improving rehabilitation services regional stakeholder event
TRANSCRIPT

www.england.nhs.uk
Improving
Rehabilitation
Services
Regional
Stakeholder
Event
Leeds - 5th April 2016

www.england.nhs.uk
Dr Mike Prentice
Regional Medical Director (North)
NHS England

www.england.nhs.uk
• Housekeeping
• Event Programme
• Workshops
• Lunch and Breaks
Twitter #improverehab16
Wi Fi Username: res1 Password: res1
WELCOME
3

www.england.nhs.uk
Suzanne Rastrick
Chief Allied Health Professions Officer
NHS England
4

www.england.nhs.uk
Lindsey Hughes
Rehabilitation Programme Lead
NHS England
5

Rehabilitation
Commissioning
Guidance
Lindsey Hughes
April 2016

www.england.nhs.uk
Regional Rehabilitation Leads, March 2015
“There is poor awareness of the scope of rehabilitation and the fact that rehabilitation happens along and across every pathway of care, from birth to end of life.”

www.england.nhs.uk
• National narrative
• Breadth and scope
• Solutions to local challenges
• Service design, redevelopment and change
• Commissioning for outcomes to drive improvement
• Demonstrating effectiveness and value
• Needs based services
• Collaboration between commissioners and providers
Regional reports and CYP scoping report
8

www.england.nhs.uk
Focus on outcomes
Centred on people’s need
Aims high and gives hope
Active and enabling process
Integration core and specialist
Responding to change in need
We know what good looks like
9

www.england.nhs.uk
In conversation with commissioners:
10
Rehab is a priority as when it is not
done well, people often have more
admissions; business cases must
show the cost-savings associated
with good rehab e.g. admissions
avoidance”.
It would be great to be allowed the time to commission
rehabilitation correctly ……a Commissioning Framework is important to give support and confidence to commissioners”
“Relationships are hugely
important and
commissioners and
providers need to be
working collaboratively
This work is massively
important…. it is currently hit
and miss and there is so
much misunderstanding
about rehabilitation…”

www.england.nhs.uk
Physical
Sensory
Communication
Cognition and behavioural
Psychosocial and emotional
Medically unexplained symptoms
Mental health
Whole person & life course
11
Birth to end of life
including 1° and 2°
prevention

www.england.nhs.uk 12

www.england.nhs.uk
• Support to ensure children and young people have the best start in
life
• Control for patients and ability to self manage
• Reduction in demand for 1° and 2° care
• Prevention of admissions, readmissions and A&E visits
• Reduction in length of stay
• Increased QOL for people with long term conditions
• Support to enter and/or stay in employment
• Improved outcomes from surgical interventions
Why commission rehabilitation?
13

www.england.nhs.uk 14

www.england.nhs.uk
• Realise the potential of children and young people
• Enable people to return to work, get into work & stay in work
• Reduce costs of nursing, residential and social care
• Reduce associated costs of mental health illness
• Reduce costs associated with diabetic care
• Reduce length of stay costs
Economic benefits of rehabilitation
15

www.england.nhs.uk
People centred services
Use existing guidance and standards
Integrated services
Commission for the whole pathway
Transitions
Along pathways
Across sectors
CYP to adult
Check list:
16

www.england.nhs.uk 17

www.england.nhs.uk
Benchmarking, the principles & evidence
18

www.england.nhs.uk
Best Practice examples:

www.england.nhs.uk
WHO, World Bank and WCPT
“Rehabilitation is a good
investment because it builds
human capacity”

www.england.nhs.uk
Go to resource for Rehabilitation
21

www.england.nhs.uk
Acknowledgements and thanks:
Denise Ross, Rehabilitation Team
Vicky Whitfield, Rehabilitation Team
Laurie Palmer, Rehabilitation Team
Jayne Pye, Service User
Amy Frounks, Service User
Regional Rehabilitation Leads (2014-2015)
Commissioning Guidance Steering Group
Rehabilitation Programme Board

www.england.nhs.uk
Thankyou @Lindseyahughes
#improverehab16 #rehabimprovers
23

www.england.nhs.uk
Lynne Barr
Project Lead in Rehabilitation
North of England Commissioning Support

Partners in improving local health Slide 25
Rehabilitation:delivering
outcomes through
changing behaviours Masterclasses re: commissioning
Lynne Barr: Project Lead in Rehabilitation

Partners in improving local health
To engage those who influence commissioning in localities to understand what is possible through rehabilitation
To share the national direction, economic value and raise the challenges
To showcase some examples of recent developments across the region
To offer dialogue and an opportunity to discuss local challenges
Develop ‘top tips’ for north of England
Aims of Masterclasses x3

Partners in improving local health
Where does rehab fit in your
sphere of influence?
Unplanned
care
Long term
conditions
Planned care Continuing
care
Integrated
care
Transitions
Survivorship
Trauma Vocational

Partners in improving local health
• National evidence increasing – Economic return on investment
• Standard complexity score : RCS (various) from neuro to trauma .
• Continuing Health Care – personal budgets
• Cardiac and pulmonary (LTCs) primary care impact
• Self management : outcomes/person centred
• Digital support for assessments /reviews/value for money ( specialists)
• Local authorities and housing : joint working /under 55year olds
Context for commissioners

Partners in improving local health
Emerging models based on
• Trajectories for rehabilitation – Long term conditions ( progressive)
– Sudden onset (recovery)
• Barriers to attending rehabilitation
• Person centred outcomes
• Specialist /generic working in the
community Slide 29

Partners in improving local health
Examples :refer to
• Longterm conditions:
• Cardiac & pulmonary combined (stage 1)
• Pulmonary rehabilitation :person centred
• Community acquired brain injury
Slide 30

Partners in improving local health
‘Get Well Stay Well’: Case for change
• Co-morbidities
• Acceptability
• Industrialise / ‘at scale’
• Pro-active
• Psychological needs
• Preventable deaths
NHS Unclassified - Slide 31

Partners in improving local health
Menu based : domains of life
(GWSW and pulmonary rehab )

Partners in improving local health
Pulmonary rehab:redesigned
Goals & actions
Slide 33

Partners in improving local health
78% of participants felt more positive and less
depressed and anxious
Reflect on barriers to attending
rehabilitation: increase those able to
attend

Partners in improving local health
Person centred outcomes
Slide 35
*Outcome Star:Triangle consulting ltd

Partners in improving local health
Acquired Brain Injury :new
whole system pathway
onset/injury: clinical needs addressed.
Information /signposting /assessment
rehabilitation :specialist,
generic with ABI support, patient
peer support
connectivity with community/ services and
vocational goals
on going patient /family peer
support
36
Partners in improving local health
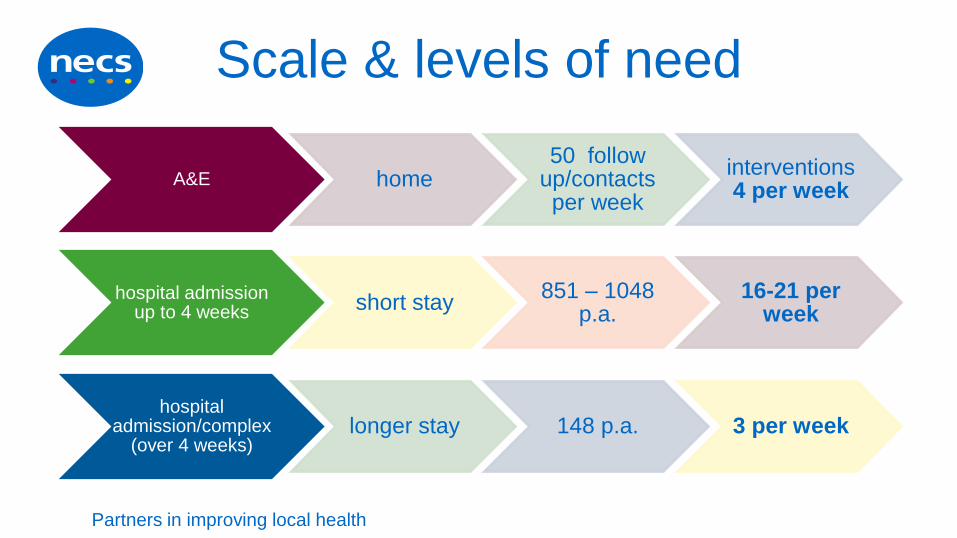
Scale & levels of need
A&E home 50 follow
up/contacts per week
interventions 4 per week
hospital admission up to 4 weeks short stay
851 – 1048 p.a.
16-21 per week
hospital admission/complex
(over 4 weeks) longer stay 148 p.a. 3 per week

Partners in improving local health
Opportunities through audit
• New ways of working – address issues raised over the years by people effected by ABI.
• Build bridges and support people with appropriate service to need ( one size does not fit all)
• Raise the profile of rehabilitation in localities including vocational outcomes/connection to local communities.
• Shift the balance of specialists established in community : build capability in community

Partners in improving local health
Outcome focus of masterclasses
• Top tips for commissioning (NECS)
• Network of interest established
• Knowledge hub (NECS)
• Sharing /distribution of information
• Commitment to action :KISS
– Individuals
– Commissioners
– Informing specifications/standard
• regional approach ?
Slide 39
Partners in improving local health
More to do !
• www.advancingpotential.co.uk
Slide 40

www.england.nhs.uk
Break
41
www.england.nhs.uk
Dr Helen Banks
Dr Ganesh Bavikatte
Alison Price
The Walton Centre
The Cheshire and Mersey Rehabilitation Network
42

The Cheshire and Mersey
Rehabilitation Network Dr Ganesh Bavikatte, Clinical Lead/Consultant in Rehabilitation Medicine, the Walton Centre
Mrs Alison Price, Manager, Cheshire and Mersey Rehabilitation Network
Dr Helen Banks, Consultant In Rehabilitation Medicine, The Walton Centre

CMRN Animation
https://www.youtube.com/watch?v=GSSnC
piDNCE

• National:
– BSRM, UKROC, Specialist rehabilitation service
specification standards with an increasing focus on
provision, access and quality of services.
• Regional:
– implementation of the Cheshire and Merseyside Major
Trauma Collaborative
The development of the Network; National and Regional Drivers
Co-ordinated Rehabilitation Pathway

Address unmet demand and inequitable provision for patients with
complex traumatic injury or illness
Establish a co-ordinated pathway, across hospital and
community services, based on need and not diagnosis
Deliver holistic specialist rehabilitation- multi-disciplinary team
approach
Promote an innovative network to optimise patients’ clinical
outcomes, improve experience and maximise independence
Driving Vocational Rehabilitation
Partnership working between health and social care
The development of the Network Local Drivers - Our Vision and USPs
Co-ordinated Rehabilitation Pathway

The Cheshire and Merseyside Rehabilitation Network (CMRN)
• 7 partner organisations across Cheshire and Merseyside and collaborative working region-wide for a wider scope of action than previously possible
• Funded by NHS England and Clinical Commissioning Groups
• Our region developing as the ‘go-to’ network for specialist rehabilitation
• Regional approach to improving health and delivering evidence-based specialist rehabilitation across inpatient and outpatient services
• Single structure to share and disseminate good practice and learning

Collaborative working region-wide
• Brain Injury Rehabilitation Centre
• Southport Spinal Injury Unit
• Cheshire and Mersey Major Trauma Collaborative
• Cheshire and Mersey Critical Care Network
• Aintree amputee and prosthetic services
• North West Assisstive Technology
• BIRT
• Headway, Neurosupport, SIA and other charitable organisations
• Isle of Man and North Wales specialist rehabilitation services

1. Establish A SERVICE PATHWAY
2. Deliver PATIENT FOCUSED services
3. Deliver COST EFFICIENT services
4. Attract and retain A HIGH CALIBRE WORKFORCE
5. Work in PARTNERSHIP to deliver High Quality Clinical
Audit, Research and Innovation and to drive
EXCELLENT PATIENT CARE
CMRN Objectives
Co-ordinated Rehabilitation Pathway

Rehabilitation Level 1A Supportive Rehabilitation
Rehabilitation Level 1A Supportive Rehabilitation
Rehabilitation Level 2 Active Rehabilitation
Rehabilitation Level 3 Extended Rehabilitation
Rehabilitation Level 3 Community
Hyper-Acute Unit Lipton Ward
The Walton Centre
Complex Rehabilitation Unit Sid Watkins Building
Rehabilitation Spoke Units Seddon Suite,
The Phoenix Centre, Clatterbridge, Walton Spoke
Health and Social Care Partnerships,
Oakvale Gardens
10
20
55
16
2 Locality teams St.Helens & Knowsley,
Liverpool, South Sefton, Southport & Formby
CCG’s
A Framework for Partnership and Collaboration

CMRN Services offered • Comprehensive therapy team
– Physiotherapy – Occupational therapy – Speech and Language therapy – Clinical and Neuro Psychology – Dietetics
• Rehabilitation consultants • Rehabilitation coordination team • Rehabilitation nurses • Vocational rehabilitation specialist • Mental health team
– Consultant Neuropsychiatrist – Mental health nurse – Liaison Psychiatry
• Links with orthotics, orthoptics, medical and surgical specialties

What is Quality in Rehabilitation?
1. Clinical Outcomes
2. Patient Experience
3. Patient Safety
4. Integrated Service
5. Governance
6. Values

Quality in Rehabilitation: 1. Clinical Outcomes
Based on rehab need not diagnosis
Individual SMART patient goals
Functional outcome and discharge destination
Cognitive education programme
Communication

Response Time 14+ Days 1-2 Days
8% 35% 8-14 Days
10%
3-7 Days
47% Average
6 Days
Quality in Rehabilitation: 1. Clinical Outcomes

Quality in Rehabilitation: 1. Clinical Outcomes

Quality in Rehabilitation: 1. Clinical Outcomes

Multi-Disciplinary Working and approach to deliver holistic rehabilitation
Patient Satisfaction
Family Involvement and Engagement
Communication
Quality in Rehabilitation: 2. Patient Experience

Quality in Rehabilitation: 2. Patient Experience – Multi-Disciplinary Working

Infection control measures
1:1 monitoring
Staff training
Monitoring of clinical interruptions
Communication
Quality in Rehabilitation: 3. Patient Safety

Whole pathway based on need not diagnosis Pathway delivered through partnership working across 7 organisations Joint working between health and social care Whole team approach in continuous review and on-going
development of services Annual work programme to support effective delivery of services and
implementation of strategies Staff experience – involvement, engagement and empowerment Communication
Quality in Rehabilitation: 4. Integrated Service

Whole pathway under one umbrella Rehabilitation Co-ordination Team Vocational Rehabilitation Model Dedicated clinical /neuro psychology and neuro psychiatry
provision Co-ordinated pathway from hospital to community Collaborative working with commissioners to support
development and delivery of specialist rehabilitation (e.g. Specifications/Standards, Research)
Quality in Rehabilitation: 4. Integrated Service – Our USP’s

Quality in Rehabilitation: 5. Governance

Continuous monitoring of quality, including: KPI’s Service Standards Agreed Criteria and Policies Standardised Medical, Nursing, Therapy Metrics UKROC National Data and Accreditation Research, Audit and Innovation Metrics Continuous Service Evaluation Training and Education Review Identification of gaps in K&S
development of accredited programme/modules in partnership with education establishment
Quality in Rehabilitation: 5. Governance
Working Together for Patients
- were always pulling together
Respect and Dignity
- we like to know what makes you tick
Empowerment
-were ready to pass the baton
Quality in Rehabilitation: 6. Values

Quality in Rehabilitation: 6. Values
Commitment to Quality and Care
- we believe in going the extra mile
Compassion and Empathy
- we put ourselves in your shoes
Honesty and Trust
- we promote transparency

Inequitable provision of spoke, extended and community specialist rehabilitation services for Cheshire patients
Changing commissioning landscape and financial sustainability/tariff
Delays in discharges and pathway transfers Management of realistic patient and family
expectations
Challenges to Quality in Rehabilitation
Commissioning: Collaborative review of our service specifications/standards
Clinical Tools: Development of outcome measures for community
Research and Innovation: Collaborative studies in hyper acute rehabilitation, vocational rehabilitation, community rehabilitation, virtual reality
Education: Collaborative Education Programme accessible for all disciplines/grades
Next Steps: Quality Initiatives in Rehabilitation
2016/17

Cost-efficiency of specialist hyper-acute inpatient rehabilitation services for medically unstable patients.
Objectives: To evaluate functional outcomes, care needs and cost-efficiency of hyper-acute rehabilitation for a cohort of inpatients with complex neurological disability and unstable medical/surgical conditions.
Design: A multicentre cohort analysis of prospectively-collected clinical data from the UK Rehabilitation Outcomes Collaborative(UKROC) national clinical database, 2012-2015.
Conclusions: Despite its relatively high initial cost, specialist hyper-acute rehabilitation can be highly cost-efficient, producing substantial savings in on-going care costs, and relieving pressure in the acute care services.

Patient experience
https://www.youtube.com/watch?v=jhEhrZ4R2Gc

Summary R - Regional co-ordinated pathway across a
whole systems model of care
E - Clinically effective and cost efficient
H - Holistic, person-centred approach
A - Achievement of regional and national
specialist rehabilitation standards
B - Based on rehabilitation needs, not diagnosis

Thank you
Any Questions?

www.england.nhs.uk
Lunch

www.england.nhs.uk
A. Children and young people's rehabilitation (Met 15)
B. Regional rehabilitation networks - supporting regional service
development (main room)
C. New Care models - regional vanguard(s) (Met 16)
D. Data sets and outcome measures - demonstrating effectiveness
(Met 17)
Workshops
74

www.england.nhs.uk
Reflection and Actions
75
• Key learning points from today’s conference.
• How will today’s conference change my practice / approach?
• Key tasks as an outcome from today’s conference.

www.england.nhs.uk
Final comments
and
closing remarks
Shelagh Morris
Deputy Chief Allied Health Professions Officer
76

www.england.nhs.uk
Thank you
77