infarction - warszawski uniwersytet medycznypathology.wum.edu.pl/en/system/files/infarction.pdf ·...
TRANSCRIPT

1
Myocardial infarction
The normal views

2
What is Ischemic Heart Disease?
- Ischemic heart disease is caused by an imbalance betweenthe myocardial blood flow and the metabolic demand of themyocardium. - Reduction in coronary blood flow is related to progressiveatherosclerosis with increasing occlusion of coronary arteries. Blood flow can be further decreased by superimposed eventssuch as vasospasm, thrombosis, or circulatory changes leadingto hypoperfusion.- Coronary artery perfusion depends upon the pressuredifferential between the ostia (aortic diastolic pressure) andcoronary sinus (right atrial pressure). Coronary blood flow isreduced during systole because of Venturi effects at thecoronary orifices and compression of intramuscular arteriesduring ventricular contraction.
Factors reducing coronary blood flow include:
1. Decreased aortic diastolic pressure
2. Increased intraventricular pressure and myocardial contraction
3. Coronary artery stenosis, which can be further subdivided intothe following etiologies:
- Fixed coronary stenosis- Acute plaque change (rupture, hemorrhage)- Coronary artery thrombosis- Vasoconstriction
4. Aortic valve stenosis and regurgitation
5. Increased right atrial pressure

3
……40 micron collateral vessels are present in all hearts withpressure gradients permitting flow, despite occlusion of major vessels. In general, the cross-sectional area of the coronaryartery lumen must be reduced by more than 75% to significantly affect perfusion. Coronary atherosclerosis isdiffuse (involving more than one major arterial branch) but isoften segmental, and typically involves the proximal 2 cm ofarteries (epicardial).
"Thrombolytic therapy" with agents such as streptokinaseor tissue plasminogen activator (TPA) is often used to tryand lyse a recently formed thrombus. Such therapy withlysis of the thrombus can re-establish blood flow in a majority of cases. This helps to prevent significantmyocardial injury, if early (less than an hour or so) in thecourse of events, and can at least help to reduce furtherdamage.
This is a normal coronary artery. Thelumen is large, without any narrowingby atheromatous plaque. Themuscular arterial wall is of normalproportion.
The coronary artery shown here hasnarrowing of the lumen due to buildup of atherosclerotic plaque. Severenarrowing can lead to angina, ischemia, and infarction.
This section of coronary arterydemonstrates remote thrombosiswith recanalization to leave only twosmall, narrow channels.
4
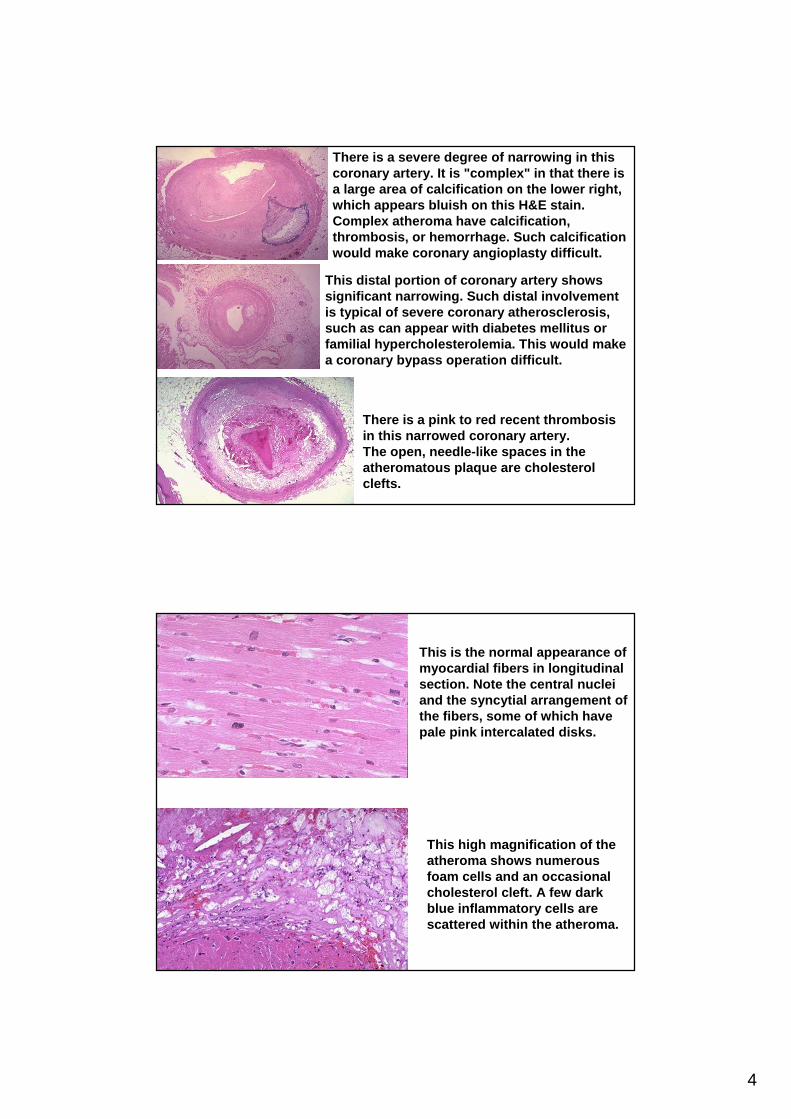
There is a severe degree of narrowing in thiscoronary artery. It is "complex" in that there isa large area of calcification on the lower right, which appears bluish on this H&E stain. Complex atheroma have calcification, thrombosis, or hemorrhage. Such calcificationwould make coronary angioplasty difficult.
This distal portion of coronary artery showssignificant narrowing. Such distal involvementis typical of severe coronary atherosclerosis, such as can appear with diabetes mellitus orfamilial hypercholesterolemia. This would make a coronary bypass operation difficult.
There is a pink to red recent thrombosisin this narrowed coronary artery . The open, needle-like spaces in theatheromatous plaque are cholesterol clefts.
This is the normal appearance ofmyocardial fibers in longitudinalsection. Note the central nucleiand the syncytial arrangement ofthe fibers, some of which havepale pink intercalated disks.
This high magnification of theatheroma shows numerousfoam cells and an occasionalcholesterol cleft. A few darkblue inflammatory cells arescattered within the atheroma.

5
Patterns of Ischemic Heart Disease (IHD)
Angina pectoris - a symptom complex of IHD characterized by paroxysmal attacks of chest pain, usually substernal or precordial, caused by myocardial ischemia that falls short of inducing infarction. There are several patterns:
1. Stable angina (typical) - paroxysms of pain related to exertion andrelieved by rest or vasodilators.subendocardial ischemia with ST-segment depression
2. Variant or Prinzmetal's angina - angina that classically occurs atrest and is caused by reversible spasm in normal to severelyatherosclerotic coronary arteries. ST-segment elevation or depressionmaybe seen during attacks.
3. Unstable angina - prolonged pain, pain at rest in a person withstable angina, or worsening of pain in stable angina. ST-segment depression (usually) and ST-segment elevation.
4. Sudden cardiac death - Unexpected death from cardiac causesusually within one hour after a cardiac event or without the onset ofsymptoms. Usually high-grade stenosis with acute coronary changes.
Myocardial infarction
- A myocardial infarct represents permanent cellularinjury and necrosis after a prolonged ischaemicepisode.
- In the vast majority (ca. 90%) of cases it followsfrom a thrombotic occlusion superimposed on atherosclerotic obstructive coronary artery disease.
- Rarely infarction follows coronary emboli, spasm, dissection or vasculitis.

6
Myocardial infarction
Symptoms Comments
Most Retrosternal chest pain May radiate to neck, back and arm .Patients ”heaviness”,”tightness”, Patient may be nauseated and/or
”weight”. Poor response perspire.or failure to respond tonitrates.
Diabetics There may be none. Unexplained diabetic com a shouldHeart failure raise suspicion. unexplained.
Heart No pain. Failure or Very poor prognosis, urgentTransplant shock (sudden death) retransplant only option.
Elderly May be none. Typicalpain and/or breathlessness.Unexplained heart failure.
INFARCT LOCALIZATION
Infarcts are categorized into:
- ANTERIOR, which usually involve occlusion ofthe left coronary artery, in particular the leftanterior descending (LAD)(The subdivisions: anteroseptal, lateral, anterolateral)
- INFERIOR, which usually reflect right coronaryocclusion but occasionally circumflexocclusion(The subdivisions: interior, inferolateral, infero-septal)
- POSTERIOR, which may involve right orcircumflex system.

7
The gross morphologic appearance of a myocardial infarction can vary. Patterns include:
- Transmural infarct - involving the entire thickness of the leftventricular wall from endocardium to epicardium, usually theanterior free wall and posterior free wall and septum withextension into the RV wall in 15-30%. Isolated infarcts of RV and right atrium are extremely rare.
- Subendocardial infarct - multifocal areas of necrosisconfined to the inner 1/3-1/2 of the left ventricular wall. Thesedo not show the same evolution of changes seen in a transmural MI.
MYOCARDIAL INFARCTIONGross morphologic changes evolve over time as follows:
White fibrosis7 weeks
Maximally yellow and soft with vascular margins10 - 21 Days
Hyperemic border with central yellowing3 - 7 Days
Pallor with some hyperemia24 - 72 Hours
Pallor of myocardium18 - 24 Hours
Gross Morphologic FindingTime from Onset

8
The anterior surface ofthe heart demonstratesan opened left anteriordescending coronaryartery.Within the lumen of the coronary can be seen a dark red recentcoronary thrombosis. The dull red color to themyocardium as seenbelow the glisteningepicardium to the lowerright of the thrombus isconsistent withunderlying myocardialinfarction.
This is the left ventricular wall which has been sectionedlengthwise to reveal a large recent myocardial infarctio n. Thecenter of the infarct contains necrotic muscle that appear syellow-tan. Surrounding this is a zone of red hyperemia. Remaining viable myocardium is reddish- brown.

9
This cross section through the heart demonstrates the leftventricle on the left. Extending from the anterior portio n andinto the septum is a large recent myocardial infarction. T hecenter is tan with surrounding hyperemia. The infarctio n is"transmural" in that it extends through the full thickness ofthe wall.
MYOCARDIAL INFARCTIONMicroscopic morphologic changes evolve over time as follows:
Fibrosis7 Weeks
Fibrovascular response with prominent granulationtissue
10 - 21 Days
Macrophage and mononuclear infiltration begin, fibrovascular response begins
3 - 7 Days
Total loss of nuclei and striations along with heavyneutrophilic infiltrate
24 - 72 Hours
Continuing coagulation necrosis, pyknosis of nuclei, andmarginal contraction bands
18 - 24 Hours
Coagulation necrosis with loss of cross striations, contraction bands, edema, hemorrhage, and earlyneutrophilic infiltrate
4 - 12 Hours
Staining defect with tetrazolium or basic fuchsin dye2 - 3 Hours
Wavy myocardial fibers1 - 3 Hours
Microscopic Morphologic FindingTime from Onset

10
The earliest change histologicallyseen with acute myocardial infarctionin the first day is contraction bandnecrosis. The myocardial fibers arebeginning to lose cross striations andthe nuclei are not clearly visible inmost of the cells seen here. Note themany irregular darker pink wavycontraction bands exten-ding acrossthe fibers.
This high power microscopic view of themyocardium demonstrates an infarction ofabout 1 to 2 days in duration. Themyocardial fibers have dark red contraction bands extending across them. The myocardial cell nuclei have almost alldisappeared. There is beginning acuteinflammation. Clinically, such an acutemyocardial infarction is marked by changes in the electrocardiogram and by a rise in the MB fraction of creatine kinase.
In this microscopic view of a recent myocardial infarction, there is extensive hemorrhagealong with myocardial fibernecrosis with contraction bandsand loss of nuclei.
This myocardial infarction isabout 3 to 4 days old. There isan extensive acute inflammatorycell infiltrate and the myocardialfibers are so necrotic that theoutlines of them are only barelyvisible.

11
This is an intermediatemyocardial infarction of 1 to 2 weeks in age. Note that there areremaining normal myocardialfibers at the top. Below thesefibers are many macrophagesalong with numerous capillariesand little collagenization.
There is pale white collagenwithin the interstitiumbetween myocardial fibers. This represents an area ofremote infarction.
The mentioned gross and microscopicchanges over time can vary. In general, a larger infarct will evolve through thesechanges more slowly than a small infarct. Clinical complications of myocardialinfarction will depend upon the size andlocation of the infarction, as well as pre-existing myocardial damage.

12
COMPLICATIONS CAN INCLUDE:- Arrhythmias and conduction defects, with possible "sudd endeath"- Extension of infarction, or re-infarction- Congestive heart failure (pulmonary edema)- Cardiogenic shock- Pericarditis- Mural thrombosis, with possible embolization- Myocardial wall rupture, with possible tamponade- Papillary muscle rupture, with possible valvular insuff iciency- Ventricular aneurysm formation
Sudden death is defined as death occurring within an hour ofonset of symptoms. Such an occurrence often complicatesischemic heart disease. Such patients tend to have severecoronary atherosclerosis (>75% lumenal narrowing). Often, a complication such as coronary thrombosis or plaquehemorrhage or rupture has occurred. The mechanism ofdeath is usually an arrhythmia.
Echocardiogramafter acute inferior
myocardialinfarction.
The posterobasaland diaphragmatic
segments areakinetic.

13
One complication of a transmuralmyocardial infarction is rupture ofthe myocardium. This is most likelyto occur in the first week between 3 to 5 days following the initial event, when the myocardium is thesoftest. The white arrow marks the point ofrupture in this anterior-inferiormyocardial infarction of the leftventricular free wall and septum. Note the dark red blood clotforming the hemopericardium. Thehemopericardium can lead to tamponade.
An example ofhemopericardium: such a massiveamount ofhemorrhage canlead to cardiactamponade.

14
In cross section, the point of rupture of the myocardium is shown with thearrow. In this case, there was a previous myocardial in farction 3 weeksbefore, and another myocardial infarction occurred, rup turing through thealready thin ventricular wall 3 days later.
A complication ofinfarction is aneurysmformation, which is the
bulge seen here in the leftventricular wall. Note thevery thin white wall of the
aneurysm toward the apex.

15
Ischemic Cardiomyopathy
In this condition, there may be previous myocardial infa rction, but the disease results from severe coronary atherosclero sisinvolving all major branches. The result is an inadequatevascular supply which leads to myocyte loss. The myocyte l osscoupled with fibrosis in the form of interstitial collagendeposition results in decreased compliance, which along w iththe accompanying cardiac dilation, results in overload ofremaining myocytes. This keeps the process going, withcompensation by continuing myocyte hypertrophy. There m ayeven be compensation through hyperplasia as well as hypertrophy, which can explain the enormous size (2 to 3 timesnormal size) of the resulting heart. Eventually, the hea rt can no longer compensate, and cardiac failure ensues witharrhythmias and/or ischemic events.
Thus, clinically, there is slow, progressive heart fail ure with orwithout a history of a previous MI or anginal pain. Ische miccardiomyopathy is responsible for as much as 40% of themortality in IHD.
The myocytes here are hypertrophied, marked by the large, darknuclei, and there is interstitial fibrosis. This is an exa mple of
cardiomyopathy. In this case, long-standing, severe o cclusiveatherosclerosis led to "ischemic" cardiomyopathy.
16
Electrocardiogram (ECG)
PRACTICAL POINTS
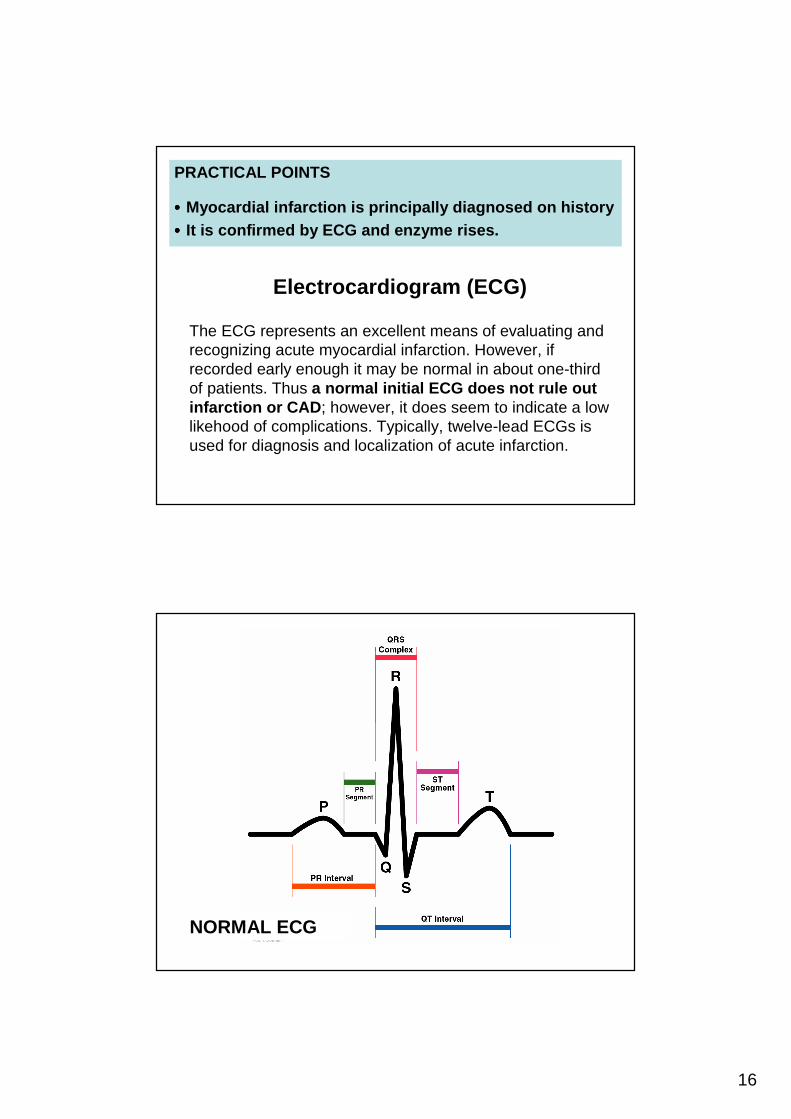
•••• Myocardial infarction is principally diagnosed on histor y•••• It is confirmed by ECG and enzyme rises.
The ECG represents an excellent means of evaluating andrecognizing acute myocardial infarction. However, ifrecorded early enough it may be normal in about one-thirdof patients. Thus a normal initial ECG does not rule out infarction or CAD; however, it does seem to indicate a lowlikehood of complications. Typically, twelve-lead ECGs isused for diagnosis and localization of acute infarction.
NORMAL ECG

17
Electrocardiogram (ECG) of a normal single heartbeat. The profile consists of 5 major waves: P, Q, R, S, and T. The P and QRS peaksrepresent atrial and ventricularcontractions, respectively. The T wave reflects electrical recovery ofthe ventricles.
Electrocardiogram (ECG) hours to days after an acute myocardialinfarction (AMI). Typicalcharacteristics are elevation of theST segment, inversion of the T wave and an enlarged Q wave.
EVOLVING ECG CHANGES OF MYOCARDIAL INFARCTION

18
EVOLVING ECG CHANGES OF MYOCARDIAL INFARCTION
ST segment elevation with tallpeaked T waves in the leadsorientated to the damaged areas –the hyperacute phase of epicardialinjury.
EVOLVING ECG CHANGES OF MYOCARDIAL INFARCTION
Q waves appear withinhours and ST elevationpersists. Pathological Q waves are usually 0.04 seconds or greater induration and/or to a depth equivalent to 25% of the height of the R wave.

19
EVOLVING ECG CHANGES OF MYOCARDIAL INFARCTION
In the subsequent daysthe ST segmentsgradually return to baseline and T waveinversion occurs.
EVOLVING ECG CHANGES OF MYOCARDIAL INFARCTION
Over weeks the ST segment usuallyreverts to normal; persistent elevation after six weekssuggests aneurysm formation. Although Q waves usually remain atfollow-up, 10% may have normalECGs.
20
Laboratory Diagnosis of Myocardial Infarction
A number of laboratory tests are available. None iscompletely sensitive and specific for myocardial infarct ion, particularly in the hours following onset of symptoms. Timing is important, as are correlation with patientsymptoms, electrocardiograms, and angiographic studie s.
The following tests are available as markersfor acute myocardial infarction:
- Creatine Kinase - Total- Creatine Kinase - MB Fraction- CK-MB Isoforms
- Troponins (I and T)- Myoglobin- Lactate dehydrogenase
Creatine Kinase - Total:
The total CK is a simple and inexpensive test that is readily available using many laboratoryinstruments. However, an elevation in total CK is not specific for myocardial injury, because
most CK is located in skeletal muscle, andelevations are possible from a variety of non-
cardiac conditions.

21
Creatine Kinase - MB Fraction: Creatine kinase can be further subdivided into three isoenzymes: MM, MB, and BB. The MM fraction is present in both cardiac andskeletal muscle, but the MB fraction is much more specific for cardiac muscle: about 15 to 40% of CK in cardiac muscle i sMB, while less than 2% in skeletal muscle is MB. The BB fraction(found in brain, bowel, and bladder) is not routinely measured.
Thus, CK-MB is a very good marker for acute myocardialinjury , because of its excellent specificity, and it rises in serum within 2 to 8 hours of onset of acute myocardial infarction. Serial measurements every 2 to 4 hours for a period of 9 to 12 hours afterthe patient is first seen will provide a pattern to determine whetherthe CK-MB is rising, indicative of myocardial injury. The CK-MB isalso useful for diagnosis of reinfarction or extensive of an MI because it begins to fall after a day, dissipating in 1 to 3 days, sosubsequent elevations are indicative of another event.A "cardiac index" can provide a useful indicator for early MI. This iscalculated as a ratio of total CK to CK-MB, and is a sensitiveindicator of myocardial injury when the CK-MB is elevated.
CK-MB Isoforms:
The CK-MB fraction exists in two isoforms called 1 and2 identified by electrophoretic methodology. The ratio ofisoform 2 to 1 can provide information about myocardialinjury.
An isoform ratio of 1.5 or greater is an excellentindicator for early acute myocardial infarction. CK-MB isoform 2 demonstrates elevation even before CK-MB by laboratory testing.
However, the disadvantage of this method is that it isskilled labor intensive because electrophoresis isrequired, and large numbers of samples cannot be run simultaneously nor continuously. False positive resultswith congestive heart failure and other conditions canoccur.

22
Troponins:
Troponin I and T are structural components of cardiac musc le. They are released into the bloodstream with myocardial inju ry. They are highly specific for myocardial injury--more so th anCK-MB--and help to exclude elevations of CK with skeleta lmuscle trauma. Troponins will begin to increase followi ng MI within 3 to 12 hours, about the same time frame as CK-MB . However, the rate of rise for early infarction may not be as dramatic as for CK-MB.Troponins will remain elevated longer than CK--up to 5 to 9 days for troponin I and up to 2 weeks for troponin T. Thi smakes troponins a superior marker for diagnosing myoca rdialinfarction in the recent past--better than lactatedehydrogenase (LDH). However, this continued elevation hasthe disadvantage of making it more difficult to diagnosereinfarction or extension of infarction in a patient who ha salready suffered an initial MI. Troponin T lacks somespecificity because elevations can appear with skeletalmyopathies and with renal failure.
Myoglobin:
Myoglobin is a protein found in skeletal andcardiac muscle which binds oxygen. It is a verysensitive indicator of muscle injury. The rise inmyoglobin can help to determine the size of aninfarction. A negative myoglobin can help to ruleout myocardial infarction. It is elevated even beforeCK-MB. However, it is not specific for cardiacmuscle, and can be elevated with any form of injuryto skeletal muscle.

23
Lactate dehydrogenase:
The LDH has been supplanted by other tests. Itbegins to rise in 12 to 24 hours following MI, andpeaks in 2 to 3 days, gradually dissipating in 5 to 14 days. Measurement of LDH isoenzymes isnecessary for greater specificity for cardiac injury. There are 5 isoenzymes (1 through 5). Ordinarily, isoenzyme 2 is greater than 1, but with myocardialinjury, this pattern is "flipped" and 1 is higher than2. LDH-5 from liver may be increased withcentrilobular necrosis from passive congestionwith congestive heart failure following ischemicmyocardial injury.
Serum enzyme elevetionin acute myocardial infarction
(AST=Aspartate transaminase, CK=creatine kinase, CK-M B=isoenzymefor cardiac muscle, LDH=lactate dehydrogenase)
24
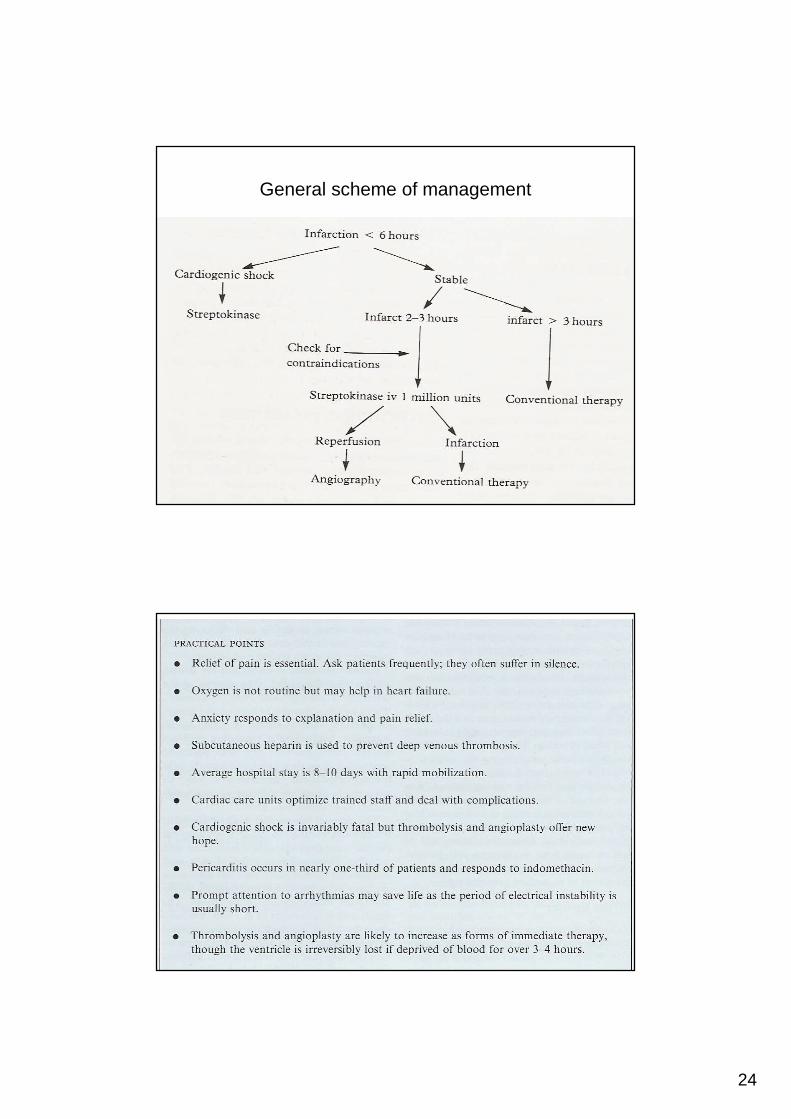
General scheme of management