insulin pump, daily injections and cardiovascular mortality · blood pressure as used by the ndr is...
TRANSCRIPT

Confidential: For Review O
nly
Insulin Pump, Daily Injections and Cardiovascular Mortality
- 18,168 Individuals with Type 1 Diabetes in the Swedish
National Diabetes Register (NDR)
Journal: BMJ
Manuscript ID: BMJ.2014.024170
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 04-Dec-2014
Complete List of Authors: Steineck, Isabelle; Aarhus Universitet, Endocrinology Cederholm, Jan; Uppsala University, Department of Public Health and Caring Sciences / Family Medicine and Clinical Epidemiology Eliasson, Björn; University of Gothenburg, Medicine Rawshani, Araz; Gothenburg University, ; University of Gothenburg, Medicine Eeg-Olofsson, Katarina; University of Gothenburg, Medicine Zethelius, Björn; Uppsala University, Department of Public Health and Caring Sciences / Family Medicine and Clinical Epidemiology Svensson, Ann-Marie; University of Gothenburg, Medicine; Centre of Registers in Region Västra Götaland, Avdic, Taric; University of Gothenburg, Medicine; Centre of Registers in Region Västra Götaland, Landin-Olsson, Mona; Clinical sciences, Department of Endocrinology Jendle, Johan; Örebro University, Health Sciences and Medicine Gubörnsdottir, Soffia; University of Gothenburg, Medicine; Centre of Registers in Region Västra Götaland,
Keywords: cardiovascular diseases, continuous subcutaneous insulin infusion , diabetes , epidemiology , multiple daily injections , mortality
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review O
nly
1
Insulin Pump, Daily Injections and Cardiovascular Mortality -
18,168 Individuals with Type 1 Diabetes in the Swedish National
Diabetes Register (NDR)
Isabelle Steineck, MD 1, Jan Cederholm, MD, PhD 2, Björn Eliasson, MD, PhD 3, Araz
Rawshani, MD 4, Katarina Eeg-Olofsson MD, PhD 3, Ann-Marie Svensson PhD 4, Björn
Zethelius MD, PhD 5, Tarik Avdic 4, Mona Landin-Olsson, MD, PhD 6, Johan Jendle MD,
PhD 7, Soffia Gudbjörnsdóttir, MD, PhD 3, 4
1 Department of Endocrinology Aarhus University Hospital, Aarhus Denmark 2 Department of Public Health and Caring Sciences/Family and Preventive Medicine, Uppsala University, Uppsala, Sweden 3 Institute of Medicine, Sahlgrenska University Hospital, University of Gothenburg, Gothenburg, Sweden 4 National Diabetes Register, Centre of Registers, Gothenburg, Sweden 5 Department of Public Health and Caring Sciences/Geriatrics, Uppsala University, Scientific Director, Medical Products Agency, Uppsala, Sweden 6 Department of Clinical Science, Lund University, Lund, Sweden 7 Faculty of Health Sciences and Medicine, Örebro University, Örebro, Sweden.
Corresponding Author:
Isabelle Steineck, M.D., Department of Endocrinology, Aarhus University Hospital, Aarhus, Denmark Mobile phone: +45-5151 9085 e-mail: [email protected]
Word count: Abstract 216 words, text 3305 words, three tables, one figure and 37
references
Page 1 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
2
Abstract
Objective No previous studies of long-term effects of continuous subcutaneous insulin
infusion (CSII) on cardiovascular diseases (CVD) and mortality in individuals with type 1
diabetes have been published.
Design Observational study.
Setting Sweden 2005 – 2012.
Participants 18,168 individuals with type 1 diabetes, 2,441 on insulin pump therapy and
15,727 on multiple daily insulin injections (MDIs).
Main outcome measures Cox regression analysis was used to estimate hazard ratios (HRs)
for the outcomes, using stratification of propensity scores including clinical characteristics,
CVD risk factors, treatments and previous diseases.
Results Follow-up was mean 6.8 years until December 2012, with 114,135 person-years.
Adjusted HRs with CSII vs. MDIs as a reference showed significant risk reductions for fatal
or nonfatal coronary heart disease (CHD), 20 % (p=0.043), fatal CVD (CHD or stroke), 45%
(p=0.002), and all-cause mortality, 31% (p=0.002). Non-significant risk reductions were seen
for fatal or nonfatal CVD and non-CVD mortality. Subgroups showed similar results
excluding lower BMI and previous cardiovascular diseases. A sensitivity analysis of
unmeasured confounders in all individuals disclosed that such an unmeasured confounder
with HR of 1.3 should be present in >80% of the MDIs-treated individuals versus no presence
in CSII-treated to invalidate the significant risk reduction for fatal CVD.
Conclusion As done in Sweden at the time, CSII implied a lower cardiovascular mortality
than MDIs.
Keywords: diabetes, cardiovascular diseases, epidemiology, multiple daily injections,
continuous subcutaneous insulin infusions, CSII
Page 2 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
3
Introduction
Nobody disputes the fact that type 1 diabetes increases the risk of death from cardiovascular
diseases (CVD). A recent study from the Swedish National Diabetes Register showed that
individuals with type 1 diabetes who have a glycated hemoglobin (HbA1c) level of 6.9% (52
mmol per mole) or lower, have a risk of death from any cause and from cardiovascular causes
twice as high as those in the general population; the risks are several times as high among
patients with poor glycaemic control.1 Evidently, close glucose control reduces the risk,
delays the onset and slows the progression of complications .2 Recent studies have indicated
that not only hyperglycaemia, but hypoglycaemia, is a risk factor for CVD.3 Continuous
subcutaneous insulin infusion (CSII) by a pump may result in fewer episodes of
hyperglycaemia and hypoglycaemia than multiple daily injections (MDIs).4, 5 Some studies
have shown CSII to provide better glycaemic control than MDIs.6 Given the importance of
glycaemic control, and the presumed advantages of CSII,1 it is important to investigate
whether CSII affects the risk of CVD mortality.
In 2013, one out of every four Swedish women and one out of every five Swedish men with
type 1 diabetes used CSII. Over half of all Swedish children with type 1 diabetes are using
CSII.7 Sceptics argue that CSII may increase treatment costs and cause practical problems for
individuals with diabetes. Due to the scarcity of data, we do not know whether CSII increases
the risk of death from CVD as compared to MDIs.
Sweden offers excellent opportunities for studying individuals with type 1 diabetes. All
Swedes with type 1 diabetes enjoy health care at a negligible personal cost. About 95% of all
individuals with type 1 diabetes have been entered in the National Diabetes Register, which
includes detailed clinical data from each appointment. The register can be linked via
Page 3 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
4
Sweden’s unique personal identity number to the cause of death, in-patient, socioeconomic
and other population-based registers. Our aim was primarily to analyse the effect of CSII on
CVD mortality.
Methods
Swedish National Diabetes Register (NDR)
The NDR was initiated in 1996 as a caregiver tool for local quality assurance and to provide
feedback as part of diabetes care. Annual reporting to the NDR is performed by trained
doctors and nurses either online or through clinical record databases. Information is collected
during appointments at hospital outpatient clinics and primary healthcare centres nationwide.
All individuals with diabetes give their informed consent before being entered. The Regional
Ethical Review Board at the University of Gothenburg approved this study. Several previous
reports have been published concerning trends in risk factor control and risk prediction based
on the NDR.8-12
Subjects
We included 18,168 individuals with type 1 diabetes entered in the NDR for whom data were
available about the use of insulin pump or MDIs. A total of 2,441 individuals were being
treated with CSII during the study period and 15,727 with MDIs during the study period.
Type 1 diabetes was epidemiologically defined as all individuals with insulin treatment only
(concerning diabetes mellitus) and onset age less than 30, almost all of whom had been
reported by outpatient clinics at Swedish hospitals. Baseline appointments were in 2005-2007
with follow-up until 31 December 2012. All individuals were recruited from the NDR with no
exclusion criteria.
Page 4 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
5
Examinations at baseline and at the end of the study
Clinical characteristics at baseline were type of glucose lowering treatment, age, diabetes
duration, gender, HbA1c, systolic blood pressure, diastolic blood pressure, height, weight,
waist circumference, physical activity, smoking habits, total cholesterol, HDL cholesterol,
triglycerides, micro-albuminuria, plasma creatinine, antihypertensive drugs, lipid-lowering
drugs, atrial fibrillation, history of CVD, heart failure, use of acetylsalicylic acid (aspirin) and
educational level. This information was obtained from Statistics Sweden. Body mass index
(kg/m2) was calculated as weight/height2. Waist circumference (cm) was measured at the
height of the navel. Physical activity was graded as low (no activity or less than once a week)
or high (2 or more times a week). Smoking was defined as one or more cigarettes per day, a
pipe per day or having quit within the past three months. The Swedish standard for recording
blood pressure as used by the NDR is the average (mmHg) of two supine readings (Korotkoff
1–5) with a cuff of appropriate size after at least 5 minutes of rest. HbA1c analyses were
quality assured nationwide by regular calibration using the HPLC Mono-S method and then
converted to mmol/mol [International Federation of Clinical Chemistry (IFCC)].13
Albuminuria was urine albumin excretion >20µg/min on two out of three consecutive tests
(micro-albuminuria or macro-albuminuria). We stratified educational level into lower (≤9
years), intermediate (10-12 years [upper secondary school]) and higher (college/university). A
history of CVD was defined the same way as for the outcome; a history of heart failure was
defined as ICD-10 code I50; atrial fibrillation prior to study start was defined as ICD-10 code
I48; previous all-cancer was defined as ICD-10 codes C00-C097; previous liver disease was
defined as ICD-10 codes K70-74; and mental disorders were defined as ICD-10 codes F20-29
and F30-39.
Follow-up, definition of endpoints
Page 5 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
6
All individuals were monitored from the baseline examination until death or the first incident
or until 31 December 2012. The mean follow-up period was 6.8 years, for a total of 114,135
person-years. The major primary endpoints were fatal or nonfatal coronary heart disease
(CHD), fatal or nonfatal CVD, fatal CVD and total mortality. Nonfatal CHD was defined as
nonfatal myocardial infarction (ICD-10 code I21), unstable angina (ICD-10 code I20.0),
percutaneous coronary intervention and/or coronary artery bypass grafting. Fatal CHD was
defined as ICD-10 codes I20-I25. Stroke was defined as fatal or nonfatal cerebral infarction,
intracerebral haemorrhage or unspecified stroke (ICD-10 codes I61, I63, I64). CVD was
defined as the composite of CHD or stroke, whichever came first. A secondary endpoint was
non-CVD mortality.
A history of heart failure was defined as ICD-10 code I50, and atrial fibrillation prior to study
start was defined as ICD-10 code I48. All events were obtained by linking to the Swedish
Cause of Death and Hospital Discharge registers, a reliable, validated alternative to revised
hospital discharge and death certificates.14, 15
Statistical analysis
Five imputations using the Markov Chain Monte Carlo technique were applied for missing
data in the sample of 18,168 individuals, using the SAS MI and MIANALYSE procedures.
Table 1 shows baseline clinical features as mean values (SD) or frequencies (%) of each
multiple imputed variable in the two treatment groups (CSII or MDIs), with significance
values for crude differences between the two groups using student’s t-test or X2 test.
Significance values are also shown for differences between the groups after adjustment with a
propensity score, including all variables listed in Table 1, estimated by General Linear Models
(GLM) or logistic regression.
Page 6 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
7
Cox regression analysis was used to estimate hazard ratios (HRs) with 95% confidence
intervals (CIs) for outcomes when comparing CSII with MDIs (Table 2). Covariance
adjustment was performed by stratification with quintiles of a propensity score16, including
the following covariates: age, gender, diabetes duration, educational levels, histories of CVD,
heart failure, atrial fibrillation, baseline HbA1c, systolic blood pressure, diastolic blood
pressure, BMI, total cholesterol, HDL cholesterol, triglycerides, albuminuria, creatinine, renal
insufficiency, smoking, physical activity, antihypertensive drugs, lipid-lowering drugs and
aspirin. We also added the educational level as a covariate according to the findings in Table
1. The proportion of the quintiles of the propensity score in each of the two groups (CSII or
MDIs) and the number of outcomes in each quintile are shown in Supplementary Table 1.
The proportional hazard assumption of the Cox regression analyses was confirmed for all
covariates with the test of all time-dependent covariates simultaneously introduced.
Interactions between the two treatment groups and all covariates included in the propensity
score (Table 1) were analysed by means of maximum likelihood estimation; no interactions
were found between any covariates.
Unmeasured confounders may affect the results if they are unrelated to, or not fully accounted
for by, measured confounders or if they affect the decision to use CSII and not MDIs
(treatment allocation bias). Thus, we performed a sensitivity analysis by quantifying the
effects of a hypothetical unmeasured confounder when comparing individuals with CSII and
MDIs (Table 3).17 All statistical analyses were performed with SAS version 9.3 (SAS
Institute, United States). A two-sided p-value <0.05 was considered statistically significant.
Page 7 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
8
Results
Table 1 shows baseline crude characteristics of the two groups (CSII or MDIs). The CSII
group was somewhat younger with similar diabetes duration, slightly lower systolic blood
pressure, fewer males, fewer smokers, greater physical activity, less albuminuria, less renal
insufficiency, less use of antihypertensive drugs, less use of lipid-lowering drugs, less use of
aspirin, less history of CVD and less history of heart failure. Significance levels between the
two compared groups after adjustment for the propensity score were strongly non-significant
in accordance with p-values for all variables. The distribution of the propensity score among
the quintiles as shown in Supplementary Table 1 reveals a satisfactory overlap between the
two treatment groups.
All individuals were monitored for a total of 114,135 person-years during a mean follow-up
period of 6.8 years. There were 1,423 cases of fatal or nonfatal CVD during the study period.
The CVD incidence rate was 1.1 cases per year, or 12.5 cases per 1,000 person-years.
Adjusted HRs for the outcomes in comparing pump with injection treatment as a reference are
shown in Table 2. After adjusting for the propensity score, including all variables presented in
Table 1, pump treatment showed a significant risk reduction of 20% for fatal or nonfatal
CHD, 45% for fatal CVD and 31% for all-cause mortality. Non-significant risk reductions
with CSII treatment were found for fatal or non-fatal CVD and for non-CVD mortality.
A sensitivity analysis of all individuals yields the quantified effects of a hypothetical
confounder in the two groups of pump or injection treatment (Table 3). To invalidate our
significant findings in Table 2 (in order for pump treatment not to have a significantly reduced
risk for the outcomes), a binary confounder with an HR of 1.3 would have to be present in
Page 8 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
9
more than 80% of injection-treated individuals with no presence in pump-treated individuals
concerning fatal CVD as an outcome, and in at least 60% of injection-treated individuals with
no presence in pump-treated individuals concerning total mortality as an outcome.
Complementary analyses
An analysis of all patients using a more stratified propensity score, with deciles instead of
quintiles, showed high and strongly non-significant p values for differences in all covariates
between the groups, as well as for the educational level score (p=0.08-0.8), age (p=0.5),
duration (p=0.3), low physical activity (p=0.20), previous CVD (p=0.21), previous heart
failure (p=0.17) and albuminuria (p=0.24). The corresponding adjusted HRs using
stratification of the propensity score by deciles were 0.82 (0.66-1.01; p=0.06) for fatal or
nonfatal CHD, 0.89 (0.74-1.07; p=0.3) for fatal or nonfatal CVD, 0.56 (0.39-0.82; p=0.003)
for fatal CVD, 0.71 (0.57-0.89; p=0.003) for all-cause mortality and 0.82 (0.62-1.09; p=0.2)
for non-CVD mortality.
Two subgroup analyses were performed, one consisting of 17,984 individuals BMI ≥18 kg/m2
(using BMI <18 kg/m2 as a marker for comorbidity) - see Supplementary Table 2 - and
16,427 individuals with BMI ≥18 kg/m2 and no history of CVD, heart failure or atrial
fibrillation - see Supplementary Table 3.
Both subgroups showed the same pattern of results as all individuals, with borderline
significant HR for fatal or non-fatal CHD of 0.81 (p=0.051) and 0.77 (p=0.047, significant
HR for fatal CVD of 0.56 (p=0.003) and 0.46 (p=0.007), and significant HR for total
mortality of 0.71 (p=0.004) and 0.71 (p=0.02) respectively, as well as non-significant HR for
the other endpoints.
Page 9 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
10
Discussion
This is the first large-sized study from a population-based setting that documents the relation
between CSII and CVM. We studied individuals with type 1diabetes during a mean follow-up
period of 6.8 years. Among 2,441 individuals with CSII and 15,727 individuals with MDIs,
CSII was associated with a reduction of 45% for fatal CVD and 31% for all-cause mortality.
We studied having an insulin pump, and do not know if the effect is through the continuous
infusion of insulin or that some, if not all, of the effect is due to intensified glucose
monitoring, increased motivation to control blood glucose or a better knowledge about having
diabetes type 1.
A reduced number of severe hypoglycaemic episodes may explain why CSII decreases
cardiovascular mortality. Hypoglycaemic episodes can trigger cardiac arrhythmias and
coronary plaque rupture.18, 19Administrating insulin by continuous infusion has been reported
to reduce the frequency of severe hypoglycaemia as compared with administrating insulin by
MDIs.20, 21 There are indications that episodes of hypoglycaemia covary with cardiac
arrhythmia.22, 23 Stahn et al monitored 30 type 2 diabetes individuals with previous CVD, with
continuous glucose measurements and continuous electrocardiograms for five days. They
found a tenfold increase in ventricular arrhythmias (mean 1.0 vs. 0.1) during hypoglycaemic
episodes. The corresponding figure for ventricular couplets was 7.6 (41.7 vs. 5.5).24
Logically, having a CSII may result in a more stable blood glucose levels than MDIs. CSII
Page 10 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
11
involves connecting a catheter on the outside of the body to an insulin pump that is
programmed to supply the body’s basal needs. The individual having the pump administers
doses to cover meals and correct blood glucose levels. Many pumps these days have a bolus
wizard that calculates how much insulin the person needs, taking expected carbohydrate
intake, current blood glucose levels and previously, still-active insulin into consideration.
Pumps can provide an accurate history of insulin usage through their menus. Often this
history can be uploaded and displayed as a graph for purposes of trend analysis.25
We have a rationale for CSII as giving a more stable blood glucose levels than MDIs. But,
available data give no clear indication that intensified insulin administration (without a pump)
affects cardio-vascular morbidity or mortality. When it comes to type 2 diabetes, large-scale
trials have yielded conflicting results regarding the impact of intensive blood glucose-
lowering therapy on mortality and cardiovascular risk.26-30 Authors argue hypoglycaemia is a
risk factor for cardiovascular events, particularly among high-risk individuals.31, 32 We have
recently found evidence that Swedish patients with type 1 diabetes and prior severe
hypoglycaemic episodes run an increased risk of mortality after a cardiovascular event.3
However, the DCCT study of type 1 diabetes did not show any statistically significant
association between frequent severe hypoglycaemic episodes and increased cardiovascular
mortality among individuals in the intensive treatment group.33 The EURODIAB Prospective
Complications Study of 2,181 individuals with type 1 diabetes who were monitored for 7
years reported no association between baseline hypoglycaemia and the risk of CVD.34
However, a retrospective analysis of a large cohort of individuals with type 1 diabetes
receiving CSII pointed to a higher prevalence of CVD in those with a history of repeated
hypoglycaemic episodes.35
Page 11 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
12
Another mechanism worth consideration is that treatment with insulin pump may lead to
lower frequency and duration of hyperglycaemia, corresponding to reduced long-term
occurrence of microvascular and cardiovascular complications, as demonstrated in the DCCT
trial on individuals with type 1 diabetes.36 At the group level, it is clear that sensor-augmented
pump therapy provides better metabolic control than MDIs in adults with type 1 diabetes. A
study in the United States and Canada randomized 329 adults with type 1 diabetes to
administration of insulin with sensor-augmented pump therapy or MDIs. After one year.
HbA1c had been reduced by 1.0 percent from baseline among those who had been randomized
to sensor-augmented pump therapy. The corresponding figure for injections was 0.4%. The
difference is statistically significant.37 A review of the literature in 2010 found some evidence
that insulin pump without continuous glucose monitoring may be better than MDIs for
glycaemic control in individuals with type 1 diabetes.6 This study did not have any
information on sensor use, but it was uncommon in Sweden during the period. The study
adjusted baseline data for HbA1c.
A major strength of this study includes its large size; the association between CSII use and
cardiovascular mortality is highly unlikely to have occurred by chance. Moreover, we have
detailed information on most major possible confounders for cardio-vascular mortality and a
strong association between CSII use and cardiovascular mortality remained after adjustment
for those. In our observational setting unmeasured confounders certainly is an issue; however,
as shown in Table 3 even the hypothetical situation when all subjects in the MDIs group and
none in the CSII group are exposed to the unmeasured confounder, an association between
CSII use and cardiovascular mortality would still remain. Thus, although we lack stringent
Page 12 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
13
criteria for going from MDIs to CSII, and although patient selection (confounding by
indication) thereby certainty exists in our observational setting, the possible unbalance in risk
factors that may result as a consequence probably does not explain the strong protective effect
we found of CSII use on cardio-vascular mortality. Attrition is not a problem, we have a
cause-of-death register that covers the entire population and can find the information through
personal identity numbers unique for each Swedish citizen. Since we have a population-based
setting of Sweden we to a large part, if not entirely, avoid selection-induced problems. We
have no reason to believe differential, between the CSII group and MDIs group, errors in
classifying death as due to a cardio-vascular event affects the relative risks. The information
about the cause of death has been collected from an almost complete national register, and
there is no reason to believe that having an insulin pump influences the quality of the data or
that more than a few individuals have died without having been entered. The physicians
assigning cause of death are not involved in the scientific use of the register information.
Moreover, the preventive effect by CSII was obvious also for mortality of any cause.
We lack information on duration of CSII. If the mechanism for the preventive effect of CSII
on cardio-vascular mortality is through a reduced frequency of lethal arrhythmia, an
adjustment for the duration of CSII would be expected to have little or no effect on the hazard
ratio we obtained. If instead the mechanism is through events with an induction-latency time
of a year or more, such as plaque formation, adjustment for duration of CSII would give even
stronger association than we found. We adjusted the hazard ratio between CSII and
cardiovascular mortality for baseline values of HbA1c. Since some subjects have had CSII for
some time at baseline, this means that the adjustment may eliminate some of the effect we are
studying. That is, if this source of error did not exist, we would have estimated the protective
effect by CSII on cardio-vascular mortality to be larger than we now found. We do not adjust
Page 13 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
14
for HbA1c after baseline since that would be adjusting for a possible mediating factor. A
mediating factor, to some or a large part, for the effect by CSII on cardio-vascular mortality
may be an increased frequency of glucose-monitoring, as well as more appropriate actions as
a result of the glucose-monitoring. Changing from MDIs to CSII in Sweden often is
accompanied by education about diabetes. That is, we do not know if some of the effect we
see can be achieved by intensified training of the individual having diabetes type 1 about the
disease, intensified blood-glucose monitoring or varying cut-off values for taking extra insulin
or sugar. The generalizability of our observation may thus be compromised by actions that are
associated to CSII, not the pump itself.
In conclusion, this nationwide observational study of individuals with type 1 diabetes shows
that CSII was associated with a considerable reduction of risk for fatal CVD and all-cause
mortality. Whether the results reflect the physiological consequences of CSII, the clinical
management that pump users receive, or the educational aspects of having the pump, remains
elusive. Regardless of the actual mechanism involved using CSII as done in Sweden at the
time of our study, has substantially lowered the cardiovascular mortality.
Acknowledgements
We wish to thank all regional NDR coordinators, contributing nurses, physicians and
individuals who contributed to the success of this study. The Swedish Society of Diabetology
and the Swedish Diabetes Association, a patient advocacy group, support the NDR. The
results and views expressed in the study represent those of the authors and not necessarily
those of the Swedish Medical Products Agency, at which one of the authors (BZ) is
employed. The study was presented at the 50th EASD Annual Meeting, Vienna, Austria,
September 2014.
Page 14 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
15
Conflicts of interest
The authors declare no conflicts of interest.
Funding
The Swedish Association of Local Authorities and Regions funds the NDR.
Contribution statement
Author contributions: IS, JC and SG researched the data, performed the statistical analyses,
wrote the article, contributed to the discussion and reviewed and edited the article. TA, BE,
KE-O, JJ, MO-L, AR, A-MS and BZ contributed to the discussion and reviewed and edited
the article.
Page 15 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
16
References
1. Lind M, Svensson AM, Kosiborod M, Gudbjörnsdottir S, Pivodic A, Wedel H, et al.
Glycemic Control and Excess Mortality in Type 1 Diabetes. N Engl J Med 2014; 371:1972-
1982.
2. The Diabetes Control and Complications Trial Research Group. The effect of intensive
treatment of diabetes on the development and progression of long-term complications in
insulin-dependent diabetes mellitus, N Engl J Med 1993;329:977-986.
3. Lung TW, Petrie D, Herman WH, Palmer AJ, Svensson AM, Eliasson B, Clarke PM.
Severe hypoglycemia and mortality after cardiovascular events for Type 1 diabetic patients in
Sweden. Diabetes Care 2014 doi: 10.2337/dc14-0405.
4. Plotnick LP, Clark LM, Brancati FL, Erlinger T. Safety and effectiveness of insulin pump
therapy in children and adolescents with type 1 diabetes. Diabetes Care 2003;26:1142-1146.
5. D. Bruttomesso, A Pianta et al, Continuous subcutaneous insulin infusion (CSII) in the
Veneto region: efficacy, acceptability and quality of life. Diabet Med 2002;19:628-634.
6. Misso ML, Egberts KJ, Page M, O'Connor D, Shaw J. Continuous subcutaneous insulin
infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus. Cochrane
Database of Systematic Reviews 2010, Issue 1. Art. No.: CD005103. DOI:
10.1002/14651858.CD005103.pub2.
Page 16 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
17
7. Annual Report 2013. The Swedish National Diabetes Register (NDR). Gothenburg,
Sweden, 2013, https://www.ndr.nu.
8. Eeg-Olofsson K, Cederholm J, Nilsson PM, Gudbjörnsdóttir S, Eliasson B for the Steering
Committee of the Swedish National Diabetes Register (NDR). Glycemic and risk factor
control in type 1 diabetes: Results from 13,612 patients in a national diabetes register.
Diabetes Care 2007;30:496-502.
9. Eeg-Olofsson K, Cederholm J, Nilsson PM, Zethelius B, Svensson A-M, Gudbjörnsdottir
S, Eliasson B. Glycemic control and cardiovascular disease in 7454 patients with type 1
diabetes: an observational study from the Swedish National Diabetes Register (NDR).
Diabetes Care 2010;33:1640-1646.
10. Cederholm J, Eeg-Olofsson K, Eliasson B, Zethelius B, Gudbjörnsdottir S; Swedish
National Diabetes Register. A new model for 5-year risk of cardiovascular disease in Type 1
diabetes; from the Swedish National Diabetes Register (NDR). Diabet Med 2011;28:1213-
1220.
11. Zethelius B, Eliasson B, Eeg-Olofsson K, Svensson A-M, Gudbjörnsdottir S, Cederholm
J. A new model for 5-year risk of cardiovascular disease in type 2 diabetes –from the Swedish
National Diabetes Register (NDR). Diabetes Res Clin Pract 2011;93:276-284.
12. Cederholm J, Gudbjörnsdottir S, Eliasson B, Zethelius B, Eeg-Olofsson K, Nilsson PM,
on behalf of the NDR. Systolic blood pressure and risk of cardiovascular diseases in type 2
Page 17 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
18
diabetes: an observational study from the Swedish national diabetes register. J Hypertens
2010;28:2026-2035.
13. Geistanger A, Arends S, Berding C, Hoshino T, Jeppsson JO, Little R, et al. Statistical
methods for monitoring the relationship between the IFCC reference measurement procedure
for hemoglobin A1c and the designated comparison methods in the United States, Japan, and
Sweden. Clin Chem 2008;54:1379–1385.
14. Merlo J, Lindblad U, Pessah-Rasmussen H, Hedblad B, Rastam J, Isacsson SO, et al.
Comparison of different procedures to identify probable cases of myocardial infarction and
stroke in two Swedish prospective cohort studies using local and national routine registers.
Eur J Epidemiol 2000;16:235-243.
15. Tunstall-Pedoe H, Kuulasmaa K, Amouyel P, Arveiler D, Rajakangas AM, Pajak A.
Myocardial infarction and coronary deaths in the World Health Organization MONICA
Project. Registration procedures, event rates, and case-fatality rates in 38 populations from 21
countries in four continents. Circulation 1994;90:583-612.
16. D’Agostino RB Jr. Propensity score methods for bias reduction in the comparison of a
treatment to a non-randomized control group. Stat Med 1998;17:2265–228.1
17. Lin DY, Psaty BM, Kronmal RA. Assessing the sensitivity of regression results to
unmeasured confounders in observational studies. Biometrics 1998;54:948–963.
Page 18 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
19
18. Pickup JC, Sutton AJ. Severe hypoglycaemia and glycaemic control in type 1diabetes:
meta-analysis of multiple daily insulin injections compared with continuous subcutaneous
insulin infusion. Diabet Med 2008;25:765–774.
19. Arbab-Zadeh A, Nakano M, Virmani R, Fuster V. Acute coronary events. Circulation
2012;125:1147-56.
20. Bode BW, Steed RD, Davidson PC. Reduction in severe hypoglycemia with long-term
continuous subcutaneous insulin infusion in type 1 diabetes. Diabetes Care 1996;19:324-327
21. Yeh, HC, Brown, TT, Maruthur, N, Ranasinghe, P, Berger, Z, Suh, YD, et al.
Comparative effectiveness and safety of methods of insulin delivery and glucose monitoring
for diabetes mellitus: a systematic review and meta-analysis. Ann Intern Med 2012;157:336-
347.
22. Chow E, Bernjak A, Williams S, Fawdry RA, Hibbert S, Freeman et al. Risk of cardiac
arrhythmias during hypoglycemia in patients with type diabetes and cardiovascular risk.
Diabetes 2014;63:1738-1747.
23. Ray KK, Seshasai SR, Wijesuriya S, Sivakumaran R, Nethercott S, Preiss D et al. Effects
of intensive control of glucose on cardiovascular outcomes and death in patients with diabetes
mellitus. Lancet 2009;373:1765-1772.
Page 19 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
20
24. Stahn A, Pistrosch F, Ganz X, Teige M, Koehler C, Bornstein S, Hanefeld M.
Relationship between hypoglycemic episodes and Ventricular Arrhythmias in Patients with
type 2 diabetes and cardiovascular diseases: Silent hypoglycemias and silent arrhythmias.
Diabetes Care 2014;37:516-520.
25. Pickup JC. Insulin-pump therapy for type 1 diabetes mellitus. N Engl J Med
2012;366:1616-1624.
26. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with
sulphonylureas or insulin compared with conventional treatment and risk of complications in
patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837–853.
27. Holman RR, Paul SK, Bethel MA, Matthews DR, Neil HA. 10-year follow-up of intensive
glucose control in type 2 diabetes. N Engl J Med 2008;359:1577–1589.
28. Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Bigger JT, Buse JB, Cushman WC et
al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med 2008;358:2545–
2559.
29. Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M et al. Intensive blood
glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med
2008;358:2560–2572
Page 20 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
21
30. Abraira C, Duckworth W, McCarren M, Emanuele N, Arca D, Reda D, Henderson W et
al. Design of the cooperative study on glycemic control and complications in diabetes mellitus
type 2: Veterans Affairs Diabetes Trial. J Diabetes Complications 2003;17:314–322.
31. Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reaven PD et al. Glucose
control and vascular complications in veterans with type 2 diabetes. N Engl J Med
2009;360:129–139.
32. Mellbin LG, Rydén L, Riddle MC, Probstfield J, Rosenstock J, Díaz R et al. Does
hypoglycaemia increase the risk of cardiovascular events? A report from the ORIGIN trial.
Eur Heart J 2013;34:3137–3144.
33. The Diabetes Control and Complications Trial Research Group. Hypoglycemia in the
Diabetes Control and Complications Trial. Diabetes 1997;46:271–286.
34. Gruden G1, Barutta F, Chaturvedi N, Schalkwijk C, Stehouwer CD, Witte DR et al.
Severe hypoglycemia and cardiovascular disease incidence in type 1 diabetes: the
EURODIAB Prospective Complications Study. Diabetes Care 2012;35:1598–1604.
35. Gimenez M, Lopez JJ, Castell C, Conget I. Hypoglycaemia and cardiovascular disease in
Type 1 Diabetes. Results from the Catalan National Public Health registry on insulin pump
therapy. Diabetes Res Clin Pract 2012;96:23–25.
Page 21 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
22
36. The Diabetes Control and Complications Trial Research Group. The effect of intensive
treatment of diabetes on the development and progression of long-term complications in
insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-986.
37. Bergenstal RM, Tamborlane WV, Ahmann A, Buse JB, Dailey G, Davis SN et al.
Effectiveness of Sensor Augmented Insulin Pump Therapy in type 1 Diabetes. N Engl J Med
2010;363:311-20.
Page 22 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
23
Table 1. Baseline data for 18,168 individuals with type 1 diabetes followed for 7 years until 2012.
Insulin pump Injections P value 1 P value 2
Numbers 2,441 15,727 - -
Age (years) 38±13 41±15 <0.001 0.16
Duration (years) 25±12 26±15 <0.001 0.23
Males % 45.0 57.1 <0.001 0.6
HbA1c (mmol/mol) 63±12 64±14 0.4 0.5
HbA1c (%) 7.9±1.3 8.0±1.3 0.4 0.5
Systolic BP (mmHg) 125±15 128±16 <0.001 0.6
Diastolic BP (mmHg) 73±8 73±9 0.1 0.7
Antihypertensives % 23.2 36.3 <0.001 0.6
Total cholesterol (mmol/l) 4.7±0.8 4.8±0.9 <0.001 0.8
HDL cholesterol (mmol/l) 1.6±0.4 1.6±0.5 0.2 0.9
Triglycerides (mmol/l) 1.0±0.6 1.1±0.7 <0.001 0.3
Lipid drugs % 21.0 26.2 <0.001 0.7
BMI (kg/m2) 25.3±3.8 25.5±4.1 0.1 0.8
Low physical activity % 20.6 24.2 <0.001 0.6
Smokers % 10.5 13.5 <0.001 0.9
Aspirin 14.6 18.7 <0.001 0.4
Creatinine (µmol/l) 82±46 85±55 0.003 0.9
eGFR <60, % 10.2 11.8 0.02 0.23
Albuminuria % 20.5 24.1 <0.001 0.7
Previous CVD % 5.4 8.0 <0.001 0.11
Previous heart failure % 0.9 2.3 <0.001 0.11
Previous atrial fibrillation, % 0.6 1.0 0.05 0.22
Previous cancer, % 0.9 1.2 0.2 0.8. Previous liver diseases, % 0.3 0.2 0.5 0.5
Previous mental disorders, % 2.0 1.8 0.6 0.5
Education level 1 8.6 17.6 <0.001 <0.001
Education level 2 48.4 50.8 0.03 <0.001
Education level 3 43.0 31.6 <0.001 0.3
Data are given as means ± 1 standard deviation or frequencies (%). 1 Crude significance values with
use of student’s t-test or X2 test. Significance values after adjustment with a propensity score including
all variables in Table 1, with use of GLM (General Linear Model) or logistic regression.
Page 23 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
24
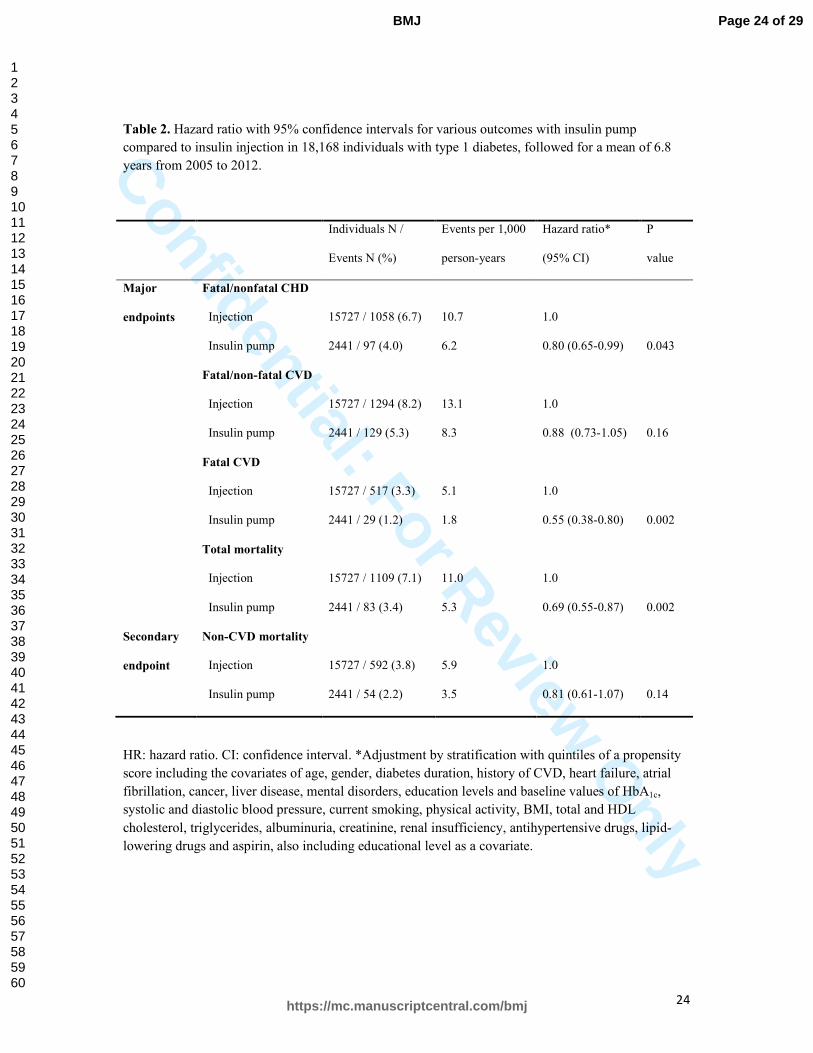
Table 2. Hazard ratio with 95% confidence intervals for various outcomes with insulin pump compared to insulin injection in 18,168 individuals with type 1 diabetes, followed for a mean of 6.8
years from 2005 to 2012.
Individuals N / Events per 1,000 Hazard ratio* P
Events N (%) person-years (95% CI) value
Major Fatal/nonfatal CHD
endpoints Injection 15727 / 1058 (6.7) 10.7 1.0
Insulin pump 2441 / 97 (4.0) 6.2 0.80 (0.65-0.99) 0.043
Fatal/non-fatal CVD
Injection 15727 / 1294 (8.2) 13.1 1.0
Insulin pump 2441 / 129 (5.3) 8.3 0.88 (0.73-1.05) 0.16
Fatal CVD
Injection 15727 / 517 (3.3) 5.1 1.0
Insulin pump 2441 / 29 (1.2) 1.8 0.55 (0.38-0.80) 0.002
Total mortality
Injection 15727 / 1109 (7.1) 11.0 1.0
Insulin pump 2441 / 83 (3.4) 5.3 0.69 (0.55-0.87) 0.002
Secondary Non-CVD mortality
endpoint Injection 15727 / 592 (3.8) 5.9 1.0
Insulin pump 2441 / 54 (2.2) 3.5 0.81 (0.61-1.07) 0.14
HR: hazard ratio. CI: confidence interval. *Adjustment by stratification with quintiles of a propensity
score including the covariates of age, gender, diabetes duration, history of CVD, heart failure, atrial
fibrillation, cancer, liver disease, mental disorders, education levels and baseline values of HbA1c, systolic and diastolic blood pressure, current smoking, physical activity, BMI, total and HDL
cholesterol, triglycerides, albuminuria, creatinine, renal insufficiency, antihypertensive drugs, lipid-
lowering drugs and aspirin, also including educational level as a covariate.
Page 24 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
25
Table 3. Simulated effect of an unmeasured confounder. For each outcome, figures are based on the
hazard ratios seen in table 2. To those hazard ratios, the effect of an unmeasured confounder has been
added, according to the prevalence of the confounder in the CSII and MDIs group, respectively.
Numbers in the tables are hazard ratios with 95% confidence intervals after adjustment the
unmeasured confounder. Bold indicates confidence intervals overlapping 1.0.
Confounder with hazard ratio 1.3, Prevalence in the CSII group
0.0 0.2
Fatal/non-fatal Prevalence in the
(confounder) *
0.0 0.80 (0.65-0.99) 0.75 (0.61-0.93)
CHD MDIs group 0.2 0.85 (0.70-1.05) 0.80 (0.65-0.99)
Fatal/non-fatal Prevalence in the 0.0 0.88 (0.73-1.05) 0.83 (0.69-0.99)
CVD MDIs group 0.2 0.93 (0.77-1.11) 0.88 (0.73-1.05)
Fatal CVD Prevalence in the (confounder) *0.0 0.55 (0.38-0.80) 0.52 (0.36-0.75)
MDIs group 0.2 0.58 (0.40-0.85) 0.55 (0.38-0.80)
0.4 0.62 (0.43-0.90) 0.58 (0.40-0.85)
0.6 0.65 (0.45-0.94) 0.62 (0.43-0.90)
0.8 0.68 (0.47-0.99) 0.65 (0.45-0.94)
Total mortality Prevalence in the 0.0 0.69 (0.55-0.87) 0.65 (0.52-0.82)
MDIs group 0.2 0.73 (0.58-0.92) 0.69 (0.55-0.87)
0.4 0.77 (0.62-0.97) 0.73 (0.58-0.92)
0.6 0.81 (0.65-1.03) 0.77 (0.62-0.97)
0.8 0.86 (0.68-1.08) 0.81 (0.65-1.03)
Page 25 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
26
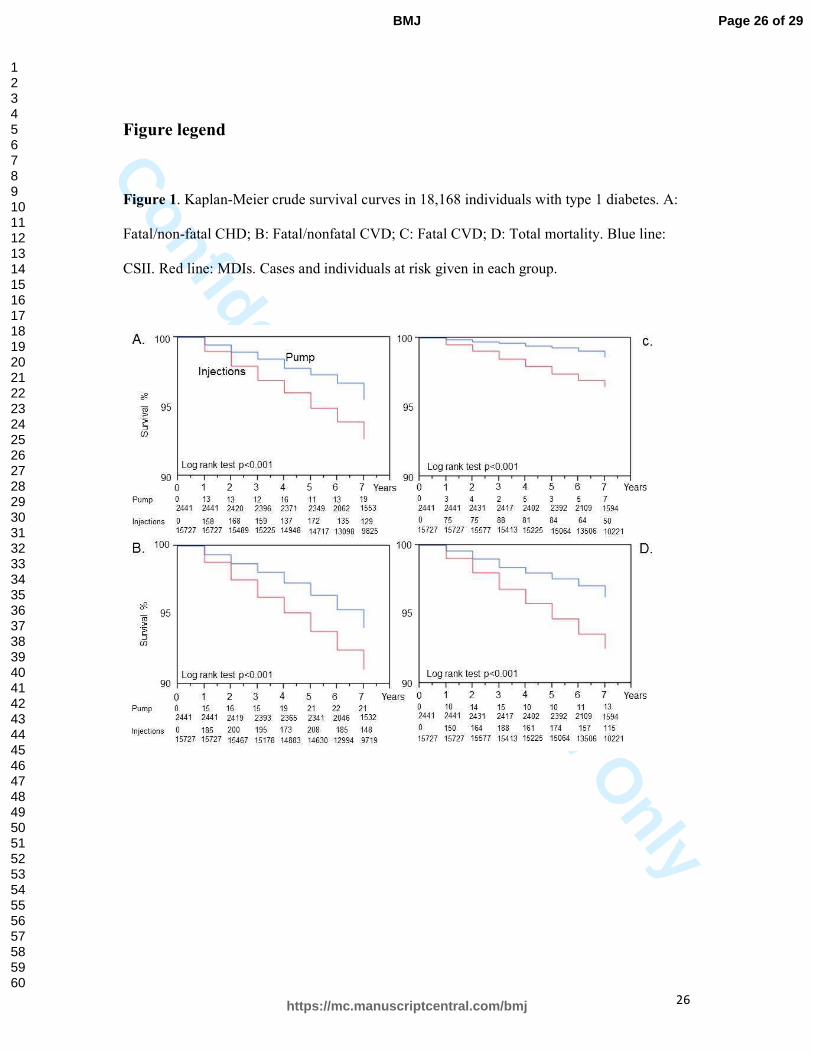
Figure legend
Figure 1. Kaplan-Meier crude survival curves in 18,168 individuals with type 1 diabetes. A:
Fatal/non-fatal CHD; B: Fatal/nonfatal CVD; C: Fatal CVD; D: Total mortality. Blue line:
CSII. Red line: MDIs. Cases and individuals at risk given in each group.
Page 26 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlySupplementary Table 1. Proportions (%) of the quintiles (Q) of the propensity score in each of the
two groups with pump or injections, number (n) of patients in each quintile, and number (n) of
outcomes in each quintiles.
Patients Outcomes
Pump Injections Total Total Total Fatal Total Non-CVD
Q % % n CHD n CVD n CVD n mort. n mort. n
1 9.7 21.7 3654 503 589 289 600 297
2 13.3 20.9 3606 256 318 116 235 130
3 18.8 20.5 3678 183 251 72 182 110
4 23.2 19.3 3604 134 171 51 112 66
5 35.0 17.6 3626 79 94 18 63 43
CHD. the notes Coronary Heart Disease
CVD. the notes Cardio Vascular Disease
Mort. the notes mortality
Page 27 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
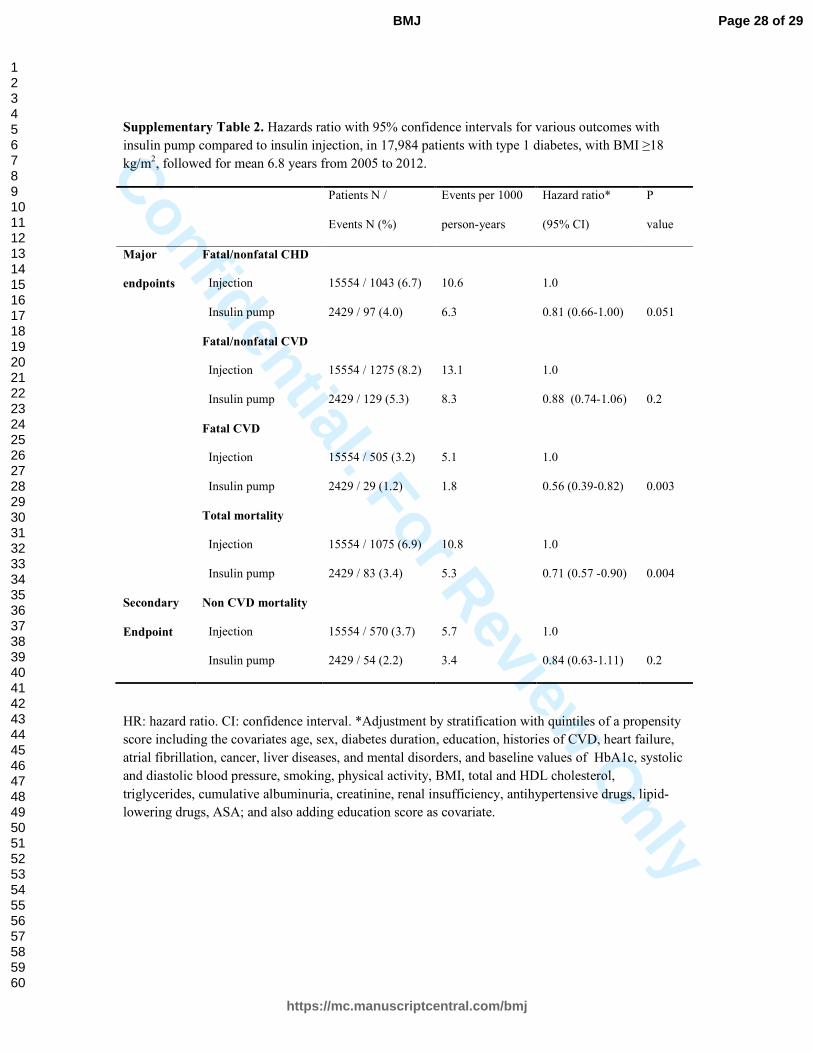
Supplementary Table 2. Hazards ratio with 95% confidence intervals for various outcomes with
insulin pump compared to insulin injection, in 17,984 patients with type 1 diabetes, with BMI ≥18
kg/m2, followed for mean 6.8 years from 2005 to 2012.
Patients N / Events per 1000 Hazard ratio* P
Events N (%) person-years (95% CI) value
Major Fatal/nonfatal CHD
endpoints Injection 15554 / 1043 (6.7) 10.6 1.0
Insulin pump 2429 / 97 (4.0) 6.3 0.81 (0.66-1.00) 0.051
Fatal/nonfatal CVD
Injection 15554 / 1275 (8.2) 13.1 1.0
Insulin pump 2429 / 129 (5.3) 8.3 0.88 (0.74-1.06) 0.2
Fatal CVD
Injection 15554 / 505 (3.2) 5.1 1.0
Insulin pump 2429 / 29 (1.2) 1.8 0.56 (0.39-0.82) 0.003
Total mortality
Injection 15554 / 1075 (6.9) 10.8 1.0
Insulin pump 2429 / 83 (3.4) 5.3 0.71 (0.57 -0.90) 0.004
Secondary Non CVD mortality
Endpoint Injection 15554 / 570 (3.7) 5.7 1.0
Insulin pump 2429 / 54 (2.2) 3.4 0.84 (0.63-1.11) 0.2
HR: hazard ratio. CI: confidence interval. *Adjustment by stratification with quintiles of a propensity
score including the covariates age, sex, diabetes duration, education, histories of CVD, heart failure,
atrial fibrillation, cancer, liver diseases, and mental disorders, and baseline values of HbA1c, systolic
and diastolic blood pressure, smoking, physical activity, BMI, total and HDL cholesterol,
triglycerides, cumulative albuminuria, creatinine, renal insufficiency, antihypertensive drugs, lipid-
lowering drugs, ASA; and also adding education score as covariate.
Page 28 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlySupplementary Table 3 . Hazards ratio with 95% confidence intervals for various outcomes with
insulin pump compared to insulin injection, in 16,427 patients with type 1 diabetes, with no histories
of CVD, heart failure or atrial fibrillation and BMI ≥18 kg/m2, followed for mean 6.8 years from 2005
to 2012.
Patients N / Events per 1000 Hazard ratio* P
Events N (%) person-years (95% CI) value
Major Fatal/nonfatal CHD
endpoints Injection 14145 / 663 (4.7) 7.3 1.0
Insulin pump 2280 /64 (2.8) 4.7 0.77 (0.59-0.99) 0.047
Fatal/nonfatal CVD
Injection 14145 / 859 (6.1) 9.5 1.0
Insulin pump 2280 / 90 (3.9) 6.8 0.84 (0.68-1.05) 0.13
Fatal CVD
Injection 14145 / 241 (1.7) 2.6 1.0
Insulin pump 2280 / 13 (0.5) 0.9 0.46 (0.26-0.80) 0.007
Total mortality
Injection 14145 / 636 (4.5) 6.9 1.0
Insulin pump 2280 / 54 (2.4) 3.7 0.71 (0.54 -0.95) 0.02
Secondary Non CVD mortality
endpoint Injection 14145 / 395 (2.8) 4.3 1.0
Insulin pump 2280 / 41 (1.8) 2.8 0.87 (0.63-1.20) 0.4
HR: hazard ratio. CI: confidence interval. *Adjustment by stratification with quintiles of a propensity
score including the covariates age, sex, diabetes duration, education, histories of CVD, heart failure,
atrial fibrillation, cancer, liver diseases, and mental disorders, and baseline values of HbA1c, systolic
and diastolic blood pressure, smoking, physical activity, BMI, total and HDL cholesterol,
triglycerides, cumulative albuminuria, creatinine, renal insufficiency, antihypertensive drugs, lipid-
lowering drugs, ASA; and also adding education score as a covariate.
Page 29 of 29
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960