indian journal of ijpp practical pediatricsijpp.in/admin/uploadimage/jan - apr.pdf · indian...
TRANSCRIPT

2009; 11(1) : 1
11
IJPPINDIAN JOURNAL OFPRACTICAL PEDIATRICS
••••• IJPP is a quarterly subscription journal of the Indian Academy of Pediatricscommitted to presenting practical pediatric issues and managementupdates in a simple and clear manner
••••• Indexed in Excerpta Medica, CABI Publishing.
Vol.11 No.1 JAN.-MAR.2009
Dr. K.Nedunchelian Dr. S. ThangaveluEditor-in-Chief Executive Editor
CONTENTS
FROM THE EDITOR'S DESK 3
TOPIC OF INTEREST - TOXICOLOGY
Organophosphate, carbamate and rodenticide poisoning 6
- Rajendiran C, Ravi G, Thirumalaikolundu Subramanian P
Hydrocarbon and related compounds poisoning 15
- Utpal Kant Singh, Prasad R, Gaurav A
Common drug poisoning 22
- Suresh Gupta
Corrosive poisoning 37
- Jayanthi Ramesh
House hold material poisoning 41 - Shuba S, Betty Chacko
Cardiotoxins 53
- Rashmi Kapoor
Narcotic poisoning 64
- Kala Ebinazer
Journal Office and address for communications: Dr. K.Nedunchelian, Editor-in-Chief, Indian Journal of PracticalPediatrics, 1A, Block II, Krsna Apartments, 50, Halls Road, Egmore, Chennai - 600 008. Tamil Nadu, India.Tel.No. : 044-28190032 E.mail : [email protected]

Indian Journal of Practical Pediatrics 2009; 11(1) : 2
2
Published by Dr.K.Nedunchelian, Editor-in-Chief, IJPP, on behalf of Indian Academy of Pediatrics,from 1A, Block II, Krsna Apartments, 50, Halls Road, Egmore, Chennai - 600 008. Tamil Nadu, Indiaand printed by Mr. D. Ramanathan, at Alamu Printing Works, 9, Iyyah Street, Royapettah,Chennai - 14.
2
FOR YOUR KIND ATTENTION
* The views expressed by the authors do not necessarily reflect those of the sponsor orpublisher. Although every care has been taken to ensure technical accuracy, no responsibility isaccepted for errors or omissions.
* The claims of the manufacturers and efficacy of the products advertised in the journal arethe responsibility of the advertiser. The journal does not own any responsibility for the guarantee ofthe products advertised.
* Part or whole of the material published in this issue may be reproduced withthe note "Acknowledgement" to "Indian Journal of Practical Pediatrics" without prior permission.
- Editorial Board
GENERAL ARTICLESIntrauterine growth retardation : Journey from conception tolate adulthood 68
- Neelam Kler, Naveen Gupta
Child adoption 82
- Ganesh R, Suresh N, Eswara Raja T, Lalitha Janakiraman, Vasanthi T
DERMATOLOGYIchthyosis - An approach 86- Anandan V
PICTURE QUIZ 91
RADIOLOGIST TALKS TO YOUDisorders of ventral induction and similar conditions - I 92
- Vijayalakshmi G, Elavarasu E, Vijayalakshmi M, Venkatesan MD
CASE STUDYUnusual complication of nasogastric tube insertion in a child 95
- Poovazhagi V, Shanthi S, Vijayaraghavan A, Kulandai Kasturi R
Congenital miliary tuberculosis 97- Vijayakumari, Suresh DV
CLIPPINGS 14,21,52,63,81,94
NEWS AND NOTES 85,90

2009; 11(1) : 3
33
FROM THE EDITOR’S DESK
The first issue for the year 2009 on“Toxicology”, covers some of the commonchildhood poisonings as topic of interest.
“Poisons and medicine are oftentimes thesame substance given with different intents” –Peter Latham [1865].
“Toxicology” is the science of poisons whichdeals with the nature, effects, detection of poisonsand the treatment of poisoning. It is worthy toconsider here few general aspects in this field.
Most frequent poisoning we come acrossinclude prescribed medications such as salicylates,paracetamol, antiseptics, anticonvulsants as wellas non medications like hydrocarbons (kerosene,polish, petrol), cleaning solutions, causticmaterials and pesticides.
The reaction to such substances can be achange from a normal state at molecular, cellular.organ systems level or involving entire bodysystem. The changes can be local or systemic,reversible or irreversible, immediate or delayedand graded or quantal. If mortality is the response,the dose that is lethal to 50% of the population isknown as LD50,which varies with individualsubstances.
The toxic effect of a substance on a livingorganism essentially depends on a) the magnitudeof hazard (potential to cause harm), which is anintrinsic property of the substance, b) risk ie,likelihood of harm which is a combination ofhazard with probability of exposure and themagnitude and frequency of doses c) exposure(concentration along with duration of contact) andd) dose ie, the amount of chemical that entersthe body .
Other important factors which maydetermine, the toxicity of a substance are: a) Route:Intravenous route is the most dangerous followed
by inhalation, intraperitonial, intramuscular,ingestion and topical in that order. b) Absorption,distribution, metabolism and excretioncharacteristics of the substance. c)Individual’ssusceptibility where 10-30 fold difference inresponse can be observed in a population.Individual susceptibility of a population inturndepends on age, nutritional, health status andprevious or concurrent exposures (additive,synergistic or antagonistic).
Principles of management include removingpoison or the patient from site, initial resuscitationand stabilization, removal of non-absorbedpoison,measures for elimination of absorbedpoison, specific antidote if any and symptomatictreatment.
Prevention is always better than cure, whichholds good for poisoning too. Younger the childmore likely the chance that they ingest or comein contact with dangerous material and theyshould not be left with out supervision.Unintentional or accidental poisoning is usuallyrare in children more than 5 years of age.Unfortunately, most of the cosmetics and cleanersare distributed in colourful packaging and thechildren get attracted to them since they look likea candy or toy. It is always better to keep themout of reach of children.
Signs of poisoning are widespread whichmay be difficulty in breathing or speaking,dizziness, unconsciousness, foaming or burningof mouth, cramps, nausea and vomiting.This should be kept in mind and a high index ofsuspicion of poisoning is needed in a situationwhere there is sudden onset of organ disturbancewhich cannot be explained otherwise.
Dr. K.Nedunchelian,Editor-in-Chief.

Indian Journal of Practical Pediatrics 2009; 11(1) : 4
4
GeneralPrint the manuscript on one side of standard size A4, white bond paper, with margins of at least 2.5 cm (1”)in double space typescript on each side. Use American English using Times New Roman font 12 size. Submitfour complete sets of the manuscript.They are considered for publication on the understanding that they are contributed to this journal solely.All pages are numbered at the top of the right corner, beginning with the title page.All manuscripts should be sent to: The Editor-in-Chief, Indian Journal of Practical Pediatrics
Manuscript1st Page –
TitleName of the author and affiliationInstitutionAddress for correspondence (Email, Phone, Fax if any)Word countNo. of figures (colour / black and white)No. of referencesAuthors contribution
2nd Page –Abstract (unstructured, not exceeding 100 words) with key words (not exceeding 4)
3rd Page -AcknowledgementPoints to remember (not more than 5 points)TextReferencesTablesFigures – should be good quality, 4 copies black & white / colour, (4 x 6 inches – Maxi size) Glossy print.(Each colour image will be charged Rs.1,000/- separately)Legends
TextOnly generic names should be usedMeasurements must be in metric units with System International (SI) Equivalents given in parentheses.
ReferencesRecent and relevant references onlyStrictly adhere to Vancouver styleShould be identified in the text by Arabic numerals in parentheses.Type double-space on separate sheets and number consecutively as they appear in the text.Defective references will entail rejection of article
TablesNumbered with Roman numerals and typed on separate sheets.Title should be centered above the table and explanatory notes below the table.
Figures and legendsUnmounted and with figure number, first author’s name and top location indicated on the back of eachfigure.Legends typed double-space on separate sheet. No title on figure.
INSTRUCTIONS TO AUTHORS
4

2009; 11(1) : 5
5
Article CategoriesReview article
Article should be informative covering the recent and practical aspects in that field. Main articles can be in1500 – 2000 words with 12 – 15 recent references and abstract not exceeding 100 words.
Case report (covering practical importance)250 – 600 words, 8 – 10 recent references
Clinical spotters section100 – 150 words write upWith 1 or 2 images of clinically recognizable condition(of which one could be in the form of clinical photograph / specimen photograph / investigation)
Letters to the Editor200 – 250 words pertaining to the articles published in the journal or practical viewpoints with scientificbacking and appropriate references in Vancouver style.
Check ListCovering letter by corresponding authorDeclaration (as enclosed) signed by all authors **Manuscript (4 copies)Accompanied by a copy in CD / or submit as an email attachment in addition to hard copy.
Failing to comply with the requirement at the time of submission would lead to the rejection of the article.Author’s contribution / Authorship CriteriaAll persons designated as authors should qualify for the authorship. Authorship credit should be based onsubstantial contributions to i) concept and design, or collection of data, and interpretation of data;ii) drafting the article or revising it critically for important intellectual content; and iii) final approval of the versionto be published. All conditions i), ii) and iii) must be met.**Declaration by authorsI/We certify that the manuscript titled ‘……………………………….’ represents valid work and that neither thismanuscript nor one with substantially similar content under my/our authorship has been published or is beingconsidered for publication elsewhere. The author(s) undersigned hereby transfer(s), assign(s), or otherwiseconvey(s) all copyright ownership, including any and all rights incidental thereto, exclusively to the IndianJournal of Practical Pediatrics, in the event that such work is published in Indian Journal of Practical Pediatrics.I / we assume full responsibility for any infringement of copyright or plagiarism.Authors’ name(s) in order of appearance in the manuscript
Signatures (date)
All manuscripts, which are rejected will not be returned to author. Those submitting articles should thereforeensure that they retain at least one copy and the illustrations, if any.
Selection proceduresAll articles including invited articles will be peer reviewed by two masked reviewers. The decision of theEditorial Board based on the reviewers’ comments is final.
5

Indian Journal of Practical Pediatrics 2009; 11(1) : 6
66
TOXICOLOGY
ORGANOPHOSPHATE,CARBAMATE AND RODENTICIDEPOISONING IN CHILDREN
* Rajendiran C **Ravi G
***Thirumalaikolundu Subramanian P
Abstract : Organophosphate, carbamate androdenticide poisoining are less common amongchildren. The mode of occurence is usuallyaccidental in children. The pathophysiology,clinical features, diagnosis and treatment ofthese poisoning are covered in this article.
Key words: Poisoning, Organophosphate,Organocarbamate, Rodenticide, Children.
Poisoning is less common among childrenand takes hundreds of innocent small lives everyyear. Unfortunately, most of these miseriesare accidental and unintentional. Poisonings dueto pesticides and rodenticides are relativelyless compared to kerosene and drug over dosagein India. But because of their easy availabilityand accessibility, practitioners should haveadequate knowledge about them. There is a needto strengthen the ability to diagnose andtreat them.
ORGANOPHOSPHATE ANDCARBAMATE POISONING
Epidemiology
In the absence of national registers orreliable hospital based data, one looks forward totertiary hospital for data. Accordinglyorganophosphate (OP) and carbamate poisoningscomprise less than one percent of total poisonings.Rodenticide poisoning is far less than pesticides.
The incidence of pesticide poisoning tendsto be higher among children from lower socio-economic class of society due to poor storagefacility and parental negligence. Inexperience,lack of maturity, illiteracy and inability to assessthe risk make them prone for accidental ingestion.
Older children and adolescents may bedirectly exposed as field workers, while youngerchildren may be brought into treated fields toaccompany their parents. Work clothes oftencarry pesticide residues, exposing both workersand family members.
Stress factors for poisoning are grouped asfamily stress (death of a parent, mental illness ina parent, financial problems, conflicts amongparents, parental alcoholism, divorce, separationetc.), parent stress (punitive parent, conflict withparents etc.) and school stress (poor academicachievement, examination failures, change ofschool, teacher stress, etc).
Pathophysiology
Organophosphorous compounds (OPC) andcarbamates bind to one of the active sites of
* Professor of Medicine** Asst. Professor of Medicine
Poison Control Training & Research Center,Institute of Internal Medicine,Madras Medical College, Chennai.
*** Director (Retd), Institute of Internal Medicine,Madras Medical College, Chennai.

2009; 11(1) : 7
7
acetylcholinesterase (AChE)1 and inhibit thefunctionality of this enzyme by means of stearicinhibition. Carbamylation of esters are quicklyreversible than phosphorylation of the esters.Phosphorylation of the esters in AChE willundergo “ageing” process. Aging means loss ofone alkyl or alkoxy group leading to stable monoalkyl or mono alkoxy phosphoryl AChE occuringover a period of 48 hours after exposure.Spontaneous regeneration of phosphorylatedAchE requires days to months.
The main function of AChE is to hydrolyzeacetylcholine (ACh) to choline and acetic acid.Therefore, the inhibition of AChE causes anexcess of ACh in synapses and neuromuscularjunctions, resulting in muscarinic and nicotinicsymptoms and signs.
The pathophysiology of intermediatesyndrome is not well defined. In some individuals,neuropathy target esterase (NTE) is targeted tocause OPC induced delayed polyneuropathy.
Poisoning dosage
Children may die of organo phosphorouscompounds (OPC) with very minimal dose of2mg(0.1mg/kg). Studies showed that younganimals were more susceptible than adult of samespecies and that may be applicable to humanbeings also. The poisoning dose varies fromcompound to compound2. In general, thoseavailable for household use (1-2% as diluteformulation) are less toxic than those used inagriculture (40-50% concentration). Whatever bethe situation, the victims should be observed forat least 48 to 72 hours.
Clinical features
Children are more vulnerable than adults dueto various risk factors like smaller size, differingmetabolism and rapidly growing and developingorgan systems. Pediatric patients show
predominately CNS depression and severehypotonia, whereas muscarinic symptoms areinfrequent3.
Pesticides can be rapidly absorbed throughthe skin, lungs, gastrointestinal tract and mucousmembranes. The rate of absorption depends onthe route of administration and the type oforganophosphate or carbamate. Symptoms usuallyoccur within a few hours after ingestion andappear almost immediately after inhalation.Patients often present with evidence of acholinergic toxic syndrome or toxidrome. It isuseful to remember the toxidrome in terms of thethree clinical effects on nerve endings1,4 and theyare nicotinic effects at neuromuscular junctionsand autonomic ganglia, CNS effects andmuscarinic effects on postganglionic andparasympathetic end organs (Table 1). Nicotinicsigns and symptoms include weakness,fasciculation and paralysis. Diaphragmaticweakness may result in respiratory difficulty andrespiratory failure. In addition as ACh is theneurotransmitter in pre–ganglionic sympatheticnerves, it may cause stimulation of sympatheticnervous system resulting in mydriasis, tachycardiaand hypertension, whereas CNS effects may leadto restlessness, tremors, confusion, seizures andCNS depression. The clinical presentation canbe a combination of these effects depending onthe receptor activity maximally affected. At lowdoses muscarinic effect predominates. In moresevere intoxication nicotinic and centralmuscarinic effects predominate. Due to thistachycardia and hypertension (nicotinic effect)may be seen in severe poisoning instead ofclassical bradycardia. Carbamates have lessCNS toxicity.
Respiratory failure5: There seems to be twounderlying mechanisms for respiratory failure andthey are an early acute mixed central andperipheral respiratory failure and a late peripheralfailure rather than two distinct clinical syndromes.

Indian Journal of Practical Pediatrics 2009; 11(1) : 8
8
Intermediate syndrome
The intermediate syndrome (IMS) occurs inapproximately 20% of patients following oralexposure to OP pesticides, with no clearassociation between the particular OP pesticideinvolved and the development of the syndrome.It usually develops 2 to 4 days after exposurewhen the symptoms and signs of the acutecholinergic syndrome (e.g. muscle fasciculations,muscarinic signs) are no longer obvious.The characteristic features of the IMS areweakness of the muscles of respiration(diaphragm, intercostal muscles and accessorymuscles including neck muscles) and of proximallimb muscles. Accompanying features ofteninclude weakness of muscles innervated by somecranial nerves. It has been commonly associatedwith OPCs like diazinon, dimethoate,methylparathion, methamidaphos, monocrotophos,fenthion and ethylparathion.3,4
Organophosphate induced delayedneuropathy (OPIDN) sets in after a period of7 to 21 days of exposure and causes significantmorbidity. The earliest symptoms to be seen are
paresthaesia and calf pain. Weakness appearsinitially in the distal leg muscles causing foot drop,followed by small muscles of the hands. Later itmay extend proximally and even involve thetruncal muscles. Gait ataxia is disproportionateto the motor and sensory loss. The cranial nervesand the autonomic nervous system are notinvolved. Deep tendon jerks are absent.
Chronic organophosphate inducedneuropsychiatric disorder (COPIND)
Follow-up studies of individuals who havebeen exposed to high levels of organophosphatecompounds revealed development of certainneurobehavioural changes in some of them,which have been termed together as COPIND.These effects include, drowsiness, confusion,lethargy, anxiety, emotional lability, depression,fatigue and irritability.
The effects of dithiocarbamate compoundsare currently suspected not only for neurotoxicity,but also as endocrine-disrupting chemicals.Although dithiocarbamates showed weakneurotoxicity in adult animals, more attentionneeds to be paid to developmental neurotoxicity.3
Table 1. Symptoms and signs of organophosphate compound poisoning
SLUDGE/BBB DUMBELS
S = Salivation D = Diarrhea and diaphoresis
L = Lacrimation U = Urination
U = Urination M = Miosis
D = Defecation B = Bronchorrhea, bronchospasm, and bradycardia
G = GI symptoms E = Emesis
E = Emesis L = Lacrimation
B = Bronchorrhea S = Salivation
B = Bronchospasm
B= Bradycardia

2009; 11(1) : 9
9
Over all the clinical features of carbamateingestion are similar to those of OP poisoning andthe presenting symptoms include both muscarinicand nicotinic features. However, central nervoussystem features are not very prominent incarbamate poisoning due to the poor permeabilityof these compounds across the blood-brain barrier.
OPC and carbamates are also known fortheir pancreatic toxicity. They may also causecardiac arrhythmias and ECG disturbances.6
Diagnosis and laboratoryinvestigations
The OPC and carbamate poisoning can beconfirmed by measuring RBC or plasmacholinesterases. RBC cholinesterase is moreaccurate and well correlated with neurotoxicity,but the test is costlier and not easily available.Normal value for plasma cholinesterase is4000-10,000 IU/L. It is otherwise called as butrylcholinesterase (BuChE) or pseudocholinesterase.These cholinesterase levels have no therapeuticas well as prognostic significance. One shouldremember that measuring enzymatic activity toarrive at a diagnosis of carbamate poisoning maybe misleading due to a transient anticholinesteraseeffect.
Besides routine blood investigations, serumhas to be collected for amylase, pancreatic lipaseand liver function test. Some patients may havehyperamylasemia, hyperglycemia and increasedliver enzymes.
ECG : The common ECG findings are ST-T wavechanges and low voltage complexes which arepresent in severe poisoning. Other less commonoccurrences are prolonged QT intervals, ectopicbeats and conduction block.
Electrophysiological studies followingOP poisoning have revealed three characteristicphenomena: (i) repetitive firing following a single
stimulus; (ii) gradual reduction in twitch heightor compound muscle action potential followedby an increase with repetitive stimulation(the ‘decrement-increment response’) and(iii) continued reduction in twitch height orcompound muscle action potential with repetitivesimulation (‘decrementing response’). Of these,the decrementing response is the most frequentfinding during the IMS, whilst repetitive firing isobserved during the acute cholinergic syndrome.
Makhaeva, et al showed that neuropathytarget esterase (NTE) assay for whole bloodcould serve as a biomarker of exposure toneuropathic OP compounds as well as a predictorof OPIDN and an adjunct to its early diagnosis.7
Treatment8-14
Like any other emergency care, maintainingairway, breathing and circulation is the first andforemost important aspect.
Decontamination9,13,14 plays a vital role in theoutcome of any poisoning. It includes thoroughwhole body wash with soap and water, washingof eyes with clean tap water and replacing theclothes worn by the patient with fresh ones.Special attention should be given to washing ofskin creases, around the ears and external auditorycanals, around the umbilicus and genitalia andunder the nails. Health care givers should takeprecautions while decontaminating, like wearingmasks with eye shields and water resistantgloves.
Treating OPC poisoned children is a greattask as they won’t cooperate for gut decontami-nation and copious ongoing vomiting alsointerferes with gut decontamination measures.Gut decontamination can be achieved by gastriclavage. If it is done within an hour, the maximumbenefit can be attained. 50-100ml of warm salinecan be used at a time and it should be repeatedtill the aspirate becomes clear.

Indian Journal of Practical Pediatrics 2009; 11(1) : 10
10
Activated charcoal is of limited valuebecause these highly lipid soluble agents arerapidly absorbed.
Antidotes
1. Atropine
Children with both OPC and carbamatepoisoning will be benefitted by atropine. Atropineantagonises the central and muscarinic cholinergiceffects and acts by blocking the muscarinicreceptors. It will not reverse the muscle weaknesscaused by the effect on nicotinic receptors.The dose of atropine is 0.05mg/kg IV every fiveminutes till the signs of atropinisation appearie. dryness of mouth, no bronchial secretions andno bradycardia. Miosis cannot be taken as a soleindicator of atropine need. The maintenancedoses can be repeated whenever it is warranted.After adequate atropinisation is established,maintenance doses are given to keeptracheobronchial tree dry for 24 hours. After thisatropine dose can be tapered gradually to preventrebound effects. One should be cautious in usingatropine in children with Down’s syndrome andin those with brain damage, as it may precipitatehyperactive response.
2. Glycopyrrolate
It is a quarternary ammonium compound.However, it does not cross blood brain barrier.So it will not alleviate the central effects of thepoison. Some investigators recommend this as analternative to atropine, since adverse effects areless.
3. Pralidoxime
It neutralises the nicotinic effects of OPC.Although there are controversies regardingbeneficial effects of pralidoxime in OPC poisoning,WHO recommends 25 to 50mg/kg in normal salineover 30 minutes followed by 10 to 20mg/kg/hr.Even though there are no randomized controlled
trials for the duration of continuous infusion inchildren, in adults it has been given for maximumof seven days. Because diethyl-OP–inhibitedAChEs reactivate and age notably slower thanthe dimethyl analogs, they generally requireprolonged oxime treatment. CNS effects andmuscarinic effects do not respond to pralidoxime,hence atropine therapy needs to be continuedalong with this.
Pralidoxime exerts nucleophilic attack on thephosphorus and a phosphoryloxime is formed,leaving the regenerated enzyme. However, highdose of pralidoxime themselves can causeneuromuscular blockade and inhibition of AChE.The side effects are mild weakness, blurred vision,diplopia, dizziness, headache, nausea andtachycardia if given more than 500mg/minute.Pralidoxime is generally not indicated forcarbamate poisoning.
4. Newer therapeutic agents
Various trials are being conducted toincrease the acetylcholinesterase levels by usingForskolin (cAMP inducer), transcriptionalinducers and Trichostatin (histone acetylaseinhibitor). Other therapeutic agents such assodium bicarbonate infusion, magnesium, clonidineand fluoride have been suggested to have a rolein OP poisoning but their use is not universallyrecommended due to a lack of good clinicalevidence.11
Supportive measures
1. Benzodiazepines: The seizures can be treatedsuccessfully with anyone of the benzo diazepines.Phenytoin has to be avoided as it may precipitatecardiac arrhythmias. Diazepam can be used inall patients showing aggressiveness as it relievesthe anxiety and counteracts the cholinergiceffects on CNS.
2. Respiratory support: Respiratory failure isone of the important complications in delayed

2009; 11(1) : 11
11
presentation. Children with respiratorycompromise have to be dealt with intubation andmechanical ventilation. Frequent suctioning shouldbe done as the secretions block the airway.
3. Other modalities: Fresh frozen plasma hasalso been tried with fruitful outcome in some ofthe studies, but adequate clinical trials should beconducted before putting them into the guidelines.
Drugs to be avoided are12 : Methyl xanthines whichantagonises PAM, aminoglycosides which canaggravate muscle weakness and drugsmetabolized by plasmacholinesterase like opioids,succinylcholine, mivacurium and esmolol. Avoidphenytoin for controlling seizures as its effect onNa+ channel may suppress cardiac activity andphysiologic autonomic response. Haloperidolshould be avoided for sedating the agitatedpatients due to atropine toxicity as it is non-sedating, but also associated with disturbance ofcentral thermoregulation, prolongation ofQT interval and pro-convulsant.
Prevention
Pediatricians should work for primaryprevention of poisoning, not only from their officesbut also in the community, by supporting effortsat educating parents about properly storing anddisposing toxic substances. The farmers who havecome from the field should not carry the childrenwithout washing their body and changing theclothes.
Community education in the rural areaswhere small or large-scale farming is practicedis very important.15 Prevention is better than cure.
Prehospital care
As in most poisoning situations, it is best to“scoop and run;” very little can be done in thefield. Always look for a container so that thespecific product can be determined. Deconta-
mination may be necessary for situations in whichpatients and their garments may be contaminatedwith the pesticide.
RODENTICIDE POISONING10,11,13,14
Rodenticides are not leading agents forsevere poisoning. Children obtain the rodenticidefrom the site at which it had been laid, as in thekitchen, lounge room or laundry, inside cupboardsor wardrobes. Rodenticides are used in two formsto kill rodents and they are single dose or multipledose type.
Ingredients
The components of rodenticide are usuallyaluminum phosphide, zinc phosphide, arsenic,thallium, barium compounds, warfarins and superwarfarins group. Super warfarins includebromadiolone, brodifacoum, difenacoum anddiaphacinone. Among them commonly used onesare warfarin group.
Pathophysiology
The anticoagulant effects of warfarins aresecondary to inhibition of vitamin K 2,3-epoxidereductase and vitamin K quinone reductase.The inhibition of these enzymes prevents theactivation of vitamin K and subsequent activationof clotting factors II, VII, IX, and X.Superwarfarins are more potent than warfarinsand have a longer duration of action. Prolongationof prothrombin time can be demonstrated after36-48 hours and may persist for long periods.
The phosphide groups can release phosphinegas which is lethal. So the gaseous nature ofphosphine poses a potential risk to healthcareproviders doing gastric decontamination; this factshould be borne in mind while undertaking theactivity. Even ‘offgassing’ in a patient’s exhaledbreath may lead to contamination of healthcarestaff.

Indian Journal of Practical Pediatrics 2009; 11(1) : 12
12
Clinical features
The phosphide groups can release phosgenegas which is lethal. The symptoms may vary fromchest pain, hypotension, vomiting tounconsciousness. Finally, they may develop liverand kidney failure. Reversible myocardial injurydue to aluminium phosphide poisoning has beenreported. Thallium causes GI disturbances,seizures and confused behavior, strangemovements of arms and legs and kidney damage.
Warfarin like substances disturb coagulationcascade causing various bleeding manifestationslike hematuria, hemoptysis and bleeding gums.A careful search should be done for petechialhemorrhages, and occult blood in the stools.Rarely, the patients may present withintracerebral bleeding and hemarthrosis.
Poisoning dosage
It varies from compound to compound.As the concentration of these substances are verylow in rodenticide, severe toxicity is rare.
Investigations
Prothrombin time at the time of admissionand 48 to 72 hours after the poisoning helpsto assess the coagulation status. Partialthromboplastin time, bleeding time and clottingtime are also helpful. Liver function and renalfunction tests help to assess the organ status.ECG may be taken to find out myocardial damage(various ST, T wave changes). Complete bloodcount is needed for evaluation of bleedingtendency. Plain x-ray of abdomen may be helpfulto detect metal rodenticide because these metalsare radio-opaque. The silver nitrate test on thegastric analysate is used for diagnosis ofaluminum phosphide poisoning. Also a variant ofthe gastric test is the breath test.
Management
Like any other poisoning, priority is given for“ABC” and decontamination techniques including
gastric lavage with activated charcoal. Routinecleansing with mild soap and water for dermalexposures is warranted.
Patients with unintentional ingestion and whoare asymptomatic should be evaluated accordingto the nature of the compound and observed ifrequired for 48 to 72 hours after exposure.
In an emergency room, in addition to abovesaid procedures, the pediatrician or practitionershould administer specific antidotes for a knowncompound. Otherwise, it is routine to administerVit.K in all rodenticide poisoning if the victim hasbleeding tendencies or prolonged prothrombintime. Fresh frozen plasma(FFP) could save thelife.
Specific antidote for thallium is potassiumferricyano ferrate (Prussian blue). It isadministered as 250mg/kg/day in four divideddoses until the concentration of thallium in theurine is less than 0.5mg over 24 hour period.
Aluminum phosphide poisoning requires onlysupportive measures as there is no specificantidote11. However absorption of poison from thegut is reduced by gastric decontamination usingpotassium permanganate in 1:10000 dilution forgastric lavage. Shock should be managed byinfusing a large amount of saline. Magnesiumsulphate has been shown to stabilize cellmembranes and reduce the incidence ofarrhythmias. N-acetylcysteine and magnesiumhave been suggested as potential therapies forthe management of poisoning but no effectivetreatment has been found. Coconut oil has beenreported to prevent rapid absorption of unabsorbedphosphine from the gut, but the strength ofevidence is at best weak.
Conclusion
Treating doctors and health care workers arereminded of the following golden rules. whiletreating poison cases.

2009; 11(1) : 13
13
1. Many cases of poisoning will recoverwith simple supportive measures and hence allof them do not require tertiary care.
2. Alleviate anxiety of the patient and thefamily members. Encourage the familymember(s) / friend(s) or accompanyingattendants to bring the remaining materials ofthe poison consumed / tablet taken and any othernote left by the patient for identification ofthe poisonous agent(s) in order to decide onappropriate antidote(s).
3. Preserve the first gastric lavage and thematerials brought by the patient or care giversfor chemical analysis.
4. Never be carried away just because vitalsigns are stable at the time of presentation, sincethe toxic manifestations may appear later.
5. Assess the condition of the patientfrequently.
6. It is ideal to observe the patients for24 to 48 hours before discharge.
7. Each patient with poisoning is differentfrom others.
8. Stabilise immediate life threateningproblems. “ABC’ Airway, Breathing andCirculation”.
9. Identifying the causative agent should notdelay the emergency treatment based on clinicalsigns.
10.Medical management of poisoning isdifficult at times in view of various biologicalfactors and chemicals consumed.
11. Some times patients will die no matterhow well managed.
12. Inform police if death occurs, and thebody should be sent for postmortem examination.
Points to Remember
• Early recognition, careful resuscitation,appropriate use of antidotes, closemonitoring and good supportive careshould minimise the morbidity andmortality in organophosphate andcarbamate poisoning.
References
1. Ganapathy N.Organophosphorous compoundpoisoning- a review. Indian J Trauma AnaesthCrit Care 2005; 6 : 432-447.
2. Rexy J, Ramakrishnan TV, Janardhan V.Surveillance and compendium preparation forcommon agricultural poison. Indian J TraumaAnaesth Crit Care 2002;3 :157-166
3. Lifshitz M, Shahak E, Sofer S. Carbamate andorganophosphate poisoning in youngchildren. Pediatr Emerg Care 1999;15: 102-103.
4. Singh S, Sharma N. Neurological syndromesfollowing organophosphate poisoning. NeurolIndia 2000;48:308-313.
5. Eddleston M, Mohamed F, Davies JOJ, et al.Respiratory failure in acute organophosphorouspesticide self-poisoning. Q J Med 2006;99:513-522.
6. Dalvi CP, Abraham PP, Iyer SS. Correlation ofelectrocardiographic changes with prognosisin organophosphorus poisoning. J PostgradMed 1986;32:115-119.
7. Makhaeva GF, Sigolaeva LV, Zhuravleva LV,et al. Biosensor detection of neuropathy targetesterase in whole blood as a biomarker ofexposure to neuropathic organophosphoruscompounds. J Toxicol Environ Health A 2003;66 :599-610.
8. Eddleston M, Dawsaon A, Karalliedde L, et al.Early management after poisoning with anorganophosphorous or carbamate pesticide -a treatment protocol for junior doctors. CritCare 2004;8 : R391-R396.

Indian Journal of Practical Pediatrics 2009; 11(1) : 14
14
9. Pillai VV. Organophosphate/carbamatepesticide poisoning – a primer for physicians.The proceedings of Toxocons-3 Mangalore,7 & 8 April 2007 & International referencesources. 2007;1-29.
10. Pillai VV. (Ed) Modern Toxicology. 3rd edn,
Jaypee Brothers Medical Publication (P) Ltd,New Delhi 2005; pp66-69.
11. Goel A, Aggarwal P. Pesticide poisioning.National Medical India 2007; 20 : 182 -191.
12. Shivakumar S. Principles of management oforganophosphorus compound poisoning.(Personal communication).
13. Basic Emergency services for poisoning.Training module for staff nurse and auxillarynurse midwife. State Health Mission, Healthand Family Welfare, Government of TamilNadu,Chennai. 2007.
14. Henry J, Wiseman H (Eds). Management ofPoisoning: a hand book for heaalth care workers.First Edition: World Health OrganisationGeneva, Switzerland, Europe. A.I.T.S. Publishersand distributors (Regd), Delhi , 2002.
15. Safer Access to Pesticides CommunityInterventions. World Health Organisation,Geneva, Switzerland. 2006.
CLIPPINGS
Continuous distending pressure for respiratory distress in preterm infants
Some benefits found in using continuous distending pressure (CDP) for respiratory distresssyndrome in preterm babies. Respiratory distress syndrome (RDS) is the most common causeof disease and death in babies born before 34 weeks gestation. Intermittent positive pressureventilation (IPPV) is the standard way of helping these babies breathe. A simpler method ofassisting breathing is to provide a continuous lung distending pressure - either no continuouspositive pressure to the airway or continuous negative pressure (partial vacuum). The reviewof trials found that continuous distending pressure (CDP) reduces the rate of death or the needfor assisted ventilation and reduced the need for IPPV. The small and mostly dated trials alsofound that CDP can increase the rate of pneumothorax (air outside the lung in the chest cavity).In preterm infants with respiratory distress the application of CDP either as CPAP or CNP isassociated with reduced respiratory failure and reduced mortality. CDP is associated with anincreased rate of pneumothorax. Four out of six of these trials were done in the 1970’s. Therefore,the applicability of these results to current practice is difficult to assess. Where resources arelimited, such as in developing countries, CPAP for RDS may have a clinical role. Furtherresearch is required to determine the best mode of administration and the role of CDP inmodern intensive care settings
Ho JJ, Subramaniam P, Henderson-Smart DJ, Davis PG. Continuous distendingpressure for respiratory distress in preterm infants. Cochrane Database of SystematicReviews 2002, Issue 2. Art. No.: CD002271. DOI: 10.1002/14651858.CD002271. Thisversion first published online: July 24. 2000 Last assessed as up-to-date: May 24.2008.

2009; 11(1) : 15
15
TOXICOLOGY
HYDROCARBON AND RELATEDCOMPOUNDS POISONING
* Utpal Kant Singh ** Prasad R *** Gaurav A
Abstract : In Indian children hydrocarbon(kerosene) is the commonest poison consumed.The clinical manifestations depend on theviscosity and amount of hydrocarbonconsumed. Pulmonary toxicity represents themost common complication of hydrocarboningestion and accounts for the majority offatalities. Management is principallyconservative but few children requiremechanical ventilation.
Key points: Hydrocarbon, Kerosene, Viscosityand Pneumonia.
Poisoning in children is the twelfth mostcommon cause of admission to the pediatricward.1,2 It constitutes 0.23 to 3.3% of totalpoisoning cases and the case fatality rates rangefrom 0.64 to 11.6%.3 Accidental poisoningcommonly involves children below 5 years of ageand hydrocarbon(kerosene) is the commonestorally consumed poison in Indian children.4,5
This is not surprising in view of the fact thathydrocarbon-based products are commonly foundin home. Children have access to kerosene during
winter months and charcoal lighter fluid insummer season. Often, the products areinappropriately stored in drinking glasses, waterbottles or unlabeled containers, and they may beattractive and pleasant-smelling, like furniturepolishes.
Hydrocarbons represent a diverse group ofsubstances and occasionally the terms“hydrocarbon” and “petroleum distillate” are usedinterchangeably. In fact, petroleum distillate refersto a type of hydrocarbon which results from theprocessing of crude oil and may be aliphatic oraromatic. Turpentine, on the other hand, is ahydrocarbon that is not a petroleum distillate sinceit is made from pine oil. The most useful meansof classifying hydrocarbons is with respect to theirclinical effects and are mentioned below.
Classification of hydrocarbons
A. Based on their chemical and clinicalproperties
1. Aliphatic hydrocarbons(easily aspiratedfollowing ingestion, poorly absorbed from GI tractand minimal systemic effects): kerosene, mineralspirits, gasoline, naphtha and mineral oil, lubricatingoil, etc.
2. Halogenated hydrocarbons(minimalaspiration following ingestion, readily absorbedfrom GI tract and produces systemic toxicity):trichloroethane, methylene bromide, chlordane,lindane.
3. Aromatic hydrocarbons(commonly usedfor inhalation): toluene, xylene and benzene
* Prof. and Head, Dept. of Pediatrics,Nalanda Medical College, Patna
** Lecturer, Institute of Medical Sciences,BHU, Varanasi
*** Senior Resident, JIPMER, Pondicherry.

Indian Journal of Practical Pediatrics 2009; 11(1) : 16
16
B. Based on viscosity
Hydrocarbons are classsified as very low,low, middle and high viscosity hydrocarbons(Table 1).
Halogenated hydrocarbons, such as thesolvent trichloroethane and methylene chloride,can produce liver and renal toxicity followingchronic exposure, as well as central nervoussystem (CNS) effects with acute exposure.Toluene, xylene, and benzene belong to the cyclic,aromatic group of hydrocarbons. The solventstoluene and xylene are commonly abused for theeuphoric effects produced by inhalation through“huffing” or “bagging.” Cardiac arrhythmias mayoccur due to sensitization of the heart tocatecholamines. Chronic exposure can causeperipheral neuropathies, electrolyte abnormalitiesand renal toxicity. Chronic exposure to benzenehas been implicated in the development of aplasticanemia and leukemia.2 Hydrocarbons may alsobe used as vehicles for highly toxic ingredientssuch as camphor, heavy metals andorganophosphate insecticides.
Pathophysiology of hydrocarbonpoisoning
The physical properties of the hydrocarbonscontribute to their ability to produce pulmonary
manifestations. The risk for aspiration is directlycorrelated with viscosity, which is measured inSaybolt Seconds Universal (SSU), the timerequired for a liquid to flow through a calibratedorifice. Products with a low viscosity (less than60 SSU) are associated with a high aspirationpotential e.g. gasoline, kerosene naphtha.In conjunction with decreased viscosity, thephysical properties of low surface tension andhigh volatility contribute to respiratory injury.Low surface tension enhances spreading of theliquid on lung tissue, while high volatility displacesalveolar gas and interferes with ventilation whenaspiration has occurred. Aspiration of mineral sealoil, with a viscosity of 47 SSU, can result in severepulmonary complications. This may in part beattributable to the ability of mineral seal oil tocause a lipoid pneumonia in addition to chemicalpneumonitis.4Hydrocarbons with a viscosity ofmore than 100 SSU, such as fuel oil, lubricatingoil and mineral oil, present a low aspiration hazard.
Pulmonary toxicity5,6 is the result ofhydrocarbon aspiration. The lower the viscosityand higher the volatility, the greater is the risk ofpulmonary aspiration. The hydrophobic nature ofhydrocarbons allows them to penetrate deep intothe tracheobronchial tree, producing inflammation.Bronchiolar exudates containing primarily
Table 1. Classification of hydrocarbons based on viscosity.
Viscosity Example
1. Very low Mineral seal oil (furniture polish)
2. Low Benzene, toluene, aniline, nitrobenzenepine oil, camphor, chlorinatedhydrocarbons, pesticides with hydrocarbon
3. Middle Gasoline, kerosene, lighter oil
4. High Lubricating greases and oils,motor oil, petroleum jelly, paraffin wax .

2009; 11(1) : 17
17
polymorphonuclear leukocytes may be foundwithin hours of aspiration. This may clinicallymanifest as bronchospasm, cough, rales andradiographic changes. Another postulatedmechanism of pulmonary damage is the loss ofsurfactant with resultant increase in alveolarsurface tension. The volatile chemical maydisplace alveolar oxygen, leading to hypoxia.Direct contact with alveolar membranes may leadto hemorrhage, hyperemia, edema, surfactantinactivation, leukocyte infiltration and vascularthrombosis. The result is poor oxygen exchange,atelectasis and pneumonitis. Pneumatocelesfollowing hydrocarbon ingestion generally occurin the areas of lung, where densest infiltrates areseen. The two postulated mechanisms forpneumatocele formation are necrosis ofpulmonary tissue and/or local obstruction leadingto over distension and rupture of alveoli. Clinicalmanifestations generally begin in the first fewhours after exposure and usually resolve in2-8 days. Complications include hypoxia,barotrauma due to mechanical ventilation andacute respiratory distress syndrome (ARDS).Prolonged hypoxia may result in encephalopathy,seizures and death.
Hydrocarbon ingestion causesgastrointestinal irritation and manifests with throatand abdominal pain, nausea and vomiting. Vomitingincreases the likelihood of pulmonary aspiration.
Hydrocarbon toxicity produces various CNSeffects, which include disinhibition, depression andeuphoria initially as observed in patients withalcohol or narcotic intoxication. Eventually,lethargy, headache, obtundation and coma mayfollow. Seizures are uncommon and are due tohypoxia. The CNS depression is related toanesthetic property of certain hydrocarbons andother CNS manifestations are secondary tohypoxia.7
Dysrhythmias are a major concern.The causes of dysrhythmias include hypoxia,
acidosis, the presence of toxic substances inhydrocarbon base, myocardial sensitization tocatecholamine and direct myocardial damage.Sudden death has been reported as a result ofcoronary vasospasm due to hydrocarboninhalation.
Hydrocarbons are reported to cause bonemarrow toxicity and hemolysis. Chlorinatedhydrocarbon toxicity may cause hepatic and renalfailure and toluene toxicity may lead to renaltubular acidosis. Direct contact with the skin andmucous membranes may cause effects rangingfrom local irritation to extensive chemical burns.
Clinical manifestations
Clinical manifestations of hydrocarboningestion, in the absence of toxic substituents, areconfined to the gastrointestinal tract and therespiratory tract. Local effects include a burningsensation in the mouth and pharynx, nausea,gastric irritation, belching, abdominal pain anddiarrhea. These rarely require treatment and areconsidered fairly innocuous.2-6 Pulmonary effects,when they do occur, are the result of aspiration.A severe necrotizing pneumonitis, with directtissue destruction, can occur. Aspiration can occurat the time of ingestion or during vomiting orgastric lavage. Pulmonary toxicity represents themost common complication of hydrocarboningestion and accounts for the majority offatalities. When aspiration occurs, the patient mayinitially experience coughing, choking, gagging orgrunting respirations. Dyspnea and cyanosis mayoccur. Rales, rhonchi and decreased breathsounds may be present on auscultation. Fever andleukocytosis may also be present but are notthought to correlate with an infectious process.2,3
This usually subsides after 24-48 hours.The breath, vomitus and urine have peculiar odor.Hydrocarbons may also result in lethargy, tremorsand rarely, convulsions or coma. The pupils arefirst constricted but become dilated later whencoma supervenes. These effects are more likely

Indian Journal of Practical Pediatrics 2009; 11(1) : 18
18
due to severe pulmonary injury or hypoxia. Salientclinical manifestations of hydrocarbon arementioned in Table 2.
On the basis of clinical manifestations,Gupta, et al8 devised a scoring system to determineoutcome and severity of hydrocarbon (kerosene)poisoning. They have taken account of fourparameters and scored as in Table 3.
Table 3. Scoring system for hydro-carbon poisoning
Parameter Absent Present Others
Fever 0 1 -
Severe 0 1 -malnutrition
Respiratory 0 2 4 (presencedistress of cyanosis)
Neurological 0 2 4 (presencesymptoms of convulsion)
The score may range from 0 to 10 in aparticular patient. If score is 4 or more; significantrisk and patients should be treated in a hospitalwith facility for advanced life support. Childrenwith a score of 7 or less are likely to survive,whereas with a score 8 or more the risk of death
is several fold higher. The predictive value of thisscoring system is about 85%.
Admission criteria9 followinghydrocarbon ingestion
1. Admit immediately, if the patient hassignificant respiratory symptoms or an abnormalchest radiograph.
2. Admit, if patient has significantCNS depression, severe gastrointestinalsymptoms or has ingested a significant amountof hydrocarbon.
3. Admit after observation if respiratorysymptoms are worsening or if the chestradiograph is becoming progressively worse.
Imaging studies
A chest radiograph must be obtained in allsymptomatic patients. Initially, the chestradiographic results may be normal, but findingsare usually significant at two to eight hours afteringestion. Common findings include fine perihilaropacities, bibasilar infiltrates and atelectasis.Following aspiration, deterioration of the patientmay occur over the first 24-72 hours, withresolution of symptoms in three to six days.3,5
The course may be prolonged with mineral sealoil exposure.2 Reported radiographic
Table 2. Clinical manifestations of hydrocarbon and related compounds
Respiratory Coughing, choking, tachypnea, grunting, cyanosis, rales, wheezing
Gastrointestinal Nausea ,vomiting ,abdominal pain, diarrhea and rarely bleeding
Cardiac Arrhythmia, congestive heart failure
CNS Headache , dizziness ,lethargy, ataxia, seizures, coma
Cutaneous Mucosal irritation, chemical burns
Miscellaneous Renal and hepatic damage, leukocytosis

2009; 11(1) : 19
19
complications of hydrocarbon aspiration includepneumatoceles, pleural effusion, empyema andpneumothorax.10 Repeat CXR is recommendedif acute change in the patient’s respiratory statusoccurs because of pneumothorax orpneumomediastinum. If discharge is beingconsidered for an asymptomatic patient, a chestradiograph should be done 6 hours after theingestion to document the negative findings.
ABG analysis is useful in documentinghypoxemia in severely affected patients.Hypercarbia may be observed in patients withrespiratory depression and decreased gasexchange. An increased anion gap may indicateco-ingestion of another toxin.
Pulse oximetry is useful in the emergencyroom because hypoxia is a direct result ofhydrocarbon aspiration. ECG should be done ifcardiac arrhythmia is a concern.
Management
Stabilization of the airway is always the firstpriority of treatment. Supplemental oxygen shouldbe given to all patients with face mask or oxygenhood and monitored on the bedside with pulseoximeter. Early intubation, mechanical ventilationand use of positive end-expiratory pressure maybe indicated in a patient in whom oxygenation isinadequate or who has severe respiratory distressor a decreased level of consciousness. A trial ofbronchodilators may prove useful in patients withsuspected bronchospasm.
The skin is decontaminated as soon aspossible by removing the involved clothing andthoroughly washing the skin with soap and water.Vapor inhalation and cutaneous absorption mayoccur long after the exposure. Regardless of theamount involved, gastric emptying is not indicatedfor accidental ingestion of a hydrocarbon lackingsystemic toxicity. This represents the majority ofcases. The risk of aspiration during vomiting or
lavage far outweighs any benefit from removalof the substance. The frequently cited amount ofmore than 1ml/kg as the indication for gastricemptying is not supported by animal studies.1,2,4
In the case of ingestion of a hydrocarboncapable of causing systemic toxicity or whencoingestion is suspected, gastrointestinal (GI)decontamination would be warranted of toxichydrocarbons i.e. camphorated, halogenated,aromatic, hydro carbon, co-injestion of heavymetals and pesticides. Gastric emptying is notwithout risk. Both ipecac-induced emesis andemesis from insertion of a lavage tube canincrease the risk of aspiration. In addition,aspiration may occur as the result of re-exposureof the larynx to hydrocarbon from the tip ofthe tube during removal. A cuffed endotrachealtube is not protective against aspiration.2
GI decontamination should be done providedthe patient has a gag reflex, is alert, and is likelyto remain so, and provided the substance is notexpected to cause seizures.2,10
Activated charcoal does not effectivelyadsorb hydrocarbons and in the absence ofco-ingestants, has no role in therapy. Oils, suchas mineral or olive oil, once advocated to increasethe viscosity of the hydrocarbon, are no longerrecommended because of the risk for lipoidpneumonia.8
If hydrocarbon aspiration occurs, oxygen andaggressive respiratory support are indicated.With severe pulmonary complications, CPAP orPEEP may be required. Steroids have not beenshown to be useful, and antibiotics should bereserved for documented infection. Antibioticsshould only be used, when there are signs ofpneumonia, in debilitated children and if there aresigns of acute infection. Routine prophylaxis withantibiotics is not necessary. A β2 selective agonistcan be given for bronchospasm, while epinephrineshould be avoided as it may precipitatedysrhythmias.

Indian Journal of Practical Pediatrics 2009; 11(1) : 20
20
Complications
Aspiration pneumonitis is the most commoncomplication of hydrocarbon ingestion, followedby CNS and cardiovascular complications.The major respiratory complications are aspirationand lung injury secondary to pneumonitis.Pneumothorax and barotrauma are potentialcomplications of mechanical ventilation.Most patients improve after 24 hoursand symptoms resolve within one week.CNS complications include seizures,encephalopathy and memory loss. These sequelaeare usually believed to be secondary to a hypoxicinsult. Myocarditis and cardiomyopathy arereported cardiovascular complications ofhydrocarbon toxicity. Cardiomyopathy, cerebellaratrophy, dementia, cognitive deficits and peripheralneuropathy have been reported with long-termhydrocarbon inhalant abuse. Sudden death mayoccur as a result of coronary vasospasm due tohydrocarbon inhalation.11
Prevention
Patient education is crucial in the preventionof accidental exposure. Parents should teachyoung children about the dangers of poisons,beginning at an early age. Advise the parentsabout the proper storage and labeling of harmfulchemicals. Parents should be informed aboutcommon household products that may bedangerous and recommend steps that they cantake to minimize the possibility of an accidentalexposure including safe storage of hydrocarbon.Educate parents about supervision of theirchildren, when they are in high-risk areas(eg, kitchen, garage, laundry room) where toxicsubstances may be present. Inhalant abuse occursin adolescents and should be discouraged.Hydrocarbons may be inhaled for recreation andas part of suicidal gestures and attempts.Treatment of the underlying causes ofthese behaviors might help in preventinghydrocarbon use.
Points to Remember
• Inducing emesis, gastric lavage andactivated charcoal are not indicated inmost hydrocarbon ingestion.
• If children remains asymptomatic evensix hours after ingestion, they can bedischarged.
• If symptomatic, do chest x-ray andmeasure oxygen saturation. Administeroxygen to maintain saturation >94%.
• If stable but symptomatic, admit ingeneral medical ward.
• If there is increasing O2 requirement,worsening respiratory distress or alteredlevel of consciousness admit in I.C.U. andconsider ventilatory support.
References
1. Datta AK, Seth A, Goyal PK, et al. Poisoning inchildren: Indian scenario. Indian J Pediatr 1998;65: 365-370.
2. Litovitz TL, Schmitz BF, Holm KC. 1988 annualreport of the American Association of PoisonControl Centers National Data CollectionSystem. Am J Emerg Med 1989 ;7:495-545.
3. Litovitz T. Hydrocarbon ingestions.Entechnology 1983; 62:142-147.
4. Arena JM. Hydrocarbon poisoning—currentmanagement. Pediatr Ann 1987;16:879-883.
5. Dice WH, Ward G, Kelley J, Kilpatrick WR.Pulmonary toxicity following gastrointestinalingestion of kerosene. Ann Emerg Med 1982;11:138-142.
6. Eade NR, Taussig LM, Marks MI. Hydrocarbonpneumonitis. Pediatrics. 1974;54: 351- 357.
7. Karlson KH Jr. Hydrocarbon poisoning inchildren. South Med J 1982;75(7):839-840.
8. Gupta P, Singh RP, Murali MV, Bhargava SK,Sharma P. Kerosene poisoning-a childhoodmenace. Indian Pediatrics 1992; 29: 979-984.

2009; 11(1) : 21
21
9. Anas N, Namasonthi V, Ginsburg CM. Criteriafor hospitalizing children who have ingestedproducts containing hydrocarbons. JAMA1981;246:840-843.
10. Khan, Awais J , Akhtar, Raja P, Faruqui, Zia S.Turpentine Oil Inhalation Leading to Lung
Necrosis and Empyema in a Toddler. PediatricEmergency Care. 2006;22:355-357.
11. Beamon RF, Siegel CJ, Landers G, Green V.Hydrocarbon ingestion in children: a six-yearretrospective study. JACEP 1976;5:771-775.
CLIPPINGS
Methods of milk expression for lactating womenThe World Health Organization recommends that infants be fed exclusively on human milk from
birth to six months of age. Children who do not receive human milk are more likely to suffer healthproblems. Not all babies are able to feed at the breast because of prematurity, illness, abnormalities orseparation from their mothers; these babies need expressed human milk. Mothers may also expressmilk for their own comfort if they have sore nipples or engorgement; to increase milk supply; or toleave milk if away from their baby. Possible adverse effects from expressing milk include injury to themother and bacterial contamination that may affect the baby. This review included 12 studies and six ofthese had data that could be used in the analyses. All the mothers in these six studies were mothers ofinfants in neonatal units in the USA, UK, Malaysia, Kenya and Nigeria. In one study, using the electricor foot-operated pump provided a greater mean volume of milk than hand expression during a six-dayperiod in the first two weeks after birth. Simultaneous pumping of both breasts and sequential pumpinggave similar volumes, though the time taken was different. In one study, mothers given a relaxationtape were more likely to produce a greater volume of milk at one expression. One small study foundthat hand-expressed and pump-expressed milk had a similar incidence of milk contamination. All studieswere small and results may not apply to pumps other than those tested. No study asked mothers if theyhad achieved their own goals for expressing milk. None of the studies examined costs involved withdifferent methods. Eight of the 10 studies that evaluated pumps or other products had support from themanufacturers. The available evidence indicates that low cost measures such as relaxation, breastmassage, frequency of expressing or pumping, and simultaneous pumping, if acceptable to mothers,may be effective in assisting mothers to provide expressed milk. Not all the studies mentioned if basicsupports were provided, particularly for mothers with hospitalised children, including access to foodand fluid, a place to rest near their baby, and knowledgeable health workers. Whatever method ofexpression is used, mothers need to feel valued and supported.Authors’ conclusions
Mothers appear to obtain greater total volumes of milk in six days after birth using the electric orfoot powered pump tested compared to hand expression, and a greater volume at one expressionduring the second week when provided with a relaxation tape. Simultaneous pumping takes less timecompared to sequential pumping. Further research with larger numbers and more comprehensivereporting is needed, and mothers’ reasons for expressing linked to their evaluation of effectivenessrather than market-led research on equipment performance.
Becker GE, McCormick FM, Renfrew MJ. Methods of milk expression for lactating women.Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD006170. DOI: 10.1002/14651858.CD006170.pub2. This version first published online: October 08. 2008
Indian Journal of Practical Pediatrics 2009; 11(1) : 22
22
COMMON DRUG POISONING
* Suresh Gupta
Abstract: Poisonings due to drug ingestionare becoming more frequent. Acetaminophenis the most commonly used antipyretic drug.When significant toxic dose is ingested,N-acetylcysteine is a specific antidote.Poisoning due to sedative-hypnotics canresult in cardiorespiratory depression.Good supportive care can save most of thepatients. Anticonvulsants can result in toxicitydue to overdose, idiosyncrasy or druginteractions. Ingestion of cardiovasculardrugs like antiarrhythmics and antihyper-tensives are relatively less common but thetoxicity can be associated with significantmorbidity and mortality. Iron ingestion isbecoming more common due to increasinguse of prenatal iron. Vomiting is the mostprominent clinical feature of iron toxicity.Older generation anti-histamines can producesubstantial toxicity due to anticholinergic andsedative effects. Most of the beta agonistingestions generate only insignificant clinicalproblems.
Key words: Poisoning, Acetaminophen,Sedative-Hypnotics, Antihypertensives,Antiarrhythmics, Iron, Antihistamines andβ agonists.
Poisoning is one of the common emergenciesin children presenting to emergency room.
Most of the poisoning in children are accidentaland trivial. But at times it can be life threateningparticularly in adolescents with suicidaltendencies. With urbanization, the types ofpoisoning are changing particularly in metropolitancities. With increasing use of prescription drugsin adults drug poisoning is becoming increasinglycommon in children. The commonly availabledrugs in households include antipyretic-analgesics(acetaminophen, non-steroidal anti-inflammatorydrugs), sedative-hypnotics (benzodiazepines,opioids, barbiturates, triclofos), anti-convulsants(older and newer anticonvulsants), hematinics(multivitamins and iron preparations),cardiovascular drugs (anti-arrhythmics and anti-hypertensives), anti-histaminics (older and neweranti-histaminics), anti-asthmatic drugs (salbutamol,theophylline). There is a huge list of drugs whichcan result in accidental ingestion and poisoningbut only accidental ingestion of common drugs inchildren will be discussed here.
ACETAMINOPHEN
Core facts and pathophysiology1
Acetaminophen (paracetamol, N-acetyl-para-aminophenol) is the most widely usedantipyretic and analgesic medication in children.The recommended therapeutic dose is10-15 mg/kg every 4 hours (max. 60 mg/kg/dayor 4 g/day). Peak plasma concentrations after asingle therapeutic dose occurs in 30 – 120 minutes,with therapeutic levels between 10–30 µg/mL.A level of 150 µg/mL at 4 hours after ingestion ishepatotoxic in 25% of cases. The toxic dose is140–150 mg/kg, although prepubertal childrenmay be less susceptible to acetaminophen toxicity
* ConsultantPediatric Emergency MedicineCenter for Child Health,Sir Ganga Ram Hospital, New Delhi
TOXICOLOGY

2009; 11(1) : 23
23
than adults due to a more active sulfationpathway; therefore, as much as 250 mg/kg in asingle acute ingestion may be needed to develophepatotoxicity.
Peak levels occur within 4 hours, even inlarge overdoses. Approximately 95% ofacetaminophen is metabolized by the liver tonon-toxic glucoronide and sulphate conjugates.Less than 5% is metabolized by the cytochromeP450 system to N-acetyl-parabenzo-quinone-imine (NAPQI), which is further conjugated byglutathione to non-toxic mercapturates.In overdose situations, glutathione is depleted, andthe excess NAPQI is toxic to hepatocytes, causingcentrilobular necrosis. Acetaminophen levelshould be obtained in the acute, single ingestionin the first 24 hours post-ingestion. The Rumack-
Matthew nomogram (Fig.1) predicts the risk ofliver damage for a single, acute ingestion ofacetaminophen. Serial levels may be helpfulwhen there is a) an unclear time course ofingestion, b) any chronicity to the ingestion, orc) ingestions involving extended release tablets.N-acetylcysteine (NAC) acts as a substitute forglutathione, and binds NAPQI, therefore blockinghepatocellular toxicity if initiated within 8–12 hoursof ingestion. It may be effective even in delayedpresentations greater than 24 hours. In this case,it is believed to work as an antioxidant andimproves hepatic microcirculation.
Clinical features
Acetaminophen toxicity is divided into fourstages2
Figure 1. The Rumack-Matthew Nomogram

Indian Journal of Practical Pediatrics 2009; 11(1) : 24
24
1. Stage 1 (0 – 24 hours): Asymptomaticor mild GI upset with anorexia, nausea, vomiting,malaise, pallor, and diaphoresis.
2. Stage 2 (24 – 48 hours): Resolution ofinitial GI symptoms with development of rightupper quadrant pain, jaundice, subclinicalelevation of transaminases and prothrombin time.
3. Stage 3 (72 – 96 hours): Peak liverdysfunction and possible multi-organ failure,hepatic encephalopathy and coagulopathy.
4. Stage 4 (days to weeks): Resolution ofliver abnormalities or progressive liver failure andoccasionally death.
Complications: Approximately 2 – 5% oftoxic ingestions (in adults and adolescents) go onto develop fulminant hepatic failure requiringtransplantation or resulting in death. Renal failureoccurs in about 25% of hepatotoxicity cases.Complications are very rare in prepubertalchildren due to altered metabolism and relativelysmaller quantities ingested.
Investigations
Aspartate aminotransferase and alanineaminotransferase levels (AST and ALT), bilirubin,and prothrombin time (PT) elevation indicates liverinflammation and injury. These can be helpfulin patients with ingestion of multiple doses orif the time course is unreliable. Baselineelectrolytes and glucose are recommended if theacetaminophen level is high enough to warranttreatment with NAC.
Blood Levels: The Rumack-Matthew nomogramis used to interpret blood levels of acetaminophen.Acetaminophen level should be done in the first24 hours for an estimated ingested dose of morethan150 mg/kg or if unknown. Serial acetamino-phen levels may help calculate the half-life toestimate the total amount ingested or pick up alate peak in an extended release preparation.
Management
Potentially toxic ingestions are defined as:1) a level above the “possible toxicity” nomogramline, 2) the ingestion that is complicated bymultiple doses, or 3) the time course is not defined.If reliable, a history of less than 150 mg/kg ofacetaminophen ingested in a single acute episodecan be managed at home.
Decontamination: GI decontamination is indicatedin the first 1 – 2 hours after potentially toxicingestions or 3 – 6 hours if there has beenco-ingestion of substances that delay gastricemptying, e.g., anticholinergics. Acetaminophenhas a high affinity for activated charcoal (AC).Early decontamination eliminates the need forgastric lavage and its potential complications.A single dose of AC 1g/kg orally or throughnasogastric tube is administered. Lavage isindicated for multiple drug ingestions. There isno role for enhanced elimination such ashemodialysis/hemoperfusion or forced diuresis.
Antidote therapy: N-acetylcysteine (NAC) isindicated in any potentially toxic ingestion or withevidence of hepatic injury (elevated AST/ALT,PT). NAC is most effective in the first24 hours post-ingestion, even if activated charcoalhas been given. NAC is administered orally orthrough nasogastric tube in 140 mg/kg initialloading dose, then 70 mg/kg q 4 hours for 18 totaldoses. One can use 10% - 20% NAC solution(10g or 20g/100ml) which is diluted to a5% solution with water, soda or juice to make itless noxious. If any dose is vomited within anhour it should be repeated in full. Emesis controlwith antiemetics like ondansetron or phenothiazineis often required to improve the tolerance.Intravenous NAC may also be considered inpatients with severe vomiting or ileus or with latepresentation of acetaminophen toxicity.3, 4, 5
Liver transplantation: Indications for a livertransplant include increasing PT on day 4,

2009; 11(1) : 25
25
pH <7.30, PT >100 seconds, creatinine>3.4 mg/dl or hepatic encephalopathy at any time.
Supportive: Supportive treatment is an integralpart of managing any child with poisoning.Rehydration and maintenance fluids are indicatedfor the severely vomiting and/or anorectic patient.Even non-toxic ingestions from a suicide attemptor gesture in adolescents should be admitted formental health evaluation and treatment.
SEDATIVES, HYPNOTICS
The common sedative-hypnotic agentsinclude barbiturates, benzodiazepines, chloralhydrate, opioids, carbromal, buspirone andglutethimide. In pediatric ingestions first four drugsare more commonly involved than others.
Core facts and pathophysiology
All the sedative-hypnotic drugs decreaseactivity, produce calmness and facilitate sleep.Agents include barbiturates, benzodiazepines,chloral hydrate, buspirone, ethchlorvynol,meprobamate, carbromal, methyprylon andglutethimide6,7. Opioid produces analgesia,euphoria and sedation. These agents producevariable degrees of CNS depression after acuteingestion. Some have direct toxic effects on otherorgans like the liver. A mixed ingestion with morethan one agent increases the toxicity and mortalityrisk. Chronic use of these agents may producetolerance to the sedative effects but not the toxiceffects. Toxic effects generally occur at10–15 times the therapeutic dose, althoughindividual variation is common.
Barbiturates: Inhibit neurotransmission atsynapses, causing generalized depression ofneuronal activity. Large doses producehypotension secondary to decreased centralsympathetic tone and direct depression ofmyocardial contractility. Barbiturates are dividedinto groups based on the duration of action.Shorter-acting barbiturates are highly lipid-soluble
and are more toxic than the long-actingcompounds. The significant renal excretion ofphenobarbital and its relatively low pKa are therationale for the use of forced alkaline diuresis.Trichloroethanol has a structure similar tohalothane, and may sensitize myocardium tocatecholamines and can lead to arrhythmias.Clinical features
Poisoning may either result from cumulativetoxicity of anticonvulsant medication(like phenobarbital) or due to accidental singledrug ingestions. Adolescents with suicidaltendencies may have poly-pharmacy ingestion.CNS Depression: All agents produce similarCNS depression. Onset of symptoms depends onthe drug and route of intoxication. Drowsiness isusually the first sign of intoxication. Paradoxicalexcitation occurs in some children. Mild tomoderate toxicity presents with slurred speech,nystagmus and ataxia. More severe toxicitypresents as stupor or coma and can progress torespiratory arrest, hypotension and cardio-vascular collapse from decreased myocardialcontractility and decreased sympatheticvasomotor tone. Patients in deep coma may haveabsent reflexes and hypothermia. Initially pupilsmay be small, but with deeper coma theymay become dilated and non-reactive.Mixed ingestions, especially ethanol, potentiateCNS depression and other toxic effects.
Bullous skin lesions may be seen in patientswith barbiturate, ethchlorvynol, meprobamate,glutethimide and benzodiazepine intoxication.Typically, the lesions are seen on the hands,buttocks or knees but may appear on other areasof the body.Opioid: Acute ingestion causes a triad of coma,pinpoint pupils and absent bowel sounds.Respiratory depression, bradycardia, hypotensionand depressed sensorium may also occur.Orthostatic hypotension may result fromsignificant histamine release. IV opiate abusers

Indian Journal of Practical Pediatrics 2009; 11(1) : 26
26
have needle tracks and are at risk for cutaneousabscesses, endocarditis, hepatitis, vasculitis,extreme constipation and HIV infection.
Benzodiazepines: Most obtunded patients can bearoused within 12 – 36 hours. Hypotension orhypothermia is rare. Respiratory depression isusually not significant with oral ingestion anddeaths are seen only in patients with combinedingestion.
Chloral hydrate: Acute poisoning producesstupor and coma about 30 minutes after ingestion.Skin and mucous membrane irritation can result.Nausea, vomiting and gastritis can occur whichcan become hemorrhagic and lead to perforation.Direct hepatic toxicity with jaundice is also seen.Cardiac dysrhythmias (atrial and ventricular) arecommon. Persistent ventricular dysrhythmias arecommon terminal events.
Complications of sedative - hypnotic ingestion:Death or hypoxic-ischemic injury may occur aftercardiopulmonary arrest. Dysrhythmias are seenwith meprobamate and chloral hydrate.Chloral hydrate can produce gastritis, esophagitisor intestinal perforation and esophageal stricture.Seizures are provoked by overdose of morphine,meperidine and propoxyphene. They are also seenin patients recovering from glutethimide andmethyprylon ingestion.
Investigations
Serum electrolytes, glucose, BUN and creatinine,are done to rule out metabolic causes of alteredmental status. Barbiturate levels do not correlatewith clinical status of patients, especially in thosewho are tolerant to the drug. Serum therapeuticrange of phenobarbital is 15 – 40 µg/mL.Levels in the range of 60 – 80 µg/mL are toxic.Diagnostically, serum phenobarbital levels arehelpful, as alkaline diuresis is a therapeutic option.Short-acting barbiturate with serum levels of>20–30 µg/mL are generally associated with
coma. Serial levels of other agents may be usefulin patients with clinical deterioration despiteaggressive therapy. Rising levels in these patientsmay indicate prolonged absorption from aconcretion. Abdominal x-rays may be useful todemonstrate radio-opaque pill fragments orsuspension in phenobarbital ingestion or chloralhydrate tablet ingestion. Atrial, ventricular, andconduction arrhythmias are seen in chloralhydrate or meprobamate ingestion. Evidence ofconcurrent tricyclic antidepressant overdoseincludes prolongation of the QRS complex,prolonged QT interval or torsades de pointes.
Management
Therapy is directed towards supporting vitalorgan functions and enhancing elimination ofingested medications.
Attend to ABCs: Intubation and/or assistedventilation may be required if protective reflexesare depressed. Myocardial depressant effects ofsingle or multiple-drug ingestion may causehypotension, arrhythmias or diminishedcontractility. IV fluids, inotropic agents orantiarrhythmics should be used as guided byprotocols.
Decontamination/Elimination: Consider gastriclavage if child is brought within 4 - 8 hours ofingestion. Intubation for airway protection maybe indicated, especially in glutethimide ingestion.Administer activated charcoal, 1 g/kg throughnasogastric tube or per oral route. Repeatcharcoal doses of 0.5 g/kg should be given every2 - 4 hours until the mental status improves.Hemodialysis or charcoal hemoperfusion toenhance elimination are indicated for extremelylarge ingestion of medication, failure to respondto aggressive supportive therapy or coma. Urinealkalinization is useful for phenobarbital poisoningbut not for other barbiturates. For urinealkalinization use sodium bicarbonate:

2009; 11(1) : 27
27
1–2 mEq/kg IV initially, then 50–100 mEq/L ofIV fluid to maintain a serum pH 7.45–7.50 andurine pH 7–8.
Antidote/Supportive therapy
1. Supportive therapy for hypotension andpoor cardiac output: Inotropic support of cardiacoutput and blood pressure may be required.Excessive fluids should be avoided to preventpulmonary edema.
2. Naloxone is a narcotic antagonist usedfor known or suspected opioid overdose.Dose: i) 0.01 mg/kg, im or iv repeated every3-10 minutes if no response occurs.
3. Flumazenil has been used to treat isolatedbenzodiazepine overdose8. Flumazenil is notindicated for comatose patients with an unknowningestion. It is not a substitute for basic emergencycare (ABCs), although in some patients it mayprevent the need for endotracheal intubation.It is given in dose of 0.01 mg/kg, IV over30 seconds and repeated as necessary every30 seconds to a maximum dose of 1 mg in children.As duration of action is 30 – 60 minutes, oneshould monitor for re-sedation. Flumazenil mayprecipitate: a) arrhythmias in patients with cyclicantidepressant or chloral hydrate ingestion,b) seizures in patients who were brought withseizures, twitching or a history of seizures,c) acute withdrawal, including seizures andautonomic instability, in patients tolerant tobenzodiazepines.
4. Propranolol or esmolol is useful fortreatment of ventricular arrhythmias in chloralhydrate and meprobamate ingestion. Standardantiarrhythmics are less effective.
5. In chloral hydrate intoxication, adequateglucose must be provided to preventhypoglycemia associated with liver injury.
6. Continuous cardiopulmonary and oxygensaturation monitoring are to be carried out for all
significant ingestions. Arrhythmias may developwith chloral hydrate and meprobamate. Frequentblood pressure determination is essentialespecially for meprobamate ingestion whereprofound hypotension may develop unexpectedly.
ANTICONVULSANTS
Phenobarbital, phenytoin, carbamazepine,valproic acid, felbamate, gabapentin andlamotrigine are the anticonvulsants commonlyused in both children and adults.
Core facts and pathophysiology9
Toxic manifestations of anticonvulsants canbe caused by accidental or intentional overdose,drug interactions, idiosyncratic reactions andhypersensitivity reactions. Consider co-ingestionsin all overdoses.
Phenobarbital: It is a CNS depressant (inhibitionof neurotransmitters) with a long half-life of morethan 48 hours. The half life may get extended inoverdose up to 7 days. Renal excretion is the mainroute for elimination.
Phenytoin: It is structurally related to barbituratesand has dose dependent kinetics with increasedhalf-life in overdose. The half-life is more than8 hours. Metabolism occurs mainly in the liver.
Carbamazepine: It is structurally related toantidepressants. Anticonvulsant properties arerelated to inhibition of sodium channels andinterference with noradrenaline and glutamatemetabolism. Oral absorption is slow and erraticand has a half life of 8 – 10 hours.
Valproic acid: It acts by increasing concentrationof GABA or inhibition of reuptake. The half-lifeis 6 – 16 hours with mainly hepatic metabolism.
Felbamate: It is a dicarbamate derivative. It actsas glycine antagonist and is partially metabolizedin liver or excreted unchanged in urine. It has ahalf-life of more than 20 hours. Felbamate hasbeen withdrawn by the FDA.

Indian Journal of Practical Pediatrics 2009; 11(1) : 28
28
Gabapentin and Vigabatrin: These are chemicalanalogues of GABA and inhibit GABA synapsesby irreversible binding. It is excreted unchangedin urine. Half-life is 5 – 7 hours.
Lamotrigine: Lamotrigine is unrelated to otheranticonvulsant drugs. It blocks sodium channels,limiting release of glutamate and aspartate, thusstabilizing neuronal membranes. It is metabolizedby the liver and has very long half-life of morethan 14 – 24 hours.
Clinical features
Toxic manifestations of phenobarbital,phenytoin, carbamazepine and valproic acid areas follows :-
• Neurotoxicity includes lethargy, nystagmus,ataxia, dystonia, dyskinesias, seizures andcoma. Respiratory depression and apnoeaas well as cardiotoxic effects such asarrhythmias and myocardial depression10,11
are also seen.
• Idiosyncratic reactions include liver failure,hematopoietic toxicity and hypersensitivityskin reactions such as erythema multiformeand Stevens-Johnson syndrome.
• Hypothermia and a vesicular rash occur withphenobarbital overdose.
• Anticholinergic effects (fever, dryness,agitation, flushing) occur with carbamazepineoverdose.
Phenytoin sodium settles in the bottle in thesuspension form. An unshaken bottle may givelow levels at the top and toxic levels at the bottom.
Newer anticonvulsants: (Felbamate, gabapentin,vigabatrin, lamotrigine)
• There are few reports of over dosage andthese drugs seem to have a high therapeuticindex. Somnolence, ataxia, nausea andvomiting can be expected with these newer
drugs and have been seen at therapeuticdoses12,13.
• Aplastic anemia, an idiosyncratic effect hasbeen reported in some patients receivingfelbamate and resulted in withdrawal offelbamate by the FDA. Stevens-Johnsonsyndrome has been reported with felbamateand lamotrigine but not with gabapentin orvigabatrin.
• A lamotrigine overdose may cause mildataxia and nystagmus. A slightly prolongedQRS may occur on EKG but no arrhythmiasare reported.
• Under or overdosage may cause statusepilepticus, especially if the patient is onanother medication which may affectmetabolism of the anticonvulsant.Co-ingestion of other CNS depressants,especially alcohol and benzodiazepinesexacerbate respiratory depression andsomnolence and increases morbidity andmortality of ingestions. Supportive careusually results in recovery in 24 – 48 hourswithout significant consequences in mostcases.
Investigations
ABG should be done if sedation or respiratorydepression is present. Gastric lavage should becautiously done with airway protection inthe presence of respiratory depression.Other investigations which needs to be doneinclude CBC, electrolytes, urinalysis, hepaticenzymes and CPK. Serial levels of ingestedanticonvulsants should be followed.
• Phenobarbital: Therapeutic levels range from15 to 40 µg/mL: Serum levels may notcorrelate with level of sedation, particularlyin those on long-term therapy, as tolerancedevelops. Sedation to coma is common above70 µg/mL level. Reversible “flat line” EEGmay be seen over 120 µg/mL.

2009; 11(1) : 29
29
• Phenytoin sodium: Therapeutic levels:10 – 20 µg/mL. Ataxia and nystagmus occurat >30 µg/mL.
• Carbamazepine: Therapeutic levels:4-12 µg/mL. Confusion, dizziness and ataxiaoccur at >14 µg/mL, while there are chancesof arrhythmias at >40 µg/mL.
• Valproic acid: Therapeutic levels:50–100 µg/mL.
Management
Decontamination: Gastric lavage is indicated forrecent ingestions. Lavage should be done untilreturns are clear and one must ensure protectionof airway during lavage. Single dose charcoal isindicated for all; multidose charcoal is effectivein phenobarbital, phenytoin and carbamazepineoverdoses. The first dose should be given in thedose 1g/kg NG or P.O. Repeat charcoal doses of0.5g/kg once in every 2-4 hours. Extracorporealelimination is useful for many anticonvulsants. Inphenobarbital, carbamazepine and valproateoverdose hemodialysis, hemo-perfusion andplasmapheresis can help to decrease serum druglevels. These measures are reserved for seriouslyill patients in whom supportive measures areinadequate. Urine alkalinization will enhancephenobarbital excretion. Hyperventilation mayachieve the same results in intubated patients.Naloxone may be effective in valproic acidoverdose.
Supportive treatment: Supportive care withsupplemental O2 should be done as necessary andairway protection/intubation may be necessaryin patients with CNS depression. Seizures shouldbe treated with benzodiazepines. Avoid the useof anticonvulsants suspected in overdose.Continuous cardiorespiratory and pulse oximetrymonitoring is necessary for any patient withCNS sedation, respiratory depression orarrhythmias. Rewarming and frequenttemperature checks should be done for barbiturate
ingestion. One should consider social serviceand psychiatric intervention for children withrepeated ingestions or teenagers with suicidalpsychopathology.
IRON
Core facts and pathophysiology14
Iron ingestion is one of the leading causesof non-intentional ingestion deaths in children. Ironis readily available to children and frequently hasa bright-colored sugar coating. Often it is not feltto be harmful by family members, and is used byexpectant mothers with other small children inthe household. The majority of toxic ingestionsoccur with prenatal vitamins (20% elemental iron)or iron-only preparations. Ingestion of more than20 mg/kg of elemental iron is toxic.Lethal ingestions occur with 180 – 300 mg/kg ofelemental iron. Normal excretion of iron is limitedto 1-2 mg/day from the GI tract, urine anddesquamated skin.
Iron toxicity occurs via two mechanisms
1. Direct caustic effects on thegastrointestinal mucosa: Mucosal ulceration alongthe stomach and proximal small bowel causesintramural hemorrhage and iron deposition.Segmental infarction occurs along the distal smallbowel and may present late as gastric outlet andsmall intestine strictures. The damage to themucosa allows bacterial invasion of the gut wall.
2. Iron also has a direct cytotoxic effect onseveral tissues and organs, principally the liver,heart and lungs. Iron can uncouple oxidativephosphorylation in the mitochondria and generateoxygen-free radicals. In acute oral ingestion, ironis absorbed in the duodenum and jejunum whereit is bound to transferrin. Once the total ironbinding capacity of transferrin is exceeded thepotential for toxicity exists. Free circulating ironcauses vasodilation, venous pooling and increased

Indian Journal of Practical Pediatrics 2009; 11(1) : 30
30
capillary permeability. This results in cellulardamage to both the liver and the myocardium alongwith metabolic acidosis and impaired glucosetolerance.
3. Toxicity of iron depends on the elementaliron ingested. The elemental iron varies frompreparation to preparation. (Table 1 and Table 2).Example: Ingestion of 20 tabs of 325 mg ferroussulfate in a 15 kg child = 20 X [325 X 0.2 mg] =1300 mg elemental Fe which is equal to87 mg/kg.
Clinical features
Vomiting is the most sensitive predictor ofserious iron ingestion. Absence of vomiting at6 hours means patient is unlikely to have ingesteda toxic amount. The classic clinical presentationhas four stages15:
1. First phase (0 – 6 hours): GI irritationincluding vomiting, (bloody) diarrhoea, nausea andabdominal pain. Severe ingestions may result infever, hyperglycaemia, hypotension, tachycardia,poor peripheral perfusion, metabolic acidosis,lethargy and coma.
2. Second phase (6 – 24 hours): Latentphase. This may or may not be present. Thepatient stabilizes during uptake of free iron bythe reticuloendothelial system.
3. Third phase (12 – 24 hours): Systemictoxicity. A minority of patients progress to thisstage. GI symptoms recur with profoundhypotension, acidosis and pulmonary hemorrhage,hepatic necrosis manifests as hypoglycemia andcoagulation defect, oliguria, seizures, lethargy andcoma. Sepsis with fever occurs because ofbacterial invasion of the gut wall.
4. Fourth phase (2 – 6 weeks): Latecomplications. Gastric or bowel obstructionoccurs secondary to progressive strictures fromgut injury at the time of ingestion.
Complications of severe iron intoxication include:
• Gastrointestinal: Bowel perforation withsubsequent peritonitis, stomach or smallbowel obstruction and hepatic/pancreaticnecrosis.
• Coagulopathy frequently occurs late in severeintoxication and is mostly due to liverdysfunction, but may also occur early due toiron’s effect on thrombin, independent ofhepatocellular dysfunction.
• Cardiopulmonary: Myocardial dysfunction ismostly due to hypovolemia and shock, but
Table 1. Iron composition ofcommon iron compounds
Iron compound Elemental Fe
Ferrous sulphate 20%Ferrous gluconate 12%Ferrous fumarate 33%Ferric phosphate 37%Ferric pyrophosphate 12%Ferroglycine sulfate 16%
Table 2. Toxicity of iron by bloodlevel
Serum Iron (mg/dL) Level of Toxicity
50 – 150 mg/dL Normal serum ironconcentration
<300 Non-toxic
300 – 500 Mild
500 – 1000 Moderate: Highlyassociated withtoxicity
>1000 Severe: Death ifuntreated

2009; 11(1) : 31
31
there is evidence that iron causes directmyocardial toxicity. Respiratory compromiseis due to physiologic derangements, but acuterespiratory distress syndrome (ARDS)frequently occurs late and is associatedwith high-dose deferoxamine treatment(15 mg/kg/day or more for more than24 hours.).
• CNS manifestations are usually associatedwith the presence of hypovolemia, metabolicacidosis and liver dysfunction.
Investigations
CBC, glucose, serum iron and TIBC maybe all that is necessary in an asymptomatic tomild intoxication or with an unknown quantity ofingestion. Total leucocyte count more than 15,000a serum glucose more than 150 mg/dL isconsidered a positive predictor of a serum ironmore than 300 mg/dl. Bicarbonate establishes theseverity of the metabolic acidosis. Coagulationstudies and liver function tests define the degreeof hepatic involvement.
Total Iron Binding Capacity (TIBC) varieswidely and currently has limited value in theevaluation of iron toxicity16. Emphasis should beplaced on the absolute serum Fe levels as serumiron levels are more important. A serum ironconcentration at 2 - 4 hours post-ingestion is thebest estimate of risk of toxicity. A level donegreater than 6 hours post-ingestionunder estimates the toxicity because of tissueaccumulation. Plain abdominal radiographobtained within 2 hours of ingestion maydemonstrate radiopaque material consistentwith iron. 60% of patients in one study with apositive radiograph had an iron concentration>300 mg/dL. Serial films may be used to assessthe efficacy of gastric decontamination. Absenceof opaque fragments does not eliminate thepossibility of toxicity.
Management
Ingestions of less than 20 mg/kg withoutsymptoms may not require ED treatment.Any patient who is symptomatic requiresevaluation in a health care facility.
Decontamination/Elimination: Gastric lavageshould be performed on patients where vomitinghas not occurred or where retained iron is visibleon abdominal radiograph or who exhibit signs ofincreasing toxicity. Pill fragments are usually largeso the largest orogastric tube possible should beutilized. Activated charcoal does not bind iron.Whole bowel irrigation is contraindicated withsevere GI haemorrhage or perforation.Hemodialysis is not effective for free iron.Exchange transfusion increases the removal rate30-fold compared to deferoxamine alone.
Antidote/Specific Therapy: Deferoxamine is aniron chelating agent17. Treatment is based onsymptoms and the serum iron level:
• Serum iron levels less than 300 mg/dLusually do not warrant therapy.
• A symptomatic patient with serum iron300 – 500 µg/dL, needs chelation therapy.
• A level more than 500 mg/dL should bechelated even if asymptomatic.
The IV dose is 15 mg/kg/hour for 4 – 6 hoursor until the patient stabilizes, then 6 mg/kg/hour.
Side effects include nausea, hypotension,rash, and anaphylaxis. Hypotension is usuallyresponsive to slowing the rate of infusion ofdesferoxamine, fluids and vasopressor.Administration for more than 15 mg/kg/hr andmore than 24 hours is associated with thedevelopment of adult respiratory distresssyndrome (ARDS).
Supportive therapy: Fluid resuscitation with Ringerlactate or normal saline (20ml/kg) is important

Indian Journal of Practical Pediatrics 2009; 11(1) : 32
32
for poor peripheral perfusion, tachycardia, orhypotension. Vasopressors may be required tomaintain an adequate blood pressure and endorgan perfusion with severe toxicity. Severe ironingestions may require oxygen therapy ormechanical ventilation if pulmonary oedema orhaemorrhage develops, or altered neurologicalstatus in late-stage of ingestion. It is essential todo continuous cardiorespiratory and oxygensaturation monitoring for ingestions more than40 mg/kg.
Admission criteria: All symptomatic patientsshould be hospitalized and receive chelationtherapy. Patients with serum iron levels more than300 mg/dL should be admitted and receivechelation therapy. If serum iron levels are notavailable, patients who have a WBC count morethan 15,000/mm³ and a serum glucose more than150 mg/dL should also be admitted.
Antiarrhythmic and antihyperten-sive cardiovascular drugs
A sudden onset of toxicity is common withantiarrhythmic drug poisoning. Sustained-releasepreparations may have a delay of 1–2 days beforeonset of symptoms, especially if decontaminationwith activated charcoal or whole bowel irrigationis not performed. Antiarrhythmic drug ingestionsare rare occurrences in terms of number ofingestions per year, but may represent adisproportionate number of deaths and severetoxicity following prescription drug poisoning.
Core facts and pathophysiology
1. Drugs that slow heart rate and may blockelectrical conductance through the AV node:
• Class Ib (Lidocaine, phenytoin, tocainide,mexiletine): Toxic effects include lethargy,confusion, coma, seizures, and apnea/respiratory arrest. QRS and QT intervalsusually remain normal. Brady arrhythmiasincluding asystole occur. Rapid infusion of
phenytoin (>1 mg/kg/min, or 50 mg/min) hasresulted in sudden asystole, possibly relatedto the propylene glycol diluent in theIV preparation.
• Class II: ß-adrenergic blockers: Toxic effectsinclude decreased cardiac contractility,centrally mediated coma, seizures, or apnea(especially propranolol). Bradycardia withAV block and hypotension are common18.Ventricular dysrhythmias, including torsadesde pointes, may occur after sotalol poisoning.Some ß-blockers (pindolol, alprenolol, andoxyprenolol) have intrinsic sympathomimeticactivity that in low doses counteracts theeffect on rate and rhythm; this effect is lostwith large overdoses. Hypoglycemia andbronchospasm occur rarely.
2. Drugs that cause QRS widening andventricular dysrhythmias (phase 0 fastNa+-channel blockade). (Class Ia: Quinidine,disopyramide, procainamide, Class Ic:Antidysrhythmic agents: Encainide, flecainide,Class III: Amiodarone)
• Ventricular dysrhythmias, hypotension,sudden onset of pulselessness may occurafter ingestion or overdose. Anticholinergicfindings such as dilated pupils, dry mouth, anddelirium may follow quinidine ordisopyramide ingestion. Quinidine oftencauses vomiting and diarrhea. Propafenoneand encainide overdoses are associated withstatus epilepticus.
3. Drugs that cause QT intervalprolongation and ventricular tachycardia/torsadesde pointes (phase 3 inwardly-rectifyingK+-channel blockade): Quinidine, procainamide,encainide, flecainide, sotalol, amiodarone.
4. Calcium channel blockers are Class IVantidysrhythmics: Toxicity produces decreasedcardiac contractility, peripheral vasodilatation with

2009; 11(1) : 33
33
hypotension in varying degrees, depending on thespecific drug ingested19.
• Bradycardia, AV block and hypotension areseen with verapamil and diltiazem. Suddenonsets of coma, apnea or seizures often occurwith verapamil poisoning.
• Bradycardia without AV block andhypotension are common with nifedipine andnewer calcium channel blockers,e.g., nimodipine.
• Hyperglycaemia may occur due to inhibitionof insulin release with ingestion of any calciumchannel blocker.
• Diltiazem and verapamil are available aslong-acting preparations.
5. Clonidine: It is a central and peripheralα2 adrenergic agonist that is rapidly absorbed.
• CNS α2 stimulation causes opioid-likeeffects, and decreases heart rate andvascular tone, resulting in hypotension20.
• Peripheral α2 stimulation may cause brief,paradoxical hypertension.
• Symptoms of overdose include altered mentalstatus, hypertension and hypotension,respiratory depression and miosis. Onset ofsymptoms occurs within 4 hours of ingestionand rarely last beyond 24 hours.
Investigations
Electrolytes and renal function:Hypokalemia and hypocalcemia may predisposeto dysrhythmias after antiarrythmic overdose.Renal functions tests can help to assess potentialfor decreased renal clearance after overdose, aswell as indicate possible prerenal azotemia fromhypoperfusion.
Imaging and EKG: EKG changes depend onthe type of drug ingested. For example:
a) ß-adrenergic blockers: Bradycardia withAV block, decreased cardiac contractility,ventricular dysrhythmias, including torsades depointes, b) Digitalis preparations: Bradycardiawith heart block, other dysrhythmias, c) Type Ibagents: Bradyarrythmias, including asystole,d) Quinidine, procainamide, disopyramide,encainide, flecainide (Type Ic agents), sotalol andamiodarone: Ventricular dysrhythmias, an R wavein aVR and prolongation of the QTc interval.
Management
Decontamination/Elimination: Activated charcoalshould be used in all patients. Multi-dose charcoalmay be considered with nadolol, atenolol, sotalol,and sustained-release preparations. Whole bowelirrigation is recommended for ingestion ofsustained-release preparations after an initial doseof activated charcoal. Endpoint is passage ofclear rectal effluent with improving clinical status.
Antidote/Specific therapy
• For ß-adrenergic blocker medications,antidote therapy include (from mostefficacious to least efficacious) i) Glucagon,50–100 µg/kg IV (up to 1 mg) followedby infusion of 70 µg/kg/hr. (ii) Epinephrine,10 µg/kg IV (0.1ml/kg of 1:10,000) bolusfollowed by infusion of 0.1–1µg/kg/min.iii) Atropine 20 µg/kg IV (upto 1 mg)every 5–10 minutes until total dose of2 mg delivered, iv) Isoproterenol dose is0.1-1 µg/kg/min IV but it may worsenhypotension due to ß2 agonism causingperipheral vasodilation or v) Transvenouspacemaker if no response to medications.In addition to these, the hypotension willneed fluid resuscitation and inotropic support.
• Drugs causing prolonged QRS andventricular dysrhythmias: The managementinclude i) Sodium bicarbonate 1 – 2 mEq/Lrapid infusion which may be repeated asnecessary to keep blood pH 7.45 – 7.50.

Indian Journal of Practical Pediatrics 2009; 11(1) : 34
34
ii) Lidocaine 1 mg/kg IV, repeat up to 2 dosesiii) Phenytoin 15 – 20 mg/kg IV at a rate notto exceed 1 mg/kg/min iv) Correct potassium,calcium, and magnesium abnormalities21.
• Drugs causing prolonged QTc andventricular dysrhythmias: i) Magnesiumsulfate 30-60 mg/kg rapid IV infusion (up to2 gms) which may be repeated once. Monitorserum calcium and magnesium levels.
• Calcium Channel Blockers: For bradycardiathe recommended treatment in order ofpreference are i) Calcium infusion (calciumgluconate or calcium chloride) IV which maybe repeated along with monitoring of serumcalcium and avoid hypercalcemia,ii) epinephrine infusion, iii) glucagon,iv) atropine and v) consider transvenouspacing if above medications fail.
• Clonidine: For hypotension, IV bolus fluidsare generally adequate. On the other handhypertension is generally transient and doesnot need treatment. For bradycardia atropinemay be used. Lethargy and apnoea, due toopioid effects, may respond to naloxonewhich may not be effective againstbradycardia or hypotension22.
Supportive therapy: Patient should be monitoredclosely for potential respiratory compromise andall equipment and medications for rapid sequenceintubation should be immediately available.Continuous cardiorespiratory monitoring andoxygen saturation by pulse oximetry should bedone for at least the first 6 hours after ingestionin every case. Further monitoring depends on theseverity of condition.
ANTIHISTAMINES
Core facts and pathophysiology
First generation antihistamines includediphenhydramine, hydroxyzine, chlorpheniramineand many others. Second generation
antihistamines include terfenadine, astemizole,loratadine, cetirizine and fexofenadine
Antihistamines are competitive inhibitors ofthe H1 receptor (H1 antagonists). Secondgeneration antihistamines act selectively onperipheral H1 receptors because they do not crossthe blood brain barrier or do so in such lowconcentrations that blockade of central histamineand cholinergic receptors does not occur,accounting for their “non-sedating” properties.CNS depression occurs at therapeutic doses offirst generation antihistamines; over-dosage mayresult in CNS stimulation in children and youngadults. A single dose of 20 – 40 mg/kg has beenreported to be a lethal dose in adults. Seizureshave been reported with as little as 150 mg in an18-month-old child. Children seem to be moresensitive to toxic effects23.
Clinical features
1. Anticholinergic effects like fixed, dilatedpupils, hyperpyrexia, facial flushing, excitation,tremors and hallucinations are seen in overdoseof first generation drugs. In severe cases evengeneralized seizures, arrhythmias and coma canoccur. Seizures occur much more commonly inchildren than adults.
2. Second generation antihistamine over-dose (terfenadine and astemizole) causesQT prolongation and ventricular arrhythmias suchas torsades de pointes24. CNS sedation andseizures have also been noted. Erythromycin andketoconazole increase the risk of arrhythmia.
3. Antihistamines are widely availablecombined with other medications in over-the-counter for common cold preparations,particularly acetaminophen and phenyl-propanolamine; therefore, co-ingestion of othermedications may also require intervention. Manyof these are available as sustained-releasepreparations, prolonging the period required forobservation or treatment.

2009; 11(1) : 35
35
Management
Decontamination: Gastric lavage is indicated forrecent ingestions with potential for altered mentalstatus. Activated charcoal is used as single dosefor non-sustained release preparations and multi-dose charcoal for slowed gastric motility orsustained release ingestions.
Supportive management: It includes control ofseizures with lorazepam or phenobarbital.Ventricular arrhythmias, torsades de pointes aretreated with either magnesium sulphate orphenytoin. Hypertension when occurs is managedwith diazoxide or methyldopa. Use ofphysostigmine for severe anticholinergic toxicity(if seizures, arrhythmias, severe hypertension areunresponsive to above measures) has beenreported. Continuous cardiorespiratory andoxygen saturation monitoring are needed forsymptomatic patients or those with secondgeneration antihistamine ingestion.
ß–ADRENERGIC AGONISTS
Core facts and pathophysiology
ß-adrenergic agonist toxicity is dosedependent. Ingestion of <1 mg/kg of salbutamol(3–10 times the normal daily dose) is non-toxic.Up to 20 times the normal daily dose of salbutamolhas been ingested without serious medicalcomplications or death25. All ß-adrenergicagonists are rapidly absorbed, and toxic effectsare seen within an hour of ingestion.
ß1-receptors are found on the heart.β2-receptors are found in blood vessels, lungs andpancreas. ß1-effects include tachycardia,increased cardiac contractility, tremor, agitationand vomiting. ß2-effects include peripheralvasodilatation, tachycardia, widened pulsepressure, tremor, hypokalemia and hyperglycemia.Hyperglycemia results from stimulation ofglycogenolysis. Hypokalemia results from
increased activity in membrane-boundNa+/K+ ATPase in skeletal muscle. This reflectsK+ shift from the extracellular to intracellularspace and does not indicate a true deficit of totalbody potassium. Therefore, potassiumreplacement is not needed following ß-agonistingestion. Tremor occurs following ß-agonistpoisoning because of differential responses amongfast- and slow-twitch muscle groups. SevereCNS effects are rare because most orallyadministered ß-agonists do not cross the blood-brain barrier in large amounts.
Management
GI decontamination is usually not necessary,definitely not needed if patient has alreadyvomited. Activated charcoal may be used if childarrives early.
Use of ß-adrenergic blockers has beensuggested as helpful in patients with severetoxicity. But it is very rare that a child withsalbutamol ingestion will ever need ß-blockeradministration.
Points to Remember
• N-acetylcysteine is indicated in anypotentially toxic acetaminophen(>150mg/kg) ingestion, and is mosteffective in the first 24 hours.
• A sudden onset of toxicity is common withantiarrhythmic poisoning but withsustained-release preparations symptomsmay be delayed up to 1-2 days.
• Toxic manifestations of anticonvulsantscan be caused by accidental or intentionaloverdose, drug interactions, idiosyncraticreactions and hypersensitivity reactions.
• Ingestion of >20 mg/kg of elemental ironis toxic. Lethal ingestions occur with180 – 300 mg/kg of elemental iron.

Indian Journal of Practical Pediatrics 2009; 11(1) : 36
36
• Clonidine toxicity includes altered mentalstatus, hypertension and hypotension,respiratory depression, and miosis.It resembles opioid poisoning.
References1. Anker AL, Smilkstein MJ. Acetaminophen:
Concepts and controversies. Emerg Med ClinNorth Am 1994; 12:335–349.
2. Howland MA, Smilkstein MJ, Weisman RS.Acetaminophen. In: Goldfrank LR, ed.Goldfrank’s toxicologic emergencies. 5
th edn
Norwalk, CT: Appleton & Lange, 1994;pp487–497.
3. Howland MA, Smilkstein MJ, Weisman RS.Antidotes in depth: N-acetylcysteine. In:Goldfrank LR, ed. Goldfrank’s toxicologicemergencies. 5
th edn, Norwalk, CT: Appleton &
Lange, 1994;pp498–499.4. Harrison P, Keays R, Bray G, et al. Improved
outcome of paracetamol-induced fulminanthepatic failure by late administration ofacetylcysteine. Lancet 1990;335:1572–1573.
5. Keays R, Harrison P, Wendon J, et al.Intravenous acetylcysteine in paracetamol-induced fulminant hepatic failure: A prospectivecontrolled trial. Brit Med J 1991;303:1026–1029.
6. Osborn H, Goldfrank LR. Sedative-hypnoticagents. In: Goldfrank LR, Flomenbaum NE,Lewin NA, Weisman RS, Howland MA,Hoffman RS, eds, Goldfrank’s toxicologicemergencies. 5
th edn, Norwalk, CT: Appleton &
Lange, 1994;pp787–810.7. Seyffart G. Antihistamines and other sedatives.
In: Haddad LM, Winchester JF, eds. Clinicalmanagement of poisoning and drug overdose.Philadelphia: W. B. Saunders, 1990;pp820–861.
8. Sugarman JM, Paul RI. Flumazenil: A review.Pediatr Emerg Care 1994;10:37–43.
9. Dodson WE, Bourgeois BFD. Pharmacologyand therapeutic aspects of antiepileptic drugsin pediatrics. J Child Neurol 1994;9(Suppl):2S1–2S7.
10. Macnab AJ, Birch P, Macready J.Carbamazepine poisoning in children. PediatrEmerg Care 1993;9:195–198.
11. Patsalos PN, Duncan JS. Anti-epileptic drugs:
a review of clinically significant druginteractions. Drug Safety 1993;9:156–184.
12. Leach JP, Brodie MJ. New antiepileptic drugs—an explosion of activity. Seizure 1995;4:5–17.
13. Schmidt D, Kramer G. The new anticonvulsantdrugs: Implications for avoidance of adverseeffects. Drug Safety 1994;11:422–431.
14. Banner W, Tong TG. Iron poisoning. PediatrClin North Am 1986;33:393–409.
15. Goldfrank LR. Iron. In: Goldfrank LR, ed.Goldfrank’s toxicologic emergencies. 5th edn,Norwalk, CT: Appleton & Lange, 1994;pp 521–531.
16. Henretig FM, Shannon M. Toxicologicemergencies. In: Fleisher GR, Ludwig S, eds.Textbook of pediatric emergency medicine.3
rd edn, Baltimore: Williams & Wilkins, 1993;
pp776–779.17. Howland MA. Deferoxamine. In: Goldfrank LR,
ed. Goldfrank’s toxicologic emergencies.5
th edn, Norwalk, CT: Appleton & Lange, 1994:
pp532–534.18. Critchley JA, Ungar A. The management of
acute poisoning due to beta adrenoceptorantagonists. Med Toxicol 1989;4:32–45.
19. Ramoska EA, Spiller HA, Winter M, Borys D. Aone year evaluation of calcium channel blockeroverdoses: Toxicity and treatment. Ann EmergMed 1993; 22:196–200.
20. Fiser DH, Moss MM, Walker W. Critical carefor clonidine poisoning in toddlers. Crit CareMed 1990;18:1124–1128.
21. Pentel PR, Benowitz NL. Tricyclicantidepressant poisoning: management ofarrhythmias. Med Toxicol 1986;1:101–121.
22. Nichols MH, King WD, James LP. Clonidinepoisoning in Jefferson County, Alabama. AnnEmerg Med 1997;29:511–517.
23. Hendes L. Efficacy and safety of antihistaminesand expectorants in nonprescription cough andcold preparations. Pharmacotherapy1993;13:154–158.
24. Wiley JF, Gelber ML, Henretig FM, et al.Cardiotoxic effects of astemizole overdose inchildren. J Pediatr 1992;120:799–802.
25. Wiley JF II, Spiller HA, Krenzelok EP, Borys DJ.Unintentional albuterol ingestion in children.Pediatr Emerg Care 1994;10:193–196.

2009; 11(1) : 37
37
CORROSIVE POISONING
* Jayanthi Ramesh
Abstract: Corrosive ingestion is accidental inchildren. Though it forms a small group, itcauses considerable morbidity and mortality.Corrosives are of 2 types, acids and alkalis.Corrosives produce coagulative necrosis andthis depends on the concentration of theingested material. Acutely, they present withintense pain, hemetemesis, respiratory distress,drooling, stridor and locally may cause burninjuries. Child may require acute caremanagement of the airway, breathing andcirculation. Steroids are given to preventesophageal stricture if the child presents within48 hours of ingestion. Endosopy is advisedwithin 24 hours. Late complications likeesophageal stricture has to be managed byperiodic dilatation and surgical interventionas required. Prognosis with corrosiveingestion is guarded.
Key words: Corrosive poisoning, Acids andAlkalis, Glottic edema, Esophageal stricture,Endoscopy.
Corrosives are widely used for cleaningmetals in industries and for domestic purposes.Most of the household cleaning agents containcorrosives which include both acids and alkalies.Children, especially toddlers are more prone foraccidental ingestion, whereas in adolescents andadults it is homicidal or suicidal. Corrosives may
TOXICOLOGY
be thrown on the face or body deliberately(vitriolage) to cause disfigurement or blindness.
Corrosives are classified into four categories:(1) Acids which include, mineral acids such assulphuric acid, nitric acid and hydrochloric acid,(2) Organic acids like oxalic acid, carbolic acid(phenol), acetic acid, and salicylic acid,(3) Vegetable acid like hydrocyanic acid, and(4) Alkalis which include, sodium hydroxide,potassium hydroxide and ammonium hydroxide.
Side effects of corrosives
It affects the skin (exposed part), mouth,throat, upper gastrointestinal tract and therespiratory system. Initial effects are burning pain,tingling sensation, blood stained vomiting, reductionin voice volume due to laryngeal edema. The lateeffects are pulmonary edema, broncho-pneumonia and oesophageal and stomachperforation. Laryngeal and oesophageal stricturesand stricture at the pyloric junction occur asdelayed complications.
Mineral acids are used commonly inautomobile industry as battery fluids, inlaboratories and as domestic cleansing agents.
Pathophysiology
Corrosive acids cause extraction of waterfrom the tissues, destroy the tissue protein andconvert the cellular protein to acid albuminates.Hemoglobin is converted into acid hematin and isprecipitated. Due to the intense stimulation causedby the acid, the vascular tone is lost. This causeslocal irritation, bleeding and sloughing of mucousmembrane and skin. In severe cases edema and
* Consultant Pediatrician,Kanchi Kamakoti CHILDS Trust Hospital,Chennai.

Indian Journal of Practical Pediatrics 2009; 11(1) : 38
38
necrosis of the deeper tissues are seen. The mostcommon area affected is the oesophageal andpyloric junction. It may lead on to perforation andstricture formation.
Clinical features
It depends on the mode, amount andconcentration of the acid ingested, contactduration and the age of the child. In acutepoisoning there is a severe burning pain in themouth, pharynx and abdomen followed byvomiting, drooling, stridor, difficulty in breathing,hematemesis, fever and oral burns. Presence ofstridor and drooling indicate injury to larynx andpharynx. Child may be in a state of cardiorespiratory failure due to hypoxia following glotticoedema. Profound shock may ensue.Occasionally severe metabolic acidosis andmultiorgan dysfunction results. If perforationoccurs, it may lead to mediastinitis and peritonitis.
Management
History has to be noted and depending upon theclinical features treatment has to be instituted.Airway patency should be maintained andif necessary intubation, cricothyrotomy ortracheostomy is performed. In case of pulmonaryedema, positive pressure ventilation is given.The presence of oropharyngeal ulcers indicatethat there is increased risk of visceral injuries.Endosopy has to be performed within 24 hoursfrom the time of injury. Hypotension if presentshould be corrected with normal saline. If thepatient is able to swallow saliva, oral feeding canbe allowed. In patients who are unable to swallowhydration and nutrition are maintained throughIV fluids or through gastrostomy. Steroids arerecommended within 48 hours if endosopy cannotbe performed or if circumferential burns areidentified during endosopy. Antacids can be usedfor burns in the stomach. Antibiotic may be usedin patients with suspected perforation of thestomach. Otherwise use of antibiotics has to bereserved for specific signs of infection.
Gastric lavage, emesis, charcoal andcathartics are contraindicated in corrosivepoisoning.
Treatment of sequelae : Esophageal strictureand gastric outlet obstruction require frequentdilatation once the healing is complete, whichtakes 4 to 6 weeks. Retrograde dilatation may berequired in some if it is impossible to dilate fromabove. This is possible because the lower end ofoesophagus is conical as opposed to the proximalend where the opening is eccentrically placed andmay be difficult to define.
Surgical treatment is indicated for failure ofdilatation to produce an adequate lumen, noncompliance of patients with bougienage, completestenosis and fistula formation. Surgeries whichcan be done include local excision of stricture ifit is short, high oesophagogastrostomy, cervicaloesophagogastrostomy, colon or jejunalinterposition.
PHENOL (CARBOLIC ACID)
Phenol or its related compounds likeresorcinol, hexachlorophene, cresol andhydroquinone are used as antiseptics, germicides,caustics and preservatives. In children poisoningis usually accidental while in adolescents it issuicidal and very rarely homicidal.
Pathophysiology
It is a protoplasmic poison and it causesdenaturation of proteins thereby killing cells.Locally it causes anaesthesia by stimulating thenerve endings causing paralysis. Capillary damageresult in thrombus formation in superficial vessels.It affects the heart, kidneys and also the centralnervous system. It stimulates respiratory centreleading to respiratory alkalosis.
Clinical features
In the acute phase : Intense pain, hematemesis,bloody diarrhea, shock, laboured breathing,

2009; 11(1) : 39
39
hyperpnoea followed by metabolic acidosis, stupor,coma, convulsions and pulmonary oedema occur.If not attended to it can cause death. If thechildren survive the acute phase, they may developrenal failure and/or hepatic dysfunction. Urinecolour is dark smoky green on exposure to air.Paralysis of respiratory and cardiac centre leadsto death.
Lab investigations
Few drops of ferric chloride is added to urine.The colour of urine in the presence of carbolicacid changes to violet or blue.
Treatment
Airway management by intubation is thepriority. Gastric lavage using plain water or 10%glycerine (only condition where gastric lavageadvocated) is done through a soft nasogastric tubetill no phenolic odour is present in the effluent.White of the egg can be given. Supportivemanagement should be given. If the childdevelops renal failure, it is managed by fluid andsalt restriction followed by peritoneal orhaemodialysis as required. Apply castor oil forsurface burns.
HYDROCYANIC ACID ANDITS SALTS
They are used in industries and for fumigatingthe homes, photography and silver polishes.Inhalation of these substances may cause cyanidepoisoning. Some fruits like cherry, plum, peach,apricot, etc contain amygdaline which on ingestioncan release cyanides.
Pathophysiology
They act on the cytochrome oxidase byinhibiting the system of electron transport andhence oxygen utilisation leading to cellulardysfunction and death. Death occurs within10 minutes after consuming the poison.
Clinical features
It depends upon the mode of intoxication.A large dose leads to death in a minute.Bitter almond odour and hyperventilation areobserved.
CNS toxicity include headache, dizziness,nausea, dilated pupils, convulsions and coma.Hypotension and dyspnoea can also be present.
Treatment
Objective of the treatment is methemoglobinproduction which competes with the cytochromeoxidase cyanide complex and dissociation occursresulting in restoration of cellular and respiratoryfunction. Oxygen through non-rebreathing maskhas to be administered. Specific antidote capsulecontaining amyl nitrite is broken and inhaled over30 seconds till sodium nitrite solution is preparedand given IV in a dose of 10mg/kg (max dose30mg/kg). 25% Sodium thiosulphate solution at adose of 1.65ml/kg is administered next. Hydroxycobalamin is another specific antidote (not freelyavailable). Supportive measures to correcthypotension, shock, and metabolic acidosis areused wherever needed. Death results due torespiratory paralysis.
ALKALIS
Potassium and sodium hydroxides, sodiumphosphate, sodium and potassium carbonates arethe examples of alkalis. They are used in soapmanufacturing industries and are used inhousehold cleansing agents. Sugar testing tabletscontain sodium hydroxide. Button batteriescontain sodium and potassium hydroxide.Accidental ingestion is very common due to theireasy accessibility.
Pathophysiology
Alkalis combine with protein to formproteinates and fat to form soaps, thus producingsoft, necrotic, deep penetrating wounds on
Indian Journal of Practical Pediatrics 2009; 11(1) : 40
40
contact with the tissues. Solubility of these agentscauses further damage in due course of time.
Clinical features
Acute presentation: Burning pain in themouth and stomach, nausea, vomiting (vomitus isslimy and blood stained), swelling of mucousmembrane of the mouth and airway compromisemay occur. Pharyngeal involvement leading torespiratory distress, dysphagia, bloody diarrhoeawith tenesmus, board like rigidity of the abdomen,shock followed by collapse ensues.
Late complications are oesophageal strictureand atrophy of the gastric mucosa. Usually buttonbatteries pass through the oesophagus, GIT withlittle or no damage. If it disintegrates may lead toperforation of bowel and may prove detrimentalto the patient.
Lab investigations
RBC count and hematocrit increases.Ingestion of button batteries-Radiography to
be done.
Treatment
Emergency measures : Nil per oral, take care ofthe airway, if patient presents with shock givesupportive therapy.
Within an hour of ingestion, a soft nasogastrictube or Levine tube can be introduced carefully.Hypocalcaemia due to phosphate ingestion shouldbe treated with calcium gluconate.
Button batteries lodged in the oesophagusshould be removed using endoscopy immediately.Usually it will be expelled in 2-3 days time ifbeyond esophagus. Cathartics can be given. Ifthey are lodged in the Meckel’s diverticulumsurgical intervention is necessary.
Eye contact : It is an emergency as it producespermanent scarring of the cornea. Wash the eyeswith running water for 30 minutes. To allaypain analgesics have to be administered.
Ophthalmology consultation to be obtained. Skinis washed with water till the soapy feelingdisappears.
Complications : Oesophageal stricture is treatedwith internal bougienage. Atrophy of gastricmucosa is at high risk of developing gastriccarcinoma.
Points to Remember
• Symptoms and signs should be correlatedwith lab investigations.
• Maintenance of airway breathing andcirculation is the priority.
• Gastric lavage is not indicated.• Endosopy has to be done within 24 hours
of ingestion.• Steroids are administered within
48 hours, preferably within an hour ofingestion when endosopy is not feasibleor if circumferential burn is seen inendoscopy.
Bibliography
1. Dreisbach RH. Corrosives. In : Text book onChildhood Poisoning, 11
nd edn, Lange Medical
Publication, California, 1983; pp 216-238.2. Utpal Kant Singh, Leyland FC, Rajniti Prasad,
Shivani Singh. Corrosive poisons. In: Poisoningin children, 3
rd edn, Jaypee Brothers Medical
Publihsing (P) Ltd., New Delhi, 2006;pp33-40.3. Penner GE, et al. Acid ingestion, toxicology and
treatment. Ann Emerg Med 1980; 9, 374-397.4. Haller JA, Andrews HG, Write JJ, et al. Acute
physiology and management of acute corrosiveburn of oesophagus, J Paediatr Surg 1971; 6:578-584.
5. Pratyush Gupta, Sanjay Verma. Uniquepresentation of epiglottis in corrosivepoisoning, A Case report. The Internt Journalof Anaesthesiology 2007;Volume 12 No.2.
6. Anderson KD, Rouse TM, Randolph IG.Controlled trial of corticosteroids in childrenwith corrosive injury of the oesophagus, N EnglJ Med 1990;323: 637- 640.

2009; 11(1) : 41
41
HOUSE HOLD MATERIALPOISONING
* Shuba S** Betty Chacko
Abstract : Poisoning in children may beaccidental, non-accidental, iatrogenic or inolder children deliberate. In majority ofchildren, poisoning is accidental and ispredominantly seen in children under 5 years.Substances taken could be medicines, plantsor household products like cleaning agents,cosmetics, insect repellants and agents usedfor home remedies. Most of them are consumedin small amounts and hence non toxic. In mildcases, symptoms are predominantlygastrointestinal. In severe cases manifestationsmay be neurological, cardiovascular orrespiratory. Most of them recover withsupportive care eventhough no specificantidotes are available. Mortality doesoccur in a small percentage of cases.Generating awareness and educatingcaregivers for safe keeping of poisonoushousehold materials would be the best strategyfor prevention.
Key words: Poisoning, Household materials
Poisoning during childhood is a universalproblem. It may be accidental, non accidental andiatrogenic or suicidal. Data from National PoisonInformation Centre, New Delhi indicate that
TOXICOLOGY
among the total poisonings, children constituted36.5%. Accidental mode of poisoning occurredin 79.7% while intentional attempts were notedin 20.2% of children above 12 years of age.1
Pediatric poisonings constituted 0.23-3.3% oftotal hospital admissions according to amulticentric study in India. Children below 5 yearsconstituted 50-90% of all cases. The male:femalesex ratio was 1.65-2.65:1. Mortality varied from0.64 to 11.6%.2 Among the various agents, thelargest group of 44.1% was constituted byhousehold products.1 These agents areheterogenous and include those used for cleaningand for home remedies, cosmetics and insectrepellants. Fortunately most of them are consumedin small amounts and hence non toxic.As symptoms are usually nonspecific and maymimic other diseases, a high index of suspicionshould be entertained in any unresponsive child.
NAPHTHALENE
Naphthalene is a constituent of coal tar. It isan ingredient of dusting powder, lavatorydeodorant discs, wood preservatives, fungicides,moth balls and insecticides, intestinal antiseptics,vermicides, as well as medicaments of pediculosisand scabies.
Lethal dose
Mean lethal dose in adult is between5–15gms. Among G6PD deficient individualseven miniscule doses induce dangerous reaction.In children absorption occurs rapidly. Ingestionof 2 gm may be fatal. Newborns are moresusceptible. Thinner skin and application of babyoil increase dermal absorption.3
* Professor, Department of Pediatrics.** Professor & Head, Department of Pediatrics
Sri Ramachandra Medical College & RI, Chennai.

Indian Journal of Practical Pediatrics 2009; 11(1) : 42
42
Toxicity
Toxicity occurs mostly in children who suckor chew moth balls. Transplacental transfer hasalso been reported. The formation of epoxidemetabolite, probably is responsible for hemolysis.Hemolysis occurs in G6PD deficiency due toinstability of erythrocyte glutathione.Ocular toxicity occurs due to oxidative stress andlipid peroxidation. Newborns have increasedsusceptibility due to inability to conjugate bothnaphthalene and bilirubin resulting in kernicterus.Erythema and dermatitis, hemolysis and jaundicehave occurred after dressing infants in clothingstored with naphthalene moth balls.
Acute Toxicity: Acute intravascular hemolysisis the most characteristic sign, particularly inpersons with red cell glucose-6-phosphatedehydrogenase deficiency; This is accompaniedby fever, jaundice, anemia, leucocytosis,haemoglobinuria, renal insufficiency andsometimes liver dysfunction. Headache,abdominal pain, nausea, vomiting, diarrhea, feverand profuse sweating can occur. Methemo-globinemia and cyanosis may be present. Irritationof the urinary bladder causes urgency, dysuriaand passage of brown or black urine with albuminand casts. Optic neuritis and liver necrosis arereported. In severe poisoning, excitement, coma,convulsion and acute renal failure are seen in olderchildren whereas kernicterus occurs in younginfants. Inhalation leads on to respiratory failureand pulmonary oedema. Abuse by inhalation hasbeen described. Dermatitis follows industrialexposure.
Chronic abuse can result in peripheralneuropathy and chronic renal failure.3-6
Investigations
Hemoglobin, hematocrit, reticulocyte count,RBC count, peripheral smear, serum bilirubin,methemoglobin levels and plasma hemoglobin
indicate presence and severity of hemolysis. Urineis tested for hemoglobin and alpha naphthol.
In hemolysis investigations show a rapid fallin RBC count, hemoglobin and hematocritfollowed by temporary increase in reticulocytecount and normoblasts in peripheral blood.RBCs contain Heinz bodies and cells may befragmented showing anisocytosis andpoikilocytosis. During hemolytic crisis, the fragilityof remaining cells increase.
Management
Contaminated skin or eyes are flushed withlukewarm running water for 20 minutes. In casesof inhalation, the person is removed from thesource of contamination. In ingestion, lavage maynot be effective after 2 hours. Lavage is to bedone with activated charcoal of 1gm/kg upto50 grams given as a slurry with water. Milk orfatty meals is avoided for 2 -3 hours, as theypromote absorption. Supportive care is needed.
Symptomatic treatment: Repeated bloodtransfusion is given till Hb is 60 – 80% of normal.Corticosteroid is useful in cases of hemolysis.In case of kernicterus, hemodialysis / exchangetransfusion is indicated. Convulsions if any are tobe controlled with diazepam. Alkaline diuresis iscarried out in the form of sodium bicarbonate 5gmorally q4H or as necessary to maintain alkalineurine and iv fluids are administered at15ml/kg/hrwith frusemide 1mg/kg. In cases of methemo-globinemia of >30%, intravenous methylene blueis indicated.3
CAMPHOR
Camphor may be naturally produced orsynthetic. It is obtained from wood of camphortree (Cinnamonum camphora).
Uses
Camphor is used as rubefacient, counter-irritant and antipruritic, as moth repellant,

2009; 11(1) : 43
43
preservative, in dentistry with para chlorophenolfor antibacterial activity, as carminative to relievegriping and as mild expectorant.7
Toxicity
Lethal dose for children is 0.5 – 1gm and forinfants 70mg / kg.8
Clinical effects
Camphor is readily absorbed from skin, GITand respiratory tract. Odour of camphor can beobserved in breath. Onset of symptoms is seenwithin 5 – 90 min after ingestion. Oral andepigastric burning sensation, nausea, vomiting andfeeling of warmth can be seen. Mydriasis andimpairment of vision are noted. Headache,confusion, vertigo, excitement, restlessness,delirium, hallucinations, increased muscularexcitability, tremors and jerky movements canoccur. Epileptiform convulsions which may besevere can be followed by depression and coma.Inhalation above 2 PPM causes irritation to noseand throat. Chronic ingestion has symptoms ofviral illness and Reye syndrome like illness withneurological deterioration, liver injury, prolongedprothrombin time and hypoglycemia.Camphor crosses placenta and has beenimplicated in fetal and neonatal death.7-11
Course and prognosis
If patient survives for 24 hours recovery islikely. Death is from respiratory failure, statusepilepticus or circulatory collapse. Autopsy showshemorrhage and brain cell degeneration
Management
If 10mg/kg has been ingested andasymptomatic by 4 hours, hospitalization is notindicated. If 30mg/kg ingested, patient is to beadmitted. Convulsive state may be life threatening.Convulsion is treated with diazepam beforeattempting emesis or gastric lavage. Gastric
lavage is done with warm water (380-400C) onlyafter airway protection. Cathartics like sodiumsulphate 250mg/kg and activated charcoal of15-30gms are administered in children. In caseof inhalation, patient is removed from exposureand administered oxygen. For external contact,skin is washed thoroughly with soap and water.Eye exposure is managed by flushing with largeamount of water.Lipid hemodialysis and resinhemoperfusion may be helpful. There is nospecific anti dote.7-10
EUCALYPTUS OIL
Eucalyptus oil is obtained from leaves ofvarious species of eucalyptus. Major activeingredient is cineole. Medicinal eucalyptus oilcontains not less than 70% w/w/ of cineole.
Uses
It is not recommended in children. It is usedby inhalation as decongestant, orally for catarrhand cough, applied as rubefacient (0.5-3%),flavouring agent and cleaning solvent.
Toxic dose
Toxicity is seen with 0.05 – 0.5 ml / kg dose.It is well absorbed orally. Minor depressionoccurs with ingestion of 2-3ml and severedepression with 5ml.1
Toxicity
Toxic effects are rapid in onset andextensive. GI symptoms like abdominal pain,vomiting, diarrhea occur initially followed by CNSsymptoms of loss of consciousness,hypoventilation, depression of reflexes andconvulsions. Onset of coma occurs within severalminutes to 2 hours. Coma lasts for half an hourto 30 days. Convulsions may be prominent inchildren. Miosis or mydriasis (miosis morecommon) occurs. Muscle weakness and ataxiaare observed.

Indian Journal of Practical Pediatrics 2009; 11(1) : 44
44
Respiratory involvement in the form ofrespiratory depression, dysphonia, pneumonitis,bronchospasm, aspiration pneumonia followingvomiting and pneumonia after inhalation mayoccur. Tachycardia, weak irregular pulse andirritation to skin and eyes may be seen. Nephritisand prolonged prothrombin time rarely occur.
Management
Close observation is required for minor ormoderate poisoning. Asymptomatic patient is tobe observed for 6 hours and x-ray to be takenafter 6 hours. ABC and neurological statusare monitored and symptomatic and supportivecare given. Attempts to induce vomiting andaggressive GI decontamination are to be avoided.Lavage and instillation of charcoal are to bedone only after ET tube is in situ. Routine useof peritoneal dialysis or hemodialysis notestablished to be useful. No specific antidote isavailable.12-15
Prognosis
Most recover within 24 hours. Prominentsequelae are not reported but death may occur.
NEEM OIL / MARGOSA OIL
Neem oil is obtained from the treeAzadirachta indica. It contains neutral oils suchas palmitic and stearic acids. Active ingredientsare terpenoids such as azadirachtin, nimbin, picrinand sialin. It also contains aflatoxin in very lowconcentrations. Seed kernels comprise primarilyof glyceride azadirachtin which is the most activeinsecticidal component of neem.
Uses
Neem oil is used as insecticide and insectrepellent, oral dentifrice, in traditional medicineto treat malaria, diabetes, helminthiasis, CVS andskin diseases and as a contraceptive, anti ulcer,antisecretory and fungicidal agent and homeremedy for respiratory infection.
Toxicity
Toxin may be a long chain monosaturatedfree fatty acid. Toxic dose is not known butsymptoms seem to be dose related. Toxicencephalopathy in the form of Reye like illnessmay result.
Neem oil ingestion can give rise to vomiting,metabolic acidosis, tachypnoea, recurrentseizures, drowsiness, coma and cerebral edema.Polymorphonuclear leucocytosis is observed.Liver enzymes may be elevated but hepatic failureis not seen. Fatty infiltrate of liver and proximalrenal tubules is seen. In animal models neem oilacts rapidly within 30 minutes on nuclei ofhepatocytes, followed by mitochondrial injury, lossof ribosomes, loss of liver glycogen and presenceof lipid droplets in the hyaloplasm.16-18
Treatment
Gastric lavage is not recommended.Convulsions are treated with diazepam.Supportive management is most important.
Prognosis
Prognosis is good in patients with mildvomiting and gastrointestinal features but fatalitiesand neurological deficits are reported in patientswith CNS symptoms.
MOSQUITO REPELLANT POISONING
Mosquito repellants are based either onsynthetic chemicals or natural ingredients. Majormethod of dispersion includes sprays, burningmosquito repellant sticks or liquids, or applicationas skin cream. Synthetic repellants containchemicals like DEET (N, N – diethyl – m-toluamide), PMD (P-menthane – 3, 8 – diol),icaridin, pyrethroid compounds as permethrin.The major plant product is extract of lemoneucalyptus tree and citronella oil

2009; 11(1) : 45
45
DEET
DEET is one of the most potent mosquitorepellants but cannot be used on damaged skin.
Products are available in varyingconcentration from 7.5%–95%. Only productscontaining lower concentration of DEET (< 15%)formulated with ethyl or isopropyl alcohol shouldbe used in children
Toxicity
DEET is generally well tolerated on externalapplication.About 50ml of 100% DEET may bepotentially lethal, though even at doses as low as21mg/kg/day children have developed toxicencephalopathy. DEET is efficiently absorbedthrough the skin and gut. Ingestion of smallamounts produces nausea, vomiting, diarrhoeaand abdominal pain. Large ingestion gives riseto coma, hypotension, abnormal hypertonicmovements, tremors and convulsions within0.5 to 6 hours. Toxic encephalitis is rarely seenbut extremely severe and is characterized byirritation, altered behaviour, restlessness,convulsions, clonic movements, CNS depression,abnormal CSF (lymphocytic pleocytosis) andaltered EEG. A Reye syndrome like finding withsevere hyperammonemia can occur and it maybe associated with ornithyl-carbamoyl transferasedeficiency. Eye exposure causes irritativeconjunctivitis and skin contact can produce mildtingling. Dermatitis with erythema and bullousreaction or urticaria may occur after prolongedor repeated skin exposure to highly concentratedformulations.
Treatment
In minor ingestion, induction of vomiting isavoided. In major ingestion, gastric lavage isdone after airway protection. Stomach should beaspirated, and a slurry of activated charcoaladministered, followed by sorbitol or salinecathartics.
In case of cutaneous exposure, skin iswashed with non-irritant soap and water. For eyecontamination, prolonged flushing of eyes withcopious amount of water is carried out.For dermatitis, topical steroids and oralantihistamines will help. Seizures are controlledwith anticonvulsants. Haemodialysis and charcoalhaemoperfusion have been tried.
Prognosis
Recovery following DEET poisoning isusually within 36 hours but death has beenreported in children with ornithyl-carbarmoyltransferase deficiency.19,20
PYRETHROIDS
Pyrethroid compounds are widely used asinsecticides both at home and in agriculture.Two types of pyrethroids are in existence, TypeII is more commonly used as agriculturalinsecticides. Some of the pyrethroid compoundssuch as Allethrin are used as mosquito repellants.Pyrethroids are primarily sodium channel toxins,readily prolonging excitation. The major site ofaction of all pyrethroids has been shown to bethe voltage-dependent sodium channel.
Type I Pyrethroids: Bioallethrin, Cismethrin,Permethrin, Pyrethrins.
Type II Pyrethroids: Cyhalothrin, Cyper-methrin, Deltamethrin, Fenvalerate.
Toxicity
Symptoms occur when exposure is large.Two basic poisoning syndromes are seendepending on the type of pyrethroids.
Signs of pyrethroid poisoning
Type I Poisoning: Severe fine tremor, markedreflex hyperexcitability, sympathetic activation,paresthesia (dermal exposure)

Indian Journal of Practical Pediatrics 2009; 11(1) : 46
46
Type II Poisoning: Profuse watery salivation,coarse tremor and seizures, increased extensortone, moderate reflex hyperexcitability,sympathetic activation, choreoathetosis,paresthesia (dermal exposure). Pyrethroidingestion gives rise to a sore throat, nausea,vomiting and abdominal pain within minutes.Systemic effects occur 4–48 hours afterexposure.There may be mouth ulceration,increased secretions and/or dysphagia. Dizziness,headache and fatigue are common, andpalpitations, chest tightness and blurred vision areless frequent. Coma and convulsions are theprincipal life-threatening features. Most patientsrecover within 6 days, although there were sevenfatalities among 573 cases in one series and oneamong 48 cases in another.Paresthesiae usuallyresolves in 12-24 hours
ALLETHRIN
It is a synthetic pyrethroid and has chemicalproperties similar to pyrethrin
Dermal exposure gives rise to tingling,pruritis, blotchy erythema. Inhalation leads torespiratory tract irritation with cough, milddyspnea, sneezing and rhinorrhea. Ingestion isassociated with nausea, vomiting, abdominal pain,headache, dizziness, anorexia and hypersalivation.Severe poisoning is characterized by impairedconsciousness, convulsions, muscle fasciculationwhich take several days or weeks to recover, andrarely non-cardiogenic pulmonary oedema.
Management
Immediate decontamination of the skin withsoap and water is essential first aid.
Topical Vitamin E (Tocopherol Acetate)reduces skin irritation and paresthesia.The mechanism of action may in part be due tosequestration of pyrethroid into the vitamin E orto a membrane interaction. In ocular exposure,irrigation with lukewarm water or 0.9% saline
for at least 10minutes is carried out and topicalanesthetic may be required for pain relief.Lavage is not undertaken because of theassociated solvents in case of ingestion.Treatment is mainly symptomatic. Fasciculationsmay be treated with atropine In experimentalanimals, ivermectin, a chloride channel agonisthas been useful to reverse the peripheral signs ofdeltamerin poisoning, while pentobarbitonereduced the motor signs but was not effective inType I pyrethroid toxicity. Diazepam or phenytoinis used for seizures.21-24
BUTTON BATTERY INGESTION
Small foreign bodies that are swallowedgenerally pass down the gut without any problem.Passage usually takes 2-6 days but occasionallymay take 2-4 weeks. Most foreign bodies thatcause trouble do so in the oesophagus.Button batteries are used to power digitalwatches, hand held calculators, hearing aids andphotographic equipments. Although these cells aresealed they contain corrosive and toxic chemicals.There are four main types of button cells -mercury, silver, alkaline manganese and lithium.
Lithium cells are mostly used in watcheswhere replacement is mostly by a specialist,thereby limiting access to children. Lithium cellsare more resistant to corrosion than others.Their thin shape may facilitate gut transit. Silvercells are nontoxic when swallowed. Used batteriesare potentially far less toxic than new ones asdischarged cells are less liable to leak or causetissue injury. In discharged mercury cells themercuric oxide is largely converted to elementalmercury which is not absorbed.
When undischarged cells are swallowed theelectric current produced by the battery causesa rise in the pH at the anode surface. It is this(possibly with the short circuit current throughthe tissues) and not leakage from the cell thatcan cause tissue burns.

2009; 11(1) : 47
47
Lodgement in the esophagus can lead tomucosal damage, tracheoesophageal fistula.Exposure to gastric acid is associated with remoterisk of leakage of the cell contents.
The hazard following disassembly of the cellsis confined to mercury cell. This can lead to toxiclevels of mercury in the blood depending uponthe size and state of discharge of the cell.
Management
Identify the type of cell swallowed.Obtain radiograph of the chest and abdomen.Five percent of those who have ingested wouldhave swallowed more than one cell. Lodgementin the nose and esophagus are indications forimmediate removal by endoscopy. Virtually allcells that have reached the stomach will be passedout spontaneously. Unless the cell is too large tonegotiate the pylorus, endoscopic or surgicalremoval is not required. Daily abdominalradiograph should be obtained to show passagefrom the stomach or show cell disassembly. If ithas crossed the pylorus, radiograph once in 4 daysis suggested. Endoscopy is indicated if the cell isin the esophagus, or if it remains fixed to thestomach or gut mucosa for a prolonged period orif there are signs of peritonitis. Endoscopicremoval may be helped by a Foley catheter or amagnet. Induction of vomiting should not beattempted as it does not work and there is atheoretical risk of fatal airway obstruction.Oral antacids may reduce corrosion of the cell.Metaclopramide to enhance gastric emptying andlaxatives to speed up intestinal transit can betried.Patient should be observed for fever,abdominal pain, vomiting, tarry or bloody stools,or decreased appetite and passage of the cell inthe stools.25-26
DEODORANT
Deodorants are a wide range of productsand include aerosol as body deodorants andantiperspirants, room fresheners, etc. while
deodorant blocks are used in toilets. Aerosolsprays, sometimes called pressure packs, aremetal cans containing chemicals under pressurewhich form a cloud of tiny droplets when releasedfrom the can. Aerosol abuse is common in somecountries as it causes a feeling of euphoria.The composition of deodorants are variable.Chemicals such as butane, propane orchlorofluorocarbons are used as propellants tocarry the active chemicals out of the can andothers are used as the active ingredients.The toxicity may be due to one or more of thesechemicals. The toxicity of a few of the chemicalsare listed below.
Para-dichlorobenzene
This is used in solid air fresheners anddeodorant blocks.Liquid air fresheners containwater perfume and detergent rather than para-dichlorobenzene. The amount of para-dichlorobenzene likely to be eaten by childrenwould probably not cause serious poisoning.It causes irritation to the gut causing nausea,vomiting, diarrhoea and abdominal pain along withirritation and redness of the eyes. Erythema andirritation of the skin can occur on contact.Hepaticand neurologic toxicity are also observed.
Management
Following ingestion if the patient is awake,water should be given. Milk and fatty foodsshould be avoided for 2-3 hours. In case ofcontact with skin or eyes, it should be washedthoroughly with soap and water preferably underrunning water for about 15 to 20 minutes.Vomiting is induced if ingestion occurred less than4 hours ago. Supportive care is important.Seizures can be controlled with benzodiazepines.
BUTANE
Butane is a simple asphyxiant on inhalationwith explosive and flammable potential. It is alsoa widely used substance of abuse. The main target

Indian Journal of Practical Pediatrics 2009; 11(1) : 48
48
organs are in the central nervous andcardiovascular systems.
Initial effects: Euphoria, excitation, blurredvision, diplopia, slurred speech, nausea, vomiting,coughing, sneezing and increased salivation occurinitially.
As dose increases, Disinhibition, confusion,perceptual distortion, hallucinations (ecstatic orterrifying), delusions (which may lead toaggressive or risk taking behaviour), tinnitus andataxia follow.Large doses: This may produce nystagmus,dysarthria, tachycardia, CNS depression,drowsiness, coma and sudden death which mayresult from anoxia, vagal inhibition of the heart,respiratory depression, cardiac arrhythmias ortrauma.Management
Supportive and symptomatic care areessential. ECG monitoring is done for at least4 hours. It is better to avoid stimulants(eg. adrenaline or noradrenaline, except forresuscitation). Arrhythmias may respond well toβ blockers (eg. atenolol). Vagal inhibition of theheart can lead to bradycardia or cardiac arrest.Recovery normally occurs quickly once exposurehas ceased but support of the cardiovascular andrespiratory systems may be needed. Seizures arecontrolled with anticonvulsants.TRICLOSAN (5 CHLORO 2 PHENOL)
Triclosan is a phenol derivative used insoaps, mouth washes, tooth paste, handwashesand cosmetics for its antibacterial property.Toxicity
Local skin irritation blisters on local contactnoticed. Internally small amount can be lethal.Cold sweat, circulatory collapse, convulsion, coma,noncardiogenic pulmonary oedema, respiratoryparalysis and death can occur. Long term
exposure may cause drug resistant bacteria andmay be carcinogenicTreatment
Symptomatic care27,28
DETERGENTS
Poisoning usually occurs through ingestion.Detergents fall into three main categories—non-ionic, anionic and cationic. Non-ionic and anionicdetergents are of low toxicity. Only observationis required if respiratory symptoms, suggestive offoam aspiration, are present. Cationic detergents,such as benzalkonium chloride and cetrimide, areless frequently encountered in domestic cleaners.They may produce corrosive effects if aconcentrated solution is consumed. Oral fluidsshould be encouraged and asymptomatic childrenmay be discharged after a short period ofobservation.Dishwasher powders, liquids, and tablets arestrongly alkaline. Accidental ingestion can producesevere corrosive injury, although this is usuallyconfined to the oral mucosa, lips, and tongue.Abdominal pain, vomiting, hematemesis,oseophageal ulcer, melena and oesophagealstricture may result. Respiratory distress, laryngealoedema, hypotension, collapse, irritation, burns,skin necrosis and metabolic acidosis are the otherserious effects.Management
At presentation any remaining productshould be washed from the skin and oral mucosa.Oral fluids should be encouraged. Attempts atneutralisation are dangerous. Further treatment,where required, is supportive. Asymptomaticchildren can be discharged. Oesophageal damagecan occur in the absence of oral burns and parentsshould be advised accordingly. Follow up isrecommended.29-31
Washing powders contain mixtures of enzymes,perfumes, softeners, and anionic and non-ionic
2009; 11(1) : 49
49
detergents. They are of low toxicity and specifictreatment is not required.
NAIL POLISH
Ingredients
Toulene, Bertyl acetates, Ethyl acetates,Dileutyl phthalate.
Toxicity
Poisoning from nail polish is either fromswallowing or breathing it. Nail polish usuallycomes in small bottles and so serious poisoning isunlikely. Increased frequency of micturition,irritation to eyes are observed. Breathlessnessand slow respiration can be due to respiratorysystem involvement. GIT manifestations notedare nausea, vomiting, and abdominal pain.Drowsiness, coma, stupor are features ofCNS involvement.
Treatment
Stomach wash is given. Antihistamines maybe given for allergic reaction. Endoscopy is donefor oesophageal erosion. Irrigation of skin andsupportive care are carried out.
NAIL POLISH REMOVER
Toxic ingredient : Acetone
Toxicity
Polyuria, polydypsia are observed.Respiratory symptoms of shortness of breath andbronchial irritation may be noted. Nausea,vomiting, abdominal pain and fruity odor may bepresent. Stupor, drowsiness and coma are theneurological features.
Investigation: Acetone in blood and urine canbe measured.
Treatment
Enuresis should not be induced. Gastriclavage with 3 – 5% sodium bicarbonate is usefulif done less than 2 hours. Syrup of ipecac may
be used and activated charcoal can be tried.Symptomatic treatment is the mainstay. O2 andaritificial ventilation for hypoventilation andtreatment of circulatory collapse are carried out.Hemodialysis may be done in severe cases.No specific antidote is available.
Acetone free nail polish remover has gammabutyrolactone which is readily converted togamma hydroxy butyrate whose toxicitysymptoms include CNS depression, hypotension,bradycardia, shock, mild respiratory acidosis,upper airway obstruction and pneumothorax.
Treatment
Symptomatic care
GLUE-ON NAIL REMOVER
Toxic ingredient: Acetonitrile which getsconverted to inorganic cyanide via hepaticmicrosomal enzymes.
Toxicity
Vomiting, drowsiness, increase in serumosmolality and osmolal gap, pulmonary oedema.
Treatment
Activated charcoal. 5%dextrose. Sodiumbicarbonate. Sodium thiosulphate. Hyperbaric O2.Amyl nitrite by inhalation.32,33
MATCH STICK POISONING
Match sticks are usually made of potassiumchlorate, sulphur, gum, glass and red phosphorus.
Ingestion of match sticks are usuallyharmless but potassium chlorate when ingestedin large amount (which is usually suicidal) is highlyreactive and toxic.
Toxicity
Toxic dose of potassium chlorate in adults is5 gm. Lethal dose : 15 – 35gm. On ingestion itleads to rapid oxidative destruction of RBCs.It can give rise to methemoglobinemia and

Indian Journal of Practical Pediatrics 2009; 11(1) : 50
50
cyanosis and may progress to renal failure.Hypoxic brain injury can occur. MRI showssymmetric hyperintense signals within deep graymatter and medial temporal lobes consistent withhypoxia caused by potassium chlorate, but thesefindings are non-specific.
Treatment
Gastric lavage with activated charcoal isgiven. Sodium thiosulphate, alkaline diuresis ormethylene blue are used. Exchange transfusionor hemodialysis are done when needed.Hyperbaric oxygen may help. Symptomatictreatment is most useful.34
VACHA/VASAMBU/SWEETFLAG
It is the dried rhizome of the plant Acoruscalamus commonly used in native medicine
Constituents
Volatile oil, Acorin, a bitter principle acoretin,calamine starch, mucilage.Root is a stimulant andaromatic, expectorant, antispasmodic and nervinesedative. Usual dose is 5 – 20 gms. Toxic dose isnot known.
Uses
It is used for diarrhea as an antidote toseveral poisons, counter irritant and asinsecticides. Root is burnt and mixed with coconutoil or castor oil and smeared over the abdomenas antiflatulant.
Side effects
Calamus oil causes hypothermia. Can leadto generalized CNS depression, sedation,hypothermia, hypotension, depression ofrespiration and diarrhoea.
PREVENTION OF HOUSEHOLD ANDCHEMICAL PRODUCTS POISONING
• Use safety locks for all cabinets. Storepotential poisons out of reach of smallchildren.
• Store all poisonous household and chemicalproducts out of sight of children.
• If you are using a product and need to answerthe telephone or doorbell, take the child withyou. Most poisonings occur when the productis in use.
• Store all products in their original containers.DO NOT use food containers such as milkjugs or soda bottles to store household andchemical products.
• Store food and household and chemicalproducts in separate areas. Mistaken identitycould cause a serious poisoning. Manypoisonous products look alike and come incontainers very similar to drinks or food.
• Return household and chemical products tosafe storage immediately after use.
• Use extra caution during mealtimes or whenthe family routine is disrupted. Manypoisonings take place at this time.
• Pesticides can be absorbed through the skinand can be extremely toxic. Keep childrenaway from areas that have recently beensprayed. Store these products in a safe placewhere children cannot reach them.
• Discard old or outdated household andchemical products.
• Take time to teach children about poisonoussubstances.
Points to Remember
• Poisoning due to household agents is aglobal problem in children. They aremainly accidental in those less than5 years of age and intentional in childrenabove 12 years.
• Most of the household agents are takenin small doses and hence do not causetoxicity. In larger doses they exhibit signs

2009; 11(1) : 51
51
of poisoning and occasionally may befatal.
• Symptoms are usually nonspecific andmay mimic other diseases and hence astrong index of suspicion is required inany unresponsive child.
• For most agents gastric lavage is avoidedunless airway is protected. The mainstayof management is good supportive care,as no specific antidote is available.
• Implementation of good safety measuresat home will bring down morbidity andmortality due to poisonings.
Acknowledgement: Mrs. Selvi for secretarialhelp.
References
1. Srivastava A, Peshin SS, Kaleekal T, Gupta SK.An epidemiological study of poisoning casesreported to the National Poisons InformationCentre, AIIMS, New Delhi. Hum Exp Toxicol2005; 24: 485.
2. Dutta A K, Seth A, Goyal P K, et al. Poisoningin children: Indian scenario. Indian J Pediatr1998; 65: 365-370.
3. Fernando R, Nissanka S. Naphthalene. ChemicalSafety Information from IntergovernmentalOrganizations. Website: http://www.inchem.org
4. Chun T, Perrone J, Osterhoudt K, Ugur S,Henretig F. Mothball blues: confusion innaphthalene toxicities and treatment. ClinToxicol 1998; 36: 465.
5. Weintraub E, Gandhi D, Robinson C. Medicalcomplications due to mothball abuse. SouthMed J 2000; 93: 427-429.
6. Santucci K, Shah B. Association of naphthalenewith acute hemolytic anemia. Acad Emerg Med2000; 7: 42-47.
7. Wickstrom E. Camphor. Safety Information fromIntergovernmental Organizations Website:http://www.inchem.org Accessed on 24 Dec.,2007.
8. Siegel E, Wason S . Camphor toxicity. PediatrClin North Am 1986; 33: 375-379.
9. Jimenez JF, Brown AL, Arnold WC . Chroniccamphor ingestion mimicking Reye’s syndrome.Gastroenterology 1983; 84: 394-398.
10. Geller RJ, Spyker DA, Garrettson LK, RogolAD. Camphor toxicity. Development of a triagesystem. Vet Hum Toxicol 1984; (Suppl 2): 8-10.
11. Manoguerra AS, Erdman AR, Wax PM ,et al.American Association of Poison ControlCenters. Camphor Poisoning: an evidence basedpractice guideline for out-of hospitalmanagement. Clin Toxicol 2006; 44: 357-370.
12. Magarey J. Victorian Poison Information Centre.International program on chemical safety.Eucalyptus oil. Website http://www.inchem.orgAccessed on 24 Dec., 2007.
13. Hindle RC Eucalyptus oil ingestion. N Z Med J1994; 185-186.
14. Tibballs J. Clinical effects and management ofeucalyptus oil ingestion in infants and youngchildren. Med J Aust 1995; 163: 177-180.
15. Webb NJA, Pitt WR. Eucalyptus oil poisoningin childhood: 41 cases in south-eastQueensland. J Paediatr Child Health 1993;29:368-371.
16. Sinniah D, Baskaran G. Margosa oil poisoningas a cause of Reye’s Syndrome. Lancet 1981; 1:487-489.
17. Sundarvalli N, Raju BB, Krishnamoorthy KA.Neem oil poisoning. Indian J Pediatr 1982; 49:357-359.
18. Lai SM, Lim KW, Cheng HK. Margosa oilpoisoning as a cause of toxic encephalopathy.Singapore Med J. 1990; 31:463-465.
19. Heick HMC, Shipman RI, Norman MG, et al.Reye syndrome associated with use of insectrepellent in a presumed heterozygote forornithine-carbamoyl-transferase deficiency.J Pediatr 1980; 97: 471-473.
20. Tenenbein M. Severe toxic reactions and deathfollowing the ingestion of Diethyltoluamide-containing insect repellents. JAMA 1987; 258:1509-1511.

Indian Journal of Practical Pediatrics 2009; 11(1) : 52
52
21. Ray DE, Ray D, Forshaw PJ. PyrethroidInsecticides: Poisoning Syndromes, Synergies,and Therapy. Clin Toxicol 2000; 38: 95 – 101.
22. Bradberry SM, Cage SA, Proudfoot AT, ValeJA. Poisoning due to pyrethroids. Toxicol Rev.2005; 24:93-106
23. Forshaw PJ, Lister T, Ray DE. The role ofvoltage-gated chloride channels in type IIpyrethroid insecticide poisoning. Toxicol ApplPharmacol 2000; 163:1-8.
24. Yang PY, Lin JL, Hall AH, Thomas C Y, Tsao,Ming-Shyan Chern. Acute Ingestion Poisoningwith Insecticide Formulations Containing thePyrethroid Permethrin, Xylene, and Surfactant:A Review of 48 Cases. Clin Toxicol 2002; 40: 107- 113.
25. David TJ, FergusonAP. Management ofchildren who have swallowed button batteries.Arch Dis Child 1986; 61: 321-322.
26. Banerjee R, Rao GV, Sriram PV, Reddy PKS,Reddy DN. Button battery ingestion. Indian JPediatr 2005; 72: 173-174.
27. Haris D, Mirza Z. Butane encephalopathy.Emerg Med J 2005; 22: 676 –7
28. Kumar PKP, Ebenezer K, Agarwal I. Deodorants-need for caution. Indian J Pediatr. 2007;74: 876.
29. Riordan M, Rylance G, Berry K. Poisoning inchildren: 4 Household products, plants, andmushrooms. Arch Dis Child 2002; 87:403-406.
30. Einhorn A, Horton L, Altieri M, OchsenschlagerD, Klein B. Serious respiratory consequencesof detergent ingestions in children. Pediatrics.1989; 84: 472-474.
31. Wheeler DS, Bonny AE, Ruddy RM, JacobsBR. Late-onset respiratory distress afterinhalation of laundry detergent PediatrPulmonol. 2003; 35: 323-325.
32. Savage T, Khan A, Loftus BG. Acetone-free nailpolish remover pads: Toxicity in a 9 month old.Arch Dis Child 2007;92:371.
33. Caravati EM, Litovitz TL. Pediataric cyanideintoxication and death from an aceto nitrilecontaining cosmetic. JAMA 1988;260:3470-3473.
34. Hakan M, Emir S, Zekai P, et al. Normal MRimaging finding of potassium chlorateintoxication . Am J Neuroradiol 2003; 24: 1396 –1398.
CLIPPINGS
Dressings for treating superficial and partial thickness burns
Superficial burns are those which involve the epidermal skin layer and partial thickness burnsinvolve deeper damage to structures such as blood vessels and nerves. There are many dressingmaterials available to treat these burns but none have strong evidence to support their use. Evidencefrom small trials, many with methodological limitations, suggests that superficial and partial thicknessburns may be managed with hydrocolloid, silicon nylon, antimicrobial (containing silver), polyurethanefilm and biosynthetic dressings. There was no evidence to support the use of silver sulphadiazine.There is a paucity of high quality RCTs on dressings for superficial and partial thickness burninjury. The studies summarised in this review evaluated a variety of interventions, comparators andclinical endpoints. Despite some potentially positive findings, the evidence, which largely derivesfrom trials with methodological shortcomings, is of limited usefulness in aiding clinicians in choosingsuitable treatments.
Wasiak J, Cleland H, Campbell F. Dressings for superficial and partial thickness burns.Cochrane Database of Systematic Reviews 2008, Issue 4. Art. No.: CD002106. DOI:10.1002/14651858.CD002106.pub3. This version first published online: October 08. 2008

2009; 11(1) : 53
53
TOXICOLOGY
CARDIOTOXINS
* Rashmi Kapoor
Abstracat : Common cardiotoxins whichpediatricians come across are oleander,aconite, digitalis, tricyclic antidepressants andantihypertensives. All cases of suspectedpoisoning with cardiac drugs must be treatedvigorously. The presense or absence ofunderlying heart disease may greatly influenceclinical problems. The pathophysiology,symptoms and signs, diagnosis and treatmentof these substances are discussed.
Key words : Cardiotoxins, Oleander, Aconite,Digitalis, Tricylic antidepressants, Anti-hypertensives.
Accidental toxic exposures resulting in injuryor death is a significant problem before a childreaches health care facility, emergencydepartment and critical care units.
Cardiotoxins are the drugs, over dosage ofwhich affect the heart either directly or throughthe nervous system. Oleander, aconite, digitalis,tricyclic antidepressants, and antihypertensivesare few of the important cardiotoxins we comeacross as childhood poisoning.
OLEANDER
The oleander plants grow wild in India. Itsflowers are used as offerings in the temples.There are two varieties, white (Nerium odorum)and yellow (Cerbera thevetia).
White Oleander (Nerium odorum, Kaner)
All parts of the plant are poisonous.The active principle is “Nerin”, consisting of threeglycosides, viz, Neriodorin, Neriodoreinand Karabin. The principal action ofNeridorin is that of digitalis (see digitalispoisoning), causing death from cardiac failure.Neriodorein causes muscular twitching andtetanic spasms more powerful than strychnine.Karabin acts on the heart like digitalis and onspinal cord like strychnine1. It is an evergreenshrub found in India, China and places withMediterranean climate and is grown as a gardenplant2.
Symptoms and signs: Clinical features includeabdominal pain, vomiting and frothy salivationfollowed by restlessness, bradycardia andtachypnea. There is difficulty in swallowing andmuscular twitching of extremities deepening intotetanic spasms. This is followed by exhaustion,drowsiness, coma and death from heart failure.
Fatal dose and fatal period: About 15 gramsof root can kill an adult in about 24 hours.
Treatment: Airway, breathing and circulationare to be maintained. The patient is connected toa cardiac monitor and observed frequently.Stomach wash will be useful. For bradycardiawith heart rate of less than 40 beats per minuteatropine may be useful. Atropine is used at a doseof 0.02mg/kg with a minimum dose of 0.1mg anda maximum single dose of 0.5mg in a child and1 mg in an adolescent. The dose may be repeatedin 5 minutes to a maximum total dose of 1 mg ina child and 2 mg in an adolescent. Sometimes
* Consultant Pediatrician,Regency Hospital Ltd.,Kanpur, Uttar Pradesh.

Indian Journal of Practical Pediatrics 2009; 11(1) : 54
54
cardiac pacing may be required. Symptomatictreatment, frequent observation, anticipation oflife threatening arrhythmias and their prompttreatment are the key to successful management.Treatment is similar to that of digitalis poisoning.
Yellow oleander (Thevetia, pila kaner)
This plant is highly poisonous. It is a smallornamental tree with bright yellow flowers andfleshy round fruits which are green when unripeand black when ripe. Plant has a milky white sap.
The yellow oleander contains at least eightdifferent cardiac glycosides including thevetin A,thevetin B (cerberoside), thevetoxin, neriifolin,peruvoside and ruvoside. All parts of the plantare dangerous especially the seeds3. Ingestionof oleander seeds is a common mode ofaccidental poisoning in children.
Pathophysiology
The myocardial effects of these compoundsare attributable to increased intracellularconcentration of Ca++ and Na+ resulting frominhibition of transmembrane Na+ / K+ ATPasepump3.
Signs and symptoms
General: It consists of burning sensation in themouth with tingling of tongue, dryness of throat,vomiting and diarrhea. In severe toxicity thesemay be followed by headache, dizziness, dilatedpupils, drowsiness, collapse, coma and death.
Cardiac signs: AV node conduction block, sinusnode block and ventricular tachycardia may occur.A few may reach the hospital in cardiac failureor arrest. There may be severe hyperkalemia.
Fatal dose and fatal period: 8 to 10 seeds or15 to 20 grams of root prove fatal to an adult.Death ensues within 24 hours.
Treatment
After maintaining airway, breathing andcirculation, the child should be connected to acardiac monitor. Gastric lavage is done followedby other symptomatic treatment. Hyperkalemiashould be taken care of. Cardiac pacing may berequired in children having heart rate of less than40/minute. At some centers anti digoxin fabfragments have been used showing good results3.Treatment by and large is similar to that of digoxintoxicity.
ACONITE POISONING
This plant is known as aconitum napellus ormonks’hood. It is grown in the Himalayan rangesin India. Aconide alkaloids are present in the rootsof this plant. The active principles are aconitineand other C19 - diterpenoid alkaloid whichare known neurotoxins and cardiotoxins.With increasing popularity of herbal medicinesamong the general public, herb induced aconitepoisoning is seen even in the western countries.The root extract is used for treating rheumatismand wounds4.
Pathophysiology
Most of the cardiovascular and neurologicfeatures of poisoning with aconitine can beexplained on the basis of its actions on voltage-sensitive Na+ channels in excitable tissues,including myocardium, nerve, and muscle.Aconitine binds with high affinity to the open gateof Na+ channels at receptor site, causingpersistent activation of these channels.This sustained Na+ influx delays the repolarizationphase of the action potential and initiatespremature excitation4.
Symptoms and signs
Patients invariably develop a combination ofneurologic, cardiovascular, gastrointestinal, andother signs and symptoms.

2009; 11(1) : 55
55
CNS: The neurologic features can besensory, motor, or both. CVS: Cardiovascularfeatures include palpitations, chest tightness,hypotension, ectopics, bradycardia, tachycardia,ventricular arrhythmias and pulmonary edema.Gastrointestinal features include nausea,abdominal pain and diarrhea.
Fatal dose and fatal period: One gram of root,250 mg of extract, 25 drops of tincture or 4 mg ofthe alkaloid prove fatal. The latent period betweeningestion of aconite roots and onset of symptomscan be as short as 10 minutes suggesting thataconitine and related alkaloids can be rapidlyabsorbed by the upper gastrointestinal tract. Insome patients, symptoms occur only after a longerlatent period4.
Treatment
After maintaining airway, breathing andcirculation, the child should be connected to acardiac monitor. Gastric lavage is effective ifpatient is brought to the hospital in time.Arrhythmia may be treated by lidocaineor amiodarone. Lidocaine is given at a loadingdose of 1mg/kg IV followed by an infusion20-50 mcg/kg/minute. Refractory arrhythmiasmay require charcoal hemoperfusion for 4 hours.Patients with severe bradycardia may requireatropine or cardiac pacing. The dose ofamiodarone is 5mg/kg IV load over 20-60 minutes(maximum dose 300mg) can repeat to maximumdaily dose of 15mg/kg (2.2g in adolescents).
DIGITALIS
Digitalis remains one of the most frequentlyprescribed proprietary drug in the developedcountries. However, just as all drugs aretherapeutic in one dose but toxic in another, digitalistherapy has always been confounded by a highincidence of inadvertent acute poisonings andchronic intoxications5. Digitalis, digoxin anddigitoxin are prepared from the foxglove plant
Digitalis purpurea. Its roots, leaves, and seedscontain several glycosides of which digitoxin,digitalin, digitalein and digitonin are themost poisonous and have a cumulative action.The glycosides act directly on the heart muscle.
Pathophysiology
Digitalis acts by inhibiting the enzymesodium – potassium ATPase, leading to increasedintracellular sodium and calcium and decreasedpotassium.
Fatal dose and fatal period: The usual fataldose is 15- 30 mg of digitalin and 4 mg of digitoxin.Digoxin is slowly absorbed and distributed, serumlevels may not correlate with the pharmacologiceffects for up to 8 hours. Elimination is primarilyby the kidney and the remainder is metabolizedby the liver. The half life ranges from 36 hours to45 hours.
Symptoms and signs
General: Nausea, vomiting, headache and lossof appetite.
Cardiovascular: Sinus arrhythmias, sinusbradycardia, premature ventricular contractions,bigeminy, ventricular tachycardia and fibrillationscan occur. Ventricular premature beats, oftenregularly spaced in the form of bigeminal rhythmand multifocal ventricular ectopics are typical ofdigitalis toxicity. Further progression of thisprocess, if digitalis is continued, may lead toventricular tachycardia. Another commonmanifestation of digitalis toxicity is disturbancesof conduction. Mild degrees of A-V block(including Wenckebach phenomenon) and evencomplete heart block may develop in the courseof digitalis therapy, indicating drug overdose.The third cardiotoxic manifestation of digitalis isthe production of varieties of junctional (nodal)rhythm. This may emerge as atrioventriculardissociation when sinus rhythm is present or asnodal tachycardia. Finally, evidence of atrial

Indian Journal of Practical Pediatrics 2009; 11(1) : 56
56
irritability may be produced by digitalis, causingatrial extrasystoles and atrial tachycardias,including atrial tachycardia with 2:1 block.The rarest of atrial arrhythmias attributed todigitalis are atrial flutter and fibrillation6.
ECG manifestations: Commonly observedchanges are depression of ST segment, inversionof T wave, shortening of Q-T interval and all typesof arrhythmias.
Central Nervous system: Dizziness,restlessness, headache, hallucinations, psychosis,depression and visual disorders are commonlyseen.
Diagnosis of digitalis intoxication
The proper use of digitalis requires a highindex of suspicion regarding the possibility of toxicreaction. Virtually every arrhythmia may becaused by digitalis. It is therefore proper to regardwith suspicion every form of rhythm disturbanceoccurring in a patient taking digitalis, which wasnot evident before the administration of this drug.The difficulty in the proper interpretation ofarrhythmias occurring in digitalized patients isenhanced by the fact that even the mostcharacteristic arrhythmias caused by digitalistoxicity are not specific and often occur inresponse to factors unrelated to the drug.
Treatment
The management of digitalis intoxication hasrelied upon good supportive care of the patient,early decontamination to remove the drug beforeit is absorbed, palliative medications such asatropine and antiarrhythmic drugs, correction ofmetabolic abnormalities and ventricular pacingfor severe conduction disturbances andbradyarrhythmias. As in any type of drug toxicity,the basic approach to digitalis toxicity is thediscontinuation of the drug. Active therapy ofdigitalis intoxication should only be undertakenwhen the arrhythmia is poorly tolerated (as in theexcessively fast or excessively slow rates).
Attention should be paid to the possiblepresence of potentiating factors, which may needcorrection, such as hypokalemia or hypoxia.In the presence of hypokalemia or total bodypotassium depletion, administration of potassiumchloride is especially efficacious.
Among antiarrhythmic agents used for thetherapy of digitalis intoxication, diphenylhydantoinand propranolol have been most extensivelystudied. Both agents can be used intravenouslyfor termination of digitalis inducedtachyarrhythmias. Lidocaine and procainamidehave also been used successfully in suchinstances6. Procainamide is given at a dose of15mg/kg IV load over 30-60 minutes. Despite bestefforts, severely poisoned patients still die, mostoften from malignant ventricular arrhythmias,asystole or pump failure and cardiogenic shock.However, within the past 15 years, a quietrevolution in the treatment of digitalis intoxicationhas been taking place. The advent ofimmunotherapy, digitalis-specific Fab antibodyfragments (digibind®), has made it possible tosalvage even those moribund patients withadvanced symptoms of digitalis toxicity. Fab isnow widely available in the United States andmany developed countries; its cost, although stillquite high, would perhaps be offset, at leasttheoretically, by a decreased need for prolonged,invasive and expensive monitoring of digitalis-intoxicated patients in the intensive care setting5.
The approximate dose of Fab fragments(mg) is 80 times the digoxin body burden (mg).If neither the dose ingested nor the plasmadigoxin/digitoxin concentration is known, in bothadults and children 380 mg of anti-digoxin Fabfragments should be given. Each vial (38 mg) willbind approximately 0.5mg of digoxin. If amountof digitalis ingested is known the required dosecan be calculated. The dose for elderly patientsor those with renal impairment should be similarto that for those with normal renal function.Fab fragments have a plasma half-life of

2009; 11(1) : 57
57
12-20 hours, but this can be prolonged in patientswith renal impairment. Factors limiting theefficacy of Fab fragments are the dose, theduration of the infusion and any delay inadministration. Guidelines for Fab fragmentadministration in children include (i) dilution to afinal Fab concentration of 1mg/ml in either5% (w/v) dextrose or 0.9% (w/v) sodium chloride;(ii) infusion through a 0.22 micron membrane filterto ensure that no undissolved particulate matteris administered (iii) administration of the total doseover a minimum of 30 minutes; and (iv) avoidingco administration of other drugs and/or electrolytesolutions. Fab fragments are generally welltolerated. Adverse effects attributable to Fabtreatment include hypokalemia and exacerbationof congestive cardiac failure; renal function couldbe impaired in some patients7.
TRICYCLIC ANTIDEPRESSANTS
The tricyclic antidepressants (TCA) are oneof the most common class of antidepressants oftoxicologic significance. They, increasinglyprescribed for multiple indications in children andadults, are responsible for many pediatricpoisonings. They include amitriptyline, nortriptylineand sinequan.
These agents block the neuronal reuptakeof norepinephrine, serotonin and dopamine, in bothcentral and peripheral nervous system8.
Pathophysiology
Tricyclic antidepressants affect theautonomic, central nervous and cardiovascularsystems. TCAs have central and peripheralanticholinergic effects. Acting centrally, theyinhibit re-uptake of neurotransmitters (thebiogenic amines: norepinephrine, serotonin, anddopamine) into presynaptic nerve terminals andinhibit central sympathetic reflexes. Additionally,TCAs block the fast sodium channels of themyocardium, particularly in the distal conducting
system. Based on their effects on the varioussystems, it is clear how TCAs cause toxicity.First, centrally, the change in neurotransmitterscauses delirium, psychosis, lethargy, coma andgeneralized seizures. The exact mechanism forthe seizures is not completely understood. Second,as competitive antagonists of muscarinicacetylcholine receptors and as H1-histamineblockers, TCAs exert central and peripheralanticholinergic effects. Finally, the blockade ofsodium channels in the heart causes the mostdangerous effects: conduction delays anddysrhythmias. The decreased inward movementof sodium at the fast sodium channels slows phasezero of depolarization in the distal conductionsystem and the ventricle, thus slowing ventriculardepolarization and prolonging the QRS complex.Phase 4 is also affected with slowedrepolarization that manifests as QT prolongation.The pathophysiology also comes into play in thedevelopment of Brugada Syndrome (thedevelopment of ST changes in leads V1 to V3because of altered sodium channel flow) in TCAoverdose. The most common dysrhythmiaresulting from TCA overdose is sinus tachycardiasecondary to peripheral anticholinergic action;however, wide complex tachycardia is thecharacteristic cardiac complication. The widecomplex tachycardia can be supraventriculartachycardia with aberrancy or actual ventriculartachycardia. Much of TCA overdose evaluationand disposition has come to depend on thepatient’s electrocardiogram (ECG).
Fatal dose: Ranges from 5 – 20 mg/kg.
Signs and symptoms
Clinical toxicity becomes evident by6 to 8 hours of an overdose and peaks within24 hours. The anticholinergic effects initiallypresent as: General: Dry mouth, ileus, dilatedpupils, urinary retention and mild sinustachycardia. CNS: Effects may be seen at any

Indian Journal of Practical Pediatrics 2009; 11(1) : 58
58
time post-ingestion and include delirium, agitation,restlessness, hallucinations, convulsions, and CNSdepression or coma. Generalized seizures mostoften develop within 1–2 hours of presentation.
CVS: The most life-threatening toxicity remainscardiac dysrhythmias. In general the symptomsconsist of coma, convulsions and cardiacarrhythmias, and in some cases acidosis.A helpful mnemonic to remember the symptomsis TCA or three Cs and an A9.
ECG changes: In either adults or children, theECG is not sensitive or specific enough to be usedalone to diagnose or predict outcome in TCAoverdose. However, the characteristic ECGchanges seen with TCAs serve to confirm TCAtoxicity. Conduction delays such as QRS and QTcprolongation seem to be associated with seizures.Leonard, et al. showed that with the EKGchanges in children, with desipramine andclomipramine included, as in adults, tachycardia,the most common change, along with PR, QRS,and QTc prolongation10.
Management
Protect the airway, ensure adequateoxygenation and ventilation, and establishcontinuous ECG monitoring. Treat arrhythmiaswith sodium bicarbonate only after establishingadequate airway and ventilation. Sodiumbicarbonate narrows QRS complex, shortensthe QT interval, and increases the myocardialcontractility. The goal of sodium bicarbonatetherapy is to raise sodium concentration andarterial pH. This can be achieved by administering1 to 2 mEq/kg bolus infusions until the arterialpH is >7.45. After the bolus administration,sodium bicarbonate may be infused as a solutionof 150 mEq NaHCO3 per liter in D5 W titratedto maintain alkalosis. If hypotension is presentadminister normal saline boluses (10 ml/kgeach)9.
For treatment of seizures induced by TCA,administer benzodiazepines. Phenobarbital maybe preferable to phenytoin in treating seizuresrefractory to benzodiazepines9. Rest of themanagement is supportive.
CALCIUM CHANNEL BLOCKERS
Calcium channel blockers (CCB) arecommonly found in the medicine cabinets of eachhousehold. They have increased in popularitysince their introduction in the 1960s and are nowthe most frequently prescribed class of cardiacmedications. As a result, these medications aremore accessible to the curious toddler than everbefore. The frequency of unintentional pediatricingestions has increased steadily; calcium channeland beta blocker ingestions rank in the top10 causes of drug-toxin-related deaths in childrenunder 6 years of age.
Most accidental pediatric ingestions areasymptomatic, a small number do result incardiovascular instability or even death. Thedihydropyridines, particularly nifedipine, and thephenylalkylamine, verapamil are most oftenimplicated in symptomatic ingestions. Calciumchannel blockers have not been approved for usein the pediatric population; nevertheless,nifedipine, diltiazem, amlodipine, and verapamilare frequently prescribed for hypertensivechildren11.
Pathophysiology
The morbidity and mortality of CCB toxicityare due to conduction system delays and blocks,loss of myocardial contractility, and loss ofsystemic vascular smooth muscle tone. Toxicityof CCBs typically manifests as an exaggerationof the therapeutic response. Verapamil anddiltiazem generally exhibit the most cardiac(negative inotropic and chronotropic) effects, andoverdoses present with bradycardia, heart block,AV conduction disturbances, and myocardial

2009; 11(1) : 59
59
dysfunction. In contrast, dihydropyridineoverdoses present initially with baroreceptor-mediated tachycardia in response to decreasedsystemic vascular resistance. However, asreceptor selectivity is overwhelmed by theavailable CCB and all L-type channels areblocked, bradycardia and sustained hypotensionmay result11. Activation of insulin secretion bythe pancreatic beta islet cells has been shown toproduce hypoglycemia via inhibition of a slowCa++ channel on the cell membrane.
Signs and symptoms
CVS: Bradycardia and hypotension are the maincardiovascular findings. Systemic: Symptoms andphysical findings are related to the physiologicevents. The most common physical finding afterCCB overdose is hypotension. Systemichypoperfusion results in a variety of symptomsranging from mild orthostatic dizzinessaccompanied by nausea and vomiting, to moresevere manifestations including syncope, mentalstatus changes, seizures, cerebrovascularischemic events, renal failure, intestinal ischemia,and liver infarction. Hypoglycemia and acutepulmonary edema (occurring via an unknownmechanism) have also been reported with CCBoverdose.
Fatal dose: Lethal and toxic doses of calciumchannel blockers in humans are poorly described.Inferences on toxic doses are made fromtherapeutic ranges and case reports of toxicingestions.
Management
The initial approach to therapy for calciumchannel blocker overdose is to provideoxygenation and ventilation, continuous ECGmonitoring and frequent assessment. Onset ofsymptoms may be immediate or delayed in casesof sustained release preparations.
The American Academy of ClinicalToxicology states that charcoal administrationmay be considered in the case of potentially toxicingestions up to 1 h after ingestion11. All patientswith significant overdose require close monitoringof blood pressure and hemodynamic status. Intraarterial blood pressure monitoring should beconsidered. Normal saline bolus in a dose of 5 to10 ml/ kg is administered if hypotension is present.The fluid bolus is restricted to 5-10ml/kg to preventpulmonary oedema and careful reassessment isrequired after each bolus. Intravenous calciumto compete at the channel receptors can be usedto support the circulatory system. Use of atropineand transcutaneous pacing to support heart rate,epinephrine and pressors to improve cardiaccontractility and maintain vascular tone, heart-lung bypass, extracorporeal membraneoxygenation to augment cardiac function, andglucagon to support cellular metabolism areindicated, although their therapeutic efficacy inthe calcium channel blocker overdose patient isvariable. High dose insulin combined withsupplemental glucose, improve intracellularmetabolism and have been associated withimproved outcomes11.
HDIDK (High dose insulin with dextrose andpotassium) should be considered if there isan inadequate response to fluid resuscitation.It should be administered with calciumand epinephrine. Calcium should be dosed as10–20 mL of 10% calcium gluconate viaperipherial venous access or 5–10 mL of10% calcium chloride via central venousaccess. Epinephrine is given i.v. at a rate of 1 µg(as the hydrochloride) per minute and increasedas necessary. Before initiation of insulin therapy,blood glucose and potassium concentrationsshould be checked. If they are <200 mg/dLand <2.5 mEq/L, respectively, then dextrose0.25 g/kg of 25% dextrose injection and potassiumchloride (2mEq/kg orally or IV) should beadministered. Regular insulin is administered as

Indian Journal of Practical Pediatrics 2009; 11(1) : 60
60
a 0.1-0.2 unit/kg bolus dose, followed by0.1–0.2 unit/kg/hr adjusted to clinical response.
Because potential adverse effects of insulininfusion include hypoglycemia and hypokalemia,capillary glucose should be monitored every20 minutes for the first hour. Next, serumpotassium and capillary glucose should be checkedhourly. Infusions of dextrose should be startedwith the insulin bolus dose to maintain adequateblood concentrations.
Administering 10% dextrose and0.45% sodium chloride injection at a rate equalto 80% of the maintenance rate is appropriatefor most patients. Potassium should bereadministered if the blood concentration fallsbelow 2.5 mEq/L. The insulin infusion may betapered off once signs of cardiotoxicity begin toresolve12.
A very high dose of vasopressors therapy(norepinephrine and epinephrine) may be requiredfor treatment of bradycardia and hypotension.
BETA ADRENERGIC BLOCKERS
There are a wide variety of therapeuticindications for beta-adrenergic antagonists,better known as beta-blockers. They are mostcommonly used in cardiovascular disease.Other indications include migraine headache,tremor, panic attacks, and as medications todecrease intraocular pressures. In the pediatricpopulation, betablockers are used primarily to treathypertension, dysrhythmias, thyrotoxicosis, andmigraine headache.
Pathophysiology
Beta adrenergic blockers compete withnorepinephrine and epinephrine at the betaadrenergic receptor, resulting in bradycardia, anddecreased cardiac contractility9. Seriousmorbidity and mortality from beta-blockeroverdose is generally the result of cardiovascular
toxicity. In addition, beta-blockers also possessthe ability to block fast sodium channels, whichis sometimes called membrane stabilizingactivity (MSA). Sodium channel blockade isgenerally believed to be an important patho-physiologic process underlying beta-blockertoxicity. MSA-related myocardial toxicity resultsin decreased contractility, bradycardia andconduction delays, all of which may contribute tohypotension. High lipid solubility also allows forrapid diffusion of the drug across the blood-brainbarrier. The subsequent central nervous system(CNS) toxicity can lead to sedation, delirium andcoma. Seizures may result from hypotensionor a direct CNS effect. Bronchospasm andhypoglycemia are a direct result of betablockadeat the β2 receptors13.
Signs and symptoms
CVS: Bradycardia, bradyarrhythmias, conductiondelays, and severe hypotension are the main signsof cardiovascular toxicity.
CNS: Sedation, delirium, seizures and coma mayoccur. Others: Bronchospasm and hypoglycemiamay also be seen.
Management of serious beta-blockeroverdose
The initial approach to therapy for beta blockeroverdose is to provide oxygenation and ventilation,continuous ECG monitoring and frequentassessment. Onset of symptoms may beimmediate or delayed in cases of sustainedrelease preparations.
Patients with suspected significant beta-blocker overdose toxicity should be placed on acardiac monitor, have frequent blood pressuremonitoring, a 12-lead electrocardiogram (ECG),and a serum glucose determination. If congestiveheart failure is suspected, chest radiograph andoxygen saturation should be obtained.

2009; 11(1) : 61
61
Pharmacologic distinctions between beta-blockers and CCBs may not be evident uponpresentation; therefore, initial treatment effortsshould be similar regardless of the type of druginvolved based on general overdose treatmentguidelines, after ensuring that the airway,breathing, and circulation are intact, GITdecontamination with orogastric lavage, activatedcharcoal, or whole bowel irrigation should beadministered12.
In addition to decontamination, therapies tosupport perfusion are often needed in cases ofoverdose. I.V.fuids (5-10 ml/kg as a bolus dose)should be used as first-line therapy for patientswho develop hypotension. Atropine sulfate0.5–1 mg i.v. is usually the first-line agent forsymptomatic bradycardia. In any pediatric betablocker exposure with the potential for serioustoxicity such as those involving a large numberof ingested pills, atropine should be given prior tolaryngoscopy or gastric cannulation, or in thepresence of persistent vomiting.
Current antidotal therapy for beta -blockerpoisoning is based on animal studies and casereports. Unfortunately, no prospective humanstudy evaluating optimal therapy has beenperformed. These therapies include beta agonists,glucagon, and phosphodiesterase inhibitors.Of these agents, glucagon is generally recognizedas first-line therapy.
High-dose glucagon is recommended forcardiotoxicity produced by beta-blocker poisoning.Glucagon is thought to activate adenylate cyclasein cardiac tissue by directly stimulating a G proteinon the beta-receptor complex.
An initial bolus dose of 50–150 µg/kgshould be administered i.v. over one to twominutes. This initial dose will have a transienteffect that should occur within approximately fiveminutes. If a benefit is seen, the initial dose shouldbe followed by a continuous i.v. infusion at a rate
of 2–5 mg/hr (maximum: 10 mg/hr) diluted in5% dextrose injection. The infusion rate can thenbe tapered downward as the patient improves12.
Approach to management ofCardiotoxins
General management14
Once poisoning is suspected evenasymptomatic patients must be admitted forobservation. In the symptomatic patient supportfor cardiac and pulmonary function is essential.The minimum duration of observation should bedetermined with reference to the drug’s half lifeand the formulation taken (some antiarrhythmicsand hypotensive agents are formulated forsustained release) and when practicable shouldbe guided by plasma drug concentrations.If immediate admission to an intensive care unitis not possible or not indicated the ward staffshould be fully aware of the risks and the intensivecare unit informed that its services may be needed.
A twelve lead electrocardiogram should beobtained as soon as possible, both to assessunderlying myocardial disease and as a baselineto measure progress. A chest radiograph, fullblood count, and samples for laboratory analysisshould also be taken early. If the drugs wereingested as a single dose the stomach should beemptied either by emesis or gastric lavage.Activated charcoal (AC) is an effective adsorbentfor all cardiac drugs and should be given orally ina dose at least 10 times the weight of thesuspected overdose (General recommended doseof AC is 1g/kg in children upto 1 year of age,25-50g in children 1-12 years of age and 25-50gin adolescents and adults).
Supportive
1) Treat all suspected cases seriously,2) support cardiac and pulmonary function,3) empty stomach and give oral activatedcharcoal, 4) avoid artiarrhythmic drugs,

Indian Journal of Practical Pediatrics 2009; 11(1) : 62
62
5) consider temporary pacemaker forbradycardia, 6) use fluids before vasopressorsfor hypotension: administer fluid boluses of5-10ml/kg slowly over 10-20 mins with carefulreassessment after each bolus, 7) persist withcardiac massage if output fails.
Whilst supportive treatment is in progress:Measure electrolytes, urea, creatinine andplasma drug concentrations, urgent correction ofhyperkalemia, correct hypokalaemia, maintainingpotassium in upper normal range, consider othertreatments, antibodies for digoxin, haemo-perfusion for disopyramide, glucagon/isoprenalinefor beta blocker, calcium for verapamil.
Prevention
Childhood poisoning is usually accidental,which makes it amenable for prevention.Most cardiotoxic drugs are either being consumedby an adult member of the household or by thechild himself/herself due to some cardiac lesion.It is important to protect children, because theycannot protect themselves. It is the duty of allmembers of the household to store thesepotentially toxic drugs/herbs with following pointsin mind:
• They should be stored at a place which isbeyond the reach of a child.
• They should not be stored in containers thatare used to store food.
• Make it a habit to properly close the pillbottles tightly after opening them.
• Explain to the child that the flowers forprayers are not to be consumed.
• Keep the herbs away from the child’s reach.
Points to Remember• Acute poisoning with cardiac drugs is
uncommon. They have a narrow toxic totherapeutic ratio and are the mosthazardous drugs in common use.
• In general poisoning with cardioactivedrugs will produce hypotension and alltypes of arrhythmias. Extracardiac effectsinclude gastrointestinal symptoms,especially nausea and vomiting, andcentral nervous system effects withirritability, convulsions, and loss ofconsciousness.
• In the critically ill patient while activatedcharcoal, continuous renal replacementtherapy and specific antidotes may be ofbenefit, maintenance of the patient’sairway, ventilation and circulation stillremain the most important aspect ofmanagement.
REFERENCES
1. Parikh C K. Cardiac poisons In: Parikh’s textbook of Medical Jurisprudence, forensicmedicine and toxicology. 6
th Edn, CBS
Publishers, Mumbai, 1999; pp10:62-10:68.2. Henry JA, Wiseman HM. Management of
poisoning A hand book for health care workers.World Health Organization Geneva 1997; pp277-278.
3. M Eddleston, Warell DA. Management of acuteYellow Oleander Poisoning. Q J Med 1999; 92:483-485.
4. Chuan LC, Thomas CYK, Fang DJ. ClinicalFeatures and Management of Herb-InducedAconitine Poisoning. Ann E Med 2004; 43: 574-579.
5. Alan W. Revising the Management of DigitalisPoisoning. Clin Toxicol 31; 2: 275 – 276.
6. Selzer Arthur, Keith CE. Production,Recognition and Treatment of DigitalisIntoxication. Western J Med 113; 4: 1-7
7. Flanagan RJ, Jones AL. Fab antibodyfragments: some applications in clinicaltoxicology. Drug Saf 2004; 27;1115-1133.
8. Rodgers GC, Matyuns J N and Jr. Poisoning In:Nelson Text book of Pediatrics 17
thEdn, W.B
Saunders Company, Philadelphia pp2362-2375.

2009; 11(1) : 63
63
9. Hazinski MF, Zritsky AL, Nadkarni VM, HickeyRW, Schexnayder SM, Berg RA eds, PALSProvider Manual. Dallas, Texas: American HeartAssociation/American Academy of Pediatrics,2002; pp305-335.
10. Rosenbaum TG, Kou M. Are one or twodangerous? Tricyclic antidepressant exposurein toddlers. J E Med 2005; 28: 169–174.
11. Ranniger C, Roche C. Are one or two dangerous?Calcium channel blocker Exposure in toddlers.J E Med 2007; 33: 145–154.
12. Shepherd G, Clinical reviews cardiovasculardrugs. Treatment of poisoning caused by beta-adrenergic and calcium-channel blockers. Am JHealth-Syst Pharm 2006; 63: 1828-1835.
13. Love J N, Sikka N. Are 1- 2 tablets dangerous?Beta-blocker exposure in toddlers. J E Med 2004;26: 309-314.
14. John H, Glyn V. ABC of Poisoning. Br Med J1984; 289: 1062- 1064.
Percutaneous central venous catheters versus peripheral cannulae for delivery ofparenteral nutrition in neonates
More trials are needed to determine whether delivering nutrition into superficial or deepveins is better for newborn infants. Preterm or sick newborn infants are often fed with aspecial nutrient solution that is delivered directly into the veins. The solutions can either begiven into a superficial vein through a standard short (peripheral) cannula or into a large deepvein via a long (central) catheter. This review found limited data from five small randomisedcontrolled trials that compared the effects of using these two different methods of deliveringnutrient solutions. There is some evidence from one study that infants who received the solutioninto a deep vein received more nutrition. The use of central catheters has been thought toincrease the risk of bloodstream infection in newborn infants, but this review did not find anyevidence that this was the case. More trials are needed to determine which method is better atimproving growth and development in newborn infants. Data from one small study suggest thatusing a percutaneous central venous catheter to deliver parenteral nutrition improves nutrientinput. The significance of this in relation to long-term growth and developmental outcomes isunclear. Three studies suggested that the use of a percutaneous central venous catheter decreasesthe number of catheters/cannulae needed to deliver the nutrition. No evidence was found tosuggest that percutaneous central venous catheter use increased the risk of adverse events,particularly systemic infection.
Ainsworth S, Clerihew L, McGuire W. Percutaneous central venous cathetersversus peripheral cannulae for delivery of parenteral nutrition in neonates. CochraneDatabase of Systematic Reviews 2007, Issue 3. Art. No.: CD004219. DOI: 10.1002/14651858.CD004219.pub3. This version first published online: April 19. 2004. Lastassessed as up-to-date: July 08. 2008
CLIPPINGS

Indian Journal of Practical Pediatrics 2009; 11(1) : 64
64
TOXICOLOGY
* Professor and Head, Pediatric Intensive Care Unit,Christian Medical College and Hospital,Vellore, Tamilnadu.
NARCOTIC POISONING INCHILDREN
* Kala Ebenezer
Abstract:Narcotic poisoning is not commonlyseen in pediatric practice. They meritparticular attention because of the potentialmortality they cause when untreated and therelative ease of reversing their effects ifrecognised.
Key words: Narcotics, Poisoning
Narcotics or more specifically opioids are agroup of drugs used for pain relief. They all causeanalgesia without loss of consciousness coupledwith euphoria, the intensity of which varies witheach drug.
Most narcotics do not produce serious sideeffects in therapeutic dosage. However, the directdepressant effect on respiration which they allshare can be life threatening when recommendeddosages are exceeded.
Narcotics have been abused for theireuphoric action and for the feeling of well beingthat they produce. Tolerance and physical andpsychological dependence develop quickly leadingto addiction and withdrawal symptoms. Narcoticuse and abuse have been reported as increasingin frequency in the past few years, a trend thathas been blamed on increasing availability andutilization of narcotics by medical personnel, aswell as illicit drug abuse.
Opium is known to humans since prehistorictimes. There are evidences that the poppy plantwas cultivated in the ancient civilisations of Persia,Egypt and Mesopotamia. Opium is obtained bylacerating the immature seed pods of the poppyplant and it contains about 25 alkaloids.Many synthetic derivatives are also available forclinical use. Table 1, shows the important opioidsclassifed according to their action.
Table 1. Shows the important opioidsclassified according to their action.
Strong agonists MorphinePethidineFentanylMethadoneHeroinRemifentanilAlfentanilSulfentanil
Moderate agonists CodeineOxycodonePropoxyphene
Mixed agonists (partial agonist and antagonists) Buprenorphine
ButorphanolNalbuphinePentazocine
Antagonists NaloxoneNaltrexone

2009; 11(1) : 65
65
The most frequently prescribed opioids inclinical medicine are morphine, pethidine, fentanyl,fortwin (pentazocine), codeine and methadone.Heroin (diacetylmorphine), the most commonlyabused narcotic, available only illicitly, is notprescribed in clinical practice.
Opioid receptors
Opioids exert their action through the opioidreceptors, the µ (mu) and ê (kappa) receptors inthe central and peripheral nervous system,particulary brain stem, substantia nigra of spinalcord, limbic system and hypothalamus.µ receptors found in the brain stem mediaterespiration, cough, nausea, vomiting, andmaintenance of blood pressure, pupillary size andcontrol of stomach secretions while ê (kappa)receptors in spinal cord and thalamus mediateanalgesia.
Narcotic poisoning
Opioid overdosage is not commonly seen.Literature search shows they constitute about3.8-5.1% of ED presentations in U.S.A.Although opioids constitute a relatively smallpercentage of pure overdoses encountered in theED, they merit particular attention because of thepotential mortality they cause when untreated andthe relative ease of reversing their effects.
Opioids are prescribed often in combinationwith other analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs) or musclerelaxants. They are frequent ingredients of coughmixtures. Overdosage in children could occuraccidentally or intentionally. Drug abuse andinadvertent overdosage by adolescents is a causefor poisoning. Unintentional medical and nursingerrors have also been described as a potentialsource for overdosage.
Clinical presentation
Opiate toxicity should be suspected whenthe clinical triad of CNS depression, respiratory
depression and miosis are present. Respiratorydepression is the most predominant cause ofmortality in opioid overdosage. Both bradypneaand hypopnea are observed. Rates as slow as4-6 breaths per minute often are observed withmoderate-to-severe intoxication. The body retainsthe hypoxic drive to breathe but may beoverridden by the CNS sedative effects of asevere overdose.
Acute mental changes and euphoria aresometimes seen. Seizures are not common butoccur with pethidine, dextromethorphan,propoxyphene, tramadol. Seizures occur mostcommonly in infants because of CNS excitation.Seizures may also occur in patients with renaldysfunction who receive repeated doses ofpethidine owing to accumulation of norpethidine.
Cardiac toxicity, ventricular arrhythmiassimilar to that seen with tricyclic antidepressantsand quinidine can occur particularly withpropoxyphene. Noncardiogenic pulmonaryedema may occur.
Reliance on miosis to diagnose opioidintoxication can be misleading. If sufficientlysevere, hypertension and pupillary dilation maypresent because of CNS hypoxia. Morphine,pethidine, pentazocine, diphenoxylate/atropine(Lomotil), and propoxyphene sometimes areassociated with mydriasis or midpoint pupils.
Mild peripheral vasodilation may occur andresult in orthostatic hypotension. However,persistent or severe hypotension should raise thesuspicion of co-ingestants and needs promptreevaluation. Pink frothy sputum, dyspnea andbronchospasm strongly suggest pulmonaryedema.
Nausea and vomiting even if present initiallyare transient. Nightmares, anxiety, agitation,euphoria, dysphoria, depression, paranoia, andhallucinations are encountered infrequently, mainly

Indian Journal of Practical Pediatrics 2009; 11(1) : 66
66
with high doses. Pruritus, flushed skin, andurticaria, conjunctival injestion may arise becauseof histamine release. Hearing loss has beenassociated with heroin and alcohol but is generallyconsidered recoverable. Needle marks may beseen indicative of drug abuse.
Table 2. Acute and chronic effects of opioids
AcuteAnalgesia VomitingRespiratory depression MiosisSedation ConstipationEuphoria Urinary retentionCough suppression Biliary spasm
ChronicTolerance Physical dependence
MetabolismPeak effects of opioids generally are
reached in 10 minutes with the intravenous route,10-15 minutes after nasal insufflation(eg, butorphanol, heroin), 30-45 minutes with theintramuscular route, 90 minutes with the oral route,and 2-4 hours after dermal application(ie, fentanyl). Toxic doses may have delayedabsorption because of delayed gastric emptyingand slowed gut motility.
Most opioids are metabolized by hepaticconjugation to inactive compounds that areexcreted readily in the urine. Neonates, owing totheir low hepatic glucuronidase activity arepredisposed to toxicity and lower doses shouldbe used. All opioids have a prolonged duration ofaction in patients with liver disease (eg, cirrhosis)because of impaired hepatic metabolism. Thismay lead to drug accumulation and opioid toxicity.
Opiate metabolites are excreted in the urine,making urine toxicology useful. Renal failure alsoleads to toxic effects from accumulated drug oractive metabolites.
Regardless of the mode of administration,narcotics taken by a pregnant addict readily passthe placental barrier and are capable of producingeffects on the infant in utero and after birth.
Investigations
Drug screens are most sensitive whenperformed on urine. Positive results are observedup to 36-48 hours post exposure, but widevariations are possible depending upon testsensitivity, dose, route, and the patient’smetabolism. However in uncomplicated patientsthey rarely alter management.
In patients with moderate-to-severe toxicity,performing baseline studies, including a CBC,comprehensive metabolic panel, and arterial bloodgas determinations, is appropriate. Blood glucoseshould not be forgotten.
Chest radiographs are obtained if pulmonaryedema is suspected. Abdominal film may behelpful when evaluating a suspected body stufferor body pack. An ECG should be obtained on allpatients with intentional overdose (possiblecardiotoxic co-ingestants) or those with significanttoxicity.
Treatment
Emergency and supportive measures:
Emergency management hinges onaggressive airway control, supplemental oxygenand intubation for respiratory depression or incomatose patients.
• Stomach wash may be given if patientspresent within 2 hours.
• Activated charcoal (1g/Kg) is theGI decontamination method of choice forpatients with opiate intoxication followingingestion. Because of impairment of gastricemptying and GI motility produced by opiate

2009; 11(1) : 67
67
intoxication, activated charcoal still may beeffective when patients present late followingingestion.
• Naloxone is the specific antidote. The doseis 2 mg in the adult and 0.1 mg/kg in the childor infant. Doses may be repeated up to amaximum cumulative dose of 10 mg.
• The onset of effect following IV naloxoneadministration is 1-3 minutes; maximal effectis observed within 5-10 minutes. Clinicalreversal occurs within 5-10 minutes andpatient quickly awakens.
• A repeat dose is indicated for partial responseand can be repeated as often as needed.Repeat doses of 2 mg can be given every 3-5 minutes as needed, up to a total of 10 mg.Reconsider the diagnosis if the patient failsto respond after 10 mg.
• Naloxone can be administered intramus-cularly, via endotracheal tube, intraosseouslyor intralingually.
• Constant infusions are particularly useful foroverdoses of long-acting opioids, such asmethadone. Larger doses of naloxone maybe required for diphenoxylate/atropine(Lomotil), methadone, propoxyphene,pentazocine, and the fentanyl derivatives.
Aggressive airway control must takeprecedence over pharmacologic reversal becausethe vast majority of morbidity and mortality resultfrom respiratory depression.
Points to Remember
• Morphine, pethidine, fentanyl andpentozocine are some of the commonlyprescribed opioids for pain relief.
• Uncommon overdosage and poisoning dooccur occasionally.
• The clinical triad of depressed consciousstate, respiratory depression and pupillarymiosis are characteristic of narcoticoverdosage.
• Naloxone is the specific antidote.
Bibliography
1. Way WL, Fields HL, Schumacher MA. Opioidanalgesics and antagonists. In: Katzung BG, ed.Basic and clinical Pharmacology. NewYork:Lange medical books/McGraw-Hill, 2001; pp512-531.
2. Opioid analgesics and antagonists. In: HarveyRA, Champe PC, eds. Lippincott’s illustratedreviews: Pharmacology. Baltimore: LippincottWilliams & Wilkins, 2006; pp157-168.
3. Unintentional poisoning deaths - Unitedstates.1999-2004. MMWR Morb Mortal WklyRep. 2007; 56:93-96.
4. Everett Stephens. Toxicity, Narcotics. http://emedicine.medscape.com/article/815784-overview.
5. Blatman S. Narcotic poisoning of children(1) Through accidental injestion of methadoneand (2) in utero. Paediatrics 1974; 54:329-332.
6. Albertson TE. Opiates and opioids. In: OlsonKR, ed. Poisoning and overdose. California:Prentice Hall International, 1999; pp242-243.
ERRATUM
To read the designation of Dr.Swati Y Bhave as Visiting Consultant, Indraprastha Apollo Hospital,New Delhi. Executive Director, AACCI (Association of Adolescents and Child Care in India)instead of the designation published in 2008; 10(4):347 issue, which is an error, for which we regret.
The Editorial Board, IJPP.

Indian Journal of Practical Pediatrics 2009; 11(1) : 68
68
INTRAUTERINE GROWTHRETARDATION: JOURNEYFROM CONCEPTION TOLATE ADULTHOOD
* Neelam Kler** Naveen Gupta
Abstract:Understanding of Intrauterinegrowth retardation (IUGR) gains importancebecause of significant perinatal morbidityand mortality related to them. It is essential todifferentiate fetus that is constitutionally smallfor gestational age (SGA) and whose growthhas been restricted in utero. IUGR represent23.8% of the newborns in developingcountries. Factors affecting fetal growth,pattern of fetal growth, their postnatal growthand development, the relation of fetal originof adult disease and future perspectives etcare discussed in this article.
Key words: IUGR, Factors, Growth andDevelopment, Adult disease.
Background
Monitoring the well being and growth ofthe fetus is a major purpose of antenatal care.Many fetuses delivered with a lower thanexpected birth weight are healthy, thriving infants;whereas others are small because their growthin utero has been impaired and they haveincreased perinatal morbidity and mortality.
GENERAL ARTICLE
A distinction therefore needs to be madebetween the fetus that is constitutionally smallfor gestational age (SGA) and one whose growthhas been restricted in utero. A diagnosis of growthrestriction implies that a fetus has not achievedits optimal growth potential; a prerequisite formaking this assessment is that the expectedgrowth pattern of the fetus could have beenpredicted. Although ultrasound biometry in secondtrimester may give some suggestion of expectedgrowth, in practice it is only with serialmeasurements (either clinically or withultrasound) that reduced growth velocity can bedemonstrated.
In many discussions of linear growthretardation there is a need to address arguablythe most important phase of human growth -Growth from conception to term.
Questions that come to mind include: 1) Canchildren be programmed in utero to be linearlygrowth retarded after birth? 2) What are therelationships between intrauterine growthretardation (IUGR) and postnatal growth?
Depending on its growth in utero, thenewborn baby can be categorized as a healthyfull-term (FT) infant within the normal birth weightrange; a macrosomic infant above the normal birthweight range; or an infant of low birth weight(ILB). Regarding the latter, WHO estimates areof great interest: they show that approximatelytwo-thirds of all infants of low birth weight bornin the developed world are true pre-term (PT)infants and one-third are small-for-gestational-age(SGA). This relationship is reversed in thedeveloping world, where about 75% of ILB are
* Chairperson,** DNB Fellow,
Department of Neonatology,Sir Ganga Ram Hospital

2009; 11(1) : 69
69
SGA. The much higher proportion of SGA infantsin the Third World seems to be due primarily tomalnutrition and infection and should thereforebe preventable.
Quantum of problem
At least 13.7 million infants are born everyyear at term with low birth weight (LBW),representing 11% of all newborns in developingcountries. This rate is approximately 6 timeshigher than in developed countries. LBW, definedas < 2500 g, affects 16.4% of all newborns, orabout 20.5 million infants each year. IUGR,defined as birth weight below the 10th percentileof the birth-weight-for-gestational-age referencecurve, represents 23.8%, or approximately30 million newborns per year. Overall, nearly 75%of all affected newborns are born in Asia - mainlyin South-central Asia - 20% in Africa and about5% in Latin America. Although some of theseare healthy, small infants who merely representthe lower tail of a fetal growth distribution, in mostdeveloping countries a large proportion ofnewborns suffer from some degree of intrauterinegrowth retardation. These data demonstrate thatmany developing countries currently exceed theinternationally recommended IUGR (> 20%) andLBW (> 15%) cut-off levels for triggering publichealth action, and that population-wideinterventions aimed at preventing fetal growthretardation are urgently required.
Factors affecting fetal growth
The principal determinants of fetal growthare fetal genotype and in utero environment.Environmental factors include maternal andpaternal genetics, maternal size, and the capacityof the placenta to provide nutrients to the fetus.These environmental factors interact with theintrinsic growth pattern of the fetus, yielding aparticular rate and composition of fetal growth.Most of the variation in fetal growth in a populationis due to variations in environmental factors, not
the fetal genome, although a genetically abnormalfetus clearly might not grow as well as a normalfetus if affected genes include those that areimportant for growth.
Genetic factors: Many genes contribute to fetalgrowth and birthweight. Techniques in whichspecific genes can either be deleted (“knockouts”)or overexpressed have led to greater under-standing of how some of these genes regulate fetalgrowth. Such studies have shown that bothmaternal and paternal influences are presentduring fetal development and are passed on tothe developing fetus by spermatozoa or oogoniaby a mechanism called imprinting. Although thematernal genetic composition exerts greaterinfluence than fetal genotype in the overallregulation of fetal growth, both maternal andpaternal genomes are important in fetal growthand development.1 For example, gynogeneticzygotes (two maternal genome copies) lead tounderdeveloped extraembryonic tissues but well-developed embryos. The more modest regulationoffered by the paternal genotype is essential fortrophoblast development. For example, zygotenuclear transfer experiments have shown thatandrogenetic zygotes (two paternal genomecopies) develop extensive trophoblast tissues butcontain underdeveloped embryonic tissues.
Although several genes have been describedas maternally or paternally imprinted, insulin-likegrowth factor I (IGF-I) and IGF-II are two proteinproducts of genes that specifically regulate thedevelopment of trophoblast cells, which form theplacenta. Gestational profiles of IGF-II,IGF-binding proteins, and IGF receptors (types1 and 2) suggest they are involved in enhancingplacental growth.2 Additionally, IGF-II mayregulate placental growth directly, as evidencedby 60% placental and fetal growth restriction inmice lacking IGF-II, which implicates IGF-II inthe proliferation of trophoblast cells.

Indian Journal of Practical Pediatrics 2009; 11(1) : 70
70
Non genetic maternal factors: Uterine Size:Under usual conditions, fetal growth follows itsgenetic potential, unless the mother is unusuallysmall and limits fetal growth by a variety of factorsconsidered collectively to represent “maternalconstraint.” Maternal constraint results primarilyfrom a limited uterine size and, thus, the capacityto support placental growth and nutrient supplyto the fetus, not to any particular genetic factor.A clear example of maternal constraint is thereduced rate of fetal growth of multiple fetusesin humans,3 who optimally support only one fetus(Fig. 1).
Fetal growth constraint from the maternalenvironment is a physiologic process that includesthe maternal-specific capacity of uterine size,placental implantation surface area of the uterus,and uterine circulation, which together support thegrowth of the placenta and its function.
Obviously, small fetuses of small parents orlarge fetuses of large parents do not reflect fetalgrowth restriction or fetal overgrowth,respectively. Their rates of growth are normal
for their genome and for maternal size.Unless maternal constraint is particularlyprominent, such fetuses would not grow faster orto a larger size if more nutrients were provided.
Pattern of gestational growth
In most species, fetal weight tends toincrease exponentially in the middle part ofgestation, but there is considerable interspeciesvariation. In humans, cross-sectional evaluationsof newborn weight versus gestational age tendsto produce a typical S-shaped curve, with anapparent slowing of fetal growth rate in the thirdtrimester following the mid-gestational exponentialincrease in fetal weight.4 In contrast, more recentultrasonographic observations show that humanfetal growth is linear over the latter third ofgestation, with no tendency for slowing of fetalgrowth that would produce the flattening of thefetal growth curve derived from the cross-sectional studies.5 The apparent slowing of growthderived from cross-sectional data most likely isdue to miscalculation of gestational dates, withinclusion of more preterm infants.
Fig. 1. Mean birth weights of single and multiple fetuses related to durationof gestation.

2009; 11(1) : 71
71
The length of gestation is more stronglycorrelated with growth of neural tissue(range, 0.015 to 0.033 g1/3/d—a 2.2-fold range)than with growth of the fetal body (range, 0.033to 0.25 g1/3/d—a 7.6-fold range). The physiologicsignificance of this relationship is not known, butintrauterine development of a large brain/bodymass ratio in humans is favored in a single fetusand is made possible by a slow rate of somaticgrowth. The latter allows a steady increase in fetalcerebral metabolic demand while the totalmetabolic demands of the conceptus are keptwithin limits that the mother can easily supportwithout stress on her own metabolism.
Maternal nutrition: Normal variations inmaternal nutrition have relatively little effect onfetal growth because they do not markedly altermaternal plasma concentrations of nutrientsubstrates or the rate of uterine blood flow, theprincipal determinants of nutrient substratedelivery to and transport by the placenta. Humanepidemiologic data from conditions of prolongedstarvation as well as nutrition deprivation inexperimental animals indicate that even severerestrictions in maternal nutrition only limit fetalgrowth by 10% to 20%.6 Calorie and proteinintakes must be reduced to less than 50% ofnormal for a considerable portion of gestationbefore marked restrictions in fetal growth areobserved.7 Such severe conditions often result infetal loss before late gestation fetal growth rateand fetal size at birth are affected. Similarly, fetalmacrosomia is only common in pregnanciescomplicated by gestational diabetes mellitus inwhich maternal plasma hyperglycemia andhypertriglyceridemia combine with fetalhyperinsulinemia to produce excessive fetaladiposity.
The placenta: Endocrine and architecturalcharacteristics of the placenta provide anadequate supply of nutrients for the developingfetus, a site for nutrient uptake and waste removal,
and a line of defence against pathogens. Membersof the GH/PRL gene family produced only in theplacenta include placental lactogen (PL), growthhormone (human (h)GH-V), and prolactin-relatedproteins (PRP).8 PL is believed to have a pivotalrole in the growth and development of the fetusby coordinating metabolic and nutrient supplyfrom the mother to the developing fetus to promotegrowth.
The placenta exerts strong control over fetalgrowth by providing nutrients directly or inmetabolically altered forms and amounts.Naturally and experimentally, placental growthprecedes fetal growth and failure of the placentato grow is directly associated with subsequentdecline in fetal growth.
Characteristically, therefore, limitations ofplacental transfer of nutrients to the fetus directlylimit fetal growth. A direct relationship betweenfetal weight and placental weight in humansindicates that large-for-gestational age (LGA),average- or appropriate-for-gestational age(AGA), and small-for-gestational age (SGA)infants are directly associated with LGA, AGA,and SGA placentas (Fig. 2).9 Clearly, placentalsize and fetal size are directly interrelated, althoughfunctional interrelationships between placenta andfetus also are important to fetal growth anddevelopment.
Fetal growth in normal and IUGRbaby
Fetal growth restriction can occur during anyor all periods of gestation. During the embryonicperiod, growth occurs primarily by increased cellnumber (hyperplasia); in the middle of gestation,cell size also increases (hypertrophy) and the rateof cell division stabilizes. In later gestation, therate of cell division declines, but cell size continuesto increase. Thus, insults that limit fetal growth inearly gestation result in global reduction in fetalgrowth. Insults in later gestation usually limitgrowth of specific tissues, such as adipose tissue

Indian Journal of Practical Pediatrics 2009; 11(1) : 72
72
Fig 2. Mean placental weights for large-for-gestational-age ( ), average-for-gestational-age (•), and small-for-gestational-age ( ) human infants at eachgestational age. ± SEM given only for average-for-gestational age infants.
and skeletal muscle, that primarily develop duringthis period and spare other organs and tissues,such as the brain and heart, whose growth ratealready has slowed.Water: Total body water content in the normalfetus increases over gestation, but fetal total bodywater content as a fraction of body weightdecreases due to relative increases in protein,mineral and fat accretion. Extracellular water also
decreases more than intracellular water asgestation advances, primarily because ofincreasing cell number and size. In fetuses thatexhibit mild-to-moderate IUGR, measurementsof extracellular fluid are usually normal forgestational age because adipose tissue, skeletalmuscle, and mineral accretion all are decreasedto about the same extent. In contrast, severeIUGR with markedly decreased fat content
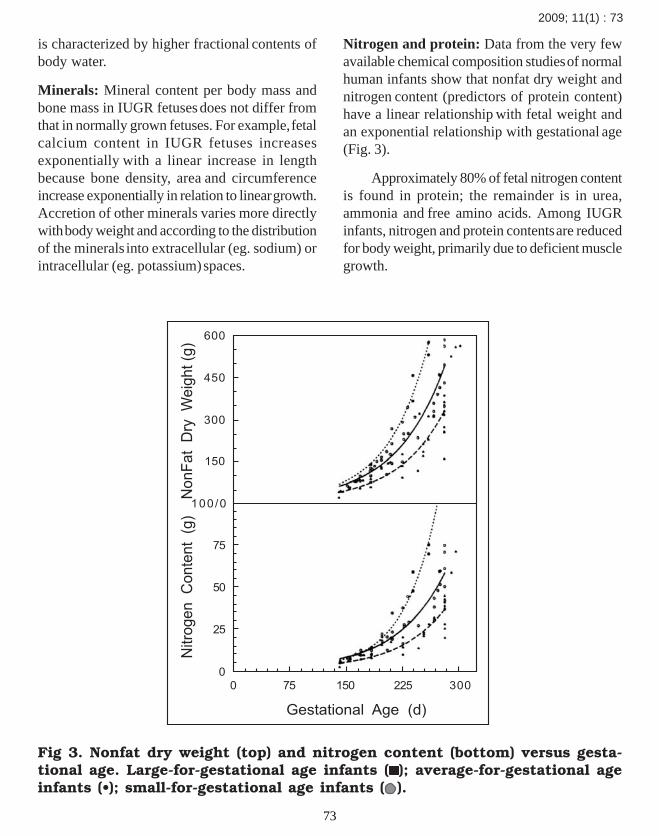
2009; 11(1) : 73
73
is characterized by higher fractional contents ofbody water.
Minerals: Mineral content per body mass andbone mass in IUGR fetuses does not differ fromthat in normally grown fetuses. For example, fetalcalcium content in IUGR fetuses increasesexponentially with a linear increase in lengthbecause bone density, area and circumferenceincrease exponentially in relation to linear growth.Accretion of other minerals varies more directlywith body weight and according to the distributionof the minerals into extracellular (eg. sodium) orintracellular (eg. potassium) spaces.
Nitrogen and protein: Data from the very fewavailable chemical composition studies of normalhuman infants show that nonfat dry weight andnitrogen content (predictors of protein content)have a linear relationship with fetal weight andan exponential relationship with gestational age(Fig. 3).
Approximately 80% of fetal nitrogen contentis found in protein; the remainder is in urea,ammonia and free amino acids. Among IUGRinfants, nitrogen and protein contents are reducedfor body weight, primarily due to deficient musclegrowth.
Fig 3. Nonfat dry weight (top) and nitrogen content (bottom) versus gesta-tional age. Large-for-gestational age infants ( ); average-for-gestational ageinfants (•); small-for-gestational age infants ( ).

Indian Journal of Practical Pediatrics 2009; 11(1) : 74
74
Glycogen: Glycogen synthetic rates are low inthe human fetus, accounting for less than 5% offetal glucose utilization. Insulin acts synergisticallywith glucose to increase hepatic glycogen stores,with cortisol, epinephrine and glucagon developingthe capacity to promote glycogenolysis andglucose release into the plasma close to term.Most tissues in the fetus, including brain, liver,lung, heart and skeletal muscle, produce glycogenover the second half of gestation. Liver glycogencontent, which increases with gestation (Fig.4) isthe most important store of carbohydrate forsystemic glucose needs because only the livercontains sufficient glucose-6-phosphate for releaseof glucose into the circulation. Skeletal muscleglycogen content increases during late gestationand forms a ready source of glucose-6-phosphatefor glycolysis within the myocytes. Lung glycogencontent decreases in late gestation with changein cell type, leading to loss of glycogen-containingalveolar epithelium, development of type II
pneumocytes and onset of surfactant production.Cardiac glycogen concentration decreases withgestation owing to cellular hypertrophy, but cardiacglycogen appears essential for postnatal cardiacenergy metabolism and contractile function.
Glycogen content is markedly reduced inIUGR infants, both in the liver and in the skeletalmuscles (Fig. 4), due to lower fetal plasmaconcentrations of glucose and insulin, which arethe principal regulators of glycogen synthesis.Repeated episodes of hypoxemia in severe IUGRcan stimulate epinephrine secretion, which willdeplete glycogen further by activating glycogenphosphorylase and increasing glycogenolysis.
Adipose tissue: The fat content of humannewborns at term is about 15% to 20%, which isconsiderably greater than the 1% to 3% found inmost other land mammals (Fig. 5). Human fataccretion begins in the late second to early thirdtrimester of gestation. In the first half of gestation,
Fig 4. Liver glycogen content (as carbohydrate) in normal human fetuses andnewborns with normal birthweights for gestational age ( ; mean±SEM) andinfants of low birthweight for gestational age (X).

2009; 11(1) : 75
75
nonfat and fat components contribute equally tothe carbon content of the fetal body. Subsequently,fat accumulation exceeds that of the nonfatcomponents such that between 36 and 40 weeks’gestation, the rate of fat accretion isapproximately linear and accounts for more than90% of the carbon accumulated by the fetus.
In human IUGR fetuses at term, fat contentmay be less than 10% of body weight. Causesinclude decreased fatty acid, triglyceride andglucose supplies from the smaller placenta as wellas a simultaneous insulin deficiency that limits fatsynthesis because of decreased stimulation offatty acid synthase in adipocytes. Because fat hasa high energy content of 9.5 kcal/g and a veryhigh carbon content of approximately 78%,decreased fat content in IUGR fetuses leads tolarge decreases in energy and carbon accretionrates.
Total energy balance and tissue mass
The relative mass of all tissue components,not just fat and glycogen stores, depends onenergy supply, particularly for protein deposition.For example, chronic selective restriction ofglucose delivery to the fetal sheep leads toincreased protein breakdown as well as tolower rates of fetal growth and lipid content.Although most studies suggest that the greatestrelative decrease in tissue mass occurs in the fatcompartment in human IUGR fetuses, others haveshown that muscle mass can be markedlydeficient, even more than fat.
Immediate postnatal growth
Infants usually lose some weightimmediately after birth, which they regain rapidlylater. On average, catch-up growth is greatest in
Fig. 5. Fetal fat content at term as a percent of fetal body weight amongspecies. Reproduced with permission from Hay WW Jr. Nutrition and devel-opment of the fetus: carbohydrate and lipid

Indian Journal of Practical Pediatrics 2009; 11(1) : 76
76
those infants most delayed in utero. As a result,there is a significant negative correlation betweenbirth weight and weight gain in the early postnatalmonths. The same phenomenon occurs for length;the smaller the infants, the more, on average, theygrow in the postnatal period.
Growth and developmental outcome
As noted previously, because most studiesof SGA infants have involved a heterogeneousgroup of babies with the potential for a variety ofoutcomes, it is difficult to predict outcomes inSGA infants. Some affected infants are smallfrom familial predisposition to small size and,therefore, may be expected to achieve their fullgrowth potential and have normal neuro-development. Infants who have specificchromosomal errors or significant congenitalinfections are likely to experience severe andunrecoverable failure of growth and development.Most infants have a less defined reason forabnormal in utero growth. The infant who hassymmetric growth restriction may have littlechance for postnatal catch-up growth after anearly, global disruption of growth. However,a neonate who had normal growth in earlygestation, but developed growth restriction fromlimited nutrient availability in later gestation, likelyhas a reasonable potential for catch-up growthand normal development. Additionally, socio-economic status and environment are among themost important, but difficult to control, variablesaffecting the growth and development ofSGA infants.
Most studies of normal and restricted fetalgrowth and development support the concept ofcritical windows of time in human developmentduring which normal growth of certain tissues(eg. fat, muscle, bone) or organs (eg. pancreas,brain) must occur. Insults at such times that limitgrowth can program persistent, even life-longfailures in growth and development.
Only relatively recently have studies of outcomesof IUGR and SGA infants included in the studydesign the recognition that the etiology of smallsize at birth carries great prognostic value hasbeen found out. Because head size correlates withbrain size, volume, weight and cellularity, headgrowth at the time of birth and the degree of catch-up growth thereafter are prognostic of futureneurodevelopment. Deficient fetal head growth,evidenced by relative microcephaly at birth,whether at term or preterm, is felt to be a poorprognostic indicator because it reflects the severityand duration of in utero growth failure. A lack ofhead sparing and small head circumference isassociated with poor neurologic and psychologicaloutcome. If catch-up head growth has notoccurred by 8 months of age, head size is apredictor of lower intelligence test scores at3 years of age. This correlation seems to beindependent of environmental or other risks.Decreased head size when compared with siblingscarries significant risks of deficient mental andmotor function.
Postnatal physical growth of SGAinfants
As with developmental outcome, long-termgrowth probably depends most on the etiologyand severity of fetal growth restriction.Many SGA infants continue to be smaller andrelatively underweight for age as they grow older,even through adolescence and early adulthood.These infants more commonly have short statureas teenagers and young adults, indicating lifelonggrowth deficit.
Differences in patterns of early growth havebeen observed in SGA infants. Normal infantsexperience a period of rapid growth during thefirst 3 years of life. Adult size correlates with theindividual growth curve after this time.Moderately affected SGA infants whosereduction in weight occurred primarily in the third

2009; 11(1) : 77
77
trimester of gestation follow the same pattern ofnormal neonatal and infant growth, but tend tohave an accelerated velocity of growth during thefirst 6 months of life. This catch-up growth occursmostly from birth to 6 months of age, with someinfants continuing an accelerated rate of growthfor the first year. A few of these infants achievea normal growth percentile and thereafter have agrowth rate similar to appropriately grownchildren. Head circumference parallels growthin length during catch-up and sustained growthperiods. After the first year, no difference in therate of growth has been noted.
Ultimate weight and height are less inSGA children compared with their normal siblings.Interestingly, a subgroup of severely growth-restricted infants (<40% of expected birthweight)showed no difference in weight or height at6 months of age compared with less-affectedSGA peers, adding concern for the growthoutcome of even modest degrees of IUGR.Former SGA infants had no delay in bone age,puberty or sexual maturation at adolescence,although they were shorter, lighter and had smallerheads. Muscle mass between the two groups wassimilar, but adipose tissue development was lessin the SGA group.
Postnatal neurodevelopmentaloutcome of term SGA infants
Neurologic disorders and other morbiditiesare generally more frequent in SGA infants,occurring 5 to 10 times more often than inAGA infants. However, IUGR may have littleimpact on behavior or mental ability in adolescenceor adulthood among term, mild-to-moderatelySGA infants who have normal brain growth, nohypoxic-ischemic injury, and good environmentalsupport. The incidence of major handicap and riskof severe neurologic morbidity in term infants bornSGA is not increased; cerebral palsy is infrequent.Findings on routine neurologic examination are
usually normal. Although the absence of grossneurologic outcome in the term SGA infant isreassuring, evidence of minimal brain dysfunctioncontinues to be of concern. Many studies haverevealed signs of minor brain damage, includinghyperactivity, short attention span, learningproblems, poor fine motor coordination andhyperreflexia.
Former term SGA infants more frequentlyhave substandard school performance and displaysubtle neurologic and behavioral problems despitenormal intelligence quotients. Sensorimotorabilities often are affected. Overall, poor earlybrain growth in infancy is associated with moreproblems. Measures of cognition at4 to 6 years correlate well with test results atadolescence, which suggests that cognitivepotential is reached early. It seems likely thatenvironmental and socioeconomic factors play asignificant role in the learning deficiencies seenin these children. At adolescence, trends towardlower test scores, especially in mathematics andan increased incidence of learning disabilities havebeen noted. Most believe, however, that thecognitive and academic differences are small anddo not significantly affect school performance orultimate intellectual ability.
Postnatal neurodevelopmentaloutcome in preterm SGA infants
The prognosis for preterm SGA infants isless clear and is confounded easily by otherproblems of preterm birth. In general, subnormalintellectual outcomes are more common amongpreterm SGA infants than term SGA infants.Some authors have shown that infants who sufferthe dual insults of preterm birth and growthrestriction are at higher risk of neurodevelopmentaldeficit. Among extremely preterm infants,gestational age (not growth status) has been themost significant predictor of intellectual outcome.Socioeconomic status is independently associatedwith learning disabilities in these children.

Indian Journal of Practical Pediatrics 2009; 11(1) : 78
78
Evidence for fetal origins of adultdisease
The importance of the early environment forlong-term health has been recognized for manyyears. Seventy years ago, observations in England,Scotland, and Sweden showed that death ratesdecreased between 1751 and 1930 due toimproved childhood living conditions. Death ratesin specific age groups at any time depended moreon the date of birth of the individuals than theyear under consideration.
In 1986, Barker and Osmond examinedmortality rates from stroke and cardiovasculardiseases in different areas of England and Wales.They noticed a parallel relationship betweenneonatal mortality in the 1920s and 1930s and themortality rates from strokes and cardiovasculardiseases in the 1960s and 1970s from the samegeographic areas. In the early 20th century, a highneonatal mortality rate was an indication of a highoccurrence of low-birthweight babies and of poornutrition and health of the mothers. Barker andOsmond concluded that the health of the motherswas important in determining the risk of stroke intheir offspring and proposed that cardiovasculardiseases might originate during fetal life or earlychildhood.
Low birth weight and adult disease
To follow up these findings, Barker andcolleagues examined records of early lifemeasurements from babies born in the 1920s and1930s. They found a strong relationship betweenlow-weight babies at birth or 1 year of age andischemic heart disease and hypertension at 50 to70 years of age. Low-birthweight babiessubsequently were shown to have increased riskfactors for coronary heart disease, includingelevated plasma glucose, insulin and low-densitylipoprotein cholesterol.
It is well known that fetal life and early
childhood are critical periods for human pancreaticbeta cell development. By 1 year of age, almost50% the adult beta cell population has developed.With this in mind, Hales and Barker investigatedwhether there was a link between low birthweightand later impaired glucose tolerance and type 2diabetes. Their initial study focused on men ages59 to 70 years (mean, 64 y) born in Hertfordshire,United Kingdom. Low birthweight was associatedwith impaired glucose tolerance and type 2diabetes. The odds ratio of impaired glucosetolerance was 6.6 times higher in men who hadthe lowest birthweights and 8.2 times higher inmen who had the lowest body weights at 1 yearof age. In both cases, these odds fell in acontinuous relationship with increasing bodyweight. They also showed that individuals whowere born small, but had a high body mass index(BMI) of more than 28 as adults had the worstglucose tolerances.
Subsequent studies found a relationshipbetween low birthweight and the metabolicsyndrome (syndrome X). In the sameHertfordshire cohort, the odds ratio of developingthe metabolic syndrome, defined as impairedglucose tolerance, hypertension andhypertriglyceridemia, was 18 times higher in low-birthweight babies. Another study by Phillips andcolleagues found that adult insulin resistance waslinked to thinness at birth.
A series of epidemiologic studies conductedsince the initial studies in Hertfordshire by manygroups in numerous populations worldwide andof varied ethnic groups confirm the originalfindings. Studies have examined men and womenin the United Kingdom, Sweden, United States(on Mexican-Americans), India, and Pima Indiansas well as on many others. Thus, the relationshipbetween low birthweight and adult disease iswidely accepted, although the mechanism isunknown, and the relative roles of genetic andenvironmental factors are debated.

2009; 11(1) : 79
79
Fetal insulin hypothesis and MODY genes:One explanation for the relationship between lowbirthweight and subsequent risk of type 2 diabetesis the possibility of genes causing both lowbirthweight and increased risk of type 2 diabetes.Hattersley and associates have suggested thatgenetically determined defects in insulin secretionor insulin action could result in poor fetal growth,low birthweight and subsequent susceptibility totype 2 diabetes. This fetal insulin hypothesis wassupported by data from individuals who hadmature onset diabetes of the young (MODY) type2. These individuals have mutations in theglucokinase gene that result in decreased insulinsecretion, reduced fetal growth and MODY2.
Thrifty phenotype hypothesis: An alternativehypothesis to explain the associations betweenlow birthweight and adult disease was put forwardby Hales and Barker in 1992. It was termed the“thrifty phenotype” hypothesis, so named tocontrast it with the “thrifty genotype” hypothesis
proposed by Neel in 1962. Neel had proposedthat genes that caused diabetes had been retainedthrough natural selection because they broughtsome benefit to the individual. It was suggestedthat the genes resulted in a greater capacity tostore fat during times of starvation andundernourishment, which had been the majorityof the time. The recent overabundance andovereating of food as well as the onset of obesitydue to lack of exercise had caused the genes tobecome detrimental.
The thrifty phenotype hypothesis suggestedthat when the intrauterine environment was poor,the fetus adopted a number of strategies tomaximize its chances of survival postnatally.A nutritionally restricted fetus would divertnutrients to the brain and away from other organssuch as muscle, liver, and pancreas. Metabolicprogramming occurred at this crucial time basedon the environmental conditions, with the fetalmetabolism adapting to survive in conditions of
Fig.6. The thrifty phenotype hypothesis as proposed by Hales andBarker (1992).

Indian Journal of Practical Pediatrics 2009; 11(1) : 80
80
poor postnatal nutrition. Problems occurred whennutrition during postnatal life was normal orexcessive, which conflicted with the earlierprogramming and led to diseases such ashypertension, ischemic heart disease and type 2diabetes (Fig.6 ). Populations that have served asgood examples of the detrimental effects of thethrifty phenotype include Ethiopian Jews, who,after relocation to Israel and an adequate dietand lifestyle, had a high prevalence of type 2diabetes compared with those who remained inEthiopia, where diet and lifestyle were inadequate.In sub-Saharan Africa, the prevalence of diabetesis very low because poor fetal nutrition is followedby poor postnatal nutrition.
In some populations, such as thePima Indians, birthweight and adult diabetes arelinked by a “U”-shaped curve, with both low- andhigh-birthweight babies having a higher risk ofthe disease. This is believed to be due to the highprevalence of gestational diabetes in thesepopulations, which is not seen in the other studiesdue to the low frequency and survival rate in theearly part of the 20th century. The highbirthweight, therefore, represents macrosomicoffspring of gestational diabetic mothers. It is wellestablished that gestational diabetes leads to anincreased risk of diabetes in the offspring.
Future prospects
Research clearly indicates a relationshipbetween the early fetal nutritional environmentand later adult disease, although the mechanisticbasis of the relationship is not known. Maternaldiet restriction leading to intrauterine growthretardation of the fetus leads to type 2 diabetesand the metabolic syndrome in the rat and it hasbeen shown to be associated with programmedchanges in protein expression. These proteins arepotential markers that would allow prediction offuture diseases and a target area of researchwould be to identify such markers in a clinically
accessible human tissue to allow implementationof intervention strategies to prevent futuredisease.
Points to Remember
• Fetal growth results from interactionsamong maternal, placental and fetalfactors and a mix of environmentalinfluences through which the fetalgenotype is expressed and modulated.
• The single most important environmentalinfluence is fetal nutrition and its principaldeterminant is the size and nutrienttransport capacity of the placenta.Placental size is determined by the size ofthe uterus and thus, the size of the mother.Increased nutrient supply to the fetussubsequently increases fetal tissue andplasma concentrations of anabolichormones and growth factors.
• The variable supply of nutrients, anabolichormones and growth factors in the fetusmodulate the expression and/or action ofgrowth-promoting genes and their geneproducts, leading to variation in fetalgrowth.
• Deficiencies in any one of these factorscan limit fetal growth and produceintrauterine growth restriction.
References
1. Surani MA, Barton SC, Norris ML. Nucleartransplantation in the mouse: heritabledifferences between parental genomes afteractivation of the embryonic genome. Cell.1986;45:127-136.
2. Hollenberg SM, Sternglanz R, Cheng PF,Weintraub H. Identification of a new family oftissue-specific basic helix-loop-helix proteinswith a two-hybrid system. Molec Cell Biol1995;15:3813-3822.

2009; 11(1) : 81
81
3. McKeown T, Record RG. Observations on foetalgrowth in multiple pregnancy in man.J Endocrinol 1952;8:386.
4. Battaglia FC, Meschia G. An Introduction toFetal Physiology. Orlando, FL: Academic, 1986;pp1-27.
5. Lubchenco LO, Hansman C, Boyd E.Intrauterine growth in length and headcircumference as estimated from live births atgestational ages from 26 to 42 weeks. Pediatrics1966;37:403-408.
6. Ounsted M, Ounsted C. On fetal growth rate.In: Clinics in Developmental Medicine No. 46.Philadelphia, JB Lippincott Co, 1973;p46.
7. Lumey LH. Decreased birthweights in infantsafter maternal in utero exposure to the Dutchfamine of 1944–1945. Paediatr Perinat Epidemiol1992;6:240-253.
8. Roberts RM, Anthony RV. Molecular biologyof trophectoderm and placental hormones. In:Findlay JK, eds. Molecular Biology of theFemale Reproductive System. Academic PressSan Diego, Calif, 1994;pp395-440.
9. Molteni RA, Stys SJ, Battaglia FC. Relationshipof fetal and placental weight in human beings:fetal/placental weight ratios at variousgestational ages and birth weight distributions.J Reprod Med 1978;21:327-334.
CLIPPINGS
Fetal fibronectin testing for reducing the risk of preterm birth
Preterm birth before 37 weeks is the main cause of death and sickness for newborn infants.While most women have preterm labor symptoms such as contractions before having a pretermbirth, most such women with symptoms deliver at term (greater than or equal to 37 weeks).Fetal fibronectin is a test that can identify the women with symptoms of preterm labor most atrisk for preterm birth by measuring the level in secretions from the vagina and/or cervix. Thisreview of five controlled studies that randomised 474 pregnant women did not find enoughevidence to support or refute the use of the fetal fibronectin test for the management of womenwith symptoms of preterm labor. Further research should be encouraged.
Authors’ conclusions
Although FFN is commonly used in labor and delivery units to help in the management ofwomen with symptoms of preterm labor, currently there is not sufficient evidence to recommendits use. Since this review found an association between knowledge of FFN results and a lowerincidence of preterm birth before 37 weeks, further research should be encouraged.
Berghella V, Hayes E, Visintine J, Baxter JK. Fetal fibronectin testing for reducingthe risk of preterm birth. Cochrane Database of Systematic Reviews 2008, Issue 4.Art. No.: CD006843. DOI: 10.1002/14651858.CD006843.pub2. This version firstpublished online: October 08. 2008
Indian Journal of Practical Pediatrics 2009; 11(1) : 82
82
CHILD ADOPTION
* Ganesh R* Suresh N
** Eswara Raja T*** Lalitha Janakiraman
*** Vasanthi T
Abstract: Adoption is the process throughwhich the adopted child is permanentlyseparated from his/her biological parents andbecomes the legitimate child of his/heradoptive parents with all the rights, privilegesand responsibilities that are attached to therelationship. In-country adoption, process ofprospective adoptive parents and its medicolegal aspects are discussed in detail.
Keywords: Adoption, Prospective adoptiveparents.
“I shall be called by a new name, embracedby a fresh pair of arms, but I shall come and go,the external me”- Rabindranath Tagore.
Adoption is the act of lawfully assuming theparental rights and responsibilities of anotherperson, usually a child under the age of 18.1
In this era of modernisation, the abandonment ofa newborn child is not uncommon. At the sametime it is also encouraging to see many personscoming forward to bring up such babies as everychild has a right to love and be loved, be grown
up in an atmosphere of love and affection.Adoption is reflected as a triad formed betweenthe child, adoptive parents and birth parents, thecorners of which are connected by organisationssuch as adoption agencies, children homes to forma complete circle so as to get a rewarding andsatisfying outcome.2 With the increasingawareness and acceptance of adoption in India,it becomes important for the doctors to be awareof the recommendations, medico legal aspects andthe role of Governmental and non-Governmentalorganizations in the process of adoption.This article outlines the step-by-step approach tothe prospective adoptive parents about howa baby is placed for in-country adoption, the rulesof adoption and the legal aspects in detail.
Reasons for adoption
The reasons for adopting a child includesa desire to give a home to a child who needs one,as an alternate method of attaining parenthoodby a childless couple, desire to have a child of theother sex, advanced age of the parents and dueto death of one spouse.
Types of adoption
Adoption may be open or closed. An openadoption involves some exchange of personalinformation between the biological and adoptiveparents. In closed adoption there is no exchangeof information or any personal contact betweenthe biological and adoptive parents.1
Laws of adoption
In India there are two laws that govern theprocess of adoption namely hindu adoption and
* Registrar in Pediatrics** Junior Consultant in Pediatrics
*** Senior consultant PediatricianKanchi Kamakoti CHILDS Trust Hospital,Chennai.
GENERAL ARTICLE

2009; 11(1) : 83
83
maintenance act (HAMA), 1956 governing allhindus adopting children and the second, theguardians and wards act (GWA) 1890, governingadoptions by parents who are not hindus byreligion. Personal laws for muslims, christians,parsees and jews do not recognize completeadoption and hence persons belonging to thesecommunities desirous of adopting a child can doso only in guardianship under the provision ofGWA, 1890. This does not provide the child thesame status as that of the child born to the familyand confers only a guardian ward relationship.In inter country adoptions, children are given foradoption under GWA 1890 in foster care till theyare finally adopted according to the law of thecountry of adoptive parents.3
The requisites of valid adoption are:
1. The person adopting has the capacity andalso the right to take in adoption
2. The person giving in adoption has thecapacity to do so
3. The person adopted is capable of being takenin adoption and
4. The adoption is made in compliance with thelaws governing the adoption.
Sources and medico legal aspectsof adoption
Now a days adoption in India is no longerthe traditional adoption-taking place in the relatedgroups. Hence adoption must always be donethrough recognized Indian placement agencies,Sishu grehas getting grant in aid from centralgovernment and licensed adoption placementagencies (LAPA).4 In all the states of India thereare many orphanages and agencies recognizedin this manner by the government for givingadoption. The child to be adopted should be legallyfree for adoption. Both verbal and written consentto be obtained for children aged above6 years. Siblings/twins/triplets should not be
separated as sibling relationship is associated withless loneliness, fewer behavior problems andenhanced their safety and well being. Prospectiveadoptive parents can adopt even if they havebiological children and a single parent has equallegal status to adopt. If the adoption is by a maleand the person to be adopted is a female, theadoptive father should be atleast 21 years olderthan the person to be adopted. If the adoption isby female and the person to be adopted is male,the adoptive mother should be atleast 21 yearsolder than the person to be adopted. A child onceadopted has to break all his/her relations with thebiological parents and can never return to themeven when he/she opts for this course whengrown up.
Adoption process
The steps involved in adoption process are asfollows:
1) Prospective adoptive parents should registerwith the local licensed adoption placementagency or any recognized Indian placementagencies. They should also be equipped withtheir marriage registration certificate ormarriage invitation, age proof certificate andmedical certificate regarding their healthstatus etc.
2) The next step is pre adoption counseling thatis offered to prospective adoptive parentswhich is done by the social worker of theagency to allay the fears and apprehensions.Home study report of the prospectiveadoptive parents is conducted by the trainedsocial worker of the agency, the guidelinesof which are available.5
3) Submission of the financial and health statusof the prospective adoptive parents to theagency. The prospective adoptive parentsshould have a minimum average monthlyincome of atleast Rs 3000 per month.However lower income may be considered

Indian Journal of Practical Pediatrics 2009; 11(1) : 84
84
taking into account other assets and supportsystem. The couple should be in good healthand remain free from communicable diseasesand should not be suffering from any healthproblem which might be physically ormentally debilitating as it will affect their caregiving ability.
4) After the home study report has beenaccepted and approved, a child will be shownto the parents and the agency takes care tomatch a child meeting the desired descriptionof the parents and if a child is above 6 yearsof age, both written and verbal consent ofthe child is obtained.
5) The child undergoes medical screening forfitness, which includes identification data,anthropometry, systemic examination,detection of any gross deficiency disorder,overt or covert anomalies and their correctability potential. Standard investigations thatare performed includes complete hemogram,urine analysis, stool for parasites, chestX-ray, Mantoux test, tests for VDRL, HIV,
hepatitis B, TORCH titres and any otherindicated tests with special reference tohypothyroidism, hemolytic anemia,chromosomal anomalies and metabolicscreening test for mental retardation likephenylketonuria, galactosemia andaminoacidurias.3 If prospective adoptiveparents are willing to adopt a child withdisability or health problem, a documentstating the same should be obtained.
6) Once a child is successfully matched, filingof a petition by the agency under the relevantact for obtaining the necessary orders in thecompetent court. If a child cannot be placedin adoption with a suitable Indian family, thechild may be transferred to the nearestrecognized Indian placement agency withprior permission from the competent authorityof the state government.
7) Payment of fees as prescribed by thegovernment to the licensed adoptionagency for maintenance and legal cost is tobe made.
Table I. Do’s and Don’ts in adoption
Do’s Don’ts
Adopt only from a recognized placement Do not adopt from nursing homes/ hospitalsagency or Licensed adoption placement directly or from unrecognized agency/ unrelatedagencies (LAPA) or shishu greha persons.
The consent of children above 6 years Do not succumb to the demands for donationshould be taken for adoption and any amount more than the prescribed
adoption fee.
The child study report should be signed Take informed decisions based on facts madeby both adoptive parents available to you.
Pay adoption fee as prescribed underguidelines and obtain fee receipt.
Obtain a copy of the receipt of registrationfrom the adoption agency

2009; 11(1) : 85
85
8) The above process is normally completed in8-12 weeks once the child has been matchedwith the parents.
9) The last step is the regular follow-up visitsand post adoption counseling done by thesocial worker till the child adjusts in his/hernew environment. The follow up shouldpreferably be for a period of one year or asdirected by the court /Juvenile JusticeBoard(JJB) and the copies of these followup reports should be sent to the district socialwelfare officer/concerned state Governmentdepartment and the court/ (JJB) where theorder was obtained.Once a child is adopted, an adopted child
shall be deemed to be the child of his/her adoptivefather/mother for all purposes with effect fromthe date of adoption and from such date all theties of the child in the family of his/her birth shallbe deemed to be settled and replaced by thosecreated by the adoption in the adoptive family.Encouraging, insisting and helping the adoptiveparents to tell the child about his/her adoption isthe most vital post adoptive follow up action tobe done usually between the ages of 6 to 10 years(ie), the time by which the child can comprehendthe concept of biological and adoptive parenthoodin order to avert the future problems.3
The Do’s and don’t’s in adoption are shownin Table 1.Conclusion
The above article outlines the adoptionprocess and its medico legal aspects. However
more efforts are needed to bring up a child in theheart and not under the heart when a desire ismade to provide a family for a child.
Points to Remember
• Adopt only from a recognized agency
• Early decision by the prospective adoptiveparents to adopt a child is preferable (ageof one parent should be at least below35 years)
Acknowledgement: We thank Mrs. SheelaJayanthi, Administrative officer, Karna PrayagTrust (welfare center for women and children)for giving us permission to visit the center andproviding us practical information regarding theadoption process in the community.
References
1. Nair MKC. Adoption. Indian Pediatr 2004; 41:653-655 .
2. Banerjee SR, Banerjee S. Adoption. In: BanerjeeSR, Ed, Community and Social Pediatrics.1
st Edn, New Delhi, Japee, 1995;pp313-324.
3. Potdar RD. Adoption. In: A Parthasarathy, MKCNair, PSN Menon, eds. IAP Text book ofpediatrics. 3
rd Edn, New Delhi, Jaypee, 2006;
pp190-192.
4. Adoption made simple. Available from URL:http://www.cara.nic.in/Article.htm, Accessed10 December, 2006.
5. h t t p : / / w w w. a d o p t i o n i n d i a . n i c . i n /guide_incountry_ann_6.htm.
NEWS AND NOTES
GEM (Pediatric Golden Hour Emergency Management) Course,Hyderabad.
February 14-15, 2009Contact:Dr. Dinesh ChirlaMobile : 09849790003, E-Mail: [email protected]

Indian Journal of Practical Pediatrics 2009; 11(1) : 86
86
ICHTHYOSIS - AN APPROACH
* Anandan V
Abstract: Ichthyosis is an age old geneticallymediated problem known as “Ekakushtha”which means fish like scales, appears in anIndian text in 250BC. Ichthyosis is basicallya disorder of keratinisation where the cell turnover time is altered by which there is retentionof cells leading to dry scaly skin which couldbe primary or secondary leading to cosmeticdisfigurement and prolonged morbidity.Advance researches in this field has focusedthat various keratins, proteins and enzymesare at fault and various treatment options arebeing suggested which boosts the physician’sconfidence in treating these disorders.
Key words : Ichthyosis, Fish like scales,Syndromes.
Ichthyosis is an age old genetically mediatedproblem known as “Ekakushtha” which meansfish like scales, appears in an Indian text in250BC.1
The clinical diversity and rarity of some ofthe ichthyosis has led to a confusing array ofclassifications by various workers, but the onegiven by Esterly identified four categories whichis widely followed globally2 and which is asfollows.
1) Major primary forms. 2) Ichthyosiformsyndromes. 3) Related disorders of cornificationand 4) Acquired ichthyosis.
Each of these in turn has got many types ofichthyosis, of which some common types will bediscussed in this article.
1. Major primary formsThis group includes ichthyosis vulgaris,
X-linked recessive ichthyosis, non bullousichthyosiform erythroderma, lamellar ichthyosis,harlequin ichthyosis, bullous ichthyosiformerythroderma, ichthyosis bullosa of Siemens andichthyosis hystrix.
a) Ichthyosis vulgarisThis is the commonest type of ichthyosis
reported which is inherited as autosomal dominantcondition with a reported incidence of 1 in 250and common in temperate climates with equalsex incidence sometimes found to be associatedwith atopic dermatitis.3 The aetiopathogeneis inshort is said to be absence of profilaggrin andreduced expression of filaggrin mRNA.
Clinically the skin appears dry and scalywhich becomes more obvious from two monthsonwards, the scales are small, white, flaky andsemi adherent with turned up edges morepronounced on the extensor surfaces of theextremities characteristically sparing the flexures.It is found that atopic eczema and keratosis pilaris(Follicular hyperkeratosis) are commonlyassociated with ichthysis vulgaris.3
Symptomatically these children may have pruritisand lichenification and an apparent increased riskof testicular cancer in men is very difficult toexplain.4
DERMATOLOGY
* Assistant Professor,Dept. of Dermatology,Govt. General Hospital andPediatric Dermatologist, ICH & HC, Chennai

2009; 11(1) : 87
87
b) X-linked recessive ichthyosis (XLRI)
XLRI has an incidence of 1 in 6190 whichaffects the male offspring’s of asymptomaticfemale carriers often associated withextracutaneous manifestations with obstetric andperinatal complications which was found to havesteroid sulphatase deficiency and the gene locushas been identified at the distal end of the shortarm of the chromosome.5 Clinically 75% of theaffected newborns present with scaling within thefirst week of life6 which progresses till teensspreading from legs to trunk with remissions insummer.6 The scales are typically medium tolarge, polygonal, adhernt, dull, light brown tomuddy in colour commonly involving posterolateralneck, superolateral abdominal wall and thepreauricular facial skin. In contrast to ichthyosisvulgaris the flexures will be involved and pruritismay be absent with palms and soles being spared.XLRI is associated with extracutaneousmanifestations like testicular maldescent,cryptorchidism, infertility, testicular cancer,7
inguinal herniae and unilateral renal agenesis.It is interesting to note that nearly 50-100% maypresent with comma shaped corneal opacities.8
The syndromes worth metioning with XLRIare
1) Kallmans syndrome : Hypogono-dotrophic hypogonodism, anosmia, nystagmus,mirror movements of hands and feet (synkinesis)and
2) Ruds syndrome : Obesity, hypogonodism,mental retardation, epilepsy and endocrinopathies.
c) Non-bullous ichthyosiform erythroderma(NBIE)
NBIE is a autosomal recessive inflammatoryichthyosis with an incidence of 1 in 300000.9
It occurs in all races, but especially in those whereconsanguinous marriage is common. Clinically
90% of NBIE presents at birth with colodionmembrane with scales appearing white to grey,light, superficial, semi adherent and featheryscales above the groin and plate like below thegroin which could be cyclical over periods of2-4 weeks. Palmoplantar hyperkeratosis canoccur in 90% of the cases and cicatricial alopeciahas been reported. Ectropion, exposure keratitis,blindness, loss of eye brows and lashes withhypoplasia of the nasal and aural cartilage withor without nail dystrophies may be present.Pruritis could be very severe.
d) Collodion baby
The incidence of collodion baby is on therise recently, clinically presenting at birth as aglistening, taut, yellowish film stretched over theskin with obliteration of normal skin markings.It can present with ectropion, eclabion, crumpledears, sausage shaped digits and constrictingbands. Shortly after birth the membrance dries,cracks around the flexures and is usually shedwithin first few weeks of life leaving backerythrodermic ichthyosis. As a pediatrician onehas to watch for hypernatremic dehydration10 andbacterial sepsis. Usually the collodion baby slipsinto NBIE and lamellar ichthyosis commonly but10% of the collodion babies become normal andthey are referred as self healing collodion babies.
2. Ichthyosiform syndromes
Even though increasing number ofsyndromes with ichthyosis are being reported inthe literature, only a few clinically importantsyndromes like (a) Netherton, (b) Sjogren-Larsonand (c) Refsum disease will be discussed in thisarticle.
a. Netherton syndrome (NSI)
This is the commnest of the multisystemichthyosiform syndromes which comprises ofichthyosis with variable erythroderma, hair shaft

Indian Journal of Practical Pediatrics 2009; 11(1) : 88
88
defects and atopic features with autosomalrecessive inheritance occurring globally with anincidence of 1 in 100000. Clinically NS presentssoon after birth with varying erythrodema,temperture instability and infections. Duringchildhood 50% of NS patients develop thecharacteristic lesion which is called as ichthyosislinearis circumflexa (ILC) presenting aserythematous, scaly, polycyclic, migrating flatpatches with incomplete advancing double edgeof peeling skin evolving cephalo caudally withflexural lichenification and with increasedtendency to develop bacterial and viral infections.The major diagnostic clue to the diagnois of NSis the hair shaft defect known as trichorrhexisinvaginata. In addition the hairs are sparse, spiky,lusterless, brittle, unruly with broken hair shaft atfollicular orifice producing “peppered”appearance.11
b) Sjogren - Larsson syndrome (SLS)
SLS is an autosomal recessive condition withan incidence of 1 in 100000 clinically comprisingof congenital ichthyosis, spastic diplegia, mentalretardation and retinopathy. Metabolically SLSwas found to have a deficiency of delta 6desaturase with elevated plasma levels ofhexadecanol and octadecanol. SLS clinicallypresents with collodion membrance later to haveerythroderma with the development of scaling bythree months of age predominantly affecting thelimbs and the face. A velvety orange brownflexural lichenification may help in the diagnosis.Delayed mile stones and uper motor neuron signsare noted in early infancy resulting in nonprogressive spastic paraperesis. 50-80% of thesepatients were found to have a characteristicretinopathy consisting of glistening dots in thefovea and Para fovea.12
c) Refsum disease (RD)
RD is a rare autosomal recessive neuro-cutaneous disorder caused by defective fatty acid
metabolism described by Refsum in 1946 asHeredopathia atactica polyneuritiformis.13 Thesepatients were found to have deficiency of phytanicacid oxidase. RD is as such a disease ofadolescence which is characaterized by mild formof ichthyosis, retinitis pigmentosa, sensory neuraldeafness, mixed peripheral neuralpolyneuropathies, cardiomegaly and conductiondefects.Infantile RD could present as aneurodegenerative disease similar to adult formdevoid of ichthyosis.
3. Isolated genetic syndromes withichthyosis
There have been various reports about theextracutaneous associations with congenitalichthyosis which could be interesting to anacademician. To mention a few are,
A) Ichthyosis with CNS defects :
a) CHIME : Coloboma, heart disease,ichthyosis, mental retardation and eyedefects.
b) KID syndrome : Keratitis, ichthyosisand deafness.
c) Sjogren - Larson syndrome
d) Refsum disease
B) Ichthyosis with renal defects
a) Fanconi syndrome with ichthyosis hasbeen reported.
C) Ichthyosis with skeletal defects
a) ICE syndrome : ichthyosis, fullness ofcheeks, thinning of eyebrows.
b) CHILD syndrome : congenital hemidysplasia, ichthyosis, limb defects.
D) Ichthyosis with immune defects
a) Nezelof syndrome : Ichthysosis, severecongenital immunodeficiency withthymic hypoplasia.

2009; 11(1) : 89
89
E) Ichthysosis with malignancy
a) XLRI : Testicular malignancy.
b) KID syndrome : Squamous cellcarcinoma.
c) NS : Squamous cell carcinoma.
4. Acquired ichthyosis
Acquired or late onset ichthyosis isassociated with or could be a manifestation ofunderlying disease the knowledge of which isimportant for the early detection and efficienttreatment of the primary cause. To mention a fewunderlying causes are : Drugs like nicotinic acid,hypocholestroloemic agents, maprotiline andclofazimine and diseases like chronic hepatitis,renal failure, thyroid and parathyroid disease,malabsorption states, sarcoidosis, leprosy, AIDS14
and lymphoma.
Treatment
Topical : The main stay of treatment is going tobe emollients like liquid paraffin and white softparaffin which keeps the ichthyotic area moistand soft by reducing the trans epidermal waterloss and it is also recommended to use itimmediately after the bath . Keratolytics like1 to 5% Salicylic acid, Alpha hydroxyl acids,5 to 10% urea cream is also being used to removethe scales and to make the skin soft and smooth.Topical retinoids, calcipotriol and topical eveningprimrose oil are also being used with varyingsuccess .
Systemic: Systemic drugs are very rarely usedunless and otherwise the ichthyosis is very muchresistant and which could endanger life in the formof non bullous ichthyosiform erythroderma whereoral retinoids like acitretin 0.5 to 0.75mg/kg bodyweight could be life saving . Usage of oralantibiotics to combat secondary infection is alsojustified. Oral primrose oil is also being used asan adjuvant.
Future trends: Gene therapy in future is theonly ray of hope in these patients .
Points to Remember
• Ichthyosis could be genetic and acquired.
• Holistic approach will highlight theunderlying syndromes.
• Sympathetic approach is alwaysrewarding.
References
1. Menon IA, Haberman HF. Dermatologicalwritings of ancient India. Med His 1969;13:387-392.
2. Esterly NB. The ichthyosiform dermatosis.Pediatrics 1968;42:990-1004.
3. Wells RS, Kerr CB. Clinical features ofautosomal dominant and sex-linked ichthyosisin an English population. Br Med J 1966;1:947-950.
4. Lykkesfeldt G, Bennett P, Lykkesfeldt AE, et al.Testis cancer; ichthyosis constitutes asignificant risk factor. Cancer 1991;67: 730-734.
5. Jobsis AC, Van de sen chr Y, Van de uries GP,et al. Trophoblast sulphatase deficiencyassociated with X-chromosomal ichthyosis.Med Tijidschr Geneesk 1976 ; 120:130-136.
6. Paige DG, Emilion GG, Boutoux PMG,Harper IL.A clinical and genetic study of X-linkedrecessive ichthyosis and contiguous genedefects . Br J Dermatol 1994; 131: 622-629.
7. Lykkesfeldt G, Lykkesfeldt AE, Hayer H, Shakkebaek NE. Steroid sulphatase deficiencyassociated with testis cancer. Lancet 1983;2:1456.
8. Costagliola C, Fabbrocini G, Illiano GM et al.Ocular findings in X-linked ichthyosis; a surveyof 38 cases. Opthalmogica 1991;202:152-155.
9. Wells RS, Kerr CB. Clinical features ofautosomal dominant and X-linked ichthyosis.inan English population. Br Med J 1966;1:947-950.
10. Buyse L, Graves C, Marks et al.Collodion babydehydration; the danger of high trans epidermalwater loss. Br J Dermatol 1993;129:86-88.

Indian Journal of Practical Pediatrics 2009; 11(1) : 90
90
11. Greene SE, Muller SA.Netherton syndrome; areport of a case and review of the literature.J Am Acad Dermatol 1985;13:329-337.
12. Nilsson SEG, Jagell S. Lipofuscin and melanincontent of the retinal pigment epithelium in acase of Sjogren-Laesson syndrome. Br JOpthalmol 1987; 71:224-226.
13. Refsum S. Heredopathica actacticapolyneuritiformis. Acta Psychiatric scand(suppl) 1946;38:1-3.
14. Young L, Stenman HK. Acquired ichthyosis ina patient with AIDS and kaposis sarcoma. J AmAcad Dermatol 1987;16:395-396.
IAP-IJPP CME 2009
NATIONAL CME ORGANIZED BY
INDIAN ACADEMY OF PEDIATRICS (IAP)and
INDIAN JOURNAL OF PRACTICAL PEDIATRICS (IJPP)
AT KAMARAJAR ARANGAM,492, ANNA SALAI, CHENNAI - 600 006.
ON SUNDAY, 7TH JUNE 2009
Delegate fee:
Up to 31st May, 2009 Rs.300/- for Post Graduates, Rs.500/- for others.From 1st June, 2009 Rs.750/- (as Cash / Cheque/DD drawn in favour of“IAP-IJPP CME 2009”, payable at Chennai)
For further details contact:
Dr.K.Nedunchelian and Dr.S.ThangaveluOrganizing Secretaries, IAP-IJPP CME 20091A, Block II, Krsna Apartments,50, Halls Road, Egmore,Chennai – 600 008.India.Phone: 044-28190032,42052900E-mail: [email protected]
NEWS AND NOTES

2009; 11(1) : 91
91
Can you spot the diagnosis?
Compiled by*Dr.Baldev S Prajapati*Dr.Rajal B Prajapati**Dr.Panna S. Patel
*Associate Professors, Smt. N.H.L.Municipal Medical College, Ahmedabad.**Counsultant Pediatrician, Aakanksha Children Hospital and Neonatal Nursery, Ahmedabad.
Answer on page: 96
PICTURE QUIZ

Indian Journal of Practical Pediatrics 2009; 11(1) : 92
92
DISORDERS OF VENTRALINDUCTION AND SIMILARCONDITIONS - 1
* Vijayalakshmi G** Elavarasu E
*** Vijayalakshmi M*** Venkatesan MD
Ultrasound of the neonatal brain is excellentfor studying the ventricular system. One reasonis the central location of the ventricles that makesit easily accessible to the ultrasound beam whilelaterally placed structures are shadowed by thebony edges of the fontanelle. The other reasonis the black colour of fluid that is easy toappreciate. Sometimes, almost the entire craniumis filled with fluid. Hydranencephaly is one suchcondition. It is a rare abnormality where thecerebral cortex is completely destroyed. It occursafter the brain and ventricles have formed, usuallyin the second trimester. Intrauterine infections andvascular insult are implicated in the pathogenesis.The brain destruction is in a bilateral internalcarotid distribution and both cerebral hemispheresare seen as bags of fluid covered by the meninges.Since the prosencephalon has already cleaved intotwo, the falx is present. This is one importantfeature that differentiates it fromholoprosencephaly. Fig.1 is an ultrasound image
of hydranencephaly.The falx is seen as a verticalwhite line within a large bag of black fluid.
Holoprosencephaly is a very early event(4-8 weeks) unlike hydranencephaly which occurslater. It is a developmental abnormality that resultsfrom absent or incomplete diverticulation of theforebrain into two hemispheres.. Therefore thefalx is not formed. There is a large single ventricle.The cavum septum pellucidum is also absent.
There are three types of holoprosencephalydepending on the degree of cleavage or separationof the telencephalon into the two cerebralhemispheres. Fig.2 is the alobar type. There isno falx, no cerebral tissue, and the thalami arefused. MRI will also demonstrate the largemonoventricle. The falx is absent. It thereforefollows the three sinuses in the edges of the falx- superior sagital sinus, inferior sagital sinus andthe straight sinus -are also absent. There is a single
RADIOLOGIST TALKS TO YOU
* Associate Professor** Asst. Professor
*** ProfessorDepartment of Radiology,Chenglepet Medical College Hospital,Chenglepet, Tamilnadu.
Fig.1. Hydranencephaly. Note the falx

2009; 11(1) : 93
93
midline artery instead of two pericallosal arteries.In the semilobar type (Fig.3) there is partialseparation into hemispheres posteriorly while thefrontal lobes are fused anteriorly. The corpuscallosum is present only posteriorly. There is stilla single ventricle but there is an attempt to formtemporal and occipital horns. The lobar type isshown in Fig.4. There is complete ventriculardivision. The ventricles are almost normal but thefrontal horns will be placed closely as the cavum
is absent. The frontal horns also have a squared-off appearance. Cortical separation is however,incomplete. MRI will show grey and white matterfused across the midline usually on the inferioraspect of the frontal lobe. The squared-offappearance of the frontal horns is also seen insepto-optic dyspalsia where there is optic nervehypoplasia and pituitary hypoplasia.Syntelencephaly (Fig.5) is sometimes describedas a variant of the lobar type. In this, there is a
Fig.2. Holoprosencephaly-alobartype. Falx is absent
Fig.3. Holoprosencephaly-semilobartype. Monoventricle with cerebrallobe formation
Fig.4. Lobar holoprosencephaly Fig.5. Syntelencephaly

Indian Journal of Practical Pediatrics 2009; 11(1) : 94
94
Fig.6. Hydrocephalus.
normal or hypoplastic falx and fusion of greymatter in the midfrontal region. There isheterotopic grey matter in the region of the corpuscallosum and the septum pellucidum is absent.
It is important to differentiate the abovetwo conditions from gross hydrocephalus as
these children require shunting of CSF.Gross hydrocephalus, however severe it may be,usually has a thin cerebral mantle whilehydranencephaly is devoid of cerebralparenchyma. The third ventricle is present(Fig.6) and both thalami are separate inhydrocephalus unlike holoprosencephaly wherethey are fused. Confusion may arise betweenhydrocephalus of the lateral ventricles alone andsemilobar holoprosencephaly. In the former thefrontal horns are well formed , while in the latterthe frontal horns are not well developed.
In holoprosencephaly the head isconsiderably smaller than expected and theremaybe other midline abnormalities which will aidin diagnosis. But in hydranencephaly the headmay be large as in hydrocephalus. Carefulinterpretation is then necessary to differentiatethe two, so that a shunting procedure may beadvised appropriately.
CLIPPINGS
Admission avoidance hospital at home
Admission avoidance hospital at home is a service that provides active treatment by health careprofessionals in the patient’s home for a condition that otherwise would require acute hospitalin-patient care, and always for a limited time period. We conducted a systematic review andmeta analysis, using individual patient data when available, to determine the effectiveness andcost of managing patients with admission avoidance hospital at home compared with in-patienthospital care. We performed meta-analyses where there was sufficient similarity among thetrials and where common outcomes had been measured. There is no evidence from theseanalyses to suggest that admission avoidance hospital at home leads to outcomes that differfrom inpatient hospital care.
Shepperd S, Doll H, Angus RM, Clarke MJ, Iliffe S, Kalra L, Ricauda NA, WilsonAD. Admission avoidance hospital at home. Cochrane Database of Systematic Reviews2008, Issue 4. Art. No.: CD007491. DOI: 10.1002/14651858.CD007491. This versionfirst published online: October 08. 2008

2009; 11(1) : 95
95
UNUSUAL COMPLICATION OFNASOGASTRIC TUBE INSERTIONIN A CHILD
* Poovazhagi V* Shanthi S
* Vijayaraghavan A** Kulandai Kasturi R
Naso gastric tube placement is a commonintervention in any pediatric intensive care unit(PICU) while managing a critically ill child.We report a rare complication of knotting ofnasogastric tube (NGT) in a child, who wasadmitted with suspected poisoning of an unknowndrug. The difficulty encountered during NGTremoval was later found to be due to knotting ofthe distal end of the NG tube. Care has to betaken during routine procedures like insertion ofnaso gastric tube or else complications may occurwith varied consequences.
Case Report
A 6 year old child presented to ouremergency room (ER) in a state ofunresponsiveness and was suspected to havepoisoning due to some medication. As part ofinitial stabilization a 12 French nasogastric tubewas inserted and child received a stomach washat the ER. Child was shifted to the PICU andneeded mechanical ventilation. Child’s clinicalparameters improved and he regainedconsciousness after 48 hours. Surprisingly an
CASE STUDY
attempt to remove the nasogastric tube on thesecond day by the nursing staff was difficult andthere appeared to be some resistance whilewithdrawing, at the level of the nasopharynx.Further effort to remove the tube by a seniormember of the team proved successful, only toreveal a tight knot at the tip of the nasogastrictube (Fig.1). In this case, a loose knot had mostprobably formed in the nasogastric tube atinsertion or later and during retrieval the knotmight have got tightened up. Knots form in thestomach when excess tubing is advancedinadvertently, allowing it to loop back on itself andform a knot in the stomach cavity.
Discussion
Nasogastric tubes are commonly used indaily practice both for stomach decompressionand for feeding purposes. Though their use is veryfrequent and simple, they are at times associatedwith complications. Reported complication ratesvary widely from 0.3% to 8%. Pneumothoraces
* Assistant Professor,** Professor of Pediatrics,
PICU, Institute of Child Health and Hospital forChildren, Chennai.
Fig.1. Knot at the end of thenasogastric tube

Indian Journal of Practical Pediatrics 2009; 11(1) : 96
96
accounted for approximately 60% ofcomplications. Fifty percent of these required achest drain. In 15%, the misdirected NG tube inthe bronchus did not cause any complications.1
In the case of knot posing difficulty in removal atthe level of nasopharynx it can be removedretrograde via the oral cavity. Difficulty in removalof the knotted NGT can be managed byendoscopic removal. The complication of knottingof nasogastric (NG) tubes on removal occursinfrequently with small diameter feeding tubes.Knotting of large caliber NG tubes is even moreuncommon.2
Too much of insertion of NGT has beenrecognized as a risk factor for knotting . A smallgastric remnant has also been reported to be arisk factor to knot formation.3 The severity ofcomplications in NGT placement can be fromasymptomatic coiling to life threateninginadvertent misplacement. Complications ofnasoenteric tubes frequently include inadvertentmalposition, epistaxis, sinusitis, inadvertent tuberemoval, tube clogging and aspiration pneumonia.4Rarely reported are misplacement of the tube inthe bronchus leading to complications,intravascular penetration and intra cranial entry.1Most of this morbidity is avoidable with carefulattention to details when placing the tube andcareful management of the tube on a day to daybasis. Tube designs influence its safety.Current polyurethane fine bore tubes have evolvedfrom the earlier use of latex, silicon andpolyvinylchloride tubes. Polyurethane does notstiffen, embrittle or biodegrade in vivo.This reduces the risk of enteric perforation and
tube cracks. Polyurethane is very flexible and hasa larger lumen to wall thickness ratio.
Most of the important complications of NGTplacement are related to penetrating theesophagus or passing the tube in trachea andbronchi. These misplacements will not be seen inthe abdominal x-ray. The traditional physicalexamination-based methods of assessing properNGT placement are inadequate when applied tothe small-bore tubes. Only a chest x-ray canassure placement in the stomach.Hence appropriate care has to be taken duringthe simple procedure of NGT insertion to preventthe rare complications.
Acknowledgement: We thank,Prof. T.L.Ratnakumari, for her guidance in thewrite up.
References
1. Pillai JB, Vegas A, Brister S. Thoraciccomplications of nasogastric tube: Review ofsafe practice. Interact CardioVasc Thorac Surg2005;4:429-433.
2. Dinsmore RC, Benson JF. Endoscopic removalof a knotted nasogastric tube lodged in theposterior nasopharynx. South Med J 1999;92:1005-1007.
3. Cappel MS, Scarpa PJ, Nadler S, Miller SH .Complications of nasoenteral tubes. Intragastrictube knotting and intragastric tube breakage.J Clin Gastroenterol 1992; 14:144-147.
4. Baskin WN. Acute complications associatedwith bedside placement of feeding tubes. NutrClin Pract 2006; 21:40-55.
Answer to picture quiz : Cornelia de Lange Syndrome
This 6 months old male have typical facies with bushy eyebrows meeting in midline (synophrys), longcurly eyelashes, hirsuitism, long philtrum, antiverted nostrils and down turned angles of mouth (Fig.1).Also has bifid scrotum and undescended testis on the left side (Fig.2).

2009; 11(1) : 97
97
CONGENITAL MILIARYTUBERCULOSIS
* Vijaya Kumari** Suresh V
Congenital tuberculosis (TB) is a rare entityand only few authentic cases have been reportedso far in India.1,2 Tuberculous bacillemia duringpregnancy may result in infection of the maternalgenital tract.3,4 Such infection may then betransmitted to the fetus by hematogenous spreadthrough placenta, in-utero aspiration and ingestionof infected amniotic fluid or secretions duringdelivery.5 The hematogenous route and in-uteroaspiration accounts for approximately half of thecases. In addition postnatal infection may occurfrom contact with a contagious mother or careror ingestion of infected breast milk from a motherwith TB breast abscess.6 Congenital TB is rareif the mother received adequate treatment duringpregnancy.4 We report an infant with congenitalTB who presented to us with respiratory distressand abdominal distension.
Case Report
An 88 days old male baby weighing 4.5 kgdelivered via naturalis presented with fever,recurrent cough and respiratory distress since20 days of birth. Baby was treated for acuteexacerbations with antibiotics, nebulization andsteroids. As respiratory distress increased andbaby did not feed for 2 days he was admitted for
CASE STUDY
evaluation. Birth weight was 2.5kg and there wasno history of birth asphyxia. Baby was kept inNICU for respiratory distress, treated as transienttachypnea of newborn initially and later forhyperbilirubinemia for 7 days. Baby was givenBCG vaccination at birth and triple antigen withOPV at the age of 1½ month. Antenatally motherwas registered and she gave history of recurrentcough with fever during her 8th month ofpregnancy which was treated symptomatically.
On examination the baby was irritable, febrile[102°F], had severe respiratory distress andsubcostal retraction. His respiratory rate was80/min and heart rate was 166/min with oxygensaturation at 78% in room air. Baby had mildabdominal distension with hepatomegaly 7cmbelow right costal margin and splenomegaly 3cmbelow left costal margin. Neurologically, anteriorfontenelle was normal and there was no focaldeficit.
As chest x-ray revealed extensive miliarymottling in both lungs (Fig.1), baby wasinvestigated for possible causes of mottlingin an infant. Blood tests revealed mildanemia (8.5g/dL), total leukocyte count of14,600 cells/cubic mm, differential count of72% neutrophils and ESR of 16mm in 1 hour.HIV 1 and 2 were non reactive and his liverfunctions were normal with SGOT of 34 IU/Land SGPT 37 IU/L. Mantoux test was 13mmpositive. Smear from gastric aspirate forAFB was positive (1+) on day 1. IgM and IgGElisa tests for CMV were positive. CSF analysiswas normal. Ultrasound abdomen revealedhepatosplenomegaly. Blood culture andCSF culture were sterile. CT brain was normal.
* Post Graduate,** Consultant Pediatrician and Neonatal Intensivist,
SKS Hospital, Salem, Tamilnadu.

Indian Journal of Practical Pediatrics 2009; 11(1) : 98
98
Fundus examination was negative for choroiditisor choroidal tubercles and was confirmed byophthalmologist. CT thorax revealed segmentalconsolidation in the left lower lobe, multiple smalldiscrete and confluent centriacinar nodules in asymmetrical basal distribution in both lungs (Fig.2).There were multiple enlarged, confluent, necroticmediastinal and right hilar lymph nodes present(Fig.3).
ESR was raised, Mantoux test was positiveand smear for AFB was positive, tuberculousetiology for military mottling in this infant wasconfirmed. Family members were screened forthe probable source of infection. Father andgrandmother’s chest X-rays were normal andMantoux test was negative in grandmother thoughweakly positive in father [9mm]. Mother’s chestX-ray was not significant but her ESR was high[57mm in 1 hour] and Mantoux test was highlypositive [60mm x 30mm] with ulceration. She wasadvised endometrial biopsy to look for genitaltuberculous lesion for which she did not return.During his week long hospital stay baby wasmanaged with O2, nebulization, IV steroids andantituberculous treatment with four drugs.Baby was supported with antibiotics, anti-emeticsand H2 blockers. At discharge, baby’s respiratorydistress and hepatospleno-megaly decreased;
repeat chest x-ray revealed miliary mottling withdecrease in size of hilar lymphadenopatahy. Babywas advised prednisolone 2.5mg twice daily andantituberculous drugs, four drugs regimen[Streptomycin, Rifampicin, Pyrazinamide andIsoniazid] for 2 months and two drugs for9 months at discharge. He came for follow-upafter one week with mild distress which decreasedwith nebulisation and later he didnot turn up.
Discussion
The diagnosis of congenital TB is oftendifficult. According to Cantwell, et al7, the infantmust have proved tuberculous lesions and at leastone of the following: (1) lesion in the first weekof life, (2) a primary hepatic complex or caseatinghepatic granulomas, (3) tuberculous infection ofthe placenta or the maternal genital tract or(4) exclusion of the possibility of post nataltransmission by a thorough investigation ofcontacts. The median age at presentation is24 days, range 1 to 84. The onset of symptomsvaries from the first few days of life to a fewmonths of age with an average 2-4 weeks.The clinical manifestations are often nonspecificand include fever, respiratory distress, abdominaldistension, lethargy, irritability, hepato-splenomegaly, lymphadenopathy, jaundice, ear
Fig 1. Chest X- ray showing extensivemiliary mottling both lungs
Fig 2. CT Scan of Chest showingmultiple centri-acinar nodules sym-metrically in both lungs

2009; 11(1) : 99
99
discharge and skin papules.3 CNS involvementoccurs in fewer than 50% cases.8 In most infantswith congenital TB chest radiographs areabnormal at presentation and include non specificparenchymal infiltrates, adenopathy and miliarymottling (50%).
Although gastric aspirate cultures are saidto be a poor diagnostic tool, it has been associatedwith a high yield of positive cultures ofM. tuberculosis in most of the reported cases ofcongenital TB.8 Gastric aspirate and PCR forAFB are the most expedient and reliable waysof establishing the diagnosis. The yield in CSF isusually low. Demonstration of a primary hepaticcomplex which requires an open surgicalprocedure or autopsy is not essential fordiagnosis.6 A percutaneous liver biopsy specimendemonstrating caseating granulomas is sufficientfor diagnosis. Our patient presented withrespiratory distress and hepato splenomegaly.Chest Xray revealed miliary mottling whichprompted us to evaluate the probable source ofinfection which is baby’s mother in this case.As the baby didn’t have features of intrauterine
CMV infection like IUGR, microcephaly,congenital chorioretinitis, periventricularcalcifications, thrombocytopenia, sensorineuraldeafness9,10 CMV in this baby could have beenacquired after birth.
References
1. Sosa LM, Calla LL, Mantilla JC. Congenitaltuberculosis associated with maternaldisseminated miliary tuberculosis. Biomedica2007; 27:475-482.
2. Kumar R, Gupta N, Sabharwal AS. CongenitalTuberculosis. Indian J Pediatr 2005;72: 631- 633.
3. Skevaki CL, Kafetzis D. Tuberculosis inneonates and infants: Epidemiology,pathogenesis, clinical manifestations, diagnosisand management issues. Pediatr Drugs 2005; 7:219-234.
4. Vallejo JG, Starke JR. Tuberculosis andpregnancy. Clin Chest Med 1992; 13:693-707.
5. Chotpitayasunondh T, Sangtawesin V.Congenital tuberculosis. J Med Assoc Thai2003;86:689-695.
6. Pablo JS, Amina A. Tuberculosis. In: TaeuschHW, Ballard RA and Gleason CA. Eds, Avery’sDiseases of the Newborn. 8
th Edn, Philadelphia,
W. B. Saunders, 2005; pp 542-547.7. Cantwell MF, shehab ZM, Costello AM, et al.
Brief report: Congenital tuberculosis. N Engl JMed 1994; 330: 1051 - 1054.
8. Chanta C, Jariyapongpaibul Y, Triratanapa K.Congenital Tuberculosis presenting as SepsisSyndrome. J Med Assoc Thai 2004;87:573-577.
9. Fowler KB, Pass RF. Risk factors for congenitalcytomegalovirus infection in the offspring ofyoung women. Pediatrics 2006; 118:286-292.
10. Schleiss MR, Mc Voy MA. Overview ofcongenitally and perinatally acquiredcytomegalovirus infections. Expert rev AntiInfect Ther 2004; 2:389-403.
Fig 3. CT Thorax showing necroticenlarged multiple mediastinal andright hilar Lymph nodes

Indian Journal of Practical Pediatrics 2009; 11(1) : 100
100
Building Happier Lives through Medicare

2009; 11(1) : 101
101
National Assembly on Pediatric Emergency Medicine“India-International Conference on Pediatric Emergency and Acute care”
27thFeb to 1st March 2009Organized by : Society for Trauma and Emergency Pediatrics, India
IAP, Delhi Branch and Centre for Child Health, Sir Ganga Ram Hospital, New DelhiVenue: India International Centre, 40 Max Mueller Marg, New Delhi
The National Assembly on Pediatric Emergency Medicine is not just another pediatric conference. It is going to be an amazinglearning experience, designed specifically for those who are involved in pediatric emergency care whether in a hospital settingor out of hospital setting. It will provide insight for most critical areas of your practice and empower the delegates with theknowledge necessary to translate science into practice and enhance the ability to treat not only common but most bizarrepediatric emergencies as well. This will provide current, evidence-based practice information and promises to reach furtherand deliver more by featuring:
• Outstanding National and International faculty• Contentious and Contemporary topics based on leading-edge research• An extraordinary amalgamation of wisdom and knowledge
If you practice Pediatric Emergency Medicine, Pediatric Intensive Care, General Pediatrics, or Family practice and treatemergent patients, this conference is designed for you! Don’t delay, register now.
• Pediatric Emergency Medicine and Acute Care in India: Past, Present and Future• Pediatric Pre-hospital Care in India: Need of innovation and instigation• Trauma Emergencies: Trauma fluid resuscitation, Head injury, Sport concussion, Trauma panel• Neuro-Emergencies: Pediatric Meningitis in 2009, Status Epilepticus: Beyond benzodiazepines, Pediatric
Stroke- Investigation and Management,• Cardiovascular Emergencies: Sepsis Guidelines 2008 : The Indian Adaptation and Implementation ,
When the pump fails: Contemporary management strategies for pediatricians• Respiratory Emergencies: Evidence Based Management of Bronchiolitis, Croup and Asthma• Infections: Community Acquired Infections including MRSA, Managing a febrile infant < 3 months in
era of Hib and Pneumoccoccal Vaccination, Defiant Malaria- How the management has changed• Surgical Emergencies: Identification and Medical Management of Surgical Emergencies, Surgeon’s
View on Medical Management• Emergency Services: Setting up Pediatric Emergency Services, Medical Transport, Disaster Triage,
Prehospital Care• Meet the Emergency Experts: Listen to his clinical case or bring your own• Pediatric Office Emergencies: Pearls from the pediatric eye, ENT, dental and emergency experts, Chest
pain- when to worry and what to do, Fainting fallacies- investigating a pediatric syncope- when, whatand how much, Do you know what are you seeing- perplexing visual diagnosis, One pill can kill
Pre-conference WorkshopsFor Doctors: Workshop on Pediatric Emergency Procedures, For Nurses, Paramedics and General Public:Pediatric Advanced Life Support Course for Nurses, Emergency Preparedness Workshop for SchoolHealthcare Providers, PEARS (Pediatric Emergency Assessment, Recognition and Stabilization) Course,Basil Life Support
Registration DetailsRegistration Fee: Upto 31st Jan 2009: Rs 2000/- After 31st Jan 2009: Rs 2500/- by Cash/Cheque/Draft in favor of“STEP, India” payable at Delhi (Spot Registration may not be available due to heavy booking)Conference Secretariat: Pediatric Ground Floor (Ward No. 6), Centre for Child Health, Sir Ganga Ram Hospital,Rajender Nagar New Delhi 110060, Phone: 42251094/42251156, [email protected] Chairman Organizing SecretaryProf. Sunit Singhi (PGI, Chandigarh) Dr Suresh Gupta (Sir Ganga Ram Hospital)Phone: 09417089782, [email protected] Phone: 9811426628, [email protected]

Indian Journal of Practical Pediatrics 2009; 11(1) : 102
102
INDIAN JOURNAL OF PRACTICAL PEDIATRICSSUBSCRIPTION TARIFF
JOURNAL OFFICE Official Journal of the Indian Academy of Pediatrics1A, Block II, Krsna Apartments, A quarterly medical journal committed to practical50, Halls Road, Egmore, pediatric problems and management updateChennai 600 008, Tamilnadu, India.Phone: +91-44-28190032, 42052900.Email: [email protected]
Enter ONE yearSubscriptionfor TEN years
Name ..................................................................................................................................
Address ................................................................................................................................
...............................................................................................................................................
City ...............................................................State ................................................................
Pin .............................. Phone (R) ...................................... (O)............................................
Mobile ...................................... Email ...................................................................................
Designation ................................................. Qualification........................................................
I am enclosing a DD No. …………….. dated ……………… drawn on ………..……...............
favoring Indian Journal of Practical Pediatrics for Rs……………
Signature
For office use
Ref. No.
Cash / DD for Rs.
DD No.
Receipt No. & Date
Subscription rate
Individual Annual Rs.400/-Ten Years Rs.4000/-
Institution Annual Rs.500/-Ten Years Rs.5000/-
Foreign Annual US $ 60/-
Send your subscription, only by crossed demanddraft, drawn in favour of INDIAN JOURNAL OFPRACTICAL PEDIATRICS, payable at Chennai andmail to Dr. K. NENDUNCHELIAN, Editor-in-Chief,1A, Block II, Krsna Apartments, 50, Halls Road,Egmore, Chennai 600 008, Tamilnadu, India.
IJPP

2009; 11(1) : 103
103
TOXICOLOGY
ISSN 0972-9607
VOL.11 NO.1
JAN.-MAR. 2009
TOXICOLOGY
ISSN 0972-9607
VOL.11 NO.1
JAN.-MAR. 2009

Indian Journal of Practical Pediatrics 2009; 11(1) : 104
104
JOURNAL COMMITTEE
Editor-in-ChiefDr.K.Nedunchelian
Executive EditorDr.S.Thangavelu
Managing EditorDr.N.C.Gowrishankar
Associate EditorsDr.Janani Sankar
Dr.P.RamachandranDr.T.L.Ratnakumari
Dr.C.V.RavisekarDr.S.Shanthi
Executive MembersDr.G.Durai Arasan
Dr.S.LakshmiDr.V.Lakshmi
Dr.E.MahenderDr.V.PoovazhagiDr.T.Ravikumar
Dr.Shanthi RameshDr.So.Shivbalan
Dr.Rohit C. Agrawal(Ex-officio)
NATIONAL ADVISORY BOARD
President 2009, IAP
Dr.Panna Choudhury
President 2010, IAP
Dr.Deepak Ugra
Editor-in-Chief, IP
Dr.Piyush Gupta
Members
Dr. Atul Kumar Agarwal
Dr.Bir Prakash Jaiswal
Dr.U.S.Jagdish Chandra
Dr. Lalitha Kailash
Dr.Monjori Mitra
Dr.Saradha Suresh
Dr.Shyamal Sen
Dr.Vijay N Yewale
Emeritus Editors
Dr.A.Parthasarathy
Dr.B.R.Nammalwar
Dr.M.Vijayakumar
Dr.A.Balachandran
Indian Journal ofPractical Pediatrics
Subscription Journal of theIndian Academy of Pediatrics
IJPP

2009; 11(1) : 105
105
PresidentDr.Panna Choudhury
President-2010Dr.Deepak UgraPresident-2008Dr.R.K.AgarwalVice President
Secretary GeneralDr.Rohit C Agrawal
TreasurerDr.Tanmay AmladiEditor-in-Chief, IP
Dr.Piyush GuptaEditor-in-Chief, IJPP
Dr.K.NedunchelianJoint Secretary
Dr.S.SanjayMembers of the Executive Board
Andhra PradeshDr.M.Arif Ahmed
Dr.Neeli RamchanderDr.P.Sudershan Reddy
Assam
BiharDr.Arun Kumar Thakur
ChandigarhDr.Sunit C. Singhi
ChhattisgarhDr.Arvind Prakash Savant
DelhiDr.Sangeeta Yadav
Dr.A.S.VasudevGujarat
Dr.Abhay Kantilal ShahDr.Yagnesh O Popat
HaryanaDr.Mahaveer Prasad Jain
Jammu & KashmirDr.Ashok Kumar Gupta
JharkhandDr.Arun Kumar Sharma
KarnatakaDr.R.Kishore Kumar
Dr.D.NarayanappaDr.R.Nisarga
KeralaDr.Achamma Joseph
Dr.George F MoolayilDr.T.U.SukumaranMadhya Pradesh
Dr.Vishwambhar P GoswamiDr.P.G.Walvekar
MaharashtraDr.Hemant A Joshi
Dr.Manoj T RathiDr.Pravin J Mehta
Dr.Upendra S. KinjawadekarDr.Vasant M Khalatkar
OrissaDr.Niranjan Mohanty
PunjabDr.Harmesh Singh
RajasthanDr.Rajiv Kumar Bansal
Dr.Tarun PatniTamilnadu
Dr.S.VenkateshwaranTripura
Dr.C.M.ChhajerUttarkhand
Dr.Sandhya BhatnakarUttar Pradesh
Dr.Ashok Kumar RaiDr.Atul Kumar Agarwal
Dr.Vineet K SaxenaWest BengalDr.Arup Roy
Dr.Nabendu ChaudhuriDr.Subroto Chakrabartty
Services
IAP’s Spl. Representative
A.A.A.Dr.Vijay N Yewale
Indian Academyof Pediatrics
Kailash Darshan, Kennedy Bridge,Mumbai - 400 007.IAP Team - 2009

Indian Journal of Practical Pediatrics 2009; 11(1) : 106
106
1A, Block II, Krsna Apartments,50, Halls Road, Egmore, Chennai 600 008,
1A, Block II, Krsna Apartments,50, Halls Road, Egmore, Chennai 600 008,