im&t strategy - whatdotheyknow.com€¦ · web viewepsom and st helier university. nhs trust....
TRANSCRIPT

Page 1 of 48 document.docx

Epsom and St Helier UniversityNHS Trust
Information Management &Technology Strategy2014-19
Page 2 of 48 document.docx

Version No: 1.0Approved by TEC: 19/03/2014Issue Date: 19/03/2014
Page 3 of 48 document.docx
Page 4 of 48 document.docx

Table of Contents
1 EXECUTIVE SUMMARY.....................................................................................................................................................................................................5
1.1 OUR VISION:..........................................................................................................................................................................................................7
1.2 OUR OBJECTIVES:...............................................................................................................................................................................................7
2 SECTION ONE: THE VISION..............................................................................................................................................................................................8
2.1 INTRODUCTION....................................................................................................................................................................................................8
2.2 STRATEGIC DIRECTIONS....................................................................................................................................................................................8
2.3 VISION....................................................................................................................................................................................................................9
2.3.1 WHAT THIS MEANS FOR PATIENTS..........................................................................................................................................................12
2.3.2 WHAT THIS MEANS FOR CLINICIANS AND STAFF..................................................................................................................................12
2.3.3 WHAT THIS MEANS FOR GPS....................................................................................................................................................................12
2.3.4 WHAT THIS MEANS FOR TERTIARY SOCIAL CARE.................................................................................................................................12
2.4 THE BLUEPRINT FOR IM&T...............................................................................................................................................................................13
2.4.1 THE INTEGRATED DIGITAL CARE RECORD (IDCR).................................................................................................................................13
2.4.2 THE CLINICAL PORTAL...............................................................................................................................................................................14
2.4.3 ELECTRONIC PATIENT RECORD (EPR) – iCM..........................................................................................................................................14
2.4.4 ELECTRONIC PRESCRIBING......................................................................................................................................................................15
2.4.5 ELECTRONIC DOCUMENT MANAGEMENT (EDM)....................................................................................................................................15
2.4.6 RADIO FREQUENCY IDENTIFICATION (RFID)..........................................................................................................................................16
2.4.7 TELEPHONY.................................................................................................................................................................................................17
2.4.8 WIRELESS & MOBILE TECHNOLOGY........................................................................................................................................................18
2.4.9 INFORMATION MANAGEMENT...................................................................................................................................................................18
2.4.10 ADMINISTRATIVE SYSTEMS................................................................................................................................................................19
2.4.11 OVERALL STRATEGIC BENEFITS.......................................................................................................................................................20
3 SECTION TWO: CURRENT POSITION............................................................................................................................................................................21
3.1 INFRASTRUCTURE.............................................................................................................................................................................................21
3.2 SYSTEMS.............................................................................................................................................................................................................22
3.3 SIGNIFICANT PROJECTS 2013/14.....................................................................................................................................................................23
3.4 EXISTING PROJECTS.........................................................................................................................................................................................24
4 SECTION THREE: COMPOSITION OF THE PROGRAMME...........................................................................................................................................26
4.1 CLINICAL APPLICATION SYSTEMS..................................................................................................................................................................26
4.2 ADMINISTRATION APPLICATION SYSTEMS....................................................................................................................................................27
4.3 INFORMATION MANAGEMENT..........................................................................................................................................................................27
4.4 IT INFRASTRUCTURE AND NETWORKS..........................................................................................................................................................27
5 SECTION FOUR: PROJECTS...........................................................................................................................................................................................29
5.1 2014/19 PROJECTS............................................................................................................................................................................................29
6 CHALLENGES...................................................................................................................................................................................................................35
7 CHANGE MANAGEMENT.................................................................................................................................................................................................36
8 EDUCATION, TRAINING AND DEVELOPMENT..............................................................................................................................................................37
9 GOVERNANCE.................................................................................................................................................................................................................37
10 COSTS...............................................................................................................................................................................................................................38
11 CONCLUSION...................................................................................................................................................................................................................38
12 APPENDIX A: TRUST CORPORATE OBJECTIVES – 2013/14.......................................................................................................................................40
13 APPENDIX B: DEFINITIONS.............................................................................................................................................................................................42
14 APPENDIX C: INVESTMENT COSTS...............................................................................................................................................................................43
15 APPENDIX D: INDICATIVE IMPLEMENTATION PROGRAMME.....................................................................................................................................44
16 APPENDIX E: EQUALITY IMPACT ASSESSMENT.........................................................................................................................................................45
17 APPENDIX F: REFERENCE DOCUMENTS.....................................................................................................................................................................47
Page 5 of 48 document.docx
18 APPENDIX G: POLICIES..................................................................................................................................................................................................48
1 EXECUTIVE SUMMARY
To achieve a paperless journey by 2018 through the use of enhanced technology, whilst enhancing and improving the quality and safety of services to patients. Our strategy will be at the core of everything we do; the strive to continually improve the effectiveness, efficiency and accessibility of our services, to be the first choice for patients and to ensure future affordability and clinical sustainability. Our staff skillset, knowledge and resources will be developed to facilitate the delivery of excellent patient care through the use of enhanced technology.
The IMT Strategy provides a 5 year strategic framework supporting the Trust’s infrastructure to develop its information, systems and technology, which will ultimately lead to a paperless journey through enhanced technology by 2018.
The strategy is in line with the NHS Information Strategy “The Power of Information: putting us in control of the health and care information we need”1.
The journey to achieving a paperless service will involve implementing the key priorities over the next five years;
a) Implementing the Integrated Digital Care Record (IDCR) across the organisation in 2014/15/16To use digital technology to ensure that vital patient information and clinical decision and support tools can be viewed by an authorised user in a joined up manner in any single instance.
b) Electronic Document Management (EDM) to Deliver Digitised NotesThe implementation of an EDM solution which will allow for the digitising of notes which is fundamental to patient safety. Given the multiple specialist notes that are routinely created for the same patients; the only way a unified record will be achieved is if the notes are all digitised.
c) Robust Infrastructure including single sign‐on and mobile computingThe Trust has a technical infrastructure that supports digital imaging across the corporate network. This will need to be enhanced with additional infrastructure but is a firm foundation for the future. Over the next year the key developments will be the continued improvements to the network including a new core on both sites, increased use of Virtual Desktop Infrastructure (VDI) leading to improved mobile bedside access for staff and upgrading of the Trust’s storage. The strategy for mobile devices will be explored based on experience of clinical use, combined with the technical assessment on security and cost.
1 Putting Patients First: The NHS England business plan for 2013/14 - 2015/16
Page 6 of 48 document.docx
d) Electronic prescribingWork is being undertaken to develop a work plan for 2014/15/16 to implement electronic prescribing and medicine administration, expanding the use of our Electronic Patient Record (EPR) system.
e) Replacing historic systems, including Picture Archiving Communication System (PACS)PACS is provided via the National Programme for IT (NPfIT), whose contracts expire in 2014. The exit strategy is now underway with the repatriation of images and planning for re-procurement to replace this system begins in 2014. Given the life span of this strategy there may be other systems that require renewal before its completion
f) A robust Data WarehouseThe development of the Trust’s data warehouse will provide a single repository for corporate data, delivering a robust and trusted source for information. It will also enable monitoring of performance at all levels supporting operational service delivery.
g) Information sharing and whole system workingThe development of agreed ways for working to support information sharing across the health and social care systems and new models of care advocated through the commissioning channels.
The strategy will align IM&T developments with the Trust’s overall objectives, clinical operations, Directorate business plans and the clinical strategy, detailing the governance arrangements underpinning further investment in IM&T. Maximum benefits will only be derived if the Trust continues to adapt its culture to fully adopt technology, requiring commitment at all levels across the organisation. In addition, adequate financial investment is required over the next 5 years to ensure that the fundamentals are right from the onset. This will require: robust scalable IT Infrastructure that delivers information where staff need it; sound information governance arrangements owned by staff operating within the
Trust; high quality information management; training and development of IT skills in staff; sound project management and procurement; robust and successful change management; working in collaboration with other NHS organisations and social care
The outline programme identifies the milestones over the next 5 years. Given the many uncertainties, especially in relation to products and services, this should be seen as work in progress. A five year capital plan has been developed for IT capital and revenue with further work expected as each business case develops.
Page 7 of 48 document.docx
1.1 OUR VISION:Vision statement leading to a paperless journey by 2018:
“To create a digitally integrated care organisation that provides secure-on-line access to the right information, to the right person, to the right place. Using information systems built on innovative and integrated solutions and local decision making, within a framework of national standards that ensures that information can move freely safety and securely around both Trust and local systems.”
This paper sets out how the use of enhanced technology will be used to develop information, systems and technology to support the Trust achieving a paperless journey by 2018. The strategy provides a vision of being the healthcare provider of choice for our local populations and our commissioners, providing exemplary high quality, safe, accessible and compassionate care to the people of Sutton, Surrey Downs, Merton and surrounding areas.
1.2 OUR OBJECTIVES:Strategic Objectives IM&T Support for this ObjectiveOur patients – improving our patient experience and outcomes
Through the use of technology patients will have access to their information, allowing them to make informed decisions regarding their care
Our Clinicians – improving access to quality real-time data
Clinicians will have with the right information at the right time at the right place to make clinical decisions.
Our services – improving the quality of our services
Through the use of data collected locally and nationally, supported by joint working between Trust Information, IT teams and Clinical Operations
Our people – developing an increasingly motivated and flexible workforce
Through the use of enhanced technology and systems to capture and access information digitally ensuring the right information is available when required to support clinical best practice.
Our finances – eliminating our deficit and moving to a position of sustained annual surplus
Through the integration of the clinical, business and information systems, providing a robust information provision to support the development of quality and cost improvement programmes. This will include understanding areas of opportunity for reducing the Trust’s deficit.
Our partners – improving our understanding of the populations
Through appropriate data sharing and facilitation to support rapid diagnosis utilising systems and
Page 8 of 48 document.docx
we serve and how we can best meet their needs and determining a long-term future for our hospitals
networking, with clinical decision support that promotes integrated system wide working.
2 SECTION ONE: THE VISION
2.1 INTRODUCTIONIn line with the National Health Service Information Strategy “The Power of Information: putting us in control of the health and care information we need”2, the ESH IM&T strategy focuses on clinical information systems, the culture surrounding real-time data entry by clinicians and a supporting infrastructure to enable this. The Trust’s IM&T department will develop the information, systems and technology to support the Trusts clinical vision in being the healthcare provider of choice for our local populations and our commissioners, providing exemplary high quality, safe, accessible and compassionate care. This strategic framework has the main objective of meeting healthcare priorities and achieving a paperless patient journey by 2018.
2.2 STRATEGIC DIRECTIONSAchieving a paperless journey by 2018 and improving the quality and safety of services to patients will be at the core of everything we do. The strive to continually improve the effectiveness, efficiency and accessibility of our services, to be the first choice for patients and to ensure its future affordability and clinical sustainability, and to be a centre of excellence for research and teaching. In order to develop the organisation to meet its strategic intentions we have an Organisational Development Strategy based on a strong set of values, a culture that puts the patient at the heart of all we do and a leadership ethos that leads the organisation as one team to continually improve its services to patients. The development of the IMT Strategy supports the culture of patients being at the heart of all we do and develops our staff with the skills, knowledge and resources to deliver excellent patient care through enhanced technology.
The direction for the IM&T Strategy is therefore set by:
the Clinical Operations directorate business plans
the Trusts corporate objectives 2013/14 (Appendix A)
the Clinical Strategy (once concluded)
2.3 VISIONThe vision for IM&T is: supporting patient care through the use of technology by making information readily
available and accessible for both the patients and clinicians2 Putting Patients First: The NHS England business plan for 2013/14 - 2015/16Page 9 of 48 document.docx
supporting clinicians and other staff to make patient care safer and more efficient, through the use of enhanced technology
achieving paperless patient journeys by 2018 thorough an enhanced use of iCM, EDM and other linked clinical information systems, accessed via one view using the clinical portal by 2018
having an information culture which regards digital capture and storage, data quality, information sharing and knowledge management as essential parts of clinical, business and operational processes to improve the care delivered to patients, both within the Trust and the wider Health Economy
building on the robust infrastructure that will support the Trust’s need, now and into the future.
Page 10 of 48 document.docx
There are a number of values that underpin this strategic vision:-
Function PrincipleInformation Patient based
Derived from existing and future operational systems
Compliant with information governance standards Available when and where required Captured only once Information used to drive integrated care across the
entire health and social care sector, both within and between organisations.
Technology Proven to minimise risk At the forefront of modern systems Integrated for once only data capture Compliant with NHS and industry standards Support carbon reduction strategy Mobile, clearly targeted for use at point of care
Staff Access to training & tools to maximise the IT benefits
Sufficient IT skills and resources Available to implement and support new systems Able to share and impart knowledge
Culture Enhancing management information to facilitate the most effective use of resources
Aligning and integrating clinical and business information systems to enable informed organisational decisions to be made
Migrating the Trust towards an electronic communications environment to reduce reliance on paper records and documents
Information regarded as a health and care service in its own right – with appropriate support in using information available for those who need it, so that information benefits everyone and helps reduce inequalities
Electronic care records progressively become the source for core information used to improve care, improve services and to inform research
Page 11 of 48 document.docx

2.3.1 WHAT THIS MEANS FOR PATIENTSPatients will be able to interact with those caring for them including requesting changes to their bookings and receiving appointment reminders by SMS, voice mail, or email. They will be able to add or amend the information stored on them. Patients will use self-check-in kiosks to register their arrival using bar-coded patient letters. Integrated screen-based calling systems will direct patients to waiting areas and into consulting rooms. Kiosks may be used to survey the patient experience or gather information around on going conditions.
Ultimately, patients will benefit from a Personal Health Record (PHR), in line with national guidance. They will be given access to summary health data via a patient portal, accessible via any internet connection. This will enable patients to share with other health professionals involved in their care, essential information such as medications, clinical letters, medical history, diagnoses, scheduled appointments and test results. It is anticipated that by 2018/19, patients will have access to their records held by the Trust.
2.3.2 WHAT THIS MEANS FOR CLINICIANS AND STAFFThere will be improved real‐time communication between clinicians and teams, supporting medical, nursing and other clinicians’ handovers, “hospital at night”, rapid response teams and others. There will be better informed, more timely and “remote” decision making as paper dependence/constraints removed. Clinical care will be further enhanced by the integration of results of patients’ vital signs to deliver a patient status index, which will forewarn critical events and alert relevant clinicians in real‐time. The removal of the paper record (by legacy and day forward scanning) eliminates large volumes of administrative work, and prevents wasted clinic visits as a result of missing notes.
2.3.3 WHAT THIS MEANS FOR GPSGPs will have timely access to information enabling shared patient care between organisations via enhanced use of technology with firm governance agreements in place. This will build on the success of the developments to date such as electronic sending of clinical documentation between ESH and the GPs since 2009 for a range of correspondence including discharge summaries, safeguarding information, clinic letters, and results, greatly improving timeliness of information and efficiency. In addition to this, GPs are also able to order diagnostic imaging and pathology tests electronically, complimenting the existing results web viewing service for diagnostic imaging and pathology results where they also have access to test results on their patients requested by our clinicians. This will enhance their local IDCRs as well as reducing the number of tests that are not required.
2.3.4 WHAT THIS MEANS FOR TERTIARY SOCIAL CAREEnhanced technology use will also be extended to tertiary social care where there will be timely access to information enabling shared patient care between organisations.
Page 12 of 48 document.docx

The governance arrangements for this will need to be developed and agreed between organisations. This expands on the electronic communication developments which are already in place for tertiary social care (for specialist referrals) with automatic generation of emails to Social Services, other Trusts, and Physiotherapy. This will also be expanded to other social care organisations, such as specialist Trusts and mental health. The use of electronic communications has been raised continually through the improving patient flow and discharge programmes, and a system that allows improved sharing of information in a timely manner would significantly improve care planning and reduce length of stay.
2.4 THE BLUEPRINT FOR IM&TThis section describes the development of the vision and the framework for the next five years building on the current EPR and infrastructure, whilst implementing new technologies including: Radio Frequency Identification (RFID) tagging, Document Management and Portal solutions to benefit patients and clinicians to support paperless working by 2018.
ELECTRONIC DOCUMENT
MANAGEMENT (EDM)
THE CLINICAL PORTAL
PATIENT HEALTH RECORD AND
PATIENT PORTAL
ADMINISTRATIVE SYSTEMS
WIRELESS & MOBILE TECHNOLOGY
THE INTEGRATED DIGITAL CARE RECORD
(IDCR)
INFORMATION MANAGEMENT
PATIENTS GPs
Ena
bler
sP
orta
lsIn
form
atio
n
TERTIARY SOCIAL CARE
STAFF
Cus
tom
ers
2.4.1 THE INTEGRATED DIGITAL CARE RECORD (IDCR)NHS England has released guidance for trusts to achieve fully integrated digital care records across all care settings by 2018. 'Safer Hospitals Safer Wards: Achieving an integrated digital care record', sets out the benefits case for adopting safe digital record keeping as a precursor to achieving integrated digital care records across the health and care system. It describes an IDCR as the ability of local health and care services to use digital technology to ensure that vital patient related information and clinical decision and support tools can be viewed by an authorised user in a joined up manner in any single instance.
At the heart of this vision, is the development of an IDCR for the Trust by creating a Clinical Portal, making best use of modern and current technology to provide one view of the patients’ clinical and administrative data. The Trust already benefits from clinicians who are well versed with using iCM and departmental systems. The Clinical Portal will provide one view for any patient data which is digitally stored, available and accessible immediately from anywhere on site. This technology will also be developed to provide links to GPs, patients and tertiary care. This system will support current
Page 13 of 48 document.docx
service transformation programmes working towards improved communication across organisational boundaries.
The use of NHS Number as the national patient identifier for systems and all cross boundary communications has been mandated by National Patient Safety Agency3. This has been further supported in the NHS England Business Plan for 2013/14 – 2015/64. The Trust already uses the NHS Number for cross boundary communications and will continue to expand its current programme of work to extend the use of NHS Numbers locally.
2.4.2 THE CLINICAL PORTAL
The clinical portal will provide a single integrated view of patient information accessible anywhere within the Trust, and potentially extending beyond Trust boundaries for use in the community and social care. This will provide clinicians views to information from: iCM EDM Patient Administration System (Patient Manager – iPM) Key departmental systems historically can only be accessed by individual
departments- Renal- Pathology- Radiology- Maternity- Cancer- Diabetes Management- EOC Theatre scheduling
The clinicians will also be able to launch any of the underpinning systems from the clinical portal with single sign-on and context management. This will be developed to support digital capture for specific clinical workflow working with mobile technology. The development could then be extended to work off-site. The progress of this project is subject to capital bid approval. Full programme of timescales can be seen in Appendix D.
2.4.3 ELECTRONIC PATIENT RECORD (EPR) – iCM
The Trust’s iCM is a fully functional EPR with: full order communications and results reporting for Pathology and Radiology
including any tests originating from the GPs inpatient TTO and OPD prescribing discharge letters clinic letters3 Risk to patient safety of not using the NHS Number as the national identifier for all patients [NPSA/2009/SPN002]
4 Putting Patients First: The NHS England business plan for 2013/14 - 2015/16
Page 14 of 48 document.docx
capture of CQUIN data such as VTE and Dementia Other orderable services such as Physiotherapy, Social Services etc.
It is envisaged that these functions will remain within iCM with information being viewed via the portal and when required, clinicians will have the ability to launch iCM from the portal directly to the patient’s record.
2.4.4 ELECTRONIC PRESCRIBING
The Trust will be expanding the use of iCM by deploying the inpatient prescribing and medicines administration in 2014/15/16 Trust wide. This project will make a significant impact on clinical staff and patient care. Medicines will be prescribed using wireless devices and computers on wheels which will also be employed during drug rounds where the nursing staff administering medicines can get clear and easy to access information for each patient, checking off each dose at the bedside.
The absence of hand-written prescriptions and the built in decision support reduces the risk of medication error as well as ensuring accurate communication about patients’ medication across the various health sectors. This will also reduce the risk of giving the wrong drug to the wrong patient, enabling the response to treatments to be recorded in relation to the treatment provided thereby supporting best practice. The system will allow for better surveillance of medicines usage across the Trust
2.4.5 ELECTRONIC DOCUMENT MANAGEMENT (EDM)
Another component of IDCR will be the Electronic Document Management (EDM) system with an underpinning wireless network, enabling the majority of patients to be treated through a paperless process. The majority of information in the EDM will be collected via the clinical process and other hospital systems. Clinicians will have access to all necessary patient information via single logons and will have remote access to hospital systems to enable them to work from community locations or from home, if required. This will be further enhanced by the expansion of the RFID technology to include scanning.
Deploying clinical documentation entry functionality within EDM (structured notes and forms such as nursing assessments, progress notes and care plans) will enhance clinical workflow and reduce paper administration. Clinicians will be able to check their clinic letters in the outsource transcription systems and these letters will be exported directly into the EDM and processed for sending to GPs. This will help improve the efficiency, quality and timeliness of clinical correspondence, as well as complimenting clinical documentation further to enhance the IDCR.
Clinicians will have access to patients’ comprehensive information (including previous medical history) readily available on readmission, facilitating more rapid diagnosis and treatment. This will enable closer management of care pathways which will improve patient safety and enable more consistent care planning, contributing towards reductions in length of stay. Moving towards paperless records will release time to care and therefore result in improved outcomes for patients.
Page 15 of 48 document.docx

Additionally, this will support the Trust’s improvement programmes based on evidence based practice for ‘Early identification, specialist assessment and intervention’ which adopts a model to support patients as soon as they arrive in hospital. Recently the Trust has established Enhanced Older People’s and Respiratory teams to in-reach to ED and support patients to return home as appropriate, availability of this information would be of benefit to these teams. Furthermore the Trust is currently enhancing Ambulatory Care services and the availability of information would significantly improve this service.
The EDM deployment will enhance the existing repository of documents allowing clinicians the ability to annotate and bookmark key documents for their review. In addition to this, they will also have the ability to export these documents onto laptops to support their off-site working practices and these documents can be synchronised back into the EDM when they return back to the Trust.
This will be followed by the deployment of clinical documentation for structured notes and forms such as nursing assessments, progress notes and care plans. This will support clinicians to capture information digitally which will be accessible 24/7. A full programme of timescales can be seen in Appendix D.
EDM enables scanning legacy paper records into digital storage with appropriate indexing to enable easy context-sensitive retrieval. The initial focus will be patient case notes, the secondary focus will be on services such as personnel and corporate records. This will enable historical case notes to be viewed alongside contemporaneous digital data for a single patient. A proportion of existing case notes will be scanned first, followed by “scan on demand”, which will allow any remaining legacy paper records to be scanned and added to the patient record when requested from an in-house library or off-site storage. By 2017-18 the Trust will have suitable technology in place to capture documentation, digitally removing the requirement for paper and allowing the Trust’s transition to paperless working in line with the NHS initiative to be paperless by 2018. Legacy paper records for long term complex cases would be retained in paper format in line with the Trust retention standards.
2.4.6 RADIO FREQUENCY IDENTIFICATION (RFID)During 2013/14 the Trust has successfully implemented an RFID tracking system for Health Records, which enables the tracking of health record around the multiple Trust sites and supports Health Records in delivering efficiencies with filing of paper case notes in the libraries. The use of RFID will enable the identification of the top 20% of records in use which could then be scanned into the EDM system, enabling the Trust to start the journey of having paperless records by 2018.
The expansion and uptake of the Radio Frequency Identification has huge potential to include:
Asset tracking such as bed, mattress Supplies and batch management Workforce management Patient location tracking for higher risk patients such as babies or dementia Integrated communications
Page 16 of 48 document.docx

Pathology process management Opportunities to link assets (beds, pumps, mattresses) to patients
2.4.7 TELEPHONYIM&T will be working with the Estate team to evaluate the Trusts future telephony requirements prior to the contract expiring in 2017/18. The review will also look at how flexible working practices can be accommodated. Legacy telephony systems cannot leverage the benefits of a wired and wireless IP network. Modern telephony/unified communications systems will give the Trust the ability to adapt to the changing needs of the organisation in a timely manner, taking advantage of desk to desk video calls, messenger chat, and social mediums.
Page 17 of 48 document.docx
2.4.8 WIRELESS & MOBILE TECHNOLOGYThe expansion of the existing wireless network will support the Trust in achieving its vision of providing access to clinical information at the point of patient care and will allow clinicians to retrieve and enter data at the bedside. This will support the use of Bar-Coding and Radio Frequency Identification technologies to improve healthcare by using systems to match patients to their care resulting in real improvements to patient safety, ensuring that progress through the patient journey can be monitored and delays minimised, and cash-releasing savings generated.
The over-riding principle for mobile technology will be to improve timeliness and efficiency delivering enhanced decision support to ensure high levels of patient safety and experience. This approach to utilising technology at the point of care has been recognised at other Trusts to improve efficiency in managing patient pathways. Significant benefits can be achieved in reducing time to ordering of diagnostics and TTOs and therefore resulting in reduced length of stay for our patients.
The mobile technologies will include:
laptops mounted on trolleys to facilitate ward rounds with point of care order communications and prescribing. Doctors and nurses will also be able to view clinical data and undertake clinical tasks such as medicines administration.
handheld tablets to facilitate discussions with patients including the capture, sign off, e.g. for consent and real-time information to support clinical decision making. This will include enabling nurses to input patient observations at the bedside.
In addition to the above, the wireless and mobile technology will support the implementation of technology (subject to a successful outcome from the Nursing Technology Fund application) and software to enable the recording of inpatient observation at the bedside to enable rapid alerting of patients who may be deteriorating. The rapid identification of this cohort of patients will lead to a reduction in length of stay, mortality and admissions to intensive care. The outcome of this project is dependent on the success of the technology fund bid and could be implemented alongside Phase 1 (Section Four) with separate project staff.
Communication throughout the hospital will be enhanced by voice-operated communication devices (a modern substitute for telephones and bleeps) enabling staff to speak directly to one another, to contact the nearest porter, for example, to ask a colleague for assistance without leaving the patient and to enable patients to speak directly to their named nurse. Incident management can be improved via the same system. The implementation of this programme will commence in 2015.
2.4.9 INFORMATION MANAGEMENTA Trust Information Strategy is currently being written as a companion document to this paper. The Trust will build on its current “information culture”, in which decisions are evidence-based and supported by appropriate information at all levels – operational, clinical, managerial and executive. A consistent, robust information provision will be expanded upon to provide reactive, predictive, real-time and comprehensive information
Page 18 of 48 document.docx

services that support the delivery of high quality patient care and improved clinical outcomes.
Management information will be derived from clinical and operational processes. This is currently supported by a centralised data warehouse, fed from interfaced clinical systems, with all information related back to a patient. The current data warehouse will be replaced by an in-house built data warehouse in 2014/15, as the current vendor will no longer provide support.
Both patients and NHS staff increasingly expect to receive information in modern and easy to use environments including web based front ends and mobile technology. The Trust will build on the development of an in-house data warehouse to review business intelligence software so that it is fit for purpose meeting both corporate and user specific expectations. This translates into information that is:
transparent and shared;
owned by those that need to use it;
consistent, reliable and of a suitable quality
provided in context (e.g. with finance & activity information presented together);
comparable with peer organisations to support best practice;
timely – better able to support proactive decision making;
effectively analysed and easy to understand / interpret;
automated, with reduced reliance on expert workarounds
2.4.10 ADMINISTRATIVE SYSTEMSThe upgrade of electronic rostering (e-rostering) for nursing will make monitoring of safe staffing levels easier and support effective staff deployment, generating savings through minimising the need for more expensive temporary or agency staff and allowing a Trust-wide view of staff availability on any day. This will be expanded to include deployment to doctors as the functionality becomes available.
In conjunction with the procurement team, just-in-time procurement will be considered. This potentially will generate cost savings through economies of scale and more strategic sourcing.
EDM could be expanded at a small cost to areas such as personnel and corporate records as the Trust has already invested in a solution for clinical use.
There is a current programme of work to migrate the existing GroupWise email system to Microsoft Exchange, with completion expected in 2014. Alongside this, there is a project currently underway to deploy Windows 7 and Office 2010 Trust wide. In the next 5 years it is widely expected that Windows and Office products will have evolved significantly leading to the requirement of further upgrade.
Page 19 of 48 document.docx
With the Trust’s ambition to expand communication using social mediums, Information Services will need to provide assurances that Trust’s systems are used appropriately. Systems will be purchased to support this.
To further support the cross-site working between Trust sites and other organisations, the video conference hardware will be upgraded.
2.4.11 OVERALL STRATEGIC BENEFITS Stable and available Information and Communications Technologies (ICT)
infrastructure
Measurable and reportable change management
Managing effectiveness through standard processes and polices
Improved productivity and satisfaction levels
Easily accessible information for business intelligence purposes
Partnerships aligned to the strategy
Page 20 of 48 document.docx

3 SECTION TWO: CURRENT POSITION
This section describes the current position of IM&T infrastructure and core systems, and gives an overview of the teams who support these within the Trust. This also includes a summary of the significant projects undertaken in 2013/14 which will support the journey of being paperless as well as the Trust’s clinical vision to be the healthcare provider of choice for our local populations and our commissioners. The Information Services Directorate supports the infrastructure and core clinical systems such as iPM and iCM. It also supports the core systems such as Email and file storage Departmental systems i.e. Pathology, Radiology, Renal, Maternity Pharmacy, EOC and Finance/HR, these are managed by application managers within individual clinical directorates.
The Trusts current IM&T infrastructure and systems cannot be utilised to their full potential due to the age of the existing core network that is in place. The current infrastructure limits the Trusts ability to implement modern solutions, such as Single Sign On, Virtual Desktop and mobile working, which would support better patient experience, improve efficiencies for staff and promote paper light working.
An upgrade of the core network will improve overall performance for users from logging on to accessing systems. In addition to this there will be increased reliability, with more robust business continuity.
3.1 INFRASTRUCTUREThe IM&T infrastructure at the Trust comprises currently of: A wired local area network (LAN) based on Alcatel technology on each site. Epsom
and St Helier are connected by an aggregated 1 Gb (Microwave) backed up by a 100 Mb resilient microwave which is in turn backed up by a 15 Mb link across the N3 network, Sutton is linked to St Helier by a 640 Mb (Microwave) link backed up by a 100 Mb microwave link
A wireless network based on Alcatel technology, which is connected to the LAN. connection to the rest of the NHS is via the N3 wide area network (WAN) and then to
the internet circa 150 separate servers on the LAN which host the application systems a virtualised server environment is in place (170 virtual servers running on 23 of the
150 physical servers), saving capital, power and space and contributing to protecting the environment
over 3000 separate devices on the LAN which enable staff to access systems –these are a combination of PCs, laptops and some iPad devices for mobile access; and over 800 printers
a remote access solution enabling connection to the systems from other sites, including home
Microsoft-based operating systems
Page 21 of 48 document.docx

3.2 SYSTEMSThe iCM system was deployed in 1996 and is currently undergoing a complete hardware refresh in 2013. This is a mature EPR system with: order communications and results reporting for Pathology and Radiology inpatient TTO and OPD prescribing discharge letters clinic letters capture of CQUIN data such as VTE and Dementia other services which are orderable (including Physiotherapy, Social Services, Hand
Therapy referrals) from clinical areas which either print in the receiving department or sent via email if they are off site
access to over 3.5 million documents including referral letters, Emergency Department casualty cards, Safe Guarding Information, departmental discharge summaries and scans.
The Patient Administration System (iPM) was deployed in 2005 and has: integrated Emergency department module integrated Theatres and scheduling modules alerts for patients administrative CQUIN/KPI data such as learning difficulties and discharge planning.
Both the iCM and iPM systems were part of the National Programme for Information Technology (NPfIT). The contracts were renewed directly with the Trusts in 2011 for a further five years. These systems are fully managed services provided by a single vendor for both hardware and software support and maintenance 24/7. The iCM system is hosted on site at the Trust’s Data Centre at St Helier and iPM is hosted off site at Sevenoaks. The different hosted environment has resulted in varying degrees of technical ability at the Trust in supporting both applications. Historically, the iCM system in the Trust has a stronger technical team who support the internal hardware. This team works alongside the vendor. Going forward, the skillsets will need to be reviewed to ensure they are fit for purpose as part of the 2015 PAS/EPR strategy review.
The options appraisal for these systems will need to be undertaken in 2014 and a paper will be presented to the Operational Management Group (OMG) in January 2015.
The 2010-12 Strategy has made some progress on the paperless patient journey to support the creation of the IDCR. These include: Transmitting discharge summaries and other clinical documents to GPs
electronically; Transmitting referrals to other organisations electronically; Making the results of tests requested by GPs available in iCM Additional alerts to support child protection with the iCM and PAS systems Printed barcoded wristbands; New functionality to support VTE assessments; New functionality to support Dementia Assessments; New Discharge Summary system using Infopath and Sharepoint with TTO
integration into iCMPage 22 of 48 document.docx
Creating a document repository for clinical documentation accessed from iCM ranging from discharge summaries, referral letters, ED casualty cards to scanned images such as cardiology investigations [>3.5 million as at January 2014];
Pilot of a in-house enhancement to iCM for Results Acknowledgement; Creating of interfaces to departmental systems for demographic feeds; Implementation of a clinic letter generation product which is integrated with iCM; Image Exchange Protocol (IEP) for exchanging images between organisations; Deploying Hypercube, an information reporting tool to managers and clinicians to
provide the organisation with the tools to use information to promote proactive management rather than react after the event.
iCM and iPM are interfaced with a key suite of major departmental systems (Pathology, Radiology/Picture Archiving Communication System (PACS), Pharmacy stock control, Endoscopy and Maternity). Projects underway for continued departmental integration in 2013 include linking Renal, Foetal Medicine, Cancer and Maternity Systems.
Sharing clinical data electronically is increasingly important and this is currently supported with electronic mailing and the Image Exchange Portal (IEP).
PACS is provided via the NPfIT, whose contracts expire in 2014. The exit strategy is now underway with the repatriation of images and planning for re-procurement to replace this system begins in 2014. This system is a fully managed 24/7 service with a third party vendor. This fully managed service will continue with the new system and the technical resources and skillset required to support a new PACS solution will be reviewed as part of this project.
Work has begun to replace the Trust’s current corporate data warehouse with an in-house built data warehouse, as it will no longer be supported post 2014.
3.3 SIGNIFICANT PROJECTS 2013/14Alongside the existing programme of works, other key Trust projects which are supported by the Information Services Directorate are:
Intelligent File and Inventory Tracking (iFIT) – New implementation to support the robust tracking of case notes, deliver efficiencies within the health records libraries for filing and case note retrieval. Its implementation will deliver significant recurring savings of around £500,000. This was implemented Trust wide in November 2013 and will provide, linked with the EDM, reduction of the Trust’s paper footprint.
Jubilee Health Centre (JHC) – Network and systems connectivity to support the transition of clinical outpatient activity from Trust site to the JHC. Trusts services went live over a staggered period in 2013.
EDM – Network, system configuration and training to support the implementation of the Trusts EDM solution. The first phase of this implementation will provide users’ will a sophisticated front end to the Trusts existing repository of documentation allowing better searching. Bookmarking, annotating and sharing of documents. The projected go live date for this service is January 2014.
Page 23 of 48 document.docx

Urgent Care Centre (UCC) – Network and system reconfiguration to support the implementation of the UCC layout. Implementation of a UCC/ED whiteboard to facilitate a more efficient patient flow and clinical processes. The projected go live date for this service is February 2014.
Renal system upgrade – implementation of a new interface from Trust systems to the upgraded Renal system. This service went live during September/October 2013.
Cancer Database (Infoflex) – creation of a new backend system for the Infoflex system to facilitate the expanded use of this system to capture Cancer outcomes alongside the implementation of a new interface from Trust systems. This service went live during September 2013.
Vacating Sutton site project – supporting the Estates and services reconfiguration decanting from Sutton, for infrastructure and system changes. Health Records consolidation into a single Trust wide library at Epsom with services relocating from Sutton, deliver recurrent Estates savings of £130,294 and recurrent Health Records savings of £94,071.
3.4 EXISTING PROJECTSThe priorities of the proposed work streams have been reviewed alongside the Trust’s Integrated Business Plan (IBP) to ensure that the infrastructure will be capable to support the current and future needs of the Trust. The first priority is the Core Network replacement project, this lays the foundation upon which current hardware and the impending work steams can maximise their performance, such as improved backend system processing of data which will provide an improved service.
Email MigrationThe existing Email environment has not been upgraded in six/seven years, by migrating to the Microsoft mail system the Trust is moving to an up to date platform which integrates with today’s systems. This project will facilitate the decommissioning of the historical Novell directory service, which will decrease the current login window. This project is currently in progress and due for completion in September 2014
Urgent Care Centre PortalThis is an existing project that will provide clinicians with one view of where their patients are in the UCC and Emergency Department (ED) with access to underlying systems. This will also facilitate faster access to underlying systems. There will clinical benefits for patients as clinicians will have access to information held on departmental systems, which historically would not have been possible to support clinical decision making. There will also be data quality benefits for clinicians as they will have the ability to capture information in the Portal and the data will updated in the core Trust systems on the patients discharge. This project is scheduled to go live in February 2014
Single Sign OnThis is an existing project for the UCC and ED that will provide clinicians with seamless logins to key clinical applications and IT systems. There will be clinical efficiencies as time will not be spent on logging onto multiple systems currently
Page 24 of 48 document.docx
needed to support patient care. This project is linked to the implementation of the Urgent Care Centre Portal and is planned to go live in February 2014.
Electronic Document ManagementThis is an existing project that will provide users with more functionality to better access the 3.5 million documents which are currently available electronically in the Clinical Manager system. These include functionality to bookmark, send documents, search phases and create alerts either at a patient or document level. The EDM solution also has a briefcase option which will allow clinicians and staff who work in the community to bring the documents with them offsite, annotate changes, create documents using e-forms which will all be synchronised with the EDM system when they are back on site. This will also be expanded to include document capture either with scanning or directly into the system.
This project is due to go live in January 2014 and there will be a rolling programme of over a period of two years to deploy the full functionality of the system.
Page 25 of 48 document.docx

4 SECTION THREE: COMPOSITION OF THE PROGRAMMEThe implementation programme will comprise of a number of projects structured into four key areas: Clinical Application Systems Administrative Application Systems Information Management Infrastructure and networks
These are significant projects which will be delivered in line with the Trusts backup and business continuity policies, to ensure that systems are implemented with robust resilience to ensure patient safety.
Timescales are indicated in Appendix D.
4.1 CLINICAL APPLICATION SYSTEMSThere will be three major Integrated Digital Care Record (IDCR) deployment Phases.
PHASE ONE: Deployment of the Electronic Document Management solution to provide a
sophisticated front end to the 3.5 million documents which are already captured in our document repository;
Deployment of an Urgent Care Centre (UCC) Whiteboard using portal technology with integration to iPM for emergency department data. In addition to this, UCC whiteboard will provide views of iCM and Adastra (the GPs out of hour’s system). This will include single sign-on with context management
Completing the hardware technology refresh for iCM
Re-procurement of a new PACS solution
Development of a results acknowledgement application
Deployment of kiosk for patient flow management
Deployment of electronic inpatient prescribing and medicines administration
PHASE TWO: Creation of a Trust wide clinical portal with single sign-on and context management
for our clinicians providing one configurable view for clinicians for information from iCM, EDM and key departmental systems. This will include the ability to launch the underlying applications from the clinical portal
Deployment of the EDM solution and associated technologies to capture information digitally
Extension of the clinical portal to create a bed management tool which could integrate with iPM
Implementation of a scanning bureau using the EDM solution for paper case notes
Page 26 of 48 document.docx
Development of clinical portal for use with mobile devices
PHASE THREE: Creation of a patient portal
Extension of the clinical portal for GPs and tertiary social care
Deployment of self-check-in kiosk
The iPM and iCM contract ends in March 2016 and will be subject to re-procurement – this will be a substantial piece of work and ESH may consider collaborating with other London Acute Trusts that use iPM and iCM. Although the procurement is collaborative, outcomes could in theory be different for different Trusts. An options appraisal paper will be presented to the Operational Management Group for support in January 2015.
PACS, another centrally provided system is now subject to re-procurement, with a contract end date in 2015. Phase 1 of this project is already underway with the repatriation of images back from the BT offsite store.
4.2 ADMINISTRATION APPLICATION SYSTEMS E-rostering for nursing is to be upgraded and then deployed to other groups. EDM could be expanded to include corporate and personnel records for minimal
cost. This has potential to make cash-releasing savings and improve efficiencies The desktop Office systems (Microsoft Word, Outlook et al) will require upgrading.
4.3 INFORMATION MANAGEMENTThe Data Warehouse system will be replaced by June 2014 with an in-house built solution. This will include expansion of current data sets to deliver enriched management information. It is essential the correct data is extracted from the PAS systems, transformed into the correct format and structure for SLAM/SUS submissions and operational reports. If the development of a new data extract process cannot be developed in-house then engagement with a third party solution will be required.
By January 2015 a review of business intelligence requirements and current Trust systems will be undertaken.
4.4 IT INFRASTRUCTURE AND NETWORKSThere will be three major deployment Phases.
PHASE ONE: Storage Area Network (SAN) expansion
wireless network expansion
virtual server expansion
email migrationPage 27 of 48 document.docx
testing of Windows 7 operating system
deployment of new Helpdesk software
deployment of desktop management solution
PHASE TWO: replacement of core network
deployment of mobile devices
Virtual Desktop Infrastructure (VDI) pilot
deployment of Windows 7 operating system
expansion of Intelligent File and Inventory Tracking (iFIT)
- patients at risk
- asset tracking
- workforce management
- drugs & batch monitoring
- integrated communications
Trust wide expansion of Single Sign On (SSO)
deploying IS Monitoring and Management system
laptop replacement programme
replacement of Wide Area Network (WAN) link
PHASE THREE: printer consolidation
remote hosting options appraisal
cloud services options appraisal
Page 28 of 48 document.docx

5 SECTION FOUR: PROJECTS
5.1 2014/19 PROJECTSBelow is a summary of projects which have been identified to support the Trust in delivering the IM&T Strategy. These have been listed in order of priority to ensure the Trust is able to support patient care, maximise the return on investment in technology, whilst solidifying the foundations to enable future growth. As such the capital bids for Information Services have been submitted in the order below.
Please refer to Appendix C for investment and recurring costs for each of the projects and Appendix D for the Indicative Implementation Programme.
Core Network Replacement – May 2014 (pending successful capital bid)The existing Core Network infrastructure is currently end of life and will be out of support in 2 years. The Core Network replacement project can be phased over 2 years with the St Helier replacement in 2014/15 and the Epsom replacement in 2015/16. The new Core Network will give us a high speed backbone from which new technologies can be implemented upon. This will also enable the Trust to implement new projects such as vital signs monitoring, The server and storage infrastructure that was purchased this year is currently running on the Core Network. This has enabled the environment to be more robust, but there are limitations on performance due to the ageing technology of the core network. When the new Core Network has been implemented the data transfer between server and storage will increase exponentially providing a faster application experience.
Page 29 of 48 document.docx
Single Sign On – May 2014 (pending successful capital bid)To provide a Trust-wide Single Sign on (SSO) solution that will enable time efficiencies for all users, by consolidating the multiple passwords that are currently required into one. This will also enable us to ensure a higher level of security on systems that currently do not have this feature.This expands on the current deployment in the St Helier ED/UCC and paves the way for the Trust to implement a Virtual Desktop Infrastructure (VDI). This project has no dependency on the completion of the Core Network project and as such can run concurrently. This will require 0.5 wte resource with specialised technical ability to support the roll out of this project.
Clinical Portal Development – May 2014 (subject to any slippage in the capital allocation this project will be funded in 2014/15)This will provide clinicians and users a view of a patient’s clinical summary taken from different departmental systems. This information will be presented in one configurable view providing ease of access to ensure that clinicians have the information they need for decision making. Users will also have the ability to launch the underlying systems directly to their chosen patient from the portal without multiple logins. This expands on the current deployment in the St Helier ED/UCC by deploying a Trust wide solution that would improve safety for patients (decision making and the reduction of patient selection errors with context management) and deliver efficiencies for staff that currently access multiple systems. This will require 1 wte with specialised technical ability to support the Trust in 2014/15.
Virtual Desktop Infrastructure (VDI) – June 2015 (pending successful capital bid)VDI gives the Trust a flexible desktop solution that in conjunction with the decommissioning of the historical Novell directory services environment and the new Core Network, will allow staff to access their virtual desktop from any PC. The implementation of SSO and the Core Network will ensure that the VDI deployment will be optimised, thus allowing the Trust to deploy the “follow me desktop” option, which will present the user with their virtual desktop as they move from PC to PC throughout their working day. This project will improve efficiencies for all staff that practice mobile working. In addition users that currently use the Remote Access Solution outside of the Trust will be presented with the same Desktop environment removing the current limitations. This will require 0.5 wte with specialised technical ability to support the Trust in 2014/15.
Business Intelligence Software – May 2015 (pending successful capital bid)Having a corporate business intelligence (BI) solution will provide staff with a single portal for information such as performance targets, quality indicators, real time reporting and finance information. It will allow the user to drill down from the high level summary information down to an appropriate granular level (patient, specialty or ward level for example). Modern BI solutions can be used on mobile devices securely and provide wide ranging benefits from open and transparent information sharing to real time alerting. BI solutions depend upon a fast and reliable network.
Page 30 of 48 document.docx
There is also a dependency to expand the wireless network and have a mobile device policy in place to see the greatest benefits.
Wireless Networking Refresh – June 2015 (pending successful capital bid)Mobile working throughout the Trust will require a fully resilient, fast and secure wireless infrastructure. The core network replacement will give us the foundations to implement a wireless infrastructure that provides a seamless wireless working experience for staff in Clinical areas and will reap the benefits of future wireless innovations.The implementation of the new wireless network will create a secure, robust and fast environment that has sufficient capacity for the growing needs of the Trust. With the implementation of the portal and VDI the staff would benefit from having the ability to work with greater mobility.
Video Conferencing refresh – June 2015 (pending successful capital bid)Refreshing the Trusts 13 video conference units to latest specification models will enable us to provide the same experience for users in each video conference suite and reap the benefits from our fully supported VC environment and increase efficiencies with cross site and inter organisational interactions.This project is not dependant on the implementation of any of the outlined projects, it is only dependant on the life expectancy of the existing equipment and how quickly the Trust would like to utilise the additional features.
IS Management and Monitoring Tools – June 2015 (pending successful capital bid)When the new Core and Wifi Network are installed the Trust will require a management and monitoring solution that will provide one single management/monitoring view for the Trusts IT systems, allowing the Trust to proactively predict how systems will perform using benchmarking and trending. Clinicians and users will have systems which are more robust and reliable as system issues will be identified in a timely manner and dealt with.
Re-procurement of iPM & iCM – June 2015The contract for iPM and iCM ends in 2016. This project will review the requirements of the Trust in terms of what it needs in an EPR and PAS solution to ensure that the future systems in place will be fit for purpose to support the users at the Trust and the business needs of the organisation.
Electronic Document Management (EDM) Scanning – September 2015 (pending successful capital bid)Creation of a scanning bureau within the health records library with scanners linked to the Trusts’ EDM system will facilitate the scanning of case notes and other documentation. This will reduce the Trusts’ dependency on paper and to ensure that information will be readily available when and where needed. In addition this project will also reduce the storage requirements both at the Trust and offsite as information will be held digitally instead of on paper. Ultimately, clinicians and users will benefit from having 24/7 access to information on patients to support decision making when delivering clinical care.
Page 31 of 48 document.docx
This project is dependent upon the completed deployment of the EDM solution Trust-wide.
EDM for Clinical and Mobile App – June 2016 (pending successful capital bid)This will provide clinicians with the ability to capture information on mobile devices which are linked to the EDM solution. This would include simple workflow data capture and will reduce the dependency on capturing information on paper charts or documents. Clinicians would also benefit from efficiencies with faster data capture of information direct at the point of patient care.This project is dependent upon the completed deployment of phase 2 of the EDM solution Trust-wide.
Uninterruptable Power Supply (UPS) Upgrade (St Helier) – June 2016 (pending successful capital bid)The Uninterruptable Power Supply (UPS) is a device that sits between the mains power and the data centre room which houses our Clinical and non-clinical systems, in the event of a power outage the UPS will prevent the Clinical and non-clinical systems from losing power and shutting down prior to the backup generators coming online. The existing UPS at St Helier is currently running at 85% capacity and the addition of new services will reduce the resilience of the UPS. In addition to this the batteries in the UPS need replacing as the current set up only allows a limited supply of emergency power.This project will focus on replacing the UPS which will in the event of a power outage will sustain the integrity of existing systems and in turn support the implementation of future projects such as vital signs monitoring, bed management, etc as driven by clinical need.
UPS Relocation (Epsom) – June 2016 (pending successful capital bid)It has been recommended by our support company that the UPS at Epsom should be relocated to a more suitable environment, as the recent UPS failure has been attributed to its environment. Users will have the benefit of a more robust UPS in the event that this is needed.
Remote Access Replacement – June 2016 (pending successful capital bid)The Trusts Remote Access Solution is an appliance that enables the Trust staff to access Trust systems from remote locations when they are working off-site. The manufacturer of the Trusts Remote Access Solution has informed the Trust that the existing equipment will become end of life in April 2014 and end of support in April 2015, the level of support available between April 2014/15 will be greatly reduced and this will prevent the provision of a service. In addition to the replacement Remote Access Solution being fully supported, the Trust will benefit from the latest technology and the ability to integrate with future technologies. Users will be able to access more business and clinical applications from home with improve speed of access.
Bluecoat – June 2016 (pending successful capital bid)Page 32 of 48 document.docx

Bluecoat is an appliance that to monitors internet traffic and will provide internet usage statistics to the management team for currently restricted sites. Other benefits include providing Guest access to the internet , providing Patients and visitors access to the internet and reaping the benefits from being able to provide an internet solution to our customers. This project will support the Trust to better manage the use of the internet. In addition to this, clinicians and users will see benefits of having no restriction on sites which they require to support their clinical workings. This will require 0.5 of a technical infrastructure resource to provide support to the Trust in 2015/16.
Data Loss Prevention – June 2016 (pending successful capital bid)Data Loss Prevention (External Email Monitoring) will enable us to provide the Trust with a level of protection from the accidental loss of PID via Trust email and provide the Trust with an Audit trail of suspect emails for review, thus closing another possible avenue for ICO enforcement action up to £500,000. This will require 0.5 of a band 6 to provide support to the Trust in 2015/16. The ICO have indicated that if there was an incident where PID data was exposed, they would look more favourably in their investigations if a technological solution was in place to help prevent the loss of PID data.
External Data Centre Hosting Appraisal – June 2017 (pending successful capital bid)The Trust houses its systems in two data centres, these are purpose built environmentally controlled rooms, with specialised cooling and fire suppression systems. The Trusts data centres are at St Helier and at Epsom. Investigating an external data centre hosting solution will enable us to discover whether there could be efficiencies and a reduced risk in relocating our service to a purpose built external environment. This may provide an environment that is more stable and more cost effective to support the Trusts growing IT requirements.
Mobile Working Technologies – June 2017 (pending successful capital bid)Using mobile devices throughout the Trust will enable the Clinicians to update, capture and view information at the bedside, thus improving data quality and the contemporaneous recording of patient information. This technology requires the implementation of the New Core and Wifi Networks and would benefit from the VDI implementation.
Kiosk Deployment in Clinic Areas – June 2017 (pending successful capital bid)This will provide patients with the ability to self-check-in when they present at clinics to improve efficiencies in the movements of patients in an outpatient setting. This will include the ability to update details seamlessly with integration to the iPM system. This will be expanded to incorporate a queue management system for the tracking of prescriptions or phlebotomy.
Bed Management Whiteboard – June 2017 (pending successful capital bid)This will provide the Trust with one view of the available beds and occupancy of each bed and will support the tracking of patients between wards. There will be
Page 33 of 48 document.docx
efficiencies in managing the flow of patients within the Trust and will enhance the discharge process.
Patient Portal Development – June 2018 (pending successful capital bid)This will provide patients with access to their information held on Trust systems thereby empowering the patients in line with national guidance and out in the NHS England strategy ‘Putting Patients First’ and ‘Safer Hospitals Safer Wards Achieving an integrated digital care record’5. Patients will be able to share information on their care with other health care professionals if they need to.
Email Upgrade – June 2018 (pending successful capital bid)By 2017/18 the current email environment will be 5 years old and will require upgrading to keep in line with new technological advances. The Trust will implement a rolling program to keep abreast with current technologies and to prevent the Trust from falling behind its peers.
Microsoft Office (MS) Upgrade – June 2018 (pending successful capital bid)By 2017/18 the current MS Office environment will be 5 years old and will require upgrading to keep in line with new technological advances. The Trust will implement a rolling program to keep abreast with current technologies and to prevent the Trust from falling behind its peers.
Integration of Departmental Systems – Business as UsualThis project will ensure that any new systems being implemented at the Trust will be linked to the iPM system to ensure that staff do not need to undertake dual data entry on systems and to ensure that the Patient Master Index (PMI) record is mirrored across systems. When required and scoped, the integration can be expanded to include episodic information. This will deliver significant improvements to data quality between systems and efficiencies in staff workings.
5 SAFER HOSPITALS SAFER WARDS Achieving an integrated digital care record: NHS England 01 July 2013
Page 34 of 48 document.docx

6 CHALLENGESThe delivery of this programme over the next few years faces a number of key challenges:
This strategy requires significant financial investment to undertake the transition in technology, software and hardware during a challenging financial climate for the NHS. Projects within this strategy can only be delivered if sufficient capital and revenue funding can be awarded within the phases.
IDCR size and nature – this is a Trust wide project which requires significant cultural change management for all levels of staff to transition from a paper-based practice to a paperless way of working. This will include adapting to new ways for working with new technology eg touch-screen devices to support data capture at the point of care and the impact this would have with patients. Understanding and supporting the change required will have a significant impact on overcoming user resistance to change.
There are technological issues with delivering NHS Number as the primary number. These will need to be assessed and reviewed as and when clearer guidance is available from NHS England.
In addition to the change management and financial investment, the Trust will also need to overcome the information governance challenges of sharing information across boundaries. This will include ensuring that the Trust continues to adhere to the Caldicott principles and the Data Protection Act 1998 eg by ensuring that Data Sharing Agreements are in place.
The seventh Caldicott principle states:
"The duty to share information can be as important as the duty to protect patient confidentiality Health and social care professionals should have the confidence to share information in the best interests of their patients within the framework set out by these principles. They should be supported by the policies of their employers, regulators and professional bodies"
National to local
Capacity and capability – the demise of the NPfIT comes at a time when national and local contracts are coming up for renewal. This means significant additional procurement activity just as centralised support nationally or from London is diminishing;
uncertainty – the full impact of re-procurement of systems previously provided nationally is emerging slowly so associated financial plans will not be robust;
The delivery of the blueprint will require significant capital investment over the next 5 years. Full programme of Investments can be seen in Appendix C.
Meeting these challenges will include:
Page 35 of 48 document.docx

rigorous prioritisation by the Clinical Information Services Programme Board (CIPSB) of approved funded projects, phased carefully with wider hospital plans
engaging with the Trust for the IDCR programme of works by meeting with the clinical directorates and seeking support from the Operational Management Group
a robust communication strategy working with the directorates, supported by the Trusts communication team, using a variety of established process such as, e-update, All-Staff emails, STEPS and briefings.
increasingly using a collaborative approach across London for joint projects in order to avoid repetition, reduce costs and increase leverage with suppliers
taking the opportunity of re-procurement to reduce operating costs
using IT to provide efficiency savings
7 CHANGE MANAGEMENTChange is often the biggest risk to successfully exploiting a new and enhanced technology.
The programmes of work outlined in this strategy introduce significant cultural, process and technological modification across the organisational structure and will require strong investment in a detailed change management programme.
An internal assurance committee will be introduced to monitor and develop plans to monitor the progress of each programme of work, providing strategic direction, support to breaking down barriers and to focus on project milestones.
Over the next five years, Trust staff can expect to see their working lives transformed as technology advances, such as:
fast user logon and swift switching of workstations allowing the user to retain their desktop view, users providing efficiencies when the user moves between different clinical areas
access to multiple system with a single password
access to comprehensive patient information from one portal view
mobile access to Trust systems.
To ensure successful delivery of each individual programme of work set out in this strategy (please see Appendix D for indicative implementation plan), the following steps will be undertaken:
a. A team will lead on each programme of work. This will include an executive sponsor who will provide leadership throughout, a project management lead who will manage expectations and work with stakeholders to break down any barriers to success and change champions within key departments to help realise change at grass roots.
Page 36 of 48 document.docx

b. Each project will be clearly defined and scoped to include the expected change for an individual through to high level organisational change. This scoping session will also contain a ‘readiness to change’ assessment recognizing any gaps.
c. Risks to change will be identified and plans developed to mitigate these.d. A clear and targeted communication plan across a range of mediums will be
developed and implemented throughout the programme.e. Specific training to support each programme will be rolled out both face to face and
via computer based training (CBT). This will ensure the relevant staff are educated in the correct use of the software and any concerns can be resolved.
f. Staff will be involved from day one of each programme of work to ensure feedback is integrated where appropriate to deliver the right solution for both the user and the Trust. This will include learning from completed projects to support effective future change.
8 EDUCATION, TRAINING AND DEVELOPMENTOur change management agenda will need to be underpinned by a comprehensive learning programme, delivered in different ways to suit staff roles, providing all staff with the confident ability to exploit new systems and improved information to the fullest extent. In conjunction with Corporate training in HR, information Services will support the improvement in Trust wide IT competencies, ensuring a mandatory minimum standard is attained.
9 GOVERNANCEThe Clinical Information Services Programme Board guides the cost-effective use of technology so that it reflects the Trusts priorities and maximum benefits are achieved. Chaired by the Clinical Lead for Health Informatics, consultants represent the clinical directorates, and provide a two-way channel with their Directorates and Information Service.
The Capital Planning process sets out how the Trust prioritises all projects annually. All projects agreed to be in the Annual Plan require business cases. The business case will include: Executive summary highlighting key points including benefits and return of
investment
Business opportunity describing the scope and objectives of the project
Benefits for the patients, staff and organisation
Costs for both capital and revenue
Financial analysis summarising the value of the project as an investment
Assumptions highlighting events which would impact on the project
Constraints highlighting potential limitations on the project
Organisation considerations on how the project would impact on the Trust
Project description
Page 37 of 48 document.docx
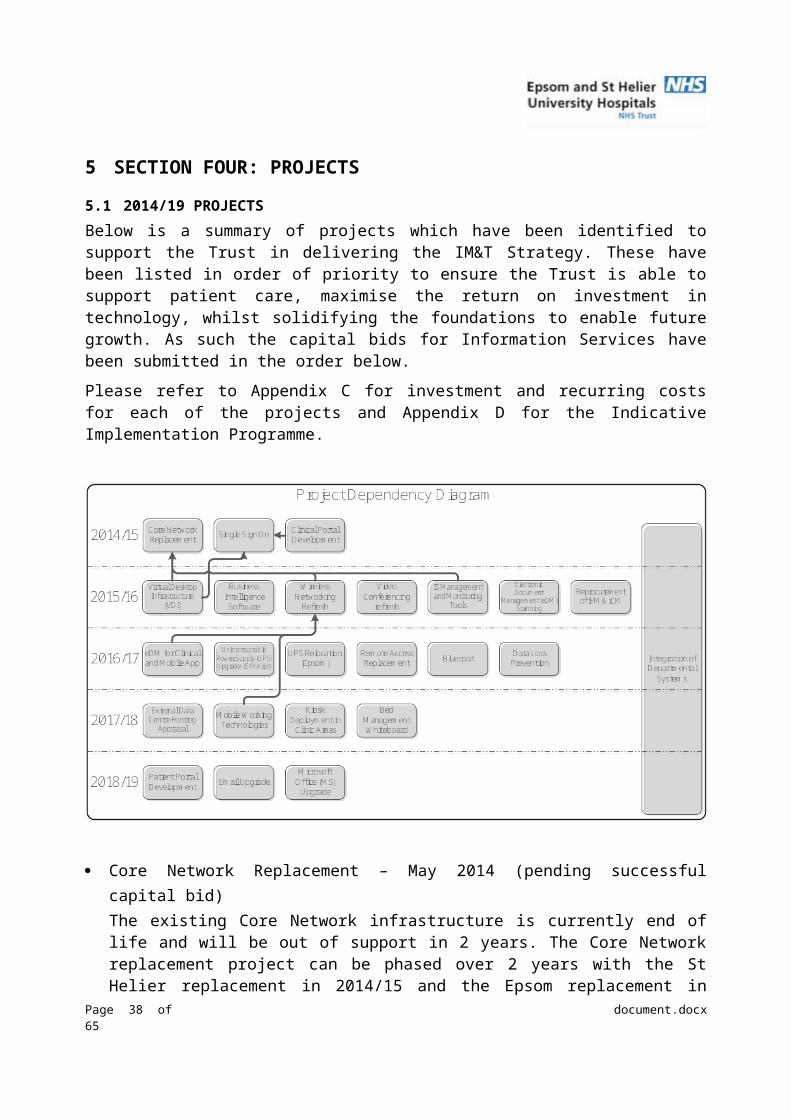
Implementation plan with milestone
Recommendations
10 COSTSProjects identified in phase one have approved Capital funding. Projects in phases two and three will be subject to the Business case approval process which will include costs and benefits analysis, these capital and revenue costs will need to be agreed by the Trust to support the delivery of this strategy.
Each project will include both capital (software, hardware, project staff costs, and operational impact costs associated with the change management) and revenue. The workforce in IS will increase by 4 wte’s to support this programme of works. In addition to this increase the PACS and ePrescribing project lead by the operational areas will increase the establishment by a further 3 wte’s. Full programme of investments can be seen in Appendix C.
The success of the IMT Strategy will be subject to sufficient financial investment over the next 5 years.
Indicative IM&T investments from other organisations are as follows:NHS Trust Spend (£m) Timeframe (years) Spend per year (£m)Epsom and St Helier Trust 5 5 1.0Guys and St Thomas Foundation Trust 219 5 43.8Hillingdon Foundation Trust 11 5 2.2West Hertfordshire Trust 67 5 13.4Royal Sussex Trust 30 5 6.0Southampton Foundation Trust 8 3 2.7
11 CONCLUSIONThe IM&T Strategy sets out the direction of travel the Trust will take to achieve a paperless environment by 2018. The success of this strategy is twofold:
- Financial investment in the programme of works- Willingness to support and undertake change management from the Trust to
support the programme of work
Patients will benefit from well informed clinicians who will have access to all their information to support clinical care and decision making. In addition to this, there will be greater sharing of information across social care boundaries ensuring that Patients have access to their own information which they may share with other health care professionals and likewise, the Trust will be able to share information directly with health care professionals as and when required.
Clinicians will benefit from having comprehensive information for patients in one configurable portal view regardless of where the information in stored in the Trust, accessible from any location to support clinical diagnosis and treatment. Clinicians also Page 38 of 48 document.docx

have the ability to capture information digitally from locations both internal and external to the Trust. In overcoming the challenges of data sharing with other organisations in line with the Caldicott principles, the Trust would also be able to access any information held about the Patients in the community or at other organisations seamlessly.
The increase of digital clinical information at the Trust will be easily shared with external stakeholder to support seamless pathways of care between secondary and primary care.
This will require commitment at all levels of the organisation: from executive leadership - to expect and demand that users actively participate in
deployments and use the tools that are provided
from the Information Services Directorate- to ensure that users’ requirements are met and that IT solutions are practical and usable
from the users themselves - to develop and change their practice to make the best use of the available technology.
Page 39 of 48 document.docx

12 APPENDIX A: TRUST CORPORATE OBJECTIVES – 2013/14
We are committed to continuously improving the care we provide to our patients, whilst ensuring our services offer best value for the taxpayer. We must also ensure our staff are well supported and are able to do their job to the best of their ability. Importantly, staff must be held to account for their own work and that of their teams.Our doctors, nurses, midwives, managers, other staff and volunteers will lead this and aim to deliver the following objectives during 2013/14.
1. OUR PATIENTS Put our patients first and treat them as individuals, with a particular focus on
excellent care, compassion and communication; Reduce our levels of healthcare associated infections, in particular Clostridium
difficile and MRSA (bacteraemia); Ensure our patients receive high quality safe care, including:
o Maintaining low mortality rates;o Further reducing the number of patient falls;o Further reduce the number of emergency readmissions;o Further improve the awareness and diagnosis of dementia;o Further improve the way we communicate with GPs after patients have
been discharged. Learn from the outcome of the Francis Report into the failings of Mid
Staffordshire NHS Foundation Trust; Further improve our patient survey results and take full advantage of the new
friends and family test; Continue to use feedback from our patients and their representatives to improve
the quality and safety of the services we provide; Launch a new quality directorate which focuses on learning from incidents,
complaints, audit, inquests and litigation.
2. OUR SERVICES Maintain and improve on the Government’s key performance and quality
standards, including keeping waiting times low; Maximise our use of the latest technology and IT systems to improve the care we
provide and the efficiency of our services; Maintain our registration and full compliance with Care Quality Commission
standards; Further improve our hospital estate through our annual capital investment
programme; Work towards gaining NHS Litigation Authority risk management standard level
two for general areas and maintain it for maternity; Increase our research and development activities in partnership with other NHS
partners.
3. OUR PEOPLEPage 40 of 48 document.docx

Continue to train, motivate and educate our staff, including ensuring they undertake their mandatory and statutory training;
Provide high quality undergraduate and postgraduate training for both nursing and medical staff;
o Improve our annual staff survey results in targeted areas, including the support provided by line managers;
Further improve the quality and maintain the frequency of staff appraisals; Further improve our staff attendance rates, bringing sickness absence in line with
the NHS average; Further improve the way we communicate and engage with our staff and
volunteers, including launching a new Trust intranet.
4. OUR FINANCES Maintain strong financial management and deliver our agreed financial target of a
deficit budget of £7.4 million; Ensure we make the best use of our resources and deliver our agreed quality
and cost improvement plan (of £19.9 million); Further reduce our use of expensive agency employees, as well as temporary
staff; Build on our success in reducing the number of patients who miss their
appointments; Increase the financial data held by our clinical specialties and support them in
using it to maximise the efficiency of our services.
5. OUR FUTURE Provide clarity on the long-term future and sustainability of our hospitals in
collaboration with primary care, social care and other NHS partners, including our local clinical commissioning groups;
Progress the £219 million redevelopment of the St Helier Hospital site; Maintain our good working relationships working relationships with key partners
and stakeholders, including MPs, council officers and elected officials, patient groups and hospital charities.
Page 41 of 48 document.docx

13 APPENDIX B: DEFINITIONSTerm DescriptionIDCR Integrated digital care recordEPR Electronic Patient recordiCM iSOFT Clinical ManageriPM iSOFT Patient ManagerEDM Electronic Document ManagementPHR Personal Health RecordSSO Single sign onMicrosoft Exchange An e-mail systemGroupWise An e-mail systemVDI Virtual Desktop InfrastructureVTE Venous thromboembolismIFIT Intelligent File and Inventory TrackingNPfIT National Programme for ITUCC Urgent Care CentreSAN Storage Area NetworkLAN Wide Area NetworkIBP Integrated Business PlanRAS Remote Access SolutionPMI Patient Master IndexCISPB Clinical Information Services Programme BoardIM&T Information Management & TechnologyOMG Operational Management GroupJHC Jubilee Health CentreIEP Image Exchange Protocol
Page 42 of 48 document.docx

14 APPENDIX C: INVESTMENT COSTS
Capital Capital Revenue Revenue Total Total2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2013/14 2014/15 2015/16 2016/17 2017/18 2018/19 2013/14 2014/15 2015/16 2016/17 2017/18 2018/19
£k £k £k £k £k £k £k £k £k £k £k £k £k £k £k £k £k £kEmail Migration £ - £ - £ - £ - £ - £ - £ - £ 105 £ - £ - £ - £ - £ - £ 105 £ - £ - £ - £ - Urgent Care Centre Portal £ 500 £ - £ - £ - £ - £ - £ - £ 20 £ 20 £ 20 £ 20 £ 20 £ 500 £ 20 £ 20 £ 20 £ 20 £ 20 Electronic Document Management £ 150 £ - £ - £ - £ - £ - £ - £ - £ - £ 32 £ 32 £ 32 £ - £ - £ 32 £ 32 £ 32
1 Core Network Replacement £ - £ 390 £ 215 £ - £ - £ - £ - £ - £ - £ 100 £ 100 £ 100 £ - £ 390 £ 215 £ 100 £ 100 £ 100 2 Single Sign On £ 30 £ 225 £ - £ - £ - £ - £ - £ 20 £ 20 £ 20 £ 20 £ 20 £ 30 £ 245 £ 20 £ 20 £ 20 £ 20 3 Clinical Portal Development £ - £ 510 £ 215 £ - £ - £ - £ - £ 95 £ 95 £ 95 £ 95 £ 95 £ - £ 605 £ 310 £ 95 £ 95 £ 95 4 Virtual Desktop Infrastructure £ - £ - £ 280 £ 260 £ 260 £ - £ - £ - £ 66 £ 66 £ 66 £ 66 £ - £ - £ 346 £ 326 £ 326 £ 66 5 Business Intelligence Software £ - £ - £ 90 £ - £ - £ - £ - £ - £ 17 £ 17 £ 17 £ 17 £ - £ - £ 107 £ 17 £ 17 £ 17 6 Wireless Networking Refresh £ - £ - £ 89 £ 89 £ 89 £ - £ - £ - £ 7 £ 7 £ 7 £ 7 £ - £ - £ 96 £ 96 £ 96 £ 7 7 Video Conferencing refresh £ - £ - £ 52 £ 52 £ 52 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 52 £ 52 £ 52 £ - 8 IS Management and Monitoring Tools £ - £ - £ 60 £ 132 £ - £ - £ - £ - £ 8 £ 35 £ 35 £ 35 £ - £ - £ 68 £ 167 £ 35 £ 35 9 Reprocurement of iPM & iCM £ - £ - £ 65 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 65 £ - £ - £ -
10 eDM Scanning £ - £ - £ 50 £ - £ - £ - £ - £ - £ 3 £ 3 £ 3 £ 3 £ - £ - £ 53 £ 3 £ 3 £ 3 11 eDM for Clinical and Mobile App £ 150 £ - £ - £ 25 £ - £ - £ - £ 37 £ - £ 62 £ 62 £ 62 £ 150 £ 37 £ - £ 87 £ 62 £ 62 12 UPS Upgrade (St Helier) £ - £ - £ - £ 198 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 198 £ - £ - 13 UPS Relocation (Epsom) £ - £ - £ - £ 90 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 90 £ - £ - 14 Remote Access Replacment £ - £ - £ - £ 25 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 25 £ - £ - 15 Bluecoat £ - £ - £ - £ 125 £ - £ - £ - £ - £ - £ 20 £ 20 £ 20 £ - £ - £ - £ 145 £ 20 £ 20 16 Data Loss Prevention £ - £ - £ - £ 150 £ - £ - £ - £ - £ - £ 25 £ 25 £ 25 £ - £ - £ - £ 175 £ 25 £ 25 17 External Data Centre Hosting Appraisel £ - £ - £ - £ - £ 30 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 30 £ - 18 Mobile Working Technologies £ - £ - £ - £ - £ 100 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 100 £ - 19 Kiosk Deployment in Clinic Areas £ - £ - £ - £ - £ 200 £ 200 £ - £ - £ - £ - £ 40 £ 40 £ - £ - £ - £ - £ 240 £ 240 20 Bed Management Whiteboard £ - £ - £ - £ - £ 100 £ 100 £ - £ - £ - £ - £ 20 £ 20 £ - £ - £ - £ - £ 120 £ 120 21 Patient Portal Development £ - £ - £ - £ - £ - £ 250 £ - £ - £ - £ - £ - £ 50 £ - £ - £ - £ - £ - £ 300 22 Email Upgrade £ - £ - £ - £ - £ - £ 250 £ - £ - £ - £ - £ - £ 14 £ - £ - £ - £ - £ - £ 264 23 MS Office Upgrade £ - £ - £ - £ - £ - £ 150 £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ - £ 150 24 Integration of Departmental Systems £ - £ 15 £ 15 £ 15 £ 15 £ 15 £ - £ - £ - £ - £ - £ - £ - £ 15 £ 15 £ 15 £ 15 £ 15
Total £ 830 £ 1,140 £ 1,131 £ 1,161 £ 846 £ 965 £ - £ 277 £ 236 £ 502 £ 562 £ 626 £ 680 £ 1,417 £ 1,367 £ 1,663 £ 1,408 £ 1,591
Funded ProjectsSubject to Business Case Approval
Page 43 of 48 document.docx
15 APPENDIX D: INDICATIVE IMPLEMENTATION PROGRAMME
2013/14 2014/15 2015/16 2016/17 2017/18 2018/19Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4 Q1 Q2 Q3 Q4
Email Migration (Groupwise to Outlook)Urgent Care Centre PortalElectronic Document ManagementData warehouseCore Network ReplacementSingle Sign OnClinical Portal DevelopmentVirtual Desktop InfrastructureBusiness Intelligence SoftwareWireless Networking RefreshVideo Conference refreshIS Management and Monitoring ToolsReprocurement of iPM & iCMEDM ScanningEDM for Clinical and Mobile AppUPS Replacement (St Helier)UPS Relocation (Epsom)Remote Access ReplacmentBluecoatData Loss PreventionExternal Data Centre Hosting AppraiselMobile Working TechnologiesKiosk Deployment in Clinic AreasBed Management WhiteboardPatient Portal DevelopmentEmail - upgrade
Page 44 of 48 document.docx
16 APPENDIX E: EQUALITY IMPACT ASSESSMENT
1. Name of function, strategy, project or policy
IM&T Strategy
2014-19
2. Name, job title, department, and the telephone number of staff completing the assessment form
Marcus Kirby
Head of Support Services
Mob: 07975 232 400
Tel: 020 8296 3284 (St Helier)
3. What is the main purpose and outcomes of the function, strategy, project or policy.
This strategy sets out how Epsom and St Helier NHS Trust (ESH) will develop its information, systems and technology, building on the 2010-12 strategy. A strategic Information Management and Technology (IM&T) framework will be provided to meet healthcare priorities for the next five years, achieving a paperless patient journey. In order to realise maximum benefit from this, the Trust must continue to adapt its culture to fully adopt technology, requiring commitment at all levels across the organisation.
4. List the main activities of the function, project/policy (for strategies list the main policy areas)
To support clinicians and other members of staff to make patient care safer and more efficient, through the use of enhanced technology and less reliance on paper for the patient journey. Information will become accessible via a Clinical Portal which will provide one view of a patient’s record obtained from various clinical systems. Information to manage the business of ESH is vital and it will be derived (in the main) from clinical information systems.
5. Who would benefit from the strategy/project/policy
All Trust staff and ultimately patients
6. Is it relevant to:
- Race Relations Act
- Sex Discrimination Act
- Disability Discrimination Act
- Employment Equality Regulations
- Religion or Belief
- Sexual Orientation
Yes No
Not relevant
Page 45 of 48 document.docx

- Age
7. Do you think that the function/strategy/project/ policy could have a negative or positive impact on :
Race
Disability
Gender
Religion
Sexual Orientation
Age
The project will have a positive impact for patients and staff.
8. How could you minimise or improve any negative impact? Explain how.
N/A
9. What consultation with relevant users on this project has taken place?
N/A
10. If there are gaps in your consultation and research, are there any experts/relevant groups that can be contacted to get further views or evidence on the issues. Please list them and explain how you will obtain their views.
NA
11 a) Have you involved your staff in taking forward this impact assessment?
11 b) How have you involved the staff
N/A
12. In the light of all the information detailed in this form what practical actions would you take to reduce or remove any adverse/negative impact.
N/A
To be signed by the Manager completing this form.
Signed: Marcus Kirby Date: 21st November 2013
Page 46 of 48 document.docx
17 APPENDIX F: REFERENCE DOCUMENTS
Safer Hospitals, Safer Wards: Achieving an Integrated Digital Care Record
Author: NHS England
Publication Date: 01 July 2013
http://www.england.nhs.uk/wp-content/uploads/2013/07/safer-hosp-safer-wards.pdf
Standards for the clinical structure and content of patient records
Author: Academy of Medical Royal Colleges
Publication Date: July 2013
http://www.rcplondon.ac.uk/resources/standards-clinical-structure-and-content-patient-records
i-care: Information, Communication and Technology in the NHS
Author: Academy of Medical Royal Colleges
Publication Date: July 2013
http://www.aomrc.org.uk/publications/reports-a-guidance/doc_details/9725-i-care-information-communication-technology-in-the-nhs.html
The Power of Information: putting all of us in control of the health and care information we need
Author: Department of Health
Publication date: 21 May 2012
https://www.gov.uk/government/publications/giving-people-control-of-the-health-and-care-information-they-need
Putting Patients First: The NHS England Business Plan for 2013/14 –15/16
Author: NHS England
Publication Date: May 2013
http://www.england.nhs.uk/wp-content/uploads/2013/04/ppf-1314-1516.pdf
Contains guidance on Digital Maturity Index.
Risk to patient safety of not using the NHS Number as the national identifier for all patients
Author: National Patient Safety Agency
Publication Date: June 2009
http://www.nrls.npsa.nhs.uk/resources/?entryid45=61913
Page 47 of 48 document.docx

18 APPENDIX G: POLICIES
Page 48 of 48 document.docx