in most cases evar substituted conventional repaire for ruptured aaa why
TRANSCRIPT

In most cases EVAR substituted conventional repair for ruptured
AAA
Why?
Antalya, 27/30-10-2011
Medical School Twente
EVAR team Medisch Spectrum TwenteEnschede, the Netherlands

Why think of EVAR?• Gut feeling: great difference rEVAR vs
open*
• Reduced peri-operative mortality in elective AAA repair- EVAR 1: EVAR 1.7% vs open 4.7%
- EVAR 2: 9% for unfit patients
• Less blood loss
• Less use of ICU
• Shorter length of hospital stay
• Less major morbidity
• Shorter recovery timeAntalya, 27/30-10-2011
Medical School Twente

Influence of EVAR on (r)AAA outcome
05
101520253035
In hospital mortality per vascular area per year(R)AAAaortic-iliac oblitfem-distal oblitcerebrovasc oblit
%
6194 arterial interventions MST 1997-2007
Medical School Twente
Antalya, 27/30-10-2011

Why think of EVAR?• Gut feeling: great difference rEVAR vs
open
• Reduced peri-operative mortality in elective AAA repair- EVAR 1: EVAR 1.7% vs open 4.7%
- EVAR 2: 9% for unfit patients
• Less blood loss
• Less use of ICU
• Shorter length of hospital stay
• Less major morbidity
• Shorter recovery timeAntalya, 27/30-10-2011
Medical School Twente

Advantages of rEVAR• Less invasive
- No laparotomy required- No retroperitoneal dissection- Local anaesthesia• Intact vascular resistance and muscular tone
abdominal wall- Reduced blood loss- Less hemodynamic disturbance
– No aortic cross clamping required• Less ischemia and reperfusion of lower body and
visceral organs- Reduced inflammatory response, cytokines →
MOFAntalya, 27/30-10-2011
Medical School Twente

Advantages of rEVAR
• Less effect on- Cardial function- Respiratory function- Renal function
• Fewer systemic complications
• Faster recovery
Antalya, 27/30-10-2011
Medical School Twente

Ruptured AAA: Evidence
• > 400 papers mentioning rEVAR– Open vs rEVAR minimum of 5 patients in
each group • 17 single center studies• 1 multicentre study• 1 single center RCT• 2 database analysis
Antalya, 27/30-10-2011
Medical School Twente

Ruptured AAA: Evidence• Analysis
– Heterogenicity of studies– Lack of standardized reporting– Small numbers– Small percentage treated with rEVAR (15-50%)– Devices: AUI vs Bifurcation vs Tube– Percentage unstable patients rEVAR 33-73% vs
open 35-68%• Definition of “unstable” varied
– Local anaesthesia 0-97%
• Mean short term mortality 25% rEVAR vs 42% open
Antalya, 27/30-10-2011
Medical School Twente

Ruptured AAA: Evidence
• Cochrane review 2008– No RCT – Heterogenicity studies– Reduction mortality rate, ICU stay and
blood loss encouraging
Antalya, 27/30-10-2011
Medical School Twente

Ruptured AAA: MST experience
• No treatment• Open procedure (MST 30% 30-day
mortality)• rEVAR?
Antalya, 27/30-10-2011
Medical School Twente
Ruptured AAArEVAR• Aortic Unilateral device
+Straight forward procedure+Small stockage– Fem-fem needed– On long term proximal migration and
type 1 endoleak• Bifurcated devices
– Enormeous stockage on the shelves needed
– Contralateral access unpredictable
Antalya, 27/30-10-2011
Medical School Twente
ANACONDA Contralateral access facilitated by
magnet system Body repositionable Device also applicable in complex
anatomy

Ruptured AAATAAR (TransAbdominal Aneurysm
Repair)• Mortality and morbidity high and
unchanged last decades (40-90%)
EVAR• Aortic Unilateral device
– Straight forward procedure– Small stockage– Fem-fem needed– On long term angulation, proximal
migration and type 1 endoleak are not negligible
• Bifurcated devices – Enormeous stockage on the shelves
needed – Contralateral access unpredictable
Antalya, 27/30-10-2011
Medical School Twente

Ruptured Aortic Aneurysm Study with the Anaconda
• Feasibility study• Single center• Prospective• Intension to treat• From April 2006 until April
2010• Consecutive patients
Antalya, 27/30-10-2011
Medical School Twente

Ruptured AAA MST
9%
61%
3%1%
24%
162 ruptured infrarenal aneurysms31 not treated89 open procedures4 Talent AUI4 Endurant (1 AUI)34 Anaconda
Antalya, 27/30-10-2011
Medical School Twente

RASA (N= 34)
Patient characteristicsGender
MaleFemale
304
AgeMean (range) 73 (58-87) years
Follow upMean (range) 25 (7-55) months
Lost to follow up 0
Antalya, 27/30-10-2011
Medical School Twente

RASA (N= 34)
Highlights anatomy
Antalya, 27/30-10-2011
Medical School Twente
Mean range
Diameter infrarenal neck
D2a (mm)D2b (mm)D2c (mm)
2223 23
16-3117-2816-30
Body sizeOversizing %
2924
21-3414-47
Neckshape Parallel || Conical \ /Rev.-conical / \Bell ( )
28231
Length infrarenal neck mm 25 9-55
Circumferential thrombus
% <10 0-25
Circumferential calcification
% <10 0-50
Angulation neck aneurysm
degrees 41 0-100
Aneurysm diameter (D3) mm 76 33-125

OR-timeX-ray time
146 min (70-300 min) 12 min (3-50 min)
ContrastPacked cells
140 cc (25-360 cc)5 (0-21)
Endoleak at “end” operation 1x Type I? (conversion, re-relap, prox inlay)7x Type II, at discharge 2, 30-day onward 0
Occlusion renal artery 2 times intentional (accessory renal artery)
IC-hospitalisation 3 days (0-15)17x < 24 hours
Conversion 3x
RASA (N=34) Peri-operative results
Antalya, 27/30-10-2011
Medical School Twente
Conversions free rupture during procedure † free rupture, balloon, thrombosis aorta † ongoing instable patient, missed type I
endoleak?final angio: no endoleakclamp infrarenal “on prosthesis”conventional suturing proximal
2 x decompression abdomen

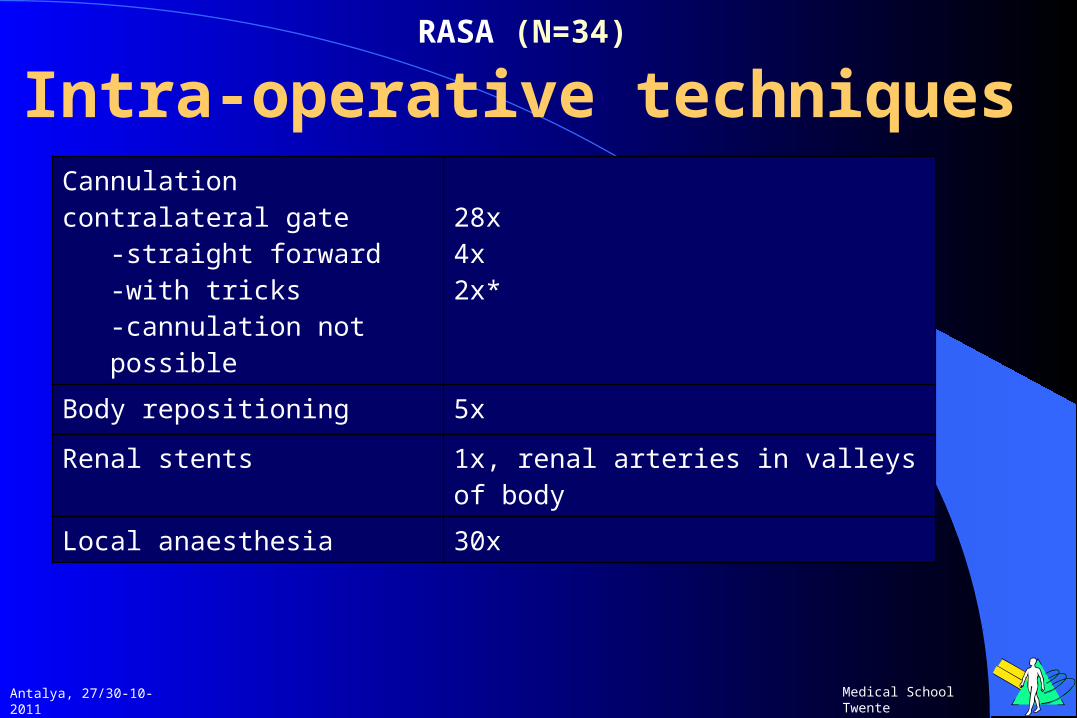
RASA (N=34) Intra-operative techniques
Antalya, 27/30-10-2011
Medical School Twente
Cannulation contralateral gate
-straight forward-with tricks-not cannulated
28x4x2x*
Body repositioning 5x
Renal stents 1x, renal arteries in valleys of body
Local anaesthesia 30x
*Cannulation not possible? free rupture during cannulation
procedure free rupture, balloon, no time for
cannulation procedure, to introduce balloon body needed to be released, thrombosis aorta
RASA (N=34) Intra-operative techniques
Antalya, 27/30-10-2011
Medical School Twente
Cannulation contralateral gate
-straight forward-with tricks-cannulation not possible
28x4x2x*
Body repositioning 5x
Renal stents 1x, renal arteries in valleys of body
Local anaesthesia 30x

Antalya, 27/30-10-2011
Medical School Twente
D3 98mmSevere iliac angulation
Body repositioning

Antalya, 27/30-10-2011
Medical School Twente

Antalya, 27/30-10-2011
Medical School Twente
Magnet system “downstream”Repositioning mainbody

RASA (N=34) Mortality
Antalya, 27/30-10-2011
Medical School Twente
period cause total
Intra-operative 2 1x cardiac arrest1x thrombosis aorta and visceral arteries
2
In hospital 3 mof, cardial, pneumonia
5 (15%)
30-day mortality 1 cardial 6 (17%)
6-months mortality
1 cardial 7
Study mortality 4 cardial 2x, malignancy, CVA
11
Aneurysm related
3
Device related 0

RASA (N=25) Re-interventions
Antalya, 27/30-10-2011
Medical School Twente
nr reason
In hospital (8) 2
2112
After conversion to aorto-bi-fem, hemicolectomy (bowel ischemia) and later rupture anastomosis left groinSigmoid resection (ischemia) and later closure abdomenStents renal arteriesOccluded leg, thrombectomy and stent flowsplitterDecompression abdomen, later suturing proximal anastomosis (type I endoleak?)
30-day (1) 1 Occluded leg, thrombectomy and kissing PTA flowsplitter
6-months 0
Study 1 After 4 yrs rupture type Ib left -> extended with leg

Conclusion RASA
• Treating a ruptured aneurysm with the Anaconda is feasible– Succesfull exclusion rAAA in 31 of 34
patients• 91% success
– 2x free rupture during operating procedure– Possible type I endoleak, converted (suturing prox.
anastomosis)
– 30 day mortality = 17%– Tricks needed, not straight forward
Antalya, 27/30-10-2011
Medical School Twente

In most cases EVAR substituted conventional repair for ruptured
AAA
Why?
Antalya, 27/30-10-2011
Medical School Twente
• Feasible• Growing evidence• Many heterogeneous studies• Lower mortality rates
• Future: • Multiple periscope and chimney
grafts for type IV TAAA or AAA
Randomised controlled trialsAJAX
IMPROVEECAR