incident investigation course - cbia - connecticut ... · incident investigation 1 3 incident...
TRANSCRIPT

Incident Investigation 1
Incident
Reporting/Investigation CBIA Conference
May 19, 2017
Christopher Mayne, Vice President
Randy M. Feranec Senior Safety Specialist

Incident Investigation 2
Have You Seen This in an Incident Report?
• Root Cause:
– The employee failed to follow established procedures.
• Follow-up Recommendation:
– Reviewed procedure with employee
– Disciplined employee
– Reviewed incident in monthly safety meetings

Incident Investigation 3
A Common Problem with Incident Investigations
1. Prematurely stopping the investigation at what the
team may call “human error.”
2. Often at “failure of employee to follow
procedures.”
3. Is that the real root cause? Not necessarily
– Were procedures out of date?
– Were they not understood?
– Was there inconsistent enforcement?
– Were there time pressures?
– Were they ambiguous (hard to understand)?
– Was it an accepted practice?
– Many others...

Incident Investigation 4
Three Mile Island Nuclear Power Plant 3/28/1979
Initial Root Cause: Control Room Operator Error
• Actual Cause after investigation: Contamination of instrument air several unit upsets/false alarms control room operators did not believe there instrumentation, leading to an assumption and accepted practice loss of reactor control unit shutdown never to restart.
• Did you know? – Virtually the same initiating event occurred a year earlier involving
contaminated instrument air.
– Incident investigation failed to identify the true root causes and implement remedies.

Incident Investigation 5
Incident Investigation
A methodology to aid in identifying the actual
root cause(s) of incidents.
A process which should aid in preventing
future incidents.

Incident Investigation 6
Process Steps
1 Introduction
2 Conduct Initial Response
- Incident Recognition & Reporting
- Determine the need for a secondary (Level 2) investigation
3 Form Investigation Team
4 Capture Data
5 Analyze Data
6 Develop Recommendations
7 Incident Report
8 Closing the Loop – Management of Change

Incident Investigation 7
Introduction
Why are we doing this ?
Incident Investigation 8
Objectives
• To Understand;
– What an incident is
– Why we need incident investigation
– What can happen if incident investigation led to wrong corrective
actions
– Why incidents happen...Incident Cause
– How to investigate an incident
– Why it’s important to get the correct information ASAP
– Why preserve the scene
– How to analyze for causes
– How to develop recommendations
– How to write the report
– Use a format that employees will actually use and makes sense for
your site.

Incident Investigation 9
Expected Outcomes
You will be able to:
• Conduct high quality Incident Investigations
• Use the Incident Investigation tools
• Identify Direct Causes and Root Causes of
Incidents
The ultimate outcome is fewer future incidents.
Incident Investigation 1
0
What is an Incident?
INCIDENT
ACCIDENT or NEAR MISS
ACCIDENT
An undesired event which
did result
in an unwanted impact on safety
or health of people, property
or the environment
NEAR MISS
An undesired event which
could have resulted
under slightly different circumstances
in an unwanted impact on safety
or health of people, property
or the environment
Incident Investigation 1
1
Scope of Incidents
• Involve safety, health or has an environmental impact
• Incidents include: – Injury/Illness (Lost time/Restricted Duty)
– Medical Treatment
– First Aid Cases
– Near misses
– Regulatory compliance violations
– Property Damage
– Security
– Fires
– Fatality
– Spills
– Permit Violations (HOT Work, Confined Space, Fire System Impairment, Energized Electrical Work)
Incident Investigation 1
2
Why do we need to do Incident Investigations ?
• To eliminate injuries, protect the environment, and reduce risk
• To reduce number and severity of incidents by
– conducting high quality incident investigations
– being proactive
– determining root causes
– better understanding and modifying the root cause behaviors that result in
incidents
– developing and implementing recommendations.
• To learn lessons from incidents and share across an ORGANIZATION
– HVLI (High Value Learning Incidents) - those with recognized important
lessons that other sites can benefit from.
• To influence local and company-wide improvement plans by
– analyzing “common causes” for multiple incidents

Incident Investigation 1
3
Incident Initial conclusion / action Result Actual issue
Equipment failure
Defective equipment /
replaced with same type
Failed again
Material incompatibility
What can happen if the incident investigation led to wrong corrective action?
Pump failed in initial start up
Defective seal / replaced
Repeated failures
Start up procedure: needed
to open discharge side first
Door being opened nearly
struck someone walking
outside
Painted sidewalk red in
area of door movement
as warning
Employee fell, slipped on
paint on humid day
Corrective action created
a new hazard
Leaking hydrogen valve
Cold weather caused
packing to leak / replaced
New valve began to leak
Valve not intended for
hydrogen service
Hand crushed in machine
pinch point while cleaning
Inadequate guarding,
alarms, and interlocks
Installed expensive and
elaborate protection system
Operating conditions were
incorrect and resulted in
unnecessary cleaning

Incident Investigation 1
4
Incident Investigation Process
• A specific order of activities is defined to ensure
quality and consistency.
• The major activities include:
– Conduct Initial Response
– Form Investigation Team (Medium & High Level)
– Capture Data (Who, What, Where, When, Why & How)
– Analyze Data
– Develop Recommendations
– Write the Report

Incident Investigation 1
5
Conduct Initial
Response
Incident Investigation 1
6
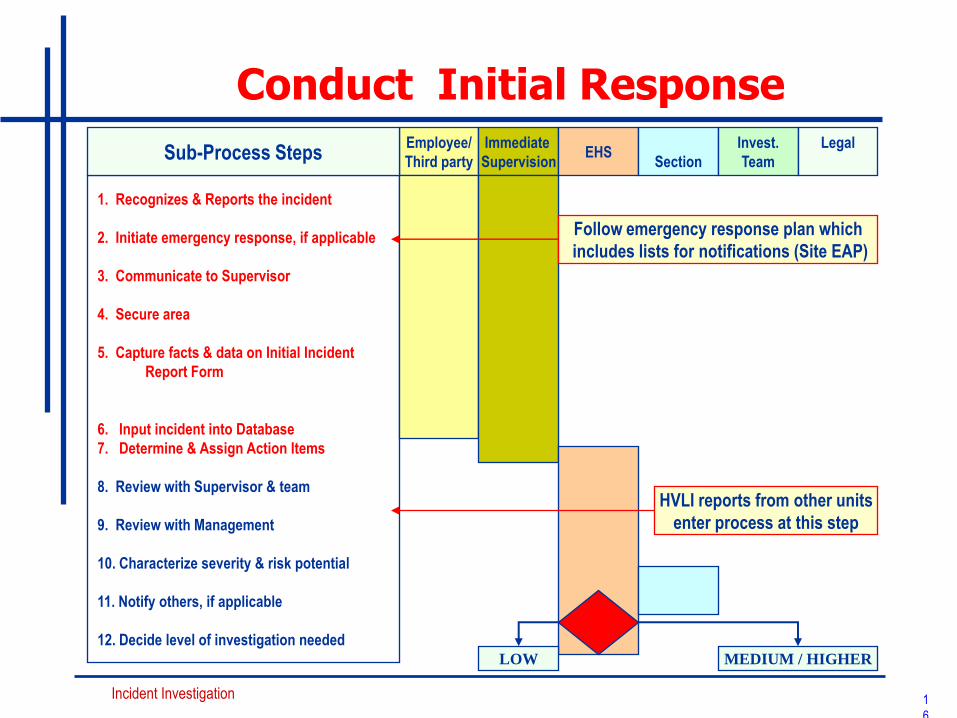
Conduct Initial Response
1. Recognizes & Reports the incident
2. Initiate emergency response, if applicable
3. Communicate to Supervisor
4. Secure area
5. Capture facts & data on Initial Incident
Report Form
6. Input incident into Database
7. Determine & Assign Action Items
8. Review with Supervisor & team
9. Review with Management
10. Characterize severity & risk potential
11. Notify others, if applicable
12. Decide level of investigation needed
Employee/
Third party
Immediate
Supervision EHS
Section Sub-Process Steps
Follow emergency response plan which
includes lists for notifications (Site EAP)
HVLI reports from other units
enter process at this step
Invest.
Team
Legal
LOW MEDIUM / HIGHER
Incident Investigation 1
7
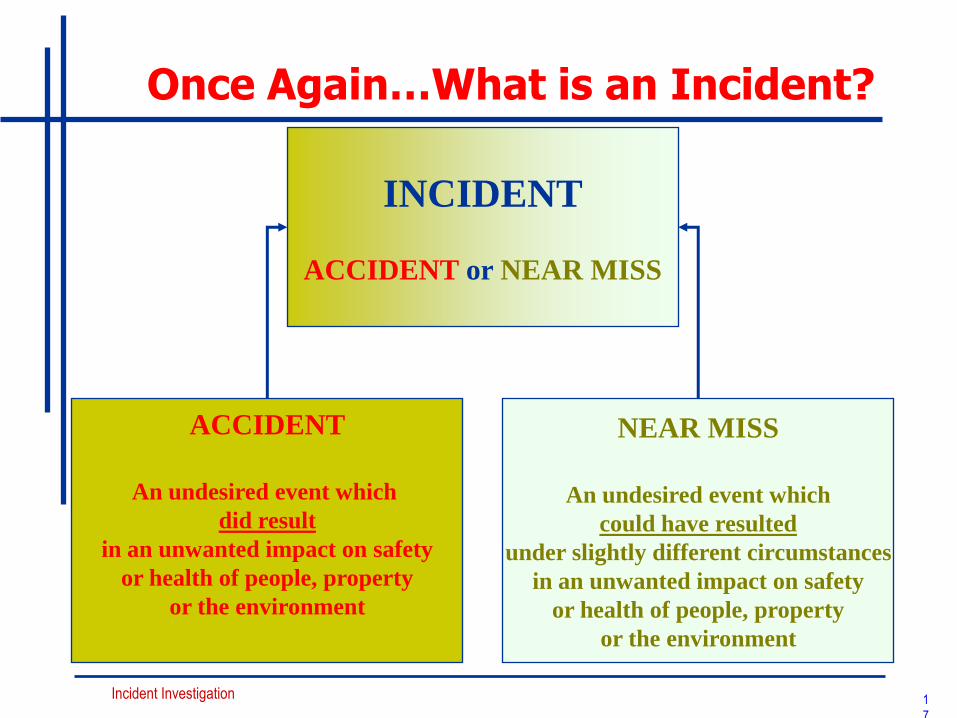
Once Again…What is an Incident?
INCIDENT
ACCIDENT or NEAR MISS
ACCIDENT
An undesired event which
did result
in an unwanted impact on safety
or health of people, property
or the environment
NEAR MISS
An undesired event which
could have resulted
under slightly different circumstances
in an unwanted impact on safety
or health of people, property
or the environment
Incident Investigation 1
8
Why Incidents Happen (Incident Causes)
• Three things to consider for the incident process to start:
– Hazard(s) A source of danger with potential to do
harm, e.g. chemical, energy, unsafe
condition or act
– Vulnerable objects Things that can be harmed, e.g.
people, environment, equipment
– Barriers Things that protect vulnerable objects
from the hazards, e.g. well designed
equipment, equipment guards, PPE,
procedures, etc.
Incident Investigation 1
9
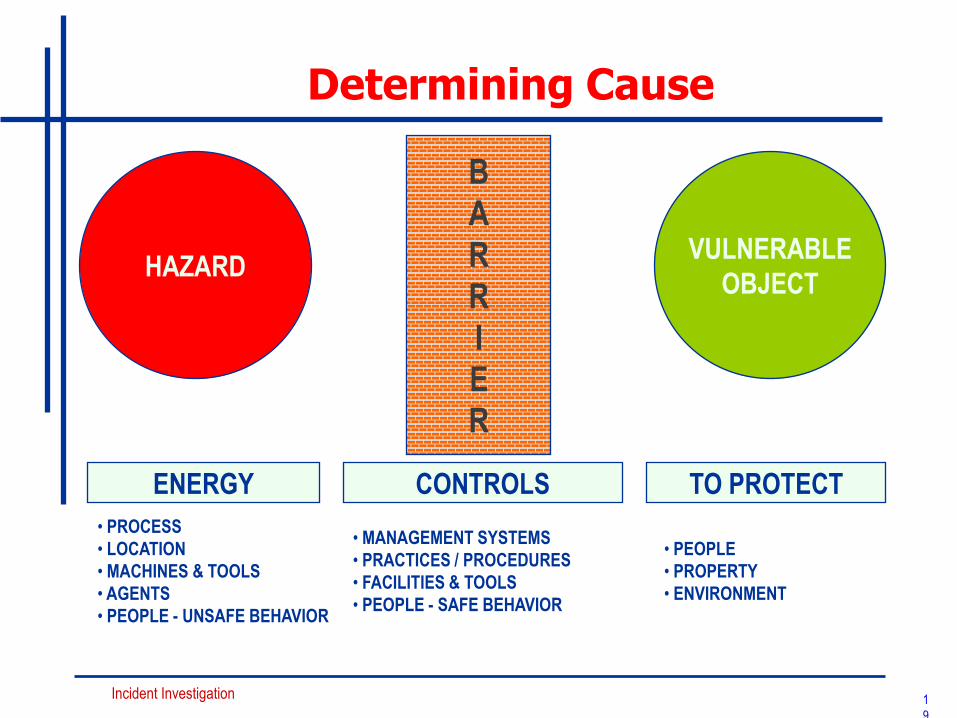
Determining Cause
HAZARD VULNERABLE
OBJECT
B
A
R
R
I
E
R
• PROCESS
• LOCATION
• MACHINES & TOOLS
• AGENTS
• PEOPLE - UNSAFE BEHAVIOR
ENERGY CONTROLS TO PROTECT
• MANAGEMENT SYSTEMS
• PRACTICES / PROCEDURES
• FACILITIES & TOOLS
• PEOPLE - SAFE BEHAVIOR
• PEOPLE
• PROPERTY
• ENVIRONMENT

Incident Investigation 2
0
When Do Incidents Happen?
Hazards + Barriers + Vulnerable Objects = Safe Condition
(Normal Operating Condition)
Hazards - Barriers - Vulnerable Objects = Near Miss
Hazards - Barriers + Vulnerable Objects = Accident
In other words:
– An accident occurs if hazards and vulnerable objects are present
and barriers are less than adequate (LTA).
Incident Investigation 2
1
Secure area
• Prevent additional injuries, illness, or incident
escalation
– Operations/work should not resume until it has been
determined to be safe to continue.
– An assessment needs to be carried out to determine if work
can continue or not. Use a simple tool like the TRA/JSA
checklist, TPA, or other local techniques,
• Preserve site/conditions for further investigation
– Barricade (if necessary)
– do not change/move anything unless key for safety reasons
– Take photos
Incident Investigation 2
2
Initial Incident Information
• Collect initial incident information
– Every facility should have a management system for Incident
Reporting, Analysis, and Follow-up.
– For all incidents, regardless of severity, the initial information
gathering is the same and is normally the primary responsibility of
First Line Supervision.
– The information generated through the first twelve steps of the
Incident Reporting and Investigation Process is needed regardless
of whether a full team investigation is conducted.

Incident Investigation 2
3
Gather / Preserve evidence (Collecting evidence ASAP increases reliability)
• Collect pertinent information.
– identification of actors (persons or equipment that were actively involved)
– record their condition
– identify witnesses
• Record anything unusual at incident scene.
– position, appearance of equipment & tools
– physical agents (e.g. by smelling, hearing sounds)
– situations caused by weather conditions or lighting
• Take photos / video of incident scene or make sketches.
• Secure relevant records :
– Computer data / TDC / alarm system print outs
– Logs (e.g... shift change, preventive maintenance files / records)
– Work permits
– Work plans
Incident Investigation 2
4
Make Initial Incident Report
• Remember that this report is the foundation for activities like – further investigation
– Generating / supporting recommended actions
– future common cause analysis
• Utilize the site-specific incident reporting protocol
_ Capture data on Initial Incident Report Form – Input into YOUR SYSTEM (INTELEX,etc.)
• Be as factual as possible
• Do not speculate or include opinions. Just State the Facts !!!!!!!!

Incident Investigation 2
5
Critical Information
1. Who
2. What
3. Where
4. When
5. Why
6. How
7. This information fills in the blanks and creates a
timeline of events

Incident Investigation 2
6
https://s-media-cache-
ak0.pinimg.com/736x/d1/ef/30/d1e
f30c685e4e08b18a14994a3e39d9c.
jp
A Typical Timeline
Incident Investigation 2
7
Characterize Severity & Risk Potential
• The level of severity of the actual or potential
consequence determines the level of investigation.
• Tools and guides to characterize risk potential:
– Incident Categorization Matrix
– Risk Matrix
– Process Safety Measurement System
– Site-specific guidelines
Incident Investigation 2
8
For Most Incidents
• Generate Initial Incident Report (G Drive, Safety INCIDENT REPORTING, Initial Incident Report)
• Complete Blood Borne Pathogen Checklist if necessary (G Drive, Safety INCIDENT REPORTING, Blood Borne Pathogen Checklist)
• Enter into your reporting system
• Assign Action Items
• Follow Up as necessary
• If necessary, Start Secondary Investigation Process based on the Severity/Risk Model

Incident Investigation 2
9
What was the Cause?
• Incident or Near Miss ?
• What’s next ?
• Write an incident report based on this incident.

Incident Investigation 3
0
INCIDENT PROCESS PLOT (Timeline of Events)
1. 23:00 H
2. PROCES CONTROL ROOM
3. C. CHECK
4. GIVES ORDER TO BLOCK THE STEAM COIL IN THE TANK-TK858
REMARKS: DECIDED THAT IT HAD TO BE SOMETHING ELSE. (NOT AN INSTRUMENT
FAILURE) AND TEMPERATURE INDICATOR SHOWED 90 0C IN THE BOTTOM OF TANK
7. C. CHECK
1. 23:15 h
2. TANKFARM
3. TK-858
4. STEAM AND VAPORS (UNDER HIGH
PRESSURE) ARE VENTING FROM
EXHAUST TANK VENT
5. OPERATOR LEAVES SCENE
BEFORE
BLOCKING CONTROL VALVE.
REMARKS
7. P. STORE (TANK FARM
OPERATOR)
1.23:05 h
2. TANKFARM
3. TCV
4. STEAM TEMPERATURE CONTROL
VALVE IN OPEN POSITION
REMARKS
7. P. STORE (TANK FARM OPERATOR)
1. 23:40 h
2. TANKFARM
3. TK-858
4. VENTING VAPOR AND STEAM - ROOF
FAILURE
6. 6 HOURS
REMARKS: NO INJURY DUE TO THE
FACT THAT THE TANK FARM OPERATOR
LEFT THE INCIDENT SCENE WHEN THE
VENTING STARTED. IMPACT ON
ENVIRONMENT NOT YET ESTABLISHED.
7. P. STORE (TANK FARM OPERATOR)
23:00 23:40
Process Shift
Supervisor (C.
Check)
Cat Cracker Feed
Storage Tank
(TK-858)
1. 22:00 H
2. PROCESS CONTROL ROOM
3. D. SCREEN
4. HIGH TEMPERATURE ALARM (400F) ACCEPTED
6. 1 HOUR
REMARKS: THOUGHT THAT IT WAS A MALFUNCTIONING
INSTRUMENT
7. C. CHECK
Panel
Operator
(D.Screen)
26 MAY 199122:00
ACTORS
LINE
TIME
LINE
Temperature
Control Valve
1.23:05 h
2. TANKFARM
3. P. STORE (OPERATOR)
4. RESPOND TO ORDER TO BLOCK STEAM
TO COIL IN TK-858
REMARKS
7. P. STORE (TANK FARM OPERATOR)
Tank Farm
Operator
(P. Stone)

Incident Investigation 3
1
Risk Analysis, Follow-up,
Understanding
Work Practices / People
Equipment / Tools
Procedures
Training
Guidance / Supervision / Monitoring
Management / Leadership
Human Factor Engineering
People / Personal Performance
Communication
Causal Factors Why Tree Getting to Root Cause
Incident Investigation 3
2
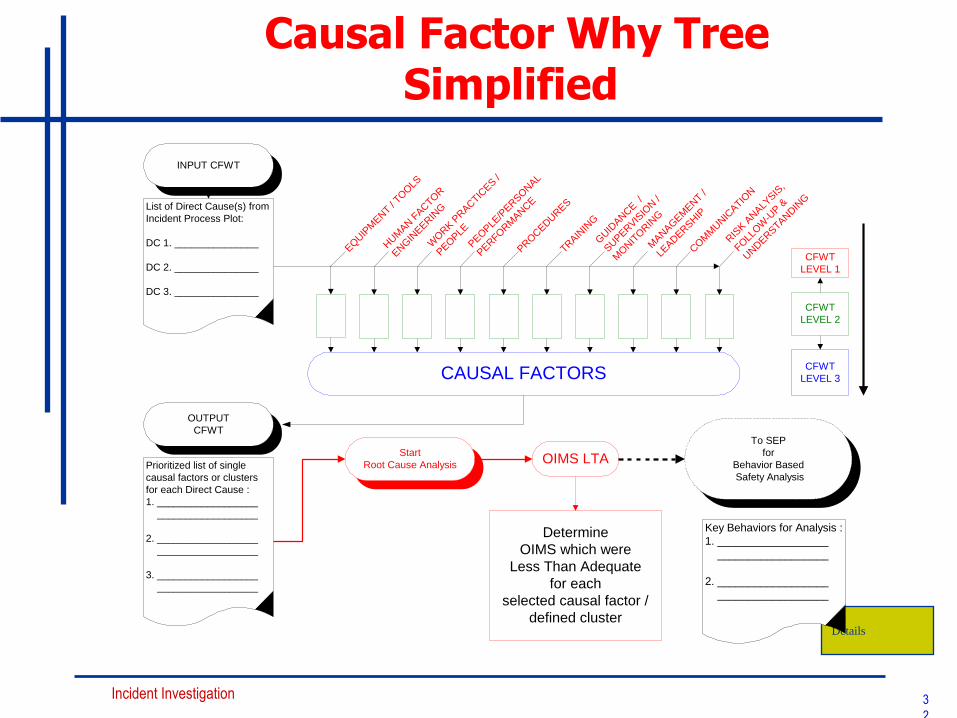
Causal Factor Why Tree Simplified
INPUT CFWT
CFWT
LEVEL 1
CFWT
LEVEL 3
CFWT
LEVEL 2
EQUIP
MENT /
TOOLS
HUM
AN F
ACTO
R
ENGIN
EERIN
G
WORK P
RACTIC
ES /
PEOPLE
PEOPLE
/PER
SONAL
PERFO
RM
ANCE
PROCEDURES
TRAIN
ING
GUID
ANCE /
SUPER
VIS
ION /
MONIT
ORIN
G
MANAGEM
ENT /
LEAD
ERSHIP
COM
MUNIC
ATIO
N
RIS
K A
NALY
SIS,
FOLL
OW
-UP &
UNDERSTA
NDIN
G
CAUSAL FACTORS
Start
Root Cause Analysis
To SEP
for
Behavior Based
Safety Analysis
Determine
OIMS which were
Less Than Adequate
for each
selected causal factor /
defined cluster
OIMS LTA
List of Direct Cause(s) from
Incident Process Plot:
DC 1. _______________
DC 2. _______________
DC 3. _______________
OUTPUT
CFWT
Prioritized list of single
causal factors or clusters
for each Direct Cause :
1. __________________
__________________
2. __________________
__________________
3. __________________
__________________
Details
Key Behaviors for Analysis :
1. __________________
__________________
2. __________________
__________________
Incident Investigation 3
3
Determine Root Causes
• For each selected Causal Factor from the CFWT, do
a separate Root Cause Analysis, identifying the
most important components in your EHS
Management System which were LTA
– For those identified management systems, determine
whether local management system was
» LTA - management system issue
» not understood - execution of management system issue
» not followed - execution/people behavior issue

Incident Investigation 3
4
Why use the CFWT
• Forces a logical, deductive analysis with repeatable results.
• Demonstrates visually where information may be missing.
• Demonstrates to others the depth and sensitivity of the
analysis.
• It yields quality identification of Causal Factors and Root
Causes which can be used to develop improvement
recommendations.
– Specific recommendations which are part of the incident report.
Incident Investigation
Assigning Action Items
• What are we going to do about this ?
• Who’s responsible for doing this ?
• What is the timeframe for completion ?
• How are we going to communicate to others?
3
5

Incident Investigation
Closing the Loop
• Tracking the action items to completion
• Document your findings
• Communication of Findings
• Training ?
• Documentation Updates ?
• USE YOUR MANAGEMENT OF CHANGE PROCESS
TO ACCOMPLISH ALL OF THE ABOVE !!!
3
6

Incident Investigation
IN A NUTSHELL ……….
This is an Analytical Troubleshooting Process that
can be used for ANYTHING ………………… QUALITY,
PRODUCTIVITY and SAFETY !!!!!!!!
3
7