incompatible kidney transplantation: strategies for ... · incompatible kidney transplantation:...
TRANSCRIPT

Apheresis Medicine in ABO Incompatible Kidney Transplantation:
Strategies for Successful Outcomes
Lance Williams, MD
Assistant Professor
Transfusion Medicine, Apheresis, and Coagulation

• No conflicts of interest to disclose relevant to this presentation

Kidney Transplant Benefits
• Life expectancy1
– In diabetics (Wolfe et al.), transplant increased life expectancy by a mean of 17 years compared with 8 years for treatment with dialysis alone
• Cost2
– 1972 Social Security Amendment guaranteed access to care for those with ESRD• Cost estimated at $75,000,000/year
– Cost of kidney transplant ~$110,000 the first year, then $19,000/year thereafter
Supply and Demand
• January 2016– 100,791 patients on the kidney transplant list
• Up from 77,684 in 2008!• ~7,000/year die or become too sick for transplant
– Median wait time on the list: 3.6 years
• In 2014, only 17,107 kidney transplants took place– 11,570 from deceased donors– 5,537 from living donors3
• Sensitization makes matching donors and recipients much more difficult– ~30% of those on the wait list are sensitized….may
increase wait time to 7 years!4,5

How to Overcome Kidney Shortage
• Redefine criteria for brainstem death
• Use dual kidney transplants for older, deceased donors
• Surgical techniques to decrease donor morbidity
– Laparoscopic
– Transumbilical
– Robot-assisted
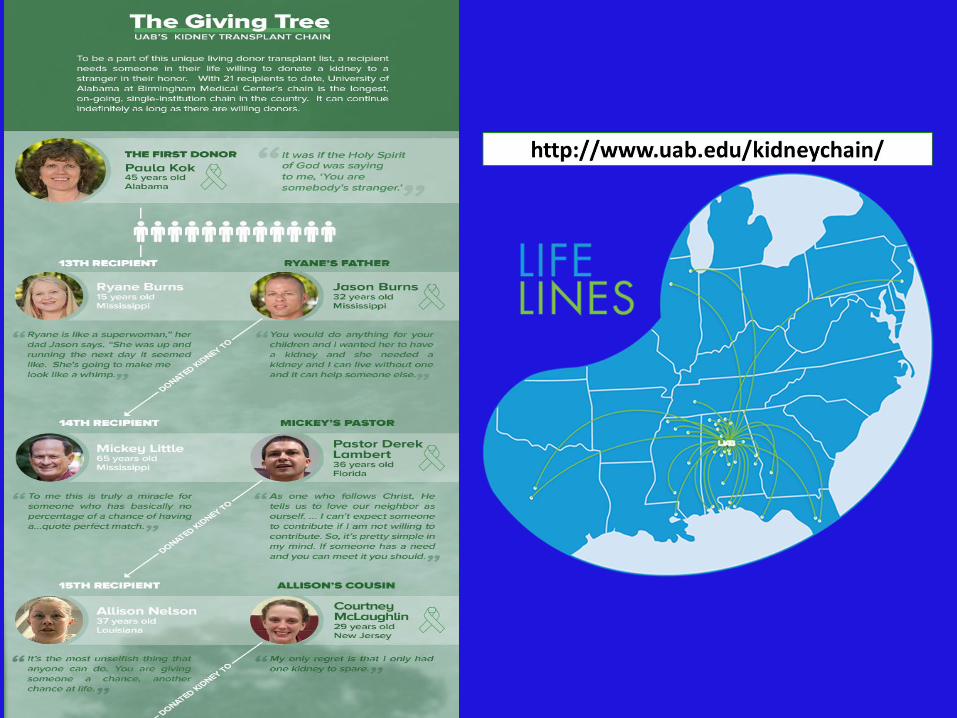
• Matched donor programs or kidney chains
• ABO-incompatible transplants

First Attempts at Kidney Transplant
• 1933 – Yurii Voronoy, MD6
– Deceased donor
– Patient Type O, Donor Type B
– Patient died after 2 days
• 1954 – Joseph Murray, MD7
– Living Donor, monozygotic twins
– Richard (recipient) and Ronald (donor) Herrick
– Richard lived 8 more years; Ronald lived 56 more years
– Dr. Murray received the Nobel Prize in 1990

Concepts of Successful Kidney Transplantation in Sensitized or
Incompatible Patients
• Remove antibodies with apheresis
– Number of procedures often based on titer
• Suppress further antibody production with immunosuppressive agents
• Monitor patient for continued graft function while accommodation takes place8
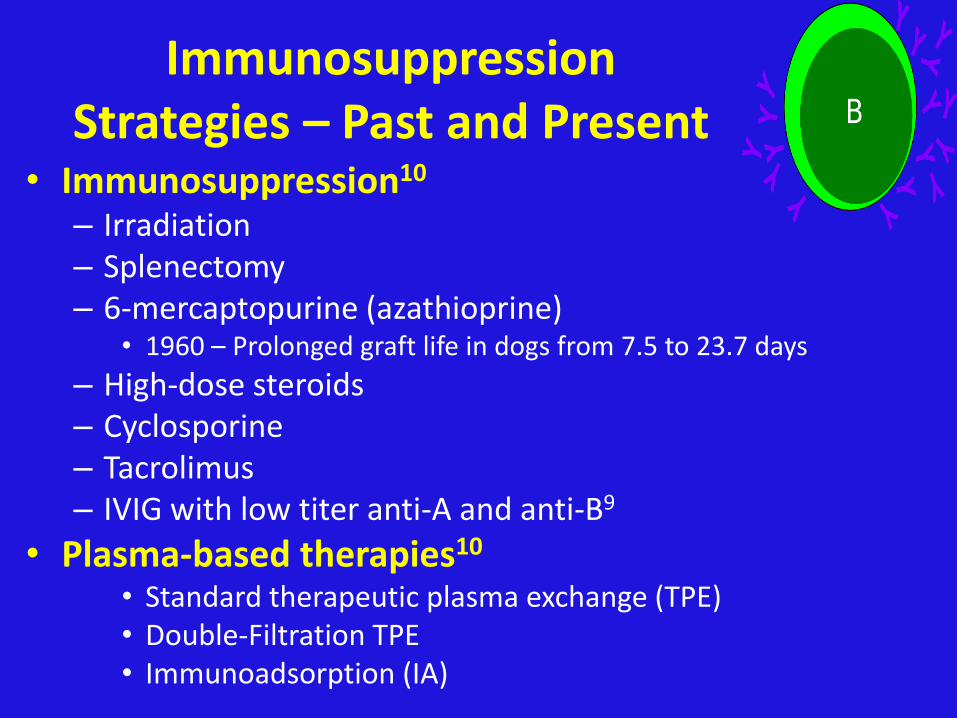
Immunosuppression Strategies – Past and Present
• Immunosuppression10
– Irradiation– Splenectomy– 6-mercaptopurine (azathioprine)
• 1960 – Prolonged graft life in dogs from 7.5 to 23.7 days
– High-dose steroids– Cyclosporine– Tacrolimus– IVIG with low titer anti-A and anti-B9
• Plasma-based therapies10
• Standard therapeutic plasma exchange (TPE)• Double-Filtration TPE• Immunoadsorption (IA)

But…What About ABOi Kidney Transplant (ABOi-KT)?
• 1955
– Another failed transplant by Hume et al. between a type B donor and a type O recipient11
• Chung et al., performed 10 ABOi transplants• 8 failed within days12
• 1982-1987• Alexandre finally has success
• 23 transplants with 75% graft survival at 1 year

ABO Basics13
ABO type
Antigens on RBC
Antibodies in serum/plasma
Prevalence in United States
Caucasian African-American
O Noneanti-A and
anti-B45% 49%
A A anti-B 40% 27%
B B anti-A 11% 20%
AB A and B none 4% 4%

ABOi-KT: A Paradigm Ready for Broad Implementation18
• 60 consecutive ABOi-KT
• 1999 to 2007
• TPE before and after transplant– Number of procedures based on starting titer
– Titer must be <16 prior to surgery
– Titers monitored daily, then at 2, 3, 6, and 12 months
– Titer rise ≥32 triggers biopsy and possible TPE
• 100 mg/kg IVIG (Cytogam) after each TPE
• Tacrolimus and mycophenolate mofetil (MMF) from day 1
• Dexamethosone 100 mg pre-op, then taper until tacrolimus in therapeutic range

ABOi-KT: A Paradigm Ready for Broad Implementation18
Transplantation. 2009 Apr 27;87(8):1246-55. doi: 10.1097/TP.0b013e31819f2024

ABOi-KT: A Paradigm Ready for Broad Implementation18

ABOi-KT: A Paradigm Ready for Broad Implementation18
• Rejection treatment
– Cellular
• 3-day course of dexamethosone (100 mg/day), followed by taper
– Antibody-mediated (AMR)
• TPE and IVIG until histologic resolution of rejection

ABOi-KT: A Paradigm Ready for Broad Implementation18
• Graft Survival
– 1 year 98.3%
– 3 years 92.9%
– 5 years 88.7%
• No hyperacute rejection or graft loss from AMR
– Splenectomy not necessary to prevent antibody mediated rejection in ABOi-KT
– Tight control of ABO titers in peri-transplant period allowed for elimination of rituximab (anti-CD20) from protocol
– High starting titer not predictive of graft failure due to AMR (controversial statement)18

Roles of Apheresis in ABOi-KT
• Pre-transplant
– “Desensitization” along with IVIG
• Post-transplant
–Continued “desensitization”
–And / or treatment of AMR
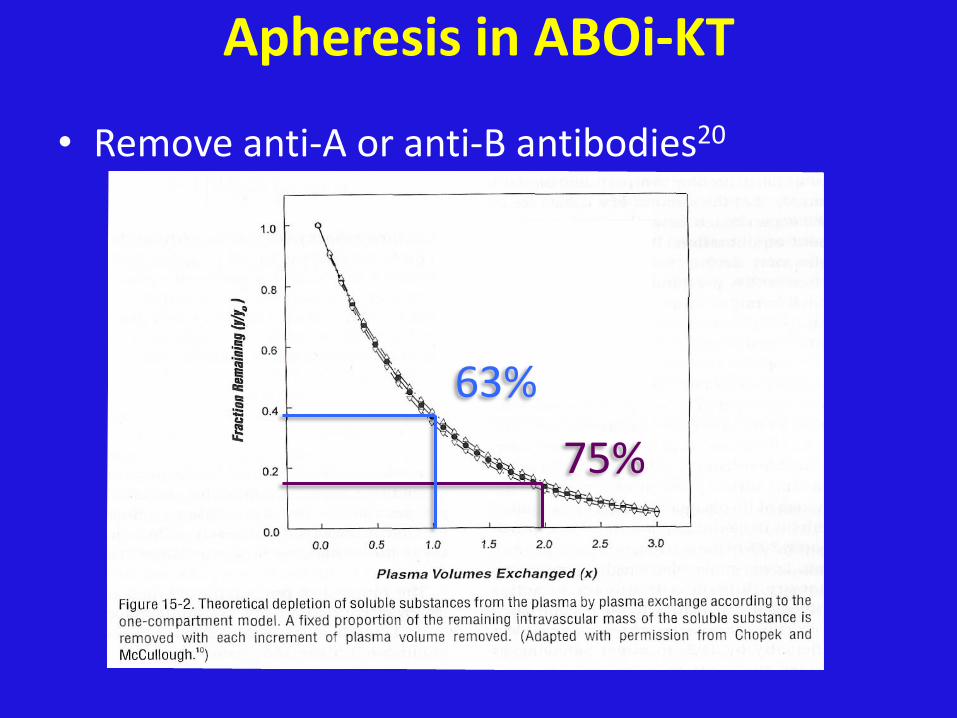
Apheresis in ABOi-KT
• Remove anti-A or anti-B antibodies20
75%
63%

ASFA Guidelines for Kidney Transplant21
J Clin Apher 2013; 28:145–284.

Evidence for Apheresis in Kidney Transplant8
J Clin Apher. 2011;26(5):252-60. doi: 10.1002/jca.20297. Epub 2011 Sep 5. Review.

Apheresis Methodologies in ABOi-KT
• Standard therapeutic plasma exchange (TPE)
• Immunoadsorption
–Mainly used in Europe
• Double filtration plasma exchange
–Mainly used in Japan

Therapeutic Plasma Exchange
TPE Advantages and Disadvantages
• Advantages
– Removes both IgG, IgM, and complement
– Allows for isovolemic plasma replacement pre-op
– May remove other antibodies that play a role in rejection
• Disadvantages
– Is non-selective in removal of immunoglobulins
– Depletes coagulation factors
– Some studies demonstrate increased bleeding and increased infections with TPE9

Immunoadsorption of ABO Antibodies
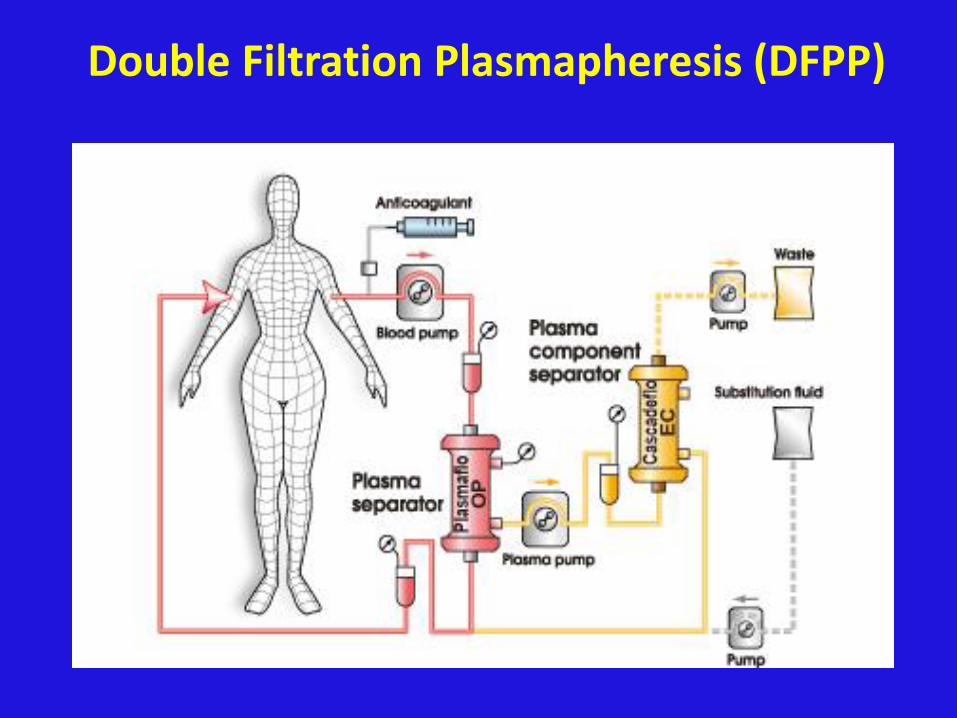
Double Filtration Plasmapheresis (DFPP)
Procedure Details for TPE
• Pre-op
– TPE typically performed every other day 3-5 times
• Post-op
– Up to the discretion of the transplant team
• Replacement fluid
– 5% Albumin for most procedures
– For the day before and day after surgery, some centers use half albumin and half plasma to prevent coagulation factor depletion perioperatively

Procedure Details for TPE • Labs
– Basic metabolic panel, mainly for electrolytes
– CBC
• Evaluate hematocrit to see if ECV will exceed 15%
• Avoid RBC transfusion, if possible
– Fibrinogen
• If low, either skip procedure or replace with blood products
– Donor-specific antibodies (DSAs) levels
– Anti-A or anti-B titers before and after procedure

Procedure Details for TPE
• Calcium supplementation
–Used to prevent citrate toxicity / hypocalcemia
– Either added to albumin bottles and / or given as IV drip
– ½ Plasma typically used the day before and the day after surgery
• Higher citrate load

Compatible Blood Products13
Recipient type
RBCsAVOID foreign
antigen
PlasmaAVOID antibody against
recipient RBCA A or O A or ABB B or O B or AB
AB AB, A, B, or O ABO O O, A, B, or AB
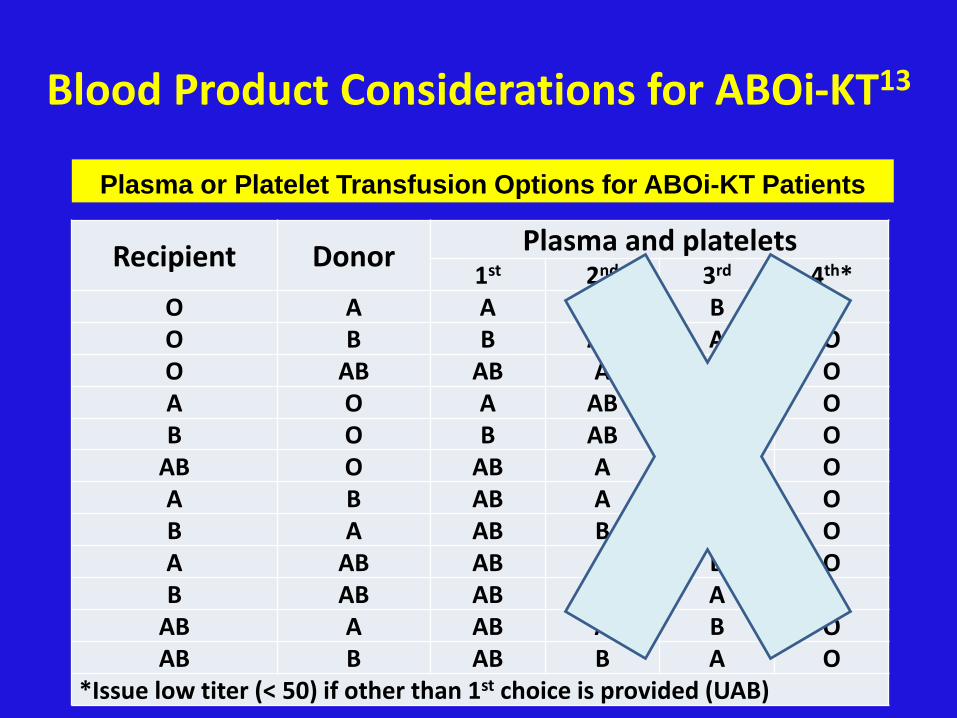
Blood Product Considerations for ABOi-KT13
Recipient Donor Plasma and platelets1st 2nd 3rd 4th*
O A A AB B OO B B AB A OO AB AB A B OA O A AB B OB O B AB A O
AB O AB A B OA B AB A B OB A AB B A OA AB AB A B OB AB AB B A O
AB A AB A B OAB B AB B A O
*Issue low titer (< 50) if other than 1st choice is provided (UAB)
Plasma or Platelet Transfusion Options for ABOi-KT Patients

Case Study• January 2014
• 59 year old male, O negative
– Donor Type A negative
• Received 5 pre-transplant TPEs
• Day before surgery, TPE with 50% O plasma and 50% albumin as the replacement fluids = BIG PROBLEM
– Anti-A titer rose from 16 to 32 (pre- to post-TPE)
– Procedure repeated overnight with the correct plasma (type A)
• Post-TPE and pre-op, titers decreased to 8
• Transplant proceeded without problems
• Graft remains functional 2 years later

Titer Measurement• IgG (anti-A or anti-B) functionally significant in
ABOi9
• High variability in tube titers among centers
– Interinstitutional variability
• 8 to 32 for IgM
• 16 to 256 for IgG
– Gel and flow cytometry more reproducible26,27
Tube Testing Gel Testing Flow Cytometry

Case Study28
• 52 year old type O male
• ESRD secondary to IgA nephropathy
• Donor is type A
• Pre-transplant anti-A titer 4 after 5 TPEs
• Post-transplant titers rising
– TPE is re-initiated along with post-TPE IVIG
• However, titers continue to rise even with daily TPE???
– Could the IVIG have high titer anti-A or anti-B???

Accommodation
• Even with optimal protocols, titer may return to baseline within 1 week of transplant15
• Intense monitoring of titers 2 weeks after transplant is advisable
• Accommodation
– Allows for survival of graft, even with increasing titers
– Thought to be a change of antibody specificity, avidity, and affinity
– Possible alteration of antigen structure9

Procedure-Related Adverse Events
• Mild allergic (urticaria, hives) - 4.3%
• Citrate toxicity (lack of renal function) - 6.8%
• Anaphylactic reactions (IgA deficiency) - rare
• Hypotension - 2.9%
– Procedure-related (ECV)
– Associated with ACE-inhibitor use
• Nausea and vomiting – 1.2%
• TRALI (plasma use pre- and post-op)29
• Infectious disease transmission from blood products (e.g. WNV)30
Apheresis in the Treatment of AMR
• AMR occurs in 30-60% of ABOi-KT
• Donor-directed antibodies: graft destruction/dysfunction
• Importantly, C4d staining cannot be used as the only sign of AMR in ABOi transplants!!!33-36
– C4d staining positive in 94% of ABOi-KT at 3 months post-KT WITHOUT any signs of AMR…compared with only 11% of ABOc-KTs with C4d staining

Apheresis in the Treatment of AMR
• Other recommended findings37
• Neutrophils in peritubular capillaries; acute tubular necrosis; arterial fibrinoid necrosis / transmural arteritis; intracapillary fibrin thrombi in glomeruli; RBC stasis
• Advanced stages => Tubular dilatation and epithelial flattening
• Laboratory and / or clinical signs of graft dysfunction

Apheresis in the Treatment of AMR - continued
• Lefaucher and colleagues39
– IVIG Group = 12 patients
• IVIG (2g/kg) given over 2 days, every 3 weeks, 4 times
• Graft survival at 36 months: only 50%
– IVIG, rituximab, and TPE Group = 12 patients
• Daily TPE for 4 days with low dose IVIG (100 mg/kg)
• High-dose IVIG as above
• Rituximab (375mg/m2) x 2 for 2 weeks
• Graft survival at 36 months: 91%!

KEYS to a Successful ABOi Program
• Communication!– Calendars
– Computer alerts
• Education– Nurses, residents/fellows, Attendings, blood bank
staff, patients, family members
• Being OCD
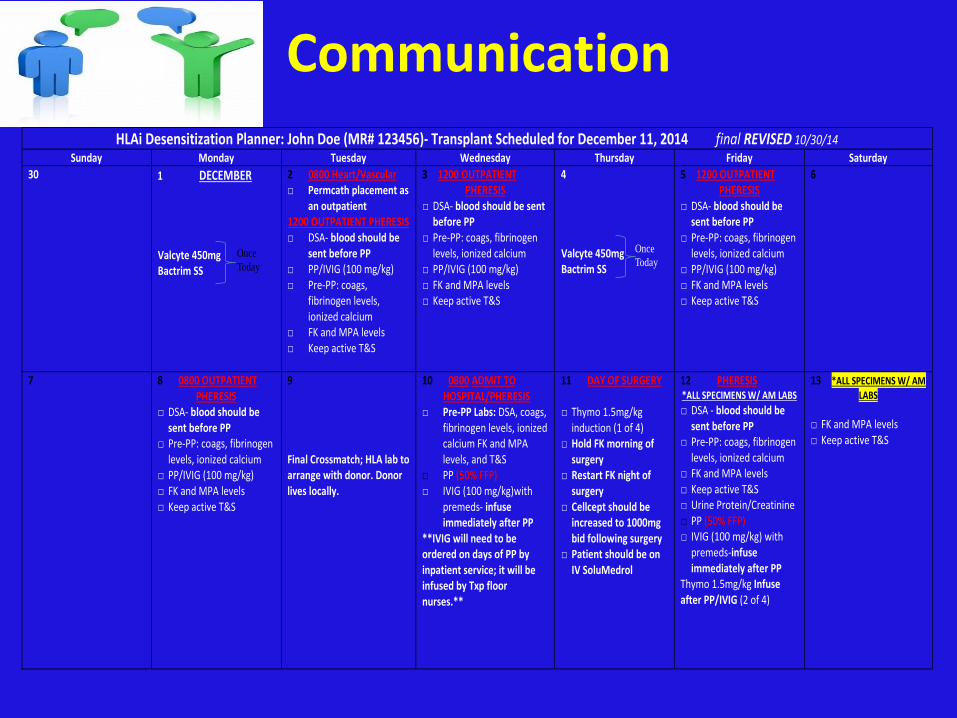
CommunicationHLAi Desensitization Planner: John Doe (MR# 123456)- Transplant Scheduled for December 11, 2014 final REVISED 10/30/14
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
30 1 DECEMBER Valcyte 450mg Bactrim SS
2 0800 Heart/Vascular □ Permcath placement as
an outpatient 1200 OUTPATIENT PHERESIS □ DSA- blood should be
sent before PP □ PP/IVIG (100 mg/kg) □ Pre-PP: coags,
fibrinogen levels, ionized calcium
□ FK and MPA levels □ Keep active T&S
3 1200 OUTPATIENT PHERESIS
□ DSA- blood should be sent before PP
□ Pre-PP: coags, fibrinogen levels, ionized calcium
□ PP/IVIG (100 mg/kg) □ FK and MPA levels □ Keep active T&S
4 Valcyte 450mg Bactrim SS
5 1200 OUTPATIENT PHERESIS
□ DSA- blood should be sent before PP
□ Pre-PP: coags, fibrinogen levels, ionized calcium
□ PP/IVIG (100 mg/kg) □ FK and MPA levels □ Keep active T&S
6
7
8 0800 OUTPATIENT PHERESIS
□ DSA- blood should be sent before PP
□ Pre-PP: coags, fibrinogen levels, ionized calcium
□ PP/IVIG (100 mg/kg) □ FK and MPA levels □ Keep active T&S
9 Final Crossmatch; HLA lab to arrange with donor. Donor lives locally.
10 0800 ADMIT TO HOSPITAL/PHERESIS □ Pre-PP Labs: DSA, coags,
fibrinogen levels, ionized calcium FK and MPA levels, and T&S
□ PP (50% FFP) □ IVIG (100 mg/kg)with
premeds- infuse immediately after PP
**IVIG will need to be ordered on days of PP by inpatient service; it will be infused by Txp floor nurses.**
11 DAY OF SURGERY
□ Thymo 1.5mg/kg induction (1 of 4)
□ Hold FK morning of surgery
□ Restart FK night of surgery
□ Cellcept should be increased to 1000mg bid following surgery
□ Patient should be on IV SoluMedrol
12 PHERESIS *ALL SPECIMENS W/ AM LABS
□ DSA - blood should be sent before PP
□ Pre-PP: coags, fibrinogen levels, ionized calcium
□ FK and MPA levels □ Keep active T&S □ Urine Protein/Creatinine □ PP (50% FFP) □ IVIG (100 mg/kg) with
premeds-infuse immediately after PP
Thymo 1.5mg/kg Infuse after PP/IVIG (2 of 4)
13 *ALL SPECIMENS W/ AM
LABS
□ FK and MPA levels □ Keep active T&S
Once
Today
Once
Today

The Future of Kidney Transplantation
• Organs grown in laboratory using stem cell technology
• Xenotransplants (transgenic pigs)
• Apheresis has allowed us to break the ABO barrier in kidney transplantation
• Apheresis is an effective part of the treatment regimen for AMR in ABOitransplants

Comments or Questions?

References• 1. Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999 Dec
2;341(23):1725-30.
•
• 2. U.S. Renal Data System Atlas of End-Stage Renal Disease in the United States. USRDS. 2010 Annual Data Report 2009. Available online at http://www.usrds.org/adr/htm
•
• 3. National Kidney Foundation. Organ Donation and Transplant Statistics. Available online at https://www.kidney.org/news/newsroom/factsheets/Organ-Donation-and-Transplantation-Stats. Accessed April 2, 2016
•
• 4. US Renal Data System, USRDS 2010 Annual Data Report. Atlas of chronic kidney disease and end-stage renal disease in the united states, national institutes of health, national institute
• of diabetes and digestive and kidney diseases, Bethesda, MD, 2010.
•
• 5. US Renal Data System, USRDS 2011 Annual Data Report. Atlas of chronic kidney disease and end-stage renal disease in the united states, national institutes of health, national institute
• of diabetes and digestive and kidney diseases, Bethesda, MD, 2011.
•
• 6. Hamilton DN, Reid WA. Yu. Yu. Voronoy and the first human kidney allograft. Surg Gynecol Obstet. 1984;159(3):289-294.
•
• 7. Guild WR, Harrison JH, Merrill JP, Murray J. Successful homotransplantation of the kidney in an identical twin. Trans Am Clin Climatol Assoc. 1955-1956;67:167-173.
•
• 8. George SM, Balogun RA, Sanoff SL. Therapeutic apheresis before and after kidney transplantation. J Clin Apher. 2011;26(5):252-60. doi: 10.1002/jca.20297. Epub 2011 Sep 5. Review.
•
• 9. Muramatsu M, Gonzalez HD, Cacciola R, Aikawa A, Yaqoob MM, Puliatti C. ABO incompatible renal transplants: Good or bad? World J Transplant. 2014 Mar 24;4(1):18-29. doi: 10.5500/wjt.v4.i1.18. Review.
•
• 10. Shrestha B, Haylor J, Raftery A. Historical perspectives in kidney transplantation: an updated review. Prog Transplant. 2015 Mar;25(1):64-9, 76. doi: 10.7182/pit2015789. Review.
•
• 11. Hume DM, Merrill JP, Miller BF, Thorn GW. Experiences with renal homotransplantation in the human: report of nine cases. J Clin Invest 1955;34:327–382.
•
• 12. Chung BH, Lee JY, Kang SH, et al. Comparison of patient outcome according to renal replacement modality after renal allograft failure. Ren Fail. 2011;33(3):261-268.
•
• 13. Williams LA, Marques MB, Fritsma MG. Quick Guide to Transfusion Medicine. AACC. 2014.
•
• 14. Alexandre GP, De Bruyere M, Squifflet JP, Moriau M, Latinne. D, Pirson Y. Human ABO-incompatible living donor renal homografts. Neth J Med 1985;28:231–234.
• 15. Alexandre GP, Squifflet JP, De Bruyere M, et al. Present experiences in a series of 26 ABO-incompatible living donor renal allografts. Transplant Proc. 1987;19(6):4538-4542.
•
• 16. Ishida H, Tanabe K, Toma H, Akiba T. Therapeutic apheresis therapy for ABO-incompatible renal transplantations. Ther Apher Dial. 2003;7(6):520-528.
•
• 17. Segev DL, Gentry SE, Warren DS, et al. Kidney paired donation and optimizing the use of live donor organs. JAMA 2005; 293: 1883.
•
• 18. Montgomery RA, Locke JE, King KE, Segev DL, Warren DS, Kraus ES, Cooper M, Simpkins CE, Singer AL, Stewart ZA, Melancon JK, Ratner L, Zachary AA, Haas M.
• ABO incompatible renal transplantation: a paradigm ready for broad implementation.
• Transplantation. 2009 Apr 27;87(8):1246-55. doi: 10.1097/TP.0b013e31819f2024
•
• 19. Opelz G1, Morath C, Süsal C, Tran TH, Zeier M, Döhler B. Three-year outcomes following 1420 ABO-incompatible living-donor kidney transplants performed after ABO antibody reduction: results from 101 centers. Transplantation. 2015 Feb;99(2):400-4. doi: 10.1097/TP.0000000000000312.
•
• 20. McLeod; Apheresis: Principals and Practice (2010).
•
• 21. Schwartz J, Winters JL, Padmanabhan A, et al. Guidelines on the use of therapeutic apheresis in clinical practice—evidence-based approach from the Writing Committee of the American Society for Apheresis. J Clin Apher 2013; 28:145–284.
References• 22. Sharif A, Alachkar N, Kraus E. Incompatible kidney transplantation: a brief overview of the past, present and future. QJM. 2012 Dec;105(12):1141-50. doi: 10.1093/qjmed/hcs154. Epub 2012 Aug 20. Review•
• 23. Tyden G, Donauer J, Wadstrom J, Kumlien G, Wilpert J, Nilsson T, Genberg H, Pisarski P, Tufveson G. Implementation of a protocol for ABO-incompatible kidney transplantation—a three center experience with 60 consecutive transplantations. Transplantation 2007;83:1153–1155.
•
• 24. Tanabe K. Double-filtration plasmapheresis. Transplantation 2007; 84: S30-S32 [PMID: 18162985 DOI: 10.1097/01.tp.0000296103.34735.b8]•
• 25. Nakanishi T, Suzuki N, Kuragano T, Nagasawa Y, Hasuike Y. Current topics in therapeutic plasmapheresis. Clin Exp Nephrol 2014; 18: 41-49 [PMID: 23887747 DOI: 10.1007/• s10157-013-0838-0]•
• 26. Kumlien G, Wilpert J, Säfwenberg J, Tydén G. Comparing the tube and gel techniques for ABO antibody titration, as performed in three European centers. Transplantation 2007; 84: S17-S19 [PMID: 18162980 DOI: 10.1097/01.tp.0000296019.85986.af]
•
• 27. TanabeK:Interinstitutionalvariationinthemeasurementof anti-A/B antibodies:theJapaneseABO-IncompatibleTransplan- tation Committeesurvey. Transplantation 84:S13–S16,2007. •
• 28. Staley EM1, Carruba SS2, Manning M2, Pham HP1, Williams LA 3rd1, Marques MB1, Locke JE3, Lorenz RG1 Anti-blood group antibodies in intravenous immunoglobulin may complicate interpretation of antibody titers in ABOi transplantation. Am J Transplant. 2016 Feb 23. doi: 10.1111/ajt.13760. [Epub ahead of print].
•
• 29. Tobian AA, Shirey RS, Montgomery RA, Tisch DJ, Ness PM, King KE. Therapeutic plasma exchange reduces ABO titers to permit ABO-incompatible renal transplantation. Transfusion• 2009; 49: 1248-1254 [PMID: 19210321 DOI: 10.1111/j.1537-2995.2008.02085.x]•
• 30. Shepherd JC, Subramanian A, Montgomery RA, et al. West Nile virus encephalitis in a kidney transplant recipient.AmJ Transplant 2004; 4: 830.•
• 31. Grim SA, Pham T, Thielke J, Sankary H, Oberholzer J, Benedetti E, Clark NM. Infectious complications associated with the use of rituximab for ABO-incompatible and positive cross-match renal transplant recipients. Clin Transplant 2007; 21: 628-632 [PMID: 17845637 DOI: 10.1111/j.1399-0012.2007.00700.x]
•
• 32. Kasiske BL, Snyder JJ, Gilbertson DT, Wang C. Cancer after kidney transplantation in the United States. Am J Transplant 2004; 4: 905-913 [PMID: 15147424 DOI: 10.1111/• j.1600-6143.2004.00450.x]•
• 33. Haas M, Segev DL, Racusen LC, Bagnasco SM, Locke JE, Warren DS, Simpkins CE, Lepley D, King KE, Kraus ES, Montgomery RA. C4d deposition without rejection correlates with reduced early scar- ring in ABO-incompatible renal allografts. J Am Soc Nephrol 20:197–204,2009.
•
• 34. Setoguchi K, Ishida H, Shimmura H, Shimizu T, Shirakawa H, Omoto K, Toki D, Iida S, Setoguchi S, Tokumoto T, Horita S, Nakayama H, Yamaguchi Y, Tanabe K. Analysis of renal transplant protocol biopsies in ABO-incompatible kidney transplantation. Am J Transplant 8:86–94, 2008.
•
• 35. Haas M, Rahman MH, Racusen LC, Kraus ES, Bagnasco SM, Segev DL, Simpkins CE, Warren DS, King KE, Zachary AA, Montgomery RA. C4d and C3d staining in biopsies of ABO- and HLA-incompatible renal allografts:correlation with histologic findings. Am J Transplant 6:1829–1840,2006.
•
• 36. Takahashi K, Saito K, Nakagawa Y, Tasaki M, Hara N, Imai N. Mechanism of acute antibody-mediated rejection in ABO- incompatible kidney transplantation: which anti-A/anti-B antibodies are responsible, natural or de novo? Transplantation 89:635–637,2010.
•
• 37. Racusen LC, Haas M. Antibody-mediated rejection in renal allografts: lessons from pathology. Clin J Am Soc Nephrol 2006;1:415–420.•
• 38. Brown CM, Abraham KA, O'Kelly P, Conlon PJ, Walshe JJ. Long-term experience of plasmapheresis in antibody-mediated rejection in renal transplantation. Transplant Proc. 2009 Nov;41(9):3690-2. doi: 10.1016/j.transproceed.2009.06.197.•
• 39. Lefaucheur C, Nochy D, Andrade J, Verine J, Gautreau C, Charron D, Hill GS, Glotz D, Suberbielle-Boissel C. Comparison of combination Plasmapheresis/IVIg/anti-CD20 versus highdose IVIG in the treatment of antibody-mediated rejection. Am J Transplant 2009;9:1099–1107.
•
• 40. Schwartz J, Stegall MD, Kremers WK, Gloor J. Complications, resource utilization, and cost of ABO-incompatible living donor kidney transplantation. Transplantation 2006; 82: 155-163 [PMID: 16858274 DOI: 10.1097/01.tp.0000226152.13584.ae]•
• 41. Schnitzler M, Machnicki G. ABO-incompatible living donor transplantation: is it economically “compatible”? Transplantation 2006; 82: 168-169 [PMID: 16858277 DOI: 10.1097/01.tp.0000226242.10027.e7]