improving quality of care in chronic disease dr. sherry rohekar september 10, 2009
TRANSCRIPT
Improving Quality of Care in Chronic Disease
Dr. Sherry RohekarSeptember 10, 2009

OverviewWhat is the program?Your goals
Results of needs assessmentBurden of arthritisApproach to arthritis
Polyarthritis Acute vs. chronic
Monoarthritis Septic vs. crystal

The Arthritis Expert Program: Why?Many communities in SW Ontario are
underserviced in terms of arthritis careArthritis Experts (AEs) will better support
local health teams in their delivery of complex medical care
Comprised of nurses, nurse practitioners and family physicians who frequently refer patients to rheumatologists at St. Joseph’s Health Care (SJHC) in London

The Arthritis Expert Program: What?Will occur over 18 months, with monthly
sessionsParticipants may attend sessions at SJHC or
attend monthly telemedicine conferences via computer
At the end of the program, we expect that participants will able to:Identify and triage rheumatologic complaintsConfidently treat some complaintsCo-manage chronic arthritic complaints in
conjunction with rheumatologists at SJHC

Course CurriculumTeleconferences / Broadcasting from
Telehealth, to be archived for use for those who can’t attend live
Knowledge assessments – at the beginning and throughout the program
Preceptorships and rounds in some regions – also telecast
Case of the month – each month a case related to the learning will be posted with each candidate giving the answers, and then answers are posted and discussion can occur

Course CurriculumInternet discussion boardChart audit –10 MSK patients sometime in
first 6 months, with data extraction tool, to be done 3 times over the course
Attendance at the Education Day (live or via broadcast / DVD) once over the course – offered at various times, usually on a Thursday, scheduled well in advance
Opportunity to do advanced training preceptorship in London (not mandatory)
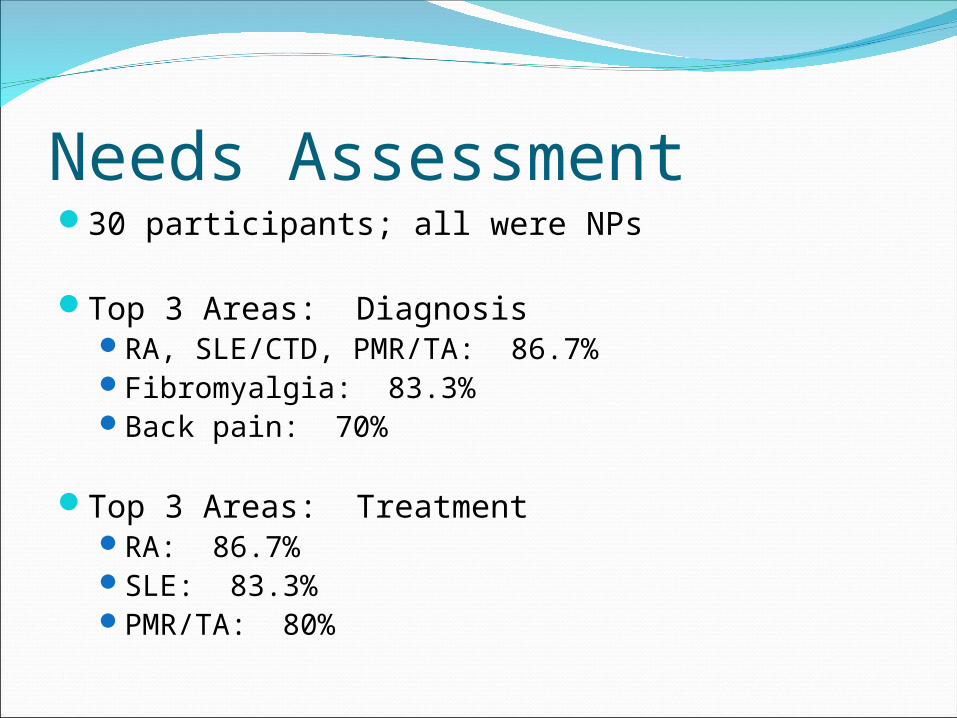
Needs Assessment30 participants; all were NPs
Top 3 Areas: DiagnosisRA, SLE/CTD, PMR/TA: 86.7%Fibromyalgia: 83.3%Back pain: 70%
Top 3 Areas: TreatmentRA: 86.7%SLE: 83.3%PMR/TA: 80%

Needs AssessmentOther areas of interest:
Comprehensive approach to MSK exam: 93.3%Medications and monitoring of RA: 90%MSK imaging: 90%Approach to lab tests (i.e. RF, ANA): 76.7%
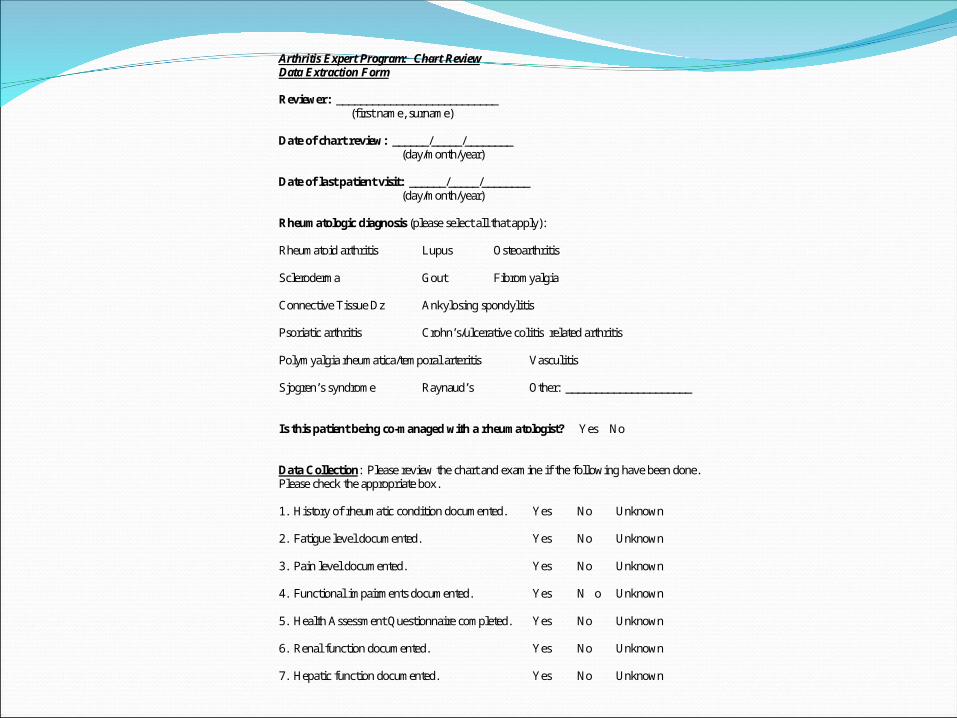
Arthritis Expert Program: Chart Review Data Extraction Form Reviewer: ___________________________ (first name, surname) Date of chart review: ______/_____/________ (day/month/year) Date of last patient visit: ______/_____/________ (day/month/year) Rheumatologic diagnosis (please select all that apply): Rheumatoid arthritis Lupus Osteoarthritis Scleroderma Gout Fibromyalgia Connective Tissue Dz Ankylosing spondylitis Psoriatic arthritis Crohn’s/ulcerative colitis related arthritis Polymyalgia rheumatica/temporal arteritis Vasculitis Sjogren’s syndrome Raynaud’s Other: _____________________ Is this patient being co-managed with a rheumatologist? Yes No Data Collection: Please review the chart and examine if the following have been done. Please check the appropriate box. 1. History of rheumatic condition documented. Yes No Unknown 2. Fatigue level documented. Yes No Unknown 3. Pain level documented. Yes No Unknown 4. Functional impairments documented. Yes N o Unknown 5. Health Assessment Questionnaire completed. Yes No Unknown 6. Renal function documented. Yes No Unknown 7. Hepatic function documented. Yes No Unknown

General Arthritis Statistics in Canada4 million Canadians have some form of
arthritis (1 in 6 people).2/3 are women3 in 5 are <65 years old
By 2026, 6 million Canadians will have arthritis.
One of the top 3 most common chronic conditions (with non-food allergies and back problems).
Health Canada. Arthritis in Canada. An Ongoing Challenge. Ottawa: Health Canada, 2003.Perruccio et al. J Epidemiol Community Health 2007;61:1056-61.

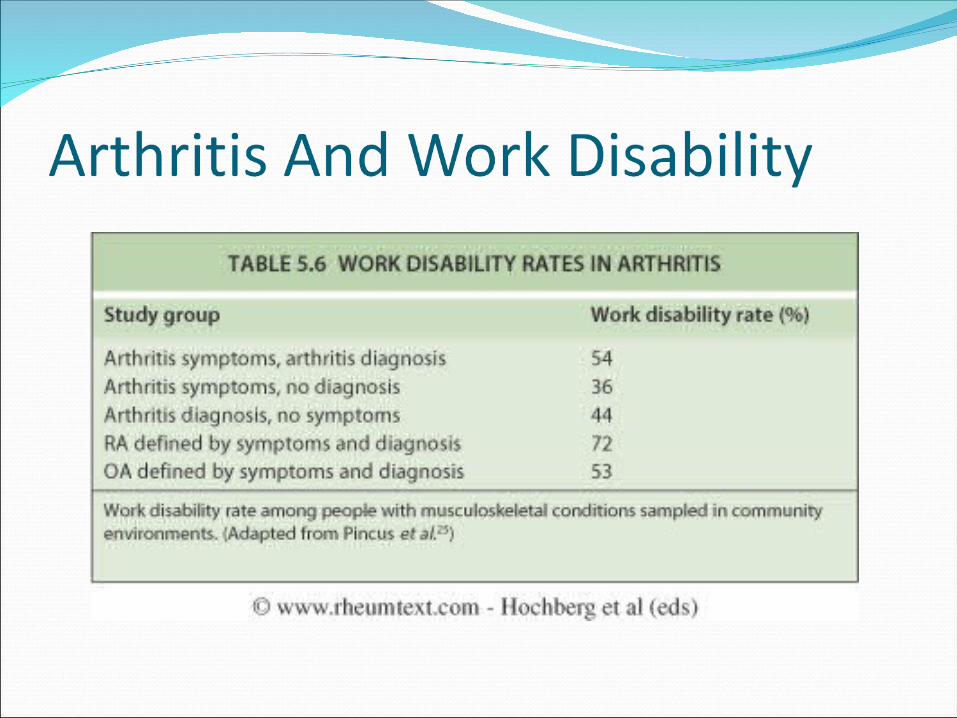
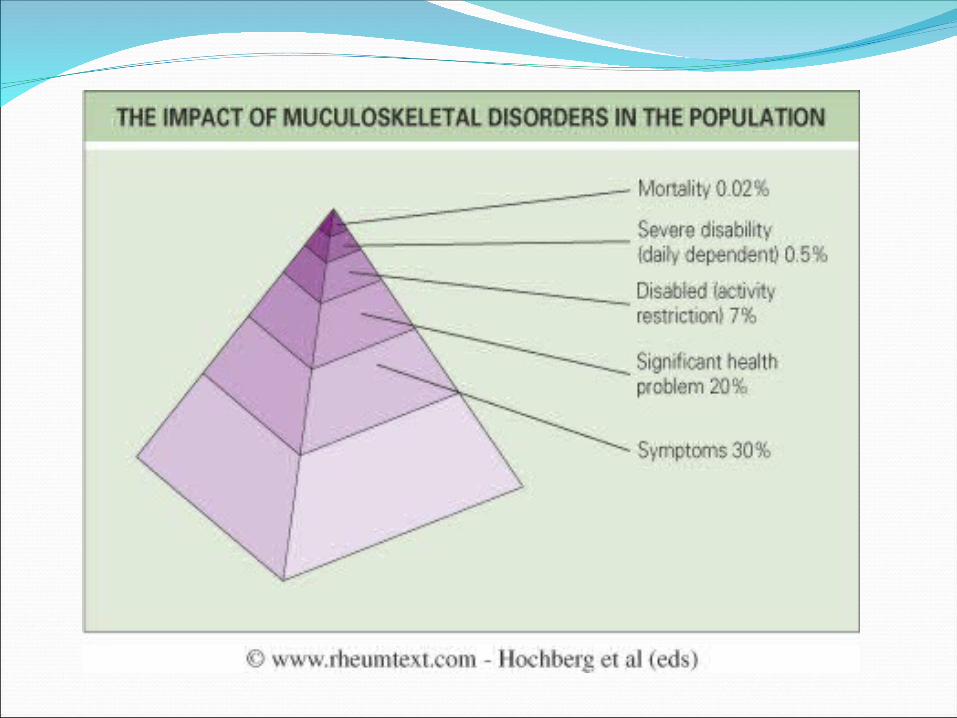
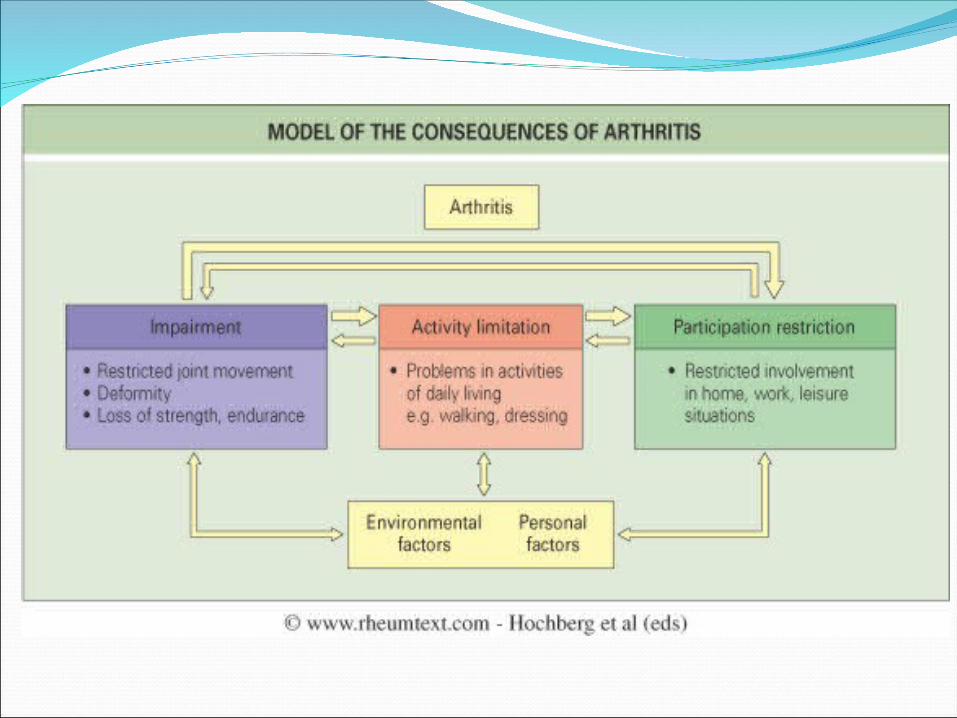
The Burden of ArthritisMajor outcome of arthritis:
chronic pain reduced mobility decreased level of function
Impact on quality of life: mobility, communication, schooling & employment.
Cost of arthritis was over $4 billion (1998) in health care expenses and loss of productivity.
In 1998, medication accounted for $270 million, or 6% of total arthritis cost. This will increase with the use of biologics.
The Arthritis Society of Canada. Arthroscope. An Ongoing Challenge, 2004.

A Chronic and Disabling DiseaseCompared to patients with other chronic
conditions, those with arthritis:Experienced more pain, activity restrictions &
long-term disabilityWere more likely to need help with daily
activitiesReported worse self-rated health, more
disrupted sleep and depressionHave more contacts with healthcare
professionals
Health Canada. Arthritis in Canada. An Ongoing Challenge. Ottawa: Health Canada, 2003.
Common Comorbidities in Rheumatic Disease• CVD & Atherosclerosis
• Metabolic Syndrome
• Fibromyalgia
• Peridontal Disease
• Effects of Smoking

Impact of ComorbiditiesPoorer outcomes (response, remission)Higher morbidityIncreased mortality (e.g., CVD)Potential for drug interactions
Krishnan E, et al. Ann Rheum2005;64:1350-2.Wasko MC. Curr Opin Rheumatol 2004;16:109-13.
Boers M, et al. Arthritis Rheum 2004;50:1734-9.



In the 1986 Canadian population.

% prevalence in the Ontario population.


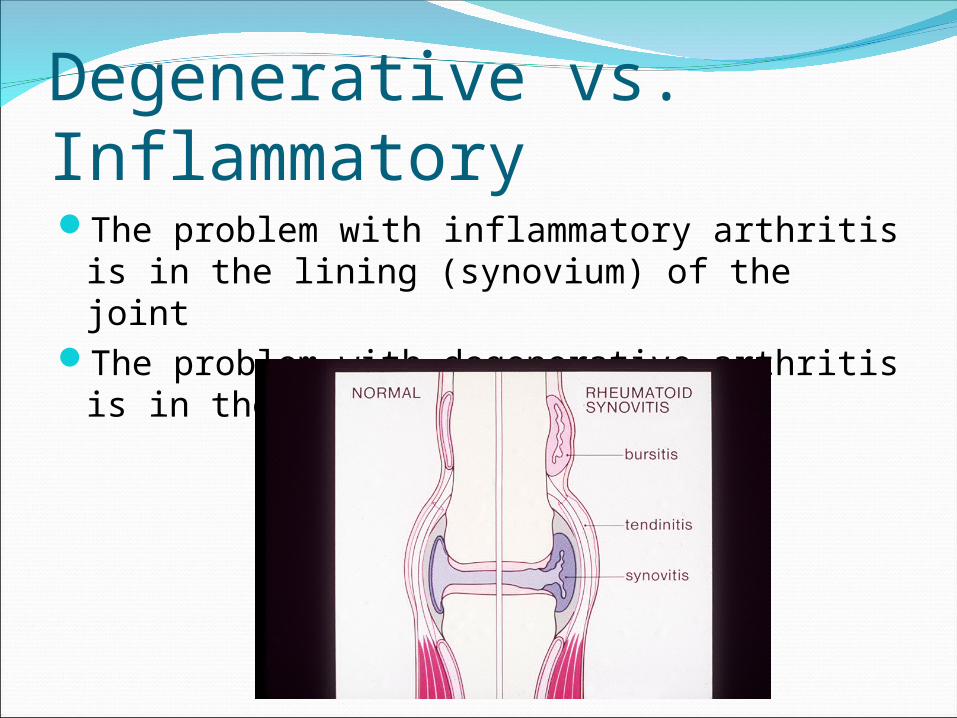
Degenerative vs. InflammatoryThe problem with inflammatory arthritis is in
the lining (synovium) of the jointThe problem with degenerative arthritis is in
the cartilage


Approach To PolyarthritisWhat is polyarthritis? How is it different
from polyarthralgia?Polyarthritis: swelling, tenderness and warmth
of >4 joints, demonstrated by physical examination
Polyarthralgia: pain in >4 joints without demonstrable inflammation on physical examination

Polyarticular SymptomsPolyarticular Symptoms
Acute (<6 wks)Acute (<6 wks) Chronic (>6 wks)Chronic (>6 wks)
InfectionInfection Not InfectionNot Infection
InflammatoryInflammatory Not InflammatoryNot Inflammatory

Polyarticular SymptomsPolyarticular Symptoms
Acute (<6 wks)Acute (<6 wks)
InfectionInfection Not InfectionNot Infection
Gonoccocal
Meningococcal
Lyme disease
Acute rheumatic fever
Bacterial endocarditis
Viral
Rubella
Hepatitis B or C
Parvovirus B19
EBV
HIV
RA
SLE
Reactive arthritis
Psoriatic arthritis
Polyarticular gout
Sarcoidosis
Serum sickness

Polyarticular SymptomsPolyarticular Symptoms
Chronic (>6 wks)Chronic (>6 wks)
InflammatoryInflammatory Not InflammatoryNot Inflammatory
RA
SLE
SSc
PM
ReA
PsA
Polyarticular crystal
Enteropathic arthritis
Sarcoid
Vasculitis
PMR
OA
CPPD
Paget’s disease
FM
Benign hypermobility syndrome
Hemochromatosis

TimingMigratory Additive Intermittant
Present for few days, remits, then
recurs in other joints
Rheumatic fever
Gonococcal
Lyme disease
Begins in some joints and persists,
then goes on to involve others
RA
PsA
Enteropathic arthritis
SLE
Repeated attacks of polyarthritis with complete
remission between attacks
RA
PsA
ReA
Sarcoid
Polyarthricular gout

Approach To Monoarthritis:Acute Hot, Red Monoarthritis1. Infection2. Infection3. Infection4. Gout5. Pseudogout6. Oh, did I mention …. Infection?

What do you want to do?Aspirate the joint (i.e. take a sample of
fluid from the joint)IF THE JOINT IS RED, THE TUBES GET
FED!

What do you send the fluid for?The 3 C’s
Cell Count: A couple of hoursCulture & Sensitivity: 24-48 hoursCrystals: A couple of hoursGram Stain

Septic Arthritis
Acute Bacterial ArthritisMedical
emergency!!
Importance Of Diagnosis
Failure to recognize and appropriately treat bacterial septic arthritides may lead to significant rates of morbidity and even mortality Specifically, debilitating destruction of
the joint

Importance Of Diagnosis
Failure to recognize and appropriately treat bacterial septic arthritides may lead to significant rates of morbidity and even mortality Specifically, debilitating destruction of
the joint

Historical Features
Acute onset of joint pain (may be superimposed on chronic pain)
History of trauma Remember iatrogenic joint aspiration
Monoarticular vs. polyarticular Extra-articular symptoms IV drug use/presence of intravenous
catheters

Historical Features
Exposure to STDs Conditions that may decrease patient’s
immunity Liver disease, DM, cancer, complement
deficiencies, hypogammaglobulinemia, immunosuppressive medication

Historical Features
Classically, present with complaints of low grade fever (40-60%), pain (75%) and decreased ROM, evolving over days or weeks
Sometimes difficult to distinguish from the presentation of crystal arthropathies Tend to have spiking fevers and chills,
rigors

Historical Features
If prosthetic joint infection, course usually low-grade with gradually increasing pain
Usually no significant swelling or fever S. aureus associated with a fulminant
course Devitalized tissues (i.e. hematomas)
more susceptible to bacterial multiplication
Course usually more muted in case of bacteremic spread

Historical Features
Tuberculous arthritis has indolent features Usually negative PPD, no signs of past
or present pulmonary TB
Physical Findings
Most commonly involved joints: knee (50%), hip (20%), shoulder (8%), ankle (7%), wrists (7%) Elbow, interphalangeal,
sternoclavicular, SI joints 1-4% cases
Physical Findings
Erythema and swelling in 90% of cases Warmth and tenderness also essential for
diagnosis Usually an obvious effusion Marked limitation of PROM and AROM Beware of locations where difficult to find:
spine, hip, shoulders Physical findings muted in elderly,
immunocompromised, IVDU and especially those with RA

Differential Diagnosis
Crystals (gout, pseudogout) RA Seronegative disease (PsA,
enteropathic arthritis) Reactive arthritis Rheumatic fever Drug-induced arthritis
Diagnosis: Acute GoutThe Disease of KingsAcute inflammatory
arthritis caused uric acid crystal deposition in the joint

Who gets Gout?First attack in men between the ages of
35 and 50.In women it starts after menopause as
estrogen has a protective effect on the excretion of uric acid.

Clinical Features of the AttackStarts quickly and very intensely – over a few
hoursVery painful (Can’t stand the bed sheets
touching it)Swollen, warm, and redMay feel unwell and have an associated feveri.e. it can look just like an infected joint!

What Joints does it affect?Usually a single joint in
the lower extremityFirst metatarsophalangeal
(MTP) joint (i.e. the big toe) is affected in 50% of cases

Common Risk Factors for GoutImpaired renal functionDiuretics: Lasix & hydrochlorothiazideExcessive Alcohol IntakeFamily historyMale Sex

Other Disease Associations“A Disease of Plenty”ObesityHypertension (high blood
pressure)DiabetesHyperlipidemia (high lipids)

What “triggers” the Attack?SMARTSSurgeryMechanical InjuryAlcoholRecent IllnessTravel / dehydrationStart/Stop Allopurinol

How to Confirm the DiagnosisMust aspirate the joint and find urate
crystals to prove diagnosis (needle shaped)
Urate crystals negatively birefringent in polarized light

What Blood Tests Should I Order?Complete Blood Count (CBC)
May see elevated WBCMay see reactive thrombocytosis (increased
platelets)
Creatinine (measure renal function)Uric Acid
Levels may be normal during an acute attack
Fasting GlucoseFasting Lipid Levels
Tryglycerides & cholesterol

A Word About Uric AcidThere are lots of people walking around with
elevated uric acid levels (hyperuricemia)Many of these people will not get goutHyperuricemia CANNOT be used to make a
diagnosis of gout!Do not treat isolated hyperuricemia

Treatment: Non-PharmacologicRest, ice, and elevate the JointDietary modification
Meat & seafood are BadVegetables & low-fat dairy are good
Reduce alcohol intakeGood hydration

PharmacologicIntra-articular corticosteroids
Inject the affected jointOral NSAIDs or COXIBs
Indomethacin 50 mg PO TIDOral colchicine
0.6 mg PO q8h Oral prednisone
50 mg po x 7 days

When To Consider Allopurinol1. Recurrent acute episodes of gout affecting
lifestyle; 2. Patients at risk from complications of
treatments required for acute attacks; 3. Patient acceptance of the need for lifelong
medication compliance;4. Uric acid tophaceous deposits

AllopurinolDo not start during an acute attackProphylaxis with an NSAID/ColchicineReduce uric acid to lower limit of laboratory
reference range
Xanthine Uric Acid Xanthine Oxidase
ALLOPURINOL inhibits
Xanthine Uric Acid Xanthine Oxidase
ALLOPURINOL inhibits

Diagnosis: Acute Pseudogout Acute inflammatory
arthritis caused by calcium pyrophosphate crystals

Who gets Pseudogout?Older individualsOften have associated osteoarthritis

Clinical Features of the AttackStarts quickly and very intensely Tends to be less intense than gout and takes
longer to reach peak than acute goutVery painful Swollen, warm, and redMay feel unwell and have an associated feveri.e. it can look just like an infected joint!
What Joints Does it Affect?Usually a single joint in
the lower extremityKnee is the most common

How to Confirm the DiagnosisMust aspirate the joint and find
intracellular calcium pyrophosphate crystals to prove diagnosis (rhomboid shaped)
CPP crystals positively birefringent in polarized light

Non-Pharmacologic TreatmentRest, ice, and elevate the jointGood hydration
PharmacologicIntra-Articular
Corticosteroids Inject the affected joint
Oral NSAIDs or COXIBsIndomethacin 50 mg PO
TID
Oral Prednisone50 mg po od x 7 days

SummaryWe hope to increase teamwork between NPs,
FPs and rheumatologistsCo-management of chronic diseaseContinuing education