www.beehive.govt.nz/release/sleepover-wages-settlement-bill-be-introduced
13 The extent of this problem is difficult to identify because the Ministry has stated that they cannot distinguish between
general price increases ad rate increases due to review/reassessment of client packages (e-mail from Sanjeev Malhotra to
Chris Harris, 28 October 2009)

8
they have not compensated for the lack of investment during the 1990s following the move to
de-institutionalisation14
they have tended to address one-off issues such as the sleep-over case, rather than systemic
issues
3.3 Funding and wages
Disability support work is low paid even though we argue (see below) that the work is highly skilled. In
1999 Burns et. al. identified some factors contributing to low wages in a related sector: labour market
segmentation, the role of the government as funder, and contract definition15. These factors are
relevant to disability residential support as well, due to the similar profile of the workforce and
dependence on government funding. While there have been structural changes since 1999 the funding
relationships that Burns et. al. describe are fundamentally the same.
They suggest that although labour market segmentation (workers who have few job options because of
discrimination and/or personal circumstances tend to be come concentrated in low paid and unstable
industries) contributes to low wages, the role of government in regulating and funding the sector may
be a more important factor16. The dominant position of funders like the Ministry of Health, which are in
turn constrained by the resources granted through Vote Health, means that they are able to set prices
and develop contracts in a way that limits the ability of providers to offer better pay and conditions.
Providers also tend to develop employment practices that reflect the requirements of their contracts.
The close link between the role of government as funder and regulator, and the wages and conditions of
disability support workers means that the only way wages will improve is if the government increases
funding.
4. The workforce
4.1 The evolution of the disability support workforce
With the increase in institutionalisation from the 1940s onward there developed greater recognition of
the need for adequate staffing and adequate training for staff. In the 1960s occupations for the care of
people with intellectual disabilities were being described in terms of providing diagnosis, care and
14
Funding for DSS for the period prior to 2004/5 also included older people disability support services so it is difficult to
disentangle the funding for over 65s from that for younger disabled people. However, providers report that they received
no funding increases for the period 1990-2001
15 Janice Burns, Maire Dwyer, Huia-ngarangi Lambie and Jo Lynch, Homecare Workers: A case study of a female
occupation, Ministry of Women’s Affairs, 1999 pp 20-21
16 Ibid pp. 21-22

9
rehabilitation. 17 Better staff:patient/resident ratios and better training were introduced for medical,
therapeutic and safety reasons.
For example, at the Kimberley Centre there was not only an on-site School of Nursing for the training of
psychopaedic nurses, but also a National Training School that ran course for training officers who
worked alongside those nurses. However, the former was disestablished in 1991 and the latter in 1989
so that by the time that Kimberley closed in 2006 a substantial proportion of the staff were untrained
and unqualified18. This was representative of the running down of training capacity within disability
support.
While much of the training of staff in the institutionalised model reinforced the paternalistic and
medical models of care, it was replaced with very little for staff who worked in the support of people
with disabilities from 1990 onwards. Training was substantially left up to employers whose response to
the challenge has been variable. As the PSA said in its submission to the Social Services Select
Committee Inquiry:
The move to community based services required a higher level of autonomy from support staff and
therefore a higher level of expertise and skill but paradoxically the shift has been characterised by
reduced access to training, reduced levels of supervision, and reduced access to peer support and
expert advice19.
Until we can reintroduce professional training that is recognised across the sector, increasing wages for
support workers will be difficult.
Qualified staff, directly employed by the state, have historically been able to maintain fairer wages and
conditions than those in contracted out services. Since the model of support has changed with de-
institutionalisation, pay and conditions for disability support workers (who have become the
predominant workers in the sector) have slipped well behind equivalent workers within the DHBs. This
reflects the pressures of the market model of funding for disability support services:
It could be argued that the government model to promote marketplace pressures (competition)
was only prepared to devolve risk to the level of providers because of the accountability and
control that it could exert as the major funder. Without an ‘industry’ or ‘programme’ that includes
monitoring accountable to the funder, it is difficult to ensure accountability of government funds20.
This distance between the funder and the provider thus enables the government to distance itself from
the effects of its decisions about funding levels, including the wages and conditions of the workers.
17
Gates, S.(2008) The Impact of De-institutionalisation on the Staff of the Kimberley Centre, Dunedin, Donald Beasley Centre p. 3
18 Ibid p. 9 The staff at the Kimberley Centre at the point of closure included management and administration staff,
registered nurse educators, registered Nurses, enrolled nurses, ‘psychopaedic’ nurses, psychopaedic assistants, and a range of maintenance staff. 19 NZ Public Service Association Te Pūkenga Here Tikanga Mahi, (2006) Submission to the Social Services Select Committee Inquiry into the quality and care of service provision for disabled people and how they might be improved p.4 20
Bonardi, p. 14

10
4.2 The disability support workforce today
Data from the Ministry of Health’s Quality and Safety Project in 2004 suggested that, at that time, the
support workforce funded by Disability Services in the Ministry of Health was somewhere between
19,000 and 22,000 workers, with an overlap between home-based and residential services of
approximately 7%21. Figures from the National Residential Intellectual Disability Providers’ survey of
salaries and wages in 200722 suggest that the figure is probably somewhat lower than that. The author
extrapolated from the returns from 32 of the 48 providers, that the total figure for staff employed in
community residential services was 13,500 - comprised of 7,400 fte, 4,100 pte and 2,000 casual staff.
Residential services employ by far the largest proportion of the workforce funded by DSS with others,
such as supported living, only employing a small number of workers. Putting together this figure with
anecdotal reports from providers of a growing workforce, plus the small number of workers employed in
other DSS funded services, we have assumed a total DSS funded workforce of approximately 15,000 fte.
The Auckland University study for the Quality and Safety Project identified that disability support
workers were typically female (93%) and middle aged (76% were aged 40-69)23. The gender split
contrasts with that applying at Kimberley for example, where of the 349 staff there just prior to closure,
61% were male and 39% were female24. The gender shift suggests that the move to a largely unqualified
workforce was co-incidental with a shift to a female dominated workforce.
A study by the Donald Beasley Institute25 into the residential disability workforce conducted between
2008 and 2010 reported that of those support workers who responded to the survey 69% were
European, 15.9% were Māori, 3.1% Pasifika, 1.7% were Indian and 0.6 were Chinese. 9.2% were other or
not known. Around 75% of respondents were female, a third were aged 45-55 years and two thirds of
were due to reach the age of eligibility for New Zealand superannuation within 20 years. 5.8% were
aged over 65.
4.3 Working conditions
The work of disability support workers is often difficult and demanding, although immensely rewarding.
The conditions under which they work are often substandard and place them, and those they work with,
21
Chal J. (2004) Disability Support Services in New Zealand: The workforce survey, Wellington, Ministry of Health cit.
Ministry of Health (2009) Disability Support Services Workforce Action Plan p. 11
22 Grant B. (2007) National Residential Intellectual Disability Providers Salary and Wage Survey Report. Hamilton, Opinion
Research p. 3
23 Chal cit. Ministry of Health Paper prepared for Low Pay in Aged Care and Disability Sector meeting 16 February 2007
24 Gates, p.8
25 Nancy Higgins, Paul Milner, Sue Gates, Brigit Mirfin-Veitch & Teresa Evans-Turner Working in Intellectual Disability
Services: Staff retention and turnover: a presentation to the PSA, January 2012.

11
at risk. There is a tension that can exist between the residences being the home of the disabled person
receiving support, and also being a workplace.
The study for the Quality and Safety Project found that in 2004 support workers perceived risks to their
safety (55% felt they might get hurt or injured at work) associated with providing personal support,
verbal abuse from those they are supporting, conflict with other workers or issues with management26.
The Donald Beasley study found that 61.6% of staff reported verbal abuse and 47.2% physical assault in
their present job27. This study did not distinguish the source of the verbal abuse, which could have
included other staff.
Evidence in the recent ‘sleepover’ case28 outlined some of the challenges of working as a disability
support worker in a residential setting. Residences require support workers to present at all times. On
average Mr. Dickson spent 71 hours every fortnight out of the 148 worked in total (i.e. an average of
14.8 hours per working day), working sleepovers. The Court found that sleepovers constituted work.
Further, in almost every shift he began sleepovers after a shift of normal work from 4pm – 10pm.
This is consistent with evidence from the Donald Beasley Institute study that 75% of respondents
worked more than 12 consecutive hours in the week prior to completing the survey. Between 40-60
hours (including sleepovers) was the most commonly reported consecutive hours worked in the week
prior to completing the survey29.
Other evidence presented in the sleepover decision demonstrated various aspects of the work. Support
workers in sleepovers had to be alert to activities or noises in the house and are often awoken, resulting
in disrupted sleep30. Some work ‘wakeover’ shifts, where workers are required to remain awake for
periods of 8 to 10 hours from 10pm because of the particular needs of those they are supporting31. Shift
work is a well-documented cause of workplace fatigue32. The room Mr. Dickson used for sleepovers
doubled as a staff room and office during the day, indicating often cramped and difficult working
conditions.
The study by the Donald Beasley Institute33 found that the providers involved with the survey reported
8% of staff were employed on a casual basis. 58% were full time and 34% were part time.
26
Chal, Workforce Survey, p. 86
27 Higgins et. al.
28 Idea Services Ltd. v Phillip William Dickson WN WRC 31/08 & 34/08 [8 July 2009]
29 Higgins et. al.
30 Idea v Dickson [24]
31 Ibid para[26]
32 http://www.dol.govt.nz/infozone/businessessentials/safety/hazards/workplace-fatigue.asp
33 Higgins et. al.

12
Casualisation is also a risk to service quality. In a Victorian disability workforce report in 2009, reliance
on casual staff could result in high induction costs, inconsistency in the induction experience and
discontinuity of support for people with disabilities34. A 2008 report to Disability Services Queensland
said that reliance on casual staff “presents as a service delivery risk and runs counter to the very nature
of the (complex) work that casuals must perform, often at short-notice and in unfamiliar surrounds”35.
4.4 Staff satisfaction
Notwithstanding the challenging working conditions, job satisfaction among disability support workers is
high. In the Donald Beasley study 75% of respondents reported at or above the neutral point of
agreement to the statement; “I am satisfied with my job”. Older staff reported higher levels of job
satisfaction. The least satisfied staff were aged between 25-55years36.
Staff satisfaction appears to be related primarily to the nature of the work. The satisfaction of working
with people who need the support provided. The Donald Beasley study37 provides real insight in the
commitment of those working in residential support. Job satisfaction seems to come from advocating
for those they are supporting, rather than from the agency itself. The longer that workers were
employed by the same agency the more importance this advocacy role appeared to assume.
Workplace conditions also impacted on job satisfaction. Being physically assaulted had a negative
impact on factors contributing to satisfaction, but much depended on how the agency responded. Those
that responded in a procedural or impersonal way to reports of assault tended to undermine workers’
satisfaction with the job, whereas those that responded in a personal supportive way helped
satisfaction. 22.9% of support worker respondents reported that their agency had been of little or no
help when they reported verbal or physical abuse.
The longer the length of service with a single employer also appeared to contribute to staff being less
satisfied with their work. One of the important factors here was that they had reached the top of the
salary scale, usually with little opportunity to progress. Staff on casual contracts also reported less
satisfaction than those on permanent employment arrangements (although some staff employed on
casual contracts, such as students, liked the flexibility of being able to turn down work).
The level of qualifications also affected level of job satisfaction. Those with higher qualifications tended
to be less satisfied, whereas people who had a certificate or diploma in human services were on average
more satisfied.
34
Cit. Teresa Iacono ‘Addressing increasing demands on Australian disability support workers’, Journal of Intellectual and
Developmental Disability, December 2010, 35(4) p.291
35 Ibid.
36 Higgins et. al.
37 Ibid. The following data is all taken from the Donald Beasley study.

13
4.5 Pay rates
Disability support workers are low paid workers. A recent survey by the NZ Disability Support Network38
reveals rates of pay in Ministry of Health DSS funded services that have an average minimum wage of
$15.00 an hour with a maximum average wage of $18.50 an hour. The weighted average was $16.36 an
hour. The lowest reported salary paid by providers in the survey that generated these figures is the
minimum adult wage of $13.50 (as at 1 April 2012). By comparison the average wage is $25.42 an hour
(as at 31 December 2011). The PSA job evaluation, cited in 4.8 below, identified that the work of
disability support workers was comparable with therapy assistants and corrections officers, while the
pay gap at the top end of the respective salary scales was 22% with therapy assistants and 52% with
corrections officers.
By comparison the minimum adult wage is $13.50 (as at 1 April 2012) and the average wage is $25.42 an
hour (as at 31 December 2011).
In the Donald Beasley study (in 2010) the average usual hourly rate for respondents was $15.53, while
the average usual hourly rate for staff that had worked for less than 1 year was $14.45. The study also
found that the usual hourly rate, on average, increased by $0.16 for every year staff worked39.
These are not decent rates of pay and nor are the annual movements significant. As has been pointed
out earlier, when disability services were provided by the state (rather than just funded) wages were
relatively higher than they are now - yet the job has become more demanding for support workers. This
reflects the market developed in the disability sector in the 1990s, which meant that wages were driven
down by providers in response to the pressures of the contracting regime. It also reflects the
feminisation of the workforce (where the skills of women are valued less than those of men40) and a
devaluing of the disability sector - both workers and people with a disability.
4.6 Skills and Qualifications
Providing appropriate disability support is complex and challenging work and must meet the individual
needs of people. The focus is on a support role i.e. working with people with disabilities in a
developmental way to enable them to live as full a life as possible, rather than on a purely caring role.
This is consistent with the social model of disability support.
Disability support workers need a wide range of skills including problem solving, physical dexterity,
being observant to changes in behaviour or wellbeing and judging how best to respond (as well as
38
Brief summary of support workers data Communication from NZDSN, Nov 2012
39 Higgins et. al.
40 See the comparison between disability support workers and corrections officers below.

14
reporting on this). They do this with less professional support than was available to their predecessors in
the large institutions – they have a high degree of autonomy.
Some people requiring support have dual diagnosis (mental health and intellectual disability), others
have sensory and/or physical disabilities as well as an intellectual disability. Some exhibit extremely
challenging behaviour, others require minimal assistance to live independently in the community.
Others are medically fragile and/or technology dependent.
All require and deserve high standards of support to live as full a life as possible. Providing the support
required for the individual needs of people is complex and challenging.
The need for improving the level of qualifications and training in the sector has been recognised for
some time. Disability support workers do not necessarily need any pre-entry minimum level of training
to enter the disability sector. On-the-job training and induction is provided by just about all providers of
disability support services but the Quality and Safety Project survey in 2004 suggested that there was
significant room to improve the knowledge and skills of disability support workers41. The Ministry of
Health’s response was the Disability Workforce Action Plan in 2009 which was established with the aim
of providing career paths for the disability support workforce to improve the status of disability support
work.
There is evidence that in 2004 about 55% of support workers in residential services had sufficient and
recognised training42. This indicates a significant qualifications gap. Since then the amount and quality
of training has increased. In 2010 1,849 people from 49 organisations were approved training grant
funding, with nearly 60% of those coming from four large organisations. More than half of the
participants were completing the National Certificate in Community Support Level 2 Foundation Skills
and 37% Level 3 Core Competencies qualifications. Employers reported that training had had a positive
impact on participants and that it contributed to reduced turnover and improved practice and service
delivery. In addition 1,989 individuals from 31 organisations received funding for short courses43.
The Donald Beasley study found that at the time they conducted their survey, 26.1% of staff reported no
secondary school qualification, while 47.9% reported having a tertiary qualification (including the 17.5%
of staff who reported having completed a Human Services Diploma or Certificate)44.
A survey of providers of residential disability support services conducted for Careerforce by the New
Zealand Disability Support Network (NZDSN) in 2010 indicated that providers were keen to promote
41
Chal
42 Te Pou, Disability Support Services: workforce training needs and barriers, Mar 2011, p. 13
43 Te Pou, Disability training and open round grants: 2010 outcomes, pp.3-4
44 Higgins et. al.

15
learning and development opportunities for their staff45. 81% of those providers had staff undergoing
study towards a qualification, with the majority working towards certificate level qualifications.
There seemed to be a large gap of skill and expertise both between staff within organisations (where
many respondents advised that there was a need to build literacy and use of English, where English was
not the first language of the workforce) and between organisations. Larger organisations backed by an
appropriate infrastructure had the ability to invest in resources such as technology that can reduce
future training costs, whereas smaller providers did not have this same capacity.
Although considerable progress had been made in increasing the number of workers with qualifications,
it had been at levels 1-3. The government will not be increasing funding at these levels unless it assists
students to higher level learning or employment46.
There is also a question about whether existing qualifications are meeting workforce needs. Only 16%
of residential providers agreed that current qualifications were meeting their needs47. They were either
awaiting further development tailored to their needs or found that they had to provide a large amount
of training from within their organisations. This, of course, is a challenge for smaller organisations.
These findings indicate that while good progress has been made the majority of qualifications are still at
the lower end of the spectrum and there are still many without any qualifications in the sector. While
feedback to Te Pou indicates that providers are reporting a positive impact on outcomes for people with
disabilities through staff training and gaining of qualifications, the NZDSN survey suggests that many are
still unhappy about content and delivery.
Another issue is thrown up by the work by Anne Junor and others, which suggests that disability support
work requires skills that may not be reflected in the traditional skills hierarchies in health and disability.
These are based mainly on technical knowledge and qualifications, but in disability support work other
high-level skills are required beyond instrumental or bodily care. Junor looks at the other skills required
in what could be called a ‘social’ model of care:
…the skills required by this ‘social’ model include interactive or emotion management skills,
cognitive skills of shaping awareness, skills used to shape long-term support relationships, and
co-ordinating skills. These skills appear to be underspecified in qualifications and job
descriptions. Firstly they need to be recognised as skills, not as ‘natural’ attributes, and
secondly there is a need to recognise how they develop to higher levels in the workplace,
through a progressively deepening capacity for reflective problem-solving in shared activities48.
45
NZ Disability Support Network, Sector Skills Strategy for members of the New Zealand Disability Support Network,
commissioned by Careerforce, January 2011 pp. 4-6
46 Ibid. p. 9
47 Ibid. p. 5
48 Anne Junor, Ian Hampson, and Kay Robyn Ogle ‘Vocabularies of Skills: The Case of Care and Support Workers’, in S.
Bolton and M. Houlihan (eds) Work Matters, Palgrave, London, 2009
16
Junor et. al. are referring to the work of care and support staff working mainly in rest homes, but these
conclusions are even more applicable to disability support workers who, because of their greater degree
of autonomy and the changing nature of disability support services, require even more advanced skills.
Junor was also involved in the development of the Spotlight skills recognition tool49 with the Pay and
Employment Equity Unit of the Department of Labour, which sought to identify and recognise the
contribution of these invisible skills. There is scope for this tool to be applied in disability support
services to illuminate the range and depth of skills required by support workers.
4.7 Turnover
There is a recent history of very high turnover in the disability sector. In 2004 turnover was 29%50 in
residential support (aged care and disability) and the median length of employment was 24 months. The
National Residential Intellectual Disability (NRID) providers group reported that their staff turnover in
2007 was 22% on average and 28% in 2006.51 The Donald Beasley study reported turnover of 17.8%52.
One of the large residential providers reports turnover rates of 24.32% in 2009, declining to 18.89% in
2012 for the year to date53.
All these results suggest a declining turnover rate, most likely due to the impact of the recession. The
HRC found that aged care employers, providers (including home support) and funders all predict that as
unemployment trends down over the coming years, supply and turnover difficulties will intensify
again.54 We expect the same to be true of residential disability services.
The literature suggests that turnover in disability support is an international problem and one that is
described as chronic.
Employee turnover in human services organisations is a chronic and extensive problem
adversely affecting the provision of care as well as taxing highly constrained budgets55.
High turnover contributes to the staff shortages in the sector. It is not uncommon for support workers
to work long hours in order to cover when there is not enough staff for each shift. Union delegates
49
http://www.spotlightworkskills.com/uploads/81857/files/166867/ResearchReportandBibliography.pdf
50 Chal, Workforce Survey, p. 86
51 Grant B. (2007) National Residential Intellectual Disability Providers Salary and Wage Survey Report. Hamilton, Opinion
Research cit. Ministry of Health, Disability Services Workforce Strategy and Action Plan (Final Draft October 2008) p. 13
52 Higgins et. al.
53 Reported by NZDSN
54 HRC p. 27
55 Razza, N. J. (1993). Determinants of direct-care staff turnover in group homes for individuals with mental retardation
[published erratum appears in Mental Retardation 12/93;31(6):402]. Mental Retardation, 31, 284-291. Cit. Higgins et. al.

17
report that members work long hours (100-110 hours a fortnight) which is unsafe but understandable
given the workforce shortages.
High turnover also acts as a disincentive to invest in staff development and training which will have an
impact on quality of support56.
The apparent decline in turnover as a result of the recession does not mean that the problem has been
solved. If people are staying in the job when they really want to move on, it is likely to make for a more
unhappy workforce, with implications for quality of service. A sustainable solution is needed, that
addresses wages and conditions.
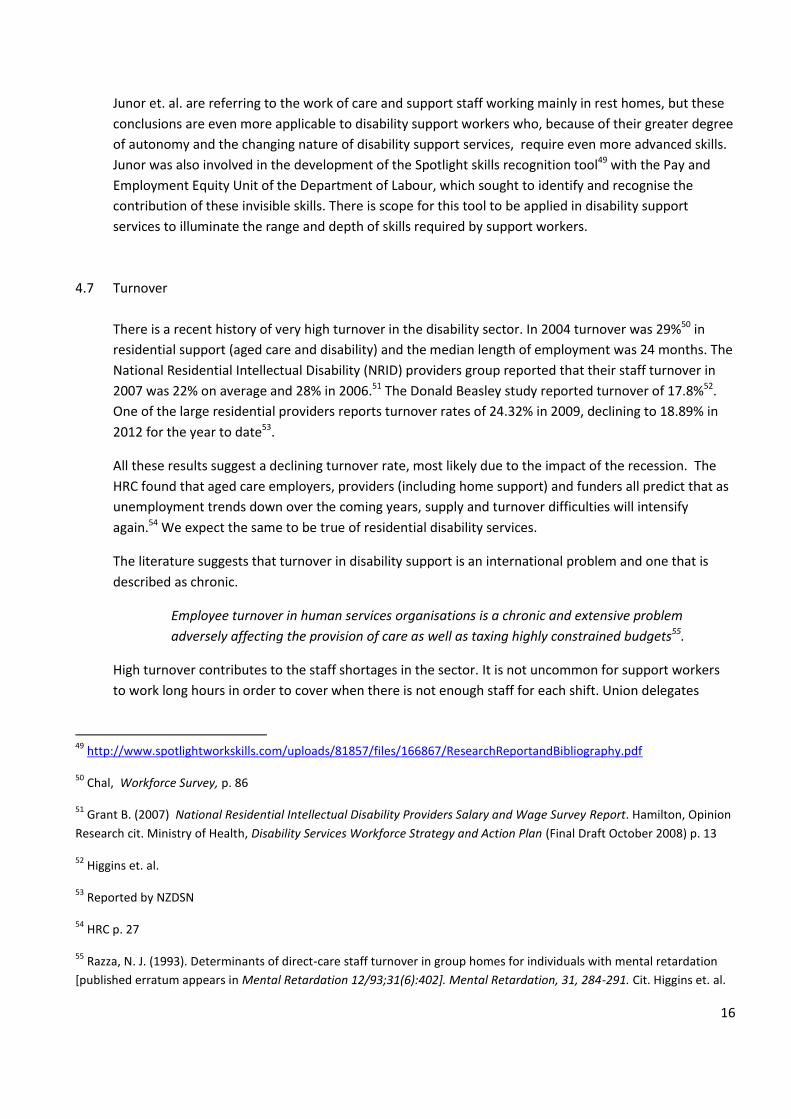
The Donald Beasley study produced some interesting analysis around turnover in residential services.
For example, most of those who left were young (see table 1), while Almost 30% of staff who reported
working for less than 1 year had left an agency at the time of a follow-up 18 months later.
Table 1: Percentage Turnover by Age Category
No association was found between: sex, pay, work hours, number of sleepovers, type of service or
whether staff had a Certificate in Human services and the likelihood they would leave. However, staff
who were on a fixed roster or reported having reliable hours were less likely to leave. The study also
found that the more emotionally exhausted staff were also the more likely they were to leave their
support service57.
The higher incidence of turnover among the young, and those with less service suggests that the job of
disability support worker is not seen as a career and that there are other competing jobs or careers that
make it difficult to retain staff. On the other hand the association of emotional exhaustion with leaving,
suggests that this could be one of the main reasons that older workers may leave the service when they
do go.
56
HRC p. 24
57 Higgins et. al. The authors identify three factors as evidence of burnout: low levels of personal accomplishment, high
levels of emotional exhaustion, and depersonalisation or low levels of empathy
0
20
40
60
80
100
17-24 25 - 34 35 - 44 45 -54 55 - 64 65+

18
Pay is therefore important as part of a career service. It is also important (as the Donald Beasley study
also found out) as a totem of the overall undervaluing of the workforce. Pay is therefore an important
part of the solution for reducing turnover.
4.8 New Zealand disability support workers - some comparisons
In 2008 to establish the extent to which the work of disability support workers was undervalued the PSA
commissioned a gender-neutral job evaluation exercise, which compared the work of disability support
workers with therapy assistants in hospitals and corrections officers in prisons58.
The Department of Labour Equitable Job Evaluation system was utilised. This system was developed to
provide a job evaluation tool that can fully describe and measure key aspects of all jobs including
previously under described and undervalued aspects of female dominated work. The system was tested
by a working group of job evaluators and equity experts. In order to use the system, the PSA had to
meet the conditions of use set by the Department of Labour, including assurance that the consultant
using the system was fully competent to do so.
Quality control was assured by having job holders and their managers verify that the job information
obtained by the consultant is an accurate and fair representation of the job. In addition, an external
independent consultant validated the evaluation results.
The PSA chose therapy assistants and corrections officers based on the following criteria:
Entry requirements to the occupation - none of the three has mandatory entry qualifications.
Level of occupational classification within the Australian and New Zealand Standard Classification of
Occupations 2005 – the classification indicated the predominant skill level of each of the sub-major
occupational group. All three occupations were described as being skill-level 4.
The level of the professional qualification available to the occupation - after appointment, there are
formal qualifications at equivalent NZQA levels (supported by the employers) available to staff.
Gender occupancy – disability support workers and therapy assistants are both predominantly
female occupations, whereas corrections officers are predominantly male.
The weighted total scores for the three jobs were similar (full report available through the PSA). The
data supports a view that these jobs are of substantially similar value.
At the time the evaluation was carried out the average starting pay for community support workers was
$13.23 an hour or $27,518 a year compared with:
The normal starting pay for therapy assistants of $ 29,266, $1748 more than community support
workers - a 6.4% pay gap.
58
PSA (2008), Community Support Workers: a job evaluation exercise

19
The starting pay for corrections officers of $41,615 a year, $14,097 more than community support
workers - a 51% pay gap.
The average top pay rate for community support workers was $16.20 an hour or $33,696 a year,
compared with:
A top rate for therapy assistants of $41,109, $7413 more than community support workers, a 22%
pay gap.
A top rate for corrections officers (with internal training) of $51,257 a year, $17,551 more than
CSWs, a 52% pay gap.
Using the current PSA data referred to earlier, it appears that the pay gap may have closed, but there is
still gap, and a significant one in the case of corrections officers.
The consultant concluded that therapy assistants and corrections officers were jobs of similar size that
could well end up in the same salary band within the same organisation. She concluded that the main
reason for the differential was probably the ability to pay, because of the funding regime, rather than
recruitment and retention.
The HRC report has called for the Minister of Health to direct DHBs to develop a mechanism to achieve
pay parity between health care assistants working in district health boards and support workers working
in home support and aged care residential facilities. They have recommended this be implemented
within 3 years59.
While the PSA job evaluation provides the basis for comparison with workers doing comparable jobs in
the state sector, there has been a major development in the remuneration of community workers in
Australia – a group that includes disability support workers. Following an application to Fair Work
Australia (FWA) Australian unions, led by the Australian Services Union (ASU) won a decision that
recognises that this group of workers has been disadvantaged in comparison to their colleagues working
in equivalent jobs in the public sector – in commonwealth, state and local government employment.
In their May 2011 decision FWA concluded that:
We agree that it would be wrong to conclude that the gap between pay in the sector with
which we are concerned and pay in state and local government employment is attributable
entirely to gender, but we are in no doubt that gender has an important influence60.
This initial decision included a call to the parties to achieve an agreement on how to implement equal
pay. This led to a joint submission by the ASU and the commonwealth government calling for substantial
increases to the applicable modern awards of between 19% and 41%, to be implemented over an 8 year
period. While debating some of the rationale, FWA has adopted an award wage increase of 23% to
Modern Award Level 2 and 26% to Modern Award level 3, which are where most disability support
59
HRC p. 3
60 [2011] FWAFB 2700 at para. 282 http://www.fwa.gov.au/decisionssigned/html/2011fwafb2700.htm

20
workers are placed. These are to be implemented in nine equal instalments (one due each December).
The FWA noted that there was substantial agreement between employers, unions and the
commonwealth government that helped make it possible. Notable was the commitment of the
commonwealth government to fund their share of the cost.
As consequence, support workers in Australia will have a starting rate of around $20A an hour in
December 2012, rising to around $28A in 202061. Those at higher grades will be earning around $24 an
hour in December 2012 increasing to around $32A in 2020.
This matters, because of the unique nature of emigration of New Zealanders to Australia. In 2001 a New
Zealand Treasury study concluded that due to a common labour market, New Zealand- Australia
migration was unique:
New Zealand consistently loses its citizens to Australia, but they are not just the highest skilled.
Instead, they are representative of the general population of New Zealand …There is no brain
drain to Australia … but what might be called a "same drain”62.
For example, one of the largest occupational groups among those that moved permanently to Australia
last year were ‘health and welfare support workers’, 822 of whom went there in 2011. Given that there
were large numbers of emigrants to Australia who either gave an unidentifiable response, a response
‘out of scope’ or didn’t state, this figure is likely to be even higher.
New Zealand disability support workers are well aware of this advantage, there will pressure on
disability support workers to shift in pursuit of better wages.
5. Future directions
5.1 Increasing demand
In section 2.1 above we outlined the current demographics regarding disability and the disability
workforce as we understand them to be. In this section we examine the likely demand for disability
support services as reflected in the prevalence of disability and its associated issues, into the near future
and ask what the implications are for the workforce.
We know that we have an ageing population. Population projections indicate that those aged over 65
will increase by 3.16% each year in the 2006-2016 period, 3.13% in the 2016-2026 period and 2.26% in
the 2026-2036 period. By comparison those in the working age population (15-64) will grow 0.55% each
61
Figures provided by Australian Services Union. It is difficult to be definite about the figures because the quantum of the annual wage decision was unknown at the time the request for information was made.
62 Hayden Glass and Wai Kin Choy, ‘Brain drain or brain exchange?’, New Zealand Treasury, 2001
http://www.treasury.govt.nz/workingpapers/2001/01-22.asp

21
year in the 2006-16 period, 0.17% in the 2016-2026 period and will undergo a small decline in the 2026-
2036 period63.
The Department of Labour study which these figures are drawn from also developed three scenarios
based on the Household Disability Survey data from 2006. They project the number of older disabled
people needing support using low, medium and high disability assumptions. They suggest that the
medium and high scenarios are unlikely for New Zealand but that under the low scenario the number of
disabled people in the 65-74 and 75-85 age groups will double between 2006 and 2036 and those over
85 will increase by 3.5 times.
Work done within the Ministry of Health in 2009 attempted to project the prevalence of disability in
New Zealand from 2006 to 201664. The work was unpublished, not peer reviewed, and created scenarios
based on a series of specified assumptions. “Therefore they do not necessarily show the currently
observed situation, but rather indicate what the situation would be if those assumptions are correct”65.
The projection was based on data relating to users of Ministry of Health funded disability support
services. The authors originally intended to project disability prevalence by disability type, but given that
many of those funded through the Ministry of Health have multiple disabilities this would make the data
less reliable. However, given the comparatively high proportion of those with an intellectual disability in
Ministry of Health funded residential care, it is reasonable to assume that people with an intellectual
disability are properly represented in these projections.
This projection also developed high, medium and low scenarios, and suggested that for planning
purposes it was probably safest to use the high scenario. Thus over the decade 2006-2016 they
projected that European/other people with disability could increase by 18% for males and 24% for
females. For Pacific people the increase for males could be 37.9% and for females 41.1%, while for
Maori the increase could be 29.7% for males and 37.3% for females66.
Neither of these studies identify the particular increased demand arising out of future projections of
people with intellectual disabilities, but we know that people with intellectual disabilities are also living
longer than previously and it is reasonable to assume that they will continue to do so into the future:
People with ID now live longer than previously expected, and the ageing of people with mild ID appears
to be equal to that of the general population, posing new challenges to health care professionals67.
63
Department of Labour, The future demand for paid caregivers in a rapidly ageing society, 2009 p.12
64 ‘Disability Projections’, unpublished HDI Technical Note November 2009
65 Don Gray, Deputy Director-General, Policy Business Unit, Ministry of Health, Letter to PSA, 24 April 2012
66 Ibid. pp. 4-5
67 Patja K. Iivianainen M. Vesala H. Oksanen H and Ruopila I. ‘ Life expectancy of people with intellectual disability: a 35-
year follow-up study’, Journal of Intellectual Disability Research, 2000 Oct;44 ( Pt 5):591-9. Abstract
http://www.ncbi.nlm.nih.gov/pubmed/11079356

22
If this is the case then the significant gap that exists between health indicators for people with
intellectual disabilities and the rest of the population means that there will be an increasing number of
health issues for those with intellectual disability. A recent Ministry of Health study on this issue has
highlighted the challenges. For example, males with intellectual disability had an average life expectancy
of 59.7 years, which is more than 18 years below the life expectancy for all New Zealand males
(78.4 years), while females with intellectual disability had an average life expectancy of 59.5 years,
which is almost 23 years below the life expectancy for all New Zealand females (82.4 years).
Compared to people without intellectual disability, people with intellectual disability were, for example:
about 1.5 times more likely to receive care or treatment for one or more of six selected chronic
health conditions (nearly a third of people with intellectual disability, 31.5 percent, had care or
treatment for one or more of these conditions)
about 1.5 times more likely to receive care or treatment for chronic respiratory disease (22.2 percent had care or treatment for chronic respiratory disease)
almost twice as likely to receive care or treatment for coronary heart disease
about 1.5 times more likely to receive care or treatment for cancer
almost twice as likely to receive care or treatment for diabetes
In conclusion, we know that with an ageing population the numbers of people with a disability are
increasing and that this is likely to require an increase in the number of support workers providing home
based support. We also know that, while it is difficult to project the number of people with an
intellectual disability into the future, people with intellectual disabilities are living longer and are
therefore likely to also be increasing in number. We also know that they face significant health
challenges. Both the growing number and the health challenges suggest that more support workers,
with increased levels of skill, will be required in the future.
5.2 New Model for Supporting Disabled People
In recent years the Ministry of Health, reflecting the international trend towards providing people with
disabilities greater choice and control over how they are to be supported so as to enable them to better
lead ordinary lives, under the framework of the New Model for Supporting Disabled People. The two
main initiatives under the New Model have been the development of individualised funding of people
with disabilities able and willing to manage their own support, and Choices in Community Living.
Individualised funding (IF) encourages people with disabilities to gain a greater measure of personal
independence and play a greater role in the communities in which they live. In practical terms IF means
that some people with disabilities will be able to hire, manage, pay, train and make their own contracts
with their support workers or choose to manage aspects of this process.

23
As a result of a review of IF completed in 2008, and endorsed by the Government Response to the
Report of the Social Services Select Committee on its Inquiry into the Quality of Care and Services
Provision for People with Disabilities (2009), the Ministry is working to:
extend eligibility for individualised funding to more disabled people who may not fit existing
criteria
increase the number of providers who wish to offer IF.
Choice in Community Living is an alternative to residential services, and is about opening up
opportunities for disabled people and their family to have more choice and control about their living
circumstances - where they live, who they live with and how they are supported. It is about increasing
their status as a tenant or home owner and separating this from their support arrangements. The
Ministry of Health is working on a project to demonstrate Choice in Community Living in the Auckland
and Waikato regions. The demonstration is limited to 150 people and will run until October 2014.
Enabling Good Lives is another initiative focused on facilitation-based support for people with
disabilities enabling them to lead ordinary lives in the community. It is broadly consistent with the
Ministry of Health’s New Model for Supporting Disabled People, but goes further in several ways. For
example, it extends the facilitation approach across government, and encompasses support funded
through the Ministries of Health and Social Development, and potentially other government agencies.
It is likely to require the development of cross-agency (or joint) facilitation, entry processes, funding
allocation, purchasing and accountability arrangements.
All these initiatives are at the early stage of development and all raise questions about the effective
management of the employment relationship and the impact on both people with disabilities and their
support workers, some of which are subject to ongoing discussion between the Ministry, providers
and unions. However, they are consistent with international thinking and experience and represent
the future of disability support services in New Zealand.
5.3 Implications for the workforce
When we consider future demand for support workers, we know that an ageing population means the
numbers of people with a disability are increasing and that, while it is difficult to project the number of
people with an intellectual disability into the future, people with intellectual disabilities are living
longer and are therefore likely to also be increasing in number. We also know that they face significant
health challenges. Both the growing number and the health challenges suggest that more support
workers, with increased levels of skill, will be required in the future.
The trend to increasing the choices available for people with disabilities is likely to increase the skill
levels required of those in support work. As people with in community living arrangements have
greater control, then support workers will require a greater ability to manage alone as well as highly
developed sense of judgement about how to allow those they work with to take the risks necessary to

24
lead their own lives, and knowing when to intervene. This will be a particular challenge for those
working with people with intellectual disabilities.
To be confident supporters of risk taking, people who provide supports must possess skills
beyond basic risk identification and developing a risk plan. They must have developed skills in:
Multidisciplinary interactions, including a common understanding of risk and the ability to
effectively empower, challenge, and support people.
Negotiation, including the ability to clearly state positions and goals, identify boundaries
(i.e. clear issues of person safety), and be prepared to ‘agree to disagree’.
Facilitation, using empowerment strategies in order to encourage people “to have more
say over their lives, but also to assume responsibility for their decisions in relation to
risk.”68
These are advanced skills, well beyond the basics of personal care, which are not reflected in the
wages paid in the sector. The Disability Workforce Action Plan aims to provide training and career
paths for the disability support workforce to allow the system to move toward more choice and
community based services. So the plan is trying to anticipate these future challenges but we may not
be identifying all the skill needs. For example, as Bonardi points out, there is “no specific reference to
the value of taking risks or mention of support for managing risk dilemmas.69”
Similarly, the kind of ‘invisible’ skills identified by Junor in section 4.6 above (for example, interactive
or emotion management skills, and the skills used to shape long-term support relationships) are also
likely to be more important in the future but these are not necessarily picked up in formal training
programmes.
So, as the skills required increase, we need to ensure that we not only increase the amount of training
we do (which is essential) but we also need to ensure that training meets the changing needs of
disability support services.
With increasing demand there is likely to be increasing pressure on wages. People with disabilities who
are managing their own arrangements under IF are going to want to employ people with whom they
can develop long term supportive relationships, and the findings of an Australian assessment of IF
programmes concluded that the level of remuneration affects the availability of qualified support
workers70. Those who could afford it often paid above award wages while those who were purely
dependent on public funding sometimes struggled to pay decent wages.
68
Bonardi, p.65
69 Ibid. p.66
70 Karen R. Fisher, Ryan Gleeson, Robyn Edwards, Christiane Purcal, Tomasz Sitek, Brooke Dinning, Carmel Laragy, Lele
D’Aegher and Denise Thompson, Effectiveness of individual funding approaches for disability support, Department of
Families, Housing, Community Services and Indigenous Affairs, 2010 p. 43

25
As the economy gradually improves we can expect turnover to increase as workers have more
opportunity. A recent survey indicated that a remarkable 61% of New Zealand workers are thinking of
changing their job in 2013, up from 33% the year before71.
6. The change that is needed
6.1 Recommendations
Two recent OECD72 reports have recommended three avenues for meeting the increased demand for
‘carers’ arising out of an ageing society:
Increasing the supply of support workers by making their jobs more attractive to under-
represented or unemployed groups in the population by addressing training, pay and
conditions at work;
Making better use of the available carer workforce by improving staff retention, again through
training, pay and conditions at work, as well as supporting informal carers;
Reduce the need for support workers through increased use of technologies and changing the
skill mix required for different tasks.
This provides a good framework for addressing the future of the disability support work workforce.
The first two avenues are about creating a stable workforce through better recruitment and retention
by addressing the current gaps in training, pay and conditions. On current funding levels and current
funding and contracting mechanisms, this will be very difficult to achieve. Increased funding and
different ways of delivering the funding are required.
The last is really about productivity. There is not much more that can be achieved in disability support
by increased use of technologies and the growth of the support workforce reflects a shift from
regulated to unregulated workers that has already taken place. If there is to be an increase in
productivity it is more likely to come from a stable workforce operating in high trust, high performing
workplaces, where the staff are respected and engaged. Again this is an investment strategy.
Accordingly we make the following recommendations:
Develop a mechanism to achieve pay parity between disability support workers and
therapy assistants working in DHBs to deliver parity within three years, using Auckland
therapy assistants service-based pay maximum as the comparator
Investigate options for achieving pay parity with corrections officers by 2020.
71
http://www.stuff.co.nz/business/industries/8069846/Majority-of-workers-plan-to-leave-next-year
72 Schoot et.al 2003, cit. Columbo, F. Help Wanted? Providing and Paying for Long-Term Care, OECD Health Policy Studies,
OECD, 2011 and Fujisawa, R. and Columbo, F. “The Long-Term Care Workforce: Overview and Strategies to Adapt Supply
to a Growing Demand”, OECD Health Working Papers, No. 44, OECD publishing 2009

26
Develop a timeline for funding against minimum levels of qualified workers as proposed in the
Disability Workforce Action Plan 73so that training and education has a clear funding path.
Increase the money available through Disability Workforce Development grants, administered
by Te Pou, to allow more funding for training in residential support.
Develop a transparent pricing model for funding disability residential services in line with the
Disability Workforce Action Plan objective74 and building on the work already done on a TPM.
Implement strategic objective 14 of the Disability Workforce Action Plan which seeks to create
“more financial certainty for providers by establishing multi-year funding contracts for core
disability support services”75.
6.2 Costing pay parity
In developing this business case economist Geoff Bertram was commissioned to calculate the cost of
increasing the wages of disability support workers to achieve pay parity with therapy assistants and
corrections officers. His work is attached as Schedule A to the Business Case.
In order to estimate the cost of bringing Disability Support Workers’ rates of pay up to parity with
other groups of workers performing similar work at comparable skill levels, three basic numbers or
sets of numbers are required:
The current rates of pay for disability support workers
The current rates of pay for selected comparator group or groups
The number of disability support workers to whom any adjustment would apply
The current rates for disability support workers are provided by the recent NZDSN survey of providers,
the current rates of pay for selected comparator groups were taken from the relevant collective
agreements and the number of disability support workers was estimated at 15,000 using the
information and assumptions outlined in section 4.2 above.
The preferred comparator of those considered by both Dr. Bertram and the earlier PSA job evaluation,
is the maximum of the service-based pay range for Auckland therapy assistants. At the time the
original job evaluation was done there was a single multi-employer collective agreement for therapy
assistants (and other allied health workers) working in DHBs. Subsequent negotiations saw the
collective agreement split into one for Auckland and another for the rest of the country. One of the
differences between the Auckland agreement and both its all-New Zealand predecessor and its rest-of-
New Zealand counterpart, is that whereas those two agreements had service-based progression to
step 5, in Auckland it goes to step 6.
The reason for choosing this higher rate is that the existence of merit steps above these service-based
rates means that there will be a reasonable number of therapy assistants around the country who
73
Disability Workforce Action Plan p. 22
74 Ibid.
75 Disability Workforce Action Plan p. 18

27
could be being paid up to $23.01 an hour or 24.4% above the comparable disability support worker
rate. By comparison the Auckland service-based maximum is 17.8% above the comparable disability
support worker rate, and the rest-of-New Zealand service-based maximum is 10.5%. The Auckland rate
is therefore almost a neat midpoint between the other possible upper and lower comparator rates.
Dr. Bertram concludes that the annual increase required to achieve pay parity using this comparator
would be around $63 million, which could be spread over three years. If the increases were to be
phased in over three years, this would be most simply done by adding a fixed amount to the hourly
rate in each of the three successive years. This procedure would result in the year-by-year changes
and total costs set out in Table 5 in Schedule A to the Business Case.
The cost of achieving pay parity with corrections officers is considerably higher, requiring a 46%
increase. Dr. Bertram estimates this to be around $250m. While the cost of achieving this renders this
move unlikely in the current financial climate, it does not undermine the case for parity between two
groups that have been formally assessed by a reputable job evaluation tool as doing comparable work.
We therefore recommend that options for achieving this goal by 2020 be further investigated.