insulin shock diseases of the pancreas. insulin shock causes: 1. insulin overdose (misread syringe)...
TRANSCRIPT

INSULIN SHOCK
DISEASES OF THE PANCREAS
Insulin Shock
Causes:1. Insulin overdose (misread syringe)2. Too much exercise3. AnorexiaSigns:Weakness, incoordination, seizures, coma

Insulin Shock
Prevention1. Consistent diet (type and amount)/consistent
exercise (less insulin with exercise)2. Monitor urine/blood glucose at same time
each day3. Feed 1/3 with insulin; the rest 8-10 h later
(at insulin peak)4. Have sugar supply handy

InsulinomaCAUSE: tumor of beta cells, secreting an
excess of insulinSIGNS: prolonged hypoglycemia→weakness,
ataxia, muscle fasciculations, posterior paresis, brain damage, seizures, coma, death,

Insulinoma: Dx
Chem Panel ↓blood glucose Simultaneous glucose and insulin tests
Low glucose, High insulin => insulinoma
Observations of Whipple’s Triad: Symptoms occur after fasting or exercise when symptomatic, blood glucose<50 mg/dl symptoms corrected with sugar administration

Insulinoma: Rx
Surgical Rx: removal of tumorMedical Rx: Acute, at home: administer glucose (Karo); keep animal quiet, seek
vet careAcute, in Hosp adm. glucose (50% Dextrose)Chronic care feed 3-6 small meals/day (high protein, low fat)
limited exerciseglucocorticooid therapy (antagonizes insulin effect at cellular level)Diazoxide (↓insulin secretion, tissue use of glucose, ↑blood glucose)Octreotide (Sandostatin) injections—inhibits synthesis and release of insulin by both normal and neoplastic beta cells

Insulinoma: Client info
1. Usually, by the time insulinoma is diagnosed, metastasis has occurred so prognosis is poor
2. With proper medical therapy, survival may be 12-24 mo
3. Always limit exercise and excitement 4. Feed multiple, small meals throughout
day; keep sugar source close during exercise 5. Karo syrup on mm provides for rapid
absorption of glucose into blood stream 6. Avoid placing hand into dog’s mouth
during seizure to avoid being bitten

EXOCRINE PANCREATIC INSUFFICIENCY
Diseases of the exocrine pancreas

Exocrine Pancreas Insufficiency (EPI)
Inability to process nutrients efficiently due to lack of production of enzymes from pancreas. Pancreatic acinar atrophy
Found most commonly in German Shepherds and Rough Collies through a recessive gene. In cats, EPI is primarily the result of chronic
pancreatitis
Diagnosis of EPI
Not usually evident until 85-90% of pancreas is unable to secrete enzymes. Weight loss although no change in
diet or appetite (appetite often increases)
Persistent tarry diarrhea. Flatulence Poor haircoat

Testing and treatment for EPI
TLI (trypsin-like immunoreactivity) Detects trypsin and trypsinogen Usually want below 2.5 in dogs to be
diagnostic Canine 5.7-45.2 Feline 12-82
Treatment includes enzymatic supplement Viokase powder Raw ox or pig pancreas

Client considerations
Usually life long treatment.Can be very expensive.Can be well controlled. Should not breed animal that has EPI.

CUSHING’S DISEASE
(HYPERADRENOCORTICISM)
ADDISON’S DISEASE
(HYPOADRENOCORTICISM)
DISEASES OF THE ADRENAL GLANDS
Adrenal Glands

ADRENAL GLANDS
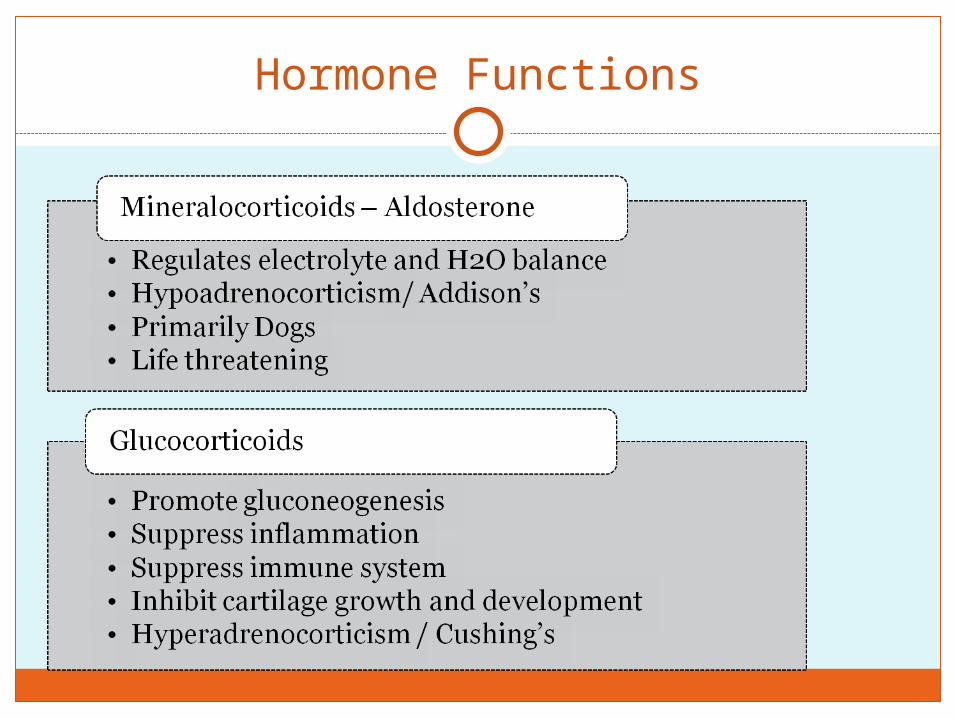
mineralocorticoids
Glucocorticoids
Androgens
epinephrine

Physiology
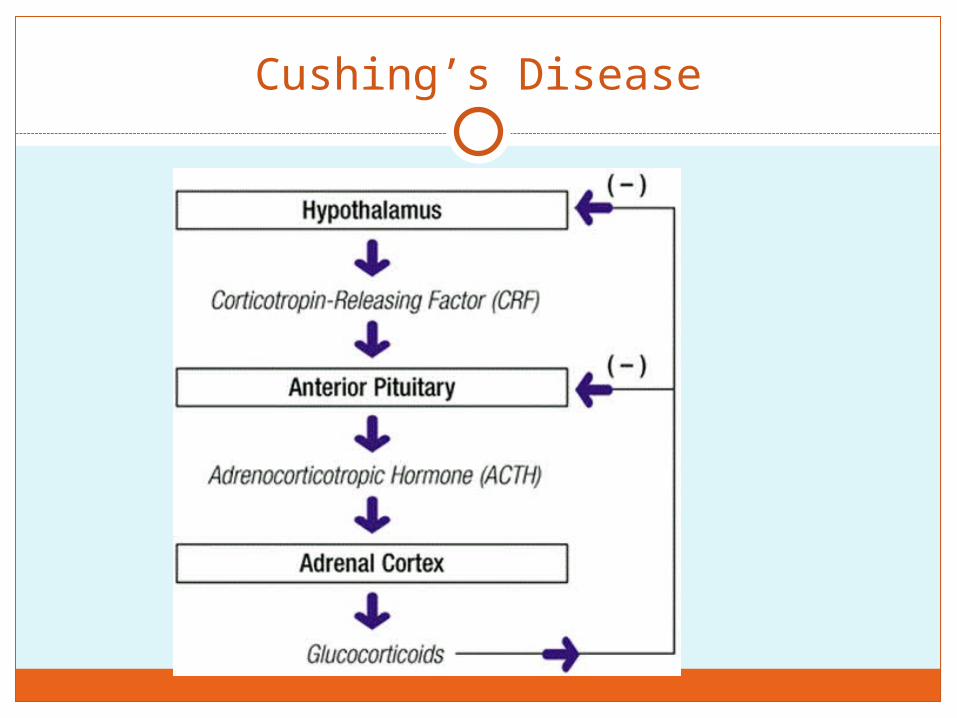
Hypothalamus – Corticotropin realeasing factor (CRF) > Anterior Pituitary Gland – Adrenocorticotropic hormone (ACTH) > ADRENAL CORTEX
Glucocorticoid hormone Mineralocorticoid hormone Sex hormones (Androgens)
Sympathetic Nerv Sys > ADRENAL MEDULLA > Epinehrine and norepinephrine Increase HR, Inc. BP, Dilated air passages – lungs,
dec. GI function, vasoconstriction
Hormone Functions
Hyperadrenocorticism (Cushing’s Disease)
Definition: Disorder caused by deleterious effects of high circulating cortisol concentrations on multiple organ systems
Systems affected: Renal Skin Cardiovascular Respiratory Endocrine/metabolic Musculoskeletal Nervous Reproductive

Cushing’s Disease
Effects of excess glucocorticoids:1. suppress inflammation2. suppress immune system3. inhibit cartilage growth, development,
and repairCauses: 1. Anterior pituitary lesion (pituitary-dependent
disease) – 85% of cases2. Adrenal tumor (excess cortisol secretion
independent of pituitary control) – 15-20% of cases3. Overmedication with glucocorticoids - Iatrogenic
Cushing’s Disease

Cushing’s Disease
Bilaterally symmetrical alopecia, pot-belly, pyoderma

Cushing’s Disease
Pot belliedPU/PDMuscle wastingThin coat

Cushing’s Disease
Clinical Signs:1. Some are similar to hypothyroidism2. Dog >6 yr old (most are female)3. PU/PD/PP4. Pot bellied; obese5. Muscle atrophy and weakness, lethargy,
excess panting6. Bilateral symmetric alopecia; pruritis;
pyoderma (↓ immune response)7. Calcinosis cutis (firm plaques of Ca++
under skin)8. Abnormal gonadal function (lack of
estrus; soft, small testicles)
signs are slow to develop and usually go unnoticed by owner
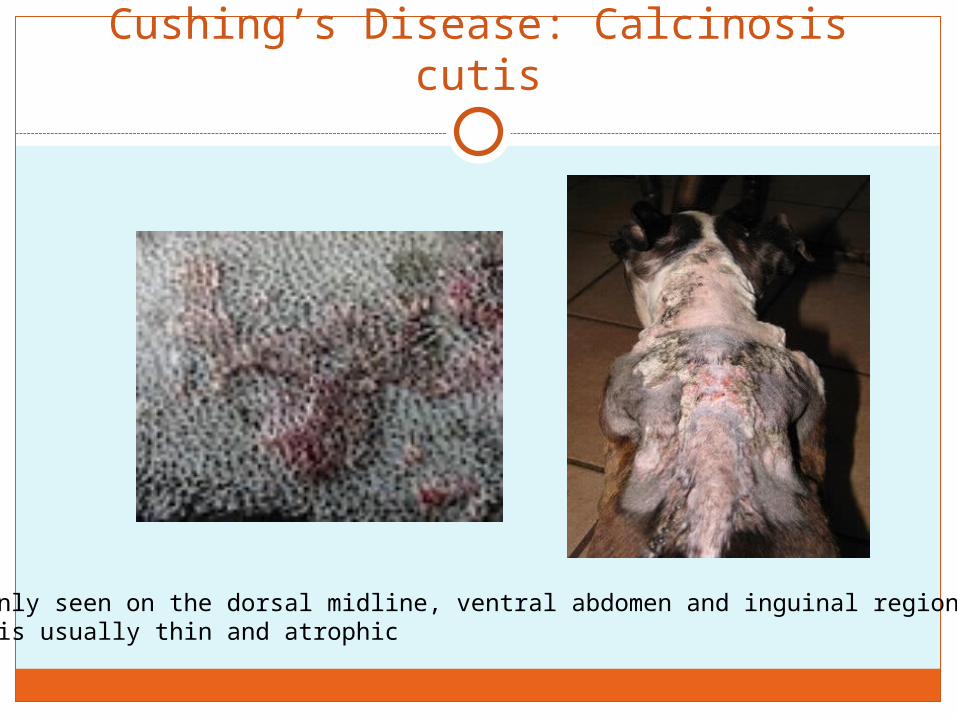
Cushing’s Disease: Calcinosis cutis
Commonly seen on the dorsal midline, ventral abdomen and inguinal region. Skin is usually thin and atrophic

Cushing’s Disease: Dx
Chemistry Panel1. ↑ ALP, ALT, cholesterol, blood glucose2. ↓ BUN3. Lipemia4. Low USG < 1.015, proteinuria, hematuria, pyuria, bactiuria
Urine cortisol/creatinine ratios (sample collected at home)1. Normal ratio=no Cushing’s2. Elevated ratio=may be Cushing’s
ACTH Stimulation test1. Normal patients show an increase of plasma cortisol2. Pituitary dependent disease (excess ACTH release) and
Adrenal tumors: 60-85% show EXAGGERATED cortisol response
3. Does not differentiate between Pit disease and Adrenal tumor

ACTH Stimulation for Hyperadrenocorticism
Take a pre blood sample.Inject ACTH stimulation gel or liquid
Verify amounts with lab as there is difference between amount to be injected with gel and liquid.
Wait two hours and take a post sample

Cushing’s Disease: Dx
Low-Dose Dexamethasone Suppression Test1. Inject low dose of steroid (should suppress ant. pit
[ACTH])2. Measure plasma cortisol at 0, 4, 8 h
Interpretation:1. Normal dogs will show decrease in plasma cortisol2. Pituitary tumor and adrenal tumor will not show
any effect at 8 h (cortisol will still be high)
Cushing’s Disease: Dx
High-Dose Dexamethasone Suppression Test (used to differentiate between Pit Dis and Adrenal tumor)
1. Collect plasma cortisol at 0, 4, and 8 h
Interpretation:1. Pituitary dependent disease—70-75% will show
decrease at 4 or 8 h2. Adrenal tumor—no change in plasma cortisol level
(tumor is autonomous)

Cushing’s Disease: Rx
Surgical removal—1. FAT - Specialized surgery; most vets would refer surgery2. Pituitary tumors are not surgically removed
Medical treatment1. Lysodren (o,p,DDD)—necrosis of z fasiculata (middle), z
reticularis (deep)-repeat ACTH stimulation q 7-10 d until cortisol normal-like chemotherapy-excess dose affects z glomerulus (Addison’s Dis)

Cushing’s Disease: Rx
2. trilostane (Vetoryl®)—less side-effects than o,p,DDD-interfers with cortisol production (doesn’t kill cells)-FDA approved
Cushing’s Disease: Client info
Serious disease; life-long treatment Periodic monitoring required Addison’s disease may result Prognosis: average life expectancy is
20-30 mo on therapy with frequent recurrence of clinical symptoms – varies with cause (pit vs adrenal, tumors)

Addison’s Disease (Hypoadrenocorticism)
Definition: Disorder caused by deficient production of glucocorticoids (cortisol) or mineralocorticoids (aldosterone) or both
Secondary disease caused by chronic administration of corticosteroids followed by sudden cessation

Addison’s Disease (Hypoadrenocorticism)
Clinical Signs:1. lethargy, weakness, anorexia, wt loss2. Vomiting/Diarrhea3. PU/PD, dehydration4. Bradycardia

Addison’s Disease
Pathophysiology Decreased aldosterone => Increased K
and decreased Na=> decreased volume => azotemia, hypotension, dehydration, weakness, depression
Hyper K => heart (bradycardia)
Glucocorticoid deficiency => vomiting, diarrhea, melena, lethargy, wt loss, hypoglycemia (less common than expected)

Addison’s Disease: Dx
Chem PanelNa:K ratio <25:1!(normal=27:1 to 40:1)↑ BUN, Creatinine, Ca++ ↓ blood glucose, albumin (less common
ACTH Stimulation test (definitive test)normal dog= ↑ cortisolhypoadrenocorticism dog= low, unchanged cortisol level
Endogenous ACTH will be increased (1º hypoadrenocorticism; lack of neg feedback)

What is your Dx?
Chem Panel (What is not normal?)
Parameter Value Normal valueBUN 81 mg/dl 7-27 mg/dlCreatinine 2.1 mg/dl 0.4-1.8 mg/dlSodium 131 meq/L 141-156 meq/LPotassium 6.5 meq/L 4.0-5.6 meq/LNa:K ratio 20 27-40

What is your Dx?
ACTH Stimulation Test ResultsValue Normal
Plasma CortisolPre-ACTH 0.2 2-6
Post-ACTH 0.3 6-18
Addison’s Disease Tx
Acute Crisis (may be life-threatening situation)
1. Normal saline IV (low Na+ is hallmark finding of Addison’s)
2. Glucorticoid replacement(cortisol will also be low)
a. Dexamethasone or Prednisone (IV or IM)
3. Mineralocorcorticoid replacementa. Florinef® (fludrocortisone acetate)—po b. Percortin-V (desoxycorticosterone pivalate)
injection

Addison’s disease TX
Chronic Management1. Glucocorticoid replacement
a. Prednisone b. Prenisolone
2. Mineralocorcorticoid replacementa. Florinef® (fludrocortisone acetate)—po daily (not
cheap; 50¢/tab)b. Percortin-V (desoxycorticosterone pivalate)—inj
~monthly (expensive)
3. Monitor electrolytes, BUN/Creatinine, clinical signs

Addison’s disease: Client info
1. Mineralocorticoid deficiency is life-threatening
2. Animal requires periodic blood tests3. Glucocorticoids needed in times of stress4. Always remind attending vet of pet’s
condition5. Hormone replacement therapy continued
for life of pet6. Prognosis: Good to excellent after
stabilization and treatment

References
Alleice Summers, Common Diseases of Companion Animals
http://www.aahanet.org/PublicDocuments/AAHADiabetesGuidelines.pdf
http://www.vetmed.wsu.edu/cliented/diabetes.aspx
http://www.sciencedirect.com/science/article/pii/S0378427408001732