integrated care for older people with frailty and multimorbidity, pop up uni, 12.00, 3 september...
TRANSCRIPT

Integrated Care for Older People with
Frailty and Multimorbidity
Helen Lyndon, Nurse Consultant, Clinical Lead Frailty, NHS England
Lucy Watson, Director of Quality, Safety and Governance, Somerset Clinical Commissioning Group
Dr Mike Pearce, General Practitioner, Somerset Clinical Commissioning Group

Our session today • Introduce the concept of frailty and multimorbidity in older people.
• To update the on the work NHS England is undertaking to promote
the concept of frailty as a long term condition including products
that can support service development within a community and
primary care setting.
• Implementation in practice - information from Somerset CCG to
embed the frailty pathway in Symphony data and collaborative working pilots and Unplanned Admissions Direct Enhanced
Service.

Where is frailty?
“ I know it when I see it but what I see may not be the same as what everyone else sees” Community dwelling adults aged 65+ = 7% - 12% Community dwelling adults aged 85+ = 25% - 50%
The Frailty Paradox Not recognised
Not diagnosed
Not recorded
Chen, X, Genxiang, M, Sean X (2014) Frailty Syndrome: an overview . Clinical Interventions in Aging
2014:9 433–441
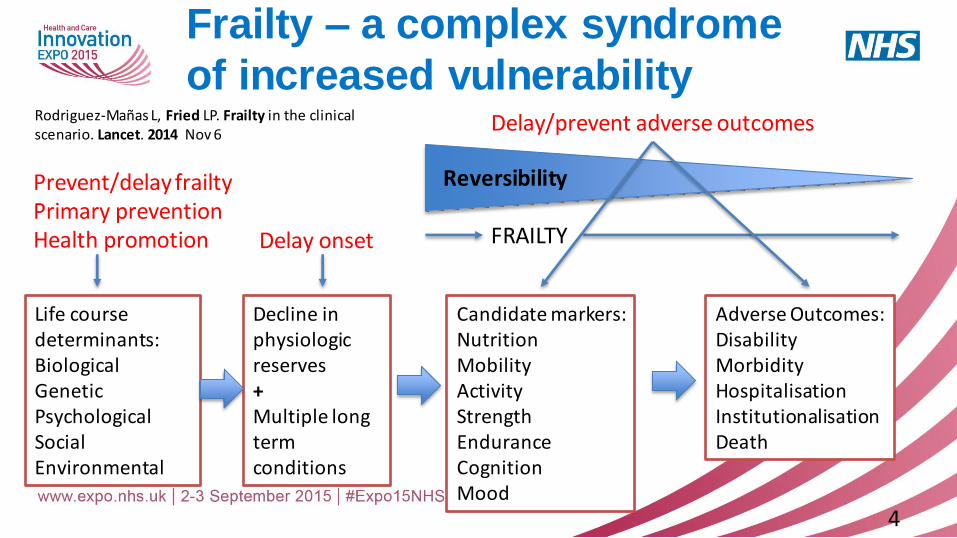
Frailty – a complex syndrome
of increased vulnerability
4
Life course determinants: Biological Genetic Psychological Social Environmental
Decline in physiologic reserves + Multiple long term conditions
Candidate markers: Nutrition Mobility Activity Strength Endurance Cognition Mood
Adverse Outcomes: Disability Morbidity Hospitalisation Institutionalisation Death
Prevent/delay frailty Primary prevention Health promotion Delay onset FRAILTY
Delay/prevent adverse outcomes Rodriguez-Mañas L, Fried LP. Frailty in the clinical scenario. Lancet. 2014 Nov 6
Reversibility
A definition of frailty
• Frailty is not a disease but a combination
of the natural ageing process and a variety
of medical problems
• It focuses on the loss of reserve, energy and wellbeing
• A useful definition is: “Multidimensional loss of reserves - energy, physical ability, cognition and health”
Rockwood et al (2005)
Ageing Fitness
Disease

Frailty is a loss of physiological reserve
Clegg, Young, Rockwood Lancet 2013

Frailty as a Long Term
Condition
A Long Term Condition is: “A condition that cannot, at present, be cured but is controlled by medication
and/or other treatment/therapies” (DH 2012)
Frailty is:
• Common (25-50% of people over 80 years)
• Progressive (5 to 15 years)
• Episodic deteriorations (delirium; falls; immobility)
• Preventable components
• Potential to impact on quality of life
• Expensive
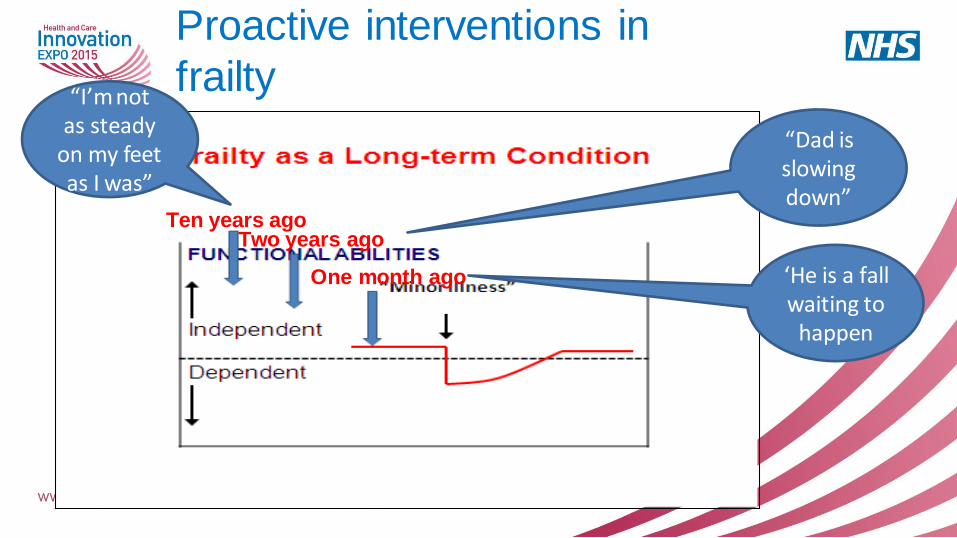
Proactive interventions in
frailty
Ten years ago Two years ago
One month ago ‘He is a fall waiting to
happen
“Dad is slowing down”
“I’m not as steady
on my feet as I was”

Proportion alive
Time
Primary care electronic Frailty Index (eFI): survival plots (n=227,648; >65y)
Fit Mild frailty Moderate frailty Severe frailty
5 yrs

Implementation of a pathway of care for older
people living with frailty – NHS England Guidance
If frail older people are supported in living independently and understanding their long-term conditions, and educated to manage them effectively, they are less likely to reach crisis, require urgent care support and experience harm.
This document summarises the evidence of the effects of an integrated pathway of care for older people and suggests how a pathway can be commissioned effectively using levers and incentives across providers.
http://www.england.nhs.uk/ourwork/pe/safe-care/
11
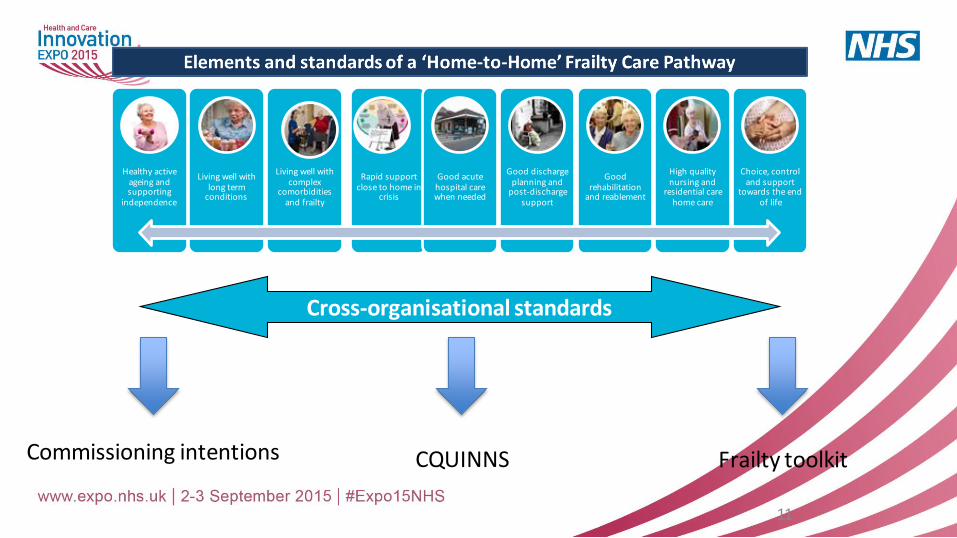
Healthy active ageing and supporting
independence
Living well with long term
conditions
Living well with complex
comorbidities and frailty
Rapid support close to home in
crisis
Good acute hospital care when needed
Good discharge planning and
post-discharge support
Good rehabilitation
and reablement
High quality nursing and
residential care home care
Choice, control and support
towards the end of life
Cross-organisational standards
Commissioning intentions CQUINNS Frailty toolkit
Frailty Toolkit for Primary Care
Includes: • Case finding tools and advice • How to populate frailty registers and
read coding • Comprehensive geriatric assessment • Care coordination • Care planning • Medication review in frail older
people http://www.nhsiq.nhs.uk/improvement-programmes/long-term-conditions-and-integrated-care/long-term-conditions-improvement-programme/house-of-care-toolkit/national/commissioning/tools-and-levers/enhanced-services-resources.aspx
Integrated Care for Older People with
Frailty and Multimorbidity
Lucy Watson, Director of Quality, Safety and Governance,
Somerset Clinical Commissioning Group
Dr Mike Pearce, GP Somerset Clinical Commissioning Group

Somerset Approach • Somerset Frail Older People’s Programme Board with
representation from health, social care, independent sector, and patient and user groups
• Reference to evidence base from the British Geriatric Society and best practice
• Somerset Pathway for Older People with frailty published in April 2014
• Workshop held in December 2014 to lead implementation of the pathway with NHS England national lead
• Good engagement from all providers and voluntary sector

Costs and Benefits Improved quality of care and experience for older people;
• Older people are admitted to hospital more frequently, have longer length of stay and occupy more bed
days
Sustainable system against rising demand;
• Older people are some of the highest cost users of services
Overall pathway to be delivered within existing resources;
• Current resource can deliver ‘better to more’
Significant opportunity to move support out from hospital centric care to community care and
supporting neighbourhoods;
• Frailty does not respond to the current single condition medical model
Efficiency savings through collaborative teams / models of working across providers, including
third sector;
• Better use of the staffing resources across the whole system

Vision & Purpose
• Maintaining health and independence for Older People
• Improve the quality of services for our patients and provide value for
money through transformation of the health and care system
• Engagement with local communities and local voluntary
organisations
• Care in the right place at the right time by the right staff.
Vision of Older People
“ I can plan my care with people who work together to understand me and my carer(s), allow me control, and bring
together services to achieve the outcomes important to me.”
National Voices

Framework for Older People

South Somerset – Vanguard programme
• Symphony Project in South Somerset to implement House of Care to improve care and outcomes for people with long term
conditions
• Development of a Symphony dataset across all health services and social care identified increasing number of co morbidities that
people have drives up the cost and use of care services
• A Symphony care model was developed
• Led to the Vanguard programme and three Local Implementation
Groups to test and learn based on the Symphony care model

Somerset Frailty Programme
• Accept frailty as a long term condition and gained support for frailty to be included in the Symphony data set
• Strong clinical leadership and support and agreement on pathway
and frailty tools • CQUIN for frailty developed for all NHS Trust contracts for 2015 –
16 to include use of Rockwood clinical frailty scale and
comprehensive geriatric assessment
• Development of personalised care planning and case management through LIGs and Test and Learn Pilots

Common Principles • Frail older people should have access to comprehensive geriatric
assessment in order to develop a co-ordinated and integrated plan for
treatment and long term follow up
• A shared definition of the target population
• Agreement on risk stratification to target the right service at the right level to
the right people to deliver the best possible outcome
• An integrated multi-disciplinary and system wide approach to include
information sharing across organisations and voluntary sector
• Care co-ordinator role with appropriate clinical skills, authority and expertise
to negotiate care across pathways and organisations.

Engage primary care • Agreement on use of screening tools and Comprehensive Geriatric
Assessment, case finding to identify frail older people and develop care
plans
• Engaged with GP champions to support development of frailty registers
using the Unplanned Admissions DES
• Using Joint Commissioning as the route with NHS E and LMC support
• Recruiting a frailty lead to support workforce development across public
and independent sector
• Provision of Master classes to support implementation in primary care
and with the voluntary sector and peer support projects through LIGs

Successes • Taunton and Somerset NHS Foundation Trust recruiting two frailty
practitioners to support implementation of the acute pathway
• Engagement with the Consultant workforce to support the pathway
and improved care for older people in hospital
• Yeovil have frail older people’s assessment unit
• Agreed one clinical management plan to follow the patient
• Benefits of using contract levers with clinical engagement

Outcomes • Older people want the ability to remain at home in clean, warm,
affordable accommodation
• To remain socially engaged; to continue with activities that give
their life meaning
• To contribute to their family or community; to feel safe and to
maintain independence, choice, control, personal appearance and dignity
• To be free from discrimination; and to feel they are not a ‘burden’ to
their own families and that they can continue their own role as caregivers

Next Steps
• Transfer of responsibility for delivery to Local Implementation
Groups and Test and Learn Pilots and integrating relevant work
programmes.
• Using our Patient Participation Groups to start social discussions
about planning for frailty and choices at end of life- starting the
conversation
• Development of electronic frailty registers in primary care
• Demonstrating we have improved care and outcomes for older
people

Thank you for listening