instructions for form submission - bcbsm.com the registration form and attachments ... for allied...
TRANSCRIPT

WF 10577 AUG 12 Page 1 of 10
Provider EnrollmentBlue Cross Blue Shield of MichiganP.O. Box 217,Southfield Mi, 48034
Questions? Call 1-800-822-2761
3. You can also mail the completed forms and documentation to:
2. Fax the registration form and attachments (i.e., signature documents) to 1-866-900-0250. Forms for multiple practitioners and groups cannot be bundled into one fax transmission.
1. BCBSM’s fax cover sheet must be the first page of your form submission. Not your personal fax cover sheet.
Instructions for form submission
Tax identification number. Type 2 NPI National Provider Identifier. Date (MM/DD/YY). From (Insert name of contact person).For group practices. Tax identification number. Type 2 NPI National Provider Identifier. Date (MM/DD/YY). From (Insert name of contact person).For allied providers.
Instructions for fax cover sheet
We cannot accept handwritten forms. To ensure forms are processed timely,please adhere to the following instructions:
1. Do not hand write anywhere on the fax cover sheet, otherwise processing will be delayed.
2. Enter all information online; press the tab key after each entry to move from field to field.
For individual practitioners.Type 1 NPI National Provider Identifier. Date (MM/DD/YY). From (Insert name of contact person).10 digit state license number.When adding an individual to an existing group be sure toinclude your group’s Type 2 National Provider Identifier and a group change form
.

WF 10577 AUG 12
Blue Cross Blue Shield of Michigan is a nonprofit corporation and independent licensee of the Blue Cross and Blue Shield Association.
10577Form Number:
Mail to: Provider EnrollmentBlue Cross Blue Shield of Michigan
Southfield, MI 48034P.O. Box 217
Date:
From:
Fax To: 866-900-0250 Provider Enrollment
IMPORTANT: Attach this page to the top of your document toavoid processing delays.
FAX OR MAIL COVER SHEETFOR DOCUMENTS
Page 2 of 10
Type 1 NPI:
State License Number:
Type 2 NPI:
NEW ALLIED PRACTITIONER ENROLLMENT FORM

Type 1 National provider identifier
Please complete this form if you are an anesthesia assistant, audiologist, certified nurse mid-wife, certified nurse practitioner, certified registered nurse anesthetist, hearing aid dealer, optometrist orthotic supplier, physician assistant, prosthetic supplier, or prosthetic and orthotic supplier (with an individual certification) applying to Blue Cross Blue Shield of Michigan and Blue Care Network for the first time. Note: If you are an orthotic supplier, prosthetic supplier or prosthetic and orthotic supplier with a facility certification, please complete the New Allied Provider Enrollment form.
State license number
WF 10577 AUG 12 Page 3 of 10
You (except anesthesia assistants) are required to complete and maintain a credentialing application through the Council for Affordable Quality Healthcare® at http://upd.caqh.org/oas/ In order for your managed care affiliation request to be processed you must complete your CAQH application within 14 calendar days. If you have already completed a CAQH application, your attestation must be up to date. If your CAQH application is not complete or if your attestation is expired after 14 calendar days, your request will be closed and you will need to reapply using the Allied Provider Change form.
Type 2 National provider identifier
*First name Middle name
*Last nameSuffix II III IV Jr. Sr.
*What type of providerare you?
anesthesia assistant
audiologistcertified nurse midwife
hearing aid dealercertified registered nurse anesthetistcertified nurse practitioner
*County where your primary addrerss is located
*Degree *Date of birth
Gender Male Female Preferred saluation Dr. Ms. Mrs. Mr. Miss
Section 1: Demographic Data
optometrist
orthotic supplier
prosthetic supplier
physician assistantprosthetic & orthotic supplier
NEW ALLIED PRACTITIONER ENROLLMENT FORM
*denotes a required field
Section 1: Demographic Data - continued
WF 10577 AUG 12 Page 4 of 10
Race/Ethnicity
Black or African AmericanWhite/Caucasian
American Indian or Alaska Native
Chinese/Chinese-AmericanAsian
FilipinoJapanese/Japanese-AmericanKorean
Native Hawaiian or other Pacific Islander
Vietnamese
Mexican/Mexican-AmericanHispanic/Latin AmericanArabOther RaceAssyrian/ChaldeanOther AsianMultiracial
Section 2: Employer ID number/Tax information
*Social Security number
*Is your EIN/Tax ID number the same as your SSN?
Tax exempt
EIN/Tax name as indicated on IRS document
Yes No
If you would like to bill with your Type 2 NPI (National provider identifier) representing your incorporated individual business, you must also complete a New Group Enrollment form to register this entity as a group.
Type 1 National provider identifier State license number
Not Disclosed
Type 2 National provider identifier
If registered with CAQH, CAQH ID number:
*denotes a required field
Yes No (If no. enter Tax ID number)
EIN/Tax ID number
NEW ALLIED PRACTITIONER ENROLLMENT FORM
WF 10577 AUG 12 Page 5 of 10
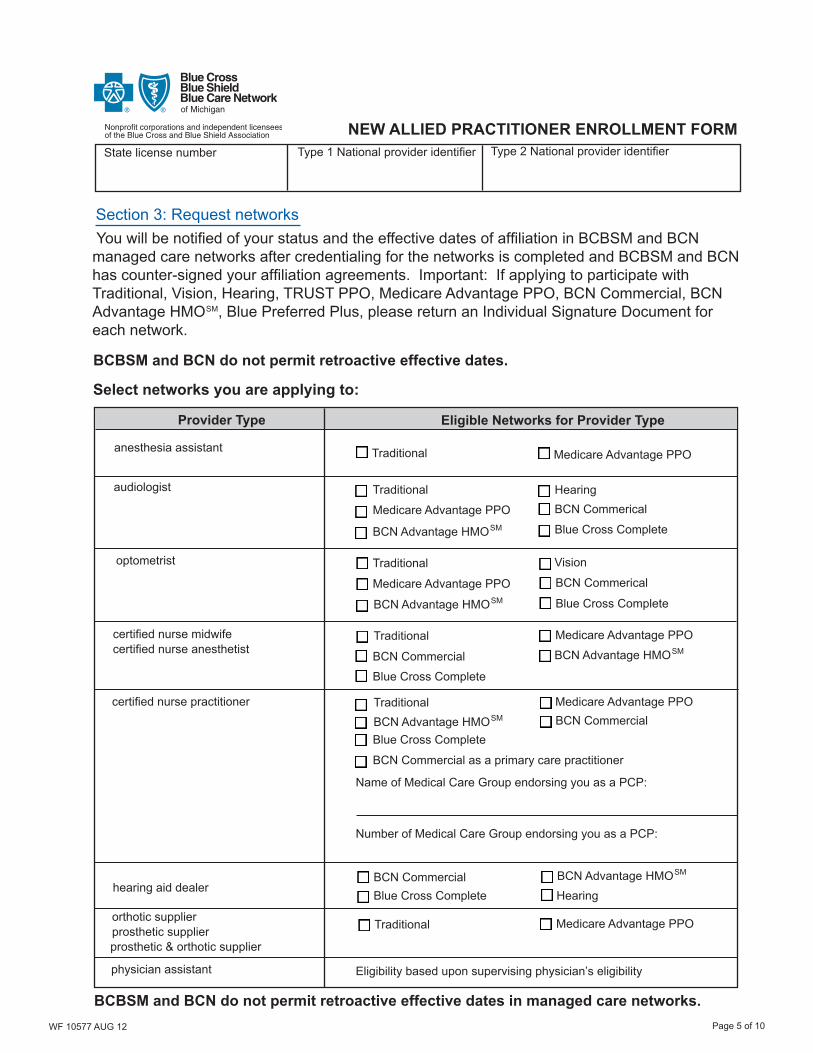
BCBSM and BCN do not permit retroactive effective dates.
Section 3: Request networks You will be notified of your status and the effective dates of affiliation in BCBSM and BCN managed care networks after credentialing for the networks is completed and BCBSM and BCN has counter-signed your affiliation agreements. Important: If applying to participate with Traditional, Vision, Hearing, TRUST PPO, Medicare Advantage PPO, BCN Commercial, BCN Advantage HMO , Blue Preferred Plus, please return an Individual Signature Document for each network.
Select networks you are applying to:
Provider Type Eligible Networks for Provider Type
anesthesia assistant
optometrist
certified nurse midwife
hearing aid dealer
Traditional
Hearing
Medicare Advantage PPO
BCN Commercial
BCN Advantage HMOSM
Traditional
BCN Commercial
BCN Commerical
BCN Advantage HMOSM
audiologist
Medicare Advantage PPO
Traditional Vision
BCN CommericalMedicare Advantage PPO
BCN Advantage HMOSM
certified nurse anesthetistTraditional Medicare Advantage PPO
certified nurse practitioner Traditional Medicare Advantage PPO
BCN Advantage HMOSM
BCN Commercial as a primary care practitioner
Name of Medical Care Group endorsing you as a PCP:
Number of Medical Care Group endorsing you as a PCP:
BCN Commercial BCN Advantage HMOSM
Traditional Medicare Advantage PPO orthotic supplierprosthetic supplierprosthetic & orthotic supplier
BCBSM and BCN do not permit retroactive effective dates in managed care networks.
Type 1 National provider identifier State license number
Blue Cross Complete
Blue Cross Complete
Blue Cross Complete
Blue Cross Complete
Blue Cross Complete
Type 2 National provider identifier
SM
NEW ALLIED PRACTITIONER ENROLLMENT FORM
physician assistant Eligibility based upon supervising physician’s eligibility
Hearing

WF 10577 AUG 12 Page 6 of 10
Type 1 National provider identifier State license number Type 2 National provider identifier
Section 4: Address Data *denotes a required field
Primary address (must be an address where health care services are rendered and may be published in BCBSM/BCN provider directories)
*Primary Telephone Number Fax Number
*Street Address
*City *State *Zip Code
Primary Telephone Number must be a phone number patients can call to make an appointment.
Payment/Remit address (if different from your primary address)Street Address
City State Zip Code
Mailing address (if different from your primary address)Street Address
City State Zip Code
Payment/Remit telephone number (if different from your Primary telephone number)
Mailing contact name Mailing contact phone number
Primary address - Accessiblity
*Handicap accessibility: Yes No *Accessible by train: Yes No *Accessible by bus: Yes No
Credentialing Contact informationPlease provide the name and contact information of a person who can answer questions about information in this application
* First Name Last Name
* Telephone Number Fax Number
Email Preferred method of contact? Email US Mail
extension
NEW ALLIED PRACTITIONER ENROLLMENT FORM
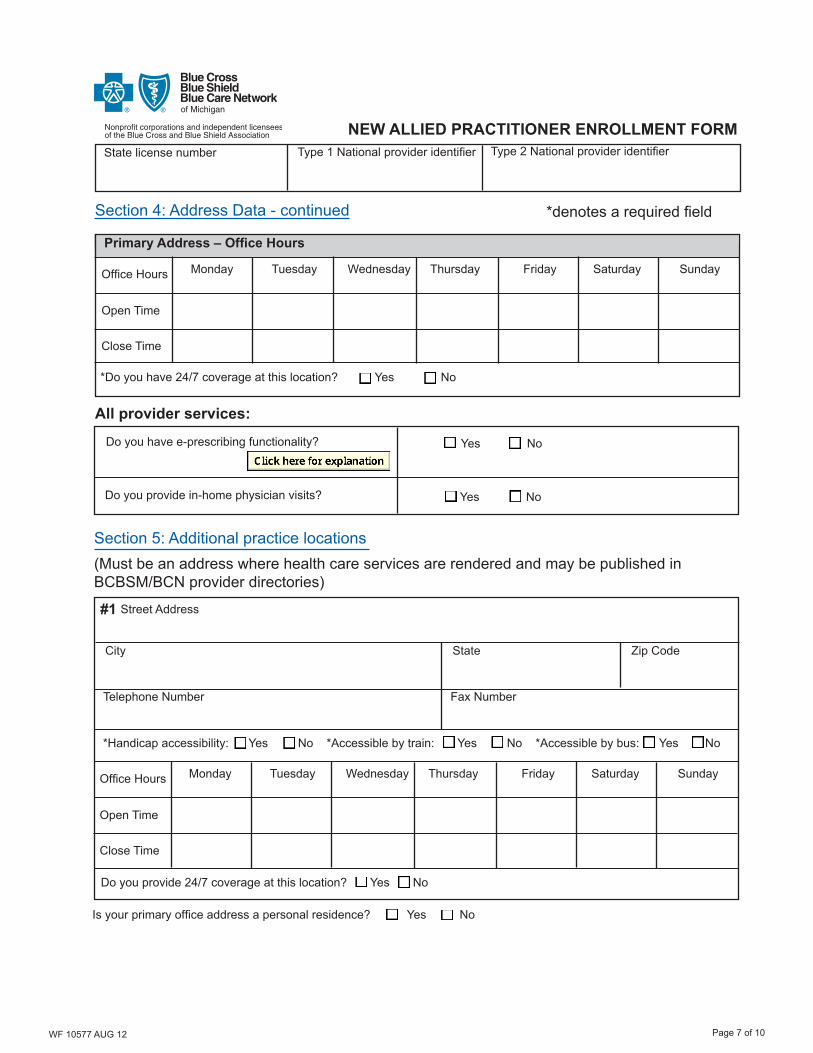
Is your primary office address a personal residence? Yes No
WF 10577 AUG 12 Page 7 of 10
Type 1 National provider identifier State license number
Section 5: Additional practice locations
Street Address
City State Zip Code
#1
*Handicap accessibility: Yes No *Accessible by train: Yes No *Accessible by bus: Yes No
Telephone Number Fax Number
Close Time
Open Time
Office Hours Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Do you provide 24/7 coverage at this location? Yes No
Type 2 National provider identifier
Section 4: Address Data - continued
Primary Address – Office Hours
Close Time
Open Time
Office Hours Monday Tuesday Wednesday Thursday Friday Saturday Sunday
*Do you have 24/7 coverage at this location? Yes No
*denotes a required field
All provider services:
Do you have e-prescribing functionality? Yes No
Do you provide in-home physician visits? Yes No
(Must be an address where health care services are rendered and may be published in BCBSM/BCN provider directories)
NEW ALLIED PRACTITIONER ENROLLMENT FORM
Is your primary office address a personal residence? Yes No
WF 10577 AUG 12 Page 8 of 10
Type 2 National provider identifier State license number Type 2 National provider identifier
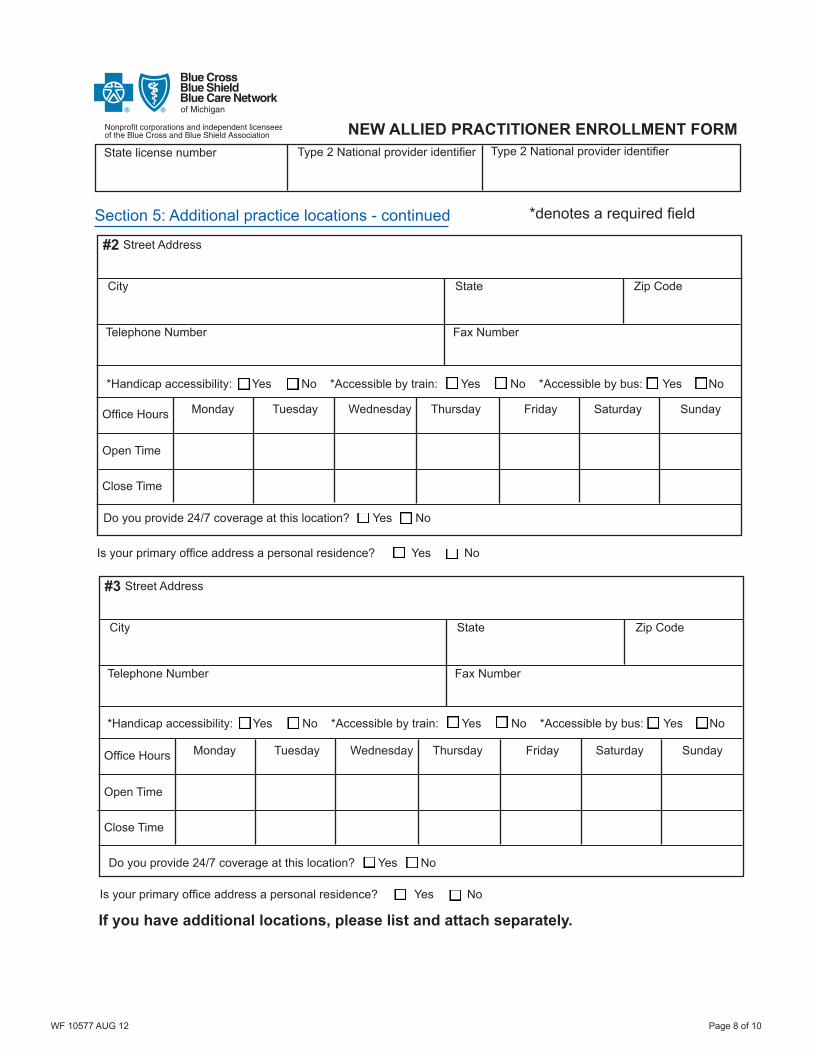
Section 5: Additional practice locations - continued
Street Address
City State Zip Code
#2
*Handicap accessibility: Yes No *Accessible by train: Yes No *Accessible by bus: Yes No
Telephone Number Fax Number
Close Time
Open Time
Office Hours Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Do you provide 24/7 coverage at this location? Yes No
Street Address
City State Zip Code
#3
*Handicap accessibility: Yes No *Accessible by train: Yes No *Accessible by bus: Yes No
Telephone Number Fax Number
Close Time
Open Time
Office Hours Monday Tuesday Wednesday Thursday Friday Saturday Sunday
Do you provide 24/7 coverage at this location? Yes No
If you have additional locations, please list and attach separately.
*denotes a required field
NEW ALLIED PRACTITIONER ENROLLMENT FORM
Is your primary office address a personal residence? Yes No
Is your primary office address a personal residence? Yes No

WF 10577 AUG 12 Page 9 of 10
Type 2 National provider identifier Type 1 National provider identifier State license number
Section 6: Provider Secured Services *denotes a required field Doing business electronically saves your office time and money. We encourage you to sign up for Provider Secured Services, a free service for BCBSM and BCN participating providers that allows you to view patient eligibility, track claims, and much more online. Begin the process by completing the information in the section below:
Authorized Web Access AdministratorProvide the name and contact information of the person who is the authorized Web Access Administrator with delegated authority to manage all access to protected health information and group practitioner records using provider secured (web) self services.* Name (type or print) *Title
* Telephone Number *E-mail
* Does the practice currently use Provider Secured Services? Yes No
Provider Secured Services AccessComplete the section below for individuals that do not have an existing Provider Secured Services(web-DENIS) login ID. Only check off the minimum necessary features for each user listed below.
* Name (full legal name of each user) *Telephone Number
EligibilityCoverageSearches Only
Claims Tracking & EFT
Provider Claims Correction (PCC)
For BCBSM Use Only
* Name 1. * Telephone Number
* Name 2. * Telephone Number
* Name 3. * Telephone Number
* Name 4. * Telephone Number
NEW ALLIED PRACTITIONER ENROLLMENT FORM
Existing Provider Secured Service users that would like to update their access to include the NPI (s)indicated on this form complete:
Section 6A: Professional/Facility Providers - Authorization to update user access for Provider Secured Services
Section 6B: Billing Services - Authorization to update user access for Provider Secured Services
BCN PCP ClaimsSummary
e-referral(BCN Only)
If no and you are requesting user access below, complete the Use and Protection Agreement and return with this application.

*Print or Type Name *Practitioner Signature/Title *Date
Section 7: Application signature *denotes a required field
Provider Secured Services
Type 2 National provider identifier Type 1 National provider identifier State license number
WF 10577 AUG 12 Page 10 of 10
NEW ALLIED PRACTITIONER ENROLLMENT FORM
The authorized signer agrees that he/she has the company’s designated authority to request and maintain minimum necessary Web access and is responsible for complying with all terms and conditionscontained within the Provider Secured Services Use and Protection Agreement.
Section 6A: Professional/Facility Provider - Authorization to update user access for ProviderSecured Services
Enter the user ID(s) below to be updated with the NPI(s) indicated on this form.
Section 6B: Billing Services - Authorization to update user access for Provider Secured Services
Complete Addendum “B” Authorization for Representative Access (PDF) to add NPI(s) to your existing Provider Secured Service ID.
.
I certify that:The information contained in this application is true and complete. I will notify Blue Cross Blue Shield of Michigan and Blue Care Network immediately in writing of changes affecting this data. If I am a practitioner in training, I will not report services that are related to my training program and rendered at the address from which I am training. Should I re-enter training, I will notify BCBSM and BCN.
.