influenza, hib and rotavirus chapters 16,9 and 20
Post on 22-Dec-2015
219 views
TRANSCRIPT
Influenza, Hib and Rotavirus
Chapters 16,9 and 20

Influenza
• Highly infectious viral illness
• First pandemic in 1580
• At least 4 pandemics in 19th century
• Estimated 21 million deaths worldwide in pandemic of 1918-1919
• Virus first isolated in 1933
Influenza Virus
• Single-stranded RNA virus
• Orthomyxoviridae family
• 3 types: A, B, C
• Subtypes of type A determined by hemagglutinin and neuraminidase
Influenza Virus Strains
• Type A - moderate to severe illness- all age groups- humans and other animals
• Type B - milder disease- primarily affects children- humans only
• Type C - rarely reported in humans- no epidemics
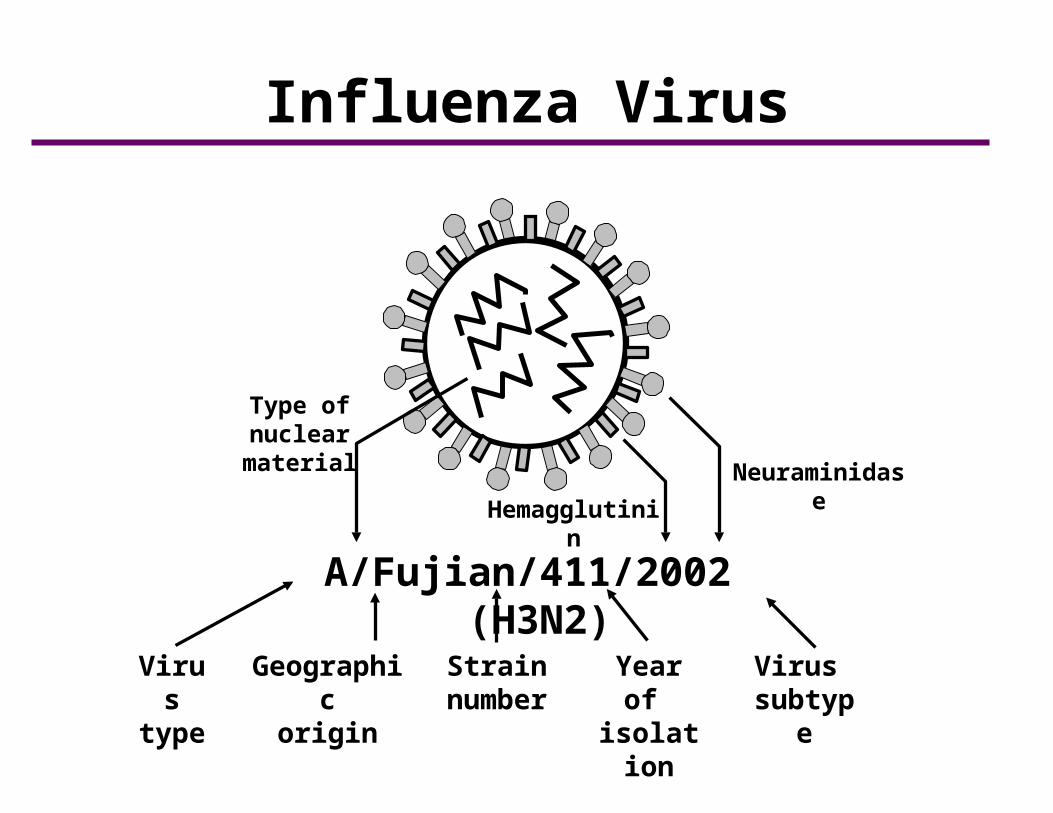
Influenza Virus
A/Fujian/411/2002 (H3N2)
Neuraminidase
Hemagglutinin
Type of nuclearmaterial
Virustype
Geographicorigin
Strainnumber
Year of isolation
Virus subtype

Influenza Antigenic Changes
• Hemagglutinin and neuraminidase antigens change with time
• Changes occur as a result of point mutations in the virus gene, or due to exchange of a gene segment with another subtype of influenza virus
• Impact of antigenic changes depend on extent of change (more change usually means larger impact)
Influenza Antigenic Changes
• Antigenic Shift
–major change, new subtype
–caused by exchange of gene segments
–may result in pandemic
• Example of antigenic shift
–H2N2 virus circulated in 1957-1967
–H3N2 virus appeared in 1968 and completely replaced H2N2 virus

Influenza Antigenic Changes
• Antigenic Drift–minor change, same subtype–caused by point mutations in gene–may result in epidemic
• Example of antigenic drift–in 2002-2003, A/Panama/2007/99
(H3N2) virus was dominant–A/Fujian/411/2002 (H3N2) appeared
in late 2003 and caused widespread illness in 2003-2004
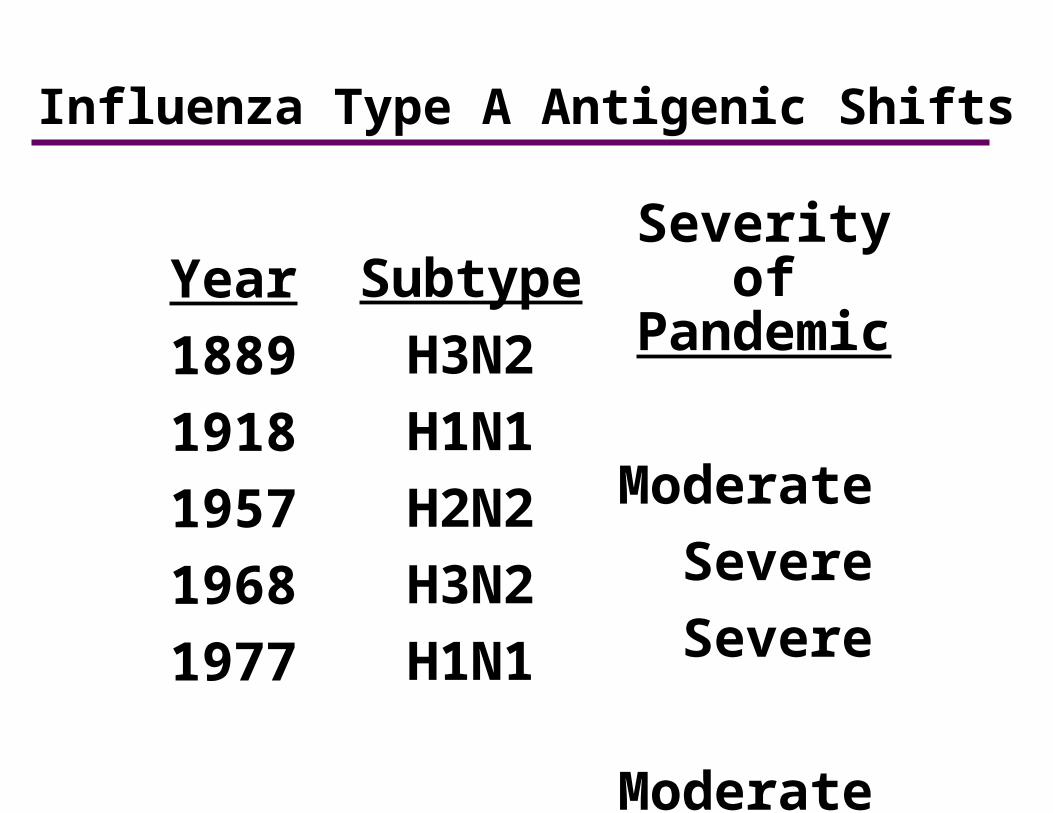
Influenza Type A Antigenic Shifts
Year
1889
1918
1957
1968
1977
Subtype
H3N2
H1N1
H2N2
H3N2
H1N1
Severity ofPandemic
Moderate
Severe
Severe
Moderate
Mild

Impact of Pandemic Influenza Today
• 200 million people could be affected
• Up to 40 million require outpatient visits
• Up to 700,000 hospitalized
• 89,000 - 200,000 deaths
Influenza Pathogenesis
• Respiratory transmission of virus
• Replication in respiratory epithelium with subsequent destruction of cells
• Viremia rarely documented
• Viral shedding in respiratory secretions for 5-10 days
Influenza Clinical Features
• Incubation period 2 days (range 1-4 days)
• Abrupt onset of fever, myalgia, sore throat, nonproductive cough, headache
• Severity of illness depends on prior experience with related variants

Influenza Complications
• Pneumonia
–secondary bacterial
–primary influenza viral
• Reye syndrome
• Myocarditis
• Death 0.5-1 per 1,000 cases
• Highest rates of complications and hospitalization among young children and person 65 years and older• Average of more than 200,000
influenza-related excess hospitalizations • 57% of hospitalizations among
persons younger than 65 years of age• Greater number of hospitalizations
during type A (H3N2) epidemics
Impact of Influenza-United States, 1990-1999

Influenza Diagnosis
• Clinical and epidemiological characteristics
• Isolation of influenza virus from clinical specimen (e.g., nasopharynx, throat, sputum)
• Significant rise in influenza IgG by serologic assay
• Direct antigen testing for type A virus

Influenza Epidemiology
• Reservoir Human, animals (type Aonly)
• Transmission RespiratoryProbably airborne
• Temporal pattern Peak December – March
in temperate climateMay occur earlier or
later
• Communicability 1 day before to 5 days after onset (adults)

Month of Peak Influenza Activity United States, 1976-2006
0
5
10
15
20
25
30
35
40
45
50
Dec Jan Feb Mar Apr May
Pe
rce
nt
13%
19%
45%
13%
3% 3%
MMWR 2007;55(RR-6):5
Influenza Vaccines
• Inactivated subunit (TIV)–intramuscular–trivalent–split virus and subunit types–duration of immunity 1 year or less
• Live attenuated vaccine (LAIV)–intranasal–trivalent–duration of immunity at least 1 year

Composition of the 2008-2009 Influenza Vaccine*
• A/Brisbane/59/2007 (H1N1)
• A/Brisbane/10/2007 (H3N2)
• B/Florida/4/2006
*manufacturers may use strains that are antigenically identical to the selected strains
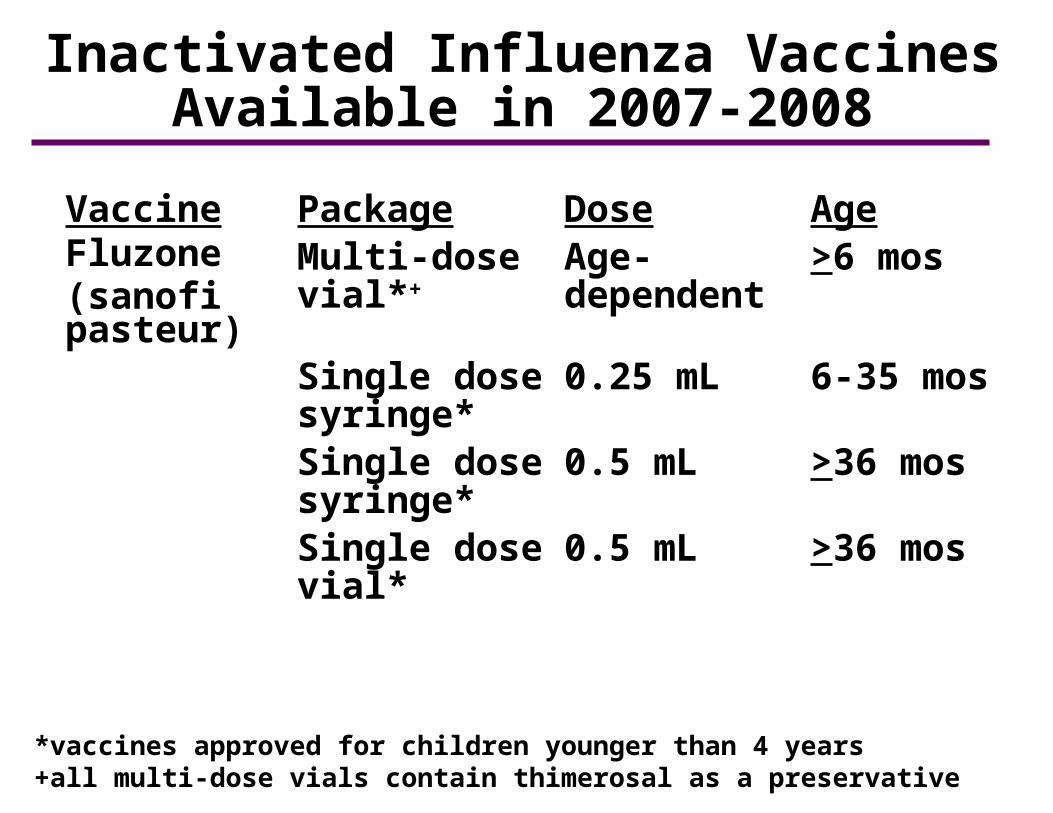
Inactivated Influenza Vaccines Available in 2007-2008
Vaccine Package Dose AgeFluzone(sanofi pasteur)
Multi-dose vial*+
Age-dependent
>6 mos
Single dose syringe*
0.25 mL 6-35 mos
Single dose syringe*
0.5 mL >36 mos
Single dose vial*
0.5 mL >36 mos
*vaccines approved for children younger than 4 years+all multi-dose vials contain thimerosal as a preservative
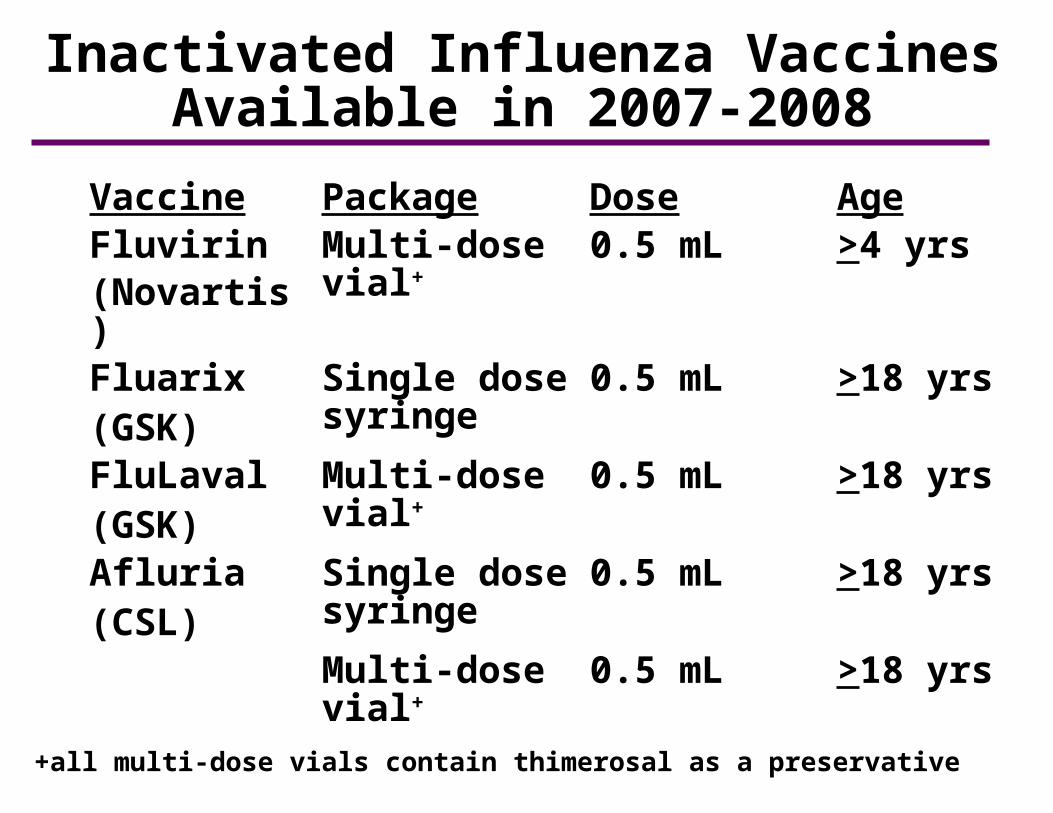
Inactivated Influenza Vaccines Available in 2007-2008
Vaccine Package Dose AgeFluvirin(Novartis)
Multi-dose vial+
0.5 mL >4 yrs
Fluarix(GSK)
Single dose syringe
0.5 mL >18 yrs
FluLaval(GSK)
Multi-dose vial+
0.5 mL >18 yrs
Afluria(CSL)
Single dose syringe
0.5 mL >18 yrs
Multi-dose vial+
0.5 mL >18 yrs
+all multi-dose vials contain thimerosal as a preservative
Transmission of LAIV Virus
• LAIV replicates in the nasopharyngeal mucosa
• Mean shedding of virus 7 days – longer in children
• One instance of transmission of vaccine virus documented in a child care setting
• Transmitted virus retained attenuated, cold-adapted, temperature-sensitive characteristics
• No transmission of LAIV reported in the U.S.
Inactivated Influenza Vaccine Efficacy
• 70%-90% effective among healthy persons younger than 65 years of age
• 30%-40% effective among frail elderly persons
• 50%-60% effective in preventing hospitalization
• 80% effective in preventing death
LAIV Efficacy in Healthy Adults
• 20% fewer severe febrile illness episodes• 24% fewer febrile upper respiratory
illness episodes• 27% fewer lost work days due to
febrile upper respiratory illness• 18%-37% fewer days of healthcare
provider visits due to febrile illness• 41%-45% fewer days of antibiotic use
Inactivated Influenza Vaccine Schedule
AgeGroup
6-35 mos
3-8 yrs
>9 yrs
Dose0.25 mL
0.50 mL
0.50 mL
No.Doses1* or 2
1* or 2
1
*Only one dose is needed if the child received 2 doses of influenza vaccine during the previous influenza season
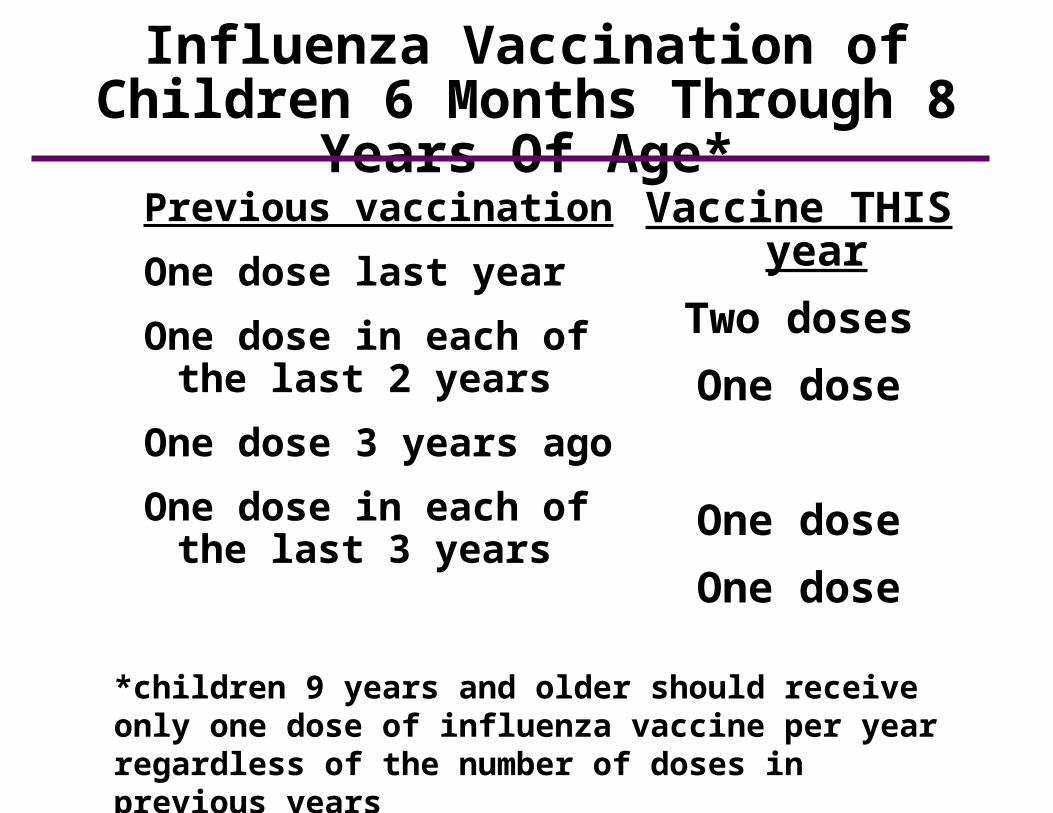
Influenza Vaccination of Children 6 Months Through 8 Years Of Age*
Previous vaccination
One dose last year
One dose in each of the last 2 years
One dose 3 years ago
One dose in each of the last 3 years
Vaccine THIS year
Two doses
One dose
One dose
One dose
*children 9 years and older should receive only one dose of influenza vaccine per year regardless of the number of doses in previous years

Inactivated Influenza Vaccine Recommendations
• All persons 50 years of age or older
• Children 6-59 months of age
• Residents of long-term care facilities
• Pregnant women
• Persons 6 months to 18 years receiving chronic aspirin therapy
• Persons 6 months of age or older with chronic illness
Inactivated Influenza Vaccine Recommendations
• Persons with the following chronic illnesses should be considered for inactivated influenza vaccine:–pulmonary (e.g., asthma, COPD)–cardiovascular (e.g., CHF)–metabolic (e.g., diabetes)–renal dysfunction–hemoglobinopathy–immunosuppression, including HIV infection–any condition that can compromise
respiratory function or the handling of respiratory secretions
Pregnancy and Inactivated Influenza Vaccine
• Risk of hospitalization 4 times higher than nonpregnant women
• Risk of complications comparable to nonpregnant women with high-risk medical conditions
• Vaccination (with TIV) recommended if pregnant during influenza season
• Vaccination can occur during any trimester
HIV Infection and Inactivated Influenza Vaccine
• Persons with HIV at increased risk of complications of influenza
• TIV induces protective antibody titers in many HIV infected persons
• TIV will benefit many HIV-infected persons
• Do not administer LAIV to persons with HIV infection
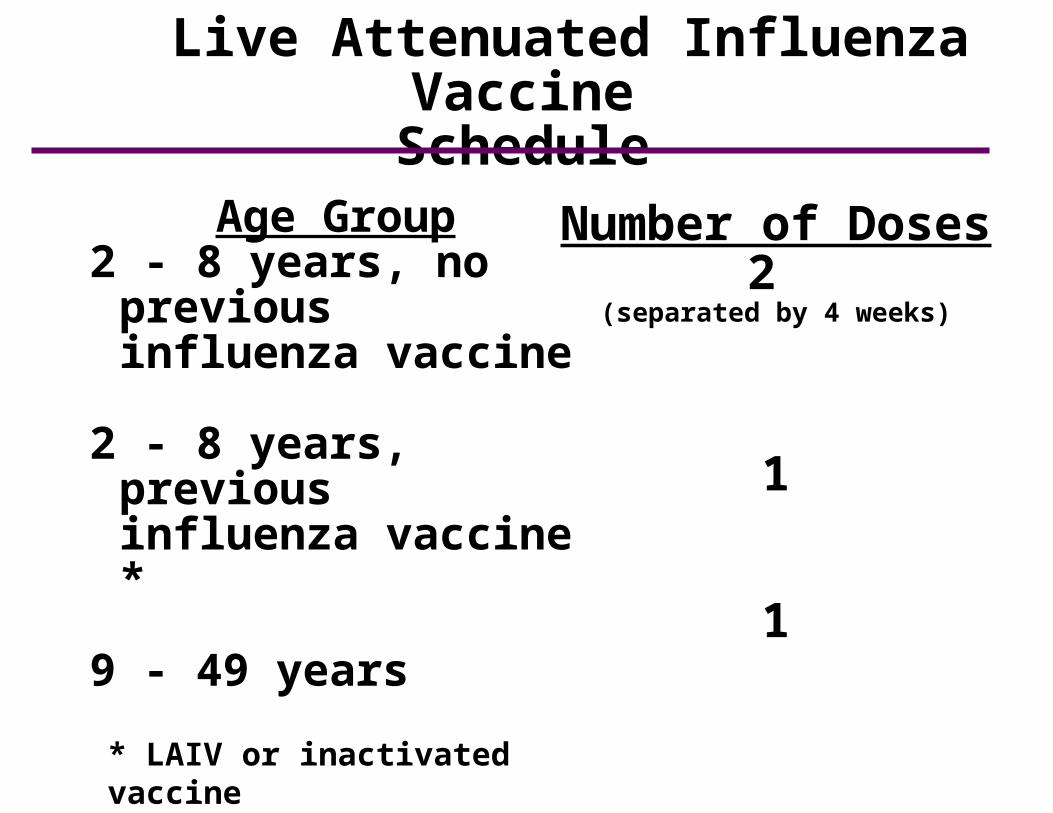
Age Group2 - 8 years, no
previous influenza vaccine
2 - 8 years, previous influenza vaccine *
9 - 49 years
Number of Doses2
(separated by 4 weeks)
1
1
* LAIV or inactivated vaccine
Live Attenuated Influenza VaccineSchedule

Live Attenuated Influenza VaccineAdverse Reactions
• Children–no significant increase in URI symptoms, fever,
or other systemic symptoms–significantly increased risk of asthma or
reactive airways disease in children 12-59 months of age
• Adults–significantly increased rate of cough, runny
nose, nasal congestion, sore throat, and chills reported among vaccine recipients–no increase in the occurrence of fever
• No serious adverse reactions identified
Inactivated Influenza VaccineContraindications and Precautions
• Severe allergic reaction to a vaccine component (e.g., egg) or following a prior dose of vaccine
• Moderate or severe acute illness
• History of Guillian Barre’ syndrome within 6 weeks following a previous dose of TIV (precaution)

Live Attenuated Influenza VaccineContraindications and Precautions
• Children younger than 2 years of age*
• Persons 50 years of age or older*
• Persons with chronic medical conditions*
• Children and adolescents receiving long-term aspirin therapy*
*These persons should receive inactivated influenza vaccine

Live Attenuated Influenza VaccineContraindications and Precautions
• Immunosuppression from any cause*
• Pregnant women*
• Severe (anaphylactic) allergy to egg or other vaccine components
• History of Guillian-Barré syndrome
• Children younger than 5 years with recurrent wheezing*
• Moderate or severe acute illness
*These persons should receive inactivated influenza vaccine

Influenza Antiviral Agents*
• Amantadine and rimantadine–Not recommended because of
documented resistance in U.S. influenza isolates
• Zanamivir and oseltamivir–neuraminidase inhibitors–effective against influenza A and B–should be used if an influenza
antiviral drug is indicated for chemoprophylaxis or treatment
*see influenza ACIP statement or CDC influenza website for details

Haemophilus influenzae type B and Hib VaccineChapter 9
Haemophilus influenzae type b
• Severe bacterial infection, particularly among infants
• During late 19th century believed to cause influenza
• Immunology and microbiology clarified in 1930s
Haemophilus influenzae
• Aerobic gram-negative bacteria
• Polysaccharide capsule
• Six different serotypes (a-f) of polysaccharide capsule
• 95% of invasive disease caused by type b
Haemophilus influenzae type bPathogenesis
• Organism colonizes nasopharynx
• In some persons organism invades bloodstream and cause infection at distant site
• Antecedent upper respiratory tract infection may be a contributing factor

Cellulitis6%
Arthritis8% Bacteremia
2%
Meningitis50%
Epiglottitis17%
Pneumonia15%
Osteomyelitis2%
Haemophilus influenzae type bClinical Features*
*prevaccination era

Haemophilus influenzae type b Medical Management
• Hospitalization required
• Treatment with an effective 3rd generation cephalosporin, or chloramphenicol plus ampicillin
• Ampicillin-resistant strains now common throughout the United States
Haemophilus influenzae type b Epidemiology
• Reservoir Human Asymptomatic carriers
• Transmission Respiratory droplets
• Temporal pattern Peaks in Sept-Dec and March-May
• Communicability Generally limited buthigher in somecircumstances
0
5
10
15
20
25
1990 1992 1994 1996 1998 2000 2002 2004
Inc
ide
nc
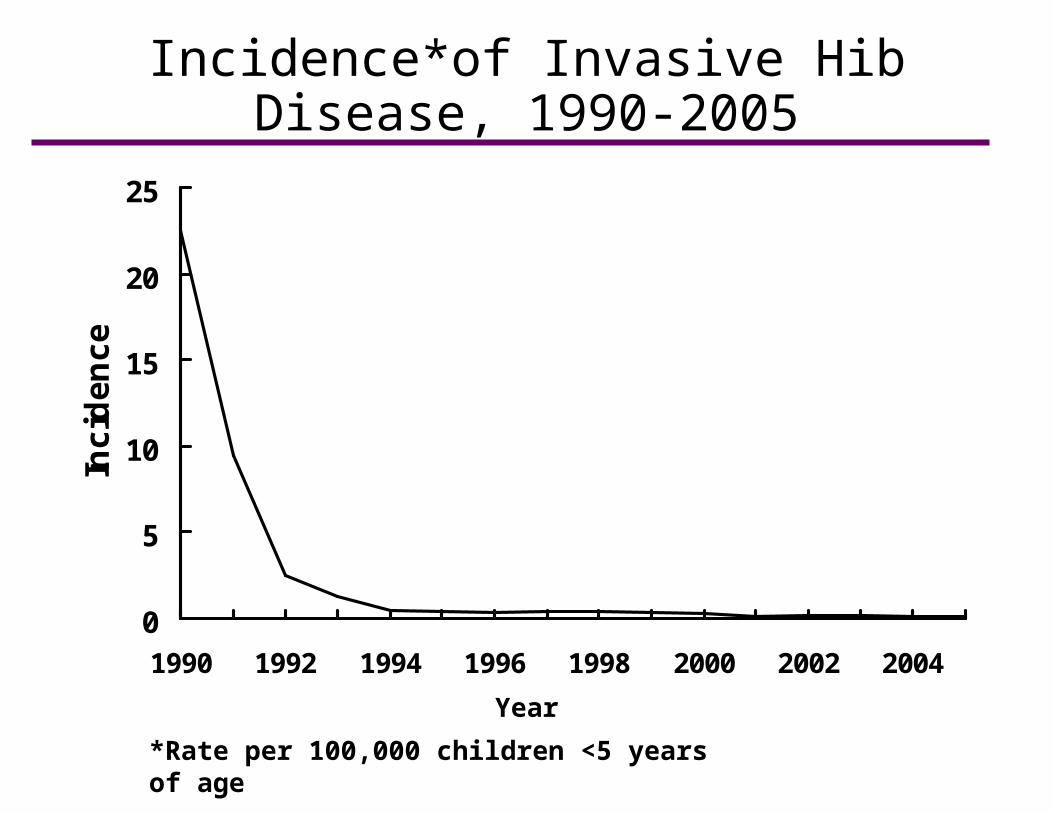
eIncidence*of Invasive Hib Disease,
1990-2005
*Rate per 100,000 children <5 years of age
Year
Haemophilus influenzae type b—United States, 2002-2006
• Incidence has fallen more than 99% since prevaccine era
• 123 confirmed Hib cases reported (average of 25 cases per year)
• Most recent cases in unvaccinated or incompletely vaccinated children
Haemophilus influenzae type bRisk Factors for Invasive Disease
• Exposure factors–household crowding– large household size–child care attendance– low socioeconomic
status– low parental education–school-aged siblings
• Host factors–race/ethnicity–chronic disease
Haemophilus influenzae type bPolysaccharide Vaccine
• Available 1985-1988• Not effective in children
younger than 18 months of age• Effectiveness in older children variable• Age-related immune response• Not consistently immunogenic in
children 2 years of age and younger• No booster response• Antibody with less functional activity
Polysaccharide Conjugate Vaccines
• Stimulates T-dependent immunity
• Enhanced antibody production, especially in young children
• Repeat doses elicit booster response
Haemophilus influenzae type b Conjugate Vaccines
• Two conjugate vaccines licensed for use in infants as young as 6 weeks of age
• Use different carrier proteins
• 3 doses of any combination confers protection
PRP-T ActHIB, TriHIBit
PRP-OMP PedvaxHIB, Comvax
Conjugate Hib Vaccines*
*HbOC (HibTiter) no longer available in the United States
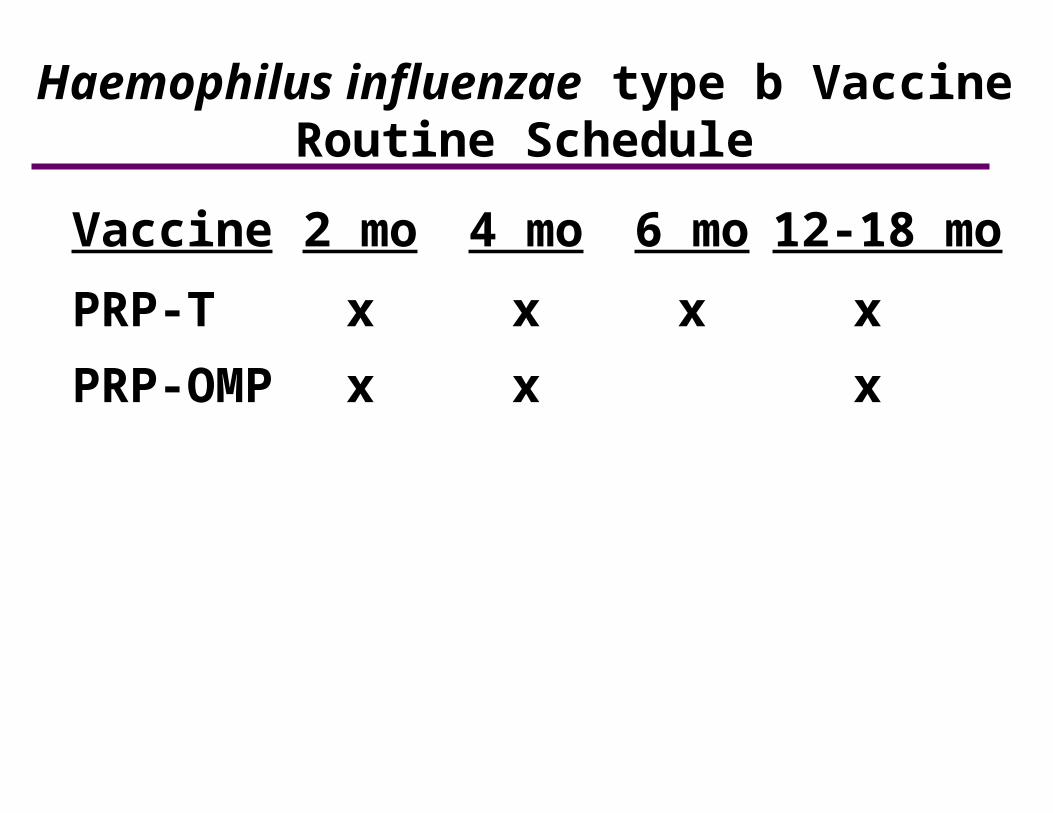
Vaccine 2 mo 4 mo 6 mo 12-18 mo
PRP-T x x x x
PRP-OMP x x x
Haemophilus influenzae type b VaccineRoutine Schedule

Haemophilus influenzae type b Vaccine Interchangeability
• Both conjugate Hib vaccines (except TriHIBit) are interchangeable for primary series and booster dose
• 3 dose primary series if more than one brand of vaccine used
Haemophilus influenzae type b Vaccine Delayed Vaccination Schedule
• Unvaccinated children 7 months of age or older may not need entire 3 or 4 dose series
• Number of doses child requires depends on current age
• All children 15-59 months of age need at least 1 dose

Lapsed Immunization
• Children who have fallen behind schedule with Hib vaccine may not need all the remaining doses of a 3 or 4 dose series
• The number of doses needed to complete the series should be determined using the catch-up schedule*, published annually with the childhood schedule
*available at ww.cdc.gov/vaccines/recs/schedules/child-schedule.htm

Haemophilus influenzae type b VaccineVaccination Following Invasive Disease
• Children younger than 24 months may not develop protective antibody after invasive disease
• Vaccinate during convalescence
• Complete series for age
Haemophilus influenzae type b VaccineUse in Older Children and Adults
• Generally not recommended for persons older than 59 months of age• Consider for high-risk persons:
asplenia, immunodeficiency, HIV infection–One pediatric dose of any conjugate
vaccine• 3 doses recommended for all persons
who have received a hematopoietic stem cell transplant

Combination Vaccines Containing Hib
• DTaP—Hib
–TriHIBit
• Hepatitis B—Hib
–Comvax
Hib Vaccination Recommendations During the Current Shortage
• The booster dose of Hib vaccine usually administered at 12-15 months of age should be deferred except for children at increased risk of Hib disease
–asplenia
–sickle cell disease
–immunodeficiency (including HIV infection and cancer)
–American Indian/Alaska Native children
MMWR 2007; 56(50);1318-1320
Rotavirus and Rotavirus Vaccine
Chapter 20
Rotavirus
• First identified as cause of diarrhea in 1973
• Most common cause of severe diarrhea in infants and children
• Nearly universal infection by 5 years of age
• Responsible for up to 500,000 diarrheal deaths each year worldwide

• Reovirus (RNA)• VP7 and VP4 antigens define virus
serotype.• 5 predominant strains in U.S. (G1-
G4, G9) and account for 90% of isolates• G1 strain accounts for 73% of
infections• Very stable and may remain viable
for weeks or months if not disinfected
Rotavirus
Rotavirus Pathogenesis
• Entry through mouth
• Replication in epithelium of small intestine
• Replication outside intestine and viremia uncommon
• Infection leads to isotonic diarrhea

Rotavirus Immunity
• Antibody against VP7 and VP4 probably important for protection
• First infection usually does not lead to permanent immunity
• Reinfection can occur at any age
• Subsequent infections generally less severe

Rotavirus Clinical Features
• Incubation period 1-3 days
• Clinical manifestations depend on whether it is the first infection or reinfection
• First infection after age 3 months generally most severe
• May be asymptomatic or result in severe dehydrating diarrhea with fever and vomiting
• Gastrointestinal symptoms generally resolve in 3 to 7 days
Rotavirus Complications
• Severe diarrhea
• Dehydration
• Electrolyte imbalance
• Metabolic acidosis
• Immunodeficient children may have more severe or persistent disease

Rotavirus Disease Burden in the United States
• Estimated 2.7 million cases per year
• 95% of children infected by 5 years of age
• The most severe disease occurs among children 3-24 months of age
• Highest incidence among children 3 to 35 months of age
• Responsible for 5%-10% of all gastroenteritis episodes among children younger than 5 years of age
Rotavirus Epidemiology
• Reservoir Human-GI tract
• Transmission Fecal-oral, fomites
• Temporal Fall and winter pattern (temperate areas)
• Communicability 2 days before to 10
days after onset
Risk Groups for Rotavirus Diarrhea
• Groups with increased exposure to virus
–Children in child care centers
–Children in hospital wards (nosocomial rotavirus)
–Caretakers, parents of these children
–Children, adults with immuno- deficiency related diseases (e.g. SCID, HIV, bone marrow transplant)
Rotavirus Vaccine (RotaTeq®)
• Approved by FDA in February 2006
• Contains five reassortant rotaviruses developed from human and bovine parent rotavirus strains
• Vaccine viruses suspended in a solution of buffer (sodium citrate and phosphate) and stabilizer
• Contains no preservatives or thimerosal
Rotarix® Rotavirus Vaccine
• Approved by FDA in April 2008
• Contains one strain of live attenuated human rotavirus (G1P[8])
• Two oral doses at 2 and 4 months of age (minimum interval 4 weeks)
• Minimum age 6 weeks
• Maximum age 24 weeks
• ACIP recommendations for use are pending
RotaTeq Vaccine Efficacy
• Phase III trials included more than 70,000 infants in 11 countries • Efficacy–All rotavirus disease - 74%–Severe rotavirus disease - 98%–Physician visits for diarrhea-86%
reduction–Rotavirus-related hospitalization-96%
reduction• Efficacy of fewer than 3 doses is not
known
N Eng J Med 2006;354:23-33

Rotavirus VaccineRecommendations
• Routine immunization of all infants without contraindications• Administered at 2, 4, and 6 months of age*• Minimum age of first doses is 6 weeks• First dose should be administered between
6 and 12 weeks of age (until age 13 weeks)• Do not initiate series after 12 weeks of age
*2 doses at 2 and 4 months for Rotarix*2 doses at 2 and 4 months for RotarixMMWRMMWR 2006;55:(RR-12):1-13. 2006;55:(RR-12):1-13.
• Minimum interval between doses is 4 weeks
• Maximum age for ANY dose is 32 weeks*
• Do not administer on or after age 32 weeks*, even if fewer than three doses have been administered
Rotavirus VaccineRecommendations
*24 weeks for Rotarix*24 weeks for RotarixMMWRMMWR 2006;55:(RR-12):1-13. 2006;55:(RR-12):1-13.
• Administer simultaneously with all other indicated vaccines• Breastfeeding infants should be
vaccinated on usual schedule• Vaccinate infants who have
recovered from documented rotavirus infection• Do not repeat dose if infant spits out
or regurgitates vaccine- administer remaining doses on schedule
Rotavirus VaccineRecommendations
MMWRMMWR 2006;55:(RR-12):1-13. 2006;55:(RR-12):1-13.
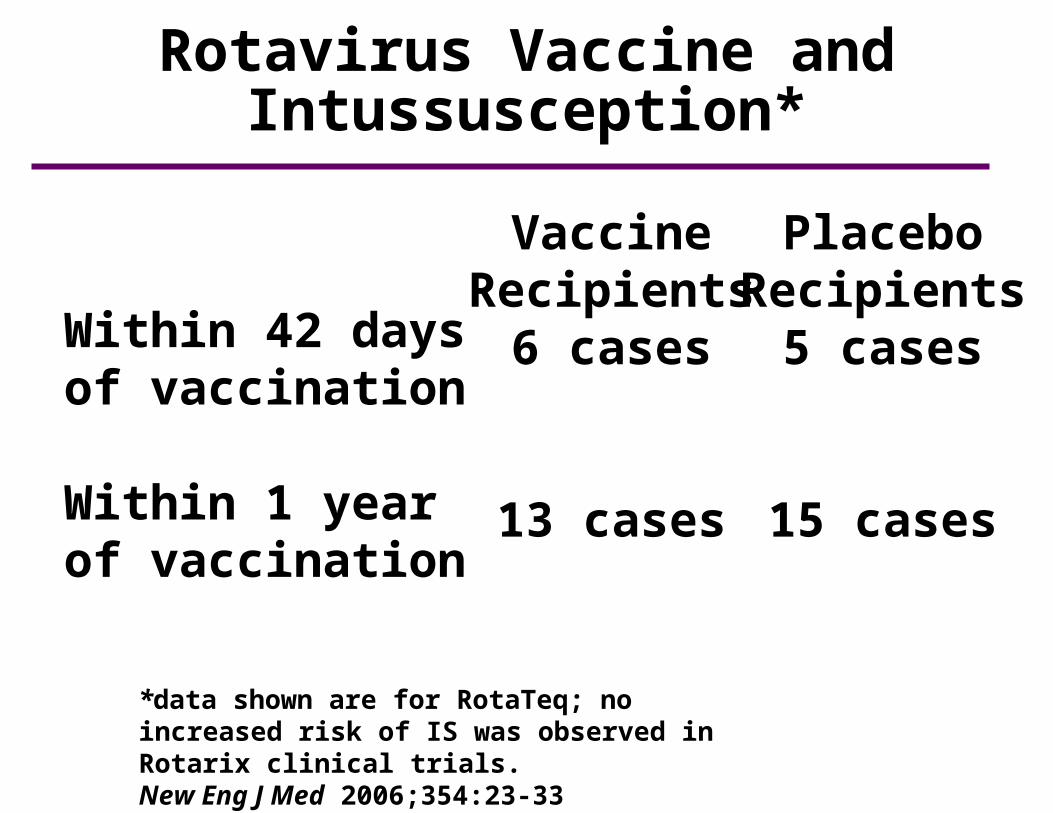
Rotavirus Vaccine and Intussusception*
Within 42 daysof vaccination
Within 1 yearof vaccination
VaccineRecipients
6 cases
13 cases
PlaceboRecipients
5 cases
15 cases
*data shown are for RotaTeq; no increased risk of IS was observed in Rotarix clinical trials.New Eng J Med 2006;354:23-33

Rotavirus VaccineAdverse Reactions
• Vomiting 15%
• Diarrhea 24%
• Nasopharyngitis 7%
• Fever 43%
• No serious adverse reactions reported
*data shown are for RotaTeq*data shown are for RotaTeqMMWRMMWR 2006;55:(RR-12):1-13. 2006;55:(RR-12):1-13.
Rotavirus VaccineContraindications
• Severe allergic reaction to a vaccine component or following a prior dose of vaccine
Rotavirus VaccinePrecautions*
• Altered immunocompetence
• Recent receipt of blood product
• Acute, moderate to severe gastroenteritis or other acute illness
• Pre-existing chronic GI disease
• Infants with history of intussusception
*the decision to vaccinate if a precaution is present should be made on a case-by-case risk and benefit basis

Rotavirus Vaccine and Preterm Infants
• Few data available
• ACIP supports the vaccination of a preterm infant if:
–the infant is at least 6 weeks of age; and
–is being or has been discharged from the hospital; and
–is clinically stable
MMWRMMWR 2006;55:(RR-12):1-13. 2006;55:(RR-12):1-13.

Immunosuppressed Household Contacts of Rotavirus Vaccine Recipients
• Protection of the immunocompromised household member afforded by vaccination of young children in the household outweighs the small risk for transmitting vaccine virus to the immunocompromised household member
• Household should employ measures such as good handwashing after contact with the feces of the vaccinated infant