increasing operating profit margin at an academic health
TRANSCRIPT

Increasing Operating Profit Margin at an Academic Health
Center through Community Expansion
Business Plan
Konye Ori, MA, FACMPE
July 22, 2021
This paper is being submitted in partial fulfillment of the requirements of Fellowship in
the American College of Medical Practice Executives.
1
Table of Contents
List of Tables .................................................................................................................2
List of Figures ................................................................................................................2
Project Summary ...........................................................................................................3
Executive Summary .......................................................................................................4
The Organization: Apex Health Systems (AHS) ...................................................................... 4
Mission Statement ................................................................................................................... 4
Market Opportunity................................................................................................................. 4
Management and Key Personnel ............................................................................................. 5
Competitors ............................................................................................................................ 7
Competitive Advantages ......................................................................................................... 7
Financial Projections ............................................................................................................... 8
The Organizational Plan ............................................................................................. 10
Summary Description of the Existing Business ...................................................................... 10 SWOT Analysis: Existing Business ....................................................................................... 10
Strategy: New Business ......................................................................................................... 12
Key Stakeholders and Decisionmakers .................................................................................. 12
Summary Description of the New Business ........................................................................... 13
SWOT Analysis: New Business ............................................................................................ 14
Strategy: New Business ......................................................................................................... 16
Strategic Relationships: New Business .................................................................................. 18
Services ................................................................................................................................ 18 Administrative Plan............................................................................................................... 19
Operational Plan ................................................................................................................... 23
Regulation and Accreditation ................................................................................................ 31
The Marketing Plan ..................................................................................................... 32
Overview of Goals of the Marketing Strategy ........................................................................ 32
Market Analysis .................................................................................................................... 32
Marketing Strategy ................................................................................................................ 34
Marketing Budget ................................................................................................................. 37
Relationship with Current Business ....................................................................................... 39
Implementation of Marketing Strategy .................................................................................. 39
Financial Documents ................................................................................................... 42
Pro Forma Cash Flow Statement (Budget) ............................................................................. 44
Three-Year Income Projection: WHD ................................................................................... 46
Projected Balance Sheet ........................................................................................................ 47
Break-Even Analysis ............................................................................................................. 47
Profit & Loss Statement (Income Statement) ......................................................................... 49
Financial Statement Analysis ................................................................................................ 50
Business Financial History .................................................................................................... 52
Innovative Elements and Expected Business Outcomes............................................. 54
Why and how does this innovative idea positively impact the health of your population and the
organization? ........................................................................................................................ 54 What challenges did you encounter during this process, and what have you learned? ............. 55
Next steps ............................................................................................................................. 55
2
List of Tables
Table 1: Three-Year Income Projection (WHD) .......................................................................... 8
Table 2: WHD Income Statement ................................................................................................ 9
Table 3: Operational Plan, Years 1–3 ........................................................................................ 23
Table 4: Marketing Budget........................................................................................................ 38
Table 5: OB/GYN Community Expansion Startup Costs ........................................................... 43
Table 6: ROI Projection Snapshot ............................................................................................. 44
Table 7: Statement of Cash Flows ............................................................................................. 44 Table 8: 3-Year Income Projection for WHD ............................................................................ 46
Table 9: Projected Balance Sheet .............................................................................................. 47
Table 10: Break-Even Analysis ................................................................................................. 48
Table 11: Income Statement ...................................................................................................... 49
Table 12: Income Projection for Years 4–6................................................................................ 52
List of Figures
Figure 1: Comprehensive Women's Health Program .................................................................. 13
Figure 2: Organizational Chart .................................................................................................. 19
Figure 3: Access Point Decision Flowchart ............................................................................... 34
Figure 4: Monroe's Motivated Sequence for AHS Marketing ..................................................... 40
Figure 5: Payor Mix .................................................................................................................. 51

3
Project Summary
In 2018, Apex Health System (AHS) established a Women’s Health Department
(WHD) to oversee its Obstetrics and Gynecology (OBGYN) community division and its
newly established Academic Health Center (AHC). The AHC, designed in part to cater to
high-risk mothers and babies, includes a labor and delivery unit staffed by maternal-fetal
medicine specialists, a comprehensive Level IV Neonatal Intensive Care Unit (NICU), a
Level I Pediatric Trauma Center, and a state-of-the-art surgical center. However, the
AHC, despite the high quality of care available, has not seen the volume of high-risk
deliveries projected to boost returns on investment in the AHC.
AHS has tasked the WHD leadership team to produce a business plan to increase
the number of women who choose AHS for their maternal-fetal care. An increased
number of women choosing AHS for their maternal-fetal care will, in turn, increase the
volume of high-risk deliveries at the AHC and ultimately increase the WHD’s operating
profit margin.
The WHD leadership team has outlined several core strategies, including plans to
meet patients in their communities by expanding access and services. The WHD plans to
improve care coordination using nurse navigation and OB outreach and expand digital
consumer-focused platforms to improve pregnancy outcomes, education, continuity of
care, and patient experience.
The time frame for this business plan is three years. Successful execution of this
plan should increase high-risk deliveries at the AHC by 35% or more, grow the AHS
statewide market share for OB care by 40% or more, and increase WHD’s operating
profit margin by 46% or more.
4
Executive Summary
The Organization: Apex Health System (AHS)
AHS is an independent, nonprofit health system with for-profit entities. Formed in
1998, AHS has grown to include more than 200 locations statewide, dozens of facilities
including 15 hospitals under the AHS brand, and a total capacity of 2,596 beds. AHS has
more than 30,000 employees statewide, including more than 1,500 board-certified or
board-eligible physicians and more than 250 advanced practice providers. In 2018, AHS
established a Women’s Health Department (WHD) to oversee its OB/GYN community
division and its newly established Academic Health Center (AHC).
The WHD currently has thirteen (13) administrative staff FTEs, seventy-one (71)
support staff FTEs, twenty-nine (29) physician FTEs, and eleven (11) nurse practitioner
FTEs. These combined FTEs managed 68,189 encounters or visits in the past twelve
months, generating 170,000 wRVUs.
Mission Statement
AHS’s mission is to improve patients’ and communities’ health through
innovation and excellence in care, education, research, and service.
Market Opportunity
The state ranks 41st in the nation in overall health, according to the 2018
America’s Health Rankings report, and 42nd in mental health, according to Mental
Health in America 2019. The state’s infant mortality rate was the 7th highest in the
country, and the maternal mortality rate was the 3rd highest (Mental Health in America,
2019). In its 2020 report, March of Dimes classified 33 counties across the state as
5
“maternity deserts.” This data highlights the need for a health system like AHS to
understand, assess, and nurture the health of high-risk maternity populations
comprehensively and continuously.
Management and Key Personnel
The WHD leadership team comprise a Vice President, a Medical Director, two
service line administrators, four practice administrators, four practice managers, and one
project manager. The WHD leadership team will work with the appropriate AHS
resource teams to implement this business proposal. With support from AHS leadership,
the WHD leadership team will oversee efforts to meet patients where they live, increase
care coordination, leverage technology, expand maternal-fetal medicine and midwifery,
and market the AHC to patients and communities across the state. The leadership team
will oversee strategic decisions that include leasing or purchasing real estate, purchasing
capital equipment, recruiting, and staffing, and upholding the standards of care expected
at AHS. Below is a breakdown of key personnel and what they bring to the table
• Vice President, WHD: The WHD VP oversees WHD community outreach
centers and clinics. The WHD VP has extensive knowledge of practice
development and clinic operations. The WHD VP holds a master’s in healthcare
administration from Southern New Hampshire University. As the executive leader
in charge of leading this implementation, the WHD VP will ensure that the
mission to offer maternal-fetal care in the thirty-three target counties across the
state is successful.
• Medical Director, WHD: The WHD Medical Director is responsible for
recruiting, hiring, and supervising all clinical team members. The WHD Medical

6
Director has extensive experience in private practice, teaching and research, and
community medicine operations. The WHD Medical Director graduated from
Augusta University and completed his medical residency and fellowship from
Emory University. The WHD Medical Director will ensure that the clinical
implications of this undertaking have a basis in medical best practices.
• Service Line Administrator, WHD- Community Division: The WHD SLA will
ensure compliance with state and federal regulations during the implementation of
this business plan. The WHD SLA has a master’s degree in hospital and
healthcare administration from Cornell University. The WHD SLA is also a
board-certified medical practice executive from the American College of Medical
Practice Executives (ACMPE). As an expert communicator, The WHD SLA will
be responsible for building partnerships and fostering healthy relationships with
all internal and external stakeholders throughout the implementation of this plan.
• Project Manager, WHD: The WHD Project Manager is responsible for the
various process flows, workflows, and deliverables throughout the
implementation of this plan. The WHD Project Manager has a master’s degree in
healthcare administration from the University of Oklahoma. The WHD Project
Manager is also a certified Project Management Professional (PMP) by the
Project Management Institute (PMI). As a transformation expert, the WHD
Project Manager will oversee this business plan from ideation to
implementation.

7
Competitors
Three other major health systems in the state compete directly with AHS. The
competing organizations have some key strengths: all three have dozens of maternity
practices across the state, labor and delivery facilities with maternal-fetal medicine
programs, and strong brand awareness. Nonetheless, the competing organizations have
some fundamental weaknesses: none have a school or college of medicine, nor a
nationally ranked or recognized medical facility or program.
Competitive Advantages
2018, 2019, and 2020 U.S. News & World Report “Best Hospitals” rankings name
AHS-AHC among the nation’s top hospitals. According to these rankings, University
Hospital at the AHC is the #1 ranked hospital and the state’s only nationally ranked adult
hospital. The Children Hospital at the AHC achieved national ranking in ten (10)
pediatric specialties, with two programs earning top-five status according to the U.S.
News & World Report.
Capital Requirements
The capital requirement to execute this proposal is $30,475,064. These funds will
go entirely into the operating expenses of the WHD cost center.

8
Funding Source
AHS will fully support this investment by providing one hundred percent (100%)
of the funding to the WHD over three years. The WHD will receive $20,790,651 in year
one, $8,842,972 in year two, and $841,436 in year three.
Financial Projections
The WHD currently has a total operating revenue of $16,393,268 a total operating
expense of $29,174,480, an operating income per investment of -$12,781,212, and an
operating profit margin of -78%. This proposal will require a $30,475,064 investment
from AHS into the WHD operations. This investment will increase the total operating
expense for the WHD to $49,965,136 in year one, $58,808,108 in year two, and
$59,649,544 in year three. However, the WHD projects volumes and subsequent
productions of Work Relative Value Units (wRVU) to increase by 77% at the end of year
three. Accordingly, the WHD projects that the total operating revenue will also increase
by 77% or more at the end of year three, and the operating profit margin will, therefore,
increase by 46% or more at the end of year four.
Table 1: Three-Year Income Projection (WHD)
Current 3-Year Income Projection Year 1 Year 2 Year 3
170,000 Projected wRVUs 220,509 250,509 300,509
$15,147,000 Patient revenue $19,602,000 $22,275,000 $26,730,000
$1,246,268 (net patient revenue per
wRVU @ $89.10) $1,420,546 $2,165,471 $2,447,865
$1,246,268 Accounts receivables $1,420,546 $2,165,471 $2,447,865
9
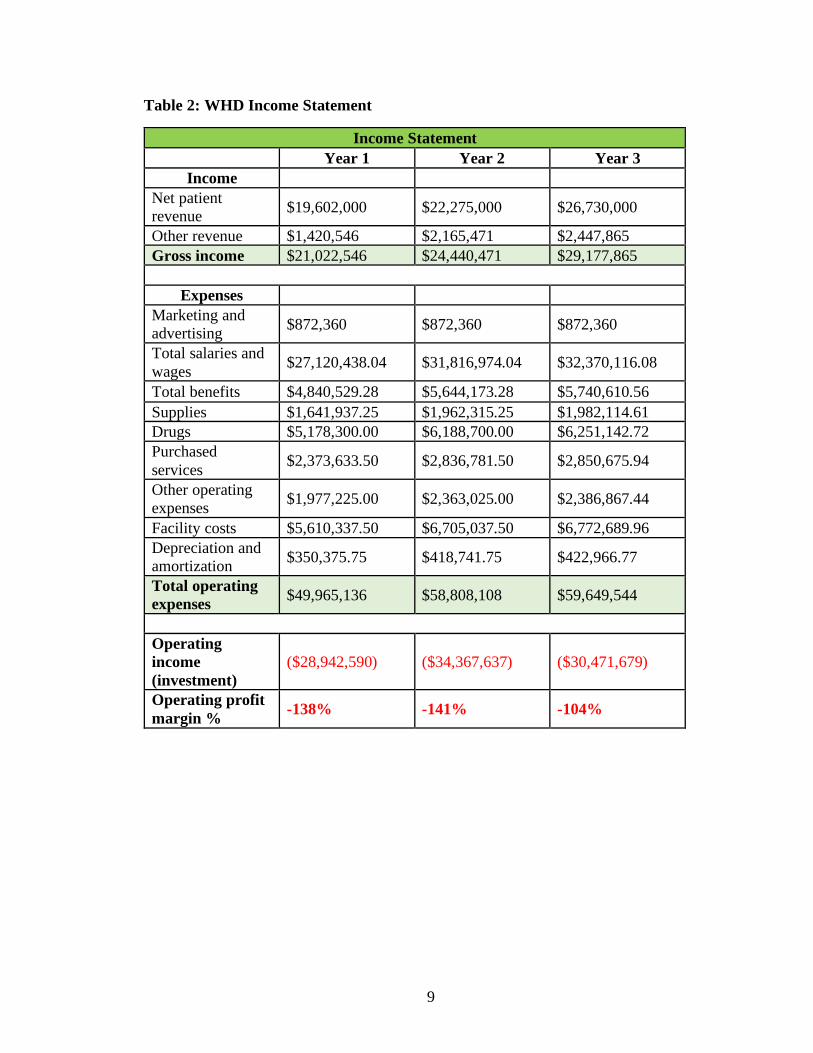
Table 2: WHD Income Statement
Income Statement
Year 1 Year 2 Year 3
Income
Net patient
revenue $19,602,000 $22,275,000 $26,730,000
Other revenue $1,420,546 $2,165,471 $2,447,865
Gross income $21,022,546 $24,440,471 $29,177,865
Expenses
Marketing and
advertising $872,360 $872,360 $872,360
Total salaries and
wages $27,120,438.04 $31,816,974.04 $32,370,116.08
Total benefits $4,840,529.28 $5,644,173.28 $5,740,610.56
Supplies $1,641,937.25 $1,962,315.25 $1,982,114.61
Drugs $5,178,300.00 $6,188,700.00 $6,251,142.72
Purchased
services $2,373,633.50 $2,836,781.50 $2,850,675.94
Other operating
expenses $1,977,225.00 $2,363,025.00 $2,386,867.44
Facility costs $5,610,337.50 $6,705,037.50 $6,772,689.96
Depreciation and
amortization $350,375.75 $418,741.75 $422,966.77
Total operating
expenses $49,965,136 $58,808,108 $59,649,544
Operating
income
(investment)
($28,942,590) ($34,367,637) ($30,471,679)
Operating profit
margin % -138% -141% -104%

10
The Organizational Plan
Summary Description of the Existing Business
The WHD teams of doctors, nurses, nurse practitioners, nurse educators,
mammography technologists, and others offer OBGYN services across urban, suburban,
and rural communities under the Community Medicine Division of the AHC. AHS built
the AHC in partnership with the State’s University School of Medicine to give patients
access to leading-edge medicine and treatment. Through the AHC, the WHD offers a full
range of specialty services for children and adults, including cancer, cardiovascular,
neuroscience, orthopedics, pediatrics, and transplant services. The AHC treats and
monitors expectant mothers with medical conditions such as high blood pressure and
diabetes or pregnancy complications such as genetic traits, prior preterm birth, early
labor, bleeding, accidents, gestational diabetes, or infections.
SWOT Analysis: Existing Business
Strengths
• Largest healthcare organization in the state (Over 35,000 employees)
• Affiliation to the States School of Medicine
• Nationally ranked and recognized medical programs and facilities (consistently
recognized by the U.S. News & World Report ‘Best Hospitals’ rankings)
• Strong state and national brand awareness.
• Comprehensive payer mix: 50% commercial, 25% Medicare (all types), 20%
Medicaid (all types), and 5% other, including self-pay.
• Convenient locations across the state (more than 200 locations statewide, dozens

11
of facilities including fifteen (15) hospitals under its AHS brand).
• Robust virtual care operations.
• Robust community benefit programs (more than $738 million serving more than 1
million individuals across the state).
• AHS can recruit well-trained physicians, including, but not limited to, trainees in
its residency and fellowship programs.
Weaknesses
• The community medicine department is new, having been founded less than three
years ago.
• AHS is a large and complex organization, meaning it is difficult to make changes.
• There is traffic and limitations for parking for patients and employees downtown.
Opportunities
• Increasing access to maternal-fetal care for patients in underserved and rural
communities will generate more high-risk OB patient volumes at the AHC.
• Coordination of care between outreach practices and the AHC can be expanded.
• Digital consumer-focused platforms could be expanded to prevent AHS patients
from leaving the system.
Threats
• Patient volume may not grow over time at the AHC, forcing a reduction in the
workforce.

12
• One of the competing organizations may decide to establish a competitive high-
risk facility in the target market areas.
Strategy: New Business
AHS’s business strategy is to align AHS resources and programs with goals,
objectives, and success indicators for addressing identified health needs in the
community. AHS, once a year, conducts a Community Health Needs Assessment
(CHNA) to understand community health needs and to inform strategies to advance
community health, including social determinants of health. AHS conducts CHNAs using
widely accepted methodologies to identify the significant needs of a specific community.
Key Stakeholders and Decisionmakers
AHS’s executive leadership includes a President and Chief Executive Officer,
Executive Vice President and Chief of Staff, Executive Vice President and Chief Nurse
Executive, Executive Vice President and Chief Medical Officer, Executive Vice
President and Chief Operating Officer, and fourteen people on the Board of Directors.
These leaders guide AHS’s pursuit of excellence through leading-edge medicine and
scientific innovation. Steering committees, advisory councils, and approval boards that
include clinical and non-clinical leaders representing multiple areas of expertise in
primary and specialty care across AHS and the state make critical decisions for AHS.
13
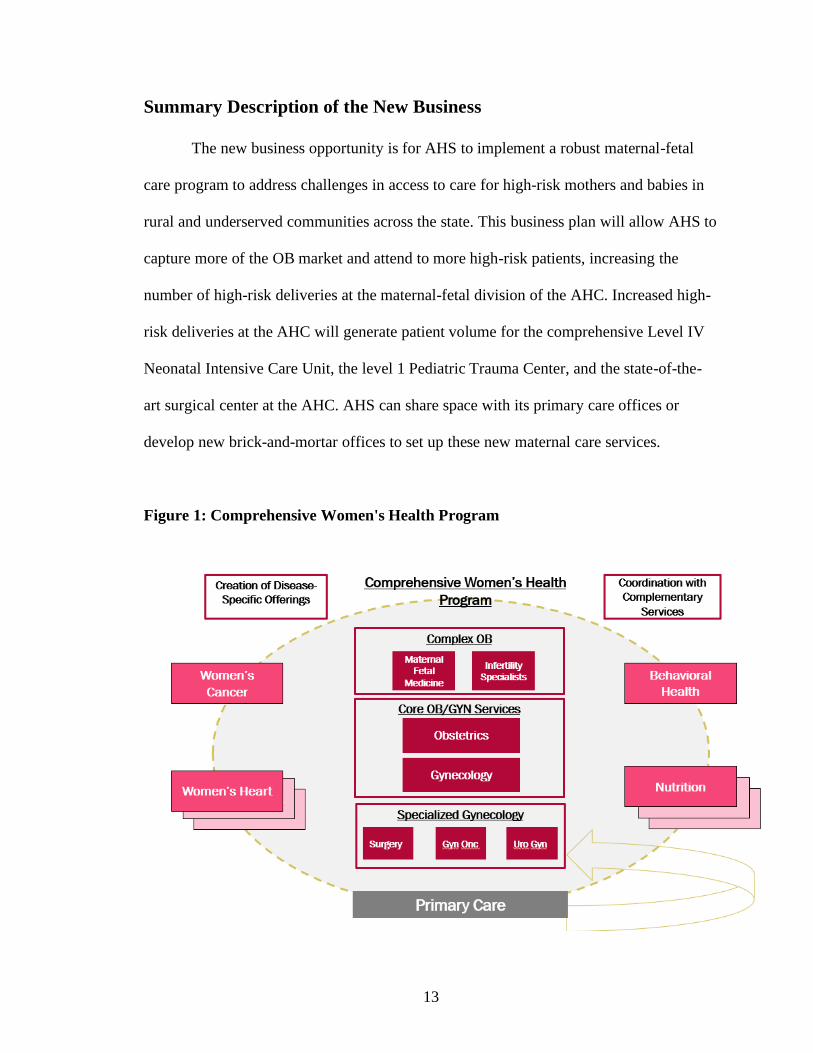
Summary Description of the New Business
The new business opportunity is for AHS to implement a robust maternal-fetal
care program to address challenges in access to care for high-risk mothers and babies in
rural and underserved communities across the state. This business plan will allow AHS to
capture more of the OB market and attend to more high-risk patients, increasing the
number of high-risk deliveries at the maternal-fetal division of the AHC. Increased high-
risk deliveries at the AHC will generate patient volume for the comprehensive Level IV
Neonatal Intensive Care Unit, the level 1 Pediatric Trauma Center, and the state-of-the-
art surgical center at the AHC. AHS can share space with its primary care offices or
develop new brick-and-mortar offices to set up these new maternal care services.
Figure 1: Comprehensive Women's Health Program
14
The above diagram is a visual representation of how AHS will funnel high-risk
OB patients from AHS community practices into the AHC for their maternal-fetal care
and other needed services.
SWOT Analysis: New Business
Strengths
• AHS provides care for women at all stages of life—from puberty through the
senior years.
• AHS women’s health program is the only nationally ranked gynecology program
in the state, according to U.S. News & World Report’s 2020-21 edition of
America’s Best Hospitals.
• AHS has over fifty (50) primary care offices across the state to partner to provide
maternal-fetal care.
• AHS primary care doctors currently focus on: family medicine, internal medicine,
sports medicine, pediatrics, and women’s health.
• AHS provides coordinated care and treatment backed by the extensive resources
and technology of the AHS community.
• Robust virtual care is offered across all AHS practices.
• For high-risk cases, AHS maternal-fetal medicine specialists can manage
pregnancies with expertise to keep the mother and baby healthier and decrease the
likelihood of premature birth.
• AHS Hospital for Children is one of the nation’s top-ranked pediatric hospitals
with the only Level IV Neonatal Intensive Care Unit (NICU) in the state.
15
Weaknesses
• AHS has only 16 OBGYN community offices across the state.
• The community medicine department is new, having been founded less than three
years ago.
• AHS is a large and complex organization, meaning it is difficult to make changes.
• There is traffic and limitations for parking for patients and employees downtown.
Opportunities
• Over thirty-three (33) counties are considered “maternity deserts” across the state.
• The state is 41st in the nation in overall health, according to the 2018 America’s
Health Rankings report, and ranks 42nd when it comes to mental health,
according to Mental Health in America 2019. Approximately one baby dies in the
state every 14 hours—amounting to 600 infant deaths a year—making the state’s
infant mortality rate one of the worst in the country.
Threats
• The American College of Obstetricians and Gynecologists estimate 500,000 fewer
births in the U.S. in 2021, a 13% drop from the 3.8 million babies born in 2019.
• Patient volume does not grow over time at the AHC, forcing a reduction in the
workforce.
• One of the competing organizations decides to establish a competitive high-risk
facility in other strategic market areas.

16
• OB patients comfort levels with receiving care virtually
• Potential to exceed the capacity to handle the additional deliveries at the AHC
Strategy: New Business
As of 2019, the targeted counties referred to as “maternity deserts” have a
combined population of 3.2 million residents. The WHD will take four strategic actions:
1) meet patients in their communities by expanding access and services; 2) increase the
ability for coordination of care using nurse navigation and OB outreach; 3) expand digital
consumer-focused platforms to improve pregnancy outcomes, education, continuity of
care, and patient experience; and 4) expand the midwifery program to establish a new
patient base and expand market share.
WHD will invest in maternal-fetal care services in new brick and mortar offices
and its existing AHS primary care offices across 33 counties in the state. The WHD
prioritization of ZIP codes and regions will focus on three factors: population of child-
bearing age women, the volume of cases that out-migrate and travel to a location farther
away than the nearest AHS facility, and the market share gap (difference in market share
between market leader and AHS or gap between AHS and next largest provider).
Establishing a footprint in ZIP codes with a greater number of child-bearing-age women
will provide AHS a stronger opportunity to expand OBGYN care in underserved
communities. Patients who leave their home location and travel farther to a competitor
facility provide AHS a chance to reduce leakage and keep more cases in-house. A low
market share gap within a ZIP code indicates there might be enough of a preference for
the AHS brand and its services for AHS to capitalize.

17
The WHD leadership team will work with the following AHS departments to
implement this phase of the proposal:
1. AHS Talent Acquisitions will search, recruit, and hire providers, nurses, social
workers, support staff, and administrators.
2. AHS Provider Enrollment will oversee enrollment, credentialing, and privileging
of new providers.
3. AHS Provider Onboarding will manage provider training and onboarding.
4. AHS Systems Support will provide IT, hardware, software, and digital consumer-
focused platforms.
5. AHS Quality Department will provide medical equipment needs and oversee
standards of care.
6. AHS Marketing will market locations, services, and providers to the targeted
communities.
7. AHS Revenue Cycle Systems will bill for services and collect the patient revenue
associated with visits and care provided.
• Short-term goals: In the first three years, AHS aims to improve access to
obstetric services for women in thirty-three (33) counties in the state. AHS
will invest in maternal-fetal care services in new brick and mortar offices and
its existing AHS primary care offices across the thirty-three (33) counties
described as “maternity deserts.” AHS will also spend resources on digital
consumer-focused platforms to improve pregnancy outcomes, education,
continuity of care, and patient experience.
18
• Long-term goals: AHS plans to increase high-risk deliveries at the AHC by
35% or more, grow AHS statewide market share for OB care by 40% or more,
and increase WHD’s operating profit margin by 46% or more. AHS will
continue to meet patients in their communities live by expanding access
throughout underserved communities, supporting the coordination of care
using nurse navigation, and expanding midwifery programs to establish a new
patient base and expand market share.
Strategic Relationships: New Business
AHS will form strategic partnerships with county health departments in the
targeted counties, rehab centers, and counseling and support centers to address healthcare
access challenges for high-risk mothers and babies in rural and underserved communities.
AHS will use its population health team to implement a digital consumer-focused
platform to improve pregnancy outcomes, education, continuity of care, and patient
experience in targeted communities. The AHS care coordination team of nurse navigators
and OB outreach nurses will partner with small and large organizations and religious
organizations to connect with OB patients and build needed communication pathways.
Services
AHS will implement a robust maternal-fetal care presence to address access to
care challenges for high-risk mothers and babies in rural and underserved communities
across the state. AHS will invest in implementing maternal-fetal care services in new
brick and mortar offices and its existing AHS primary care offices across thirty-three (33)

19
counties in the state. AHS will meet patients where they live by expanding access
throughout underserved communities, supporting care coordination using nurse
navigation, develop digital consumer-focused platforms to improve pregnancy outcomes,
education, continuity of care, and patient experience.
Administrative Plan
With support from AHS leadership, the WHD leadership team will oversee efforts to
expand maternal-fetal care for high-risk OB patients, increase care coordination, leverage
technology, expand maternal-fetal medicine, and market the AHC to patients and
communities across the state.
Organizational Chart
Figure 2: Organizational Chart
Vice President, WHD
Service Line Administator,
Community Division
Practice Administrators
Practice Managers
Medical Director, WHD
Project Manager,
WHD
Service Line Administator, AHC
Division
Practice Administrators
Practice Managers

20
Approval Plan
AHS leadership has tasked the WHD leadership team to produce a business plan
to increase the volume of high-risk deliveries at the AHC and improve AHC’s operating
profit margin. The WHD is responsible for expanding the funnel of women choosing
AHS for their maternal-fetal care and increasing the volume of high-risk deliveries at the
AHC. Therefore, the decision to proceed with implementing a robust maternal-fetal care
presence to address access to care challenges for high-risk mothers and babies in rural
and underserved communities across the state will come from the Vice President of the
Women’s Health Department.
Responsibilities
• Vice President: The Vice President will be responsible for approving/signing
all the contracts, netting new spaces, and negotiating space-sharing
agreements with existing AHS primary care offices in the target markets. The
Vice President will provide strategic leadership and direction for the approval,
planning, and implementation of the overall business plan, including
resources, processes, and tools.
• Medical Director: The Medical Director will be responsible for hiring,
onboarding, and training all new providers and clinical personnel. The
Medical Director will also be responsible for developing the clinical workflow
and documentation processes to ensure consistency in practice standards and
expectations.
• Service Line Administrator: The current service line administrators will

21
plan and oversee the operational activities of existing and new practices,
including hiring new practice administrators. Working closely with the Vice
President and the Medical Director, the service line administrators will
coordinate adherence to AHS policies, projects, initiatives, and interests. The
service line administrators will be accountable for the operational and
financial performance results of the service line.
• Practice Administrators: The current and new practice administrators will
oversee existing and new practices’ operational activities, including hiring
new practice managers. Working closely with the service line administrator,
the practice administrators will coordinate adherence to AHS policies and
accurate communication to subordinate personnel regarding current and new
practice operations. The practice administrators will be accountable for
current and new medical practices’ operational and financial performance
results under the WHD.
Key Personnel
• Project Manager: The project manager will manage the expansion project
timeline and ensure the project stays on or ahead of schedule. The project
manager will work closely with the Vice President and Medical Director to
move the project from start to completion. The project manager will determine
when each project phase is complete.
• Operations Analyst: The operations analyst will support the project manager
in overseeing the expansion project timeline and ensure the project stays on or

22
ahead of schedule. The operations analyst will also work with the marketing
team, care coordination team, and population health team to coordinate
marketing efforts, communication flow, and operational consistencies.
• Practice Managers: The practice managers will oversee the daily operations
of the current and new medical practices. The practice managers will plan,
prioritize, and advise day-to-day operations to include staffing, practice
growth, patient satisfaction, clinic space options, number of clinic days per
month, and purchases for daily operations.
• Lead Nurse Practitioner: The lead nurse practitioner will create the nursing
workflow that the outpatient nurse practitioners will follow to ensure
consistency in nursing practice. The lead nurse practitioner will be responsible
for hiring clinic staff, patient referral analysis, and providing OR efficiency
and functionality assessment. The lead nurse practitioner will perform
miscellaneous job-related duties as assigned by the Medical Director.
• Lead Registered Nurse: The lead registered nurse will create the nursing
workflow for triage, nurse navigation, and OB outreach. The lead RN will be
responsible for hiring clinic staff, patient referral analysis, and providing OR
efficiency and functionality assessment. The lead RN will enforce the support
of patients throughout the healthcare process, from detection to treatment and
beyond.
23
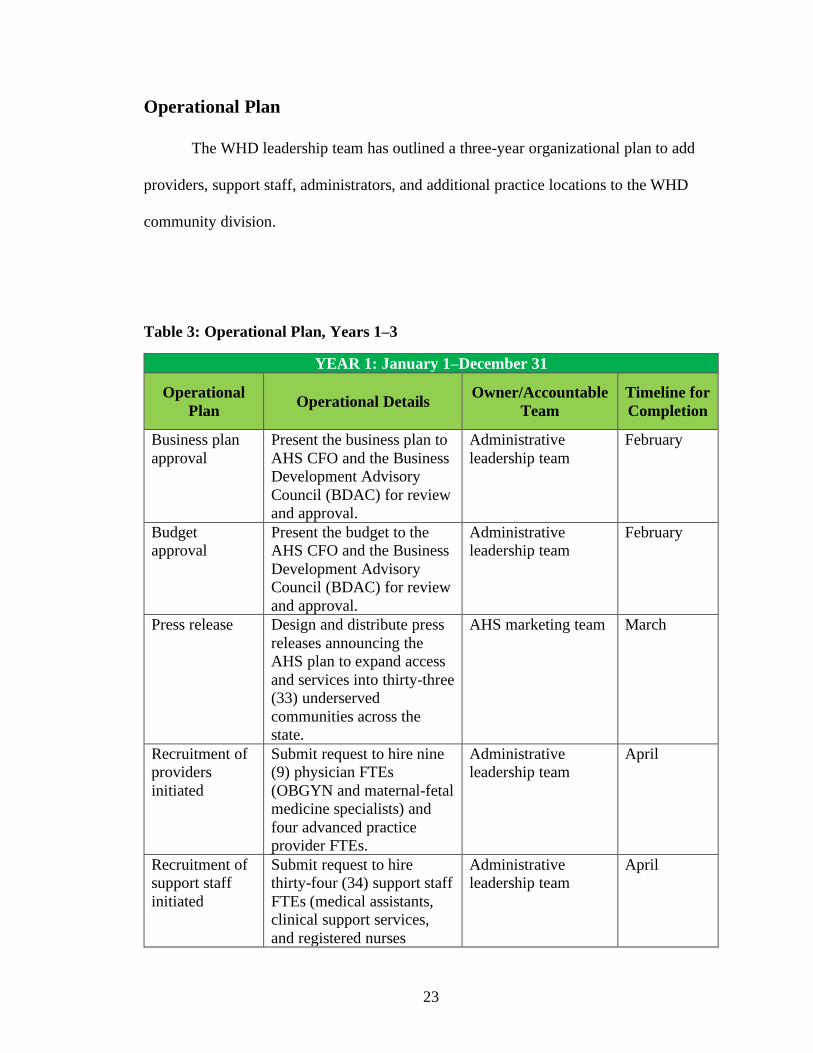
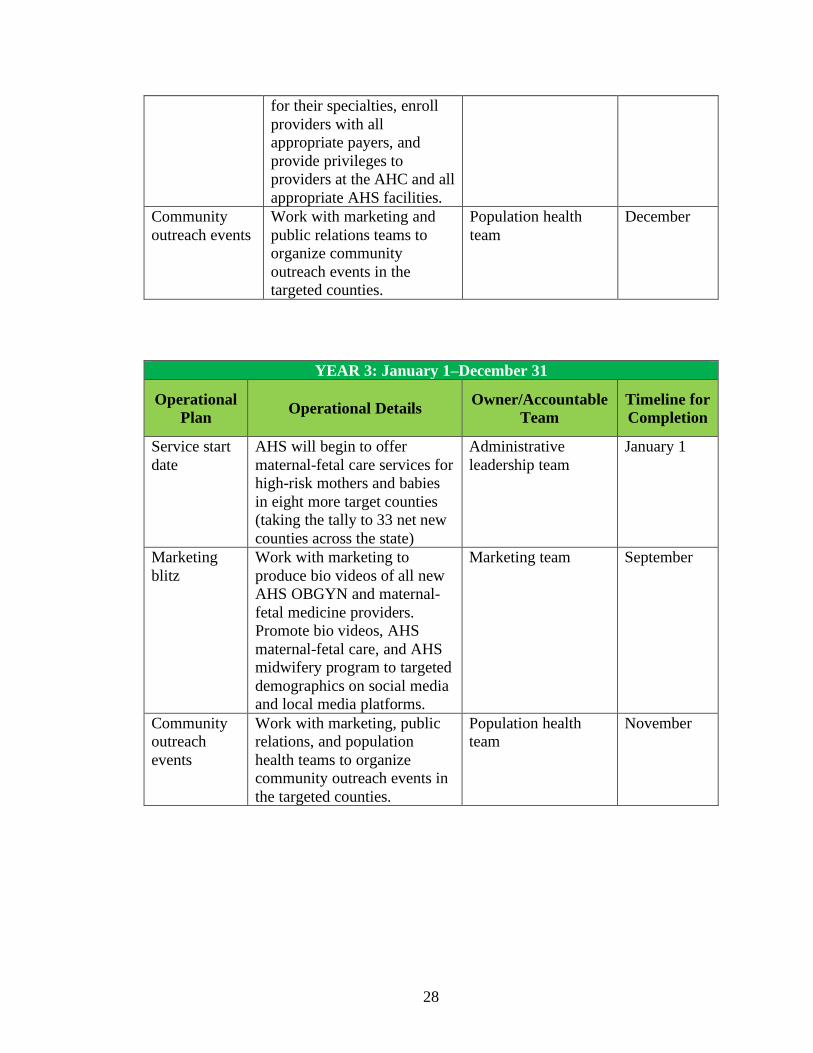
Operational Plan
The WHD leadership team has outlined a three-year organizational plan to add
providers, support staff, administrators, and additional practice locations to the WHD
community division.
Table 3: Operational Plan, Years 1–3
YEAR 1: January 1–December 31
Operational
Plan Operational Details
Owner/Accountable
Team
Timeline for
Completion
Business plan
approval
Present the business plan to
AHS CFO and the Business
Development Advisory
Council (BDAC) for review
and approval.
Administrative
leadership team
February
Budget
approval
Present the budget to the
AHS CFO and the Business
Development Advisory
Council (BDAC) for review
and approval.
Administrative
leadership team
February
Press release Design and distribute press
releases announcing the
AHS plan to expand access
and services into thirty-three
(33) underserved
communities across the
state.
AHS marketing team March
Recruitment of
providers
initiated
Submit request to hire nine
(9) physician FTEs
(OBGYN and maternal-fetal
medicine specialists) and
four advanced practice
provider FTEs.
Administrative
leadership team
April
Recruitment of
support staff
initiated
Submit request to hire
thirty-four (34) support staff
FTEs (medical assistants,
clinical support services,
and registered nurses
Administrative
leadership team
April

24
including navigators, OB
outreach, and midwives).
Recruitment of
administrative
staff initiated
Submit request to hire
twelve (12) administrative
support staff FTEs (practice
administrators and practice
managers).
Administrative
leadership team
April
Primary care
partnership
Work with AHS real estate
team to identify and embed
maternal care practices in
AHS Primary Care facilities
located in eighteen (18) of
the target counties across
the state.
Administrative
leadership team
May
Lease/buy
office spaces
Identify and lease or buy net
new office spaces in seven
(7) target counties where
AHS has no primary care or
OBGYN presence.
Administrative
leadership team
August
Space
renovation
Renovate and enhance
newly leased facilities for
optimal patient flow,
clinical flow, and workflow.
Design and
construction team
August
Marketing blitz Send brochures, flyers,
targeted messages to
targeted community
members through strategic
multimedia campaigns: TV,
radio, print, social media,
and billboard advertising.
Marketing team September
Bill areas and
cost centers
Create bill areas and cost
centers or new maternal-
fetal care practices in a
shared primary care space or
net new space.
Revenue cycle team September
Equipping Furnish new maternal-fetal
care locations with clinical
and non-clinical furniture,
hardware, equipment, and
supplies.
Supply chain
management team
September
Recruitment of
providers
completed
Hire nine physicians
(OBGYN and maternal-fetal
medicine specialists) and
four advanced practice
providers with a January 1
start date.
Administrative
leadership team
September

25
Recruitment of
support staff
completed
Hire thirty-four (34) support
staff members, including
RN navigators, OB outreach
nurses, and midwives, with
a January 1 start date.
Administrative
leadership team
October
Recruitment of
administrative
staff completed
Hire twelve (12)
administrative support staff
FTEs (practice
administrators and practice
managers) with a January 1
start date.
Administrative
leadership team
October
Systems
integration
Work with clinical
informatics team to
integrate all new clinics
with AHS EHR and IT
platforms, devices, and
systems.
IT team October
Convene project
team
WHD and AHS leadership
teams meet to review,
evaluate, and revise the plan
as needed.
Administrative
leadership team
November
Credentialing,
enrollment, and
onboarding
Work with AHS onboarding
team and revenue cycle
team to credential all
providers for their
specialties, enroll all
providers with all payers,
and provide privileges for
providers at the AHC and
all appropriate AHS
facilities.
Revenue cycle team November
Community
outreach events
Work with marketing and
public relations teams to
organize community
outreach events in the
targeted counties.
Population health
team
December

26
YEAR 2: January 1–December 31
Operational
Plan Operational Details
Owner/Accountable
Team
Timeline for
Completion
Service start
date
AHS will begin to offer
maternal-fetal care services
for high-risk mothers and
babies in twenty-five (25) of
the thirty-three (33) target
counties across the state.
Administrative
leadership team
January 1
Press release Distribute press releases
announcing the AHS plan to
expand access and services
into eight underserved
communities across the
state.
AHS marketing team February
Recruitment of
providers
initiated
Submit a request to hire
eight (8) physician FTEs
(OBGYN and maternal-fetal
medicine specialists) and
five advanced practice
provider FTEs.
Administrative
leadership team
April
Recruitment of
support staff
initiated
Submit a request to hire
sixteen (16) support staff
FTEs (medical assistants,
clinical support services,
and registered nurses
including navigators, OB
outreach, and midwives)
Administrative
leadership team
April
Recruitment of
administrative
staff initiated
Submit a request to hire two
(2) administrative support
staff FTEs (practice
administrators and practice
managers).
Administrative
leadership team
April
Lease or buy
office spaces
Identify and lease or buy net
new office spaces in eight
(8) target counties where
AHS has no primary care or
OBGYN presence.
Administrative
leadership team
May
Space
renovation
Renovate and enhance
newly leased facilities for
optimal patient flow, clinical
flow, and workflow.
Design and
construction team
July
Marketing blitz Send brochures, flyers,
targeted messages to
targeted community
Marketing team July

27
members through strategic
multimedia campaigns: TV,
radio, print, social media,
and billboard advertising.
Bill areas and
cost centers
Establish bill areas and cost
centers for each new
maternal-fetal care practice
in a shared Primary Care
space or a net new space.
Revenue cycle team August
Operational
needs
Furnish new maternal-fetal
care locations with clinical
and non-clinical furniture,
hardware, equipment, and
supplies.
Supply chain team August
Recruitment of
providers
completed
Hire eight (8) physician
FTEs (OBGYN and
maternal-fetal medicine
specialists) and five
advanced practice provider
FTEs with a start date of
January 1.
Administrative
leadership team
September
Recruitment of
support staff
completed
Hire sixteen (16) support
staff FTEs (medical
assistants, clinical support
services, and registered
nurses, including navigators,
OB outreach, and midwives)
with a start date of January
1.
Administrative
leadership team
September
Recruitment of
administrative
staff completed
Hire two (2) administrative
support staff FTEs (practice
administrator and practice
manager) with a start date of
January 1.
Administrative
leadership team
September
Systems
integration
Work with the clinical
informatics team to integrate
all new clinics with AHS
EHR and IT platforms,
devices, and systems.
IT Team September
Convene project
team
WHD and AHS leadership
teams meet to review,
evaluate, and revise the plan
as needed.
Administrative
leadership team
November
Credentialing,
enrollment, and
onboarding
Work with AHS onboarding
team and revenue cycle
team to credential providers
Revenue cycle team November
28
for their specialties, enroll
providers with all
appropriate payers, and
provide privileges to
providers at the AHC and all
appropriate AHS facilities.
Community
outreach events
Work with marketing and
public relations teams to
organize community
outreach events in the
targeted counties.
Population health
team
December
YEAR 3: January 1–December 31
Operational
Plan Operational Details
Owner/Accountable
Team
Timeline for
Completion
Service start
date
AHS will begin to offer
maternal-fetal care services for
high-risk mothers and babies
in eight more target counties
(taking the tally to 33 net new
counties across the state)
Administrative
leadership team
January 1
Marketing
blitz
Work with marketing to
produce bio videos of all new
AHS OBGYN and maternal-
fetal medicine providers.
Promote bio videos, AHS
maternal-fetal care, and AHS
midwifery program to targeted
demographics on social media
and local media platforms.
Marketing team September
Community
outreach
events
Work with marketing, public
relations, and population
health teams to organize
community outreach events in
the targeted counties.
Population health
team
November

29
Key Milestones for Success
The success of this business plan depends on the execution of the strategy and
milestones. AHS will look to the following critical milestones to measure success:
• Budget approval: Was the proposed budget required to execute the business plan
approved by AHS Chief Finance Officer and to the Business Development
Advisory Council (BDAC)?
• Space procurement: Was the team able to identify, share, lease or purchase
adequate space to embed a maternal-fetal care practice in each targeted county?
• Recruitment of providers and support staff: Was the team able to hire the
budgeted number of providers and support staff to build and grow maternal-fetal
care practices in the targeted counties?
• Credentialing, enrollment, and onboarding: Was the team able to credential,
enroll, obtain hospital or facility privileges, train, and onboard providers and
support staff on time for their service start dates?
• Service start dates: Was the team able to open the maternity practice doors to see
high-risk mothers and babies in the targeted counties at the planned start dates?
The answers to these questions will give the team a sense of where things stand and what
changes in strategy or tactics are needed.
Potential Operational Roadblocks and Resolutions
Once the project is approved, the team must consider several critical milestones
that, if not met, could derail the entire project. The chief of this potential roadblock is the
provider and support staff recruitment.

30
The WHD will hire twenty-six (26) new providers, thirteen (13) in year one and
thirteen (13) in year two. However, the provider recruitment window is limited. Suppose
the Physician and Advanced Practice Provider Recruitment Team miss that window. In
that case, it could take longer than expected to land a qualified candidate that is agreeable
to all parties within the scheduled time frame.
Most providers are unwilling to work in a rural setting or commute long distances
to build and grow their practice. Recruiting the required number of providers to work in
these counties will take time and could be expensive.
Furthermore, WHD plans to hire fifty (50) support staff in two years: Thirty-four
(34) in year one with a January 1 start date and sixteen (16) in year two with a January 1
start date. However, there is a documented shortage of medical assistants and registered
nurses locally and nationally for diverse reasons. The entire project hinges on finding an
adequate number of physicians, nurse practitioners, qualified medical assistants, clinical
services specialists, and registered nurses to support the physician practices.
Resolution
AHS will offer providers up to three (3) years of guaranteed compensation to
mitigate the provider recruitment concern. AHS must also offer sign-on bonuses,
relocation bonuses, and student loan assistance if needed.
AHS will pay above market value to mitigate the support staff recruitment
concern, offer referral and sign-on bonuses, relocation bonuses, and student loan
assistance if needed.

31
The cost of guaranteed compensation, sign-on bonuses, relocation bonuses,
student loan assistance, and supplemental pay for physicians, nurse practitioners,
and support staff is baked into the proforma financial statements of this plan.
Incorporation Strategy
The expansion of maternal-fetal care into thirty-three counties across the state is
under the operations, governance, and management of the existing corporate structure of
the women’s health department at AHS.
Regulation and Accreditation
The AHS Revenue Cycle Team will create bill areas for each new practice
location, credential all new providers for their specialties, enrolled all providers with all
appropriate payers, and provide privileges to providers at the AHC and other appropriate
AHS facilities.

32
The Marketing Plan
Overview of Goals of the Marketing Strategy
The general objective of the AHS marketing strategy for maternal-fetal care is to
increase unique high-risk OB patients by driving net new patient growth, increasing
overall patient volumes, and facilitating AHS loyalty for childbirth. To this end, AHS
will implement a robust maternal-fetal care presence to address access to care challenges
for high-risk mothers and babies in rural and underserved communities across thirty-three
counties in the state. AHS is determined to expand the funnel of women choosing AHS
for their maternal-fetal care, which will, in turn, increase the volume of high-risk
deliveries at the AHC. Successful execution of this market plan and business proposal
should increase high-risk deliveries at the AHC by 35% or more, grow AHS statewide
market share for OB care by 40% or more, and increase WHD’s operating profit margin
by 46% or more.
Market Analysis
• Target market and audience: The target market is women of child-bearing age
across the state, especially women of child-bearing age in underserved
communities. The target categories include women (aged 16–40), first-time
mothers, women planning to become pregnant, and newly pregnant women.
• Competition: There are three major health systems in the state that compete
directly against AHS. The competing organizations have some key strengths: All
three competing organizations have dozens of maternity practices across the state,
labor and delivery facilities with maternal-fetal medicine programs, and strong
33
brand awareness. Nonetheless, the competing organizations have some critical
weaknesses: Neither of the competing organizations has a school or college of
medicine in the state. Neither of the competing organizations has nationally ranked
or recognized medical facilities or programs related to maternal-fetal care.
• Market trends: ACOG estimates 500,000 fewer births in the U.S. in 2021, a
thirteen percent (13%) drop from the 3.8 million babies born in 2019. Historical
unique patient trends show increases around +2.5% year-over-year (YoY), with
2020 coming in at a -10% deficit to the previous year baseline for OBGYN. While
consumer sentiment is on the rise and the concern related to seeking healthcare
falls, acquiring new patients early in the year will continue to be more challenging
than the pre-COVID-19 timeframe. Recent patient acquisition requires cross-team
collaboration as consumer expectations demand business developments such as
virtual care, urgent care, connected care, and the integration of other services into
the Primary Care offices.
• Market research: According to the 2020 OBGYN Mom’s Journey market
research, most first-time and experienced mothers follow a traditional approach to
childbirth, and first-time mothers are less aware of the non-traditional approach.
For most women of child-bearing age, the critical factors in their access point
decision include in-network insurance, a recommendation from friends and family,
online reviews and information, distance from home, their birth plan, and ease of
getting appointments.

34
Figure 3: Access Point Decision Flowchart
There are three main takeaways from OBGYN Mom’s Journey market research: 1)
patients are looking for comfort, control, and connection to access, 2) patients want
coordinated care across all sites of care, and 3) when it comes to access, patients interpret
it as “seeing the doctor I want, when I want, where I want.”
Marketing Strategy
AHS will continue to meet patients where they live by expanding access and
services, increase the ability for care coordination, and develop digital consumer-focused
platforms to improve pregnancy outcomes, education, continuity of care, and patient
experience.
Strategy Objective
• Drive unique new patient appointments for OBGYN care across the AHS
system.
Media Target
35
• Women, ages 16–40
• First-time mothers
• Women planning to become pregnant
• Newly pregnant women
Timing
• Q1–Q4
Geography
• 33 counties across the state
Tactics
o Broadcast TV
▪ Cable run dates: March 29–May 9 and June 7–October 12
• Featuring: 30-second spots
o Connected TV
▪ Run dates: April 1–December 1
• 30-second videos on Connected TV with unique Calls to
Action (CTA) by geography
o Paid Social
▪ Facebook run dates: February 8–May 5, and June 1–October 31
• A variety of static, video, carousel, and slideshow posts,
including 2020 top-performing creative.
o Print
▪ Local Newspapers: March 1, April 2, April 30, May 17, June 23,
August 8, and September 30

36
• Ten total insertions to target minority audiences will engage
African American and Hispanic publications.
o Search Engine Marketing (SEM)
▪ Run January 1–December 31
• Include a variety of keywords.
o Digital Bio Video
▪ Run January 1–December 31
• Create 30-second videos that include a mix of creative
messaging.
o Includes African-American and Hispanic minority
targeting layers.
o Native Display
▪ Run March 1–May 30, and August 2–October 31
• Include a variety of image, headline, and description copy
options to test and optimize.
• Includes African American and Hispanic minority targeting
layers.
o Transit Advertising
▪ Run March 1–October 30
• Include a variety of image headlines and description copy
options to test and optimize.
o Utilize bus services, including Amtrak, Greyhound,
and Megabus.

37
o Billboards
▪ Run March 1–May 30, and August 2–October 31
• Include a variety of image, headline, and description copy
options to test and optimize.
o Community Events
▪ Run January 1–December 31
• Organize health fairs, health education sessions, medication
review sessions, and clinic sessions.
Marketing Budget
AHS will establish a marketing budget of $872,360 per year for three years. The
cost approximations are related to market research, brief creative designs, media
planning, advertising development, production, and post-campaign evaluation.

38
Table 4: Marketing Budget
Marketing Budget
Estimated
quantity
Estimated
cost per unit Estimated total
Press releases
Brochures 200,000 $0.20 $40,000
Flyers 100,000 $0.15 $15,000
Radio 20 $500 $10,000
Television 10 $12,000 $120,000
Social media 4 $5,000 $20,000
Total $205,000
Advertising
Broadcast TV 10 $15,000 $150,000
Connected TV 20 $2,000 $40,000
Print 80 $800 $64,000
Native display 20 $2,000 $40,000
Paid social 4 $5,000 $20,000
Search engine
marketing
1 $136,640 $136,640
Digital video
(Sabio)
26 $500 $13,000
Transit advertising 100 $600 $60,000
Billboards 50 $1,000 $50,000
Total $573,640
Community outreach
Hotel (6 rooms/6
people x 2 nights x
2 trips)
24 $200 $4,800
Food 24 $30 $720
Rental car/mileage
reimbursement
26,400 $0.50 $13,200
Gifts and supplies 1,000 $20 $20,000
Total $38,720
Media Total $817,360
Commission $55,000
Estimated Marketing Grand Total $872,360

39
Relationship with Current Business
The WHD Community Medicine Division will connect thousands of high-risk
maternity patients across the state to the AHC. The WHD, in conjunction with crucial AHS
departments, will create and sustain trusted partnerships between maternal-fetal care
providers and women of child-bearing age, leading to a lifetime commitment to the AHS
system.
Implementation of Marketing Strategy
Mode and Methods for marketing: The implementation of this market strategy will
follow Monroe’s Motivated Sequence: Attention, need, satisfaction, action, and
visualization.
40
Figure 4: Monroe's Motivated Sequence for AHS Marketing
Attention:
AHS will gain the attention of community members across the
targeted counties by sounding the alarm on infant and
maternal mortality rates across the state.
Need:
AHS marketing will communicate the need for high-level
maternal-fetal medical care for high-risk pregnancies across
the counties.
Satisfaction:
AHS marketing will introduce its high-level, high-ranking,
and highly rated AHC for high-risk mother and child including
its robust maternity care outreach expansions
Action:
AHS marketing will instruct target community members on
what, where, and how to access the highest level of care for
mother and baby in their communities and at the AHC.
Visualization:
AHS marketing will show community members how much
better life is and will become for mothers and babies, families,
and communities when women chose AHS for their maternal-
fetal care.

41
Through press releases, multimedia marketing blitzes, and community outreach
events, AHS will communicate access, safety, convenience, highly skilled care, and trusted
partnerships with women of child-bearing age. Through each implementation step, the
marketing team will ensure the following key performance indicators: 1) improved access
in Efficient Consumer Response (ECR) and Share of Category Requirements (SCR), 2)
Utilization of Customer Relation Management (CRM) for external new patient acquisition,
3) Increased completed web provider profiles (online scheduling, bio videos, tagging,
uncover and highlight unique and inspiring patient stories, and 4) Communicate improved
access via net new locations and providers.

42
Financial Documents
Summary of Financial Needs
The maternal-fetal care services expansion will operate under the WHD
Community Medicine Division. AHS will fund the growth with a $30,475,064
investment over three years: $20,790,651 in year one, $8,842,972 in year two, and
$841,436 in year three.
Startup Capital
The capital requirement to fund Year one is intended to meet the following
milestones: 1) hire nine physician FTEs (OB/GYN and maternal-fetal medicine
specialists); 2) hire four advanced practice provider FTEs; 3) hire thirty-four support staff
FTEs (medical assistants, clinical support services, and registered nurses including
navigators, OB outreach, and midwives); 4) hire twelve administrators (practice
administrators and practice managers); 5) embed maternal care practices in AHS Primary
Care facilities in eighteen counties; 6) lease or buy net new office spaces in seven target
counties where AHS has no primary care or OB/GYN presence; 7) renovate and enhance
the new facilities for optimal patient flow, clinical flow, and workflow; 8) furnish the
new maternal-fetal care locations with clinical and non-clinical furniture, hardware,
equipment, and supplies; 9) credential, enroll, and onboard care providers; 10) market net
new sites, services, and providers; and 11) organize community outreach events in the
targeted counties. The startup capital required is $20,790,651.

43
Table 5: OB/GYN Community Expansion Startup Costs
OB/GYN Community Expansion: Startup Costs
Startup Costs for
Year 1 (Monthly) Quantity Unit Cost
Monthly
Cost Year 1 Cost
Salaries, wages,
and benefits 59 $13,642 $804,895 $9,658,744.00
Supplies 25 $3,273 $81,830 $981,958.57
Drugs 25 $10,323 $258,073 $3,096,876.00
Purchased services 25 $4,778 $119,454 $1,433,443.06
Other operating
expenses 25 $3,942 $98,540 $1,182,477.00
Facility costs 25 $11,184 $279,605 $3,355,255.50
Marketing and
advertising $72,696.67 $872,360
Depreciation and
amortization $17,461.82 $209,541.79
Total Cost
$20,790,655.92
Expectations around ROI
AHS will fund this expansion project for three years. The WHD will receive
$20,790,651 in year one, $8,842,972 in year two, and $841,436 in year three. By the end
of Year four, AHS can expect to see high-risk deliveries at the AHC increased by 35% or
more, AHS statewide market share for OB care increase by 40% or more, and WHD’s
operating profit margin increase by 46% or more.

44
ROI Projection Snapshot
Table 6: ROI Projection Snapshot
Pro Forma Cash Flow Statement (Budget)
The WHD will see negative cash flows in years one, two, and three. However, as
total operating revenue continues to grow and total operating expenses continue to decline,
profit margins and cash flow will improve accordingly. However, AHS will cover the cash
needs of the WHD.
Current state Transition/investment period Future state
Year 0 Year 1 Year 2 Year 3 Year 4
Total
operating
revenue
$16,393,268 $21,022,546 $24,440,471 $29,177,865 $41,876,000
Total
operating
expense
$29,174,480 $49,965,136 $58,808,108 $59,649,544 $59,330,326.12
Operating
income
(investment)
($12,781,212.40) ($28,942,590) ($34,367,637) ($30,471,679) ($17,454,326)
Operating
profit
margin (%)
-78% -138% -141% -104% -42%

45
Table 7: Statement of Cash Flows
Statement of Cash Flows
Year 1 Year 2 Year 3
Cash flow from operations
Cash inflow
Cash received from patient
services $19,602,000 $22,275,000 $26,730,000
Accounts receivable $1,420,546 $2,165,471 $2,447,865
Total cash inflow $21,022,546 $24,440,471 $29,177,865
Cash disbursements
Marketing and advertising $872,360 $872,360 $872,360
Total salaries and wages
$27,120,438.04
$31,816,974.04
$32,370,116.08
Total benefits
$4,840,529.28
$5,644,173.28
$5,740,610.56
Supplies
$1,641,937.25
$1,962,315.25
$1,982,114.61
Drugs
$5,178,300.00
$6,188,700.00
$6,251,142.72
Purchased services
$2,373,633.50
$2,836,781.50
$2,850,675.94
Other operating expenses
$1,977,225.00
$2,363,025.00
$2,386,867.44
Facility costs
$5,610,337.50
$6,705,037.50
$6,772,689.96
Depreciation and
amortization
$350,375.75
$418,741.75
$422,966.77
Total cash disbursement
$49,092,776.32
$57,935,748.32
$58,777,184.08
Net increase/decrease in
cash ($28,070,230) ($33,495,277) ($29,599,319)
Beginning cash balance ($12,781,212.40) ($40,851,443) ($74,346,720)
Ending cash balance ($40,851,443) ($74,346,720) ($103,946,039)

46
Three-Year Income Projection: WHD
AHS will implement a robust maternal-fetal care presence to address access to care
challenges for high-risk mothers and babies in rural and underserved communities across
the state. The WHD will begin with twenty-five (25) new locations in year one and eight
additional locations in year two. The WHD income projections depend on volume
projections, wRVU projections, net patient revenue per wRVU of $89.10, and annual
accounts receivables at 10% of total patient revenue. Below is the three-year income
projection for the WHD.
Table 8: 3-Year Income Projection for WHD
Current 3-Year Income Projection Year 1 Year 2 Year 3
170,000 Projected wRVUs 220,509 250,509 300,509
$15,147,000 Patient revenue $19,602,000 $22,275,000 $26,730,000
$1,246,268 (net patient revenue per
wRVU @ $89.10) $1,420,546 $2,165,471 $2,447,865
$1,246,268 Accounts receivables $1,420,546 $2,165,471 $2,447,865

47
Projected Balance Sheet
Table 9: Projected Balance Sheet
Projected Balance Sheet
Year 1 Year 2 Year 3
Assets
Cash $21,022,546 $24,440,471 $29,177,865
Accounts receivable $1,420,546 $2,165,471 $2,447,865
Property and
equipment $2,915,060.68 $7,252,274.75 $8,667,352.75
Depreciation and
amortization $350,375.75 $418,741.75 $422,966.77
Total assets $25,007,777 $33,439,475 $39,870,116
Liabilities
Accrued salary,
wages, and benefits $31,960,967.32 $37,461,147.32 $38,110,726.64
Accounts payable $6,953,190.39 $4,021,672.32 $1,759,389
Total liabilities $25,007,776.93 $33,439,475.00 $39,870,115.98
Break-Even Analysis
Although AHS is a nonprofit organization and does not expect to profit from its
operations, the WHD performed a break-even analysis to determine the number of wRVUs
needed to cover the operating cost of the WHD. The below table shows that the WHD will
have to generate 325,020 wRVUs to break even in the first year of business.
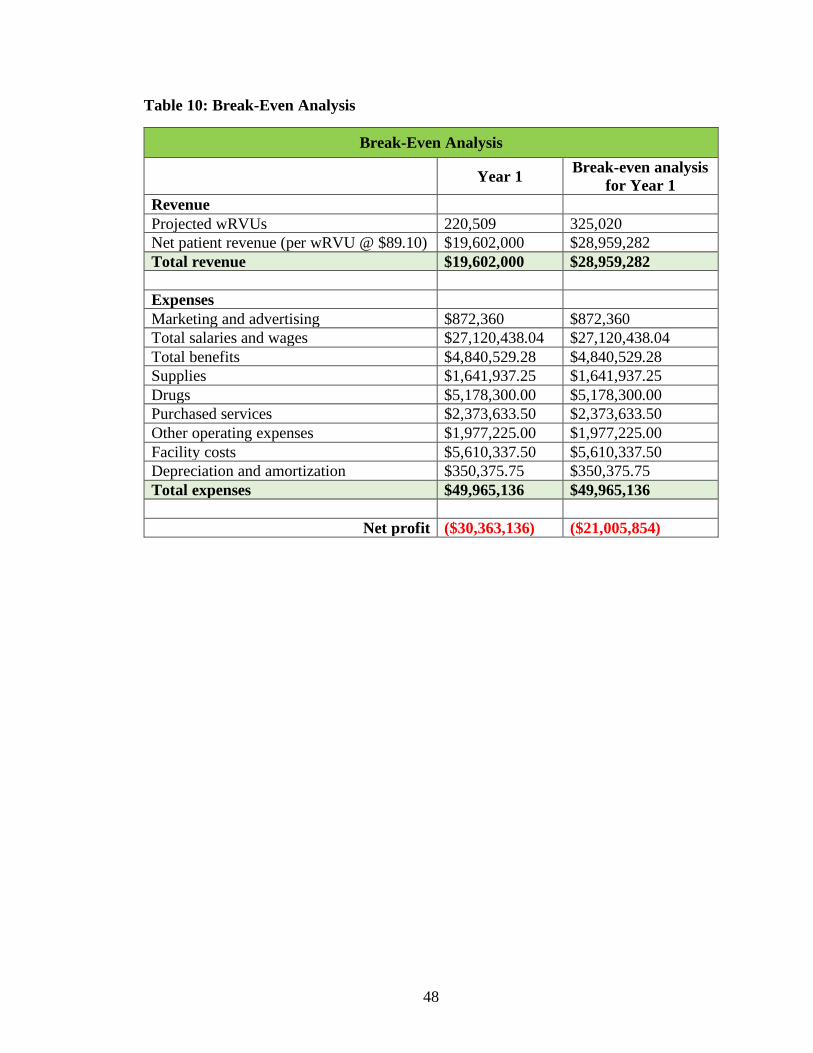
48
Table 10: Break-Even Analysis
Break-Even Analysis
Year 1 Break-even analysis
for Year 1
Revenue
Projected wRVUs 220,509 325,020
Net patient revenue (per wRVU @ $89.10) $19,602,000 $28,959,282
Total revenue $19,602,000 $28,959,282
Expenses
Marketing and advertising $872,360 $872,360
Total salaries and wages $27,120,438.04 $27,120,438.04
Total benefits $4,840,529.28 $4,840,529.28
Supplies $1,641,937.25 $1,641,937.25
Drugs $5,178,300.00 $5,178,300.00
Purchased services $2,373,633.50 $2,373,633.50
Other operating expenses $1,977,225.00 $1,977,225.00
Facility costs $5,610,337.50 $5,610,337.50
Depreciation and amortization $350,375.75 $350,375.75
Total expenses $49,965,136 $49,965,136
Net profit ($30,363,136) ($21,005,854)

49
Profit & Loss Statement (Income Statement)
Table 11: Income Statement
Income Statement
Year 1 Year 2 Year 3
Income
Net patient revenue $19,602,000 $22,275,000 $26,730,000
Other revenue $1,420,546 $2,165,471 $2,447,865
Gross income $21,022,546 $24,440,471 $29,177,865
Expenses
Marketing and
advertising $872,360 $872,360 $872,360
Total salaries and
wages $27,120,438.04 $31,816,974.04 $32,370,116.08
Total benefits $4,840,529.28 $5,644,173.28 $5,740,610.56
Supplies $1,641,937.25 $1,962,315.25 $1,982,114.61
Drugs $5,178,300.00 $6,188,700.00 $6,251,142.72
Purchased services $2,373,633.50 $2,836,781.50 $2,850,675.94
Other operating
expenses $1,977,225.00 $2,363,025.00 $2,386,867.44
Facility costs $5,610,337.50 $6,705,037.50 $6,772,689.96
Depreciation and
amortization $350,375.75 $418,741.75 $422,966.77
Total operating
expenses $49,965,136 $58,808,108 $59,649,544
Operating income
(investment) ($28,942,590) ($34,367,637) ($30,471,679)
Operating profit
margin % -138% -141% -104%

50
Financial Statement Analysis
According to the financial statements and projections, the WHD will see a decrease
in operating profit margin in year one and year two before a steady improvement from year
three onward. By year four, the operating profit margin would have increased by 46%.
Based on the income statement, precisely the patient revenue line item, the total operating
revenue is projected to grow by 13% from year one to year two, and by 19% from year two
to year three. By the end of year four the WHD is projected to see a 43% increase in total
operating revenue from year three. AHS estimate accounts receivables at 10% per year.
Payor Mix
The AHS market research team’s analysis of demographic and insurance data for
all 33 counties show an excellent payor mix for AHS: Anthem, United Health Care (UHC),
Medicaid (all types), Healthy (State) Plan (all types), AHS Health Plans, Medicare (all
types), all other commercial plans, and self-pay. The high Medicaid (all types) population
in these thirty-three target counties would continue to serve as a yardstick for income
projection work beyond year three.

51
Figure 5: Payor Mix
Financial Impact from Competition
According to AHS market research and analysis, two of the three major health
systems that compete directly against AHS have announced plans to establish brand new
women’s health centers in two of the thirty-three targeted counties. AHS expects the three
major competitors to expand into more counties in Year four or five of its operation. The
entry threat of AHS competitors into the target markets in year four or five will have a
financial impact of 5% to 10% by the end of the fiscal year of record. AHS plans to expand
its high-risk maternal-fetal care services into all thirty-three (33) counties for a total of
seventy-five (75) sites by year four. AHS anticipates this will help serve as a barrier to
entry for other competing healthcare systems in the state. With the expansion into these
targeted counties, AHS can expect to see high-risk deliveries at the AHC increased by 35%

52
or more, AHS statewide market share for OB care increase by forty percent 40% or more,
and WHD’s operating profit margin increase by 46% or more.
Table 12: Income Projection for Years 4–6
Income Projection- Years 4 - 6 Year 4 Year 5 Year 6
Projected wRVUs 469,988 479,388 488,788
Patient revenue $41,875,931 $42,713,471 $43,551,011
Accounts receivables $1,673,765 $1,506,389 $1,339,012
Total Income $43,549,696 $44,219,860 $44,890,023
Business Financial History
The WHD Community Medicine Division has often taken a conventional approach
to expand its community presence, adding new providers and new office spaces. However,
WHD has made these investments when the data analytics team could demonstrate a
sustained level of demand in each case. The market analysis and data on the thirty-three
target counties provided strong indications that expansion into these communities would
be economically sustainable. AHS has the cash reserves needed to supply the operating
and capital needs required for this project.
The WHD currently has a total operating revenue of $16,393,268 a total operating
expense of $29,174,480, an operating income per investment of -$12,781,212, and an
operating profit margin of -78%. The WHD currently has thirteen administrative staff
FTEs, seventy-one support staff FTEs, twenty-nine physician FTEs, and eleven nurse
practitioner FTEs. These combined FTEs managed 68,189 encounters or visits in the past
twelve months, generating 170,000 wRVUs. By the end of this plan implementation, the
53
WHD will have twenty-seven administrative staff FTEs, 121 support staff FTEs, forty-six
physician FTEs, and twenty nurse practitioner FTEs. These combined FTEs are projected
to manage over 200,000 encounters in year four, generating over 450,000 wRVUs.
This project requires a $30,475,064 investment from AHS into the WHD
operations. This investment will increase the total operating expense for the WHD to
$49,965,136 in year one, $58,808,108 in year two, and $59,649,544 in year three. AHS is
a nonprofit and does not expect to produce a positive operating profit margin. However, it
expects the WHD to improve its operating profit margins. Accordingly, the WHD projects
the operating profit margin to increase by 46% or more at the end of year four.
54
Innovative Elements and Expected Business Outcomes
Why and how does this innovative idea positively impact the health of your
population and the organization?
Realizing the vision of the School of Medicine to “lead the transformation of health
care through quality, innovation, and education and make the state one of the nation’s
healthiest states” requires big thinking, strong collaborations, and hard work. The current
state of Indiana’s health is disheartening. The state is 41st in the nation in overall health,
according to the 2018 America’s Health Rankings report, and ranks 42nd when it comes to
mental health, according to Mental Health in America 2019. One baby dies in Indiana
approximately every fourteen hours—amounting to 600 infant deaths a year—making the
state’s infant mortality rate one of the worst in the country. In its 2020 report, March of
Dimes published a list of thirty-three counties across the state classified as “maternity
deserts.”
Through this business plan, AHS will fill a gap for high-risk OB patients to access
maternal-fetal care. By opening 33 new clinic locations and expanding obstetrics coverage
to high-risk patients in underserved counties, AHS aims to positively impact community
members’ health and wellbeing by reducing infant and maternal mortality across the state.
In the thirty-three targeted counties, patients are accustomed to driving two or more
hours to see their healthcare provider. By opening clinics in thirty-three counties, AHS will
provide a welcome convenience to patients in the community. As an organization, AHS
can take the lead in boosting the health, safety, and wellbeing of millions of women.

55
What challenges did you encounter during this process, and what have you learned?
One major challenge encountered during this process is making business
projections about the volume of patients, service utilization, and revenue against the
backdrop of operational uncertainties. An inherent unpredictability associated with
obstetrics requires investing in provider and support staff to ensure access, safety, and
timeliness. Recruiting and retaining enough skilled personnel at clinics in the targeted
communities will be a continuous challenge.
Next steps
The next step required to put this proposal into action is to develop a mutually agreeable
strategy between the WHD and the AHS project teams with milestones and triggers in
place. The WHD team must initiate a project team meeting to review the business plan.
The success of this business plan depends on two factors: how well the strategy is executed
and whether each milestone is met or exceeded. AHS will look to the following critical
milestones to measure success:
• Budget approval: Was the proposed budget required to execute the business plan
approved by the AHS Chief Finance Officer and the Business Development
Advisory Council (BDAC)?
• Space procurement: Was the team able to identify, share, lease, or purchase
adequate space to embed a maternal-fetal care practice in each targeted county?
• Recruitment of providers and support staff: Was the team able to hire the
necessary number of providers and support staff to build and grow maternal-fetal
care practices in the targeted counties?
56
• Credentialing, enrollment, and onboarding: Was the team able to credential,
enroll, obtain hospital or facility privileges, train, and onboard providers and
support staff in time for their service start dates?
• Service start dates: Was the team able to open the maternity practice doors to see
high-risk mothers and babies in the targeted counties at the planned start dates?
The answers to these questions will give the team a sense of where things stand
and what changes in strategy or tactics are needed. Overall, success will primarily be
measured by clinical outcomes, patient satisfaction scores, and financial gains or losses.
By meeting patients in their communities, expanding access and services, increasing care
coordination, and expanding digital consumer-focused platforms, AHS will positively
impact women and families in thirty-three (33) additional counties for many years to
come.