inquiry into life twelfth edition chapter 17 lecture powerpoint to accompany sylvia s. mader...
TRANSCRIPT

Inquiry into LifeTwelfth Edition
Chapter 17
Lecture PowerPoint to accompany
Sylvia S. Mader
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.

17.1 Nervous Tissue
• The Nervous System – Two Anatomical Divisions
• Central Nervous system (CNS)– Brain and Spinal Cord
• Peripheral Nervous System (PNS)
– Two Types of Cells• Neurons (transmit nerve impulses)
• Neuroglia– Support and nourish neurons

17.1 Nervous Tissue
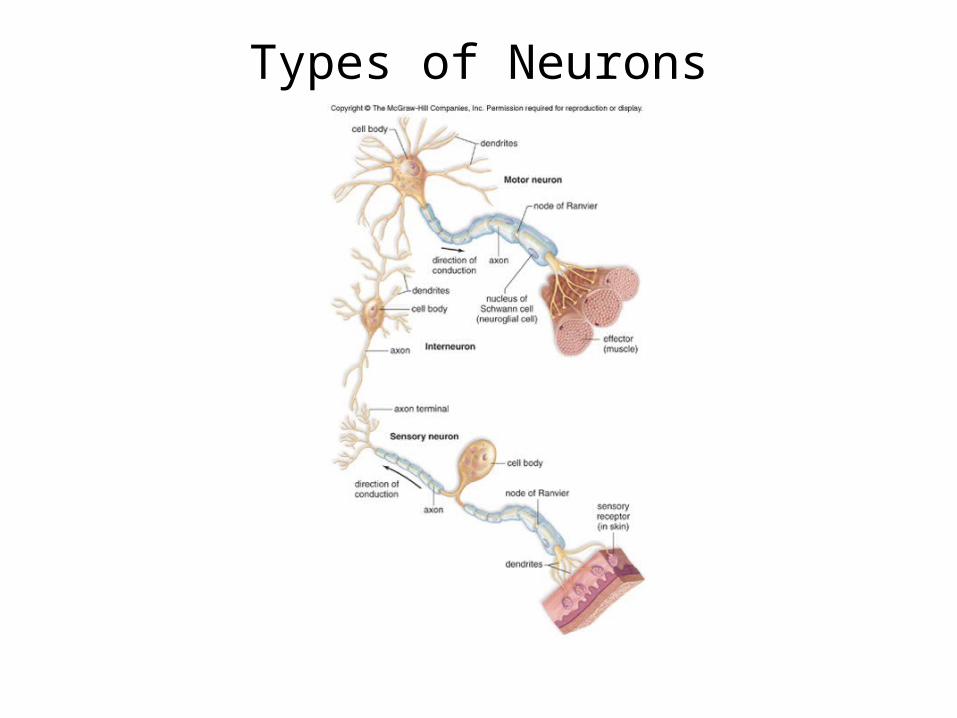
• Types of Neurons and Neuron Structure– Three Classes of Neurons
• Sensory Neurons– Takes messages to the CNS– May have specialized endings (sensory receptors)
• Interneurons– Always in the CNS– Receive input from sensory neurons and other interneurons– Summarize messages – Communicate with motor neurons
• Motor Neurons– Carries messages from the CNS to an effector

Organization of the Nervous System
17.1 Nervous Tissue
• Types of Neurons and Neuron Structure
– Three Parts of a Neuron• Dendrites: Extensions that send impulses to the
cell body
• Cell Body: Contains the nucleus and other organelles
• Axon: Conducts nerve impulses away from
the cell body toward other neurons or
effectors
Types of Neurons

17.1 Nervous Tissue
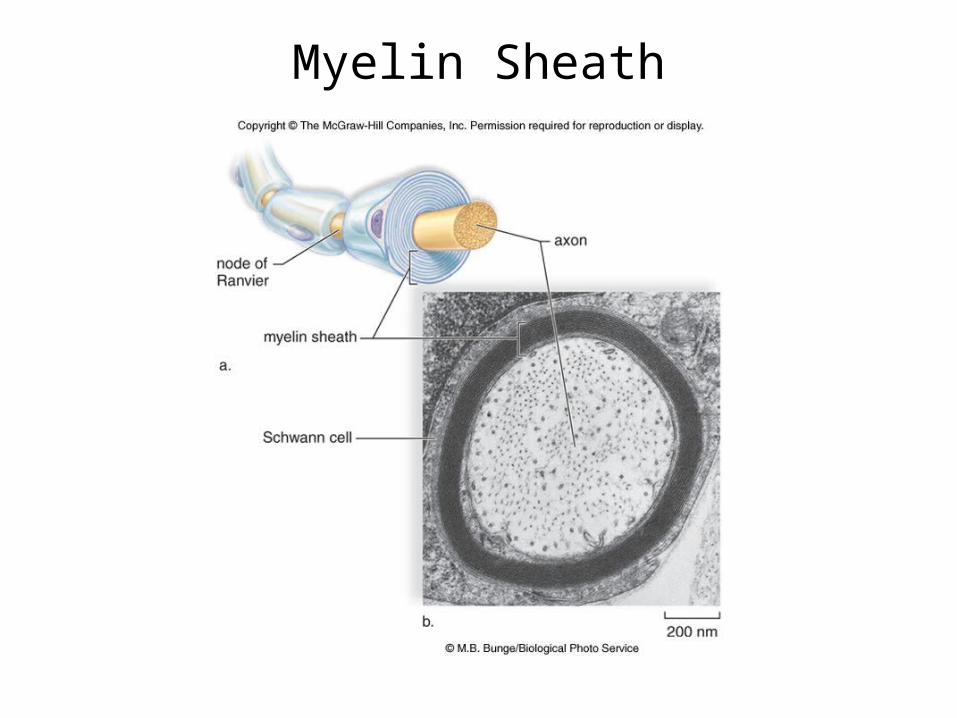
• Myelin Sheath– Covers some axons
• Nodes of Ranvier: gaps in the myelin sheath• In the Peripheral Nervous System
– Acts as an insulator– Important in nerve regeneration– Myelin is formed by Schwann cells (neuroglia)
• In the Central Nervous System– Myelin is formed by oligodendroglial cells– Little nerve regeneration in the CNS
17.1 Nervous Tissue
• Myelin Sheath– In the Central Nervous System
– Neurons with short axons are nonmyelinated» Make up gray matter
– Neurons with myelinated axons-» Make up white matter
– Brain» Surface layer of brain is gray matter» White matter lies deep
– Spinal cord» Central portion is gray matter» White matter surrounds the gray matter
Myelin Sheath

17.1 Nervous Tissue
• The Nerve Impulse– Resting Potential
• Inside of axon is electronegative with respect to outside (-65mV)
• Resting potential is due to– Unequal distribution of ions across membrane
» More sodium outside than inside» More potassium inside than outside» Presence of negatively charged ions inside
• Resting potential is maintained by– Unequal permeability of membrane
» More permeable to potassium than sodium (at rest)» Membrane tends to “leak” positive charges
– Sodium-potassium pump-maintains concentrations of sodium and potassium

Resting Potential

17.1 Nervous Tissue
• The Nerve Impulse– Action Potential
• Rapid change in polarity across membrane as impulse occurs
• All or none phenomenon• Threshold stimulus
– Causes axonal membrane to depolarize to threshold level
– Generates an action potential– Intense stimulus causes axon to fire more often in a
given time interval– Requires Two types of gated channel proteins
» Sodium channels» Potassium channels

17.1 Nervous Tissue
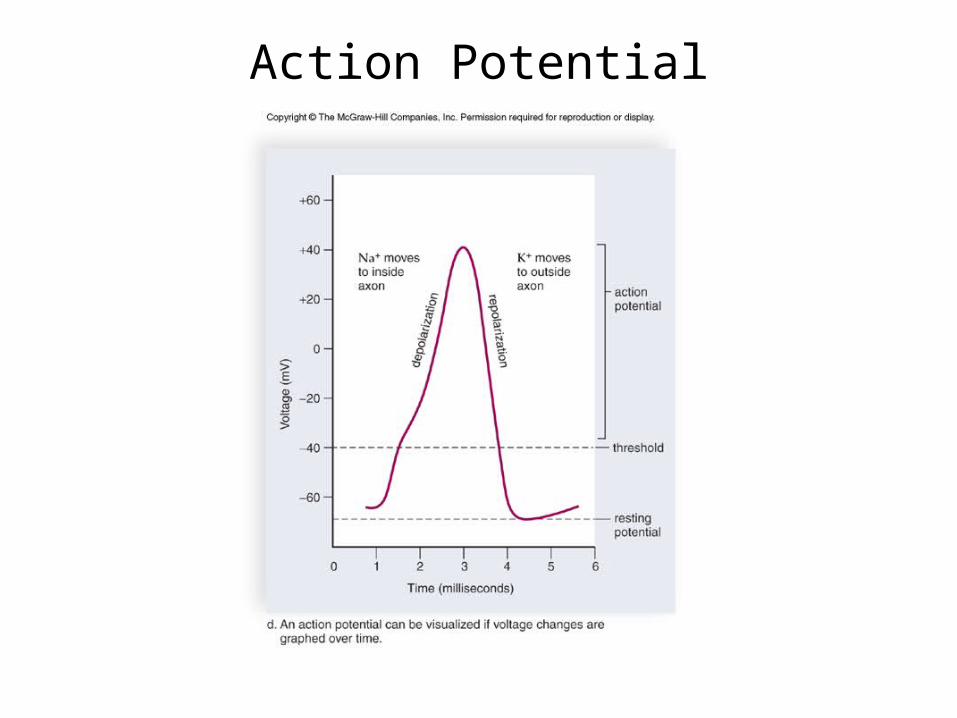
• The Nerve Impulse– Events of an Action Potential
• Sodium Gates Open First– Sodium flows down the concentration gradient into the axon– Membrane potential changes from -65mV up to +40mV– Called depolarization because inside changes from negative to
positive– Gates close
• Potassium Gates Open– Potassium flows down its concentration gradient out of the axon– Brings potential back to -65mV– Called repolarization because it returns to original polarity– Gates close

Action Potential(insert 17.4 b, c)
17.1 Nervous Tissue
• The Nerve Impulse– Conduction of an Action Potential
• Nonmyelinated Axons– Action potential travels down axon one small segment at a time– As soon as action potential moves on, the previous section
undergoes a refractory period» Sodium gates cannot reopen» Prevents an action potential from moving backward» During this time sodium-potassium pump restores ions to
original positions• Myelinated Axons
– Gated ion channels concentrated in Nodes of Ranvier– Action potential travels faster
» “Jumps” from node to node (saltatory conduction)
Action Potential

Chemical SynapseStructure and Function

17.1 Nervous Tissue
• Transmission Across a Synapse– Synaptic Integration
• A single neuron may receive many signals, both excitatory and inhibitory
• Synaptic integration is the summing up of excitatory and inhibitory signals
– This determines if an action potential will travel along an axon

Synaptic Integration
17.1 Nervous Tissue
• Transmission Across a Synapse– Neurotransmitters
• Acetylcholine (ACh) and norepinephrine (NE) are examples
• Both are excitatory neurotransmitters• Once released and responses initiated,
neurotransmitters are removed from cleft– Some removed by enzymes
» ACh is removed by acetylcholinesterase– Others are taken back up by presynaptic neuron– Prevents repeated stimulation of postsynaptic membrane
17.1 Nervous Tissue
• Transmission Across a Synapse
– Neurotransmitters
• Many drugs affect nervous system by interfering with or
potentiating neurotransmitters
– Can enhance or block release
– Can interfere with removal from cleft

Organization of the Nervous System

17.2 The Central Nervous System
• Bone surrounds both the brain and the spinal cord
• Meninges are protective membranes that wrap around the brain and spinal cord– Cerebral spinal fluid fills the spaces between the
meninges• Cushions and protects the CNS
• The brain has interconnecting cavities called ventricles– These also connect with the hollow central canal of
the spinal cord
17.2 The Central Nervous System
• The Spinal Cord– Structure
• Extends from base of brain into vertebral canal• Protected by vertebrae
– Intervertebral disks cushion and separate• Cross-sectional anatomy
– Central gray matter» Shaped like letter “H”» Dorsal root- sensory fibers entering gray matter» Ventral root-motor fibers leaving gray matter» Dorsal and ventral roots join as spinal nerve» Spinal nerves are part of the CNS

17.2 The Central Nervous System
• Spinal Cord – White matter
• In areas around gray matter• Ascending and descending tracts
– Ascending tract is located dorsally» Sends information to the brain
– Descending tract is located ventrally» Sends information from the brain to spinal nerves» Many tracts cross over to opposite side» Left side of brain controls right side of body and vice versa

Spinal Cord
17.2 The Central Nervous System
• Functions of Spinal Cord– Communication between brain and body– Center for many reflex arcs
• Sensory receptors generate an action potential• Sensory neurons transmit impulse to the spinal cord• Sensory neurons synapse with interneurons in the spinal
cord• Interneurons synapse with motor • Motor neurons carry impulse to effectors

17.2 The Central Nervous System
• Four Major Areas of the Brain– The Cerebrum
– The Diencephalon
– The Cerebellum
– The Brain Stem

The Human Brain
17.2 The Central Nervous System
• The Brain– Cerebrum
• Two cerebral hemispheres– Divided by longitudinal fissure but connected by the corpus
callosum
– Covered by a convoluted layer of gray matter
• The cerebral cortex is the region that accounts for sensation,
voluntary movement, and conscious thought

The Lobes of a Cerebral Hemisphere
17.2 The Central Nervous System
• The Brain– Cerebrum
• Primary Motor and Sensory Areas of the Cortex• Primary Motor Area
– All voluntary motor movements originate here» Each body part is controlled by a specific section
• Primary Somatosensory Area– Receives sensory information from skin and skeletal
muscles

Primary Motor and Somatosensory Areas

17.2 The Central Nervous System
• The Brain– Cerebrum
• Association Areas (integration)
• Premotor Area– Organizes skilled motor activities (ex: riding a bike)
• Somatosensory Association Area- – Analyzes incoming information– Visual and auditory association areas
» Compares incoming information with past experience
17.2 The Central Nervous System
• The Brain– Cerebrum
• Processing Centers– Receive information from all association areas
• Prefrontal Area– Perform higher-level analytical functions– Integration here accounts for critical thinking abilities
• Wernicke’s Area– Understanding of written and spoken words
• Broca’s Area-– Directs motor actions for speech– Grammatical refinements
17.2 The Central Nervous System
• The Brain– Cerebrum
• Central White Matter– Composes most of cerebrum deep to cortex– Composed of tracts of axons that take information
between different sensory, motor, and association areas
• Basal Nuclei– Masses of gray matter deep within cerebrum– Integrate motor commands
17.2 The Central Nervous System
• The Brain– The Diencephalon
• Composed of the Hypothalamus and the Thalamus– The hypothalamus is a homeostatic control center
» Body temperature» Water balance» Hunger and thirst» Sleep
– The hypothalamus manufactures hormones and controls the pituitary gland

17.2 The Central Nervous System
• The Brain– The Diencephalon
• Composed of the Hypothalamus and the Thalamus– The thalamus is a sensory relay center
» Receives incoming information and sends it to appropriate area
» Arousal of cerebrum» Memory, emotional responses
– The pineal gland is located in the thalamus

17.2 The Central Nervous System
• The Brain– The Cerebellum
• Receives both sensory and motor input• Integrates information and sends impulses to skeletal
muscles by way of the brain stem• Can compare actual movements with intended movements• Functions to assure smooth, coordinated motor movements

17.2 The Central Nervous System
• The Brain– The Brain Stem
• Midbrain: A relay center for tracts passing between cerebrum, cerebellum, and breathing, reflex movements of the head
• Medulla oblongata: Control center for– Heart rate, breathing, blood pressure, swallowing, coughing,
vomiting• Pons (bridge)
– Contains bundles of axons traveling between the cerebellum and the rest of the CNS

17.3 The Limbic System and Higher Mental Functions
• The Limbic System– Complex network of tracts and nuclei
– Blends primitive emotions (fear, aggression, pleasure)
with higher mental functions (reasoning, memory)
17.3 The Limbic System and Higher Mental Functions
• Anatomy of the Limbic System– Hippocampus
• Communicates with the prefrontal area of the brain
– Amygdala• Allows us to respond to and respond to:
– Anger, defensiveness, avoidance, fear
• Promotes the release of adrenaline

The Limbic System
17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Memory and Learning
• Memory is the ability to hold on to or recall a piece of information
• Learning is the ability to retain and apply past memories– Types of Memory
• Short-Term Memory– Retained for short period (ex: a phone number you look up)
• Long-Term Memory– Retained for long period, perhaps for life– Semantic memory (words, numbers, etc) – Episodic memory (people, events, etc.)
17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Types of Memory
• Skill Memory– Involved in performing motor activities
» Riding a bike is one example– Involves all motor areas of the cerebrum below the level of
consciousness
17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Long-Term Memory Storage and Retrieval
• Memories are stored in bits and pieces in association areas• Hippocampus pulls these all together to allow us to recall
them all as a single event• Amygdala is responsible for emotions associated with some
memories
17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Long-Term Potentiation (LTP)
• An enhanced synaptic response in hippocampus• Important to memory storage• Excitotoxicity is the death of postsynaptic neuron
– Most likely from mutation– Glutamate may mediate this– Explains small memory difficulties as we age

17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Language and Speech
• Language is dependent upon semantic memory• Seeing and hearing words-
– dependent upon primary visual cortex (occipital lobe) – dependent upon primary auditory cortex (temporal lobe)
• Speaking words-– dependent upon primary motor cortex function

17.3 The Limbic System and Higher Mental Functions
• Higher Mental Functions– Language and Speech
• The left and right cerebral hemispheres have different functions related to language and speech
– Broca’s and Wernicke’s areas are only in the left hemisphere» Broca’s- ability to speak» Wernicke’s- ability to comprehend speech
– Both hemispheres process information, but differently» Left is very specific» Right is very global

Language and Speech

17.4 The Peripheral Nervous System
• The Peripheral Nervous System is composed of:– Nerves (bundles of
nerve fibers)– Ganglia (collection of
nerve cell bodies)

17.4 The Peripheral Nervous System
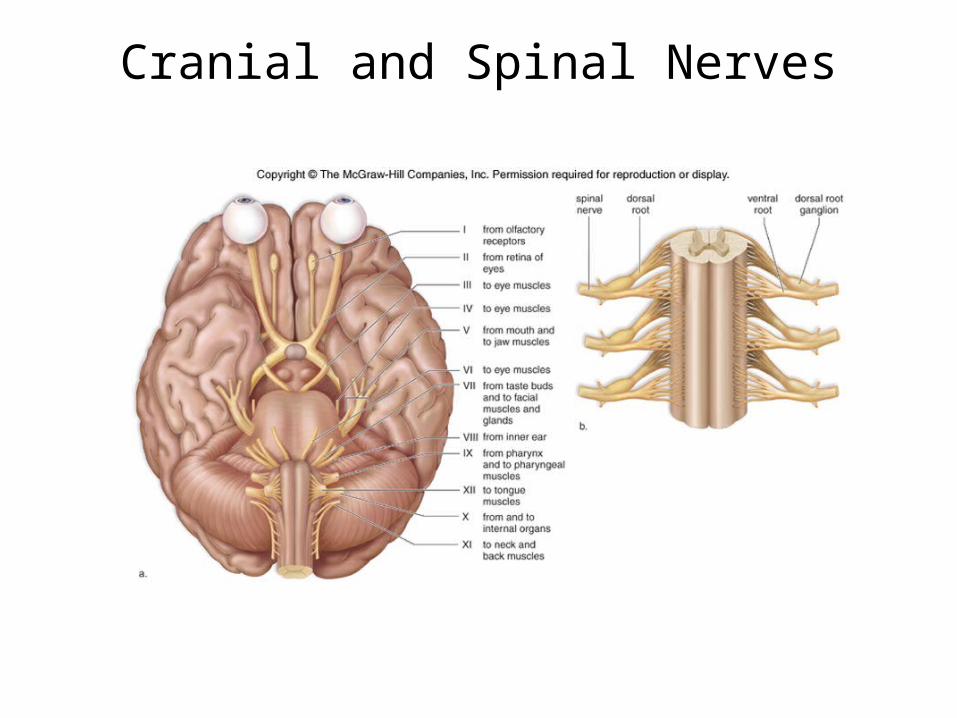
• Cranial and Spinal Nerves– Cranial Nerves- 12 pairs
• Attached to the brain• Some are purely sensory, some motor, and some are mixed• Largely concerned with head, neck, and face with the
exception of the vagus nerve which extends to thorax and abdomen
– Spinal Nerves- 31 pairs• Emerge from spinal cord between vertebrae• All are mixed nerves
– Cell bodies of sensory neurons are located in dorsal root ganglia
– Ventral roots contain axons of motor neurons
Cranial and Spinal Nerves
17.4 The Peripheral Nervous System
• Divisions of the Peripheral Nervous System
– The Somatic System
– The Autonomic System

17.4 The Peripheral Nervous System
• Somatic System– Serves the skin, skeletal muscles and tendons
– Includes nerves that carry sensory information from
receptors to the CNS and nerves that carry motor
responses to muscles
– Some actions are due to reflexes• Automatic responses to a stimulus
– Some actions are voluntary

A Somatic Reflex

17.4 The Peripheral Nervous System
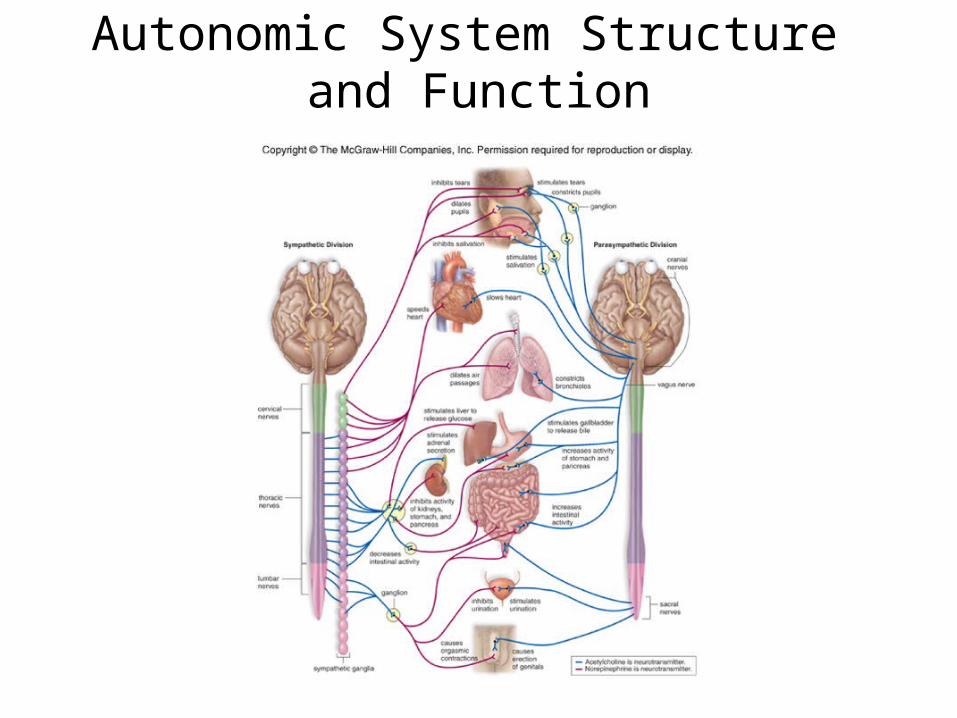
• Autonomic System– Regulates the activity of cardiac and smooth muscle
and glands– Two Divisions
• Sympathetic and Parasympathetic Nervous Systems• Features in common
– Function automatically and generally are involuntary– Innervate all internal organs– Pathway consists of two motor neurons that synapse at a
ganglion» The first is the preganglionic neuron and its cell body is in
the CNS» The second is the postganglionic neuron and its cell body
is in the ganglion

17.4 The Peripheral Nervous System
• Autonomic System– Cell bodies of preganglionic neurons are in the thoracic and
lumbar regions of the spinal cord– Preganglionic neurons are short, postganglionic neurons are
long– The sympathetic division stimulates the release of epinephrine
and norepinephrine from the adrenal medulla– Mediates the “fight or flight” response
• Increases heart rate and contractility, dilates bronchi• Inhibits the digestive tract

17.4 The Peripheral Nervous System
• Parasympathetic Division– Includes a few cranial nerves and fibers that arise
from the sacral portion of the spinal cord– Preganglionic fibers are long, postganglionic fibers
are short– Mediates “rest and digest” functions
• Promotes digestion• Decreases heart rate
– Neurotransmitter is acetylcholine
Autonomic System Structure and Function
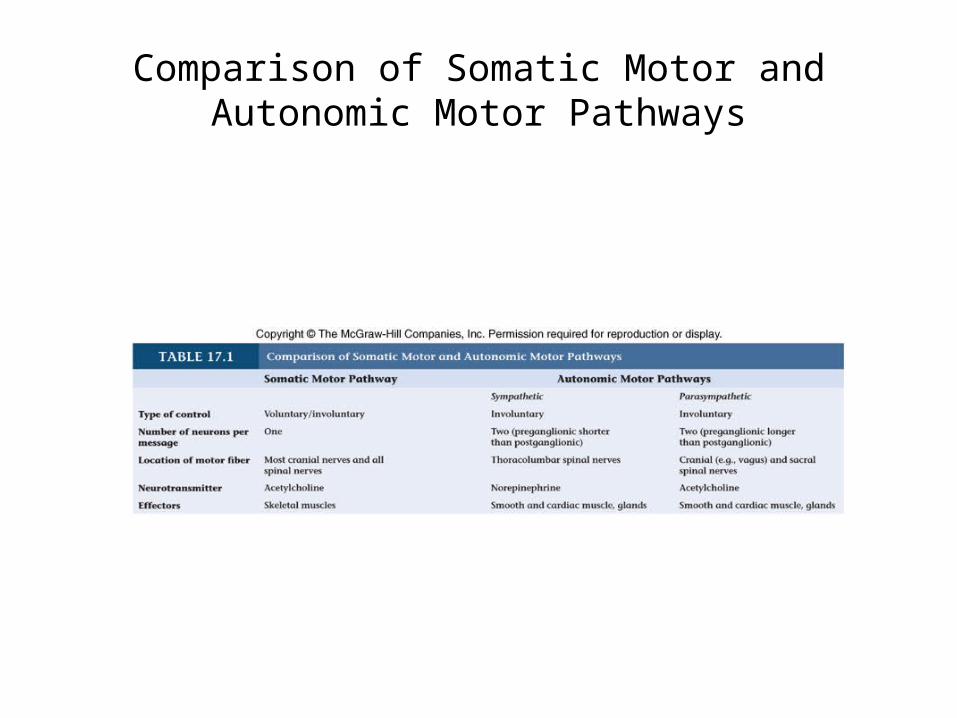
Comparison of Somatic Motor and Autonomic Motor Pathways

17.5 Drug Abuse
• Action of Drugs– Impact the limbic system or– Affect the action of neurotransmitter (synapse)
– Stimulants: increase neuron excitation– Depressants: decrease neuron excitation
– Dopamine is one neurotransmitter involved with physical dependence (addiction)
17.5 Drug Abuse
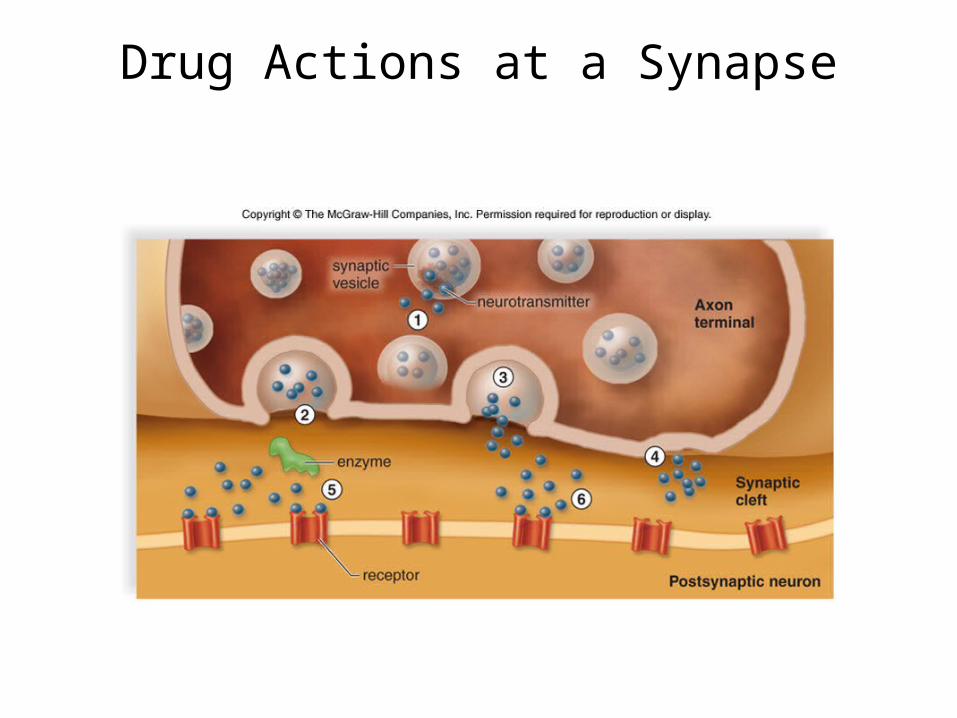
• Drug Actions at a Synapse– Cause the release of a neurotransmitter from a
synaptic vesicle into the axon terminal– Prevent the release of a NT– Promote the release of a NT– Prevent the reuptake of a NT– Block enzymatic breakdown of a NT– Mimic the action of a NT by binding to a receptor
Drug Actions at a Synapse

17.5 Drug Abuse
• Some Specific Drugs of Abuse

17.5 Drug Abuse
• Nicotine– Found in tobacco products– Causes a release of epinephrine
• Increases blood sugar levels• Then blood sugar levels fall, depression and fatigue set in
– In the CNS, nicotine causes the release of dopamine• This has a reinforcing effect leading to drug dependence
– Nicotine caused both physiological and psychological dependence

17.5 Drug Abuse
• Alcohol– Influences GABA (inhibitory neurotransmitter) and
glutamate (excitatory neurotransmitter)– Metabolized in the liver
• Prevents liver from breaking down fats• Fat accumulates in liver-after only 1 night of drinking!!!!
– First stage of damage– Reversible
• Continued consumption causes fibrous scar tissue formation– Still reversible
• Long term consumption causes cirrhosis– Liver cells die– irreversible

17.5 Drug Abuse
• Alcohol– Alcohol is a carbohydrate– Can be used as energy source
• Lacks vitamins, minerals, essential amino acids, fatty acids
– Alcoholics are vitamin-deficient, undernourished, and prone to illness
– Alcohol freely crosses the placenta• Leads to fetal Alcohol Syndrome
– Mental retardation – Physical defects

17.5 Drug Abuse
• Marijuana– Cannibus sativa– Resins contain THC- tetrahydrocannabinol– Binds to receptors for anandamide
• Influence short-term memory processing• Creates feeling of contentment
– Short term use causes mild euphoria, alterations in judgment and motor coordination
– Heavy use causes anxiety, paranoia, psychotic symptoms
– Long-term use leads to brain impairment
17.5 Drug Abuse
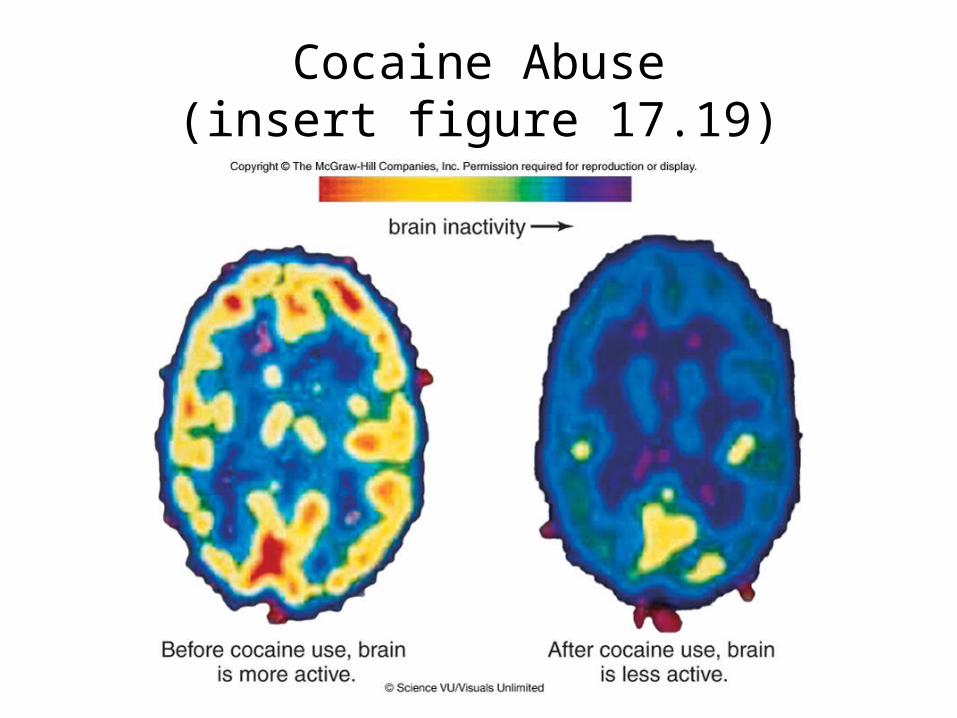
• Cocaine and Crack– Derived from the shrub Erythroxylon coca– Prevents synaptic uptake of dopamine
• Accounts for state of euphoria– Binge phase of cocaine use
• Hyperactivity, decreased appetite, increased sex drive– Crash phase
• Depression, irritability, decreased sex drive (impotency in males)
– Cocaine causes extreme physical dependence• Users develop a tolerance and an intense craving for the
drug• Overdosing causes seizures and cardiac arrest
Cocaine Abuse(insert figure 17.19)

17.5 Drug Abuse
• Heroin– Derived from morphine which is an alkaloid of opium– Heroin binds to endorphin receptors
• Produces euphoria, pain relief• Side effects include nausea, vomiting, restlessness, anxiety,
mood swings• Over time body stops producing natural endorphins
– Tolerance develops. A user must take more drug just to prevent withdrawal symptoms• Perspiration, tremors, dilated pupils, cramps, increased
blood pressure and respiratory rate– Heroin may cause convulsions, respiratory failure,
and death
17.5 Drug Abuse
• “Club” Drugs– Ecstasy (MDMA)
• Chemically similar to methamphetamine• May increase feelings of well being• Other effects are an increase in heart rate and blood
pressure, muscle tension, and blurred vision• MDMA may interfere with temperature regulation and also
cause damage to the liver, heart, and kidneys.• Chronic use leads to memory damage and depression
– Rohypnol– Ketamine
17.5 Drug Abuse
• “Club” Drugs– Rohypnol (roofies)
• A sedative• When mixed with alcohol, victims may be incapable of
resisting (ex: sexual assault)• Victims may not remember anything that happened while
using the drug– Ketamine
• Used by veterinarians as an anesthetic• Can cause dangerous reductions in heart and respiratory
functions• It can render a victim unable to move
– Sometimes used as a date rape drug

17.5 Drug Abuse
• Methamphetamine – Called “meth” or “crank”– Many times made in make-shift home laboratories– An ingredient found in cold medicines is a component
of the drug– Large amounts of dopamine stay in a synapse– After an initial rush, irritability and violent behavior
may set in– Chronic use leads to paranoia, tremors,
cardiovascular collapse, and death– Users develop a tolerance and an intense craving for
the drug

17.6 Disorders of the Nervous System
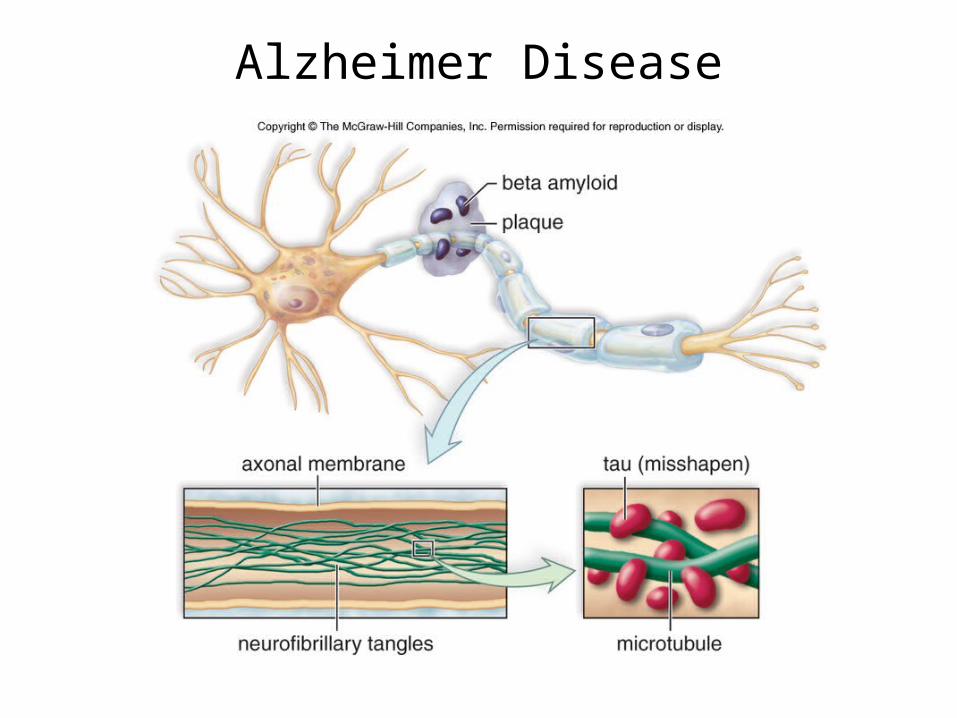
• Disorders of the Brain– Alzheimer Disease (AD)
• Most common cause of dementia• AD is chronic and progressive• Loss of memory (of recent events) is an early symptom• Abnormal neurons especially in the hippocampus and
amygdala– Plaques– Neurofibrillary tangles
• Several genes have been identified that predispose a person to AD
Alzheimer Disease

17.6 Disorders of the Nervous System
• Parkinson Disease (PD)– Gradual loss of motor control
• Typically begins between 50 and 60 years of age– Later characteristics include tremors and muscle
rigidity, speaking may be difficult– Caused by a degeneration of dopamine producing
neurons– Dopamine (as a drug) cannot be administered
because it cannot cross the blood-brain barrier– L-dopa is a drug that the body can convert to
dopamine, at least for a while
17.6 Disorders of the Nervous System
• Multiple Sclerosis (MS)– Affects the myelin sheath of white matter in the brain– MS in an autoimmune disease– Symptoms include: Fatigue, muscle weakness, vision
problems, tingling or numbness– MS can take several forms (mild severe)– No treatment is available, but the progression can be
slowed

Multiple Sclerosis

17.6 Disorders of the Nervous System
• Stroke– A disruption to the blood supply in the brain– Two major forms:
• Hemorrhagic: Small arteries leak blood into the brain• Ischemic: Sudden loss of the blood supply to an area
of the brain
– Symptoms depend on the amount and area of the brain tissue that is affected
– Factors such as age and race influence the likelihood of having a stroke

17.6 Disorders of the Nervous System
• Meningitis– An infection of the meninges that surround the brain
and spinal cord caused by bacteria or viruses– Infection may spread into the brain tissue– A diagnoses is usually confirmed by sampling
cerebrospinal fluid– A vaccine is available for protection against some
types of the disease
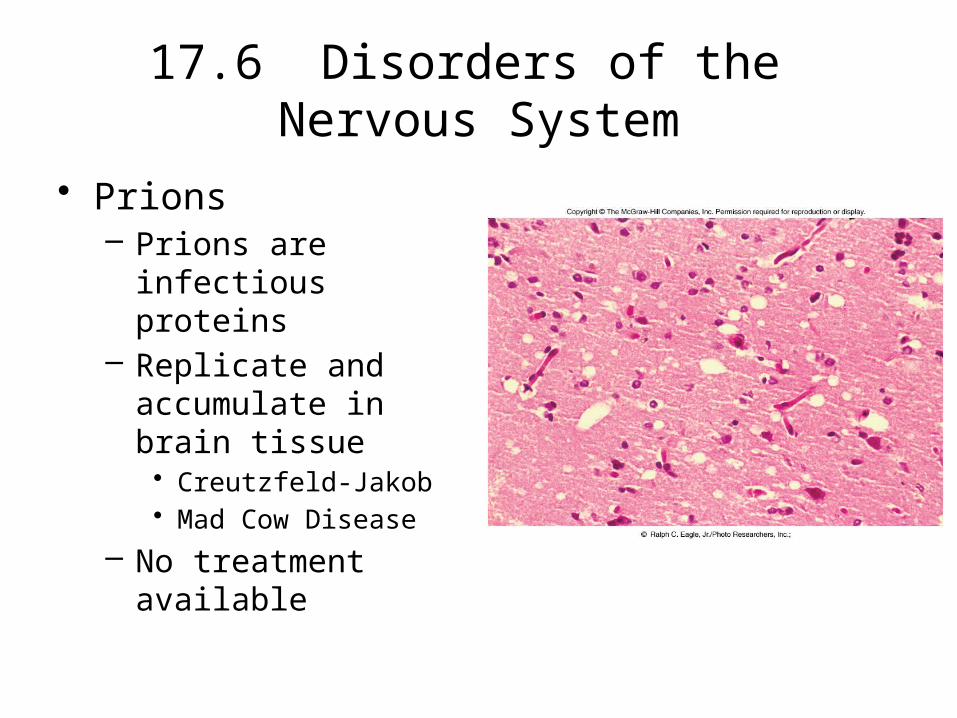
17.6 Disorders of the Nervous System
• Prions – Prions are infectious
proteins– Replicate and
accumulate in brain tissue• Creutzfeld-Jakob• Mad Cow Disease
– No treatment available
17.6 Disorders of the Nervous System
• Disorders of the Spinal Cord– Spinal cord injuries may stop impulses from traveling
along neurons in the spinal cord.• This can result in paralysis of the areas located below the
site of injury
– Amyotrophic Lateral Sclerosis (ALS)• Also called Lou Gehrig’s disease• Affects the motor nerves of the spinal cord• Incurable, people usually die within five years of diagnosis• There may be multiple causes of nerve cell death

17.6 Disorders of the Nervous System
• Disorders of the Peripheral Nerves– Guillain-Barre Syndrome (GBS)
• Demyelination of of peripheral nerve axons• Hypothesized to result from abnormal immune reactions• Muscle weakness begins in the lower limbs then ascends to
the upper limbs• Patients usually recover within a year
17.6 Disorders of the Nervous System
• Disorders of the Peripheral Nerves– Myasthenia Gravis (MG)
• An autoimmune disease• Antibodies react against acetylcholine receptors of
skeletal muscles, ACh cannot bind• Muscle weakness can lead to death if untreated• Patients respond well to immunosuppressive drugs
and ACh inhibitors