injury prevention and sports rehab in the weightlifting...
TRANSCRIPT

Injury prevention and sports rehab in the weightlifting sport
Dr Massimiliano Febbi Phd (c),Pt,Bsc Kin, DO,CSCS*D,CPT*D
Professor Faculty Exercise Science University of Tor Vergata Rome
Educational Director NSCA Italy
Italian Weightlifting Team Head Physiotherapist
EWF Scientific Seminar
Lignano February 09,2013

INJURies Rehabilitation
INJURIES PREVENTION
InjuryINJU

INJURIES REHABILITATION
we lost our time

Prevention
• Injuries are prevented by:
• Identifying risk factors
• Addressing risks with preventive measures

Posture
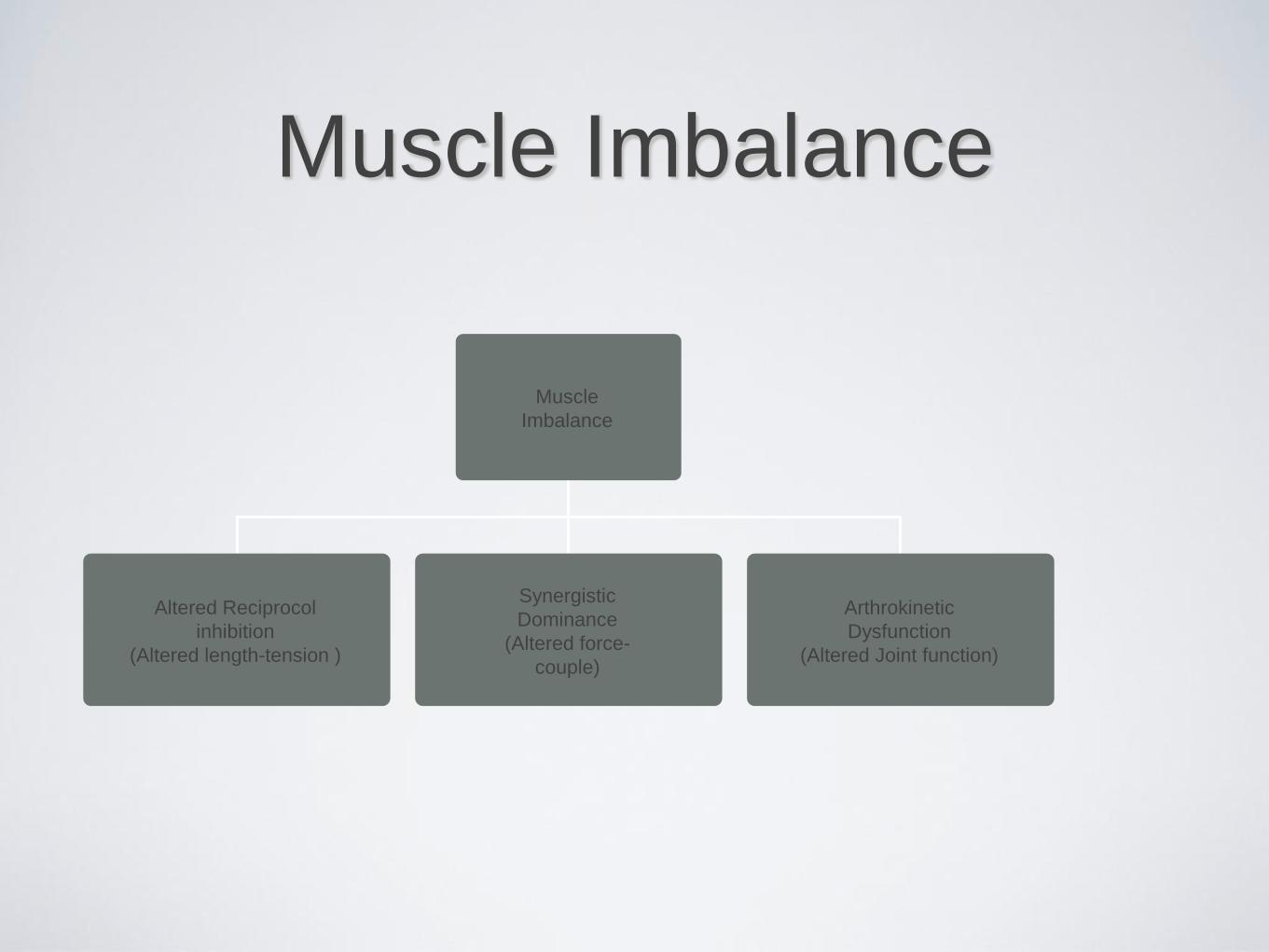
Muscle Imbalance
Muscle
Imbalance
Altered Reciprocol
inhibition
(Altered length-tension )
Synergistic
Dominance
(Altered force-
couple)
Arthrokinetic
Dysfunction
(Altered Joint function)

Dysfunction
• Altered reciprocal inhibition- a tight muscle causes decreased neural drive to its functional antagonist
• Synergistis dominance- compensation of synergistic muscles in order to maintain force production
• Myofascial dysfunction (trigger points)
• Arthrokinematic dysfunction- joint dysfunction affecting the surrounding muscles
• Faulty movement patterns

Dysfunction Leads to
• Altered neuromuscular control
• Tissue fatigue
• Injury and impaired performance
Causes of Muscle Imbalances
• Postural stress
• Pattern overload
• Repetitive movement
• Lack of core stability
• Lack of neuromuscular efficiency
Muscle Imbalance
• The relationship between the tone or strength and
length of the muscles around a joint
• Stronger will shorten and the opposite will lengthen
• Weakness causes faulty alignment or an imbalance
• Bilateral and unilateral
• Common example is low back pain can be contributed to a
weak abdomen

PATTERNS OF DYSFUNCTION
When a chain reaction evolves in which some
muscles shorten and others weaken, in predictable
patterns of imbalance (Janda)
1. Upper crossed syndrome
2. Lower crossed syndrome

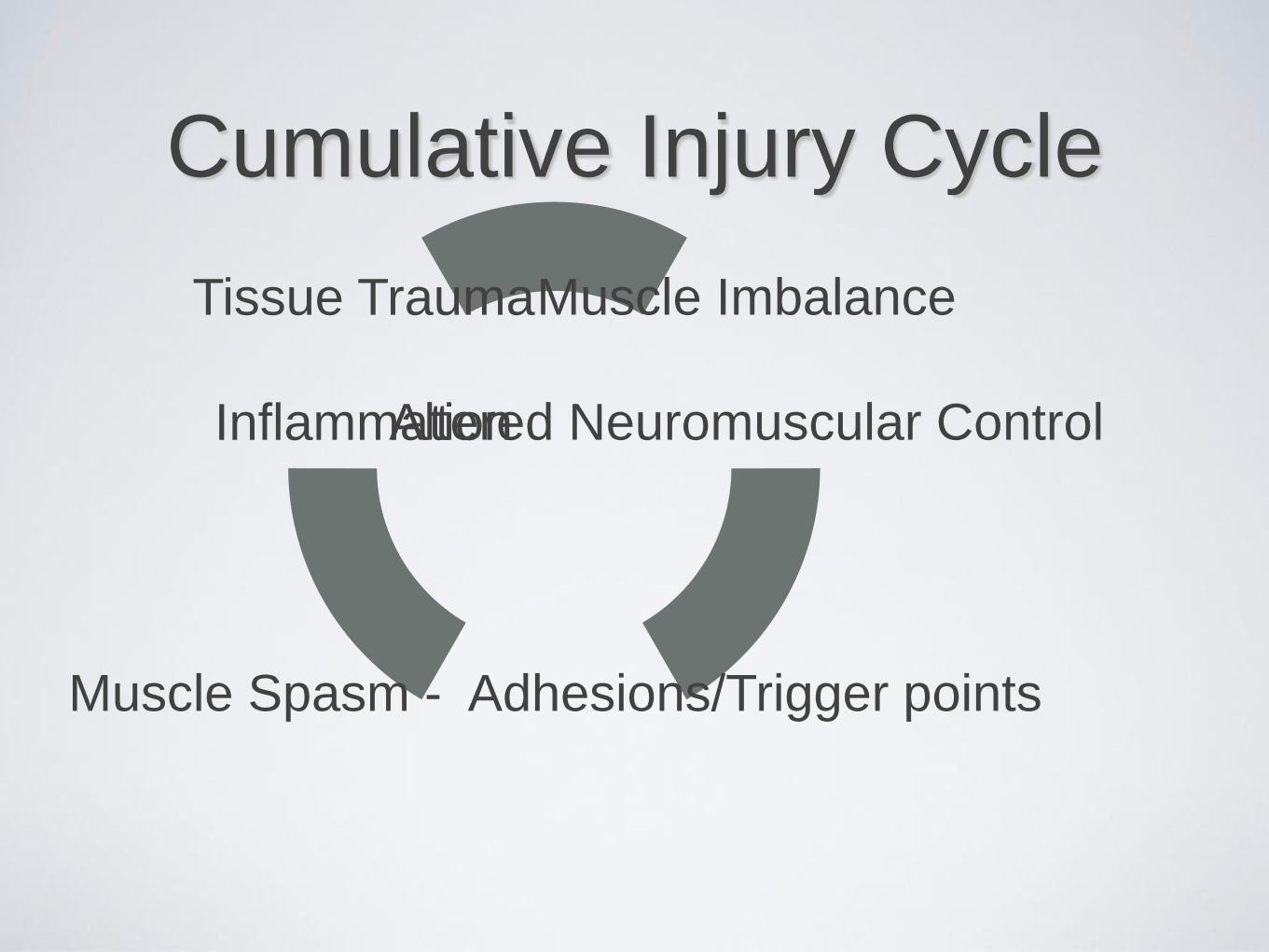
Cumulative Injury Cycle
Muscle Imbalance
Altered Neuromuscular Control
Muscle Spasm - Adhesions/Trigger points
Tissue Trauma
Inflammation


Screening
• To recognize candidates for possible injury
• Manual Muscle Testing
• A muscle is isolated and tested for strength
• Muscle length
• Stretched to endpoint

Strengthening
• The agonist needs to be lengthened
• The antagonist needs to be trained to work again or strengthened
• Statically then dynamically
• Static requires both the agonist of that movement to be strengthened and the antagonist of that movement to be stretched lengthening the muscle
• Dynamic exercises can be done in a variety of ways to contribute to the benefits needed

Prevention
• Education
• Proper posture
• Proper and equal weight lifting
• Hamstring vs. quadriceps muscles
• Stretching

Weaknesses Usually Found
• Hip Stabilizers (gluteus medius, adductors, quadratus
lumborum, hip external rotators)
• Lumbar Stabilizers (transverse abdominus, internal
obliques)
• Scapular Stabilizers (lower traps, rhomboids)

In Other Words… “The Core”
• Evolving concept of trunk strength & stability
• “Pillar” a more inclusive concept, more than just the
abdominals
• It is the integration of the hips, trunk and shoulders
Some other roles of the
Core
• Posture
• Balance
• Energy transfer (LB to UB & vice-versa)
• Protection (internal organs)
• Anchoring (muscle origins & insertions)

FUnctional Assessment

What is Function? • Function – from Latin
“functio” meaning to perform, the special action or physiologic property of an organ or other part of the body (Stedman’s)
• What constitutes lower extremity “function”?
– Speed
– Agility
– Hopping
– Jumping
– Landing
– Balance
– Proprioception
– Stability
– Strength
– Muscle Reaction Time
– Joint Laxity
– Kicking
– Subjective considerations

Ultimate Rehabilitation Goal
• Return the
athlete/patient to the
highest functional level
in the most efficient
manner!

Functional Performance
Testing • Can assist the clinician in making
return to play decisions
• “These tests are designed to
simulate, in a controlled manner,
the stresses produced and
imposed on the LE during athletic
participation” – Drouin and Riemann -
ATT 2004
• The outcome measure is a
summary variable that represents
a patient’s sensorimotor function,
muscle strength and power,
flexibility, pain, and confidence

Concepts of Functional
Rehabilitation
• Begins on the day of injury and continues until pain-
free gait & activities are achieved!
• Four Aspects of Functional Rehabilitation:
• ROM
• Strengthening
• Proprioception
• Activity-Specific Training

Lower Extremity
Functional Testing • Balance Tests
• Numerous variations of
the Romberg test are
available
• Valid and reliable
• Scoring may include time
or use of the Balance
Error Scoring System
(BESS)
• Can be performed on a
variety of surfaces

The BESS
Reliable with SL and TS on a firm
surface, and DL, SL, and TS on a foam
surface!
Lower Extremity
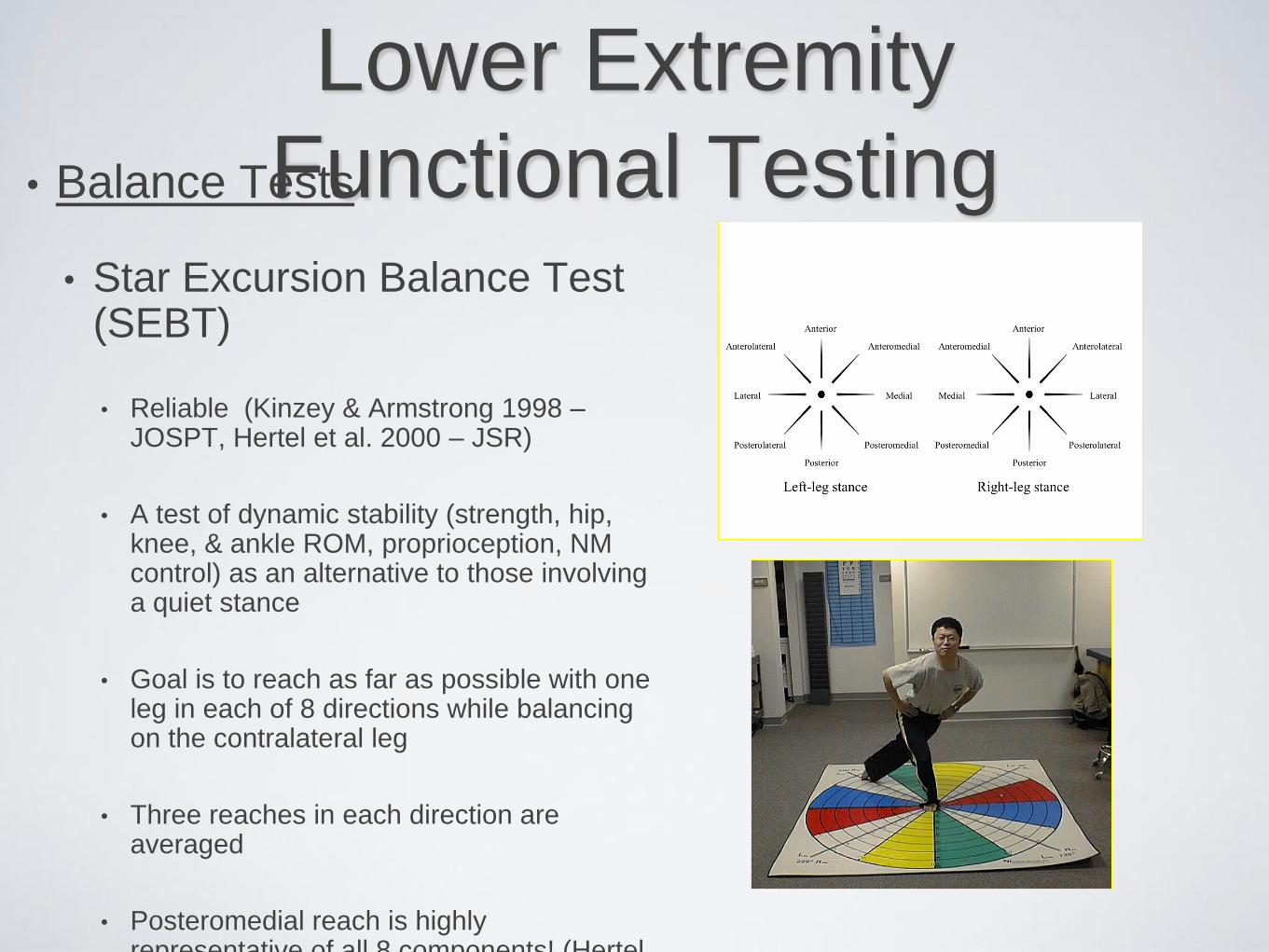
Functional Testing • Balance Tests
• Star Excursion Balance Test (SEBT)
• Reliable (Kinzey & Armstrong 1998 – JOSPT, Hertel et al. 2000 – JSR)
• A test of dynamic stability (strength, hip, knee, & ankle ROM, proprioception, NM control) as an alternative to those involving a quiet stance
• Goal is to reach as far as possible with one leg in each of 8 directions while balancing on the contralateral leg
• Three reaches in each direction are averaged
• Posteromedial reach is highly representative of all 8 components! (Hertel

Functional Movement
Screening

What is FMS? • Series of movements designed to
screen for:
Flexibility
Body movement asymmetry
Core muscle weakness
• Screening can potentially predict injury
If we can predict it, we can prevent it
• Find the weak link and fix it!
• Less Injuries =
Decreased training losses
Better soldier retention

What is FMS? • 7 fundamental movement patterns
• Graded by trained examiner
• Each movement graded 0 to 3
• Able to target problem movements
• Creates individual functional
baseline
• Simple, quick, reproducible
• Deficits corrected by physical
therapy program

7 Movements
• Deep Squat
• Hurdle Step
• In-Line Lunge
• Shoulder Mobility
• Straight Leg Raise
• Push-Up
• Rotational Stability

Summary
• Certain physiologic measures are good indicators of
performance
•Many performance tests can be conducted
•Multiple variations of training programs can be
devised to improve performance
• All energy systems should be trained.

•THANK YOU