increased in cd8 t lymphocytes in the bal fluid of patients with sulfur mustard gas-induced...
TRANSCRIPT

ARTICLE IN PRESS
Respiratory Medicine (2007) 101, 786–792
0954-6111/$ - see frdoi:10.1016/j.rmed.
�Corresponding au
E-mail address: l
Increased in CD8 T lymphocytes in the BAL fluid ofpatients with sulfur mustard gas-inducedpulmonary fibrosis
Ali Emad�, Yasaman Emad
Shiraz University of Medical Sciences, Pulmonary Section, Shiraz, Iran
Received 3 June 2006; accepted 4 August 2006
KEYWORDSBAL;CD8;Pulmonary fibrosis;Mustard
ont matter & 20062006.08.003
thor. Tel.: +98 711
SummaryObjective: In an attempt to understand better the potential role of the T cell in thepathogenesis of pulmonary fibrosis (PF) due to sulfur mustard gas inhalation, this study wasdesigned to analyze bronchoalveolar lavage (BAL) lymphocyte subsets and to determinethe ratio of CD4 to CD8 lymphocytes in BAL fluid.Setting: University hospital.Patients: Twenty-one veterans with mustard gas-induced pulmonary fibrosis and 20normal veterans as control group.Intervention: Chest roentgenograms, pulmonary function tests (PFTs), tests for carbonmonoxide diffusing capacity of the lung (DLCO), high-resolution CT scans of the chest, BALvia fiberoptic bronchoscopy, analyses of BAL fluids for cellular and Flow-cytometric analysisof the phenotype of bronchoalveolar cells were performed in all cases. A transbronchiallung biopsy was done in all patients following BAL.Results: Neutrophilic alveolitis was the predominant feature. Neutrophils (Po0:0001) andeosinophils (P ¼ 0:0006) were the predominant cell types in the BAL fluid of patients withPF. CD8 lymphocytes expressed as percentage or absolute number were significantly higherin patients with PF than in healthy controls (22.9677.48% vs. 14.1677.73%, respectively;P ¼ 0:0006; and 2.2870.84 vs. 1.1070.55� 103 cells/ml, respectively; Po0:0001). TheCD4/CD8 ratio was significantly lower in patients with PF than in healthy controls(0.7370.25 vs. 1.5870.67; Po0:0001). Except for the percentage and the absolutenumber of the BAL fluid neutrophils (r ¼ 0:70, P ¼ 0:001: r ¼ �0:62, P ¼ 0:005;respectively), no correlation was found between DLCO% and the other BAL cells. Asignificant negative correlation was observed between the percentage of DLCO and boththe percentage and the absolute number of CD8 lymphocytes in BAL fluid in patients withPF (r ¼ �0:81, P ¼ 0:0003; r ¼ �0:61, P ¼ 0:006; respectively). A significant correlationwas also seen between the percentage of DLCO and the CD4/CD8 ratio (r ¼ �0:60,P ¼ 0:006) in our patients.
Elsevier Ltd. All rights reserved.
8321345.
s.ac.ir (A. Emad).

ARTICLE IN PRESS
Role of T lymphocytes in pathogenesis of pulmonary fibrosis 787
Conclusion: CD8 Tcells in BAL fluid were significantly elevated in patients with pulmonaryfibrosis. Patients with higher grades of pulmonary fibrosis expressed as percentage ofDLCO, revealed higher percentages and the absolute number of CD8 T cells and a lowerCD4/CD8 ratio.& 2006 Elsevier Ltd. All rights reserved.
Introduction
The toxicity of the chemical warfare blistering agent sulfurmustard (2,20-dichlorodiethyl sulfide; SM) has been investi-gated for nearly a century.1,2 This toxic gas can damage tothe eyes and respiratory tract when present in high doses.3
Pulmonary fibrosis (PF) is a well-known late complicationof sulfur mustard gas exposure in human.4 Although therespiratory tract lesions represent the major debility aftersulfur mustard exposure, only a few studies have investi-gated the pathophysiology of sulfur mustard-induced re-spiratory diseases, in particular the mechanisms involved ininflammatory processes.
CD8 T cells infiltrate the lung in many clinical conditions,particularly in interstitial lung disease.5 The role(s) that CD8T cells might be playing in the pathogenesis of inflammatorylung disease is unclear at present, as is the directcontribution of CD8 T cell effector activities to lung injury.According to this fact alterations in bronchoalveolar lavage(BAL) CD4/CD8 T cell subset ratios have been demonstratedin a variety of different respiratory disorders and themeasurement of these changes may be diagnostically help-ful. Therefore, the CD4/CD8 ratio in BAL is an index that isconsidered, at least in clinical respiratory medicine, asindicative for different types of interstitial lung disease. Anelevated CD4/CD8 ratio in BAL is often seen in patients withsarcoidosis and other granuloma-producing diseases, such asasbestosis, Crohn’s disease berryliosis, and rheumatoidarthritis.6–10 A reduced CD4/CD8 ratio has been observedin various other immunologic interstitial lung diseases,including drug-induced alveolitis, extrinsic allergic alveoli-tis, bronchiolitis obliterans organizing pneumonia (BOOP),and in patients infected with HIV.11–14 A normal CD4/CD8BAL proportion has been described in patients with silicosisand asymptomatic granite workers.15,16
It could, therefore, be anticipated that the lymphocytesmay also play a role in the response to inhaled mustard gas.In an attempt to understand better the potential role of theT cell in the pathogenesis of PF due to sulfur mustard gasinhalation; this study was designed to analyze BAL lympho-cyte subsets and to determine the ratio of CD4 to CD8lymphocytes in BAL fluid in our victims with PF.
Methods
Patient population
Of all the veterans admitted to our university teachinghospital in 1986 with a single large exposure to sulfurmustard gas, 21 male patients were enrolled into this studyafter meeting all of the following criteria for PF diagnosis:(a) an interstitial pattern on a chest roentgenogram, (b) arestrictive pattern in spirometric studies, (c) a decreased
single-breath carbon monoxide diffusing capacity of the lung(DLCO), and (d) a confirmatory transbronchial lung specimenbiopsy specimen showing evidence of interstitial pneumoni-tis with varying degrees of interstitial fibrosis withoutevidence of granuloma formation.17 The patients’ exposureto sulfur mustard gas had been confirmed by studies on theirurine and vesicular fluid in 1986.
None of the patients had any evidence of connectivetissue disorders, sarcoidosis, eosinophilic granuloma, pneu-moconiosis, carcinomatosis, or lymphoma. Patients withevidence of bacterial, mycobacterial and fungal infectionswere also excluded. All these patients had persistentintermittent cough from their exposures till now. Gradualdecline in pulmonary function tests (PFTs) occurred follow-ing the initial gas exposure. The diagnosis of PF was madewithin 2 years of the acute and massive sulfur mustard gasinhalation in these victims. All were treated by intermittentlow dose prednisolon (2.5–7.5mg) for more than 6 years. Allof the cases were lifetime nonsmokers. They signed awritten informed consent form and underwent a thoroughhistory and physical examination. Prior to undergoingbronchoscopy and PFTs, oral corticosteroid therapy waswithdrawn for at least 1 month. A chest roentgenogram, anECG, and a high-resolution CT (HRCT) of the chest wereobtained in each patient. The HRCT scans were done with1- to 1.5-mm sections taken at 1-cm intervals through theentire thorax and were reconstructed using a bonealgorithm. The study was approved by the Ethics Committeeof our university.
Control group
The control group consisted of 20 normal, healthy nonsmok-ing veterans with a mean (7SD) age of 35.6074.51 years old(range, 29–48 years old); the control subjects had partici-pated in the Iran–Iraq War but had not been exposed tomustard gas. All subjects voluntarily entered the study andsigned an informed consent form before their enrollment.All subjects had a complete history and physical examina-tion. No subjects had a history of exposure to organic orinorganic dusts. In addition to obtaining a chest radiographand an ECG for each subject, PFTs were measured prior tobronchoscopy as well. The examination of BAL cells and thedetermination of T cells were carried out for all cases usingthe same techniques as described for the patients group. Notransbronchial biopsies were performed in the controlgroup.
Measurement of pulmonary function and DLCO
Prior to bronchoscopy, PETs were performed in all patients.These tests were measured through spirometric and lungvolumes assessment according to the standards advocated

ARTICLE IN PRESS
A. Emad, Y. Emad788
by the American Thoracic Society.18 An experienced physi-cian did all spirometric and lung volumes measurements bythe helium dilution method with a Master Screen apparatus(Erich Jaeger GmbH, Wuerzburg, Germany), and DLCO bythe single breathholding helium dilution method.19 Eachpatient was well trained to give his best effort. Results wereexpressed as percentage predicted based on acceptedreference standards.20 The highest values were chosen andreported.
Bronchoscopy and bronchoalveolar lavage (BAL)
All of the patients underwent a bronchoscopic examinationin 2005. Before any lung biopsy specimens were taken, BALwas performed using a flexible fiberoptic bronchoscope(Olympus BF1T; Tokyo, Japan). Each patient was premedi-cated with atropine (0.75mg IM) before the procedure. Mildsedation was achieved with intravenously administeredmidazolam, and supplementary oxygen was given through-out the procedure. Patient oxygenation was monitored bypulse oximetry. After applying 4% lignocaine spray to thenose and throat of the patient, the flexible bronchoscopewas introduced. Local anesthesia of the larynx was achievedwith topical 4% lignocaine, whilst a 2% solution was usedbelow the vocal cords to suppress coughing. The broncho-scope was wedged for lavage in the middle lobe segmentalbronchus, and four 60-ml aliquots of sterile physiologicsaline solution warmed to 37 1C were infused. The fluid wasimmediately recovered by gentle suction after each instilla-tion. The first aliquot reflecting a bronchial sample wasdiscarded, while the others were pooled for our study. TheBAL fluid was passed through monolayer surgical gauze toeliminate mucus. One small aliquot of this fluid was utilizedto count the total cell number, and another aliquot was spunin a cytometer at 400 revolutions/min for 10min. The cellpellet was washed once in Hanks’ balanced salt solution(without calcium and magnesium). A May–Grunwald–Giemsastain smear was used to identify the differential profilesafter cytospin preparation. Total cell counts were deter-mined with a hemocytometer. The differential cell count oflymphocytes, neutrophils, macrophages, and eosinophilswas made under light microscopy � 1000 by countingapproximately 300 cells in a random field. The result wasexpressed as cells � 103/ml. The unconcentrated super-natant was frozen at �70 1C before the protein wasmeasured.
Transbronchial lung biopsyA transbronchial lung biopsy was performed in all patientsfollowing BAL. Biopsy specimens were obtained from allthree lobes on the right side or from the upper and lowerlobes of the left lung. The lung biopsy specimens wereinterpreted by a pathologist who did not know the patient’sclinical data. Individual slides of the lung biopsy specimenswere stained with hematoxylin-eosin and Masson trichome.The degree of fibrosis was estimated in comparison with anormal lung specimen. The degree of fibrosis was estimatedto be mild (+1), moderate (+2), or severe (+3) when therewas a respective increase of o25%, 25–40%, or 440% in theamount of collagen seen in the biopsy specimens.
Flow-cytometric analysis of the phenotype ofbronchoalveolar cells
To determine the T-lymphocyte phenotype, we employedimmunofluorescent staining and flow cytometry. In order toidentify the proportions of T lymphocytes, CD4, CD8 T cells,B cells and natural killer (NK) cells subpopulations of BALfluid, cells were simultaneously stained with fluoresceinisothiocyanate or (FITC) and phycoerythrin-conjugated (PE)monoclonal antibodies (CD3, -CD4, -CD8, -CD19, -CD56)(Beckon Dickinson, Mountain View, CA) according to themanufacturer’s protocol.
To determine the borderline between stained andunstained cells, cells were also stained with mouse IgG1and IgG2a-conjugated FITC or PE. A cell gate containinglymphocytes was established on the basis of forward andside light scatter. Lymphocytes which were gated for CD3expression, then further subdivided by CD4 or CD8expression and analysed by two color flow cytometryon a FACScan. In other words, the relative ratio of CD4 orCD8 in CD3-positive cells was assayed by a dual-coloranalysis. Data were obtained and analyzed using BectonDickinson BD LYSYS II and Cytometric Bead Array (CBA)software (San Jose, CA).
Statistical analyses
Data are presented as mean7SD unless otherwise stated.Comparisons were made using the Mann–Whitney nonpara-metric test for continuous data and by w2 analysis fordiscontinuous data. Correlations between different para-meters were determined by Spearman’s rank correlationcoefficient. Po0:05 was considered significant.
Results
Demographics
The characteristics of all study subjects are listed in Table 1.No control subject had an obstructive or restrictive patternin his PFTs. The two groups were similar in age (P ¼ 0:24).
Chest radiography and high-resolution computedtomographic examinations
On chest radiography (CXR), prominent reticular interstitialshadows, which are usually diffuse and patchy and mostextensive in the lower zones, were seen in all cases.Bilateral abnormalities that may be asymmetrical areevident in all cases. However, overt honeycombing was notseen. CXR was normal in 2 cases. No nodules were seen.
The most common findings on HRCT were bilateral,reticular opacities with interlobular septal thickening c/w‘‘fibrosis’’ (21 cases), ground-glass attenuation (10 cases),subpleural, bibasilar rim of increased attenuation (20 cases)and traction bronchiectasis (4 cases). Overt honeycombchanges were not seen.
ARTICLE IN PRESS
Table 1 Demographic and physiologic data of patients with pulmonary fibrosis (PF) due to mustard gas exposure and normalcontrol subjects.�
Controls (n ¼ 20) PF (n ¼ 21) P value
Age (y) 35.6074.51 37.2874.61 0.24FVC, % of predicted 98.2272.07 61.4173.66 o0.0001FEV1, % of predicted 97.6274.61 82.6476.16 o0.0001DLCO (%) 96.4578.07 55.8179.73 o0.0001
�Values are mean7SD.
Role of T lymphocytes in pathogenesis of pulmonary fibrosis 789
Degree of fibrosis
The biopsy specimens of the mustard gas-exposed patientsindicated that 9 patients had mild (+1) PF and 12 patientshad moderate (+2) PF.
BAL fluid cellular constituents
The cellular contents of BAL fluids in both groups are shownin Table 2. Patients with PF had a higher total cell count thanthe normal group, but it was not significant (P ¼ 0:06).
Total and differential cell counts in patients with PFshowed, when compared to healthy controls, an increaseboth of neutrophil percentage (13.2573.94 vs. 2.4971.32;Po0:0001) and neutrophil absolute number (12.1973.68 vs.2.1571.08� 103 cells/ml; Po0:0001). Eosinophil percen-tage, as well as total count, showed a significant increasein PF patients when compared to healthy controls(2.3371.68 vs. 0.6470.71%, respectively; P ¼ 0:0002; and2.2371.70 vs. 0.5570.60� 103 cells/ml, respectively;P ¼ 0:0006). No significant changes in lymphocyte meanpercentage and the absolute number of alveolar lympho-cytes were seen when compared to the control group(10.9072.57 vs. 9.3874.12%, respectively; P ¼ 0:11; and10.0472.33 vs. 8.2573.71� 103 cells/ml, respectively;P ¼ 0:06). The proportion of alveolar macrophages, how-ever, was significantly lower (Po0:0001) in patients with PFthan in the control group.
Lymphocyte subsets in BALF
The summarized results of the lymphocyte phenotyping inthe BALF of both the control and patients with PF are shownin Table 3. The profile of T-cell subtypes showed that whendata were expressed as percentage or as absolute number ofpositive cells, CD8 lymphocytes were significantly higher inpatients with PF than in healthy controls (22.9677.48 vs.14.1677.73%, respectively; P ¼ 0:0006; and 2.2870.84 vs.1.1070.55� 103 cells/ml, respectively; Po0:0001). Theproportion of CD4 cells in BAL fluid was significantlydiminished in patients with PF compared to the controlgroup (15.8075.61 vs. 24.9279.59; P ¼ 0:0006), while theabsolute number of CD4 cells showed no significantdifference between the two groups (1.5770.59 vs.1.9070.85; P ¼ 0:15).
Consequently, the CD4/CD8 ratio was significantly lowerin patients with PF than in healthy controls (0.7370.25 vs.1.5870.67; Po0:0001).
When CD3, B and NK alveolar lymphocytes were evaluatedeither as a percentage or as absolute number, no significantdifferences were found between the patients with PF andthe control group (see Table 3).
Comparison of the DLCO percentage with BAL fluidcellular constituents
Except for the percentage and the absolute number of theBAL fluid neutrophils (r ¼ �0:70, P ¼ 0:001: r ¼ �0:62,P ¼ 0:005; respectively), no correlation was found betweenDLCO% and the other BAL cells.
Comparison of the DLCO percentage with BALlymphocyte subpopulations
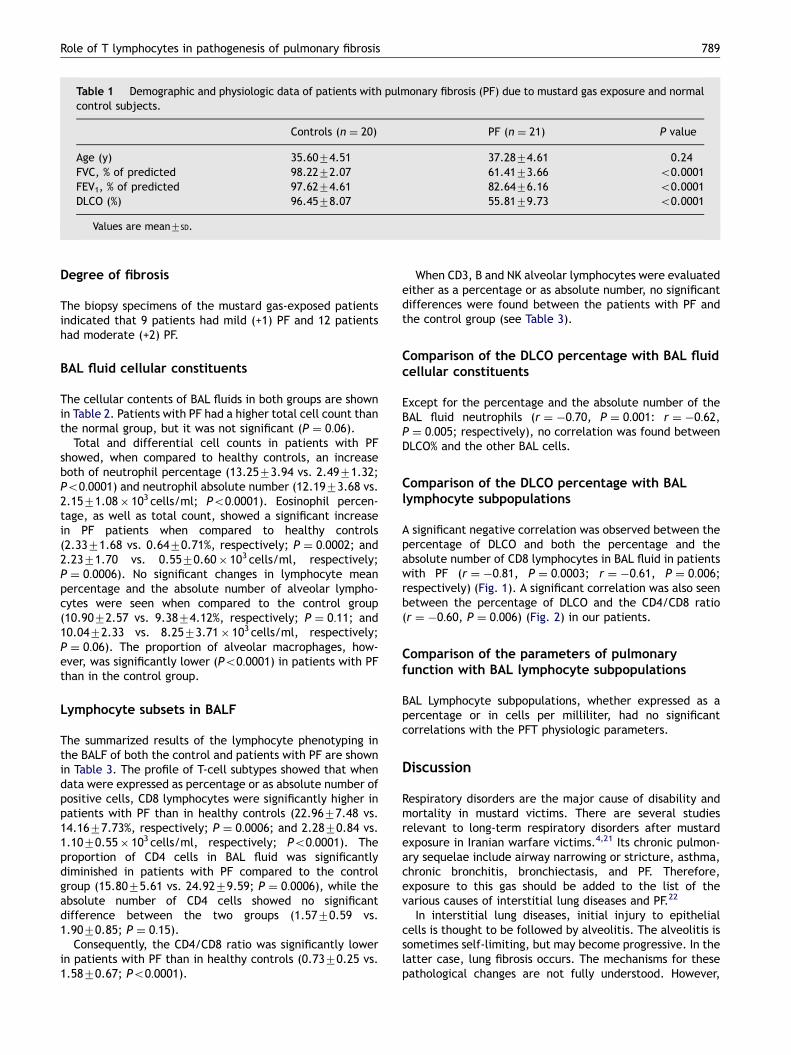
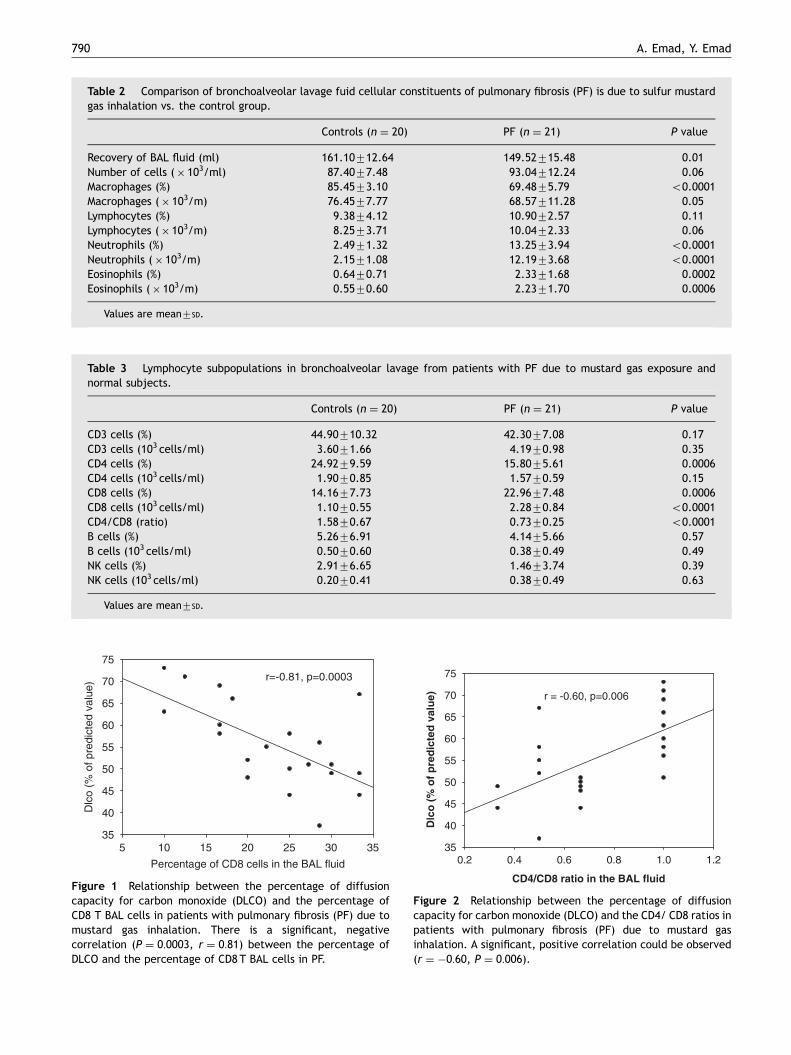
A significant negative correlation was observed between thepercentage of DLCO and both the percentage and theabsolute number of CD8 lymphocytes in BAL fluid in patientswith PF (r ¼ �0:81, P ¼ 0:0003; r ¼ �0:61, P ¼ 0:006;respectively) (Fig. 1). A significant correlation was also seenbetween the percentage of DLCO and the CD4/CD8 ratio(r ¼ �0:60, P ¼ 0:006) (Fig. 2) in our patients.
Comparison of the parameters of pulmonaryfunction with BAL lymphocyte subpopulations
BAL Lymphocyte subpopulations, whether expressed as apercentage or in cells per milliliter, had no significantcorrelations with the PFT physiologic parameters.
Discussion
Respiratory disorders are the major cause of disability andmortality in mustard victims. There are several studiesrelevant to long-term respiratory disorders after mustardexposure in Iranian warfare victims.4,21 Its chronic pulmon-ary sequelae include airway narrowing or stricture, asthma,chronic bronchitis, bronchiectasis, and PF. Therefore,exposure to this gas should be added to the list of thevarious causes of interstitial lung diseases and PF.22
In interstitial lung diseases, initial injury to epithelialcells is thought to be followed by alveolitis. The alveolitis issometimes self-limiting, but may become progressive. In thelatter case, lung fibrosis occurs. The mechanisms for thesepathological changes are not fully understood. However,
ARTICLE IN PRESS
Table 3 Lymphocyte subpopulations in bronchoalveolar lavage from patients with PF due to mustard gas exposure andnormal subjects.�
Controls (n ¼ 20) PF (n ¼ 21) P value
CD3 cells (%) 44.90710.32 42.3077.08 0.17CD3 cells (103 cells/ml) 3.6071.66 4.1970.98 0.35CD4 cells (%) 24.9279.59 15.8075.61 0.0006CD4 cells (103 cells/ml) 1.9070.85 1.5770.59 0.15CD8 cells (%) 14.1677.73 22.9677.48 0.0006CD8 cells (103 cells/ml) 1.1070.55 2.2870.84 o0.0001CD4/CD8 (ratio) 1.5870.67 0.7370.25 o0.0001B cells (%) 5.2676.91 4.1475.66 0.57B cells (103 cells/ml) 0.5070.60 0.3870.49 0.49NK cells (%) 2.9176.65 1.4673.74 0.39NK cells (103 cells/ml) 0.2070.41 0.3870.49 0.63
�Values are mean7SD.
Table 2 Comparison of bronchoalveolar lavage fuid cellular constituents of pulmonary fibrosis (PF) is due to sulfur mustardgas inhalation vs. the control group.�
Controls (n ¼ 20) PF (n ¼ 21) P value
Recovery of BAL fluid (ml) 161.10712.64 149.52715.48 0.01Number of cells (� 103/ml) 87.4077.48 93.04712.24 0.06Macrophages (%) 85.4573.10 69.4875.79 o0.0001Macrophages (� 103/m) 76.4577.77 68.57711.28 0.05Lymphocytes (%) 9.3874.12 10.9072.57 0.11Lymphocytes (� 103/m) 8.2573.71 10.0472.33 0.06Neutrophils (%) 2.4971.32 13.2573.94 o0.0001Neutrophils (� 103/m) 2.1571.08 12.1973.68 o0.0001Eosinophils (%) 0.6470.71 2.3371.68 0.0002Eosinophils (� 103/m) 0.5570.60 2.2371.70 0.0006
�Values are mean7SD.
Percentage of CD8 cells in the BAL fluid
5 10 15 20 25 30 35
Dlc
o (%
of p
redi
cted
val
ue)
35
40
45
50
55
60
65
70
75
r=-0.81, p=0.0003
Figure 1 Relationship between the percentage of diffusioncapacity for carbon monoxide (DLCO) and the percentage ofCD8 T BAL cells in patients with pulmonary fibrosis (PF) due tomustard gas inhalation. There is a significant, negativecorrelation (P ¼ 0:0003, r ¼ 0:81) between the percentage ofDLCO and the percentage of CD8 T BAL cells in PF.
0.2 0.4 0.6 0.8 1.0 1.235
40
45
50
55
60
65
70
75
Dlc
o (
% o
f p
red
icte
d v
alu
e)
CD4/CD8 ratio in the BAL fluid
r = -0.60, p=0.006
Figure 2 Relationship between the percentage of diffusioncapacity for carbon monoxide (DLCO) and the CD4/ CD8 ratios inpatients with pulmonary fibrosis (PF) due to mustard gasinhalation. A significant, positive correlation could be observed(r ¼ �0:60, P ¼ 0:006).
A. Emad, Y. Emad790

ARTICLE IN PRESS
Role of T lymphocytes in pathogenesis of pulmonary fibrosis 791
T-cells may have an important role in the pathophysiology ofthese diseases.15
The aim of this study was to characterize and compareBAL lymphocyte subpopulations in patients presenting withthe clinical features of PF due to sulfur mustard gasinhalation and healthy subjects. To the best of the authors’knowledge, this is the first study in which BAL Lymphocytesubpopulations have been evaluated in these victims.
We demonstrated that patients with PF, when comparedto healthy, were characterized by an increase eosinophilsand neutrophils in BAL fluid. A positive correlation betweeneither the percentage or the absolute number of BAL fluidneutrophils and percentage of DLCO from patients with PFhas already been demonstrated.22 This study group corro-borates our previous findings.22 These data also clearlydemonstrate that the degree of lung function impairmentclosely related to neutrophilic alveolitis in patients with PF.It might act as a triggering factor in the development of PFin mustard gas-exposed patients.
The role of CD4+ or CD8+ T-cells in the regulation of PFhas been investigated in several models of fibrosis.5,6,12,15
Analysis of T-lymphocyte subsets in BAL fluid indicates that,in patients with PF due to mustard gas exposure, CD4 T cellsdecrease and both the percentage and total numbers of CD8T cells increase. This study on BAL fluid has also shown thatthe CD4/CD8 ratio is significantly decreased in patients withPF. We measured the relationship between T-lymphocytesubsets and physiologic indexes of pulmonary function testsin the patients with PF due to mustard gas inhalation. Thepercentage and the absolute number of CD8 T cells highly,negatively correlated with the percentage of DLCO(r ¼ �0:81, P ¼ 0:0003; r ¼ �0:61, P ¼ 0:006; respectively).As reported in other studies, the single breath DLCO is a verysensitive parameter for following-up deterioration andresponse to therapy in patients with idiopathic PF.23,24
Therefore, we present a set of observations that reveal thatpatients with more advanced lung function impairment asreflected by the DLCO, tended to reveal lower CD4/CD8ratios.
Furthermore, it should be mentioned that the role of CD8T-cells would be important in sulfur mustard gas-induced PF,since the CD8 population is greater than CD4 T-cell subset inthe BAL fluid. The CD8 T-cell population could also befunctionally divided into two subsets, Tc1 and Tc2, based onthe cytokine secretion pattern.25 Recent reports disclosedthat they may contribute to tumor rejection, protectionagainst viral infection, and pathological changes in chronicobstructive pulmonary diseases.26,27
Therefore, It is possible that increased CD8 T cells in theBAL fluid may contribute to parenchymal destruction andtherefore to the development of chronic fibrosis in thesepatients by releasing cytokines capable of increasing thesusceptibility of target cells to cytotoxicity, or by secretingchemokines that attract other cells to the site of inflamma-tion.28,29 The significant correlation observed in our veter-ans between increased number of CD8 Tcells in the BAL fluidand reduced percentage of DLCO supports this hypothesis.
Although CD8 T cells are important effectors of cell-mediated immunity, their precise role in the pathogenesis ofmustard gas-induced PF is unclear. An initial insult may leadto an influx of acute and chronic inflammatory cells thatmaintain immunological and inflammatory responses and
thus produce progressive disease. It may be generallyaccepted that immune mechanisms are likely to make acontribution to pathogenesis; circumstantial support for animmunopathogenetic hypothesis includes the abundance ofCD8 T-cells within the lung interstitium. Other inflammatorycells may be involved. Macrophages may produce a numberof cytokines and neutrophils are likely to contribute totissue damage by the generation of oxygen radicals andproteolytic enzymes.30 Eosinophils may contribute to lunginjury through release of secretory products (eosinophiliccationic protein, vasoactive amines), cationic protein,vasoactive amines.31 Therefore, the end result of inflam-matory and immunological events in mustard gas-induced PFis the presence of excess collagen within the lungs.
This analysis of BAL fluid from our patients with PF as alate sequela of massive sulfur mustard gas inhalation issimilar to an experimental model of bleomycin-induced PF,it was found that the helper-to-suppressor ratio of T-celllymphocytes shifted with time, having a value 41 at thebeginning of the disease and a value o1 at the latest phasesof disease.32
Overall, the BAL profile in our patients with PF due tosulfur mustard gas inhalation is characterized by severalfeatures: cell differentials with an increase in neutrophils,eosinophils and a decreased CD4/CD8 ratio. These featuressuggest this BAL profile pattern may be similar to the BALfluid cellular constituents in usual interstitial pneumonia(UIP) but the finding of a decreased CD4/CD8 ratio (theabsolute value) in the BAL fluid may be somewhat similar tocryptogenic organizing pneumonia (COP) or BOOP.33,34
In conclusion, CD8 T cells in BAL fluid were significantlyelevated in patients with PF. Patients with higher grades ofpulmonary fibrosis expressed as percentage of DLCO,revealed higher percentages and the absolute number ofCD8 T cells and a lower CD4/CD8 ratio.
References
1. Smith KJ, Skelton H. Chemical warfare agents. Their past andcontinuing threat and evolving therapies. Part I. Skin Med2003;2:215–21.
2. Cowan FM, Broomfield CA, Smith WJ. Suppression of sulfurmustard-increased IL-8 in human keratinocyte cell cultures byserine protease inhibitors: implications for toxicity and medicalcountermeasures. Cell Biol Toxicol 2002;18(3):175–80.
3. Urbannetti JS. Battlefield chemical inhalation injury. Luke J,editor. Pathophysiology and treatment of inhalation injuries,vol. 34. New York: Dekker; 1988. p. 281–348 (Lung Biol. HealthDis. Ser.).
4. Emad A, Rezaian GR. The diversity of the effects of sulfurmustard gas inhalation on respiratory system 10 years after asingle, heavy exposure: analysis of 197 cases. Chest1997;112:734–8.
5. Mukae H, Kadota J, Kohno S, Matsukura S, Hara K. Increase ofactivated T-cells in BAL fluid of Japanese patients withbronchiolitis obliterans organizing pneumonia and chroniceosinophilic pneumonia. Chest 1995;108:123–8.
6. Costabel U. CD4/CD8 ratios in bronchoalveolar lavage fluid: ofvalue for diagnosing sarcoidosis? Eur Respir J1997;10:2699–700.
7. Sprince NL, Oliver LC, McLoud TC, Eisen EA, Christiani DC, GinnsLC. Asbestos exposure and asbestos-related pleural andparenchymal disease. Associations with immune imbalance.Am Rev Respir Dis 1991;143:822–8.

ARTICLE IN PRESS
A. Emad, Y. Emad792
8. Fellermann K, Stahl M, Dahlhoff K, Amthor M, Ludwig D, StangeEF. Crohn’s disease and sarcoidosis: systemic granulomatosis?Eur J Gastroenterol Hepatol 1997;9:1121–4.
9. Epstein PE, Dauber JH, Rossman MD, Daniele RP. Bronchoalveo-lar lavage in a patient with chronic berylliosis: evidence forhypersensitivity pneumonitis. Ann Intern Med 1982;97:213–6.
10. Kolarz G, Scherak O, Popp W, Ritschka L, Thumb N, Wottawa A,et al. Bronchoalveolar lavage in rheumatoid arthritis. Br JRheumatol 1993;32:556–61.
11. Akoun GM, Cadranel JL, Milleron BJ, D’Ortho MP, Mayaud CM.Bronchoalveolar lavage cell data in 19 patients with drug-associatedpneumonitis (except amiodarone). Chest 1991;99:98–104.
12. Wahlstrom J, Berlin M, Lundgren R, Olerup O, Wigzell H, EklundA, et al. Lung and blood T-cell receptor repertoire in extrinsicallergic alveolitis. Eur Respir J 1997;10:772–9.
13. Costabel U, Teschler H, Guzman J. Bronchiolitis obliteransorganizing pneumonia (BOOP): the cytological and immunocy-tological profile of bronchoalveolar lavage. Eur Respir J1992;5:791–7.
14. Plata F, Autran B, Martins LP, Wain-Hobson S, Raphael M, MayaudC, et al. AIDS virus-specific cytotoxic T lymphocytes in lungdisorders. Nature 1987;328:348–51.
15. The BAL Cooperative Group Steering Committee. Bronchoal-veolar lavage constituents in healthy individuals, idiopathicpulmonary fibrosis, and selected comparison groups. Am RevRespir Dis 1990;141:S169–202.
16. Christman JW, Emerson RJ, Graham WG, Davis GS. Mineral dustand cell recovery from the bronchoalveolar lavage of healthyVermont granite workers. Am Rev Respir Dis 1985;132:393–9.
17. American Thoracic Society. Idiopathic pulmonary fibrosis:diagnosis and treatment. International consensus statement.Am J Respir Crit Care Med 2000;161:646–64.
18. Gardner R, Kankinson J, Clausen J, et al. Standardization ofspirometry-1987 update. Am Rev Respir Dis 1987;136:1285–98.
19. Cotes JE, Chinn DJ, Quanjer PhH, Roca J, Yernault J-C.Standardization of the measurement of transfer factor (Diffus-ing Capacity). Report working party, Standardization of lungfunction tests, European Community for steel and coal.OfficialStatement of the European respiratory Society. EurRespir J 1993:41–52.
20. American Thoracic Society. Lung function testing: selection ofreference values and interpretative strategies. Am Rev RespirDis 1991;144:1202–18.
21. Emad A, Rezaian GR. Characteristics of bronchoalveolar lavagefluid in patients with sulfur mustard gas-induced asthma orchronic bronchitis. Am J Med 1999;106:689–90.
22. Emad A, Rezaian GR. Immunoglobulins and cellular constituentsof the BAL fluid of patients with sulfur mustard gas-InducedPulmonary Fibrosis. Chest 1999;115:1346–51.
23. Schwartz DA, Van Fossen DS, Davis CS, et al. Determinants ofprogression in idiopathic pulmonary fibrosis. Am Respir CritCare Med 1994;149:444–9.
24. Agusti C, Xaubet A, Agusti AGN, Roca J, Ramirez J, Rodriguez-Roisin R. Clinical and functional assessment of patients withidiopathic pulmonary fibrosis: results of 3 year follow-up. EurRespir J 1994;7:643–50.
25. Mosmann TR, Li L, Sad S. Functions of CD8 T-cell subsetssecreting different cytokine patterns. Semin Immunol1997;9:87–92.
26. Kemeny DM. CD8z T cells in atopic disease. Curr Opin Immunol1998;10:628–33.
27. Kemeny DM, Vyas B, Vukmanovic-Stejic M, et al. CD8(+) T cellsubsets and chronic obstructive pulmonary disease. Am J RespirCrit Care Med 1999;160:S33–7.
28. Walter U, Santamaria P. CD8+ Tcells in autoimmunity. Curr OpinImmunol 2005;17(6):624–31.
29. Mosmann TR, Li L, Sad S. Functions of CD8 T-cell subsetssecreting different cytokine patterns. 1: Semin Immunol1997;9(2):87–92.
30. Rahman I, Skwarska E, Henry M, et al. Systemic and pulmonaryoxidative stress in idiopathic pulmonary fibrosis. Free Radic BiolMed 1999;27:60–8.
31. Davis WB, Sun XH, Gadek JE, Jaurand MC, Bignon J, Crystal RG.Cytotoxicity of eosinophils for lung parenchymal cells. Am RevRespir Dis 1982;125:178A.
32. Thrall RS, Barton RW. A comparison of lymphocyte populationsin lung tissue and in bronchoalveolar lavage fluid of rats atvarious times during the development of bleomycin-inducedpulmonary fibrosis. Am Rev Respir Dis 1984;129:279–83.
33. Costabel U, Teschler H, Guzman I. Bronchiolitis obliteransorganizing pneumonia (BOOP): the cytological and immunocy-tological profile of bronchoalveolar lavage. Eur Respir J1992;5:791–7.
34. Cordier JF, Loire R, Brune J. Idiopathic bronchiolitis obliteransorganizing pneumonia: definition of characteristic clinicalprofiles in a series of 16 patients. Chest 1989;96:999–1004.