inges&ón(de(cáus&cos( - endoscopia ucendoscopia.uc.cl/reuniones/reuniones2015/ingestion de...
TRANSCRIPT
Inges&ón de Cáus&cos
Dra. Daniela Ga6ni V. Residente de Gastroenterología y Nutrición Pediátrica

Obje&vos
• Describir la epidemiología, fisiopatología y presentación clínica de la ingesta de cáus&cos en pediatría.
• Caracterizar el uso de la Endoscopía Diges&va Alta en pacientes que consultan por ingesta de cáus&cos.
• Revisar el manejo del paciente con ingesta de cáus&cos.

Introducción
• Se define cáus&co a toda sustancia química que es capaz de producir daño por acción directa sobre la piel y mucosas.
• Existen valores de pH que se consideran crí&cos para producir daño por cáus&cos.
• La exposición de la mucosa del tracto diges&vo a los extremos del pH puede producir quemaduras de diferentes grados.
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Introducción public health issue in Western countries despite education and regulatory efforts to reduce its occurrence. These in-juries are still increasing in developing countries[1,2], relat-ed to the social, economic, and educational variables and mainly to a lack of prevention[3,4]. The problem is largely unreported in these settings and its true prevalence sim-ply cannot be extrapolated from the scarce papers or personal experience. Data available are heavily skewed towards well-resourced centers and do not mirror the full reality of the condition. Moreover, in industrialized and developing countries, the therapeutic approach and man-agement strategies appear to be different, likely because of technology and endoscopic expertise.
Two independent MEDLINE and EMBASE searches from 1990-2012 were performed to identify relevant ar-ticles. The following medical subject headings terms were used in the searches: caustic ingestion, caustic lesions, corrosive injuries, esophagus, esophageal dilatation. Bibli-ographies of retrieved studies were reviewed and general medical and major gastroenterology journals manually searched over the previous 5 years.
!"#$!%#&'&()*+,$*"+-.&".)/#&'&()Worldwide, children represent 80% of the ingestion injury population globally[5], primarily due to accidental ingestion[6]. In contrast, ingestion in adults is more often suicidal in intent, and is frequently life-threatening.
Traditionally, ingested corrosive substances are either alkalis or acids (Table 1). Alkaline material accounts for most caustic ingestions in Western countries whereas injuries from acid are more common in some developing countries, like India, where hydrochloric acid and sulfuric acid are easily accessible[7]. Acids and alkalis produce dif-ferent types of tissue damage. Acids cause coagulation necrosis, with eschar formation that may limit substance penetration and injury depth[8]. Conversely, alkalis com-bine with tissue proteins and cause liquefactive necrosis and saponification, and penetrate deeper into tissues, helped by a higher viscosity and a longer contact time through the esophagus. Additionally, alkali absorption leads to thrombosis in blood vessels, impeding blood flow to already damaged tissue[9]. Injury occurs quickly, depending on the agent’s concentration and time of exposure (Figure 1)[10], with a 30% solution of sodium hydroxide being able to produce full thickness injury in 1 s[11]. Accordingly, alkali ingestion may lead to more serious injury and complications, but this distinction is probably not clinically relevant in the setting of strong acid or base ingestion, both being able to penetrate tis-sues rapidly, potentially leading to full-thickness damage of the esophageal/gastric wall. The conventional accep-tance that acids preferentially damage the stomach, due to the protective esophageal eschar, has recently been questioned, with observation of extensive esophageal damage and perforations after acid ingestion[12]. Likewise, compared with alkali, ingestion of a strong acid may be
associated with a higher incidence of systemic complica-tions, such as renal failure, liver dysfunction, disseminated intravascular coagulation and hemolysis[13].
Esophageal injury begins within minutes and may persist for hours. Initially, tissue injury is marked by eo-sinophilic necrosis with swelling and hemorrhagic con-gestion[9]. Experimental findings suggest that arteriolar and venular thrombosis with consequent ischemia may be more important than inflammation in the pathogenesis of acute corrosive injury[10]. Four to 7 d after ingestion, mucosal sloughing and bacterial invasion are the main findings. At this time granulation tissue appears, and
during this period if ulceration exceeds the muscle plane. Fibroblasts appear at the injury site around day 4, and around day 5, an “esophageal mold’’ is formed, consisting of dead cells and secretions. Esophageal repair usually begins on the 10th day after ingestion, whereas esophageal ulcerations begin to epithelialize approximately 1 mo af-ter exposure. The tensile strength of the healing tissue is
not begin until the second week. Hence, endoscopy (and of course dilatation) is preferably avoided 5-15 d after ingestion[14]. Scar retraction begins by the third week and may continue for several months, resulting in stricture formation and shortening of the involved segment of the gastrointestinal tract. Additionally, lower esopha-geal sphincter pressure becomes impaired, leading to
accelerates stricture formation[15]
to sequential esophageal dilatations. Esophageal motility studies report low amplitude and nonperistaltic contrac-
compared with control groups[16]. Therefore, all caustic
3919 July 7, 2013|Volume 19|Issue 25|WJG|www.wjgnet.com
Contini S et al . Upper gastrointestinal caustic lesions
!!"#$%&'(!%$)%&#*(+ !!!!!!,-.+ "/00+1('#22-!#3#'2#)2+!4/10
Acids Sulfuric BatteriesIndustrial cleaning agentsMetal plating
Oxalic Paint thinners, strippersMetal cleaners
Hydrochloric SolventsMetal cleanersToilet and drain cleanersAntirust compounds
Phosphoric Toilet cleaners Alkali Sodium hydroxide Drain cleaners
Home soap manufacturingPotassium hydroxide Oven cleaners
Washing powdersSodium carbonate Soap manufacturing
Fruit drying on farms Ammonia Commercial ammonia Household cleaners Ammonium hydroxide Household cleaners Detergents, bleach Sodium hypochlorite Household bleach, cleaners
Sodium polyphosphate Industrial detergents Condy’s crystals Potassium permanganate Disinfectants, hair dyes
,#)2+!5!!6/%&!(/00/*2-!'*7+%&+8!(#$%&'(!%$)%&#*(+%
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Epidemiología
• Ingresos a Servicio de Urgencia desde 0,22% hasta 4,5%, y un 9,2% corresponde a sustancias de limpieza en el hogar.
• En pediatría, 80% de las intoxicaciones son accidentales, afectando en un 58% a menores de 6 años (38,7% < 3 años).
• 1,5 veces más frecuente en hombres, excepto adolescentes.
• La mortalidad fluctúa entre 1% y 4%.
Moreno C. Vox Pediatrica. 2002;10:51-‐55. Bronstein AC. Clin Toxicol (Phila). 2012;50:911-‐1164.
Epidemiología
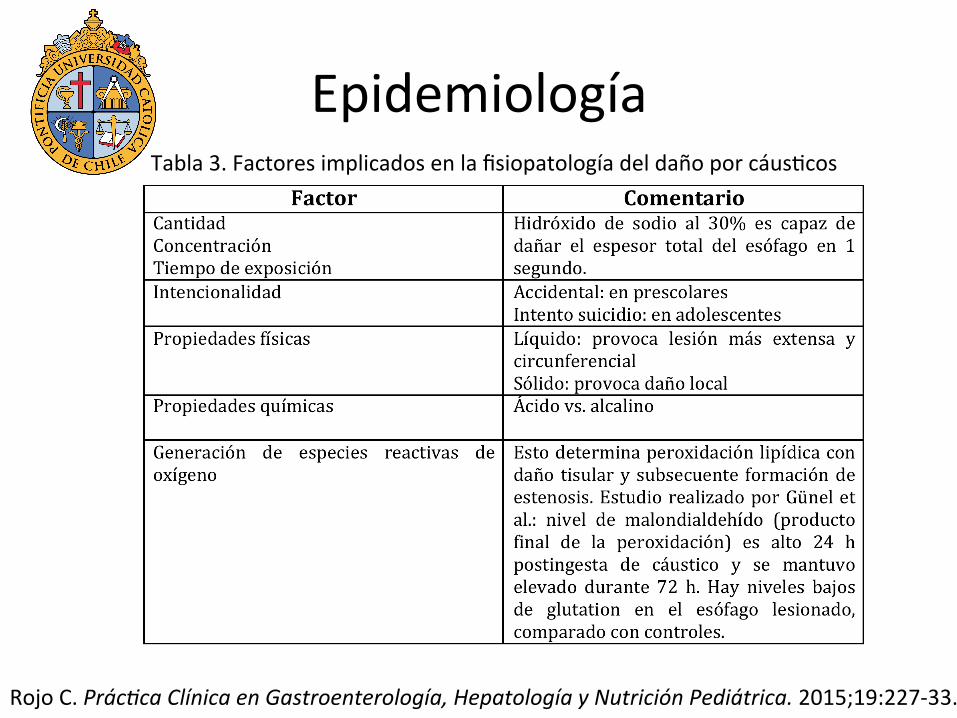
Rojo C. Prác:ca Clínica en Gastroenterología, Hepatología y Nutrición Pediátrica. 2015;19:227-‐33.
Tabla 3. Factores implicados en la fisiopatología del daño por cáus&cos
Fisiopatología Primera fase (día 1 al 3): • Necrosis con saponificación, trombosis vascular e intensa
reacción inflamatoria. • Debe efectuarse el diagnós&co. • Iniciar las medidas terapéu&cas.
Segunda fase (día 3 al 5): • Ulceración. • Desprendimiento de la mucosa e invasión microbiana. • Perforación.
Salzman M, O´Mally R. Emerg Med Clin N Am. 2007;25:459-‐479. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Fisiopatología Tercera fase (día 6 al 14): • Fenómenos reparadores, aparición de tejido de granulación. • Pared es muy débil (evitar manipulación).
Cuarta fase (día 15 al 30; hasta el día 45): • Consolidación de cicatrización. • Estenosis esofágica. • Indicación de dilataciones.
Salzman M, O´Mally R. Emerg Med Clin N Am. 2007;25:459-‐479. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

cias ácidas pueden producir lesión esofágica con pHinferior a 4 (Fig. 1).
Los ácidos producen una necrosis por coagulaciónproteica, con pérdida de agua, formándose una esca-ra firme y protectora que dificulta en parte la penetra-ción, salvo en concentraciones elevadas.
Los álcalis provocan una necrosis por licuefac-ción, con desnaturalización de las proteínas, saponi-ficación de las grasas y trombosis capilares. La reten-ción de agua que provoca aumenta la quemadura porhidratación. Estas reacciones favorecen la profundi-zación de las lesiones.
Es más frecuente que los ácidos se relacionen conlesiones gástricas que los álcalis, pero en la realidadlos álcalis también originan severas lesiones gástri-cas, ya que con el espasmo pilórico asociado retienenla sustancia cáustica en la cavidad gástrica incre-mentándose la lesión.
Distinguimos 4 fases evolutivas: – 1ª fase. Del 1º al 3er día; es cuando se produce
la necrosis con saponificación, trombosis vascu-lar e intensa reacción inflamatoria. Por eso en esta
fase debe efectuarse el diagnóstico, sentar el pro-nóstico e iniciar las medidas terapéuticas.
– 2ª fase. Del 3er al 5º día; está caracterizada por laulceración.
– 3ª fase. Del 6º al 14º día; se inician los fenómenosreparadores; el edema inflamatorio es sustituidopor tejido de granulación. En este momento lapared es muy débil y no debe ser manipulada paraevitar complicaciones
– 4ª fase. Del 15º al 30º día; aunque puede prolon-garse hasta el 45º día; se va consolidando la cica-trización y es aquí cuando se establece la esteno-sis esofágica y cuando estaría indicado el iniciode las dilataciones. Cuanto más grave es la que-madura, antes aparece la estenosis.
SINTOMATOLOGÍALa clínica es enormemente variable, desde moles-
tias orofaríngeas banales hasta el shock y la perfora-ción temprana.
La ingestión del cáustico suele dar lugar a undolor local inmediato y odinofagia. Con frecuencia
122 Protocolos diagnóstico-terapéuticos de Gastroenterología, Hepatología y Nutrición Pediátrica SEGHNP-AEP
Licuefacción tisular
Saponificacióngrasas
Desnaturalizaciónproteínas
Coagulación proteica
Pérdida de agua
Escara mucosa
Menor poder de penetración
Trombosiscapilar
Retención agua
Gran poder de penetración
ÁlcaliÁcido
4 7 12
Quemadura térmica por hidratación
FIGURA 1.
Fisiopatología
Bau&sta et al. Protocolos AEPED. 2010. doi:10.1016/j.anpedi.2011.03.024
Valores de pH crí$cos: pH>12 pH < 4
Perforación Lesiones gástricas

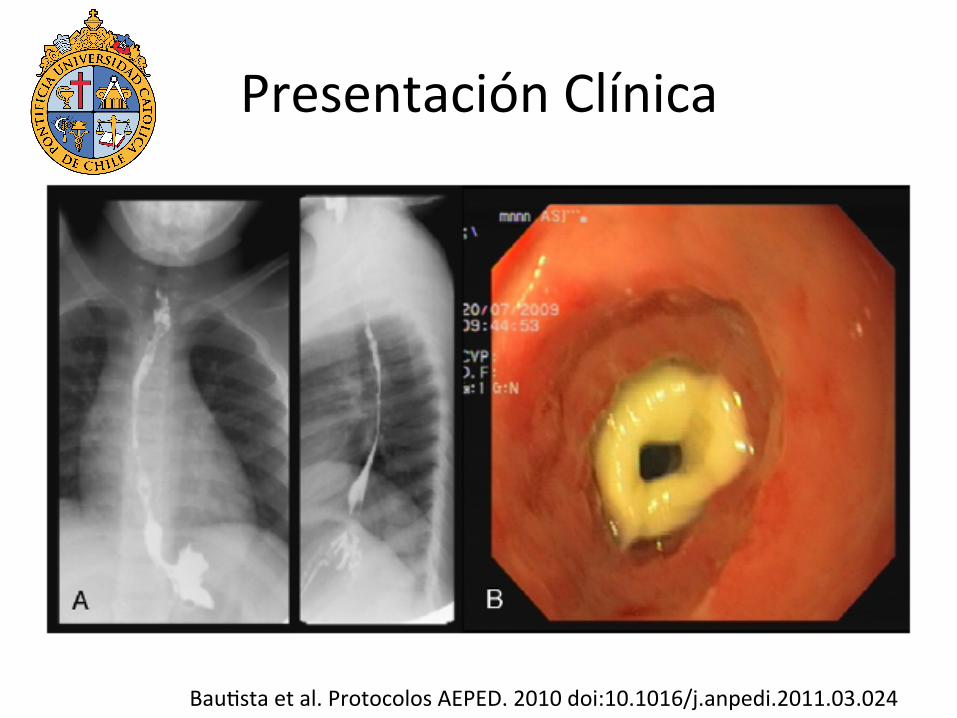
Presentación Clínica Fase Aguda: • Dolor local inmediato y odinofagia. • Vómitos y náuseas inmediatas a la inges&ón. • Edema y úlceras en mucosa oral. • Pueden presentar disnea, sialorrea, estridor. • Epigastralgia y hematemesis (gástrico). • Forma de presentación grave (perforación temprana) à dolor
torácico, enfisema subcutáneo, sepsis, shock.
Bau&sta et al. Protocolos AEPED. 2010. doi:10.1016/j.anpedi.2011.03.024

Presentación Clínica Complicaciones tempranas: • Neumonía • Medias&ni&s • Peritoni&s • Abscesos pulmonares • Sepsis Síntomas agudos remiten en 2 a 3 días si no hay perforación • Regularización de la deglución
Bau&sta et al. Protocolos AEPED. 2010. doi:10.1016/j.anpedi.2011.03.024
Presentación Clínica
Fase Latente (2ª-‐3ª sem): • Síntomas en regresión. • Riesgo de perforación. • Dolor de aparición brusca. • Más frecuente entre 5º a 15º día. • Epigastralgia y hematemesis en compromiso gástrico. • Se ha descrito hematemesis severa hasta 2 semanas posterior
a ingesta.
Bau&sta et al. Protocolos AEPED. 2010. doi:10.1016/j.anpedi.2011.03.024

Presentación Clínica
Fase Crónica o de Secuelas: • Disfagia por estenosis esofágica. • 80% se desarrollan en los 2 meses posteriores. • Saciedad precoz, vómitos, baja de peso por síndrome pilórico
y obstrucción gástrica. • Riesgo carcinoma esofágico 1000-‐3000 veces mayor que
población general. • Vigilancia con EDA de por vida.
Bau&sta et al. Protocolos AEPED. 2010. doi:10.1016/j.anpedi.2011.03.024
Presentación Clínica
Bau&sta et al. Protocolos AEPED. 2010 doi:10.1016/j.anpedi.2011.03.024
Presentación Clínica
Expert Rev. Gastroenterol. Hepatol. 5(5), (2011)642
Review
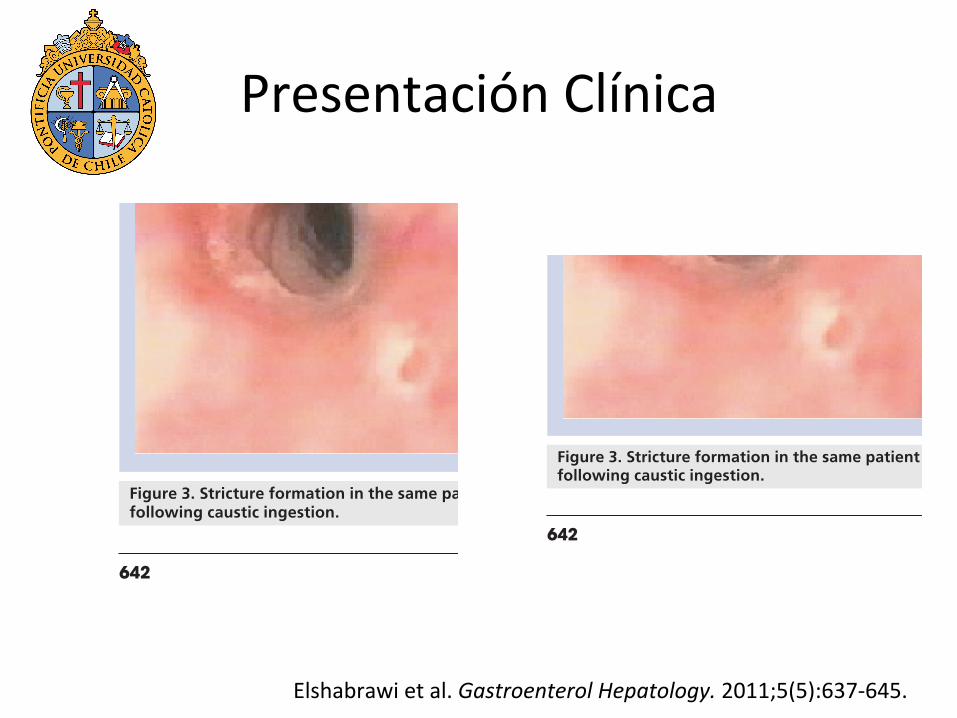
may reach 100% in patients with grade III [48]. A ninefold increase in morbidity and mortality has been associated with each increased injury grade [12]. Stricture formation can occur as early as 3 weeks following ingestion and is usually established in 80% of the patients who ultimately will develop stricture by 8 weeks [49].
Once strictures develop most patients will require repeated dilatations. A variety of methods can be used to dilate the esophagus including mercury-filled bougies, Maloney antegrade
dilators or Tucker dilators used in retrograde dilatation and dila-tors passed over a guide wire or pulled through with a string left in situ between dilatations. Balloon dilatation under endo-scopic control has been used successfully to treat children with caustic stricture (FIGURE 4) [50]. This technique is considered safe as it avoids the shearing longitudinal force exercised by other dilatation techniques. In some stable cases the patients may be trained to dilate their esophagus at home eliminating the need for hospitalization. Although retrograde dilatation is the saf-est method it requires gastrostomy and string guidance. Some investigators have advocated the injection of steroids into the stricture to decrease the number of dilatation sessions needed for stricture resolution [51]. A promising strategy is the local appli-cation of mitomycin C (an inhibitor of fibroblast proliferation) post-dilatation which has been reported to successfully reduce the need for dilatation [52]. However, clinical trials are needed to validate its efficacy.
Unfortunately, in some patients, surgical intervention is needed. Extensive necrosis noted on endoscopy and patients with evidence of perforation are indications for immediate sur-gical intervention. Exploratory thoracotomy and/or laparotomy may be needed if there is strong suspicion of full thickness injury with wide spread necrosis. Esophagectomy, esophago-gastrectomy or gastrectomy may be indicated if wide necrosis is confirmed. Surgical intervention is also warranted in patients with long and tight strictures. Esophageal reconstruction may be achieved by small bowel or colon interposition and gastric transposition. The two main methods are retrosternal and posterior mediastinal. Thoraciscopic as well as laparoscopic techniques have been described [53]. Esophageal replacement should not be conducted within 6 months after conservative therapy [54]. Gastric tube formation should be conducted only in the absence of gastric lesion. However, it is recommended that all efforts be exhausted in order to keep the native esophagus. Although colon interposition can be successful, patients may continue to have dysphagia due to motility issues in addition to anastomotic strictures and gastrocolic ulceration and secondary reflux [55,56]. Coopman et al. evaluated the long-term nutritional, digestive and respiratory outcome of 32 patients who underwent colon interposition during childhood. Complications occurred less than 1 year postoperatively in 53% and long-term compli-cations occurred in 84%. Long-term complications included digestive symptoms in 85% (most frequently observed during the first 5 years of follow-up), abnormal lung function in 58% of those tested, feeding difficulties in 50%, scoliosis in 35% and nutritional complications in 25% [57]. Raboei and Luoma reported encouraging results regarding the successful use of colon patch esophagoplasty as an alternative to total esophagus replacement [58].
Pyloric stenosis and gastric outlet obstruction may follow both alkali and acid ingestion [59]. Although balloon dilatation has been successfully used in a child with caustic ingestion and pyloric stenosis [60] surgical bypass may be necessary. Y-V advancement antro-pyloroplasty has been described as a corrective surgery for corrosive antral strictures [61].
Figure 3. Stricture formation in the same patient 24 days following caustic ingestion.
Figure 2. Third-degree esophagitis following caustic ingestion.
Elshabrawi & A-Kader
Expert Rev. Gastroenterol. Hepatol. 5(5), (2011)642
Review
may reach 100% in patients with grade III [48]. A ninefold increase in morbidity and mortality has been associated with each increased injury grade [12]. Stricture formation can occur as early as 3 weeks following ingestion and is usually established in 80% of the patients who ultimately will develop stricture by 8 weeks [49].
Once strictures develop most patients will require repeated dilatations. A variety of methods can be used to dilate the esophagus including mercury-filled bougies, Maloney antegrade
dilators or Tucker dilators used in retrograde dilatation and dila-tors passed over a guide wire or pulled through with a string left in situ between dilatations. Balloon dilatation under endo-scopic control has been used successfully to treat children with caustic stricture (FIGURE 4) [50]. This technique is considered safe as it avoids the shearing longitudinal force exercised by other dilatation techniques. In some stable cases the patients may be trained to dilate their esophagus at home eliminating the need for hospitalization. Although retrograde dilatation is the saf-est method it requires gastrostomy and string guidance. Some investigators have advocated the injection of steroids into the stricture to decrease the number of dilatation sessions needed for stricture resolution [51]. A promising strategy is the local appli-cation of mitomycin C (an inhibitor of fibroblast proliferation) post-dilatation which has been reported to successfully reduce the need for dilatation [52]. However, clinical trials are needed to validate its efficacy.
Unfortunately, in some patients, surgical intervention is needed. Extensive necrosis noted on endoscopy and patients with evidence of perforation are indications for immediate sur-gical intervention. Exploratory thoracotomy and/or laparotomy may be needed if there is strong suspicion of full thickness injury with wide spread necrosis. Esophagectomy, esophago-gastrectomy or gastrectomy may be indicated if wide necrosis is confirmed. Surgical intervention is also warranted in patients with long and tight strictures. Esophageal reconstruction may be achieved by small bowel or colon interposition and gastric transposition. The two main methods are retrosternal and posterior mediastinal. Thoraciscopic as well as laparoscopic techniques have been described [53]. Esophageal replacement should not be conducted within 6 months after conservative therapy [54]. Gastric tube formation should be conducted only in the absence of gastric lesion. However, it is recommended that all efforts be exhausted in order to keep the native esophagus. Although colon interposition can be successful, patients may continue to have dysphagia due to motility issues in addition to anastomotic strictures and gastrocolic ulceration and secondary reflux [55,56]. Coopman et al. evaluated the long-term nutritional, digestive and respiratory outcome of 32 patients who underwent colon interposition during childhood. Complications occurred less than 1 year postoperatively in 53% and long-term compli-cations occurred in 84%. Long-term complications included digestive symptoms in 85% (most frequently observed during the first 5 years of follow-up), abnormal lung function in 58% of those tested, feeding difficulties in 50%, scoliosis in 35% and nutritional complications in 25% [57]. Raboei and Luoma reported encouraging results regarding the successful use of colon patch esophagoplasty as an alternative to total esophagus replacement [58].
Pyloric stenosis and gastric outlet obstruction may follow both alkali and acid ingestion [59]. Although balloon dilatation has been successfully used in a child with caustic ingestion and pyloric stenosis [60] surgical bypass may be necessary. Y-V advancement antro-pyloroplasty has been described as a corrective surgery for corrosive antral strictures [61].
Figure 3. Stricture formation in the same patient 24 days following caustic ingestion.
Figure 2. Third-degree esophagitis following caustic ingestion.
Elshabrawi & A-Kader
Elshabrawi et al. Gastroenterol Hepatology. 2011;5(5):637-‐645.

Presentación Clínica
• Estudios han correlacionado síntomas y signos con gravedad de la lesión esofágica con resultados contradictorios.
• Un 12% de pacientes con lesiones esofágicas graves eran asintomá&cos; un 82% de los sintomá&cos no tenían lesiones.
• Tras una ingesta de álcalis, 61% de pacientes sin lesiones en cavidad oral tenían quemaduras esofágicas.
Marsha K, Wyllie R. Curr Opin Pediatr. 2009;21651-‐654. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
Presentación Clínica
• La incidencia de injuria esofágica coexistente con injuria gástrica varía en la literatura desde 20% a 62,5%.
• Los álcalis causan lesiones de color amarillo-‐café, mientras que los ácidos pueden ocasionar úlceras blanco-‐grisáceas.
• Lesiones orofaríngeas muestran edema de los labios, lengua de aspecto depapilada, eritema, membranas y úlceras.
. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
Endoscopía Diges&va Alta
• No hay estudios controlados que comparen la efec&vidad de la EDA precoz versus tardía.
• Puede esperarse entre 6 a 12 horas para estabilizar paciente.
• Se recomienda en las primeras 12-‐48 posterior a ingesta, podría ser segura hasta 96 horas después.
• El grado de lesión esofágica determinado por endoscopía es un predictor de morbimortalidad.
Elshabrawi M, A-‐Kader H. Gastroenterol Hepatology. 2011;5(5):637-‐645. Ananthakrishnan N, et al. Gastroenterology. 2011:914013. doi:10.5402/2011/914013.

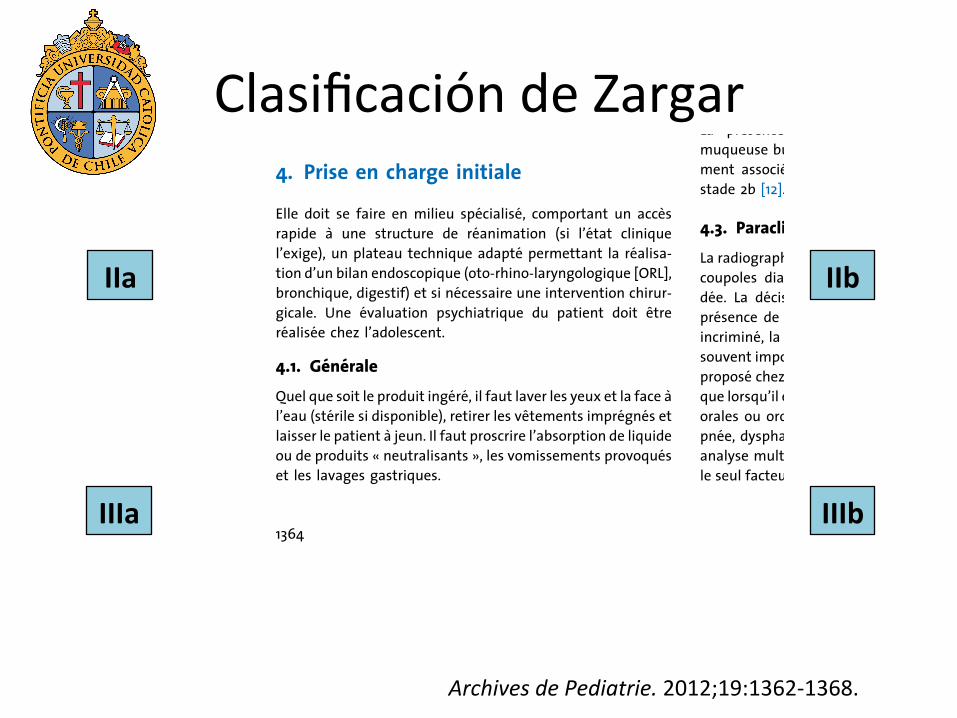
Clasificación de Zargar
Zargar SA, Kochhar R, Mehta S, et al. Gastrointest. Endos. 1991;37:165-‐169.
Clasificación de Zargar
24 % des patients avec une frequence croissante selon lestade lesionnel : 3,6 % au stade 2a ; 14,5 % au stade 2b ; 28,2 %au stade 3a et 53,7 % au stade 3b [11]. Le stade lesionnel 3b etaitassocie a une duree d’hospitalisation plus longue, a l’admis-sion en unite de soins intensifs, a la survenue de stenoses etde complications systemiques (pneumopathies, detresse res-piratoire).
4. Prise en charge initialeElle doit se faire en milieu specialise, comportant un accesrapide a une structure de reanimation (si l’etat cliniquel’exige), un plateau technique adapte permettant la realisa-tion d’un bilan endoscopique (oto-rhino-laryngologique [ORL],bronchique, digestif) et si necessaire une intervention chirur-gicale. Une evaluation psychiatrique du patient doit etrerealisee chez l’adolescent.
4.1. GeneraleQuel que soit le produit ingere, il faut laver les yeux et la face al’eau (sterile si disponible), retirer les vetements impregnes etlaisser le patient a jeun. Il faut proscrire l’absorption de liquideou de produits « neutralisants », les vomissements provoqueset les lavages gastriques.
Il est important de recueillir un echantillon ou le flacond’emballage du produit en cause afin d’en preciser la compo-sition et le pH (avec une bandelette s’il n’est pas connu) avecl’aide du centre antipoison le plus proche.
4.2. CliniqueLa presence d’une hypersialorrhee, de brulures de lamuqueuse buccale et d’une hyperleucocytose est habituelle-ment associee a des lesions œsogastriques superieures austade 2b [12].
4.3. ParacliniqueLa radiographie de thorax de face avec un cliche centre sur lescoupoles diaphragmatiques est systematiquement deman-dee. La decision d’un examen endoscopique repose sur lapresence de signes cliniques et sur la causticite du produitincrimine, la quantite ingeree accidentellement etant le plussouvent impossible a determiner. Plusieurs auteurs [13–15] ontpropose chez l’enfant de ne realiser une endoscopie digestiveque lorsqu’il existait des signes cliniques, soit mineurs (lesionsorales ou oropharyngees, vomissements), soit majeurs (dys-pnee, dysphagie, hypersialorrhee, hematemese). En effet, enanalyse multivariee, la presence de symptomes cliniques estle seul facteur predictif de lesions severes de l’œsophage [15].
E. Mas et al. Archives de Pediatrie 2012;19:1362-1368
Figure 1. Aspects endoscopiques des œsophagites caustiques, selon la classification de Zargar : a : stade 2a ; b : stade 2b ; c et d : stade 3b.
1364
IIa
IIIb
IIb
IIIa
Archives de Pediatrie. 2012;19:1362-‐1368.
Endoscopía Diges&va Alta
• Se recomienda realizar procedimiento con cuidado e insuflar poco.
• Uso adecuado de sedación y anestesia en niños.
• Estudios recientes han demostrado endoscopías en periodo de 5-‐15 días post-‐ingesta, incluso dilataciones, sin consecuencias, aunque recomiendan evaluar caso a caso.
• Es posible completar EDA en presencia de quemaduras grado II y III, con cautela.
Elshabrawi M, A-‐Kader H. Gastroenterol Hepatology. 2011;5(5):637-‐645. Ananthakrishnan N, et al. Gastroenterology. 2011:914013. doi:10.5402/2011/914013.

Betalli et al. Gastrointest Endosc. 2008;68:434-‐439.
Obje:vo: • Evaluar si en niños con ingesta accidental de cáus&co es
siempre necesario realizar una Endoscopía Diges&va Alta. • Evaluar si síntomas iniciales son predictores de lesiones
esofágicas graves.

Betalli et al. Gastrointest Endosc. 2008;68:434-‐439.
Materiales y Métodos: • Estudio mul&céntrico observacional en Italia. • Enero 2005 a enero 2007. • 162 niños < 15 años con ingesta accidental de cáus&co con pH
< 2 o >12, concentración > 5%. • EDA 12-‐24 hrs post inges&ón.

Betalli et al. Gastrointest Endosc. 2008;68:434-‐439.
Betalli et al. Gastrointest Endosc. 2008;68:434-‐439.
accidental caustic substance ingestion should not undergoan endoscopy. Christensen15 published a retrospectivestudy on 115 children with caustic substance ingestionand concluded that an endoscopy is unnecessary inasymptomatic children but is warranted in symptomaticchildren.
Gupta et al1 showed that all patients with clinicallysignificant (second-degree and third-degree) injury weresymptomatic at initial assessment and that asymptomaticpatients with alleged unintentional caustic substance inges-tion do not necessarily have to undergo an esophagoscopy.
In an editorial in the Journal of Pediatric Gastroenter-ology and Nutrition, Kay and Wyllie16 claim that the pub-lished literature on the management of caustic substanceingestion is still limited and confusing. They recommendavoiding an endoscopy in a patient with a dubious caseof ingestion if the patient is asymptomatic and has nooropharyngeal burns; this recommendation is based onclinical experience and the acknowledgement that mostchildren have no real esophageal damage after an episodeof suspected caustic substance ingestion.
In subsequent years, all the published articles on largepediatric series17-19 focused their attention on the man-agement of complications, so the role of an endoscopyin asymptomatic or scarcely symptomatic patients hasremained unclear.
Early positive EGDs distinguish patients who requirehospital management from those without burns who needno therapy. Although the risk of injury is low, an EGD in chil-dren always demands sedation in the operating room andcarries a percentage of iatrogenic injury.20 A study by Thak-kar et al21 suggests that an immediate complication rate ofpediatric upper endoscopy is approximately 2.3%, which ishigher than reported in the adult literature. Among compli-cations, 65.7% were because of reversible hypoxia, likely re-lated to sedation; GI bleeding was the second mostcommon complication reported (11.7%). No perforationsor deaths were reported in 10,236 procedures.
The results of the present study demonstrated that theincidence of patients with third-degree lesions without
any early signs and symptoms was very low, and theendoscopy could be avoided. Because most ingestionsare not witnessed by an adult, one could consider the in-formation reported as only partially reliable. Besides,some parents will not be as precise in observing and re-porting signs and symptoms after the event. Nevertheless,the correspondence found in our study between reportedsigns and symptoms and esophageal injury suggests thatsuch inquiry is reasonably trustworthy. However 2 of 19patients with third-degree esophageal lesions were asymp-tomatic and, according to our recommendation, wouldnot have had an endoscopy. The point is to weigh the ben-efits of avoiding EGDs in most asymptomatic patients withno injury against the risks of missing a major treatment forthe outcome in a few asymptomatic cases with third-degree lesions. When considering costs and benefits ofendoscopy, we believe that, for the time being, ourrecommendation is reasonable.
We would like to introduce the concept of ‘‘accidental-deliberate’’ ingestion to describe the cases of ingestionbecause of the presence of a caustic substance in a normalbeverage container. Most of these cases of ingestion occurin older children who deliberately drink a large amount ofthe substance, which is accidentally a caustic one. Our 2asymptomatic patients with severe esophageal lesionswere a boy and a girl between 25 and 36 months of age,and were both cases of ‘‘accidental-deliberate’’ ingestion,ie, they had deliberately drunk a large amount of thecontents of a normal beverage container unaware that itcontained a caustic substance (most of such cases of inges-tion occur in older children). Both asymptomatic childrenpresented grade IIIa lesions of the esophagus but did notdevelop esophageal stenosis, as confirmed by a bariumswallow performed 20 days after ingestion and by anendoscopy carried out 1 month after the ingestion.
We speculate that this kind of ingestion episode is moredangerous, because a larger quantity of liquid is ingested,because the child believes the fluid is a normal beverage.An endoscopy, therefore, might be considered mandatoryfor asymptomatic patients who present with a history of‘‘accidental-deliberate’’ caustic substance ingestion.
The risk of severe damage to the esophagus increasesproportionally with the number of the patient signs andsymptoms. The presence of only ‘‘minor’’ symptoms,such as oropharyngeal lesions and vomiting, does notrule out any presence of relevant injuries to the esopha-gus, although important symptoms, such as hematemesis,dyspnea, and stridor, are naturally the most obvious pre-dictors of the presence of severe lesions. An endoscopyis warranted in all symptomatic children.
DISCLOSURE
The authors report that there are no disclosures rele-vant to this publication.
TABLE 4. Multivariate analysis with 3rd-degree lesionsas the dependent variable
CharacteristicsAdjusted
OR95% CI adjusted
ORP
value
Women vs men 1.276 0.40-3.97 .674
Substance(alkali vs acid)
1.791 0.35-9.08 .482
Age(continuousvariable) (mo)
1.015 1.002-1.023 .026
Symptoms(no vs yes)
2.308 1.57-3.38 .001
438 GASTROINTESTINAL ENDOSCOPY Volume 68, No. 3 : 2008 www.giejournal.org
Caustic ingestion in children Betalli et al
Betalli et al. Gastrointest Endosc. 2008;68:434-‐439.
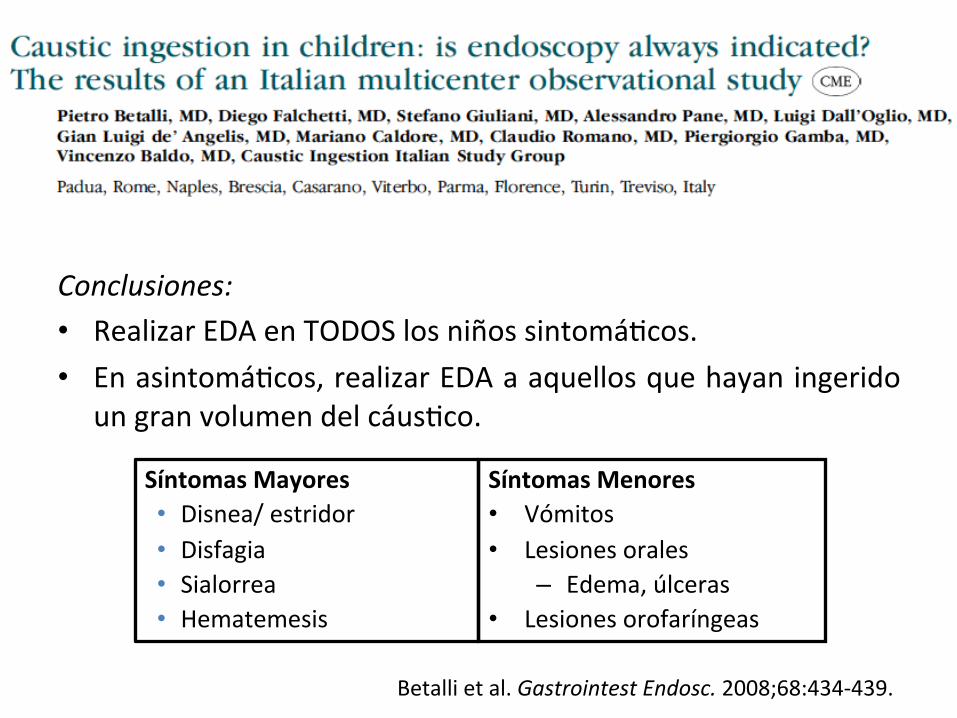
Conclusiones: • Realizar EDA en TODOS los niños sintomá&cos. • En asintomá&cos, realizar EDA a aquellos que hayan ingerido
un gran volumen del cáus&co.
Síntomas Mayores • Disnea/ estridor • Disfagia • Sialorrea • Hematemesis
Síntomas Menores • Vómitos • Lesiones orales
– Edema, úlceras • Lesiones orofaríngeas

Contraindicaciones EDA
• Sospecha clínica o radiológica de perforación.
• Quemaduras supragló&cas o epigló&cas con edema (sugiere obstrucción de vías respiratorias).
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Estudios de Imágenes
Tabla 5. Estudios Imagenológicos.
Rojo C. Prác:ca Clínica en Gastroenterología, Hepatología y Nutrición Pediátrica. 2015;19:227-‐33.
TAC
3921 July 7, 2013|Volume 19|Issue 25|WJG|www.wjgnet.com
EndoscopyEsophagogastroduodenoscopy is considered crucial and
-gestion, though it is safe and reliable up to 96 h after the injury[13,42] -datory during the procedure. Endoscopy and even dilata-tion have been performed without consequences from 5 to 15 d after corrosive ingestion[43], though potentially hazardous due to tissue softening and friability during the healing period. Adequate sedation (general anesthesia in children) is compulsory, yet endotracheal intubation is strictly required only for patients in respiratory distress. The constraint to stop the endoscope in the presence of a circumferential second or third degree esophageal burn is not mandatory[44,45].
When lip and oropharyngeal injuries are the main -
ly no greater than grade 1[46]. Although severe esophageal injuries have been reported in 12.0%[47] and 19.3%[48] of asymptomatic children, significant lesions at endoscopy are not usually observed when symptoms are absent after unintentional ingestion of less aggressive substances[24,49], thus making routine post-ingestion endoscopy question-able in this group of patients. All adult patients must undergo endoscopy after suicidal ingestion, because of the larger amount of more corrosive agents swallowed compared with unintentional injuries, where early esoph-agoscopy has been questioned[50]. Ultimately, though endoscopy is considered by most a cornerstone in the diagnosis of corrosive ingestions, which patients would clearly benefit from it is still debated. Considering that 10%-30% of caustic ingestions globally do not show any upper gastrointestinal injury[22,51], the indication for early endoscopy should be made on a case-by-case basis, with consideration of symptoms, otorhinolaryngeal injuries, and the amount and nature of the ingested substance.
Contraindications to endoscopy are a radiologic sus-picion of perforation or supraglottic or epiglottic burns with edema, which may be a harbinger of airway obstruc-tion, therefore indicating endotracheal intubation or tra-cheostomy. A third degree burn of the hypopharynx is a further contraindication for endoscopy[22].
[8] is important for prognosis -
and of emergency surgery[33]. Essentially, laboratory stud-ies are more useful in monitoring and guiding patient management than in predicting morbidity or mortality[34].
Traditional radiologyShortly after ingestion, a plain chest radiograph may reveal air in the mediastinum suggesting esophageal per-foration, as well as free air under the diaphragm, indicat-
a clinically suspected perforation, a water-soluble agent,
than barium sulphate, should probably be used, though both can be equally irritant[35]. Conversely, barium sulfate should be the preferred contrast agent in late barium swallowing, providing greater radiographic details than water-soluble contrast agents[22].
UltrasoundsEvaluation of esophageal wall caustic damage by endo-scopic ultrasound (EUS) using a miniprobe seems safe, though prolongs examination time without showing any difference with endoscopy in predicting early complica-tions[36]. The destruction of the muscular layers of the esophagus observed at EUS seems a reliable sign of future stricture formation[37]; furthermore, ultrasound examination with a radial probe may predict the response to dilatation, which usually requires more sessions when the muscolaris propria is involved at EUS, as in Figure 2[38]. In spite of these encouraging reports, the role of US ex-amination in caustic injuries is still under evaluation.
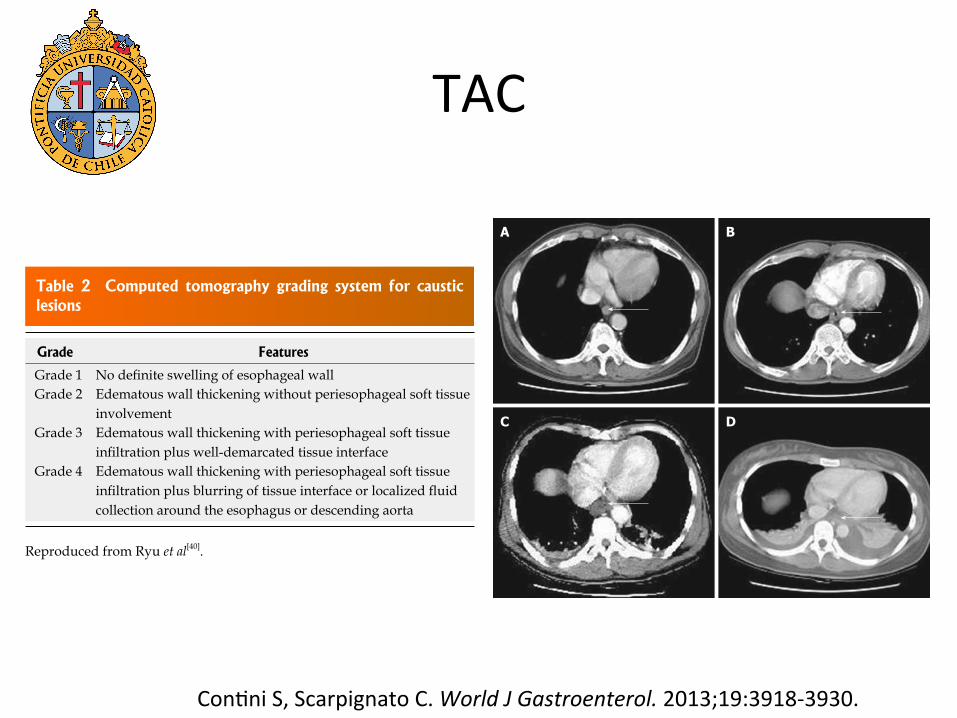
CT scanA CT scan likely offers a more detailed evaluation than early endoscopy about the transmural damage of esopha-geal and gastric walls and the extent of necrosis[39]. It is more valuable than endoscopy in assessing threatened or established stomach perforation[29], and a CT grading sys-tem (Table 2 and Figure 3) has been proposed to predict esophageal stricture[40,41]. With the advantage of not being invasive, CT scan has a promising role in the early evalua-tion of caustic injury damage.
Figure 2 Endoscopic ultrasound showing involvement of the muscularis propria of esophageal wall. Reproduced from Kamijo et al[37].
!!"#$%& '&$()#&*
Grade 1 Grade 2 Edematous wall thickening without periesophageal soft tissue
involvement Grade 3 Edematous wall thickening with periesophageal soft tissue
Grade 4 Edematous wall thickening with periesophageal soft tissue
collection around the esophagus or descending aorta
+$,-&!.! !/012)(&%!(0103#$245!3#$%673! *5*(&1!80#!9$)*(69!-&*607*
Reproduced from Ryu et al[40].
Contini S et al . Upper gastrointestinal caustic lesions
3922 July 7, 2013|Volume 19|Issue 25|WJG|www.wjgnet.com
sions do not develop delayed sequels, such as esophageal strictures or gastric outlet obstruction, whose incidence increases with the severity of the lesion. Additionally, the degree of esophageal injury at endoscopy is an accurate predictor of systemic complications and death, with each increased injury grade correlated with a 9-fold increase in morbidity and mortality[14]. Emergency surgery can be planned according to the endoscopic degree of burn, though an isolated black eschar does not always indicate full-thickness injury and the need for immediate surgical treatment: such patients may deserve further evaluation
been raised about the correlation between endoscopic findings and the extent of necrosis[39]: gastrectomy was considered unnecessary at laparotomy in 12% of patients with gastric injuries staged 3b at endoscopy, while the decision to perform esophagectomy based exclusively on endoscopic findings led to unnecessary esophagectomy in 15% of cases[52], suggesting the need for better criteria
to improve patient selection for emergency surgery.
!"#"$%!%#&Acute managementImmediate treatment is usually conservative, as the de-
after ingestion. Hemodynamic stabilization and adequacy of the patient’s airway are priorities. If the airway is un-stable, fiberoptic laryngoscopy allows intubation under direct visualization, avoiding ‘‘blind’’ intubation with the risk of bleeding and additional injuries. In challenging
and induced emesis are contraindicated for the risk of re-exposure to the corrosive agent and additional injury to the esophagus. The effectiveness of milk and water either as antidotes or to dilute the corrosive agents has never been proven. pH neutralization, with either a weak acid or base, is not recommended for fear of an exothermic reaction, which may increase the damage. Milk and acti-vated charcoal are contraindicated because may obscure subsequent endoscopy. Nasogastric tubes may be applied to prevent vomiting and as stent in severe circumferential burns, but their validity has never be proven. In any case they should not be placed blindly because of the risk of esophageal perforation[53].
H2 blockers in minimizing esophageal injury by suppress-
endoscopic healing after iv omeprazole infusion has been observed in a small prospective study[54].
The utility of corticosteroid is controversial. A meta-analysis of studies between 1991 and 2004, and an ad-
A B
C D
Figure 3 Computed tomography grading of esophageal caustic injuries. A: Grade 1; B: Grade 2; C: Grade 3; D: Grade 4. Reproduced from Ryu et al[40]. Arrows show the esophageal wall.
!!"#$%& '&$()#&*
Grade 0 Normal Grade 1 Grade 2 Mucosal and submucosal ulcerations Grade 2A Grade 2B Deep discrete or circumferential ulcerations Grade 3 Transmural ulcerations with necrosis Grade 3A Focal necrosis Grade 3B Extensive necrosis Grade 4 Perforations
Reproduced from Zargar et al[14].
Contini S et al . Upper gastrointestinal caustic lesions
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Endosonograua
Elshabrawi et al. Gastroenterol Hepatology. 2011;5(5):637-‐645. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
3921 July 7, 2013|Volume 19|Issue 25|WJG|www.wjgnet.com
EndoscopyEsophagogastroduodenoscopy is considered crucial and
-gestion, though it is safe and reliable up to 96 h after the injury[13,42] -datory during the procedure. Endoscopy and even dilata-tion have been performed without consequences from 5 to 15 d after corrosive ingestion[43], though potentially hazardous due to tissue softening and friability during the healing period. Adequate sedation (general anesthesia in children) is compulsory, yet endotracheal intubation is strictly required only for patients in respiratory distress. The constraint to stop the endoscope in the presence of a circumferential second or third degree esophageal burn is not mandatory[44,45].
When lip and oropharyngeal injuries are the main -
ly no greater than grade 1[46]. Although severe esophageal injuries have been reported in 12.0%[47] and 19.3%[48] of asymptomatic children, significant lesions at endoscopy are not usually observed when symptoms are absent after unintentional ingestion of less aggressive substances[24,49], thus making routine post-ingestion endoscopy question-able in this group of patients. All adult patients must undergo endoscopy after suicidal ingestion, because of the larger amount of more corrosive agents swallowed compared with unintentional injuries, where early esoph-agoscopy has been questioned[50]. Ultimately, though endoscopy is considered by most a cornerstone in the diagnosis of corrosive ingestions, which patients would clearly benefit from it is still debated. Considering that 10%-30% of caustic ingestions globally do not show any upper gastrointestinal injury[22,51], the indication for early endoscopy should be made on a case-by-case basis, with consideration of symptoms, otorhinolaryngeal injuries, and the amount and nature of the ingested substance.
Contraindications to endoscopy are a radiologic sus-picion of perforation or supraglottic or epiglottic burns with edema, which may be a harbinger of airway obstruc-tion, therefore indicating endotracheal intubation or tra-cheostomy. A third degree burn of the hypopharynx is a further contraindication for endoscopy[22].
[8] is important for prognosis -
and of emergency surgery[33]. Essentially, laboratory stud-ies are more useful in monitoring and guiding patient management than in predicting morbidity or mortality[34].
Traditional radiologyShortly after ingestion, a plain chest radiograph may reveal air in the mediastinum suggesting esophageal per-foration, as well as free air under the diaphragm, indicat-
a clinically suspected perforation, a water-soluble agent,
than barium sulphate, should probably be used, though both can be equally irritant[35]. Conversely, barium sulfate should be the preferred contrast agent in late barium swallowing, providing greater radiographic details than water-soluble contrast agents[22].
UltrasoundsEvaluation of esophageal wall caustic damage by endo-scopic ultrasound (EUS) using a miniprobe seems safe, though prolongs examination time without showing any difference with endoscopy in predicting early complica-tions[36]. The destruction of the muscular layers of the esophagus observed at EUS seems a reliable sign of future stricture formation[37]; furthermore, ultrasound examination with a radial probe may predict the response to dilatation, which usually requires more sessions when the muscolaris propria is involved at EUS, as in Figure 2[38]. In spite of these encouraging reports, the role of US ex-amination in caustic injuries is still under evaluation.
CT scanA CT scan likely offers a more detailed evaluation than early endoscopy about the transmural damage of esopha-geal and gastric walls and the extent of necrosis[39]. It is more valuable than endoscopy in assessing threatened or established stomach perforation[29], and a CT grading sys-tem (Table 2 and Figure 3) has been proposed to predict esophageal stricture[40,41]. With the advantage of not being invasive, CT scan has a promising role in the early evalua-tion of caustic injury damage.
Figure 2 Endoscopic ultrasound showing involvement of the muscularis propria of esophageal wall. Reproduced from Kamijo et al[37].
!!"#$%& '&$()#&*
Grade 1 Grade 2 Edematous wall thickening without periesophageal soft tissue
involvement Grade 3 Edematous wall thickening with periesophageal soft tissue
Grade 4 Edematous wall thickening with periesophageal soft tissue
collection around the esophagus or descending aorta
+$,-&!.! !/012)(&%!(0103#$245!3#$%673! *5*(&1!80#!9$)*(69!-&*607*
Reproduced from Ryu et al[40].
Contini S et al . Upper gastrointestinal caustic lesions
www.expert-reviews.com 641
Review
Esophageal rest can be achieved by making the patient nil per os and providing nutrition by total parenteral nutrition or tube feeding (nasogastric, gastrostomy or jujeunostomy). Chibisev has shown that the group with esophageal rest had a smaller percentage of post-corrosive complications than the patients who were given food or liquids immediately after poisoning [43]. Kikendall recommended esophageal rest for 10 days followed by diet advancement [44].
Other therapeutic modalities may be validated in the future. Tissue injury may result from oxygen species generated follow-ing caustic ingestion. Therefore, the use of antioxidants such as vitamin E has been suggested in patients with caustic inges-tion. In animal models vitamin E has been shown to decrease granulation tissue formation and the risk of stricture forma-tion following caustic ingestion [45]. Another promising agent is ketotifen, an H-I blocker and mast cell stabilizer. Ketotifen can decrease stricture formation when administered orally or intraperitoneally in rats [46]. Another approach is to stimulate collagenase activity with phosphatidylcholine which has been shown to prevent stricture formation in rats [47]. Other agents that can inhibit cross linking of collagen deposited by fibroblasts in the healing wound such as N-acetylcysteine, penicillamine and
-aminopropionitrile may be proven to be beneficial. However, we still lack human data and clinical trials are warranted to inves-tigate the possible role for these approaches in the management of patients with caustic ingestion.
Long-term complicationsEsophageal stricture is the major complication following caustic ingestion (FIGURES 2 & 3). The risk for stricture formation may be as high as 77% in patients with grade IIb [29] and the risk
Table 2. Esophageal grading system based on endoscopic ultrasonographic imaging.
Stage Characteristics
Grade 0 Intact muscle layer
Grade I Well-defined thickened layers
Grade IIa Indistinct muscle layer (noncircumferential)
Grade IIb Indistinct muscle layer (full circumferential)
Grade IIIa Indistinguishable muscle layer (noncircumferential)
Grade IIIb Indistinguishable muscle layer (full circumferential)
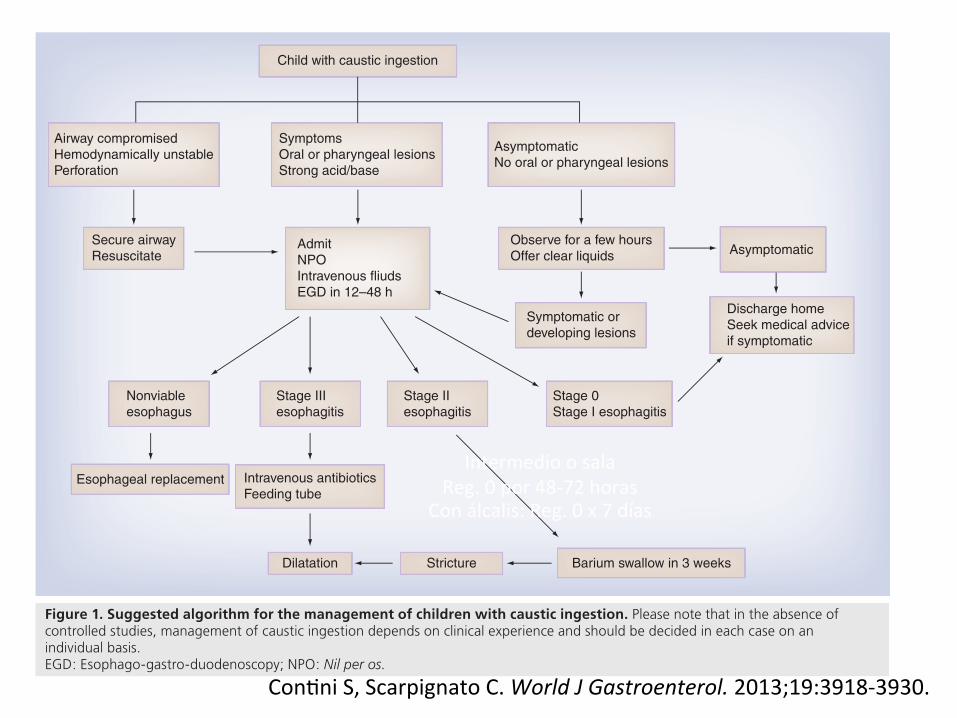
Child with caustic ingestion
Airway compromisedHemodynamically unstablePerforation
SymptomsOral or pharyngeal lesionsStrong acid/base
AsymptomaticNo oral or pharyngeal lesions
Secure airwayResuscitate
AdmitNPOIntravenous fliudsEGD in 12–48 h
Observe for a few hoursOffer clear liquids Asymptomatic
Symptomatic or developing lesions
Discharge homeSeek medical advice if symptomatic
Nonviable esophagus
Esophageal replacement
Stage III esophagitis
Intravenous antibioticsFeeding tube
Dilatation
Stage II esophagitis
Stage 0Stage I esophagitis
Stricture Barium swallow in 3 weeks
Figure 1. Suggested algorithm for the management of children with caustic ingestion. Please note that in the absence of controlled studies, management of caustic ingestion depends on clinical experience and should be decided in each case on an individual basis.EGD: Esophago-gastro-duodenoscopy; NPO: Nil per os.
Caustic ingestion in children
Expe
rt R
evie
w o
f Gas
troen
tero
logy
& H
epat
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n U
nive
rsity
Lib
rary
on
01/1
4/15
For p
erso
nal u
se o
nly.

Medidas Generales
Rojo C. Prác:ca Clínica en Gastroenterología, Hepatología y Nutrición Pediátrica. 2015;19:227-‐33.
Cor&coides
• La u&lidad de los cor&coides es contradictoria.
• El uso precoz podría disminuir las estenosis en lesiones severas y la necesidad de tratamiento endoscópico, pero conllevan mayor riesgo de perforación e infección.
• Un metanálisis de estudios entre 1991-‐2004 y un análisis posterior de la literatura hasta el 2006, no encontró ningún beneficio en prevenir la estenosis.
Pelclova D, Navra&l T. Toxicol Rev. 2005;24:125-‐129. Fulton JA, Hoffman RS. Clin Toxcol. 2007;45:402-‐408.

• Obje&vo: Estudiar efecto de altas dosis de cor&coides en la prevención de estenosis esofágica.
• Estudio prospec&vo (RCT) 2005-‐2008, 83 niños con ingesta de cáus&cos y EDA dentro de 24-‐48hrs.
• Con quemaduras grado IIb (Zargar).
• Edad: 4,10 ± 2,63 años.
Usta M, Erkan T, Cullu F, et al. Pediatrics. 2014;133:e1518.
DOI: 10.1542/peds.2013-3331; originally published online May 26, 2014; 2014;133;e1518Pediatrics
Gulcan and Tufan KutluMerve Usta, Tülay Erkan, Fugen Cullu Cokugras, Nafiye Urganci, Zerrin Onal, Mahir
BurnsHigh Doses of Methylprednisolone in the Management of Caustic Esophageal
http://pediatrics.aappublications.org/content/133/6/e1518.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from

• Obje&vo: Estudiar efecto de altas dosis de cor&coides en la prevención de estenosis esofágica.
• Estudio prospec&vo 2005-‐2008, 83 niños con Grado IIb.
• Grupo estudio (42 niños): Me&lprednisolona dosis altas 1gr/1,73m2 por 3 días + Rani&dina + Ceyriaxona + Nutrición parenteral total.
• Grupo control (41 niños): Sin me&lprednisolona.
• Outcome: Desarrollo de estenosis.
Usta M, Erkan T, Cullu F, et al. Pediatrics. 2014;133:e1518.
DOI: 10.1542/peds.2013-3331; originally published online May 26, 2014; 2014;133;e1518Pediatrics
Gulcan and Tufan KutluMerve Usta, Tülay Erkan, Fugen Cullu Cokugras, Nafiye Urganci, Zerrin Onal, Mahir
BurnsHigh Doses of Methylprednisolone in the Management of Caustic Esophageal
http://pediatrics.aappublications.org/content/133/6/e1518.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from

Usta M, Erkan T, Cullu F, et al. Pediatrics. 2014;133:e1518.
DOI: 10.1542/peds.2013-3331; originally published online May 26, 2014; 2014;133;e1518Pediatrics
Gulcan and Tufan KutluMerve Usta, Tülay Erkan, Fugen Cullu Cokugras, Nafiye Urganci, Zerrin Onal, Mahir
BurnsHigh Doses of Methylprednisolone in the Management of Caustic Esophageal
http://pediatrics.aappublications.org/content/133/6/e1518.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from
route for better access to the burn area.Because the histologic observation of thestrictures revealed acute esophagitiswith !brosis and abundant in!ltration ofin"ammatory cells, we have consideredthe blockade of the initial in"ammationas an important step for prevention ofstricture development.18 We did notobserve any side effects of corticoste-roid therapy in study group during thestudy period.
A second-look endoscopywas performedon the tenth day, and the endoscopic!ndings in both groups were also com-pared. The results were similar in bothgroups, and the difference was notfound to be statistically signi!cant.
All the patients in our study were ad-ministered TPN. TPNwas taperedafter 1week, but if the patients did not tolerateoral feeding, TPN continued. The dura-tion of TPN in the control group was
longer than the study group, and thisdifference was statistically signi!cant(P , .01). This leads to the conclusionthat the duration of hospitalization wasshorter in the study group.
Because we also aimed to evaluate thelate complications including strictureformationat theendof the thirdweekorlater, the results of the second-lookendoscopy performed on the tenthday were inconclusive. The duration ofTPNwasshorter in the studygroup. Thismeans that although the difference inthe endoscopic results was statisticallyinsigni!cant, the patients in the studygroup were discharged from the hos-pital earlier than the control group.
The rate of stricture formation aftercorrosive substance ingestion is 26% to55% in the literature.19,20 In our study,the stricture development percentagewas 20.8% among all the patients. Thelower percentages observed in our studycompared with the literature may be as-sociated with the exclusion of the gradeIIIa and IIIb patients from our study. This
TABLE 2 Clinical, Radiologic, and Endoscopic Findings During Outpatient Follow-up
Study Group, n (%) Control Group, n (%) P or OR (95% CI)
Upper GSI with barium mealAbnormal 5 (14.3) 18 (45.0) .004Normal 30 (85.7) 22 (55.0) 4.90 (1.58–15.25)
Clinical signsa during follow-upYes 8 (21.6) 16 (40.0) .082No 29 (78.4) 24 (60.0)
ES with upper GIS endoscopyb
Yes 4 (10.8) 12 (30.0) .038*No 33 (89.2) 28 (70.0) 3.536 (1.03–12.20).
Required esophageal dilatationYes 4 (10.8) 12 (30.0) .038*No 33 (89.2) 28 (70.0)
* P , .05; ES, esophageal stenosis; OR, odds ratio.a E.g., vomiting, abdominal pain, dysphagia.b x2 test.
FIGURE 2Survival rate (stricture formation as the end point) in both groups (Kaplan-Meier analysis). Cum, cumulative.
e1522 USTA et al at Pontificia Universidad Catolica de Chile on October 3, 2014pediatrics.aappublications.orgDownloaded from
Supresión de Secreción Ácida
• El uso de bloqueadores H-‐2 inmediatamente después de la inges&ón de cáus&cos puede agravar la lesión gástrica.
• Un estudio prospec&vo pequeño muestra curación endoscópica luego de infusión endovenosa de Omeprazol.
• Se recomienda iniciar al menos 24 horas después de la inges&ón de cáus&cos.
Mamede RC, de Mello Filho FV. Sao Paulo Med. J. 2001;119:10-‐15. Cakal B, Akbal E, Koklu S, et al. Dis Esophagus. 2013;26:22-‐26.

Sucralfato
• Sucralfato 1 g/1,73 m2/día.
• Efectos cito-‐protectores de la mucosa lesionada.
• Forma un complejo con las proteínas del tejido que va a proteger de otros factores agresivos.
Bau&sta et al. Protocolos AEPED. 2010 doi:10.1016/j.anpedi.2011.03.024
An&bió&cos
• Su uso ru&nario es controversial.
• Podrían reducir la carga bacteriana y disminuir la inflamación, pero no hay suficiente evidencia para su uso universal.
• Algunos autores recomiendan su uso en lesiones grado II y III.
• Ampicilina 100-‐200 mg/kg/día EV y luego VO por 3 semanas.
Salzman M, O´Mally R. Emerg Med Clin N Am. 2007;25:459-‐479.
Tratamiento Médico
Diagnostic and Therapeutic Endoscopy 3
Table 2: Medical therapy in caustic ingestion.
Grade I Grade II Grade III
Corticosteroids No No YesPPI No Yes YesAntibiotics No No Yes
e!ective than Prednisone (2 mg/kg/day) to reduce the degreeof stenosis [5, 6, 15, 20]. De Jong et al. [20] insteadindicate how the use of high doses CS could lead to anincreased risk of perforation in the paediatric populationand in patients with grade III injury. Anderson and Rouse[22] in a prospective study found no statistically significantdi!erences in favour of patients undergoing steroid therapycompared to the risk of forming stenosis. Despite the absenceof conclusive data, the maximum e"cacy is achieved whentreatment is started within the first 8 hours [23]; in case ofgrade III lesions it is suggested Dexamethasone 1 mg/kg/dayfor 3 days and gradually weaned at 10 days [13]; however,further prospective studies are needed for demonstratingthe e"cacy of the CS in changing the natural history andreducing the risk of stenosis.
The Nasogastric tube can be useful in the most seriouscases to avoid the formation of adhesions between theoesophageal wall preventing the oesophageal stenosis [24].Controversial is the use of antibiotics in the treatmentof serious injuries. The only description in the recentliterature is the one that requires the use of Ampicilline 50–100 mg/kg/day for 10 days [13, 25].
Medical therapy based on endoscopic grading of lesionsis in Table 2 summarized.
1.6. Step VI: Endoscopic Management of Oesophageal Stenosis.Two attitudes regarding the treatment of oesophageal stric-tures are described in the literature. The first is conservativeand involves a quick execution of oesophageal endoscopicdilatation. The second, less common, provides the consol-idation of stenosis, possibly around an NG-tube, and theexecution of surgical oesophageal replacement. According tothe majority of the literature [26–31], the panel consideredthat in subjects with clinical and socioeconomic favourablesituations, the conservative attitude gives better results interms of quality of life, morbidity, and mortality.
When to Start with Dilatations? Early (from fourth to sixthweeks after the ingestion) start of expansion in order to avoidstenosis tortuous and slim. Various authors [22, 30, 31] agreethat the treatment should be started with expansion after thehealing of the mucosal lesions, which usually occurs about 3weeks after the ingestion.
Which Kind of Dilatation? The panel suggests the pneu-matic dilatation in the treatment of stenosis of the recentappearance and semirigid (Savary) in stenosis with scarringconsolidated results.
Timing and size of Dilatations. On this point there is nocorrelation. The panel, based on its experience and the
literature [22], suggests to increase the size of 2–4 mm perexpansion. Regarding the timing of expansion, it is generallyaccepted at an interval between 3 and 6 weeks on firstapproach. The following timing must be based on signs andsymptoms.
Mitomycin C. It has been proposed to use topical MitomycinC, applied after dilatation, in order to slow the fibroblasticproliferation and relapse of stenosis. It is suggested at a con-centration of 0.1 mg/mL and 5 minutes of application [32].
Interruption of Dilatation Program (Refractory Stenosis). Thepanel believes, according to the literature [33] that a stenosisis defined refractory [34], when it is not possible to dilate upto a diameter that reduces dysphagia.
2. Foreign Body (FB) Ingestion
2.1. Step 1: Emergency Assessment . FB ingestion is a quitecommon event in childhood, with the highest peak incidencebetween 1 and 2 years of life. FB ingestion is always anaccidental event (93% of cases) except for patients withneurological defects or psychiatric diseases. An FB usuallypasses through the digestive tract without damage; amongpaediatric patients, approximately 80% eliminate the FBnaturally over a week [35]; 20% require an endoscopicremoval; 1% undergoes surgery for removal itself or for thepresence of complications [35].
The di!erent types of ingested FB can be schematicallylisted, both on the basis of morphological categories, both inrelation to their potential hazard:
(i) Foods: meat boli, large pips, bones, cartilage, bonesof fish).
(ii) Objects: harmless (e.g., coins or similar) or danger-ous (pins, sticks, paper clips, long or bulky objects)
(iii) Toxiccontainers (disk batteries, items containinglead, containers of drugs).
Children may be asymptomatic but may also present scialor-rhea, food refusal and odynophagia, hematemesis, vomiting,dysphagia, drooling, cough, wheezing, and dyspnoea. Thesymptoms depend on the location of the FB and itscharacteristics.
If the FB has exceeded the lower oesophageal sphincter,the patient is usually asymptomatic, as occurs in approxi-mately 50% of children [36].
In case of ingested substance containing lead, symptomsof acute intoxication may occur, involving the digestive tractas well as the renal function and the nervous system [37].
The main goal of the physical examination of the patientshould be to highlight signs of damage or oesophageal perfo-ration, as the subcutaneous emphysema of the neck (cracklesand/or hyperaemia of the neck region). If the patient presentswith inspiratory stridor, we are certainly facing an obstruc-tion of the upper airway. Unilateral wheezing or a localizedreduction of murmur vesicular can suggest lower airwayobstruction. The abdomen should always be examined to
Temiz et al. World J Gastroenterol 2012;18(10):1098-‐103.
Cirugía • Considerar de acuerdo al grado endoscópico de quemadura.
• No siempre hallazgos de EDA se correlacionan con extensión de la necrosis (hasta 15% de esofagectomías innecesarias basadas en hallazgos en EDA).
• Necesidad de adoptar criterios adicionales para mejorar la
selección de pacientes.
• Se discute en pacientes sin respuesta a dilataciones luego del tercer mes.
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Dilatación Endoscópica • Riesgo de estenosis esofágica hasta 77% con quemaduras
grado IIb y hasta 100% en las grado III.
• Desde la tercera semana de posterior a ingesta, esta presente en 80% de los que desarrollaran estenosis a las 8 semanas.
• La dilataciones con balón bajo endoscopía han sido usadas en
niños (segura y evita tracción longitudinal de otros métodos).
• Riesgo de perforación por dilatación en estenosis por cáus&cos 0,4% a 32% (vs 0,1 a 0,4% por causas benignas).
Osman M, Russell J, Shukla D, et al. J Pedi-‐atr Surg. 2008; 43: 1672-‐1678. Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Dilatación Endoscópica
www.expert-reviews.com 643
Review
Figure 4. Balloon dilatation with endoscopic control for an esophageal stricture following caustic ingestion.
Key issues
Caustic ingestion continues to be a significant problem.The presence or absence of symptoms or signs does not predict the presence or absence of lesions.Endoscopy is the mainstay diagnostic modality.The decision to carryout an endoscopy should be made on a clinical case-by-case basis.Stricture is the main complication following caustic ingestion.The use of steroids has no proven value.Caustic ingestion can lead to carcinoma formation.Surgical intervention is needed in some patients.All efforts should be exhausted to keep the native esophagus.
Caustic ingestion can lead to carcinoma formation (both adeno-carcinoma and squamous cell carcinoma) with an incidence of 2–8% [62]. The latency period may be as long as 42 years. The incidence may be higher if patients were followed for 30 years [63]. The incidence is 1000-times that expected in the normal popula-tion of similar ages. Carcinomas usually develop at the strictured site or the area of bifurcation of trachea and are often resectable. However they usually carry a poor prognosis (40% survival rate at 1 year and 13% at 5 years) [64]. There is controversy regarding the need for periodic surveillance for the development of dyspla-sia and carcinoma following caustic ingestion. It has been sug-gested that periodic endoscopy should be considered in patients 20 years of age or older after the initial ingestion [64]. However, prompt evaluation with the appearance of any symptoms, such as dysphagia, is mandatory.
Expert commentaryThe high incidence of caustic ingestion highlights the great need for educating the public through information campaigns directed specifically at care givers of toddlers, stressing that children should have no access to caustics which should always be stored separately in safe containers. The high rate of complications fol-lowing esophageal replacement stresses the need for multidisci-plinary long-term follow-up and research for alternatives to colon interposition as a surgical approach for esophageal strictures.
Five-year viewThe search continues for novel therapeutic modalities to prevent and treat the complications associated with caustic ingestion. An active and promising area of research for prevention of stricture formation is the development of agents that can inhibit cross link-ing of collagen deposited by fibroblasts in the healing wound such as N-acetylcysteine, penicillamine and -aminopropionitrile. The
use of these agents may be validated in the next 5 years. However, clinical trials are needed to prove its efficacy.
Financial & competing interests disclosureThe authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.
References1 Contini S, Swarray-Deen A, Scarpignato C.
Oesophageal corrosive injuries in children: a forgotten social and health challenge in developing countries. Bull. World Health Organ. 87(12), 950–954 (2009).
2 Bronstein AC, Spyker DA, Cantilena LR Jr et al. 2007 Annual Report of the American Association of Poison Control Centers’
National Poison Data System (NPDS), 25th Annual Report. Clin. Toxicol. 46(10), 927–1057 (2008).
3 Arévalo-Silva C, Eliashar R, Wohlgelernter J et al. Ingestion of caustic substances: a 15-year experience. Laryngoscope 116(8), 1422–1426(2006).
4 Friedman EM. Caustic ingestion and foreign bodies in the aerodigestive tract of
children System. Pediatr. Clin. North Am. 36, 1403–1410 (1989).
5 Wheeler DS, Bonny AE, Ruddy RM et al. Late-onset respiratory distress after inhalation of laundry detergent. Pediatr. Pulmonol. 35, 323–325 (2003).
6 Einhorn A, Horton L, Alteri M et al. Serious respiratory consequences of detergent ingestion in children. Pediatrics 84, 472–474 (1989).
Caustic ingestion in children
Expe
rt R
evie
w o
f Gas
troen
tero
logy
& H
epat
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y W
ashi
ngto
n U
nive
rsity
Lib
rary
on
01/1
4/15
For p
erso
nal u
se o
nly. Elshabrawi et al. Gastroenterol Hepatology. 2011;5(5):637-‐645.
Otras Terapias para Estenosis Esofágica en Estudio
• Inyección local de cor&coides (triamsinolona); dosis óp&ma,
frecuencia y técnica de administración aun en estudio.
• Mitomicina C (QMT) con resultados promisorios, pero efectos adversos a largo plazo desconocidos.
• Stent de silicona o poliflex con eficacia < 50%.
• Otros en estudio (an&oxidantes, Vitamina E, 5-‐fluorouracilo).
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Complicaciones Gástricas • Dolor abdominal intratable, retención gástrica, aclorhidria
tardía, gastroenteropa{a perdedora de proteínas, metaplasia mucosal y desarrollo de carcinoma.
• Incidencia de obstrucción pilórica de 5% por espasmo pilórico y estenosis en más de 60% de los pacientes.
• Cuando se ingiere un volumen significa&vo de corrosivo, el estómago completo cicatriza alterando la contrac&lidad de forma difusa.
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
www.expert-reviews.com 641
Review
Esophageal rest can be achieved by making the patient nil per os and providing nutrition by total parenteral nutrition or tube feeding (nasogastric, gastrostomy or jujeunostomy). Chibisev has shown that the group with esophageal rest had a smaller percentage of post-corrosive complications than the patients who were given food or liquids immediately after poisoning [43]. Kikendall recommended esophageal rest for 10 days followed by diet advancement [44].
Other therapeutic modalities may be validated in the future. Tissue injury may result from oxygen species generated follow-ing caustic ingestion. Therefore, the use of antioxidants such as vitamin E has been suggested in patients with caustic inges-tion. In animal models vitamin E has been shown to decrease granulation tissue formation and the risk of stricture forma-tion following caustic ingestion [45]. Another promising agent is ketotifen, an H-I blocker and mast cell stabilizer. Ketotifen can decrease stricture formation when administered orally or intraperitoneally in rats [46]. Another approach is to stimulate collagenase activity with phosphatidylcholine which has been shown to prevent stricture formation in rats [47]. Other agents that can inhibit cross linking of collagen deposited by fibroblasts in the healing wound such as N-acetylcysteine, penicillamine and
-aminopropionitrile may be proven to be beneficial. However, we still lack human data and clinical trials are warranted to inves-tigate the possible role for these approaches in the management of patients with caustic ingestion.
Long-term complicationsEsophageal stricture is the major complication following caustic ingestion (FIGURES 2 & 3). The risk for stricture formation may be as high as 77% in patients with grade IIb [29] and the risk
Table 2. Esophageal grading system based on endoscopic ultrasonographic imaging.
Stage Characteristics
Grade 0 Intact muscle layer
Grade I Well-defined thickened layers
Grade IIa Indistinct muscle layer (noncircumferential)
Grade IIb Indistinct muscle layer (full circumferential)
Grade IIIa Indistinguishable muscle layer (noncircumferential)
Grade IIIb Indistinguishable muscle layer (full circumferential)
Child with caustic ingestion
Airway compromisedHemodynamically unstablePerforation
SymptomsOral or pharyngeal lesionsStrong acid/base
AsymptomaticNo oral or pharyngeal lesions
Secure airwayResuscitate
AdmitNPOIntravenous fliudsEGD in 12–48 h
Observe for a few hoursOffer clear liquids Asymptomatic
Symptomatic or developing lesions
Discharge homeSeek medical advice if symptomatic
Nonviable esophagus
Esophageal replacement
Stage III esophagitis
Intravenous antibioticsFeeding tube
Dilatation
Stage II esophagitis
Stage 0Stage I esophagitis
Stricture Barium swallow in 3 weeks
Figure 1. Suggested algorithm for the management of children with caustic ingestion. Please note that in the absence of controlled studies, management of caustic ingestion depends on clinical experience and should be decided in each case on an individual basis.EGD: Esophago-gastro-duodenoscopy; NPO: Nil per os.
Caustic ingestion in childrenEx
pert
Rev
iew
of G
astro
ente
rolo
gy &
Hep
atol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Was
hing
ton
Uni
vers
ity L
ibra
ry o
n 01
/14/
15Fo
r per
sona
l use
onl
y.
Intermedio o sala Reg. 0 por 48-‐72 horas
Con álcalis: Reg. 0 x 7 días

EDA Tipo de Lesión
Sin lesión o Lesión &po I
Alta al comprobar buena tolerancia oral
Eventual control a las 3 semanas con Rx EED (ingesta ácidos)
Lesión Tipo IIa
Intermedio o sala Reg. 0 por 48-‐72 horas
Con álcalis: Reg. 0 x 7 días con NPT
Lesión Tipo IIb o III
Manejo Intensivo NPT o yeyunostomía (48-‐72
hrs.) por 7 a 21 días.
Manejo quirúrgico de lesiones necró&cas

Otras Terapias en Estudio • Vitamina E
• Keto&feno
• Fosfa&dilcolina
• N-‐ace&lcisteína
• Penicilamina
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.

Prevención • Para disminuir los accidentes por ingesta de cáus&cos es
fundamental establecer estrategias de prevención.
• Prevención en la fabricación, envasado, manipulación y almacenaje de estas sustancias.
Con&ni S, Scarpignato C. World J Gastroenterol. 2013;19:3918-‐3930.
Conclusiones • La inges&ón de cáus&cos es un mo&vo de consulta infrecuente,
pero asociado a alta morbimortalidad.
• Los síntomas o signos no siempre predicen la presencia de lesiones.
• La EDA es la principal herramienta de diagnós&co, y la clasificación de Zargar &ene un rol pronós&co.
• La estenosis esofágica es la principal complicación.
• El uso de cor&coides en el manejo de quemaduras por inges&ón de cáus&cos es controversial.
Conclusiones • Algunos pacientes pueden requerir cirugía.
• Se requieren más estudios prospec&vos, controlados, mul&céntricos para iden&ficar mejores protocolos de manejo.
• La inges&ón de cáus&cos puede llevar a formación de carcinoma, por lo que se requiere control EDA a largo plazo.
• Lo más importante es la prevención.

¿Preguntas o cometarios?