influenza in clinical care & vaccine efficacy/effectiveness · influenza in clinical care &...
TRANSCRIPT
Influenza in Clinical Care & Vaccine Efficacy/Effectiveness
University of Minnesota Medical CenterDepartment of Medicine Grand Rounds
25 October 2012
Jose L. (“Toti”) Sanchez, MD, MPHMichael J. Cooper, PhD
Alice Y. Tsai, MPH
The Armed Forces Health Surveillance CenterDivision of GEIS Operations
Silver Spring, [email protected]
The views expressed in this presentation are those of the author and do not necessarily reflect the official policy or position of the US
Army, Department of Defense, nor of the US Government.
I have financial relationships to discuss and I will not discuss off-label use and/or investigational use of any commercial products.
Mention of any commercial product in this paper does not imply DoDendorsement or recommendation for or against the use of any such
product. No infringement on the rights of the holders of the registered trademarks is intended.
Disclaimer & Disclosures
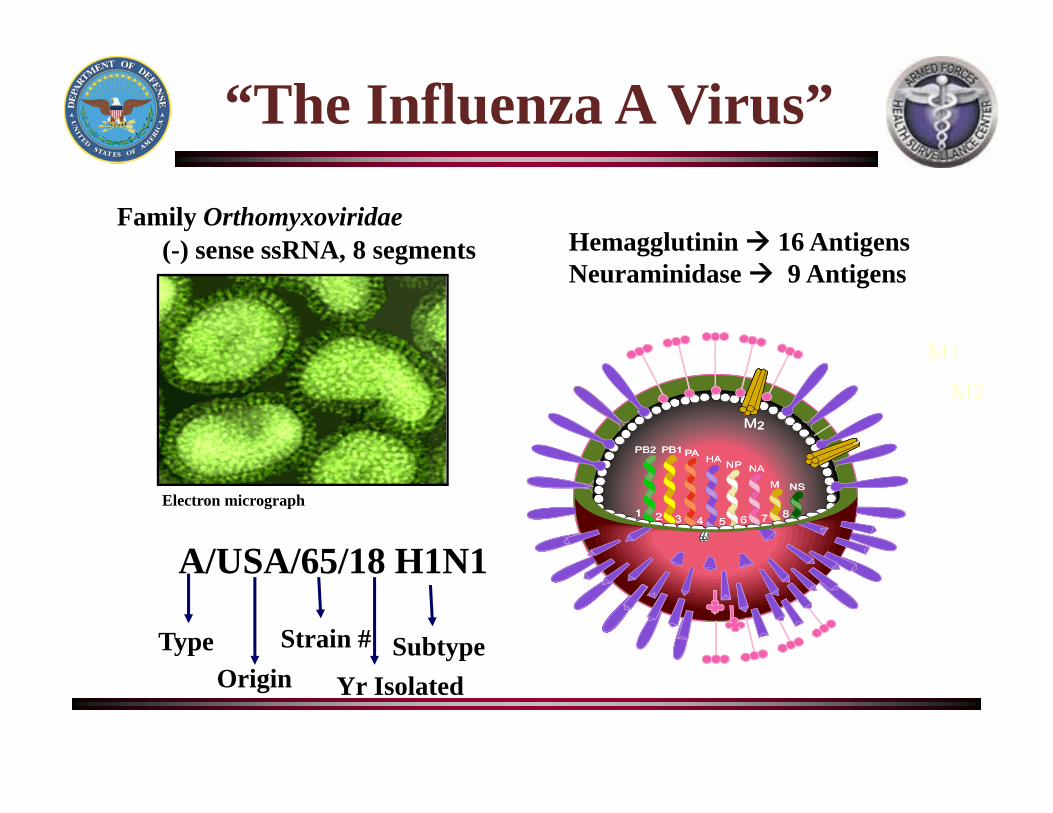
Family Orthomyxoviridae(-) sense ssRNA, 8 segments
Origin
A/USA/65/18 H1N1
Type Strain #
Yr IsolatedSubtype
Electron micrograph
Schematic
M1
M2
“The Influenza A Virus”
Hemagglutinin 16 AntigensNeuraminidase 9 Antigens
Flu in Civilian Populations
• A and B cause epidemics, pandemics only caused by A– 10-20% of US population may be affected
• ~ 36,000 deaths/year (range, 3,000 – 49,000)
• ~ 200,000 - 250,000 hospitalizations/year– In 2009 pandemic ~ 270,000 hospitalizations
• C causes mild respiratory illnesses
• C not thought to cause epidemics
Sources: CDC, Key facts about influenza (Flu) & Flu vaccine, 23 Dec 11, http://www.cdc.gov/flu/keyfacts.htmThompson WW, et al, Estimates of US influenza-associated deaths made using four different methods, Influenza Other Respi Viruses 2009; 3:37–49 Thompson WW, et al, Influenza-associated hospitalizations in the United States, JAMA 2004; 292:1333–40
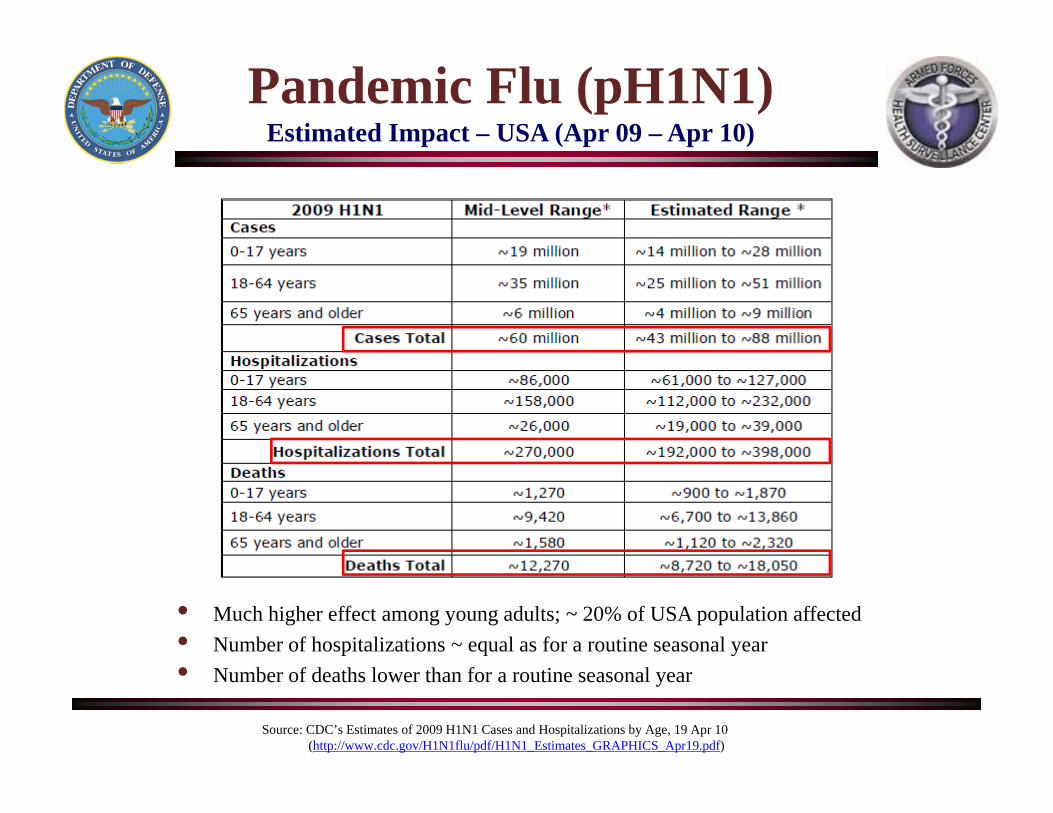
Pandemic Flu (pH1N1)Estimated Impact – USA (Apr 09 – Apr 10)
Source: CDC’s Estimates of 2009 H1N1 Cases and Hospitalizations by Age, 19 Apr 10(http://www.cdc.gov/H1N1flu/pdf/H1N1_Estimates_GRAPHICS_Apr19.pdf)
• Much higher effect among young adults; ~ 20% of USA population affected• Number of hospitalizations ~ equal as for a routine seasonal year• Number of deaths lower than for a routine seasonal year
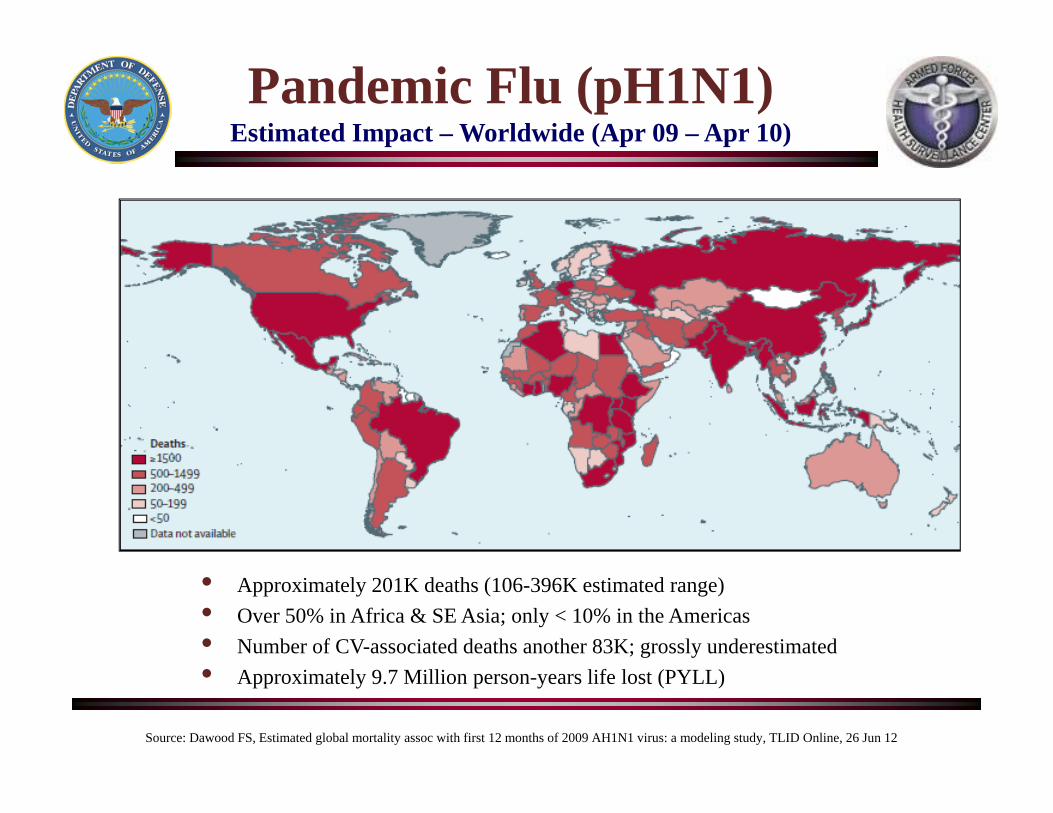
Pandemic Flu (pH1N1)Estimated Impact – Worldwide (Apr 09 – Apr 10)
Source: Dawood FS, Estimated global mortality assoc with first 12 months of 2009 AH1N1 virus: a modeling study, TLID Online, 26 Jun 12
• Approximately 201K deaths (106-396K estimated range)• Over 50% in Africa & SE Asia; only < 10% in the Americas• Number of CV-associated deaths another 83K; grossly underestimated• Approximately 9.7 Million person-years life lost (PYLL)
Pandemic Flu (pH1N1)Mortality Worldwide (Apr 09 – Apr 10)
Sources: Dawood FS, Estimated global mortality assoc with first 12 months of 2009 AH1N1 virus: a modeling study, TLID Online, 26 Jun 12Mounts A & Simonsen L, WHO estimation global mortality in 2009 pandemic, ISIRV conference, Munich, GE, 7 Sep 12
• CDC regional (sAR x CFR) modeling estimates ~ 201K deaths (106-396K range)• European (GLaMOR) modeling estimates ~ 220K deaths (120-390K range)
• Using Worldwide Mortality Rate ~ 10-15 deaths/Million (50% underestimate)• Total Deaths (for 7 Billion population) ~ 160-210K deaths
• Using Worldwide Case Fatality Rate (CFR) ~ 0.01-0.02%• Assuming 25% sAR (for 7 Billion population) ~ 175-350K deaths
• Shift in mortality towards younger age groups (18-64yo)• Lower CFR than for seasonal flu (0.02-0.04%)
Pretty Similar Estimates – “Mild Seasonal Flu”
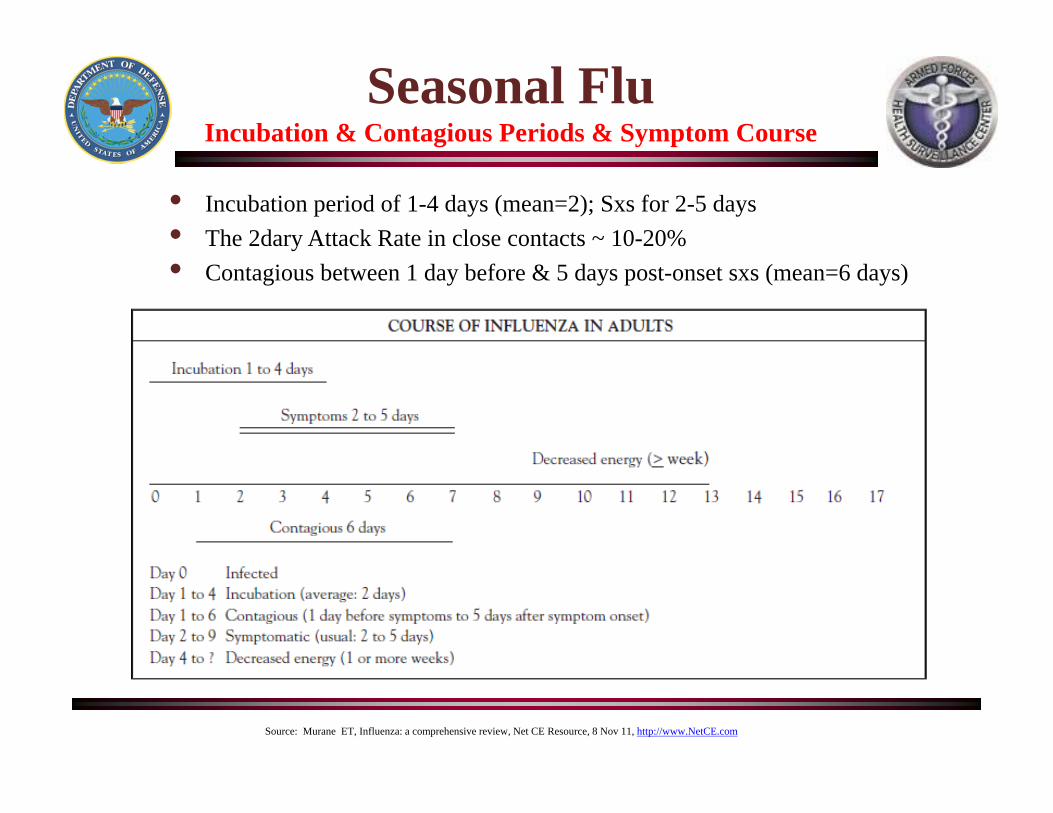
Seasonal FluIncubation & Contagious Periods & Symptom Course
• Incubation period of 1-4 days (mean=2); Sxs for 2-5 days• The 2dary Attack Rate in close contacts ~ 10-20%• Contagious between 1 day before & 5 days post-onset sxs (mean=6 days)
Source: Murane ET, Influenza: a comprehensive review, Net CE Resource, 8 Nov 11, http://www.NetCE.com
InfluenzaWho is at High Risk for Flu-related Complications?
Sources: CDC, People at High Risk of Developing Flu-related Complications, 3 Nov 09, http://www.cdc.gov/h1n1flu/highrisk.htmJain & Kamimoto, Hospitalized patients with 2009 H1N1 influenza in the US, April-June 2009, NEJM, 12 Nov 09, http://content.nejm.org/cgi/reprint/NEJMoa0906695.pdfWHO Writing Committee, Clinical Aspects of Pandemic 2009 A(H1N1) Infection, NEJM, 6 May 10, http://content.nejm.org/cgi/reprint/362/18/1708.pdfCDC, Influenza Activity-United States, 2011-12 Season & Composition of the 2012-13 Influenza Vaccine, MMWR, 8 Jun 12CDC, Lisa Grohskopf,, Influenza Vaccination-ACIP Recommendations, National Influenza Vaccine Summit, 16 May 12Punpanich W, A review on the clinical spectrum & natural history of human influenza, IJID Online, 11 Jul 12; http://www.ijidonline.com/article/S1201-9712(12)01177-0/abstract
• Children younger than 5, but especially children < 2 years old• Adults 65 years of age and older• Women who are pregnant or post-partum (2 weeks)• Persons younger than 19 years on long-term aspirin therapy-seasonal flu only• American Indians & Alaskan Natives• Persons who are morbidly-obese (body mass index > 40)-pH1N1 only• Residents of nursing homes & other chronic-care facilities• People who have medical conditions including:
– Asthma and/or chronic lung disease (COPD, cystic fibrosis)– Heart disease such as congenital, CHF and coronary artery disease– Diabetes and other endocrine disorders– Hemoglobinopathy such as sickle cell disease (uncertain for pH1N1)– Chronic kidney and liver disorders (uncertain for pH1N1)– Neuromuscular, neurocognitive & other neuro-developmental conditions– Transplant patients or those chronically immunosuppressed (cancer, chronic steroid therapy)– Persons with HIV infection or full-blown AIDS (uncertain for pH1N1)
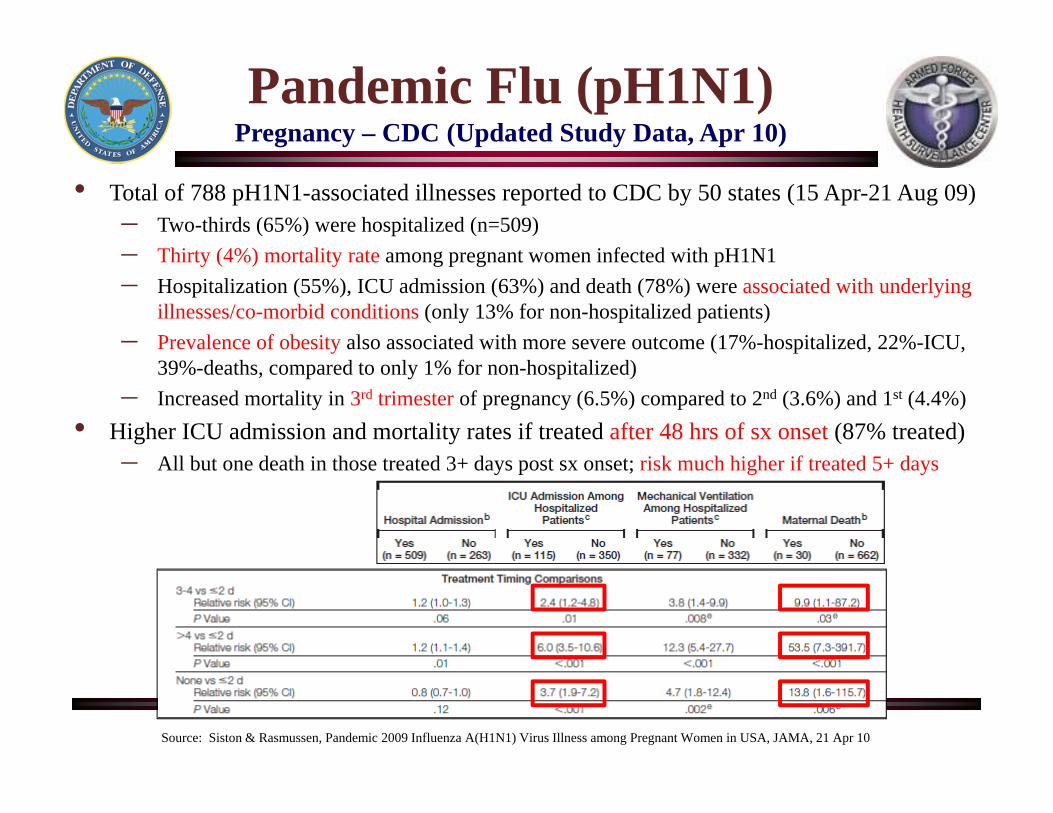
Pandemic Flu (pH1N1)Pregnancy – CDC (Updated Study Data, Apr 10)
• Total of 788 pH1N1-associated illnesses reported to CDC by 50 states (15 Apr-21 Aug 09)– Two-thirds (65%) were hospitalized (n=509)– Thirty (4%) mortality rate among pregnant women infected with pH1N1– Hospitalization (55%), ICU admission (63%) and death (78%) were associated with underlying
illnesses/co-morbid conditions (only 13% for non-hospitalized patients)– Prevalence of obesity also associated with more severe outcome (17%-hospitalized, 22%-ICU,
39%-deaths, compared to only 1% for non-hospitalized)– Increased mortality in 3rd trimester of pregnancy (6.5%) compared to 2nd (3.6%) and 1st (4.4%)
• Higher ICU admission and mortality rates if treated after 48 hrs of sx onset (87% treated)– All but one death in those treated 3+ days post sx onset; risk much higher if treated 5+ days
Source: Siston & Rasmussen, Pandemic 2009 Influenza A(H1N1) Virus Illness among Pregnant Women in USA, JAMA, 21 Apr 10

•11
Seasonal & Pandemic Flu
Diagnosis
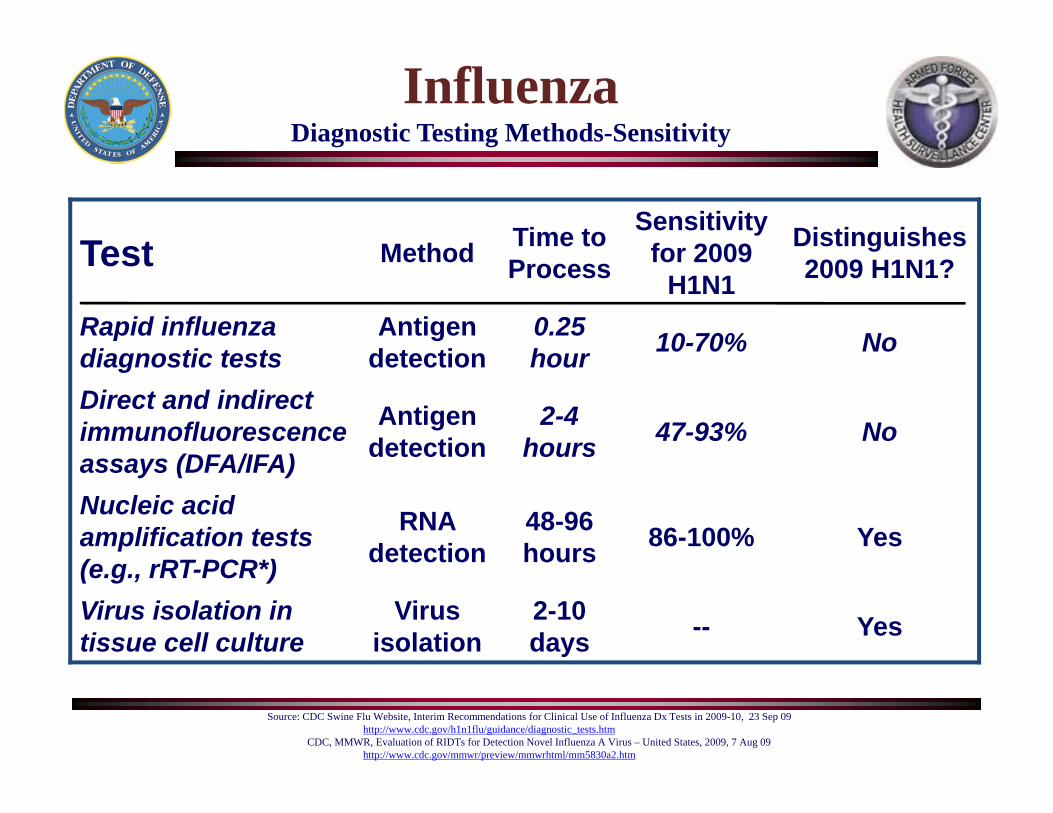
InfluenzaDiagnostic Testing Methods-Sensitivity
Source: CDC Swine Flu Website, Interim Recommendations for Clinical Use of Influenza Dx Tests in 2009-10, 23 Sep 09http://www.cdc.gov/h1n1flu/guidance/diagnostic_tests.htm
CDC, MMWR, Evaluation of RIDTs for Detection Novel Influenza A Virus – United States, 2009, 7 Aug 09http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5830a2.htm
Test Method Time to Process
Sensitivity for 2009
H1N1
Distinguishes 2009 H1N1?
Rapid influenza diagnostic tests
Antigen detection
0.25 hour 10-70% No
Direct and indirect immunofluorescence assays (DFA/IFA)
Antigen detection
2-4 hours 47-93% No
Nucleic acid amplification tests (e.g., rRT-PCR*)
RNA detection
48-96 hours 86-100% Yes
Virus isolation in tissue cell culture
Virus isolation
2-10 days -- Yes
InfluenzaCDC’s & US Military’s Improved rRT-PCR Testing Panels
• Upgrade of 2009 rRT-PCR Swine Flu Panel (EUA expired 23 Jun 10) – Approved by FDA on 2 Sep 11
• ABI-based rRT-PCR testing on ABI 7500 FAST DX platform with new 5-target panel (in vitro diagnostic, IVD)
• Incorporates the 2009 pdmH1-seasonal primer in addition to universal A/B, H3-seasonal and H5-avian primers
• Sensitivity and Specificity is very good (> 96%)• Diagnosis within 4 hrs of specimen receipt• Can use upper (OP, NP) and lower resp tract (BAL,
endotracheal aspirate) samples
• CBMS-JPMO development of a new 5-target ABI assay on the JBAIDS platform – Approved by FDA on mid-Sep 11
• Previously extended EUA for Swine Flu Panel use in JBAIDS platform past its EUA expiration date (EUA granted on 24 Aug 09)
Sources: CDC Press Release, 2 Sep 11, http://www.cdc.gov/media/releases/2011/p0902_diag_lab.htmlABI website, 22 Jun 10, https://products.appliedbiosystems.com/CBMC-JPMO Fact Sheet, JBAIDS, 17 Mar 10, https://jacks.jpeocbd.army.mil/Jacks/Public/FactSheetProvider.aspx?productId=344AFHSC note, Influenza detection kit helps AFHSC identify outbreaks before they start, 23 Sep 11, http://science.dodlive.mil/2011/09/23/influenza-detection-kit-helps-afhsc-identify-outbreaks-before-they-start/
InfluenzaWho Should Get Tested?
• Hospitalized patients with suspected influenza• Those with high-risk conditions
– Neurodevelopmental conditions or cerebral palsy– Chronic pulmonary conditions– CHD, metabolic/endocrine or immunosuppression
• Patients who died of an acute illness with suspected influenza– Suspected viral pneumonia or ARDS
• Other cases where it is needed for infection control or management of close contacts– In MTFs for HCWs/staff and inpatients – “limiting spread”– Close contacts (< 2 meters) of pH1N1-infected patients (see next slide)
Source: CDC Swine Flu Website, Interim Recommendations for Clinical Use of Dx Tests in 2009-10, 23 Sep 09http://www.cdc.gov/h1n1flu/guidance/diagnostic_tests.htm
•15
Seasonal & Pandemic Flu
Antivirals
• Used for both treatment and chemoprophylaxis• Widespread outbreak prophylaxis not practical• “Ring prophylaxis” shown to limit transmission in Singaporean military
(Lee VJ, NEJM, 10 Jun 10)
• Limited supply and cost need to be considered• Dosage and duration of treatment could vary from strain to strain
(usual Tx is 75 mg BID, may go up to 150 mg bid for > 10 days, WHO, Feb 10)• Time to treatment (preferably within 48 hrs) is critical !!!
(McLean E, Epidemiol & Infect, Jul 10)
• Treatment within 3 days of onset decreases viral shedding!!! (Ling LM, CID, 1 Apr 10)
• No proven effect on limiting person-to-person transmission• No proven effect on reducing risk of hospitalization or complications
(Jefferson T, et al, The Cochrane Collaboration, 18 Jan 12)
Antivirals in Influenza“Take Home” Points
Sources: CDC Guidance on Use of Antiviral Agents during 2010-2011 Influenza Season, 14 Jan 11, Health Alert Network, http://www.cdc.gov/flu/professionals/antivirals/index.htmCDC, Antiviral Agents for the Treatment & Chemoprophylaxis of Influenza, MMWR, Vol. 60, No. 1, 21 Jan 11, URL: http://www.cdc.gov/mmwr/PDF/rr/rr6001.pdf?source=govdelivery
WHO Influenza Update # 125, 14 January 2011, http://www.who.int/csr/disease/influenza/2011_01_14_GIP_surveillance/en/index.html#whereisLing LM, Oseltamivir & Viral Shedding, Singapore, Clin Infect Dis, 1 Apr 10; Lee VJ, Oseltamivir Ring Prophylaxis for Containment of 2009 H1N1 Influenza Outbreaks, NEJM, 10 Jun 10Tramontana AR, Oseltamivir Resistance in Oncology & Hematology Patients with Pandemic H1N1 in Australia, EID, Jul 10, http://www.cdc.gov/eid/content/16/7/pdfs/1068.pdfHill-Cawthorne GA, Oseltamivir-resistant Pandemic H1N1 in Patient with Impaired Immune System, EID, Jul 10, http://www.cdc.gov/eid/content/16/7/pdfs/1185.pdfMcLean E, Pandemic H1N1 in the UK: clinical & epidemiological findings from FF100 cases, Epidemiol & Infect, Jul 10, doi:10.1017/S0950268810001366 Jefferson T, et al, Neuraminidase inhibitors for preventing and treating influenza in healthy adults and children, Cochrane Database of Systematic Reviews, Art No. CD008965, 18 Jan 12, http://www.thecochranelibrary.com/details/file/1440293/CD008965.html
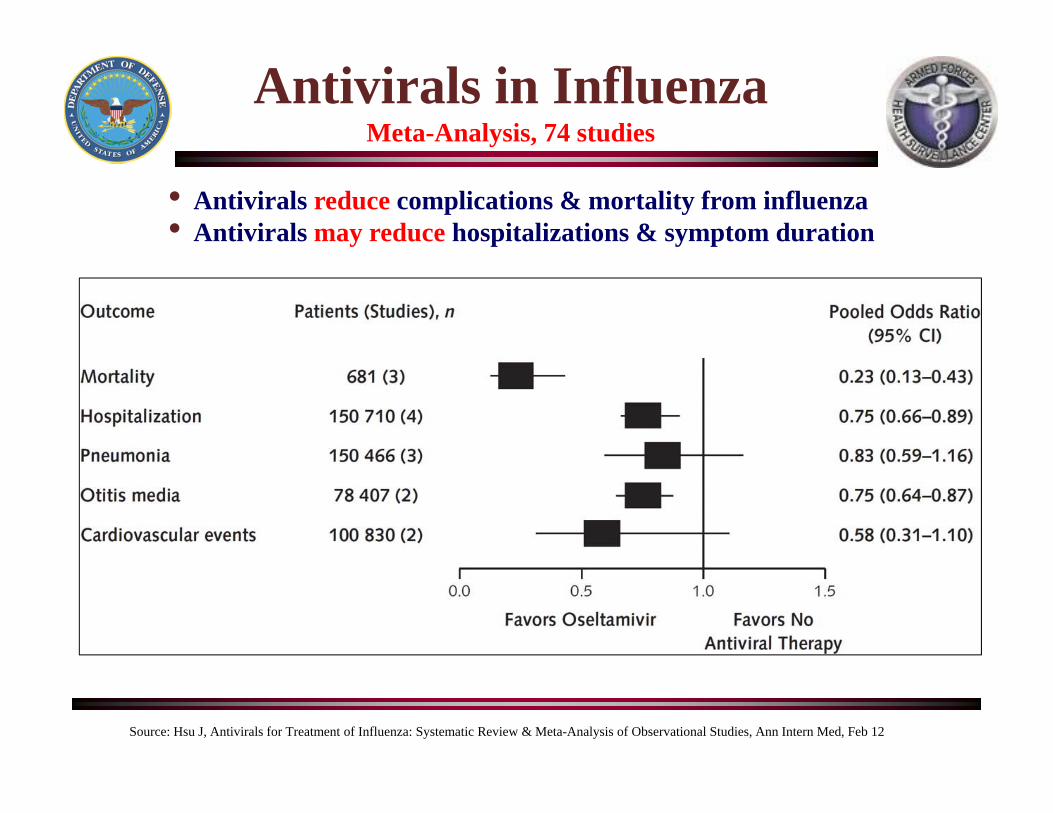
• Antivirals reduce complications & mortality from influenza• Antivirals may reduce hospitalizations & symptom duration
Antivirals in InfluenzaMeta-Analysis, 74 studies
Source: Hsu J, Antivirals for Treatment of Influenza: Systematic Review & Meta-Analysis of Observational Studies, Ann Intern Med, Feb 12
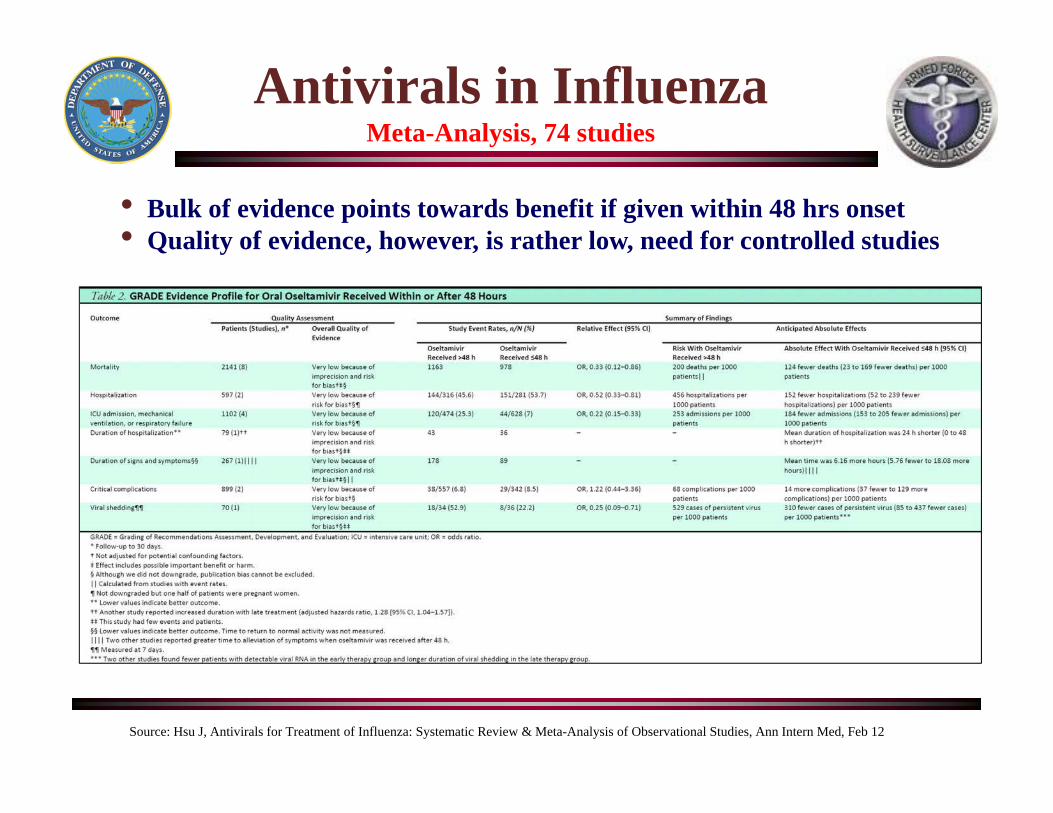
• Bulk of evidence points towards benefit if given within 48 hrs onset• Quality of evidence, however, is rather low, need for controlled studies
Antivirals in InfluenzaMeta-Analysis, 74 studies
Source: Hsu J, Antivirals for Treatment of Influenza: Systematic Review & Meta-Analysis of Observational Studies, Ann Intern Med, Feb 12
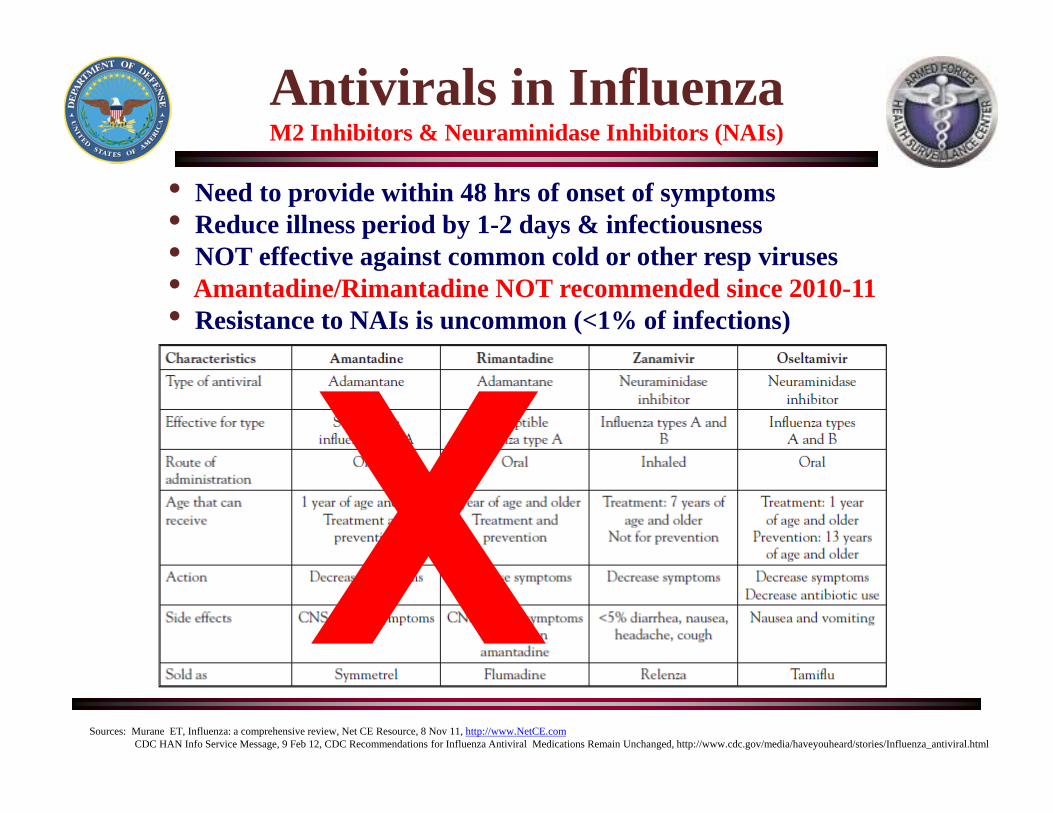
Antivirals in InfluenzaM2 Inhibitors & Neuraminidase Inhibitors (NAIs)
• Need to provide within 48 hrs of onset of symptoms• Reduce illness period by 1-2 days & infectiousness• NOT effective against common cold or other resp viruses• Amantadine/Rimantadine NOT recommended since 2010-11• Resistance to NAIs is uncommon (<1% of infections)
Sources: Murane ET, Influenza: a comprehensive review, Net CE Resource, 8 Nov 11, http://www.NetCE.comCDC HAN Info Service Message, 9 Feb 12, CDC Recommendations for Influenza Antiviral Medications Remain Unchanged, http://www.cdc.gov/media/haveyouheard/stories/Influenza_antiviral.html
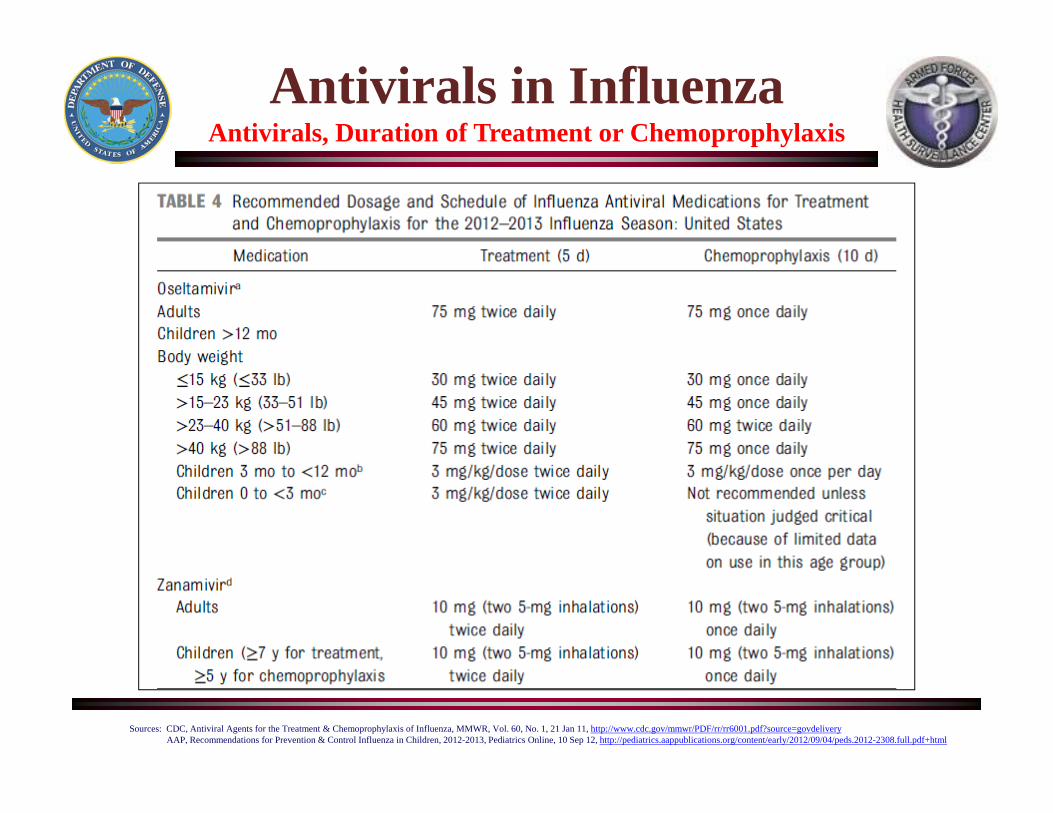
Antivirals in InfluenzaAntivirals, Duration of Treatment or Chemoprophylaxis
Sources: CDC, Antiviral Agents for the Treatment & Chemoprophylaxis of Influenza, MMWR, Vol. 60, No. 1, 21 Jan 11, http://www.cdc.gov/mmwr/PDF/rr/rr6001.pdf?source=govdeliveryAAP, Recommendations for Prevention & Control Influenza in Children, 2012-2013, Pediatrics Online, 10 Sep 12, http://pediatrics.aappublications.org/content/early/2012/09/04/peds.2012-2308.full.pdf+html
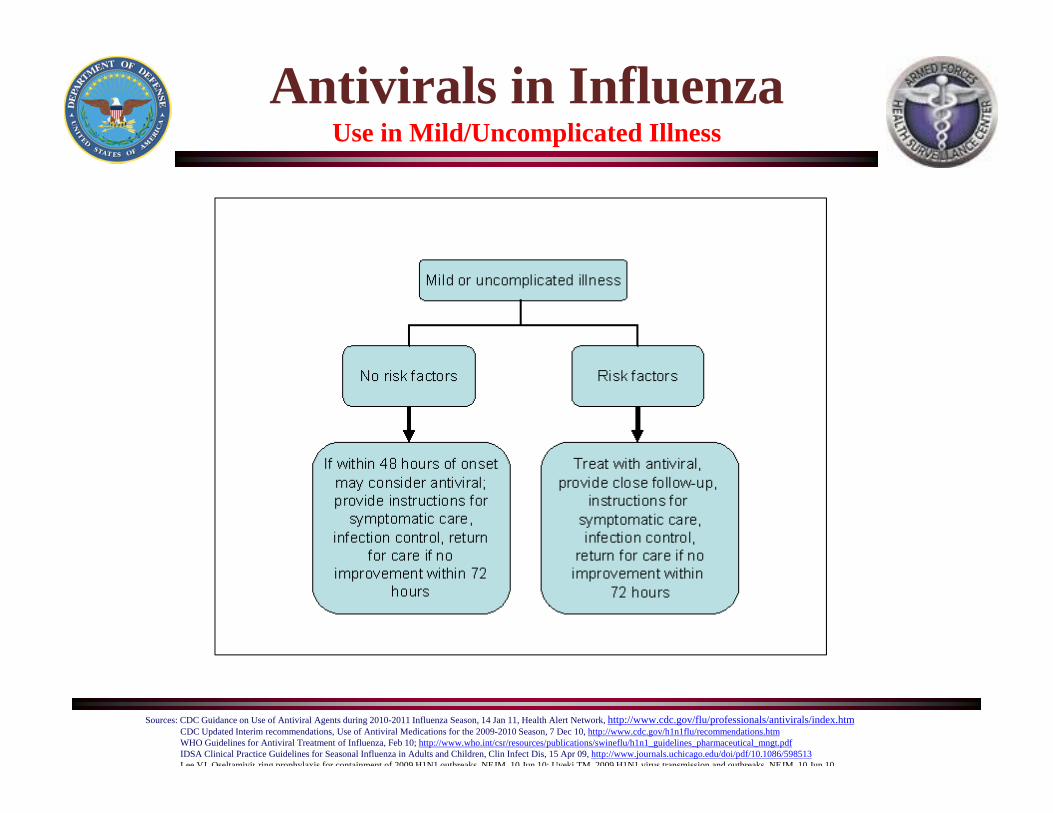
Antivirals in InfluenzaUse in Mild/Uncomplicated Illness
Sources: CDC Guidance on Use of Antiviral Agents during 2010-2011 Influenza Season, 14 Jan 11, Health Alert Network, http://www.cdc.gov/flu/professionals/antivirals/index.htmCDC Updated Interim recommendations, Use of Antiviral Medications for the 2009-2010 Season, 7 Dec 10, http://www.cdc.gov/h1n1flu/recommendations.htmWHO Guidelines for Antiviral Treatment of Influenza, Feb 10; http://www.who.int/csr/resources/publications/swineflu/h1n1_guidelines_pharmaceutical_mngt.pdfIDSA Clinical Practice Guidelines for Seasonal Influenza in Adults and Children, Clin Infect Dis, 15 Apr 09, http://www.journals.uchicago.edu/doi/pdf/10.1086/598513Lee VJ Oseltamivir ring prophylaxis for containment of 2009 H1N1 outbreaks NEJM 10 Jun 10; Uyeki TM 2009 H1N1 virus transmission and outbreaks NEJM 10 Jun 10
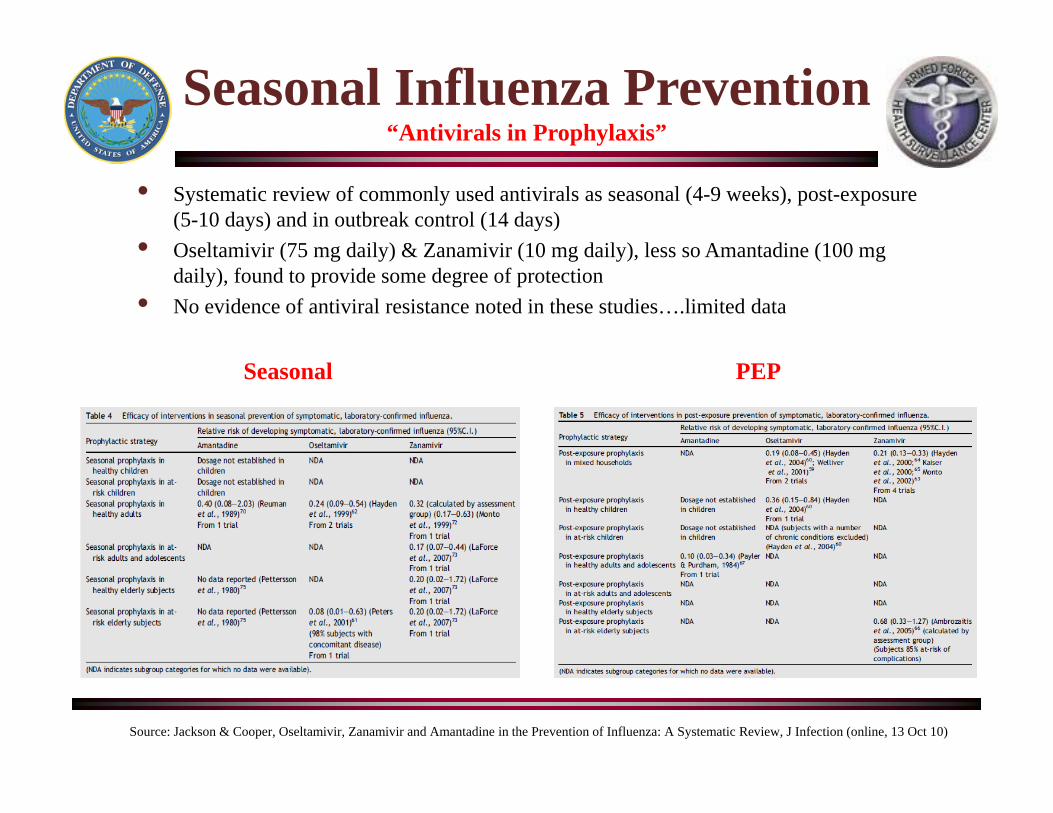
Seasonal Influenza Prevention“Antivirals in Prophylaxis”
• Systematic review of commonly used antivirals as seasonal (4-9 weeks), post-exposure (5-10 days) and in outbreak control (14 days)
• Oseltamivir (75 mg daily) & Zanamivir (10 mg daily), less so Amantadine (100 mg daily), found to provide some degree of protection
• No evidence of antiviral resistance noted in these studies….limited data
Source: Jackson & Cooper, Oseltamivir, Zanamivir and Amantadine in the Prevention of Influenza: A Systematic Review, J Infection (online, 13 Oct 10)
Seasonal PEP
• Seasonal Influenza Pre-Exposure (?) Prophylaxis:– Reduction in lab-confirmed influenza ~ 50-75% (adult HH contacts)– Reduction in lab-confirmed influenza > 80% (at-risk adult HH contacts)
• Seasonal Influenza Post-Exposure Prophylaxis:– Reduction of lab-confirmed influenza ~ 80-90% (adult HH contacts)– Analysis of UK pandemic data (UK FF100 study) revealed reduction in lab-confirmed influenza ~ 92% in adult HH contacts (Pebody, EID, 2011)
• New compounds (Laninamivir & Peramivir, approved in Japan & Korea) will need to be evaluated in RCT for prophylaxis efficacy in the future
Antivirals in InfluenzaPost-pandemic Review of anti-Influenza Drug Effectiveness (PRIDE)
Source: Van Tam J, Use of antivirals to reduce impact of seasonal & pandemic influenza, ISIRV conference, Munich, GE, 6 Sep 12Univ Nottingham, PRIDE study data & preliminary analysis, http://www.nottingham.ac.uk/chs/research/projects/pride/index.aspx
Antivirals for InfluenzaMain Reference – CDC-ACIP Recommendations
Sources: CDC, Antiviral Agents for the Treatment & Chemoprophylaxis of Influenza, MMWR, Vol. 60, No. 1, 21 Jan 11URL: http://www.cdc.gov/mmwr/PDF/rr/rr6001.pdf?source=govdelivery
CDC, Influenza Antiviral Medications: A Summary for Clinicians, 30 Aug 11, http://www.cdc.gov/flu/professionals/antivirals/index.htm
• Updates previous recommendations by CDC’s ACIP in 2008 (MMWR, Vol 57, No. RR-7)
• Incorporates data on antiviral resistance of pH1N1 and A/H3 and B subtypes in USA
• Outlines advice on use of NAIs (Oseltamivir or Zanamivir) in severely ill and high-risk patient groups to be targeted for Tx
• Updates advice on NAI use among infants
• Incorporates recommendation for early Tx of healthy patients, if within 48 hrs of onset
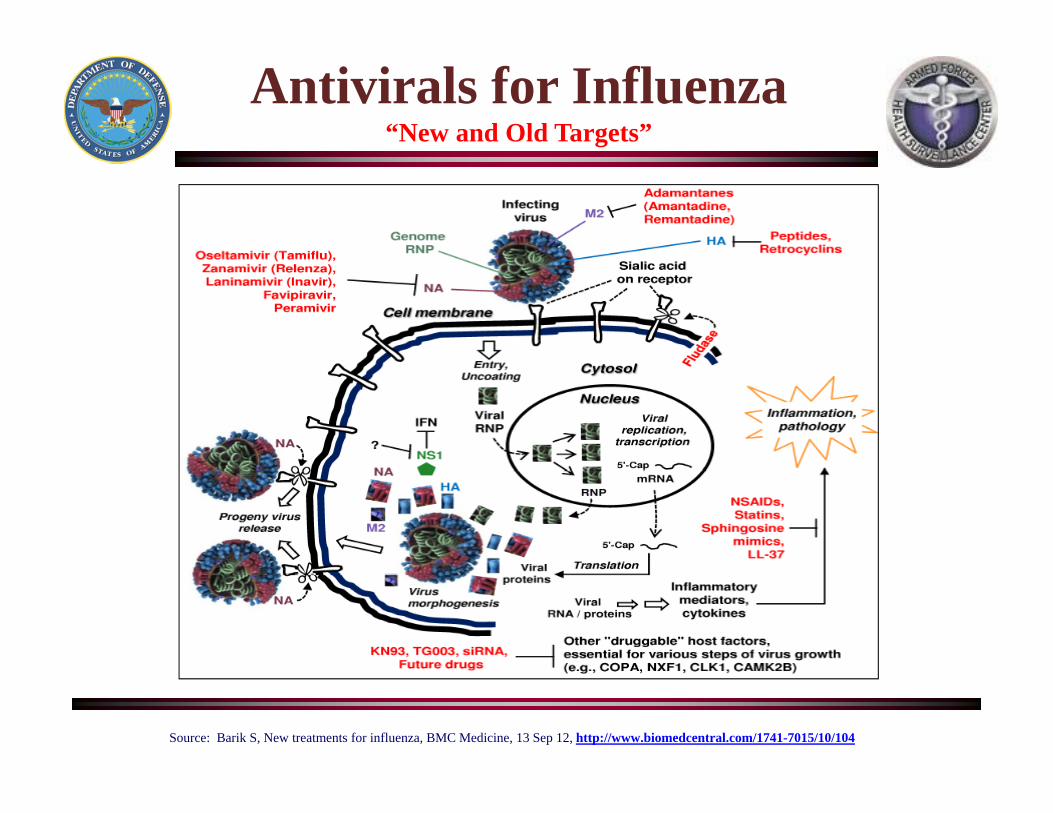
Antivirals for Influenza“New and Old Targets”
Source: Barik S, New treatments for influenza, BMC Medicine, 13 Sep 12, http://www.biomedcentral.com/1741-7015/10/104
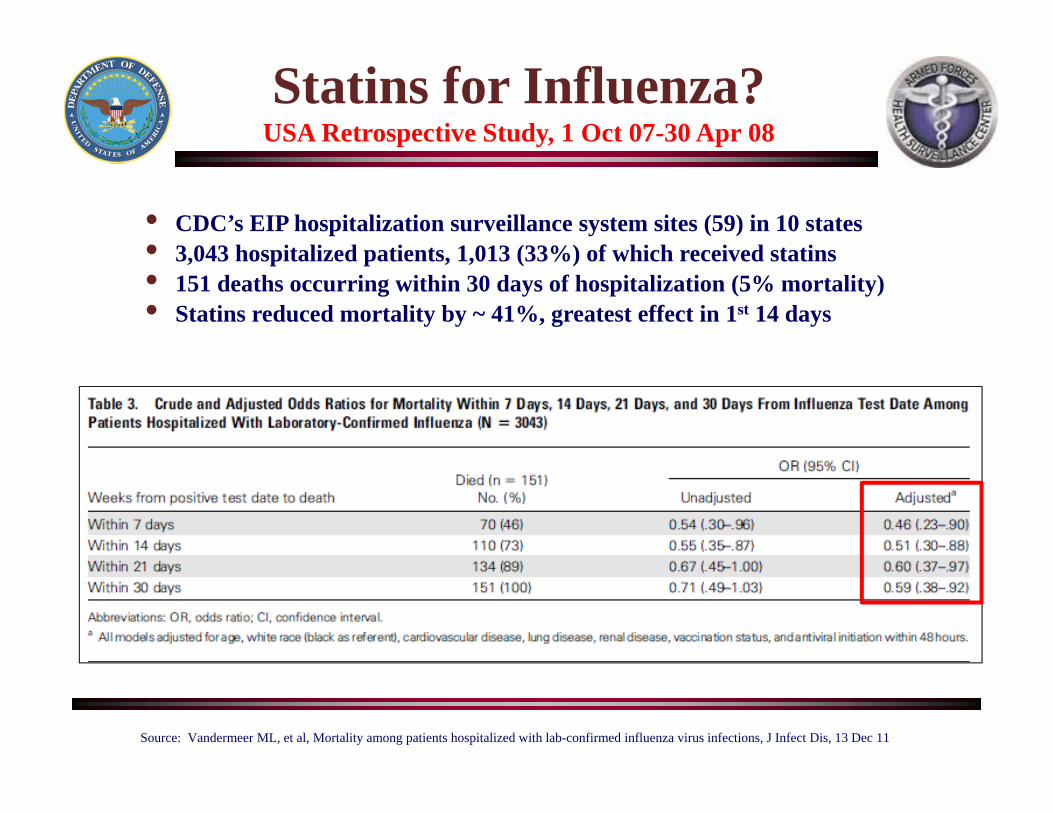
Statins for Influenza?USA Retrospective Study, 1 Oct 07-30 Apr 08
Source: Vandermeer ML, et al, Mortality among patients hospitalized with lab-confirmed influenza virus infections, J Infect Dis, 13 Dec 11
• CDC’s EIP hospitalization surveillance system sites (59) in 10 states• 3,043 hospitalized patients, 1,013 (33%) of which received statins• 151 deaths occurring within 30 days of hospitalization (5% mortality)• Statins reduced mortality by ~ 41%, greatest effect in 1st 14 days
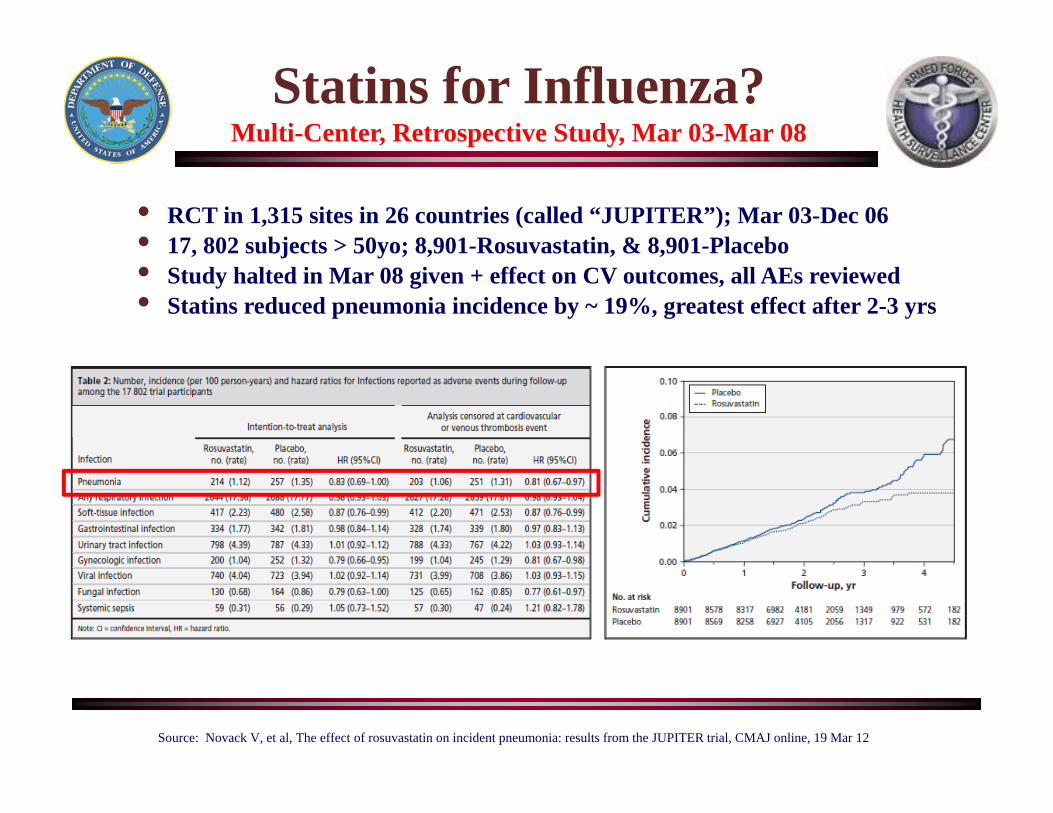
Statins for Influenza?Multi-Center, Retrospective Study, Mar 03-Mar 08
Source: Novack V, et al, The effect of rosuvastatin on incident pneumonia: results from the JUPITER trial, CMAJ online, 19 Mar 12
• RCT in 1,315 sites in 26 countries (called “JUPITER”); Mar 03-Dec 06• 17, 802 subjects > 50yo; 8,901-Rosuvastatin, & 8,901-Placebo• Study halted in Mar 08 given + effect on CV outcomes, all AEs reviewed • Statins reduced pneumonia incidence by ~ 19%, greatest effect after 2-3 yrs
•28
Seasonal & Pandemic Flu
Vaccines
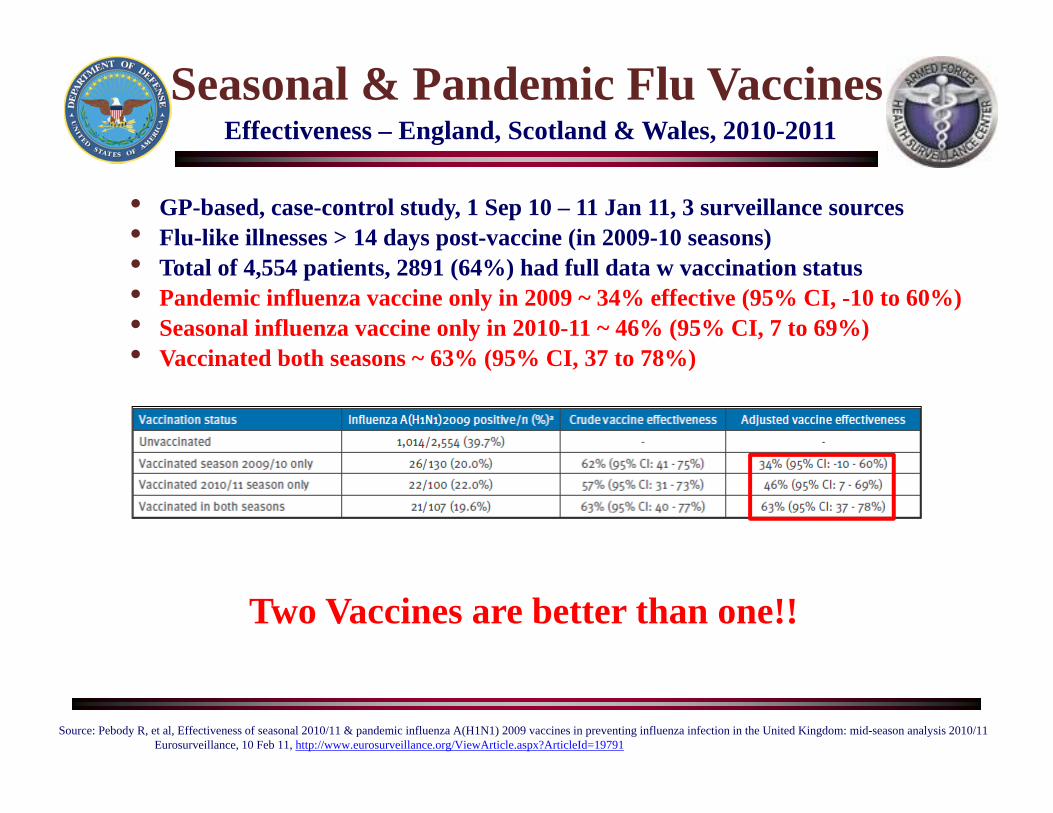
Seasonal & Pandemic Flu VaccinesEffectiveness – England, Scotland & Wales, 2010-2011
Source: Pebody R, et al, Effectiveness of seasonal 2010/11 & pandemic influenza A(H1N1) 2009 vaccines in preventing influenza infection in the United Kingdom: mid-season analysis 2010/11Eurosurveillance, 10 Feb 11, http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19791
• GP-based, case-control study, 1 Sep 10 – 11 Jan 11, 3 surveillance sources• Flu-like illnesses > 14 days post-vaccine (in 2009-10 seasons)• Total of 4,554 patients, 2891 (64%) had full data w vaccination status• Pandemic influenza vaccine only in 2009 ~ 34% effective (95% CI, -10 to 60%)• Seasonal influenza vaccine only in 2010-11 ~ 46% (95% CI, 7 to 69%)• Vaccinated both seasons ~ 63% (95% CI, 37 to 78%)
Two Vaccines are better than one!!
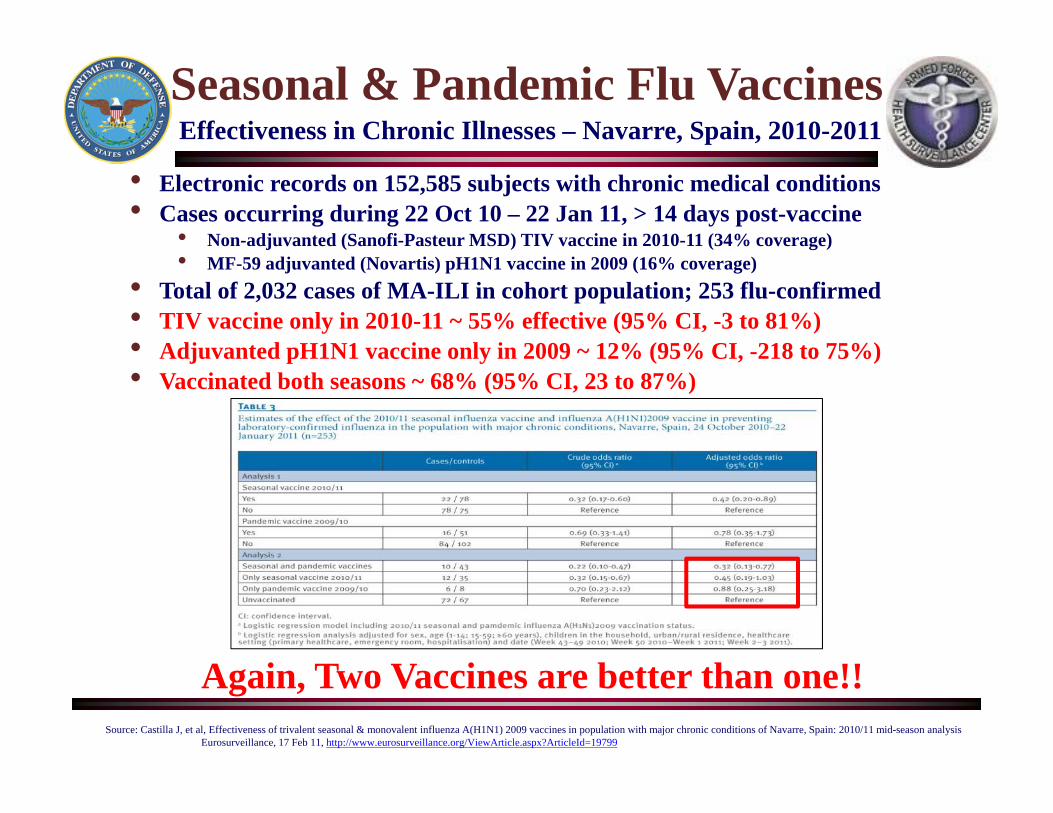
Seasonal & Pandemic Flu VaccinesEffectiveness in Chronic Illnesses – Navarre, Spain, 2010-2011
Source: Castilla J, et al, Effectiveness of trivalent seasonal & monovalent influenza A(H1N1) 2009 vaccines in population with major chronic conditions of Navarre, Spain: 2010/11 mid-season analysisEurosurveillance, 17 Feb 11, http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19799
• Electronic records on 152,585 subjects with chronic medical conditions• Cases occurring during 22 Oct 10 – 22 Jan 11, > 14 days post-vaccine
• Non-adjuvanted (Sanofi-Pasteur MSD) TIV vaccine in 2010-11 (34% coverage)• MF-59 adjuvanted (Novartis) pH1N1 vaccine in 2009 (16% coverage)
• Total of 2,032 cases of MA-ILI in cohort population; 253 flu-confirmed• TIV vaccine only in 2010-11 ~ 55% effective (95% CI, -3 to 81%)• Adjuvanted pH1N1 vaccine only in 2009 ~ 12% (95% CI, -218 to 75%)• Vaccinated both seasons ~ 68% (95% CI, 23 to 87%)
Again, Two Vaccines are better than one!!
H1N1 Pandemic VaccinesSafety Monitoring – GBS, Taiwan (1 Nov 09-16 Mar 10)
Sources: Langmuir AD, et al, An epidemiologic and clinical evaluation of Guillain-Barre´ syndrome reported in association with the administration of swine influenza vaccines. Am J Epidemiol. 1984;119(6):841-879Institute of Medicine. Immunization Safety Review: Influenza Vaccines and Neurological, Complications. Washington, DC: National Academies Press; 2003Stratton K, Ford A, Rusch E, Wright Clayton E, eds; Institute of Medicine Committee to Review Adverse Effects of Vaccines. Adverse Effects of Vaccines: Evidence and Causality. Washington, DC: National Academies Press; 2012
Wan-Ting Huang, Monitoring the Safety of Pandemic H1N1 Vaccine, Lancet, 3 Apr 10
• Previously identified association of GBS post-H1N1 “swine flu” vaccination in 1976-77 & subsequent IoM review in 2003 (risk ~ 2 per Million vaccinees)
• Increased risk only seen previously with H1N1-specific vaccines but not seasonal vaccines (IoM report, 2012)
• National Health Insurance in Taiwan provides influenza immunization to high-risk groups; retrospective study
• Prior vaccination with seasonal influenza vaccine in 2004-2008 associated with a risk of GBS ~ 0.5 to 3 per 100,000 person-years
• Very low adverse event rates for pH1N1 vaccinees• Only 4 GBS cases among 5.66 Million doses administered
(< 1 per Million doses)
H1N1 Pandemic VaccinesSafety Monitoring – GBS, Quebec, Canada (13 Oct 09-31 Mar 10)
Source: De Wals P, et al, Risk of GBS following Pandemic H1N1 Influenza Vaccination in Quebec, JAMA, 11 Jul 12
• Massive pH1N1 vaccination program in Oct 09-Mar 10 (adjuvanted AS03 vaccine, GSK); ~ 4.5 Million of 7.8 Million residents vaccinated
• Population-based cohort (vaccinees vs non-vaccinees) with mandatory reporting of potential GBS cases to PH authorities
• 83 confirmed GBS cases (incidence =2.3 per 100,000), 25 post-pH1N1 vaccination (8 weeks), 19 of which occurred within 4 weeks
• By Poisson regression, higher GBS rates for pH1N1 vaccinees within 8 wks post-vaccine (RR=1.80, 95% CI=1.12-2.87); even higher GBS risk within 4 wks post-vaccine (RR=2.75, 95% CI=1.63-4.62)
• Increased risk only seen in those > 50 yo (RR=2.69, 95% CI=1.51-4.80)• GBS risk ~ 2.0 per 1 Million doses administered (range of 1.3-2.7)
H1N1 Pandemic VaccinesSafety Monitoring – CDC, UK & DoD (Nov 09-May 10)
• In the USA, using CDC’s EIP population-based program sites:• Small increased risk of post-vaccine GBS (non-adjuvanted) detected
(RR=2.1-3.0)• GBS risk ~ 2.0 per 1 Million doses administered (range of 1.5-2.8)• Risk for GBS following pH1N1 inactivated monovalent vaccination
similar to risk observed for seasonal TIV in previous seasons
• In the UK, using self-reports & hospital-based databases:• No significant increased risk of post-vaccine GBS (adjuvanted ASO3
vaccine, GSK)
• In the DoD, using hospitalization and self-reported adverse event data (AFHSC/MILVAX) & clinical Dx of all GBS cases at > 400 MTFs• Comparison of post-vaccinee vs non-vaccinee GBS rates• GBS risk ~ 1.5 per 1 Million doses administered• Risk in vaccinees (RR=1.9) not significantly different from non-vaccinees
Sources: Tokars JI, Lewis P, DeStefano F, et al, The risk of Guillain-Barre´ syndrome associated with influenza A(H1N1) 2009 monovalent vaccine and 2009-2010 seasonal influenza vaccines: results from selfcontrolled analyses. Pharmacoepidemiol Drug Saf. 2012;21(5):546-552Lasky et al. The Guillain-Barré syndrome and the 1992-1993 and 1993-1994 influenza vaccines. N Engl J Med. 1998;339:1797-802. Juurlink et al. Guillain-Barré syndrome after influenza vaccination in adults: a population-based study. Arch Intern Med. 2006;166:2217-21
Andrews N, Stowe J, Al-Shahi Salman R, Miller E, Guillain-Barre´ syndrome and H1N1 (2009) pandemic influenza vaccination using an AS03 adjuvanted vaccine in the United Kingdom: selfcontrolled case series. Vaccine. 2011;29(45):7878-7882AFHSC-MILVAX, Monitoring Safety of H1N1 Vaccine, Executive Summary, 3 Jun 10; CDC, Tom Shimabukuro, ACIP Mtg Presentation, Update on Influenza Vaccine Safety Monitoring, 20 Jun 12, http://www.cdc.gov/vaccines/recs/acip/slides-jun12.htm#flu
Seasonal Influenza VaccineDo Not Forget!
• Majority of illnesses and deaths can be prevented by immunization
• Proven to be highly efficacious & cost-effective in many studies
• Single most important tool for pre-pandemic preparation of general public
– Confers initial immunity which may be partially cross-protective or “prime” the immune system
– pH1N1 vaccine not seen to fully protect against other seasonal flu viruses
– Would assist in preventing mixed infections between novel/seasonal viruses
– Would assist in defining true/false novel PI virus infections
Getting a Flu Shot
Sources: CDC, Immunization of Health-Care Personnel, MMWR 2011; 60 (No. RR-7): 8-10, 25 Nov 11, http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6007a1.htm?s_cid=rr6007a1_wCDC, Prevention and control of influenza, MMWR 2010; 60:1128-32, 26 Aug 11, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6033a3.htmNichol KL, Efficacy and effectiveness of influenza vaccination, Vaccine 2008; 26S:D17-D22
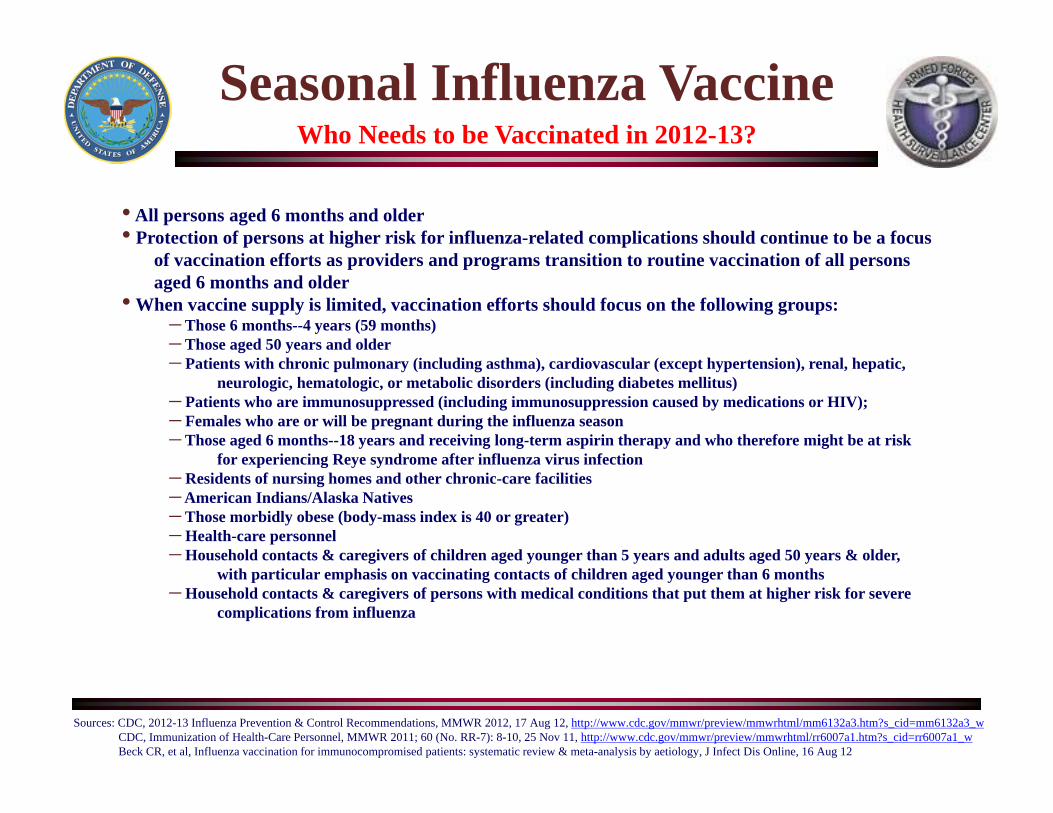
Seasonal Influenza VaccineWho Needs to be Vaccinated in 2012-13?
Sources: CDC, 2012-13 Influenza Prevention & Control Recommendations, MMWR 2012, 17 Aug 12, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6132a3.htm?s_cid=mm6132a3_wCDC, Immunization of Health-Care Personnel, MMWR 2011; 60 (No. RR-7): 8-10, 25 Nov 11, http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6007a1.htm?s_cid=rr6007a1_wBeck CR, et al, Influenza vaccination for immunocompromised patients: systematic review & meta-analysis by aetiology, J Infect Dis Online, 16 Aug 12
• All persons aged 6 months and older• Protection of persons at higher risk for influenza-related complications should continue to be a focus
of vaccination efforts as providers and programs transition to routine vaccination of all personsaged 6 months and older
• When vaccine supply is limited, vaccination efforts should focus on the following groups: – Those 6 months--4 years (59 months) – Those aged 50 years and older– Patients with chronic pulmonary (including asthma), cardiovascular (except hypertension), renal, hepatic,
neurologic, hematologic, or metabolic disorders (including diabetes mellitus)– Patients who are immunosuppressed (including immunosuppression caused by medications or HIV); – Females who are or will be pregnant during the influenza season– Those aged 6 months--18 years and receiving long-term aspirin therapy and who therefore might be at risk
for experiencing Reye syndrome after influenza virus infection– Residents of nursing homes and other chronic-care facilities– American Indians/Alaska Natives– Those morbidly obese (body-mass index is 40 or greater)– Health-care personnel– Household contacts & caregivers of children aged younger than 5 years and adults aged 50 years & older,
with particular emphasis on vaccinating contacts of children aged younger than 6 months– Household contacts & caregivers of persons with medical conditions that put them at higher risk for severe
complications from influenza
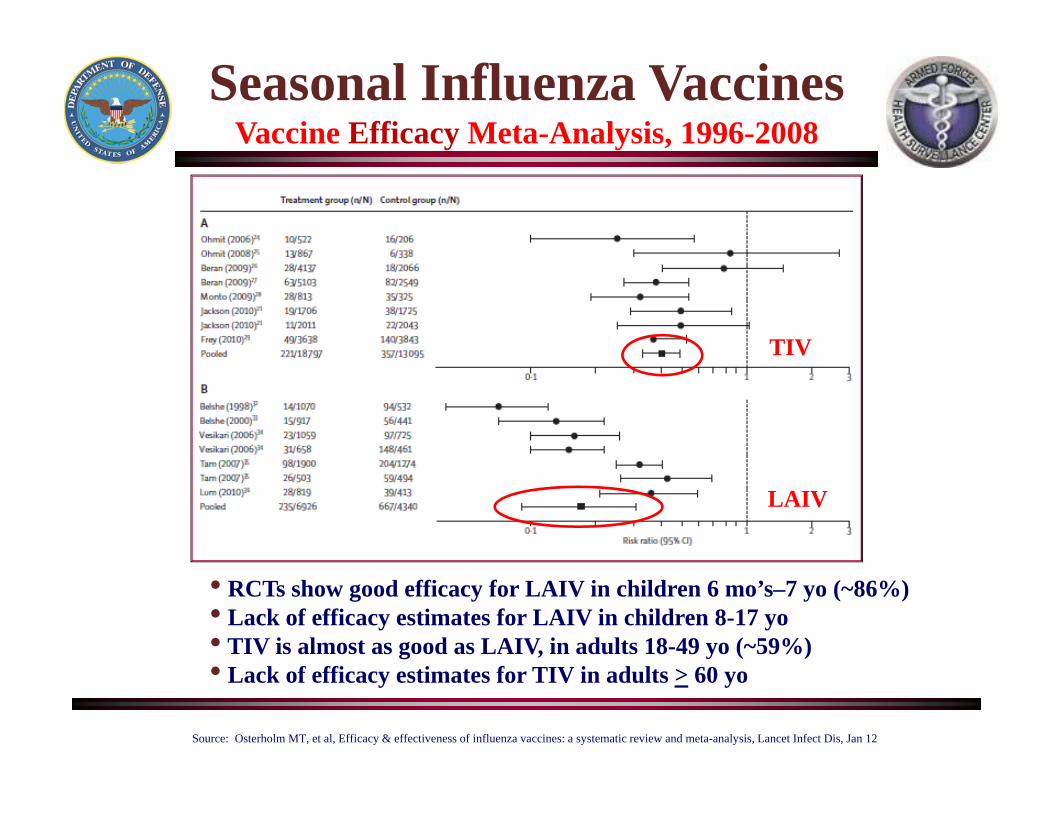
Seasonal Influenza VaccinesVaccine Efficacy Meta-Analysis, 1996-2008
• RCTs show good efficacy for LAIV in children 6 mo’s–7 yo (~86%)• Lack of efficacy estimates for LAIV in children 8-17 yo• TIV is almost as good as LAIV, in adults 18-49 yo (~59%)• Lack of efficacy estimates for TIV in adults > 60 yo
Source: Osterholm MT, et al, Efficacy & effectiveness of influenza vaccines: a systematic review and meta-analysis, Lancet Infect Dis, Jan 12
TIV
LAIV
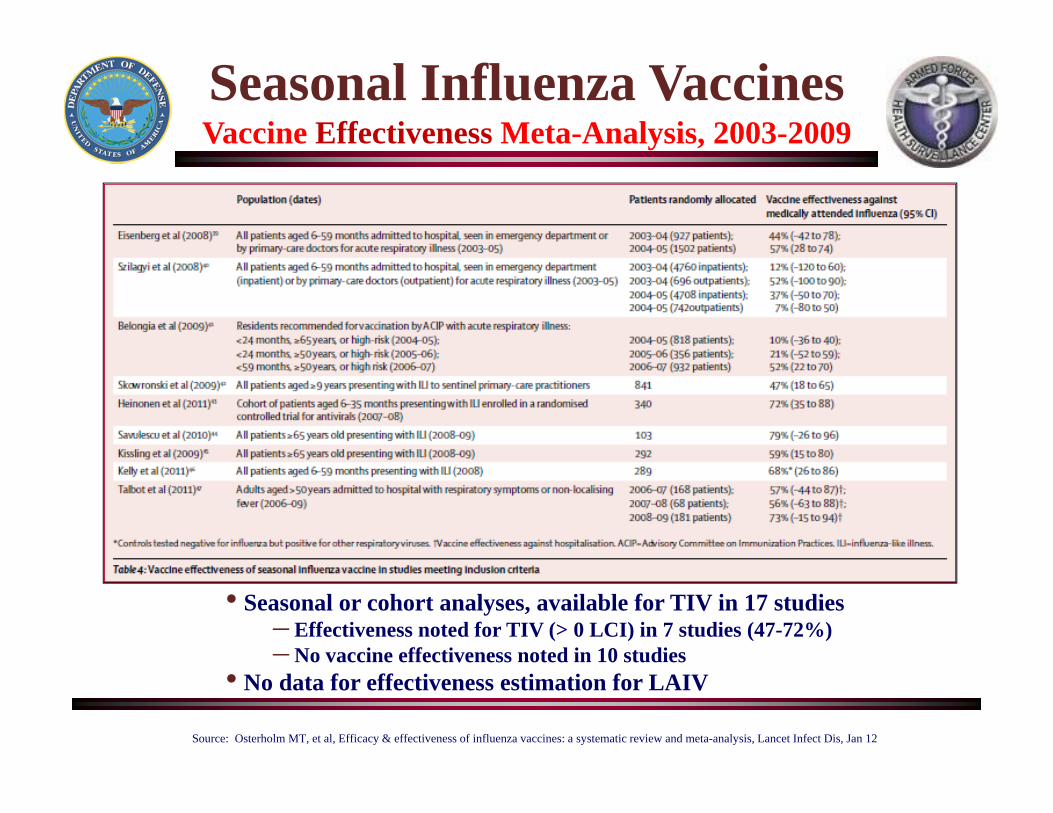
Seasonal Influenza VaccinesVaccine Effectiveness Meta-Analysis, 2003-2009
• Seasonal or cohort analyses, available for TIV in 17 studies– Effectiveness noted for TIV (> 0 LCI) in 7 studies (47-72%)– No vaccine effectiveness noted in 10 studies
• No data for effectiveness estimation for LAIV
Source: Osterholm MT, et al, Efficacy & effectiveness of influenza vaccines: a systematic review and meta-analysis, Lancet Infect Dis, Jan 12
• DoD continued to track year-to-year vaccine effectiveness among recruits, dependents & active duty personnel as part of a comprehensive laboratory-based influenza surveillance program
• Evidence of high influenza vaccine protection among recruits in 2004-05 through 2008-09 seasons (~80-85%), less so in post-pandemic period with predominance of A/H1 virus circulation (~30-60%)
• Potential evidence of lesser protection against A/H1, particularly with the Live Attenuated Influenza Vaccine among recruits (in 2009-10)
• Higher VE in military personnel (91% in recruits, 77% in active duty) noted in 2011-12 season when analysis is based on RT-PCR/culture confirmed cases vs test-negative controls (anti-H1 immunity)
Seasonal Influenza VaccineVaccine Effectiveness in the US Military
Summary
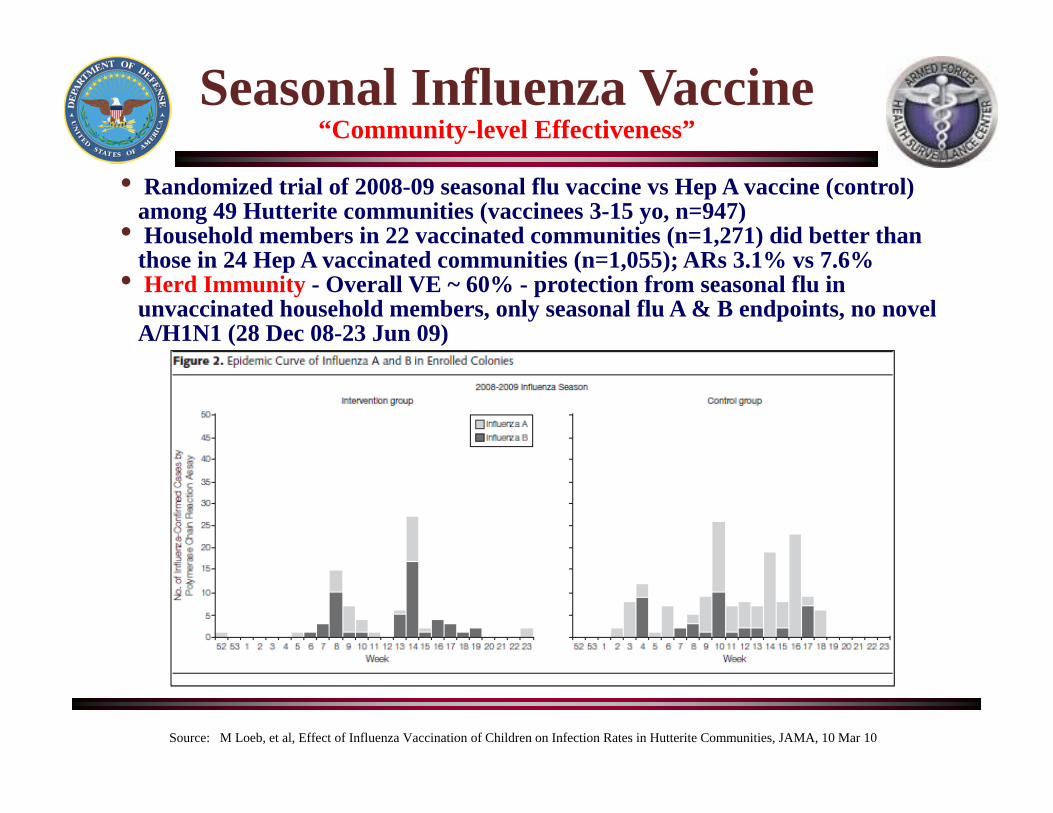
• Randomized trial of 2008-09 seasonal flu vaccine vs Hep A vaccine (control) among 49 Hutterite communities (vaccinees 3-15 yo, n=947)
• Household members in 22 vaccinated communities (n=1,271) did better than those in 24 Hep A vaccinated communities (n=1,055); ARs 3.1% vs 7.6%
• Herd Immunity - Overall VE ~ 60% - protection from seasonal flu in unvaccinated household members, only seasonal flu A & B endpoints, no novel A/H1N1 (28 Dec 08-23 Jun 09)
Seasonal Influenza Vaccine“Community-level Effectiveness”
Source: M Loeb, et al, Effect of Influenza Vaccination of Children on Infection Rates in Hutterite Communities, JAMA, 10 Mar 10
• Non-randomized, prospective, observational cohort study, Nov 02-Sep 05• Navajo & White Mountain Apache Indians, 7 hospitals, children < 6 mos• Cases were DFA-positive for influenza virus or paired sera HI titer increases at
3/6 mos (n=83 of 1,160 infants)
• VE = 41% (95% CI, 7-63%) for infants < 6 mos (vaccinated vs unvacc mothers)• VE increased with serum HI titer > 1:40 in cord blood (range, 32-58%)
Seasonal Influenza VaccineResults in Pregnant Women and Infants (3rd & best study)
Source: Eick AA, et al, Maternal influenza vaccination and effect on influenza virus infection in young infants, Arch Pediatr Adolesc Med, Feb 11
• Randomized, controlled trial, Bangladesh, Aug 04-Dec 05• “Mother’s Gift Project”, children < 6 mos, gestational age, mean BW, Wt for Age• Adjusted for periods of influenza circulation (Feb-Oct) & non-circulation (Sep-Jan)
• Proportion of infants w LBW was reduced by 19% (26%-vacc vs 45%-unvacc)• Mean BW also higher in vacc (3,178g) compared to unvacc (2,978g)
Seasonal Influenza VaccineBenefit for Infant Outcomes Also!
Source: Steinhoff MC, et al, Neonatal outcomes after influenza immunization during pregnancy: a RCT, CMAJ, 21 Feb 12

Seasonal Influenza VaccineImmunocompromised Patients, over 200 studies
Odds of ILI or Lab-confirmed Influenza
Source: Beck CR, et al, Influenza vaccination for immunocompromised patients: systematic review & meta-analysis by aetiology, J Infect Dis Online, 16 Aug 12
Health Care PersonnelNeed to Vaccinate!
• Influenza virus enters hospitals from the community when infected employees, patients or visitors bring it in.
• Secondary transmission between patients and HCPs occurs within the hospital when influenza is not recognized and standard precautions are inadequate.
• Patient morbidity and mortality, HCP absenteeism and disruption of hospital function may result during hospital-acquired influenza outbreaks.
• Vaccinated HCPs break the cycle of hospital associated-influenza exposure and reduce absenteeism.
• Vaccinated HCPs thus “protect” patients, hospital function and the community during influenza epidemics.
• Use TIV preferably, can use LAIV in those not working in protected environments (eg, bone marrow transplant unit)
• Best to require all HCPs to receive annual influenza vaccination
Sources: Plotkin, Orenstein and Offit, Vaccines, Saunders (5th Ed), Chapter 66, 2007CDC, Immunization of Health-Care Personnel, MMWR 2011; 60 (No. RR-7): 8-10, 25 Nov 11, http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6007a1.htm?s_cid=rr6007a1_wMaltezou H, Tsakris A, Vaccination of health-care workers against influenza: our obligation to protect patients, Influenza & Other Resp Viruses, Nov 11, http://onlinelibrary.wiley.com/doi/10.1111/j.1750-2659.2011.00240.x/abstractTalbot TR, The use of LAIV in healthcare personnel (HCP): Guidance from the Society for Healthcare Epidemiology of America (SHEA), Inf Cont Hosp Epid Online, 6 Sep 12, http://www.jstor.org/stable/pdfplus/10.1086/667772.pdf?acceptTC=trueIDSA, Pandemic & Seasonal Influenza: Principles for United States Action, Sep 12, http://www.idsociety.org/uploadedFiles/IDSA/Policy_and_Advocacy/Current_Topics_and_Issues/Influenza_and_Bio-Threats/Seasonal_and_Pandemic_Influenza/IDSA%20Seasonal%20and%20Pandemic%20Influenza%20Principles%20for%20US%20Action%202012.pdf
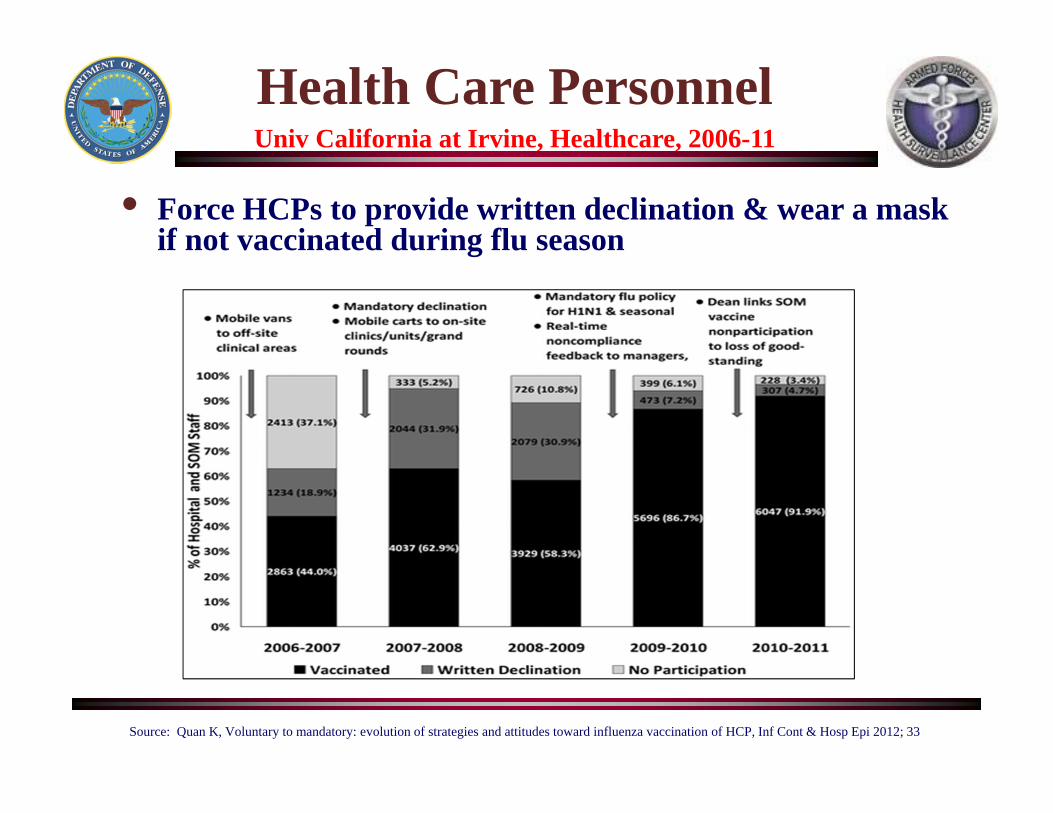
Health Care PersonnelUniv California at Irvine, Healthcare, 2006-11
• Force HCPs to provide written declination & wear a mask if not vaccinated during flu season
Source: Quan K, Voluntary to mandatory: evolution of strategies and attitudes toward influenza vaccination of HCP, Inf Cont & Hosp Epi 2012; 33
Influenza VaccinesNorthern Hemisphere Vaccine for 2012-13
Sources: WHO, Recommended composition of influenza virus vaccines for use in the 2012-2013 northern hemisphere influenza season, 23 Feb 12, http://www.who.int/influenza/vaccines/virus/recommendations/2012_13_north/en/Reed C, et al. Vaccine (2012), doi:10.1016/j.vaccine.2011.12.098CDC, Lisa Grohskopf, Proposed Influenza Vaccination Recs for 2012-2013, ACIP Mtg Presentation, 20 Jun 12, http://www.cdc.gov/vaccines/recs/acip/slides-jun12.htm#fluCDC, ACIP-Recommended Influenza Vaccines, 2012-13 Season, 17 Aug 12, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6132a3.htm?s_cid=mm6132a3_w
• Maintain same strain composition for A/H1N1, an A/California/7/2009 (H1N1)pdm09-like virus (eg, pandemic virus has not drifted much since Apr 09)
• Change strain composition for A/H3N2 to an A/Victoria/361/2011 (H3N2)-like virus (previously used an A/Perth/16/2009 virus)
• Change strain composition for B to a B/Wisconsin/1/2010-like virus, a B/Yamagata/16/88 lineage virus (previously used B/Brisbane/60/2008, a B/Victoria/2/87 lineage virus)
• Quadrivalent LAIV (FluMist Quadrivalent, MedImmune) approved by FDA in Feb 12 (available in 2013-14 season)
Novel A/H3N2 viruses –A(H3N2)v - USASwine-origin Viruses in Humans
Sources: CDC, MMWR Dispatch, 23 Nov 11, http://www.cdc.gov/mmwr/PDF/wk/mm60d1123.pdf, CDC Health Advisory, 3 Aug 12 (CDCHAN-00325-ADV-N)CDC, MMWR Early Release, 10 Aug 12, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm61e0810a1.htm?s_cid=mm61e0810a1_wCDC, Update: Influenza A(H3N2)v transmission and guidelines-five states, 2011-12, 23 Dec 11, 6 Jan 12 & 3 Aug 12, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6051a4.htm?s_cid=mm6051a4_wCDC, Interim Guidance for Influenza Surveillance: Additional specimen collection for detection of Influenza A(H3N2)v Virus infections, 5 Jan 12, http://www.cdc.gov/flu/swineflu/h3n2v-surveillance.htmCDC, Updated information & guidance documents on A(H3N2)v viruses, 20 Sep 12, Website: http://www.cdc.gov/flu/swineflu/h3n2v-outbreak.htm
• In the USA, a total of 306 cases of swine-origin H3 “variant” influenza viruses since Aug 2011, 294 cases since Jul 12 [all triple reassortant, swine-origin A(H3N2)v strains]
• Largest 2 outbreaks associated with swine fairs in Indiana (138) & Ohio (106) in Jul-Aug 12• Previous to 2011 only < 6 cases per year (increased surveillance since 2007)• These “variant” viruses contain the M gene of pH1N1 virus; easier spread from pigs to people than other variants• Nineteen (6%) of these 306 A(H3N2)v-infected patients were hospitalized (16 in Jul-Sep 12)
– One death in a 61yo female in Ohio with predisposing chronic conditions (visited swine fair)– Swine exposure in cases (or close family contacts) noted in > 90% of cases (direct contact or attendance at an agricultural fair)– Limited Human-to-Human transmission in 3 single family-associated cases in Iowa (Nov 11)– Limited Human-to-Human transmission in 2 DCC-associated cases in West Virginia (Nov 11)– Limited Human-to-Human transmission in three separate family cases (Aug 12)
• Enhanced vigilance for swine-origin strains among exposed populations is needed!!!– ILI outbreaks, particularly among children in DCC & school settings (potential human-to-human transmission)– Unusual number of, or severely-ill ILI cases, especially among children, especially if associated with swine fairs/exposures– Medically-attended ILI & ARI in those pregnant, < 5 yo, > 65 yo or w chronic conditions (high-risk flu-related complication)– Increased sanitation at fairs, avoid eating, drinking & smoking in animal areas; washing hands
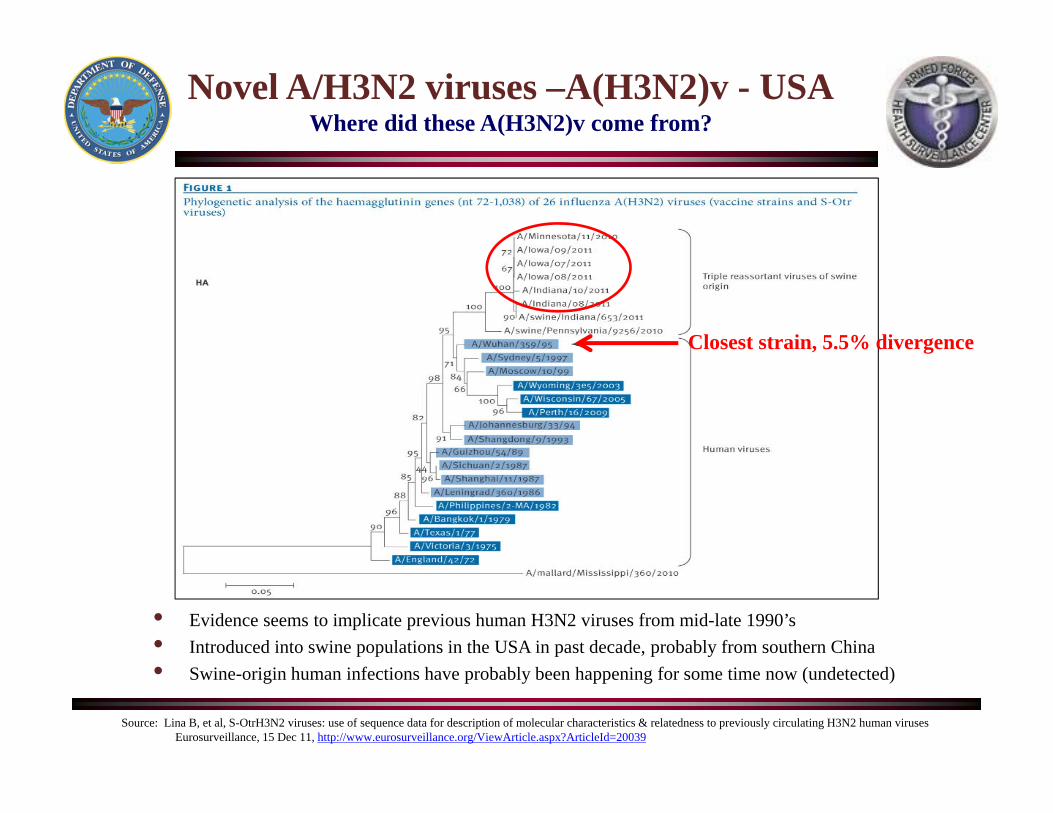
Novel A/H3N2 viruses –A(H3N2)v - USAWhere did these A(H3N2)v come from?
Source: Lina B, et al, S-OtrH3N2 viruses: use of sequence data for description of molecular characteristics & relatedness to previously circulating H3N2 human virusesEurosurveillance, 15 Dec 11, http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20039
• Evidence seems to implicate previous human H3N2 viruses from mid-late 1990’s• Introduced into swine populations in the USA in past decade, probably from southern China• Swine-origin human infections have probably been happening for some time now (undetected)
Closest strain, 5.5% divergence
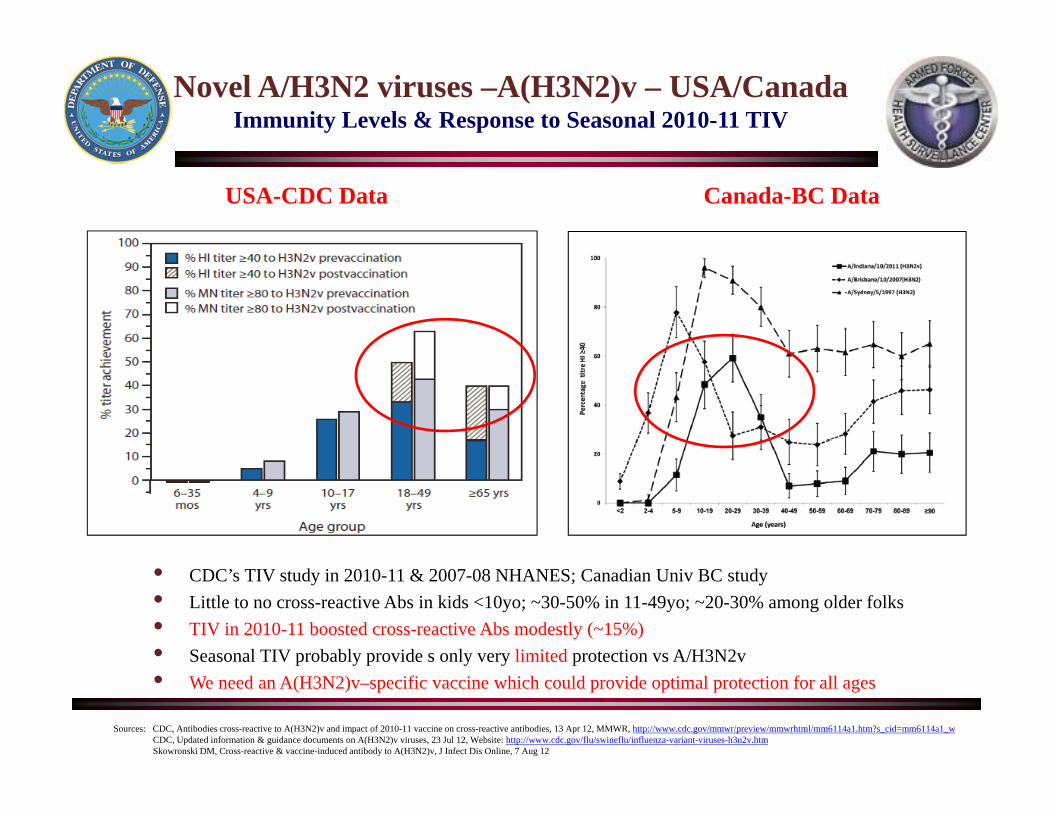
Novel A/H3N2 viruses –A(H3N2)v – USA/CanadaImmunity Levels & Response to Seasonal 2010-11 TIV
• CDC’s TIV study in 2010-11 & 2007-08 NHANES; Canadian Univ BC study• Little to no cross-reactive Abs in kids <10yo; ~30-50% in 11-49yo; ~20-30% among older folks• TIV in 2010-11 boosted cross-reactive Abs modestly (~15%)• Seasonal TIV probably provide s only very limited protection vs A/H3N2v• We need an A(H3N2)v–specific vaccine which could provide optimal protection for all ages
Sources: CDC, Antibodies cross-reactive to A(H3N2)v and impact of 2010-11 vaccine on cross-reactive antibodies, 13 Apr 12, MMWR, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6114a1.htm?s_cid=mm6114a1_wCDC, Updated information & guidance documents on A(H3N2)v viruses, 23 Jul 12, Website: http://www.cdc.gov/flu/swineflu/influenza-variant-viruses-h3n2v.htmSkowronski DM, Cross-reactive & vaccine-induced antibody to A(H3N2)v, J Infect Dis Online, 7 Aug 12
USA-CDC Data Canada-BC Data
New Influenza Vaccine?”New A(H3N2)v Vaccines for Clinical Trials”
Source: CIDRAP, 6 Jan 12, http://www.cidrap.umn.edu/cidrap/content/influenza/general/news/jan0612vaccine-br.html
Influenza VaccinesLimitations
• Efficacy is less than optimal in most population groups– Not optimal (~ 70%) in general population
– Decreased efficacy in the elderly & those < 2 yo
– Less immunogenic in transplant, dialysis, hem/onc & advanced HIV
• Breadth of protection (cross-protection is limited and subtype specific)
– Based on HA and NA now, so relies on antigenic match, need universal type
– Efficacy vs B component is not as good, quadrivalent vaccine? (Yamagata & Victoria)
• Duration of protection is limited (no more than 1 year)
• Egg-based & cell-based production is tricky and lengthy (20-24 months)– Surveillance in real-time, vaccine seed production, optimization of growth
– Reagent production, potency testing, stability, formulation, delivery
• Correlates of protection from infection/disease not well understood
Sources: Adapted from KM Neuzil & A Monto, Vaccine Development: Needs for the Future, IDSA’s Sasonal & Pandemic Flu Mtg, Arlington, VA, 27-28 Jan 11Adapted from Bartlett JG, Medscape Education, Lessons from 2009 H1N1: implications for seasonal influenza management (20 Dec 11), http://www.medscape.org/viewarticle/755067
Influenza & PneumococcusWhat is the Connection?
• Pneumococcal NP carriage increases during influenza season• Increase in pneumococcal pneumonia rates noted in previous pandemics*• CAP studies have documented that concurrent influenza infection appears
to increase risk of pneumococcal pneumonia in kids• RCT of PCV-9 shown to reduce rates of influenza-associated pneumonia
in S African kids by ~ 45%**• Experimental animal models of pneumococcal infection superimposed on
preceding influenza infection results in more severe disease (in mice, ferret & monkey models)***
• Influenza infection in 1918 shown to interact (increase) risk of infection with other bacterial pathogens such as S. aureus & H. influenzae****
Sources: Grijalva CG & Griffin MR, Unveiling the burden of influenza-associated pneumococcal pneumonia, J Infect Dis editorial (1 Feb 12)*Brundage JF, Interactions between influenza and bacterial respiratory pathogens: implications for pandemic preparedness, Lancet Infect Dis 2006; 6:303-12
**Madhi SA, et al, Vaccine Trialist Group, A role for Streptococcus pneumoniae in virus-associated pneumonia, Nat Med 2004; 10:811-3***McCullers JA. Insights into the interaction between influenza virus and pneumococcus, Clin Microbiol Rev 2006; 19:571–82***McCullers JA, et al, Influenza enhances susceptibility to natural acquisition of and disease due to Streptococcus pneumoniae in ferrets, J Infect Dis 2010; 202:1287-95
****Brundage JF & Shanks GD, Deaths from bacterial pneumonia during 1918-19 influenza pandemic, Emerg Infect Dis 2008; 14:1193-9****Chien YW, et al, Bacterial pathogens and death during the 1918 influenza pandemic, NEJM 2009; 361:2582-3
Influenza & PneumococcusPrevention of Pneumococcal Infection-Vaccination!!!
• Two vaccines available:– Use polysaccharide vaccine (PPSV23) in those 2-18 years if at high-risk, booster
dose after 5 years– Use conjugate vaccine (Prevnar –PCV7 till 3 Mar 2010, Prevnar -PCV13 after 3 Mar
2010) in those 6 weeks – 59 months of age (6-71 months if at high-risk)– Use conjugate vaccine (Prevnar -PCV13) in those > 50 yo (30 Dec 2011)– PCV13 - Four-dose basic series at 2, 4, 6 & 12-15 months
• Persons at high-risk who should also be vaccinated include:– People 2 years of age and older who have a chronic illness such as:
• Chronic CVD (including congestive heart failure and cardiomyopathies)• Chronic pulmonary disease (including COPD and emphysema)• Sickle cell disease or diabetes • Alcoholism or chronic liver disease (including cirrhosis)• Cerebrospinal fluid (CSF) leak or Cochlear implant
– People 2 years of age and older with a weakened immune system• HIV infection and AIDS• Chronic renal failure or nephrotic syndrome• Organ or bone marrow transplantation• Malignancies such as Hodgkin’s disease, leukemia, lymphoma or multiple myeloma
– Those receiving immunosuppressive chemotherapy (including corticosteroids)– Asplenic patients or those with dysfunctional spleens due to illness– Residents of nursing homes or long-term care facilities– People 19 to 64 years of age who smoke cigarettes or have asthma
Sources: CDC, Prevention of Pneumococcal Infections 2dary to Seasonal & 2009 H1N1 Influenza, 23 Oct 09 (http://www.cdc.gov/h1n1flu/vaccination/public/public_pneumococcal.htm)CDC Health Advisory, Pneumococcal vaccination recommended to help prevent secondary infections, 16 Nov 09FDA News Release, FDA Approves Pneumococcal Disease Vaccine with Broader Protection, 24 Feb 10 (http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201758.htm)CDC ACIP’s Provisional Recommendations for Use of 13-valent PCV13 in Infants & Children, 3 Mar 10, http://www.cdc.gov/vaccines/recs/provisional/downloads/pcv13-mar-2010-508.pdfCDC ACIP’s Revised Recommendations for Use of PCV13 and PPSV23 vaccines among infants and children, 10 Dec 10, http://www.cdc.gov/mmwr/pdf/rr/rr5911.pdfFDA News Release, FDA expands use of Prevnar 13 vaccine for people ages 50 and older, 30 Dec 11, http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm285431.htm
Questions?

AFHSC’s Website
http://www.afhsc.mil