improving access to primary care for the uninsured in davidson county april 2010
TRANSCRIPT

Improving Access to Improving Access to Primary Care for the Primary Care for the
Uninsured in Davidson Uninsured in Davidson CountyCountyApril 2010April 2010

Davidson County Access Davidson County Access to Care Teamto Care Team
• Layton Long – Davidson County Health DepartmentLayton Long – Davidson County Health Department
• Cyrus Bush – Thomasville Medical CenterCyrus Bush – Thomasville Medical Center
• Sandy Motley – Davidson Medical Ministries ClinicSandy Motley – Davidson Medical Ministries Clinic
• Dale Moorefield – Davidson County Social ServicesDale Moorefield – Davidson County Social Services
• Robert Hyatt – Davidson County Managers Robert Hyatt – Davidson County Managers DepartmentDepartment
• Chris White – Lexington Memorial HospitalChris White – Lexington Memorial Hospital
• The Problem The Problem
– Increasing Number of Uninsured PatientsIncreasing Number of Uninsured Patients– Lack of Access to Preventative Health CareLack of Access to Preventative Health Care– Davidson Medical Ministries StrugglingDavidson Medical Ministries Struggling– Poorer Health OutcomesPoorer Health Outcomes
• Working Toward a SolutionWorking Toward a Solution
– Developing a Leadership TeamDeveloping a Leadership Team
• The SolutionThe Solution
– Transition of Davidson Medical Ministries Clinic (DMMC) to a Federally Transition of Davidson Medical Ministries Clinic (DMMC) to a Federally Qualified Health Center (FQHC)Qualified Health Center (FQHC)
Overview

Target MarketTarget Market
• Davidson County Residents 18-64 Davidson County Residents 18-64 (primary)(primary)
– UninsuredUninsured
– UnderinsuredUnderinsured
– Others without a medical homeOthers without a medical home

Definition of PlanDefinition of Plan• The primary safety net provider for the The primary safety net provider for the
uninsureduninsured
• Declining Resources with Increasing DemandDeclining Resources with Increasing Demand– Loss volunteersLoss volunteers– Reduced Donations and GrantsReduced Donations and Grants– Reductions in ServicesReductions in Services
• Current Model is UnsustainableCurrent Model is Unsustainable
• Decision to Transition to FQHC Decision to Transition to FQHC

BenefitsBenefits• Expanded Clinical hours … Expanded Clinical hours …
increased patient capacityincreased patient capacity
• Expanded Dental ServicesExpanded Dental Services
• A Medical Home for residents with a A Medical Home for residents with a chronic diseasechronic disease
• More cost effective careMore cost effective care
Benefits (cont.)Benefits (cont.)• Hours of OperationHours of Operation
– From 29 hours at Lexington to 48 hoursFrom 29 hours at Lexington to 48 hours
• StaffingStaffing– From 5 hrs/week MD and 2 Mid Levels to 1 Full From 5 hrs/week MD and 2 Mid Levels to 1 Full
Time MD and 2 Mid LevelsTime MD and 2 Mid Levels– From volunteer dentist to 1 paid staff dentistFrom volunteer dentist to 1 paid staff dentist– Increased support staffIncreased support staff
• FinancesFinances– Lessened dependency on grants and donationsLessened dependency on grants and donations– Secure payor sources through Medicaid, Secure payor sources through Medicaid,
Medicare, Sliding Fees, and private insurancesMedicare, Sliding Fees, and private insurances– Stable annual federal grant funding Stable annual federal grant funding
Operations and ManagementOperations and Management
• Move forward as Satellite with Gaston Family Health Services(GFHS) Move forward as Satellite with Gaston Family Health Services(GFHS) as sponsoring board.as sponsoring board.
• Corporate Board with 2 members of DMMC advisory boardCorporate Board with 2 members of DMMC advisory board– Fiduciary responsibilitiesFiduciary responsibilities– 51% consumer based51% consumer based
• Advisory BoardAdvisory Board– General Operations oversightGeneral Operations oversight– Community outreach and supportCommunity outreach and support
• Site AdministratorSite Administrator– Responsible to Executive Director of GFHS and BoardResponsible to Executive Director of GFHS and Board
• Operations ModelOperations Model– 5 primary programs with managers: Clerical-Eligibility, Medical, 5 primary programs with managers: Clerical-Eligibility, Medical,
Dental, Pharmacy and Thomasville.Dental, Pharmacy and Thomasville.– Responsible for staff, volunteers, students, patient services.Responsible for staff, volunteers, students, patient services.– 3 coordinators: Hispanic, Social Work, Volunteer3 coordinators: Hispanic, Social Work, Volunteer
• Services provided:Services provided:– Currently at 4 days per week or 30 hours Currently at 4 days per week or 30 hours
• Expand to 40 hours immediately and up to 60 hours by end of year 2. Expand to 40 hours immediately and up to 60 hours by end of year 2.

Gaston Family Health Services, Inc. General Board
2 members of Davidson Medical Ministries Board will serve on this board.
Davidson Medical Ministries Clinic, Inc.
DMMC Advisory Board
Sandy Motley, DMMC site Administrator
DMMC Medical Director
Clerical-Eligibility Program Manager
Medical Clinic/RN program manager
Dental Clinic Program Manager
Pharmacy (RPh) Program Manager
Thomasville Clinic/RN Program Manager
Robert Spencer, Executive Director, GFHS,
Inc.
Volunteer Coordinator
Hispanic Services Coordinator
Social Services Coordinator
2 front office staff 1 Eligibility screener Volunteers Interns Work Experience Students
1 MD (Medical Dir.) 2 Mid-level providers 3 Medical Assistants Volunteer providers Volunteer nursing support Medical Students PA/NP students Nursing students
1 Dentist 1 Dental Hygienist 2 Dental Assistants 1 Clerical/reception Volunteer dentists Volunteer hygienists Volunteer assistants Students
1 Pharmacist 2 Technicians 1 MAP technician 1 Clerical/reception Volunteer pharmacists Volunteer technicians Students Work Experience
1 PT Mid-level provider 1 PT Medical Assistant 1 PT Eligibility coordinator 1 PT Clerical/Reception Volunteer providers Volunteer nursing support Medical Students Nursing Students PA/NP Students Work Experience
Organizational Flow Chart for Federally Qualified Health Center Satellite Facility

Access to Care - Need Access to Care - Need IndicatorsIndicators
• 19% - overall lack any health care coverage19% - overall lack any health care coverage
• 23.6% - under age 65 lack health care 23.6% - under age 65 lack health care coveragecoverage
• 15.4% - under age 65 working for wages lack 15.4% - under age 65 working for wages lack health health care coverage care coverage
• 17.7% - indicated a time when they needed 17.7% - indicated a time when they needed health health care but could not afford it. care but could not afford it.

MarketingMarketingLow Key ApproachLow Key Approach
– Full advertising not advisableFull advertising not advisable– Unwanted attention could bring Unwanted attention could bring
negative consequencesnegative consequences
• Retaining paying patientsRetaining paying patients
• Accepting referrals Accepting referrals

Uninsured Health Care Uninsured Health Care IndustryIndustry
• No direct competition for uninsuredNo direct competition for uninsured
• Private providers not competing Private providers not competing for uninsured patientsfor uninsured patients
• Limited options for care results in Limited options for care results in
costly emergency room visits costly emergency room visits

Safety Net Clinic Models Safety Net Clinic Models
• Free ClinicsFree Clinics • Community Health CentersCommunity Health Centers • Federally Qualified "Look-a-like" Health Federally Qualified "Look-a-like" Health
CentersCenters • Federally Qualified Health Center Federally Qualified Health Center
(Independent or Satellites)(Independent or Satellites)

FQHC Satellite AdvantagesFQHC Satellite Advantages
Partnering with an existing FQHCPartnering with an existing FQHC
– Established track record of successEstablished track record of success – Section 330 Federal Funding - $650,000 Section 330 Federal Funding - $650,000
annuallyannually
– Expand primary care services in Expand primary care services in communitiescommunities
– Administrative Support for FQHC operationAdministrative Support for FQHC operation

MeasurementsMeasurements CurrenCurrent t
Year Year 1 1
Year2 Year2
Client visits/week Client visits/week 193 193 212212 240240
Adult dental Adult dental visits/week visits/week
1212 3333 6666
Pharmacy Rx/week Pharmacy Rx/week 769769 808808 918918
Eligibility Eligibility interviews/weekinterviews/week
5050 6060 7070
Social worker Social worker visits/week visits/week
2020 2929 3636
Increase physician FTE Increase physician FTE 00 .5.5 11
Measures of SuccessMeasures of Success
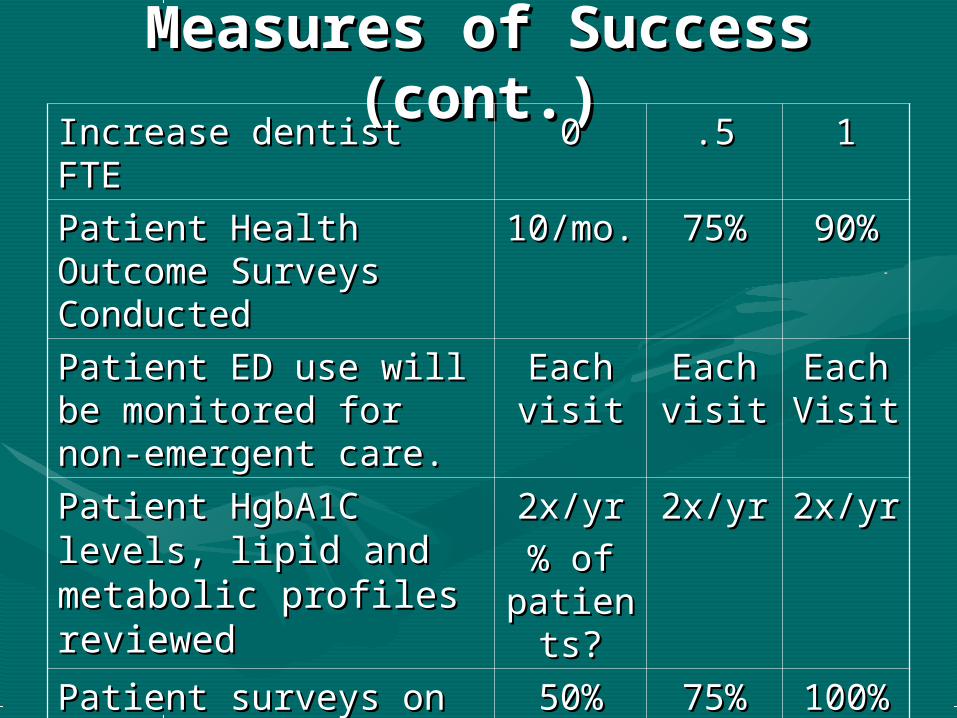
Measures of Success Measures of Success (cont.)(cont.)
Increase dentist FTE Increase dentist FTE 00 .5.5 11
Patient Health Patient Health Outcome Surveys Outcome Surveys ConductedConducted
10/mo.10/mo. 75%75% 90%90%
Patient ED use will be Patient ED use will be monitored for non-monitored for non-emergent care.emergent care.
Each Each visitvisit
Each Each visitvisit
Each Each VisitVisit
Patient HgbA1C levels, Patient HgbA1C levels, llipid and metabolic ipid and metabolic profiles reviewed profiles reviewed
2x/yr2x/yr
% of % of patientpatient
s?s?
2x/yr2x/yr 2x/yr2x/yr
Patient surveys on ED Patient surveys on ED use and hosp. use and hosp. admissionsadmissions
50%50% 75%75% 100%100%

RisksRisks
• Finding a FQHC partnerFinding a FQHC partner
• Comprehensive health care reformComprehensive health care reform
• Revenue generation / Medicaid billingRevenue generation / Medicaid billing
• New patientsNew patients
• Retention of existing staffRetention of existing staff
Exit PlanExit Plan
• Continue operation as DMMCContinue operation as DMMC
• Establishing independent FQHC Establishing independent FQHC

Budget (Revenue)Budget (Revenue)Revenue FY2011 FY2012 FY2013 FY2014 FY2015
Partners in Care/Individuals $ 211,558 $ 169,246 $ 135,397 $ 108,317 $ 86,654
Churches/Business/Civic Groups $ 104,000 $ 83,200 $ 66,560 $ 53,248 $ 42,598
Fundraisers $ 47,200 $ 37,760 $ 30,208 $ 24,166 $ 19,333
Local Foundations $ 19,200 $ 5,360 $ 12,288 $ 9,830 $ 7,864
Grants $ 155,000 $ 124,000 $ 99,200 $ 79,360 $ 63,488
United Way $ 96,000 $ 76,800 $ 61,440 $ 49,152 $ 39,322
Insured patient rev. ($58 per visit) $ 58,000 $ 87,000 $ 130,500 $ 195,750 $ 293,625
Uninsured patient rev.($10 per visit) $ 100,000 $ 110,000 $ 121,000 $ 133,100 $ 146,410
Dental patient rev. ($75 per visit) $ 128,700 $ 257,400 $ 267,696 $ 278,404 $ 289,540
Pharmacy revenue ($3 per Rx) $ 126,000 $ 143,182 $ 164,373 $ 191,119 $ 225,695
Section 330 Grant Funding $ 650,000 $ 975,000 $ 1,300,000 $ 1,300,000 $ 1,625,000
In Kind Rev. (hosp. labs/radiology) $ 800,000 $ 800,000 $ 800,000 $ 800,000 $ 800,000
Total Revenue $ 2,495,658 $ 2,878,948 $ 3,188,662 $ 3,222,447 $ 3,639,529
Prescriptions Filled 42,000 47,727 54,791 63,706 75,232
Medical Insured Visits 1,000 1,500 2,250 3,375 5,063
Medical Uninsured Visits 10,000 11,000 12,100 13,310 14,641
Total Medical Visits 11,000 12,500 14,350 16,685 19,704
Total Dental Visits 1,716 3,432 3,569 3,712 3,861
Total Visits 12,716 15,932 17,919 20,397 23,564

Budget (Expense)Budget (Expense)Expense FY2011 FY2012 FY2013 FY2014 FY2015
Salaries/Benefits $ 1,259,000 $ 1,623,795
$ 1,750,883 $ 1,803,409
$ 2,040,407
Professional Fees $ 25,400 $ 26,162 $
26,947 $ 27,755 $ 28,588
Supplies $ 176,100 $ 220,637 $
248,159 $ 282,473 $
326,331
Utilities $ 29,900 $ 30,797 $
31,721 $ 32,673 $ 33,653
Insurance $ 35,000 $ 36,050 $
37,132 $ 38,245 $ 39,393
Repairs and Maintenance $ 8,600 $ 8,858 $ 9,124 $ 9,397 $ 9,679
Purchased Services $ 88,350 $ 91,001 $
93,731 $ 96,542 $ 99,439
Marketing $ 12,000 $ 12,360 $
12,731 $ 13,113 $ 13,506
Other Expense $ 46,200 $ 47,586 $
49,014 $ 50,484 $ 51,999
In Kind Expense (hospital labs/radiology) $ 800,000 $ 800,000
$ 800,000 $ 800,000
$ 800,000
Total Expenses $ 2,480,550 $ 2,897,246
$ 3,059,439 $ 3,154,092
$ 3,442,994
Profit/(loss) $ 15,108 $
(18,298) $
129,222 $ 68,356 $
196,535

Questions ??Questions ??