integrated care for persons with serious mental illness: deinstitutionalization redu x? steve leff,...
TRANSCRIPT
Integrated Care for Persons with Serious Mental Illness:
Deinstitutionalization Redux? Steve Leff, Ph.D.
Human Services Research InstituteHarvard Medical School Department of Psychiatry
at the Cambridge Health AllianceCarl Taube Award Lecture
American Public Health AssociationBoston, MA
November 4, 2013
Presenter Disclosures
(1) The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Steve Leff, Ph.D.
No Relationships to Disclose
Persons with primary diagnoses of schizophrenia, bipolar disorder and other disorders commonly associated with
major functional impairments
Serious Mental Illness
National Institute of Mental Health, (1987). Community Support Systems for Persons With Long-Term Mental Illness: Questions and Answers Rockville. Rockville, MD.

What I’m going to cover
1. Problems in the early planning of services for persons with serious mental illness under deinstitutionalization
2. What we know so far about integrated care3. A simulation approach to planning services for
persons with serious mental illness: some theory and a demonstration
4. Lessons learned from applying a simulation approach in multiple sites
1. Problems in Early Planning for Persons with Serious Mental Illness
Under Deinstitutionalization
Although some planners and planning agencies continue to stress the development of model programs as solutions for the varied problems of deinstitutionalization, discrepancies between isolated successful model endeavors and widespread service system failures are becoming so apparent that the need for systems-oriented planning strategies is increasingly acknowledged.
Bachrach, Leona. L. (1983). "New directions in deinstitutionalization planning." New Directions for Mental Health Services 1983(17): 93-106
Davis, L., et al. (2012). "Deinstitutionalization? Where Have All the People Gone?" Current Psychiatry Reports 14(3): 259-269.
While access to mental health care and the well-being of individuals with mental illness continues to improve overall, the shift from long-term psychiatric care in large and isolated state hospitals to a more diversified short-term outpatient care model may primarily benefit those with less severe mental health conditions…. In contrast, those with more severe and chronic mental illnesses, with the greatest need, often fare the worst. Overall, evidence suggests that a high prevalence of functional impairment, unemployment, poverty, and isolation characterizes present-day life for most individuals with chronic and severe mental illness [58•, 71••,73]. Following deinstitutionalization, individuals with SMI were discharged and seemingly scattered about, ending up everywhere and nowhere. Where are they now? While the answer to the question is not always easy to find, at least asking the question implies that someone is looking, and we need to be asking both where they are and how they are.
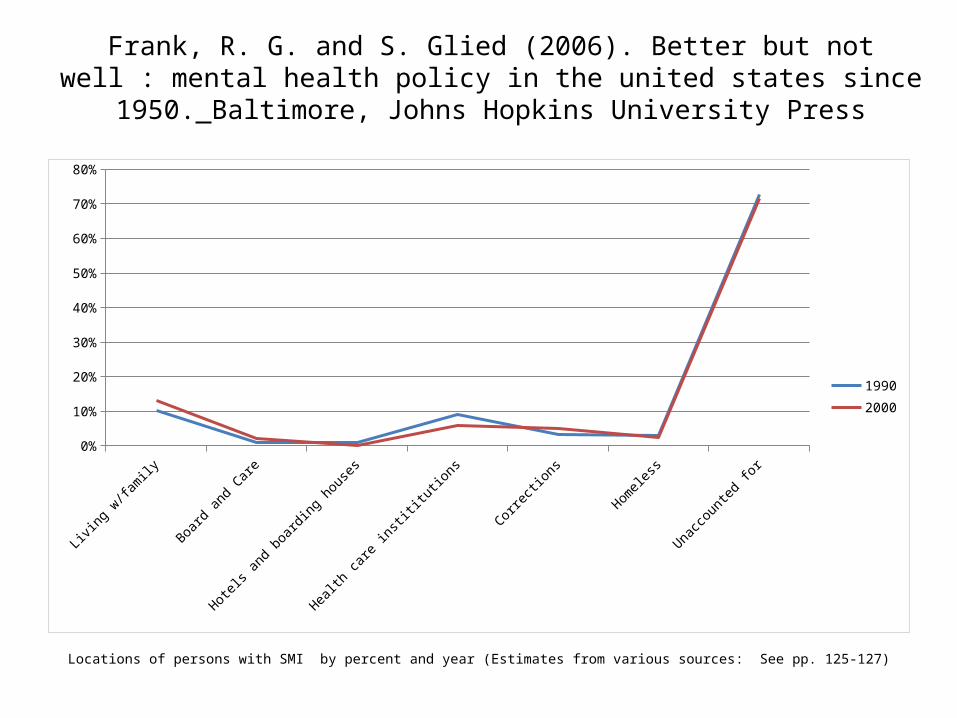
Locations of persons with SMI by percent and year (Estimates from various sources: See pp. 125-127)
Living w
/family
Board an
d Care
Hotels a
nd boarding h
ouses
Health
care
instititutions
Correcti
ons
Homeless
Unaccounted
for
0%
10%
20%
30%
40%
50%
60%
70%
80%
19902000
Frank, R. G. and S. Glied (2006). Better but not well : mental health policy in the united states since 1950. Baltimore, Johns
Hopkins University Press
Program planning for the chronically mentally ill must proceed from certain basic, and interrelated, planning principles - principles whose importance has been demonstrated through a quarter of a century’s experience. These include …the exercise of caution and careful reasoning in adopting and implementing new program plans.
Bachrach, L. L. (1983). "New directions in deinstitutionalization planning." New Directions for Mental Health Services 1983(17): 93-106
At the present time, deinstitutionalized services for the chronically mentally ill are less than satisfactory. If planning for the future is to reverse the trend of incomplete service delivery for this population, it must start with the recognition and application of certain fundamental concepts. Effective planning requires idealism, vision, and a sense of reality.
Bachrach, L. L. (1979). "Planning Mental Health Services for Chronic Patients." Hosp Community Psychiatry 30(6): 387-393
Garber, A. M. (2008). "A menu without prices." Ann Intern Med 48(12): 964-966.
We won’t have an efficient health care system until we learn the [cost] of … interventions and use the knowledge effectively.
Another problem with “vision”: A menu without prices.
For example, we knew that a day in a community support program might cost less than a day in the community, but would 365 days in community support cost less than 2 weeks in the hospital followed by some unspecified community care?
2. What we know so far about integrated care
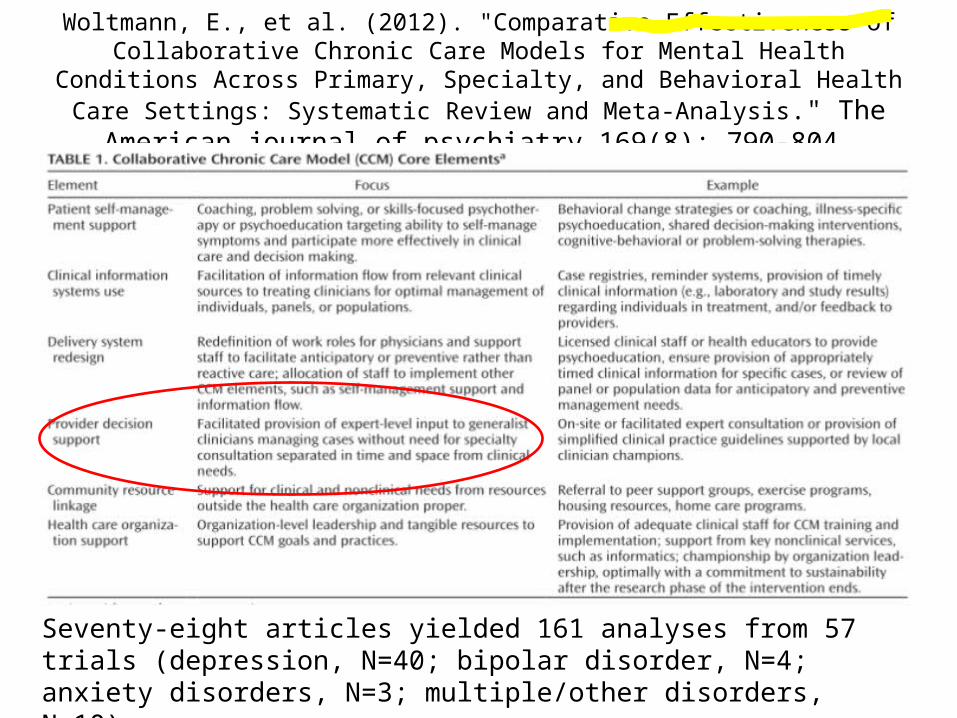
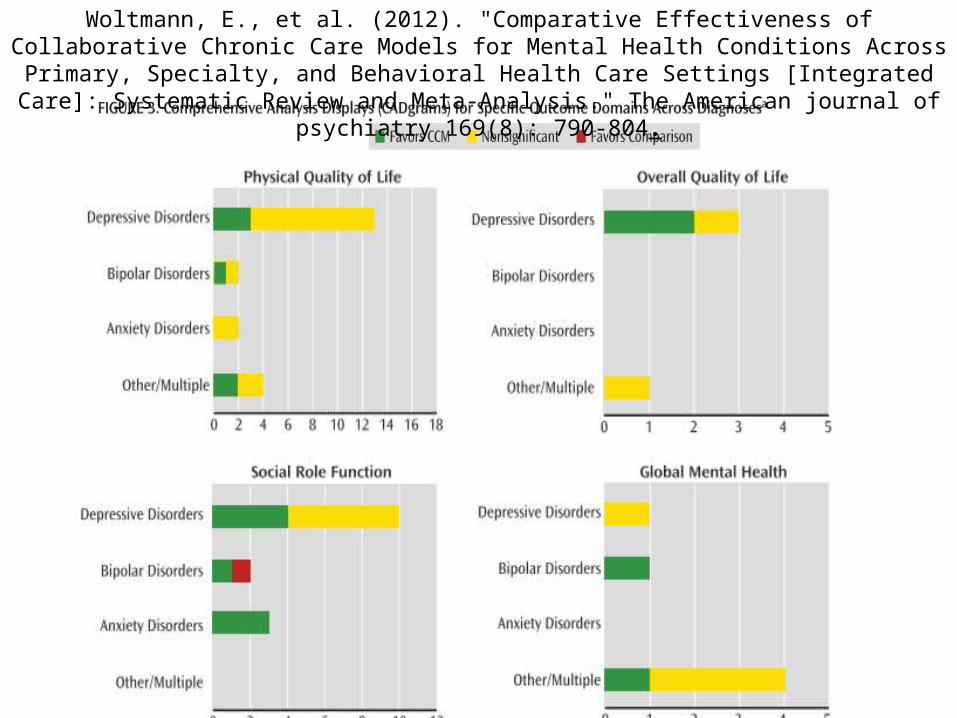
Woltmann, E., et al. (2012). "Comparative Effectiveness of Collaborative Chronic Care Models for Mental Health Conditions Across Primary, Specialty, and Behavioral Health
Care Settings: Systematic Review and Meta-Analysis." The American journal of psychiatry 169(8): 790-804.
Seventy-eight articles yielded 161 analyses from 57 trials (depression, N=40; bipolar disorder, N=4; anxiety disorders, N=3; multiple/other disorders, N=10).
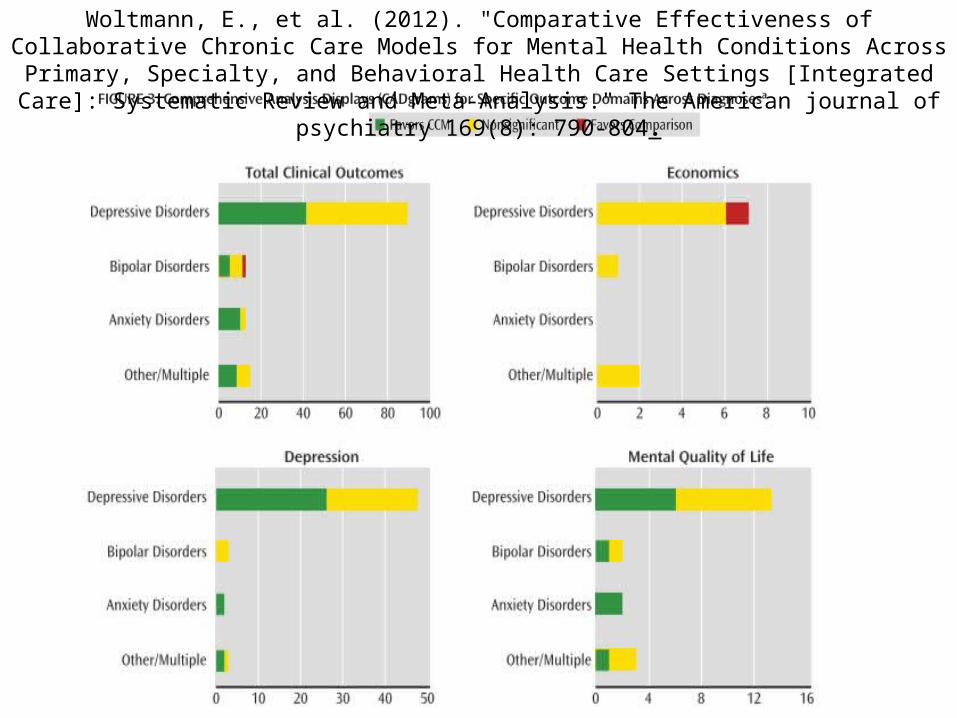
Woltmann, E., et al. (2012). "Comparative Effectiveness of Collaborative Chronic Care Models for Mental Health Conditions Across Primary, Specialty, and Behavioral Health Care Settings [Integrated Care]: Systematic Review and Meta-Analysis." The American journal of psychiatry 169(8): 790-804.
Woltmann, E., et al. (2012). "Comparative Effectiveness of Collaborative Chronic Care Models for Mental Health Conditions Across Primary, Specialty, and Behavioral Health Care Settings [Integrated Care]: Systematic Review and Meta-Analysis." The American journal of psychiatry 169(8): 790-804.
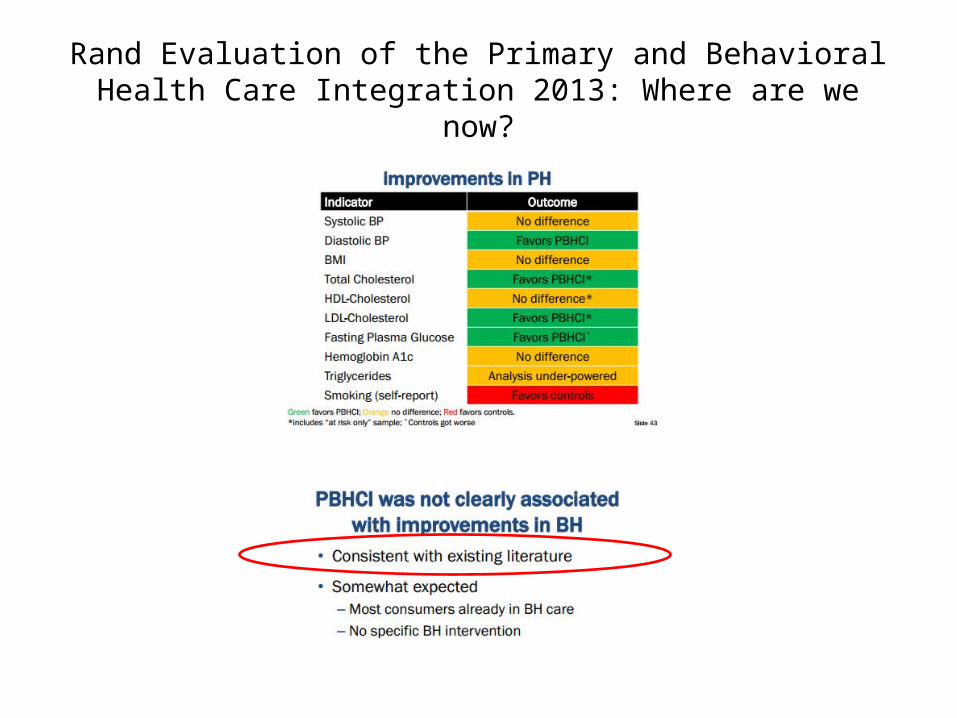
Rand Evaluation of the Primary and Behavioral Health Care Integration 2013: Where are we now?
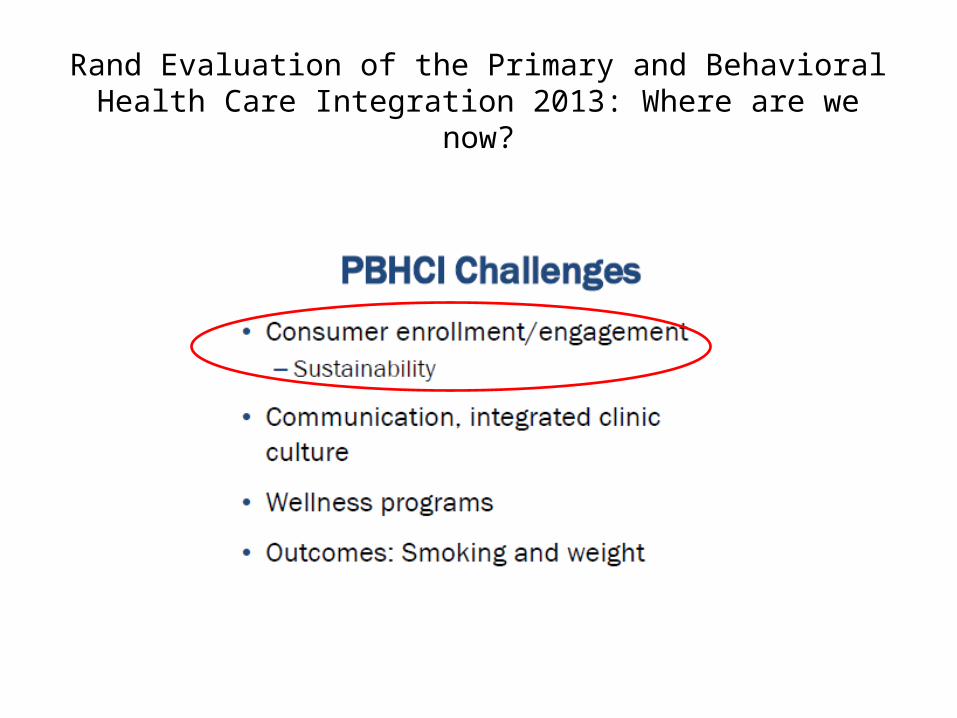
Rand Evaluation of the Primary and Behavioral Health Care Integration 2013: Where are we now?
Have we jumped the gun?
Levin, G. and E. B. Roberts (1976). The dynamics of human service delivery. Cambridge, Mass., Ballinger Pub. Co.
If many studies ranging over a long period of time are needed to build a good scientific account of some social phenomenon, the social practitioner will probably not have time to wait….At every moment he must do something “next.” (p.7)
3. A Simulation Approach to Planning Services for Persons with Serious
Mental Illness: Theory and a Demonstration
Hargreaves, W. A. (1986). "Theory of psychiatric treatment systems. An approach." Arch Gen Psychiatry 43(7): 701-705.
If we want to optimize treatment system effectiveness within available resources, we need some logical tools to help us calculate the implications of the knowledge gained from clinical trials. This logic should also tell us which of our gaps in knowledge are the most important to fill. My view is that this requires a theory of the way treatment systems interact with the life course of persons … To be useful, such a theory of mental health services must be sufficiently detailed and valid to forecast an array of impacts of proposed system changes. Such theory would be a stimulus and guide to research, as well as a tool for program management.
Bachrach, L. L. (1983). "New directions in deinstitutionalization planning." New Directions for Mental Health Services 1983(17): 93-106
The simplest kind of [planning] involves studying the patient’s level of functioning and attempting to place him in the setting most compatible with that level. But deinstitutionalization is most sensitive and meaningful if it carries the process one step further and enhances, where appropriate, the patient’s skill development.
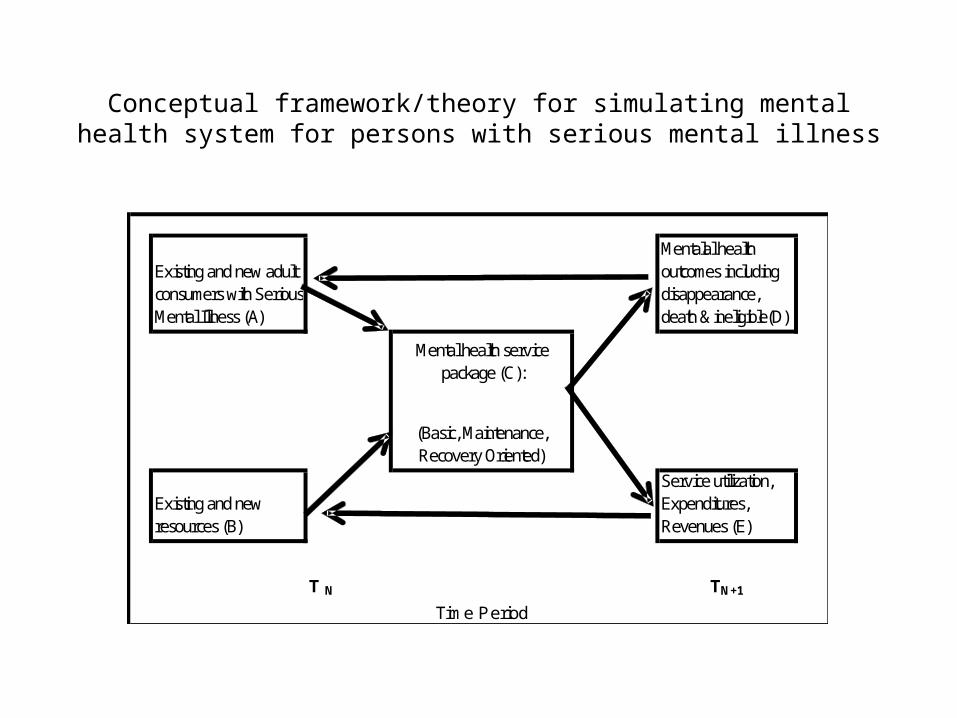
Conceptual framework/theory for simulating mental health system for persons with serious mental illness
Existing and new adult consumers with Serious Mental Illness (A)
Mentalal health outcomes including disappearance, death & ineligible(D)
Mental health service package (C):
(Basic, Maintenance, Recovery Oriented)
Existing and new resources (B)
Service utilization, Expenditures, Revenues (E)
T N TN+1
Time Period
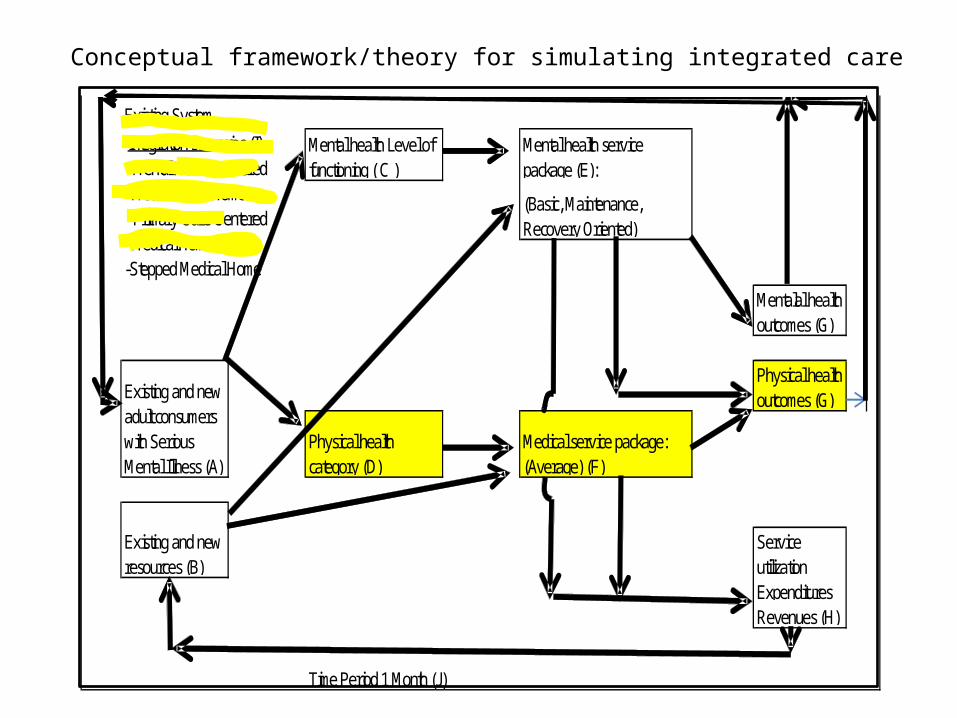
Conceptual framework/theory for simulating integrated care
Existing System
Mental health Level of functioning ( C )
Mental health service package (E):
(Basic, Maintenance, Recovery Oriented)
Mentalal health outcomes (G)
Physical health outcomes (G)
Physical health category (D)
Medical service package: (Average) (F)
Service utilizationExpendituresRevenues (H)
Time Period 1 Month (J)
Integration scenarios (I) -Mental Health Centered Medical Care Home -Primary Care Centered Medical Home-Stepped Medical Home
Existing and new resources (B)
Existing and new adult consumers with Serious Mental Illness (A)
Sonnenberg, F. A. and J. R. Beck (1993). "Markov Models in Medical Decision Making: A Practical Guide." Med Decis Making 13(4): 322-338.
Markov models are useful when a decision problem involves [operations that are] continuous over time, when the timing of events is important, and when important events may happen more than once…Markov models assume that a patient is always in one of a finite number of discrete health states…[and]…All events are represented as transitions from one state to another. …The ability of the Markov model to represent repetitive events and the time dependence of both probabilities and utilities allows for more accurate representation of clinical settings that involve these issues...

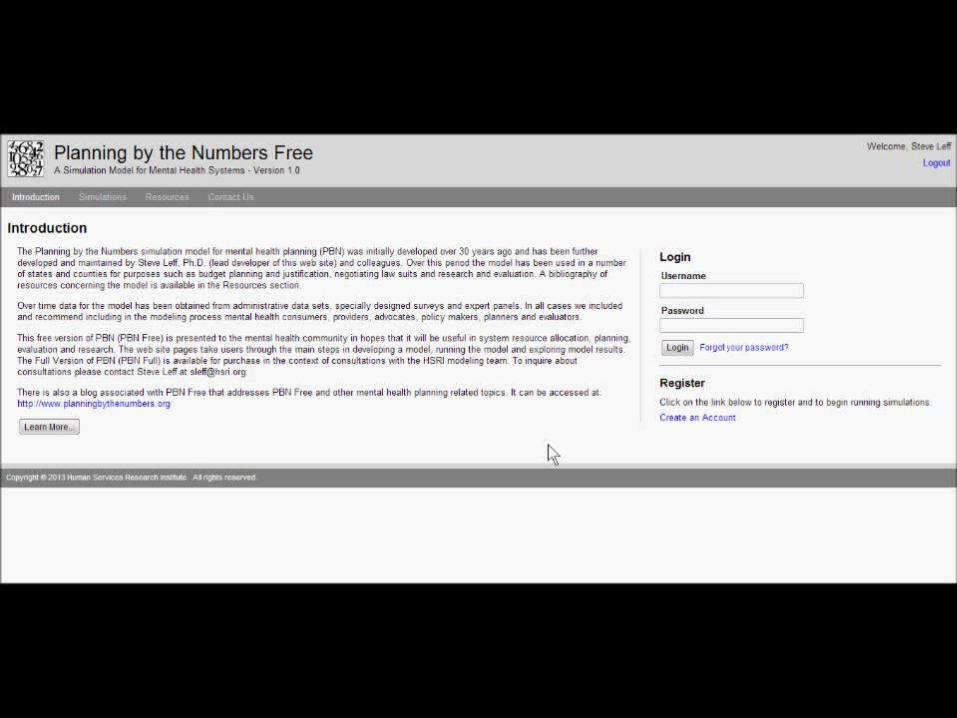
PBN Free Demonstration: Web and PC-based Plans When You Need Them
PBN Free: a web and PC implemented simulation for planning services for persons
with serious mental illness
4. Lessons Learned From Applying a Simulation Approach in Multiple Sites
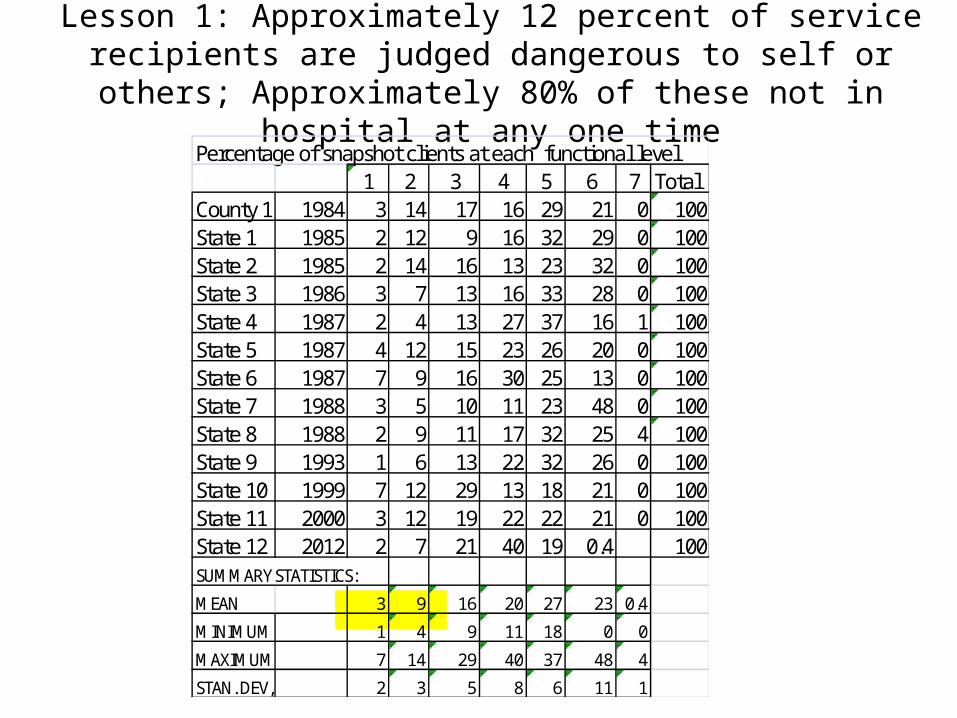
Lesson 1: Approximately 12 percent of service recipients are judged dangerous to self or others; Approximately 80% of these not in
hospital at any one timePercentage of snapshot clients at each functional level
1 2 3 4 5 6 7 Total County 1 1984 3 14 17 16 29 21 0 100State 1 1985 2 12 9 16 32 29 0 100State 2 1985 2 14 16 13 23 32 0 100State 3 1986 3 7 13 16 33 28 0 100State 4 1987 2 4 13 27 37 16 1 100State 5 1987 4 12 15 23 26 20 0 100State 6 1987 7 9 16 30 25 13 0 100State 7 1988 3 5 10 11 23 48 0 100State 8 1988 2 9 11 17 32 25 4 100State 9 1993 1 6 13 22 32 26 0 100State 10 1999 7 12 29 13 18 21 0 100State 11 2000 3 12 19 22 22 21 0 100State 12 2012 2 7 21 40 19 0.4 100SUMMARY STATISTICS:
MEAN 3 9 16 20 27 23 0.4
MINIMUM 1 4 9 11 18 0 0
MAXIMUM 7 14 29 40 37 48 4
STAN. DEV, 2 3 5 8 6 11 1
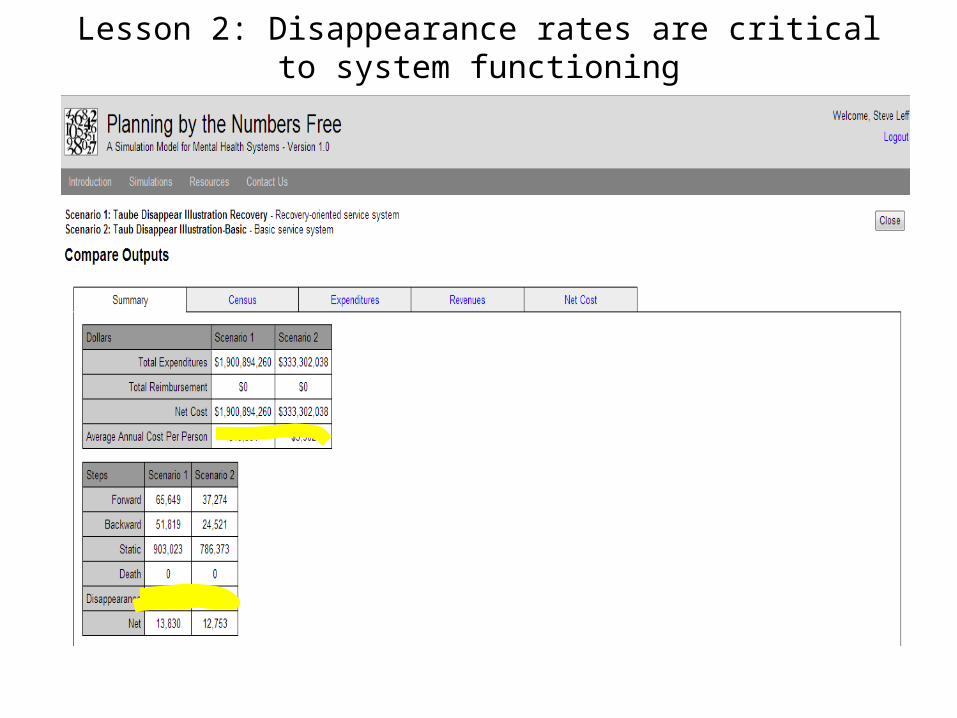
Lesson 2: Disappearance rates are critical to system functioning
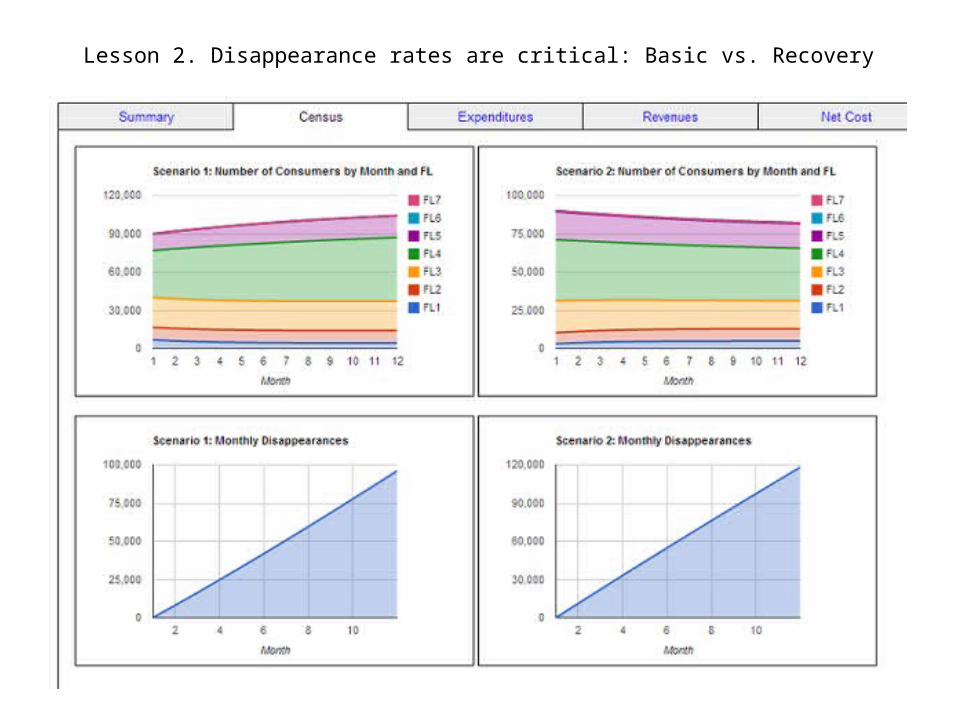
Lesson 2. Disappearance rates are critical: Basic vs. Recovery
Olfson, M., et al. (2009). "Dropout From Outpatient Mental Health Care in the United States." Psychiatr Serv 60(7): 898-907.
Roughly one-fifth of adults in mental health treatment dropped out before completing the recommended course of treatment. Dropout was most common in the general medical sector and varied by patient characteristics across treatment sectors. Interventions focused on high-risk patients and sectors that have higher dropout rates will likely be required to reduce the large proportion of patients who prematurely terminate treatment.
Lesson 2. Disappearance rates are critical
Lesson 2. Disappearance rates are criticalLevin, G. (1977). "Point of view: poor quality is the solution, not the problem."
Health Care Manage Rev 2(3): 69-72.
Edlund, M. J., et al. (2002). "Dropping Out of Mental Health Treatment: Patterns and Predictors Among Epidemiological Survey Respondents in the United States
and Ontario." Am J Psychiatry 159(5): 845-851.
Mental health treatment dropout is a serious problem, especially among patients who have low income, are young, lack insurance, are offered only single-modality treatments, and have negative attitudes about mental health care. Cost-effective interventions targeting these groups are needed to increase the proportion of patients who complete an adequate course of treatment.
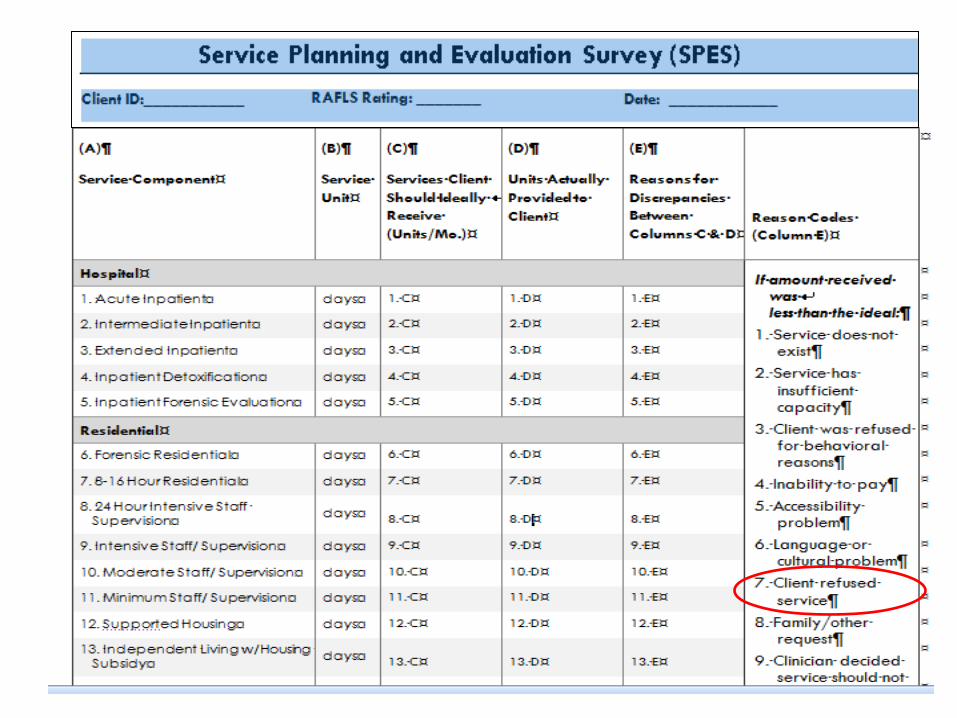
Lesson 3. Consumers must be included in system planning
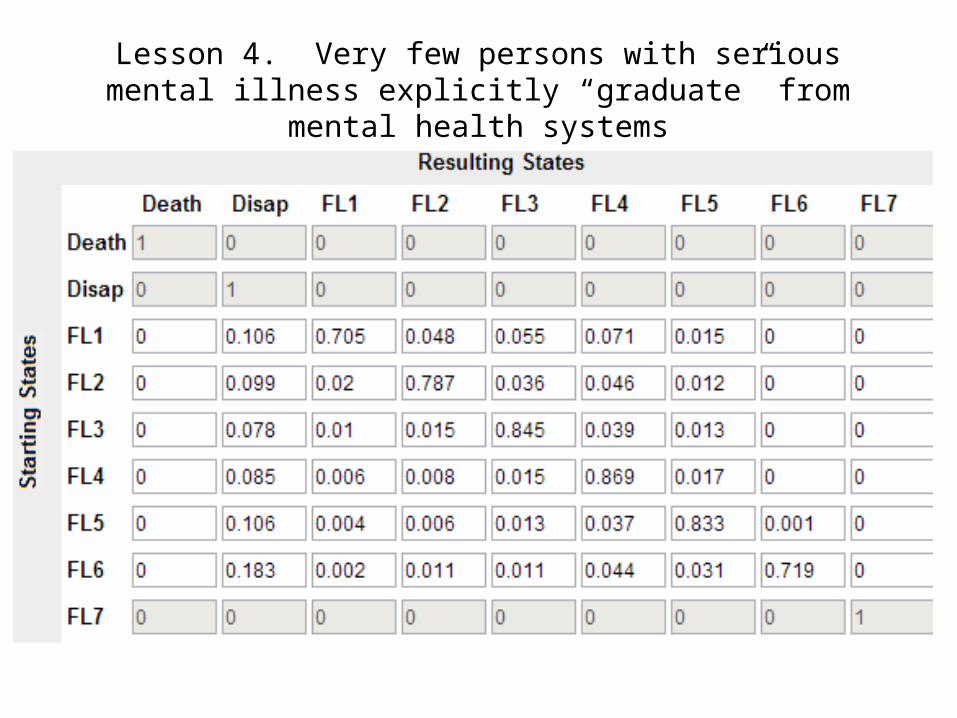
Lesson 4. Very few persons with serious mental illness explicitly “graduate” from mental health systems
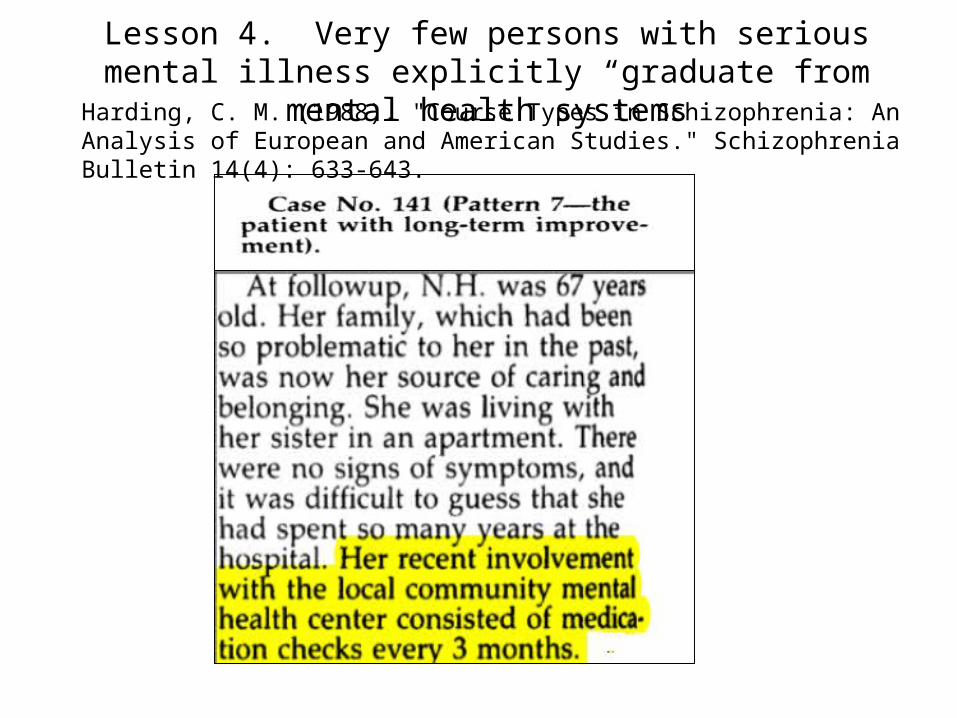
Harding, C. M. (1988). "Course Types in Schizophrenia: An Analysis of European and American Studies." Schizophrenia Bulletin 14(4): 633-643.
Lesson 4. Very few persons with serious mental illness explicitly “graduate from mental health systems
Lesson 5. Health state models have several distinct advantages over traditional multivariate approaches to analyzing data for
complex diseases such as serious mental illnesses.
1. Health states provide a convenient framework for performing longitudinal analyses. Can estimate long-run fraction of people in each health state in addition to cross-sectional distributions during study periods..
2. Partitioning of population into health states leads to a more richly informative analysis than simply examining mean differences.
3. Health states can be combined with wide variety of outcome and output variables, such as costs …to calculate long-run financial or utility consequences. Allows objective long-term health policy decisions by balancing treatment effectiveness against societal costs.
James, G. M., et al. (2006). "A comparison of outcomes among patients with schizophrenia in two mental health systems: a health state approach."
Schizophr Res 86(1-3): 309-320.
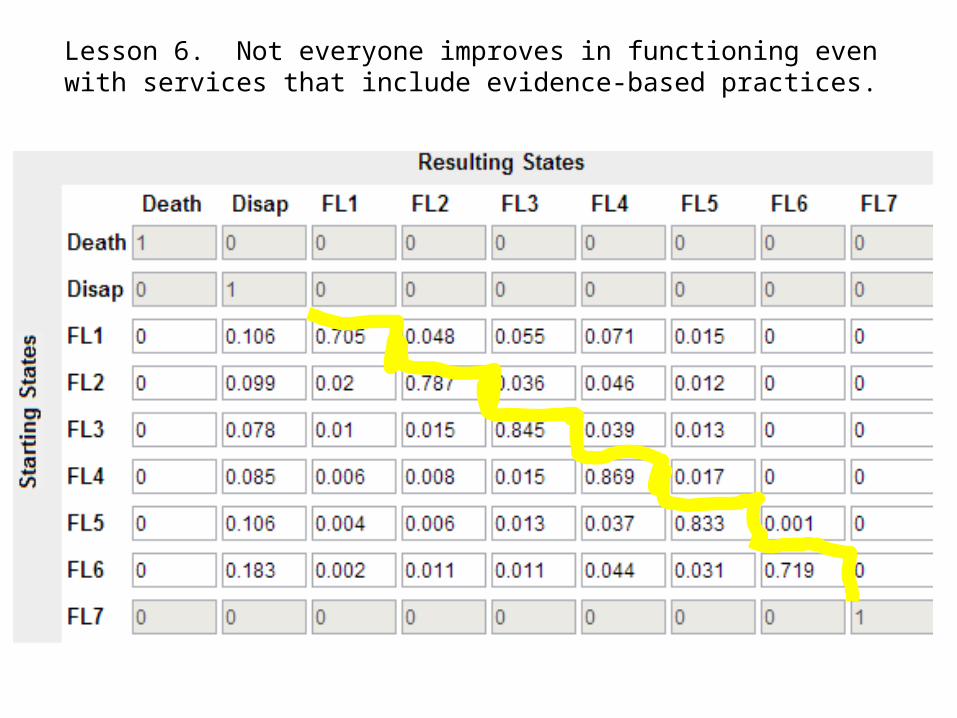
Lesson 6. Not everyone improves in functioning even with services that include evidence-based practices.
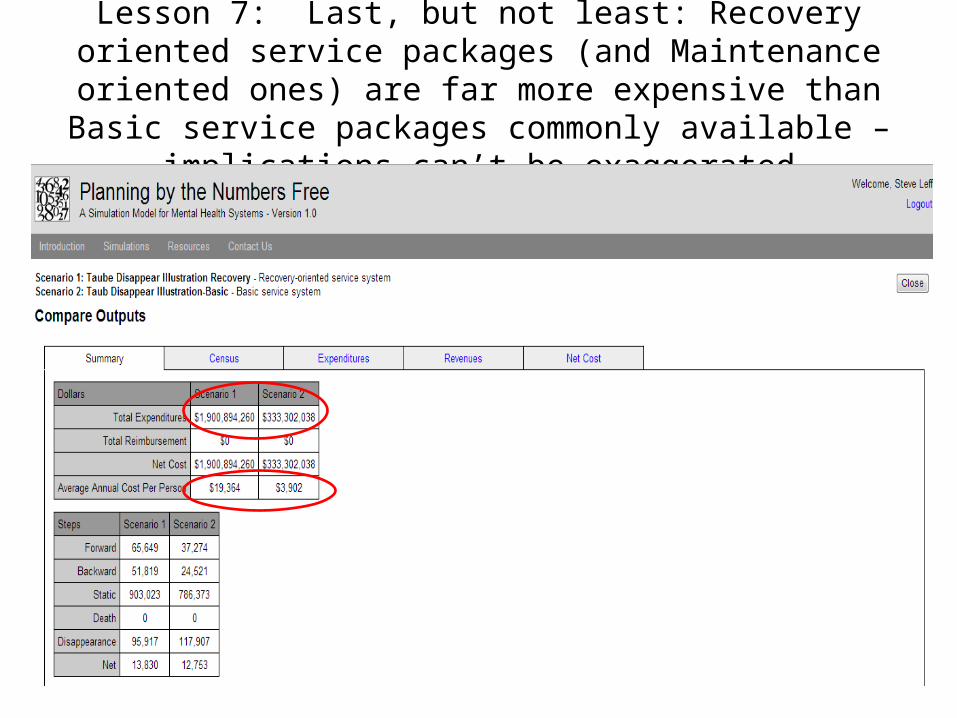
Lesson 7: Last, but not least: Recovery oriented service packages (and Maintenance oriented ones) are far more expensive than Basic service packages commonly available – implications can’t
be exaggerated
Implications for Different Audiences: The pessimism of science and the optimism of clinicians and consumersa
• For researchers: Some things systems planners would like to know:– Outcomes as transition probabilities for service packages differing in effectiveness– Costs for service packages differing in effectiveness– Information on what happens to consumers who drop out of treatment systems: How many
no longer need care? How many enter other systems (e.g. Corrections, Primary care) etc.? – What are models for integrating care and what are their costs and effectiveness– How can psychosocial services for persons with SMI be delivered in integrated care
• For planners: Go beyond visionary planning. Generalize from the evidence available cautiously. The devils are in empirically determined cost and effectiveness details “laid end-to-end.” No menus without prices.
• For clinicians: Improving systems will be extremely difficult and take considerable time, but keeping some of these lessons in mind, you can improve things for the individuals you serve
• For consumers: Achieving recovery within mental health systems may become more complicated, perhaps more possible. It’s important to participate in the planning process and pay close attention to what is being considered. Don’t assume there is good evidence and careful analysis behind options being considered.
aBurawoy, M. (2011). "Making Public Sociology: Its Pitfalls and its Possibilities." Global Labour Journal 2(1): 1-4: “Pessimism of the intellect, optimism of the will”
“The history of mental health treatment is replete with examples of well-intentioned interventions, developed and perpetuated on the basis of nothing more than a potentially innovative concept, a desperate patient and provider population, a charismatic proponent, and little, if any, evidence…. In the face of budgetary pressures and outright cutbacks, states and local communities will inevitably seek additional funding for direct service support. Tempting as it is to respond with reprogramming of funds and reduction or elimination of knowledge enhancement efforts, there can be no more foolish and shortsighted a decision”.
For the Federal Government and Other Mental Health Program Funders
Bernard S. Arons, M.D. Letter in response to: S. Sharfstein: The Loss of Federal Support for Multisite Demonstrations. Psychiatric Services, Dec 2005; 56 (12); 1621-1621. doi: 10.1176/appi.ps.56.12.1621
For the Federal Government and Other Mental Health Program Funders
1. In designing programs, consider what is already known2. Involve evaluators in program design before the program is begun, not,
as in some cases, one year after3. Provide enough resources for at least quasi-experimental designs with
appropriate control groups4. Include formative evaluation with implementation monitoring5. Provide staffing to require and enforce program fidelity6. Use outcome measures appropriate to the program. If the National
Outcome Measures (NOMS) are going to be used enforce best measurement practices
7. Make results known once they pass quality tests8. Provide funds for dissemination of evaluation results