integrated health service delivery during covid-19: a
TRANSCRIPT

1Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
Integrated health service delivery during COVID-19: a scoping review of published evidence from low- income and lower- middle- income countries
Md Zabir Hasan ,1,2 Rachel Neill,2 Priyanka Das,2 Vasuki Venugopal,3 Dinesh Arora,2 David Bishai,4 Nishant Jain,5 Shivam Gupta2
Original research
To cite: Hasan MZ, Neill R, Das P, et al. Integrated health service delivery during COVID-19: a scoping review of published evidence from low- income and lower- middle- income countries. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
Handling editor Stephanie M Topp
► Additional supplemental material is published online only. To view, please visit the journal online (http:// dx. doi. org/ 10. 1136/ bmjgh- 2021- 005667).
Received 10 March 2021Accepted 19 May 2021
For numbered affiliations see end of article.
Correspondence toDr Md Zabir Hasan; zabir. hasan@ gmail. com
© Author(s) (or their employer(s)) 2021. Re- use permitted under CC BY. Published by BMJ.
AbsTrACTbackground Integrated health service delivery (IHSD) is a promising approach to improve health system resilience. However, there is a lack of evidence specific to the low/lower- middle- income country (L- LMIC) health systems on how IHSD is used during disease outbreaks. This scoping review aimed to synthesise the emerging evidence on IHSD approaches adopted in L- LMIC during the COVID-19 pandemic and systematically collate their operational features.Methods A systematic scoping review of peer- reviewed literature, published in English between 1 December 2019 and 12 June 2020, from seven electronic databases was conducted to explore the evidence of IHSD implemented in L- LMICs during the COVID-19 pandemic. Data were systematically charted, and key features of IHSD systems were presented according to the postulated research questions of the review.results The literature search retrieved 1487 published articles from which 18 articles met the inclusion criteria and included in this review. Service delivery, health workforce, medicine and technologies were the three most frequently integrated health system building blocks during the COVID-19 pandemic. While responding to COVID-19, the L- LMICs principally implemented the IHSD system via systematic horizontal integration, led by specific policy measures. The government’s stewardship, along with the decentralised decision- making capacity of local institutions and multisectoral collaboration, was the critical facilitator for IHSD. Simultaneously, fragmented service delivery structures, fragile supply chain, inadequate diagnostic capacity and insufficient workforce were key barriers towards integration.Conclusion A wide array of context- specific IHSD approaches were operationalised in L- LMICs during the early phase of the COVID-19 pandemic. Emerging recommendations emphasise the importance of coordination and integration across building blocks and levels of the health system, supported by a responsive governance structure and stakeholder engagement strategies. Future reviews can revisit this emerging evidence base at subsequent phases of COVID-19 response and recovery in L- LMICs to understand how the approaches highlighted here evolve.
InTroduCTIonThe COVID-19 has been one of the most signif-icant healthcare emergencies in the past 100 years, claiming over 3.14 million lives world-wide from December 2019 to April 2021.1 Although initially concentrated in developed countries, the pandemic has increasingly taken a toll on low/lower- middle- income countries (L- LMICs),2–4 with India second in
Key questions
What is already known? ► Integrated health service delivery (IHSD) is a prom-ising approach towards Universal Health Coverage and can improve health systems resiliency during health emergencies.
► There is a lack of evidence on IHSD in low/lower- middle- income countries (L- LMICs), and there are no existing reviews on IHSD in L- LMICs during the COVID-19 pandemic.
What are the new findings? ► IHSD is occurring in L- LMICs during COVID-19, with the bulk of evidence coming from India.
► Horizontal and systematic integration was most re-ported in the literature, including the development of COVID-19 specific surveillance, testing, triage, quarantine and treatment protocols integrated into existing service delivery systems while maintaining routine health service delivery.
► A range of innovative approaches and integration typologies are also being operationalised, including the use of digital health technologies, integration with pharmaceutical and AYUSH (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy—the six types of traditional or complementary medicine systems practiced in India) providers, triage algo-rithms for mental health referrals and leveraging military infrastructure.
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
2 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Key questions
What do the new findings imply? ► IHSD approaches are potentially viable for L- LMIC health systems during health emergencies; however, the design and operational approaches remain context- specific.
► Limited studies outside India were identified, which could either reflect more integration in the Indian health system, a higher COVID-19 burden in India than other L- LMICs at the time of the review, or increased publication opportunities from Indian authors.
► Additional research can update these emerging findings to explore how they evolve throughout the COVID-19 pandemic and to identify additional evidence from other contexts.
total COVID-19 cases.1 Health systems in L- LMICs have faced significant strain during the pandemic. Improving or expanding case surveillance, contact tracing, commu-nications campaigns, combating misinformation and maintaining access to essential health services were estab-lished as the risk mitigation strategies.5–7 However, the fragmented nature of health service delivery in L- LMICs poses extraordinary challenges to meet the dual goal of pandemic response and routine service continuity.8
Integrated health service delivery during CoVId-19 pandemicIntegrated, people- centred health systems are increas-ingly considered a central component of Universal Health Coverage and are globally recognised with an adopted resolution of the 69th World Health Assembly in 2016.9 ‘Integration’ of the health service delivery has many meanings in global health policy and systems research. However, an all- encompassing and appro-priate definition provided by the WHO Regional Office for Europe characterised the integrated health service delivery (IHSD) system as:
An approach to strengthen people- centered health systems through the promotion of the comprehensive delivery of quality services across the life- course, designed accord-ing to the multidimensional needs of the population and the individual and delivered by a coordinated multidisci-plinary team of providers working across settings and lev-els of care … with feedback loops to continuously improve performance and to tackle upstream causes of ill health and to promote well- being through intersectoral and mul-tisectoral actions.10
Integrated care systems are characterised into four typologies,11 which includes: (a) organisational integra-tion, where different organisations coordinated with each other using a single governing structure, (b) functional integration, when non- clinical services were integrated to facilitate health service delivery, (c) service integration, where multiple providers and/or facilities across the level of health system organise themselves for service provi-sions, and (d) clinical integration, when providers or facilities streamlines their clinical care procedures based on a standardised protocol for care.
However, these four typologies are not mutually exclu-sive. One or any combinations of the typologies may be
present while implementing an IHSD model across the primary, secondary or tertiary level of care—also known as vertical integration12—or integrating multiple oper-ating units and/or organisations at the same stage of the health system, known as horizontal integration.13 Regard-less of the integration structure—vertical, horizontal or a mix of both—the IHSD system can be integrated via two mutually exclusive mechanisms.10 When the integration was based on the ethos of shared understanding, mutual collaboration and trust, it is defined as normative integra-tion. On the other hand, systematic integration is led by specific policies and guidelines adopted across the organ-isational and health system levels.
Integrated service delivery is increasingly being emphasised as countries focus on improving the overall resiliency of their health systems.14–16 However, the goals of IHSD reforms and the modalities of implementa-tion often differ across high- income, middle- income, lower- middle- income and low- income country’s health systems. In L- LMICs, most IHSD approaches aim to increase access, coverage and efficacy of specific services for predefined populations,17 including integrating vertical services in primary care18 or merging of multiple vertical services into a common delivery package or inter-vention. The integration processes are often observed at the facility or service delivery level, particularly for HIV/AIDS, tuberculosis, family health and reproductive health services.17–19 However, the evidence base for IHSD is still nascent17–20 and often focused on over- simplified debates of vertical versus horizontal service delivery structure.21
While exploring the history of previous disease outbreaks, it is very much evident that an IHSD model is well suited in response to all four phases of a pandemic14—(a) interpandemic: the period between the pandemics, (b) alert: when a new disease with pandemic potential has been identified in humans, (c) pandemic: period of the global spread of the disease and (d) tran-sition: de- escalation of response and movement towards recovery as risk is reduced across the world. The poten-tial benefit of the integrated care approach is well docu-mented during the HIV/AIDS pandemic in sub- Saharan Africa22 and pandemic influenza in the USA.23 Since the emergence of COVID-19, new evidence is emerging—mainly from the developed countries, such as the UK,24 Italy,25 Greece and Spain26—which has demonstrated a promising outcome of the IHSD approach.
However, there is a dearth of evidence from the L- LMICs on the effect of the IHSD system when COVID-19 is overwhelming their strained resources and fragmented healthcare system.27 According to the Global Health Security index, developed in 2019,28 most L- LMICs are least- prepared in response planning and operationalising health services during a potential pandemic. Consid-ering the fragmented health systems and limited capacity of L- LMICs, they are highly likely to encounter consid-erable challenges in effective and timely response to COVID-19. However, in countries like Bangladesh, India
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 3
BMJ Global Health
and Vietnam, the government response to the pandemic was as stringent as some developed countries.29
For instance, according to the Oxford COVID-19 Government Response Tracker, the stringency of Vietnam and the USA are at the same level (stringency index=56.94). While we cannot directly compare the strategic response of these two countries against COVID-19, Vietnam’s experience with containment of the SARS epidemic may have provided them valuable lessons in pandemic response.30 Following their experience in managing SARS, Vietnam designed to mobilise an inte-grated and comprehensive response with the community and preventive healthcare services, acting together as one united workforce.
Innovation in the IHSD system that emerged from a limited resource setting can provide critical insight for rapid response and decisive action to manage the ongoing or future pandemics. This scoping review aims to compile the existing published evidence of the inte-grated service delivery approach adopted in response to the COVID-19 pandemic in the L- LMICs, systematically map the features, and build the knowledge base of the IHSD systems for practical and evidence- based decision making.
MeTHodsWe have followed the scoping review framework devel-oped by Arksey and O’Malley to structure and imple-ment this scoping review,31 adhering to the checklist of PRISMA Extension for Scoping Reviews32 (see online supplemental file 1 for more details). The collection, screening, synthesis and reporting of evidence in this scoping review adhered to the following five steps: (a) conceptualising the research questions, (b) identifica-tion of relevant peer- reviewed literature, (c) selection of the studies from electronic databases, (d) charting of evidence and (e) collation and synthesis of the data. The detailed protocol of this review is registered at the OSF,27 and we encouraged our readers to review the published protocol of this review.27
Conceptualising the research questionsIn this scoping review, we have aimed to explore published evidence on the IHSD systems implemented in the L- LMICs in response to the COVID-19 pandemic. To achieve this aim, we have tried to answer the following research questions:1. What are the features of the IHSD systems in the L-
LMICs during the COVID-19 pandemic?2. How were the IHSD systems operationalised within
the health systems of L- LMICs to provide healthcare in the context of the COVID-19 pandemic?
3. Considering the opportunities and challenges posed while implementing the IHSD system in L- LMICs, what recommendations can be made for COVID-19 preparedness, response and recovery?
While answering these research questions, we used the broad definition of IHSD proposed by WHO,10 and considered service integration during COVID-19 as—(a) integration of newly developed COVID-19 response activ-ities within the existing health system; (b) integration of specific aspects of the existing health service provision within the COVID-19 response that had relevance for the overall health system and (c) integration of services to support continuity of routine health systems operations during the COVID-19 pandemic.
Identification of relevant peer-reviewed literatureTo identify the initial pool of peer- reviewed literature on COVID-19, a comprehensive search strategy was imple-mented with a wide range of keywords and search terms related to four primary concepts: (a) ‘integrated health service delivery’, (b) ‘COVID-19’, (c) ‘pandemic prepar-edness’ and (d) ‘low and lower- middle income countries’. We conducted a systematic search of the literature in seven electronic databases: PubMed/MEDLINE, Scopus, EMBASE, Web of Science, CINHAL Plus, LitCovid and the WHO COVID-19 literature database. We have restricted the search parameters within an article published in the English language, considering the feasibility of the study. The complete search strategy for PubMed/MEDLINE is provided in online supplemental file 2.
study selectionThe search was implemented across the seven electronic databases on 12 June 2020. Title, abstract and the cita-tion of the searched articles were imported into the Covi-dence systematic review software ( covidence. org) system, which facilitated the removal of duplicates and screen the articles for eligibility. The screening was conducted in two stages—(a) review of title and abstracts and (b) screening of full text—based on predefined eligibility conditions presented in table 1. To align these criteria with our specific research questions, we have consid-ered the ‘Population- Concept- Context’ framework33 to develop the inclusion and exclusion criteria.
Studies that did not explore any implementation of the IHSD system in response to the COVID-19 pandemic in L- LMICs were excluded during the screening process. We included a wide range of literature, such as original arti-cles, protocols, editorials and commentaries, published in the English language between 1 December 2019 and 12 June 2020; however, news and media watch, author’s reply and research highlights were excluded, as they often do not offer the full context of the evidence. Three researchers independently conducted the screening process, with any undisputed disagreement for an article’s inclusion that was adjudicated on by a senior researcher.
Charting of evidenceNext, all eligible articles were re- read, and evidence on IHSD was charted using a standardised data extraction template in Microsoft Excel. As a test extraction exercise, three researchers charted data from five articles, and
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
4 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Table 1 Inclusion and exclusion criteria for the study selection process of the scoping review
Inclusion criteria Exclusion criteria
Concept Integrated health service delivery system
Article without evidence or discussion on integrated health service delivery (eg, a case report on patients with COVID-19 which recommend implementation of integrated health service delivery, and it did not explore any such systems)
Context Health service organised during COVID-19 pandemic
Population Low- income countries and lower- middle- income countries
Countries from the upper- middle- income and high- income categories
Article type Original research, case studies or case reports, commentary or editorial, systematic, scoping, or rapid review, research letter
Author’s reply or opinion, research highlight, news or media watch
Time frame 1 December 2019–12 June 2020
Reporting Published peer- reviewed articlesArticles written in the English language
Article not published in English or without translation
Low- income economies are defined as Gross National Income (GNI) per capita of $1035 or less in 2019 (n=29). Lower- middle- income economies are defined as GNI per capita $1036 and $4045 (n=50) (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups, accessed 26 April 2020).
the result was triangulated to develop a shared under-standing. After completing the data extraction, the entire team reviewed the results to ensure the consistency and robustness of the analysis. Details of the data elements extracted during the charting process are provided in online supplemental file 2.
Collating, synthesising, and reporting the resultsFirst, we summarised the place of origin, objective and design of the studies. The evidence of IHSD systems during the COVID-19 pandemic was summarised into thematic areas to answer the postulated research ques-tions of this scoping review. We have organised the char-acteristics of IHSD systems according to their implemen-tation during different phases of a pandemic (such as alert, pandemic, transition and interpandemic),14 their
structure, and mechanism as a part of the IHSD system. We have also explored the example of integration across all health systems building blocks, informed by recent work by Salam et al,34 which used the nomenclature of the building blocks to compare integration across compo-nents of the health system. Finally, the integrated system’s features were described based on the typology of the inte-gration—clinical, service, functional and organisation. Using a narrative format and with the help of tables, we have reported the result of this scoping review in the next section.
Patient and public involvementThis review was conducted using previously published peer- reviewed literature. Thus, no patients or the public were involved in the planning, design, data acquisition, analysis and dissemination of the study result.
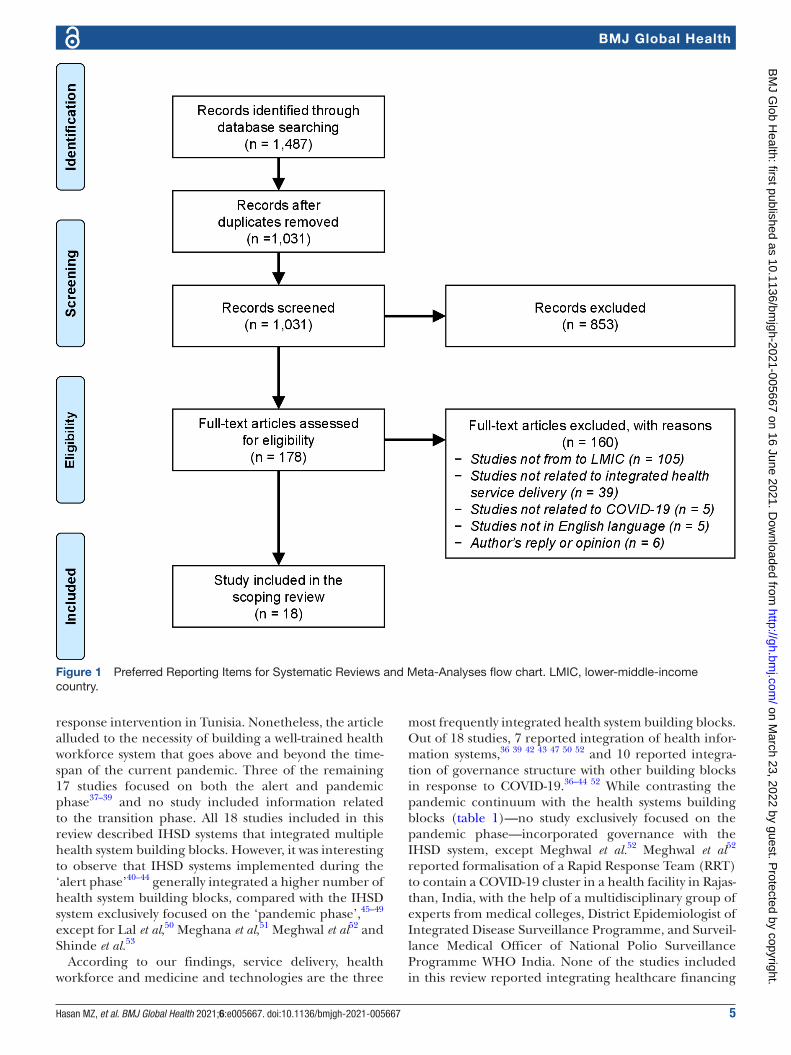
resulTsselection and features of the evidence on IHsd systemThe search process retrieved 1487 published articles from the seven databases. From the pool of retrieved articles, 456 duplicates were removed, and 1031 articles were selected for screening. In total, 853 studies were excluded during the title and abstract review process, and additional 160 articles were excluded after full- text review. In total, 18 articles were included in the scoping review after full- text review. The result of the searching, screening and study selection process is summarised in figure 1 according to the PRISMA chart.35
The majority of the articles included in the review orig-inated from the WHO South- East Asia region (n=14), including 12 studies from India and 1 study from Nepal and Vietnam. The remaining studies are from Tunisia, Bolivia, African Region (information reported from Algeria, Cameroon, Cote d’Ivoire, Gambia, Madagascar, Nigeria, Rwanda, Senegal, South Sudan, Uganda) and East Mediterranean Region (information reported from Egypt, Iraq, Jordan, Morocco, Saudi Arabia, Sudan, Tunisia). While most of the articles were commentary or editorial (n=7) and reviews (n=6), the eligible articles also included three observational studies and two inter-vention protocols.
operational features of the IHsd system with the health systems of l-lMICsTable 2 presents the operationalisation of IHSD systems reported within the selected studies considering the context of COVID-19 and based on their primary focus on the phase of the pandemic, the structure and mech-anism of integration and the health systems building blocks considered to be integrated as part of the IHSD effort.
The majority of the study focused on either alert or the pandemic phase while implementing the IHSD system, except Zgueb et al,36 which focused both on the interpandemic and alert phases to describe the develop-ment and implementation of a novel psychological crisis
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 5
BMJ Global Health
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta- Analyses flow chart. LMIC, lower- middle- income country.
response intervention in Tunisia. Nonetheless, the article alluded to the necessity of building a well- trained health workforce system that goes above and beyond the time-span of the current pandemic. Three of the remaining 17 studies focused on both the alert and pandemic phase37–39 and no study included information related to the transition phase. All 18 studies included in this review described IHSD systems that integrated multiple health system building blocks. However, it was interesting to observe that IHSD systems implemented during the ‘alert phase’40–44 generally integrated a higher number of health system building blocks, compared with the IHSD system exclusively focused on the ‘pandemic phase’,45–49 except for Lal et al,50 Meghana et al,51 Meghwal et al52 and Shinde et al.53
According to our findings, service delivery, health workforce and medicine and technologies are the three
most frequently integrated health system building blocks. Out of 18 studies, 7 reported integration of health infor-mation systems,36 39 42 43 47 50 52 and 10 reported integra-tion of governance structure with other building blocks in response to COVID-19.36–44 52 While contrasting the pandemic continuum with the health systems building blocks (table 1)—no study exclusively focused on the pandemic phase—incorporated governance with the IHSD system, except Meghwal et al.52 Meghwal et al52 reported formalisation of a Rapid Response Team (RRT) to contain a COVID-19 cluster in a health facility in Rajas-than, India, with the help of a multidisciplinary group of experts from medical colleges, District Epidemiologist of Integrated Disease Surveillance Programme, and Surveil-lance Medical Officer of National Polio Surveillance Programme WHO India. None of the studies included in this review reported integrating healthcare financing
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

6 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Tab
le 2
O
per
atio
nal f
eatu
res
of t
he in
tegr
ated
hea
lth s
ervi
ce d
eliv
ery
syst
em id
entifi
ed fr
om t
he 1
8 st
udie
s in
clud
ed in
the
sco
pin
g re
view
Incl
uded
ar
ticl
esC
oun
try
or
geo
gra
phy
Pri
mar
y fo
cus
on
the
pan
dem
ic c
ont
inuu
mH
ealt
h sy
stem
s b
uild
ing
blo
cks
invo
lved
in t
he in
teg
rati
on
Str
uctu
re o
f in
teg
rati
on
Inte
gra
tio
n m
echa
nism
Inte
rpan
dem
ic
pha
seA
lert
p
hase
Pan
dem
ic
pha
seTr
ansi
tio
n p
hase
Ser
vice
del
iver
yH
ealt
hw
ork
forc
eM
edic
ine
&te
chno
log
y
Hea
lth
info
rmat
ion
syst
emH
ealt
hfi
nanc
ing
Go
vern
ance
Vert
ical
Ho
rizo
ntal
Bo
thS
yste
mat
icN
orm
ativ
e
Al N
sour
et
al40
Eas
tern
M
edite
rran
ean
Reg
ion*
Ban
erji41
Ind
ia
Che
llam
uthu
an
d M
uthu
45In
dia
Gar
g et
al46
Ind
ia
Gup
ta e
t al
42In
dia
Gup
ta e
t al
43In
dia
Ha
et a
l37V
ietn
am
Iyen
gar
et a
l47In
dia
Kap
lan
et a
l38B
oliv
ia
Lal e
t al
50In
dia
Luce
ro- P
risno
et
al39
Afr
ican
re
gion
†
Meg
hana
et
al51
Ind
ia
Meg
hwal
et
al52
Ind
ia
Piry
ani e
t al
44N
epal
Ras
togi
et
al48
Ind
ia
Ras
togi
et
al49
Ind
ia
Shi
nde
et a
l53In
dia
Zgu
eb e
t al
36Tu
nisi
a
18 s
tud
ies
wer
e in
clud
ed in
the
sco
pin
g re
view
, whi
ch m
et t
he in
clus
ion
crite
ria.
*Egy
pt,
Iraq
, Jor
dan
, Mor
occo
, Sau
di A
rab
ia, S
udan
, Tun
isia
.†A
lger
ia, C
amer
oon,
Cot
e d
’Ivoi
re, G
amb
ia, M
adag
asca
r, N
iger
ia, R
wan
da,
Sen
egal
, Sou
th S
udan
, Uga
nda.
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 7
BMJ Global Health
structure (revenue generation, pooling or purchasing strategies) while responding to the COVID-19.
Almost 55% (n=10) of the studies implemented IHSD via a horizontal structure of integration.36 45–53 This variant of integration structure incorporates health services and health systems components within a single level of the health system or with a healthcare facility. The second most common integration structure—reported in seven studies38–44—was a mix of horizontal and vertical integration, where a multipronged approach was taken to execute a system- wide response against COVID-19. The only example of vertical integration was identified in Ha et al,37 highlighting specific measures adopted across the primary and secondary care systems. Finally, most of the studies (n=14) systematically imple-mented the IHSD models with guidelines and protocols specifically developed for the COVID-19 pandemic. Only four studies reported more of a normative mechanism of IHSD implementation,46 48 49 51 where no COVID-19 specific guideline was implemented; instead, the existing health systems structures and guidelines were adopted in response to the pandemic. Interestingly, all four of these studies were associated with implementing the IHSD system at the pandemic phase (table 2).
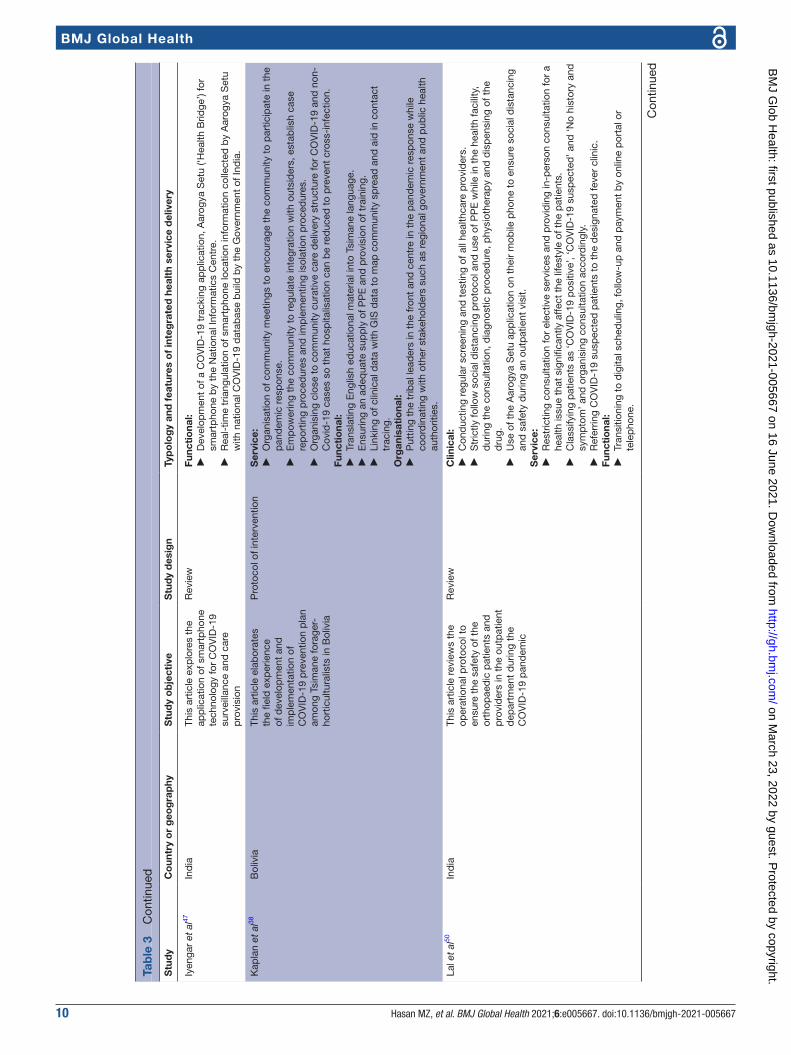
Regardless of the structure or mechanism of IHSD described in the studies, 72% (n=13) studies reported implementing multiple typologies of integration simultaneously. Among the 18 studies included in the scoping review, 7 studies described the IHSD system, which contains all four integration typologies (clin-ical, service, functional and organisational),36 37 39 41–44 5 studies reported implementing three typologies of integration,38 40 45 50 52 1 reported a combination of two typologies51 and 5 studies reported only one typology of integration.46–49 53 Considering the individual typology of health system integration, the functional variant was most frequently applied—either independently46 or in combi-nation with other typologies.36–47 50–52 This was followed by service integration in 14 studies,36–45 49–52 clinical inte-gration in 11 studies36 37 39 41–45 48 50 53 and finally organ-isational integration was observed in 10 studies.36–44 52 Table 3 presents the objective, designs and typologies of the 18 included articles with a detailed description of their IHSD design.
When implemented at the alert phase, organisational integration emerged as a cardinal feature of the IHSD system.36–44 While we have observed collaboration between local, state and federal institutions for screening, isolation and case management,36–38 41–44 51 cross- country collabo-ration and partnership with international development organisations were also evident as organisational inte-gration.39 40 52 Among the included studies in this review, the most common examples of functional integration—coordination between clinical and non- clinical func-tions—involved knowledge management and training of healthcare providers,36 38–41 43 45 46 51 52 maintain the inven-tory and supply chain of personal protective equipment, clinical equipment and medication,37 38 41 42 44 46 infection
control of the healthcare facilities43 46 52 and mobilising community- based contact- tracing of recently discharged patients.52 We have also observed a unique archetype of functional integration where Global Positioning System and smartphones were used for contact tracing and case surveillance of COVID-19,38 47 52 and digital health tech-nologies were used for teleconsultation and follow- up of routine cases to ensure social distancing measures.49 50
Beyond the conventional features of service integra-tion—coordination of prevention and treatment for COVID-19 within and/or across facilities or through a team of multidisciplinary provider team37–45 48 50 52—some of the unique examples of service integration involved incorporating allied healthcare providers such as AYUSH (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy—the six types of traditional or comple-mentary medicine systems practiced in India) and phar-macy professionals (PPs) in COVID-19 response49 51 and organising psychological counselling helpline.36 Finally, as part of clinical integration, 11 studies advocated devel-oping and implementing COVID-19 specific guidelines to ensure the coherence of rules and policies at various health systems levels.36 37 39 41–45 48 50 53
Shifting the perspective from the operational features of IHSD to country- level results has provided further insights into how integration approaches were adopted in various regions. Several countries from the African region (Algeria, Cameroon, Cote d’Ivoire, Gambia, Madagascar, Nigeria, Rwanda, Senegal, Sudan, South Sudan, Tunisia, Uganda) demonstrated a robust IHSD system.36 39 40 These integrations involved all the compo-nents of the health systems building blocks (except healthcare financing), including service delivery through community engagements for behavioural change, surveillance and monitoring programmes, leveraging technology to support information dissemination and ensuring governance through active involvement of the respective health departments. We also observed an ecosystem of partnership among different entities, such as communities and health facility teams, interdepart-mental working groups, the Africa Task Force for Novel Coronavirus and the WHO.
In the context of India, the majority of IHSD cases were during the pandemic phase, except two that were observed for the alert phase.41 43 Most studies refer to integration mechanisms that correspond to only two or three building blocks of the health systems. Only two studies reported activities related to COVID-19 response, encompassing all the building blocks (except healthcare financing).42 52 Notably, we have found that the health workforce was integrated through the formation of RRTs of specialists from public health, epidemiology, respi-ratory medicine, paediatrics, general medicine, micro-biology and otorhinolaryngology.52 Besides, the health systems governance structure was integrated through the coordination between the Indian Council of Medical Research and the WHO to ensure effective delivery of services,42 43 and health information infrastructure
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

8 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Tab
le 3
S
umm
ary
inte
grat
ed h
ealth
ser
vice
del
iver
y sy
stem
of t
he 1
8 st
udie
s in
clud
ed in
the
sco
pin
g re
view
(ord
ered
alp
hab
etic
ally
acc
ord
ing
to t
he n
ame
of t
he fi
rst
auth
or)
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Al N
sour
et
al40
Eas
tern
Med
iterr
anea
n re
gion
(E
MR
) (E
gyp
t, Ir
aq, J
ord
an,
Mor
occo
, Sau
di A
rab
ia, S
udan
, Tu
nisi
a)
This
art
icle
ela
bor
ates
on
the
resp
onse
of t
he G
lob
al
Hea
lth D
evel
opm
ent
and
E
aste
rn M
edite
rran
ean
Pub
lic H
ealth
Net
wor
k,
and
the
Fie
ld E
pid
emio
logy
Tr
aini
ng P
rogr
amm
es
(FE
TPs)
dur
ing
the
CO
VID
-19
pan
dem
ic
Com
men
tary
or
edito
rial
Ser
vice
:
►S
cree
ning
and
sur
veill
ance
act
iviti
es c
ond
ucte
d b
y FE
TPs
at t
he p
oint
of e
ntrie
s in
the
E
MR
cou
ntrie
s.Fu
ncti
ona
l:
►C
olla
tion,
syn
thes
is a
nd d
isse
min
atio
n of
info
rmat
ion
by
the
Pub
lic H
ealth
Em
erge
ncy
Man
agem
ent
Cen
tre
in r
esp
onse
to
the
pan
dem
ic.
►
Con
duc
ting
orie
ntat
ion
sess
ion
with
phy
sici
ans
and
pub
lic h
ealth
pra
ctiti
oner
s to
b
uild
a s
hare
d u
nder
stan
din
g of
the
pro
toco
ls, c
ase
defi
nitio
ns a
nd p
ublic
mes
sagi
ng
stra
tegi
es.
Org
anis
atio
nal:
►
Col
lab
orat
ing
with
FE
TPs
by
pro
vid
ing
tech
nica
l sup
por
ts a
nd e
duc
atio
nal m
ater
ials
.
Ban
erj41
Ind
iaTh
is a
rtic
le s
umm
aris
es
the
Ind
ian
Arm
ed F
orce
s M
edic
al S
ervi
ces
(AFM
S)
resp
onse
to
the
CO
VID
-19
pan
dem
ic
Com
men
tary
or
edito
rial
Clin
ical
:
►W
ith t
he g
uid
ance
of t
he M
inis
try
of H
ealth
and
Fam
ily W
elfa
re, A
FMS
dev
elop
ed a
st
and
ard
op
erat
ing
pro
ced
ure
(SO
P) t
o es
tab
lish
qua
rant
ine
faci
litie
s.S
ervi
ce:
►
Arm
ed fo
rce
med
ical
faci
lity
was
des
igna
ted
as
a C
OV
ID-1
9 tr
eatm
ent
hosp
ital w
ith
CO
VID
-19
test
ing
faci
litie
s.
►S
ervi
ce d
eliv
ery
was
sep
arat
ed fo
r p
atie
nts
with
CO
VID
-19
and
non
- CO
VID
-19
for
bot
h in
pat
ient
and
out
pat
ient
faci
litie
s.Fu
ncti
ona
l:
►A
ircra
ft fr
om In
dia
n A
ir Fo
rce
wer
e us
ed t
o es
tab
lish
a su
pp
ly c
hain
of p
erso
nal
pro
tect
ive
equi
pm
ent
(PP
E),
clin
ical
eq
uip
men
t an
d m
edic
atio
n.
►G
ener
al d
uty
sold
iers
wer
e re
crui
ted
as
volu
ntee
rs a
nd u
nder
wen
t tr
aini
ng fo
r C
OV
ID-1
9 p
and
emic
res
pon
se, a
nd p
artic
ipat
ed in
the
imp
lem
enta
tion
of p
reve
ntiv
e m
easu
res.
Org
anis
atio
nal:
►
AFM
S fo
rmal
ised
rap
id r
esp
onse
med
ical
tea
ms
and
coo
rdin
ated
with
loca
l, st
ate
and
fe
der
al g
over
nmen
t in
scr
eeni
ng, i
sola
tion
and
CO
VID
-19
case
man
agem
ent
in t
he
qua
rant
ine
faci
litie
s.
Che
llam
uthu
and
M
uthu
45In
dia
This
art
icle
exp
lore
s th
e m
anag
emen
t of
or
thop
aed
ic c
are
in a
te
rtia
ry c
are
hosp
ital u
sing
a
pan
dem
ic r
esp
onse
p
roto
col d
urin
g th
e C
OV
ID-1
9 p
and
emic
Rev
iew
Clin
ical
:
►M
aint
aini
ng in
pat
ient
vis
itor
reco
rd, p
erfo
rm s
cree
ning
and
rec
ord
the
full
hist
ory
by
stric
tly fo
llow
ing
infe
ctio
n co
ntro
l mea
sure
s.S
ervi
ce:
►
Cre
atin
g a
sep
arat
e gr
oup
of p
hysi
cian
s to
pro
vid
e in
pat
ient
and
out
pat
ient
ser
vice
w
ithou
t en
gagi
ng w
ith e
ach
othe
r.
►R
educ
ing
elec
tive
surg
ical
car
e.
►U
sing
tel
emed
icin
e an
d o
nlin
e to
ols
to p
rovi
de
reha
bili
tativ
e an
d p
osto
per
ativ
e ca
re.
Func
tio
nal:
►
Incl
udin
g p
hysi
cian
s in
the
pan
dem
ic r
esp
onse
tas
k fo
rce,
pro
vid
ing
app
rop
riate
tr
aini
ng t
o th
e p
hysi
cian
s in
pan
dem
ic r
esp
onse
.
Gar
g et
al46
Ind
iaTh
is a
rtic
le h
ighl
ight
s th
e p
rep
ared
ness
of 5
1 p
rimar
y he
alth
care
faci
lity
linke
d t
o m
edic
al c
olle
ges
and
inst
itutio
ns t
o p
rovi
de
safe
out
pat
ient
s se
rvic
es in
In
dia
dur
ing
the
CO
VID
-19
pan
dem
ic
Ob
serv
atio
nal s
tud
yFu
ncti
ona
l:
►C
hem
ical
ly d
isin
fect
ing
the
faci
litie
s (8
0% o
f the
faci
litie
s im
ple
men
ting
the
dis
infe
ctio
n p
roce
dur
es e
ither
dai
ly o
r on
alte
rnat
ive
day
s).
►
Pro
vid
ing
PP
E t
o th
e p
hysi
cian
(PP
E s
uite
s av
aila
ble
=27
.4%
, N95
mas
k av
aila
ble
=50
.9%
and
sur
gica
l mas
k av
aila
ble
=39
.3%
).
►Tr
aini
ng t
o sa
fely
man
age
pat
ient
s w
ith C
OV
ID-1
9 w
ere
pro
vid
ed in
78.
4% o
f the
fa
cilit
ies.
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 9
BMJ Global Health
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Gup
ta e
t al
42In
dia
This
art
icle
det
ails
m
easu
res
take
n b
y th
e G
over
nmen
t of
Ind
ia in
p
rep
arat
ion
and
res
pon
se
to t
he C
OV
ID-1
9 p
and
emic
Rev
iew
Clin
ical
:
►S
tric
tly fo
llow
ing
infe
ctio
n co
ntro
l mea
sure
s.
►S
trea
mlin
ing
scre
enin
g, s
amp
le c
olle
ctio
n, d
iagn
ostic
and
tre
atm
ent
pro
toco
l.S
ervi
ce:
►
Cat
egor
isat
ion
of in
tern
atio
nal t
rave
llers
bas
ed o
n th
eir
CO
VID
-19
exp
osur
e an
d
sym
pto
ms.
►
Imp
lem
entin
g st
rict
qua
rant
ine
pro
ced
ure
for
inte
rnat
iona
l vis
itors
, sus
pec
ted
and
co
nfirm
ed c
ases
.
►R
educ
ing
elec
tive
care
pro
visi
on in
the
hos
pita
ls.
Func
tio
nal:
►
Pro
visi
onin
g in
fect
ion
cont
rol m
odal
ities
in t
he h
ealth
care
faci
litie
s.
►U
sing
onl
ine
(e- l
earn
ing)
pla
tfor
m fo
r tr
aini
ng o
f hea
lthca
re w
orke
rs.
Org
anis
atio
nal:
►
Dev
elop
ing
coor
din
atio
n am
ong
inst
itutio
ns a
nd s
take
hold
ers
(suc
h as
Nat
iona
l C
entr
e fo
r D
isea
se C
ontr
ol, M
inis
try
of H
ealth
and
Fam
ily W
elfa
re, S
tate
Pub
lic H
ealth
D
epar
tmen
ts, V
irus
Res
earc
h an
d D
iagn
ostic
Lab
orat
orie
s (V
RD
Ls),
Ind
ian
Cou
ncil
of
Med
ical
Res
earc
h (IC
MR
) - N
atio
nal I
nstit
ute
of V
irolo
gy).
Gup
ta e
t al
43In
dia
The
artic
le d
escr
ibes
th
e co
ntrib
utio
n of
a
coun
tryw
ide
netw
ork
of
VR
DLs
in In
dia
for
scal
ing
up t
estin
g ca
pac
ity fo
r S
AR
S- C
oV-2
Com
men
tary
or
edito
rial
Clin
ical
:
►Th
e IC
MR
, Nat
iona
l Ins
titut
e of
Viro
logy
(NIV
), an
d D
epar
tmen
t of
Hea
lth R
esea
rch
(DH
R) c
oord
inat
ed w
ith 1
06 V
RD
Ls t
o ha
rmon
ise
the
SO
P o
f sam
ple
col
lect
ion,
sh
ipm
ent
and
rep
ortin
g p
roce
dur
es.
Ser
vice
:
►E
arly
iden
tifica
tion
and
act
ivat
ion
of V
RD
Ls in
the
citi
es w
ith in
tern
atio
nal a
irpor
ts t
o p
erfo
rm r
eal-
time
PC
R a
ssay
s
►A
ssig
ning
sp
ecifi
c V
RD
Ls a
s sa
mp
le c
olle
ctio
n si
te v
s te
stin
g la
bor
ator
ies
to
rest
ruct
ure
the
CO
VID
-19
test
ing
stra
tegy
Func
tio
nal:
►
Ad
equa
te p
rovi
sion
of t
he lo
gist
ics
(reag
ents
, prim
ers
and
con
trol
s) t
o th
e V
RD
Ls fr
om
NIV
by
situ
atio
nal a
naly
sis
of t
he in
vent
ory.
Org
anis
atio
nal:
►
All
pub
lic h
ealth
age
ncie
s, in
clud
ing
the
Inte
grat
ed D
isea
se S
urve
illan
ce P
rogr
amm
e (ID
SP
), es
tab
lishe
d a
n ef
fect
ive
chan
nel o
f com
mun
icat
ion
with
VR
DLs
at
the
stat
e an
d
regi
onal
leve
l.
Ha
et a
l37V
ietn
amTh
is a
rtic
le h
ighl
ight
s sp
ecifi
c m
easu
res
adop
ted
in V
ietn
am fo
r th
e p
reve
ntio
n an
d c
ontr
ol o
f C
OV
ID-1
9
Rev
iew
Clin
ical
:
►Is
suin
g V
ietn
ames
e co
ntex
t- sp
ecifi
c cl
inic
al g
uid
elin
e fo
r C
OV
ID-1
9 m
anag
emen
t.S
ervi
ce:
►
Set
ting
up t
he c
entr
e fo
r m
anag
emen
t of
clin
ical
sup
por
t sp
ecifi
cally
for
pat
ient
s w
ith
CO
VID
-19.
►
Eng
agin
g fr
ontli
ne h
ealth
wor
kers
to
pro
vid
e he
alth
ed
ucat
ion,
con
tact
tra
cing
and
set
- up
loca
l/hom
e is
olat
ion
faci
litie
s.Fu
ncti
ona
l:
►E
nsur
ing
the
pro
visi
on o
f med
ical
and
PP
E in
the
hea
lthca
re fa
cilit
ies.
Org
anis
atio
nal:
►
Est
ablis
hmen
t of
a T
askf
orce
Gro
up o
n C
OV
ID-1
9 p
reve
ntio
n an
d c
ontr
ol b
y in
clud
ing
per
sonn
el fr
om m
inis
trie
s, o
ther
gov
ernm
ent
com
mitt
ees
and
med
ia.
►
Act
ivat
ion
of E
mer
genc
y P
ublic
Hea
lth O
per
atio
ns C
entr
e w
ithin
the
Gen
eral
D
epar
tmen
t of
Pre
vent
ive
Med
icin
e to
coo
rdin
ate
with
pro
vinc
ial C
ente
r fo
r D
isea
ses
Con
trol
(CD
Cs)
.
Tab
le 3
C
ontin
ued
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from
10 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Iyen
gar
et a
l47In
dia
This
art
icle
exp
lore
s th
e ap
plic
atio
n of
sm
artp
hone
te
chno
logy
for
CO
VID
-19
surv
eilla
nce
and
car
e p
rovi
sion
Rev
iew
Func
tio
nal:
►
Dev
elop
men
t of
a C
OV
ID-1
9 tr
acki
ng a
pp
licat
ion,
Aar
ogya
Set
u (‘H
ealth
Brid
ge’)
for
smar
tpho
ne b
y th
e N
atio
nal I
nfor
mat
ics
Cen
tre.
►
Rea
l- tim
e tr
iang
ulat
ion
of s
mar
tpho
ne lo
catio
n in
form
atio
n co
llect
ed b
y A
arog
ya S
etu
with
nat
iona
l CO
VID
-19
dat
abas
e b
uild
by
the
Gov
ernm
ent
of In
dia
.
Kap
lan
et a
l38B
oliv
iaTh
is a
rtic
le e
lab
orat
es
the
field
exp
erie
nce
of d
evel
opm
ent
and
im
ple
men
tatio
n of
C
OV
ID-1
9 p
reve
ntio
n p
lan
amon
g Ts
iman
e fo
rage
r-
hort
icul
tura
lists
in B
oliv
ia
Pro
toco
l of i
nter
vent
ion
Ser
vice
:
►O
rgan
isat
ion
of c
omm
unity
mee
tings
to
enco
urag
e th
e co
mm
unity
to
par
ticip
ate
in t
he
pan
dem
ic r
esp
onse
.
►E
mp
ower
ing
the
com
mun
ity t
o re
gula
te in
tegr
atio
n w
ith o
utsi
der
s, e
stab
lish
case
re
por
ting
pro
ced
ures
and
imp
lem
entin
g is
olat
ion
pro
ced
ures
.
►O
rgan
isin
g cl
ose
to c
omm
unity
cur
ativ
e ca
re d
eliv
ery
stru
ctur
e fo
r C
OV
ID-1
9 an
d n
on-
Cov
id-1
9 ca
ses
so t
hat
hosp
italis
atio
n ca
n b
e re
duc
ed t
o p
reve
nt c
ross
- inf
ectio
n.Fu
ncti
ona
l:
►Tr
ansl
atin
g E
nglis
h ed
ucat
iona
l mat
eria
l int
o Ts
iman
e la
ngua
ge.
►
Ens
urin
g an
ad
equa
te s
upp
ly o
f PP
E a
nd p
rovi
sion
of t
rain
ing.
►
Link
ing
of c
linic
al d
ata
with
GIS
dat
a to
map
com
mun
ity s
pre
ad a
nd a
id in
con
tact
tr
acin
g.O
rgan
isat
iona
l:
►P
uttin
g th
e tr
ibal
lead
ers
in t
he fr
ont
and
cen
tre
in t
he p
and
emic
res
pon
se w
hile
co
ord
inat
ing
with
oth
er s
take
hold
ers
such
as
regi
onal
gov
ernm
ent
and
pub
lic h
ealth
au
thor
ities
.
Lal e
t al
50In
dia
This
art
icle
rev
iew
s th
e op
erat
iona
l pro
toco
l to
ensu
re t
he s
afet
y of
the
or
thop
aed
ic p
atie
nts
and
p
rovi
der
s in
the
out
pat
ient
d
epar
tmen
t d
urin
g th
e C
OV
ID-1
9 p
and
emic
Rev
iew
Clin
ical
:
►C
ond
uctin
g re
gula
r sc
reen
ing
and
tes
ting
of a
ll he
alth
care
pro
vid
ers.
►
Str
ictly
follo
w s
ocia
l dis
tanc
ing
pro
toco
l and
use
of P
PE
whi
le in
the
hea
lth fa
cilit
y,
dur
ing
the
cons
ulta
tion,
dia
gnos
tic p
roce
dur
e, p
hysi
othe
rap
y an
d d
isp
ensi
ng o
f the
d
rug.
►
Use
of t
he A
arog
ya S
etu
app
licat
ion
on t
heir
mob
ile p
hone
to
ensu
re s
ocia
l dis
tanc
ing
and
saf
ety
dur
ing
an o
utp
atie
nt v
isit.
Ser
vice
:
►R
estr
ictin
g co
nsul
tatio
n fo
r el
ectiv
e se
rvic
es a
nd p
rovi
din
g in
- per
son
cons
ulta
tion
for
a he
alth
issu
e th
at s
igni
fican
tly a
ffect
the
life
styl
e of
the
pat
ient
s.
►C
lass
ifyin
g p
atie
nts
as ‘C
OV
ID-1
9 p
ositi
ve’,
‘CO
VID
-19
susp
ecte
d’ a
nd ‘N
o hi
stor
y an
d
sym
pto
m’ a
nd o
rgan
isin
g co
nsul
tatio
n ac
cord
ingl
y.
►R
efer
ring
CO
VID
-19
susp
ecte
d p
atie
nts
to t
he d
esig
nate
d fe
ver
clin
ic.
Func
tio
nal:
►
Tran
sitio
ning
to
dig
ital s
ched
ulin
g, fo
llow
- up
and
pay
men
t b
y on
line
por
tal o
r te
lep
hone
.
Tab
le 3
C
ontin
ued
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 11
BMJ Global Health
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Luce
ro- P
risno
et
al39
Afr
ica
n re
gion
(Alg
eria
, Cam
eroo
n,
Cot
e d
’Ivoi
re, G
amb
ia,
Mad
agas
car,
Nig
eria
, Rw
and
a,
Sen
egal
, Sou
th S
udan
, Uga
nda)
This
art
icle
pro
vid
es
a co
mm
enta
ry o
n th
e p
and
emic
res
pon
se e
ffort
of
the
Afr
ican
con
tinen
t
Com
men
tary
or
edito
rial
Clin
ical
:
►D
evel
opm
ent
of c
ount
ry- s
pec
ific
clin
ical
cas
e m
anag
emen
t p
roto
col.
Ser
vice
:
►C
oord
inat
ion
of a
wid
e ra
nge
of s
ervi
ces
acro
ss A
fric
an c
ount
ries,
whi
ch in
clud
es
the
scre
enin
g of
inco
min
g tr
avel
lers
at
the
poi
nt o
f ent
ry, s
urve
illan
ce, c
omm
unity
en
gage
men
t fo
r C
OV
ID-1
9 p
reve
ntio
n, c
apac
ity b
uild
ing
of t
he h
ealth
care
faci
litie
s fo
r te
stin
g an
d c
ase
man
agem
ent.
►
Bui
ldin
g p
ublic
aw
aren
ess
thro
ugh
an in
tera
ctiv
e C
OV
ID-1
9 d
ashb
oard
.Fu
ncti
ona
l:
►C
ond
uctin
g tr
aini
ng a
nd k
now
led
ge d
isse
min
atio
n se
ssio
ns w
ith t
he R
apid
Res
pon
se
Team
(RR
T).
Org
anis
atio
nal:
►
Est
ablis
hing
the
Afr
ica
Task
For
ce fo
r N
ovel
Cor
onav
irus
by
the
Afr
ica
CD
Cs,
in
colla
bor
atio
n w
ith t
he W
HO
.
►Fo
rmat
ion
of E
mer
genc
y O
per
atio
ns C
entr
es a
nd R
RT
for
cros
s- co
untr
y co
llab
orat
ion.
Meg
hana
et
al51
Ind
iaTh
is a
rtic
le e
xplo
res
the
enga
gem
ent
of 2
4 p
harm
acy
pro
fess
iona
ls
(PP
s) a
cros
s se
ven
stat
es
of In
dia
on
Em
erge
ncy
Pre
par
edne
ss &
Res
pon
se
of C
OV
ID-1
9 p
and
emic
Ob
serv
atio
nal s
tud
yS
ervi
ce:
►
PP
s re
por
ted
tha
t th
ey r
outin
ely
scre
ened
pat
ient
s fo
r fe
ver
and
cou
gh
►P
Ps
ofte
n p
rovi
des
tel
epho
ne c
onsu
ltatio
ns t
o p
atie
nts
and
dis
sem
inat
ed in
form
atio
n re
gard
ing
mas
k us
e an
d h
and
was
hing
Func
tio
nal:
►
Min
istr
y of
Hea
lth a
nd F
amily
Wel
fare
inst
ruct
ed t
he P
harm
acy
Cou
ncil
of In
dia
to
enlis
t p
harm
acis
ts a
nd t
rain
the
m a
s a
par
t of
the
CO
VID
-19
resp
onse
(suc
h as
sup
ply
cha
in,
inve
ntor
y m
anag
emen
t, in
fect
ion
cont
rol a
nd r
atio
nal u
se o
f the
dru
g).
Meg
hwal
et
al52
Ind
iaTh
is a
rtic
le e
lab
orat
es
the
field
exp
erie
nce
of C
OV
ID-1
9 cl
uste
r co
ntai
nmen
t st
rate
gies
in
a h
ealth
care
faci
lity
by
Cen
tral
and
the
Sta
te R
RTs
at
Bhi
lwar
a,R
ajas
than
, Ind
ia
Ob
serv
atio
nal s
tud
yS
ervi
ce:
►
Imp
lem
entin
g a
doo
r- to
- doo
r sc
reen
ing
pro
ced
ure
of in
fluen
za- l
ike
illne
ss in
the
dis
tric
t b
y th
e M
obile
Hea
lth T
eam
s.
►S
ched
ulin
g ro
tatio
nal s
ervi
ce fo
r th
e p
hysi
cian
s.Fu
ncti
ona
l:
►Im
ple
men
tatio
n of
dis
infe
ctio
n p
roce
dur
e in
the
hea
lth fa
cilit
ies
and
dev
elop
men
t of
b
uffe
r zo
nes.
►
Con
tact
tra
cing
and
imp
lem
enta
tion
of is
olat
ion
pro
ced
ure
of t
he d
isch
arge
d p
atie
nts.
►
Usi
ng t
he R
ajas
than
Soc
ial M
edia
Pla
tfor
m a
pp
licat
ion
on s
mar
tpho
ne d
evic
es t
o su
re
the
hom
e q
uara
ntin
e m
easu
res
of t
he s
usp
ecte
d c
ases
.
►Tr
aini
ng o
f all
the
med
ical
, par
amed
ical
, ad
min
istr
ativ
e st
aff f
or im
ple
men
tatio
n of
co
ntai
nmen
t gu
idel
ines
.O
rgan
isat
iona
l:
►Fo
rmat
ion
of a
mul
tidis
cip
linar
y R
RT
whi
ch in
clud
es e
xper
ts fr
om s
ever
al d
epar
tmen
ts
of a
sta
te m
edic
al c
olle
ge, I
DS
P D
istr
ict
Ep
idem
iolo
gist
and
Sur
veill
ance
Med
ical
O
ffice
r of
Nat
iona
l Pol
io S
urve
illan
ce P
rogr
amm
e W
HO
Ind
ia.
Tab
le 3
C
ontin
ued
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

12 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Piry
ani e
t al
44N
epal
This
art
icle
sum
mar
ises
N
epal
’s r
esp
onse
bef
ore
and
aft
er W
HO
dec
lare
d
CO
VID
-19
as a
pan
dem
ic
Com
men
tary
or
edito
rial
Clin
ical
:
►D
evel
opm
ent
of N
epal
’s t
reat
men
t p
roto
col f
or C
OV
ID-1
9 sa
mp
le c
olle
ctio
n,
tran
spor
tatio
n an
d c
ase
man
agem
ent
bas
ed o
n b
y U
N H
ealth
Age
ncy’
s re
com
men
dat
ion.
►
Dra
ftin
g an
d im
ple
men
ting
the
‘Qua
rant
ine
Pro
ced
ure
for
Nep
ali S
tud
ents
rep
atria
ting
from
Chi
na’.
Ser
vice
:
►D
edic
atin
g sp
ecifi
c sp
ace
and
isol
atio
n fa
cilit
ies
to t
reat
CO
VID
-19
as e
arly
as
Janu
ary
2020
.
►Im
ple
men
ting
scre
enin
g p
roce
dur
e at
the
Trib
huva
n In
tern
atio
nal A
irpor
t an
d e
nsur
ing
safe
tra
nsp
ort
of s
usp
ecte
d c
ases
to
des
igna
ted
hos
pita
ls—
del
iver
ing
CO
VID
-19
spec
ific
info
rmat
ion
by
a fr
ee c
all c
entr
e.Fu
ncti
ona
l:
►B
uild
ing
the
CO
VID
-19
dia
gnos
tic c
apac
ity o
f Nat
iona
l Pub
lic H
ealth
Lab
orat
ory
on
27 J
anua
ry 2
020,
follo
win
g up
by
initi
atio
n of
tes
ting
at t
he P
rovi
ncia
l Pub
lic H
ealth
La
bor
ator
ies
from
Ap
ril 2
020.
►
Ens
urin
g ad
equa
te P
PE
for
heal
thca
re fa
cilit
y an
d t
estin
g la
bor
ator
ies.
Org
anis
atio
nal:
►
Form
atio
n of
a h
igh-
leve
l tec
hnic
al t
eam
for
the
pan
dem
ic r
esp
onse
, whi
ch in
clud
es
Dep
artm
ent
of H
ealth
Ser
vice
s, M
inis
try
of H
ealth
and
Pop
ulat
ion,
Min
istr
y of
Soc
ial
Dev
elop
men
t, H
ealth
Em
erge
ncy
Op
erat
ion
Cen
tre
and
Pro
vinc
ial H
ealth
Em
erge
ncy
Op
erat
ion
Cen
tre.
Ras
togi
et
al48
Ind
iaTh
is a
rtic
le a
dvo
cate
s th
e in
tegr
atio
n of
Ayu
rved
ic
ther
apy
with
Allo
pat
hic
med
icin
e to
ens
ure
effe
ctiv
e p
and
emic
m
anag
emen
t
Com
men
tary
or
edito
rial
Clin
ical
:
►A
dvo
catin
g A
yurv
edic
inte
rven
tion
and
hea
lthy
lifes
tyle
as
pro
phy
laxi
s.
►R
ecom
men
din
g sp
ecifi
c A
yurv
edic
tre
atm
ent
for
CO
VID
-19
infe
cted
pat
ient
s co
nsid
erin
g th
eir
bro
ad- s
pec
trum
ant
ivira
ls p
rop
ertie
s.
Ras
togi
et
al49
Ind
iaTh
is a
rtic
le e
xplo
res
the
opp
ortu
nity
of W
hats
Ap
p
faci
litat
ed v
ideo
Ayu
rved
a co
nsul
tatio
n d
urin
g th
e C
OV
ID-1
9 p
and
emic
Com
men
tary
or
edito
rial
Ser
vice
:
►C
ond
uctin
g on
line
cons
ulta
tion
as a
n al
tern
ativ
e to
out
pat
ient
car
e se
rvic
e.Fu
ncti
ona
l:
►A
ssig
nmen
t of
an
onlin
e co
nsul
tatio
n co
ord
inat
ion
team
to
coor
din
ate
the
calls
, rec
ord
ke
epin
g an
d e
xpla
inin
g th
e co
mp
onen
ts o
f ad
vice
.
Shi
nde
et a
l53In
dia
This
art
icle
rev
iew
s th
e tr
iage
gui
del
ine
for
the
surg
ical
pro
ced
ure
for
canc
er u
sing
CO
VID
-19
pan
dem
ic
Rev
iew
Clin
ical
:
►C
linic
al d
ecis
ion
of c
ond
uctin
g su
rger
y or
del
ayin
g th
e p
roce
dur
e sh
ould
be
bas
ed o
n p
rogn
osis
and
pat
ient
’s c
ond
ition
—sc
reen
ing
and
dia
gnos
tic t
est.
►
Sur
gica
l pro
toco
l and
gui
del
ines
nee
d t
o ac
com
mod
ate
add
ition
al in
fect
ion
cont
rol
mea
sure
s, s
uch
as c
ond
uctin
g th
e su
rger
y in
the
op
erat
ive
room
with
neg
ativ
e p
ress
ure,
tak
ing
extr
a p
reca
utio
ns fo
r an
aest
hesi
a- re
late
d p
roce
dur
es, t
hora
cic
and
he
alth
- nec
k su
rger
y.
Tab
le 3
C
ontin
ued
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 13
BMJ Global Health
Stu
dy
Co
untr
y o
r g
eog
rap
hyS
tud
y o
bje
ctiv
eS
tud
y d
esig
nTy
po
log
y an
d f
eatu
res
of
inte
gra
ted
hea
lth
serv
ice
del
iver
y
Zgu
eb e
t al
36Tu
nisi
aTh
is a
rtic
le d
escr
ibes
th
e d
evel
opm
ent
and
im
ple
men
tatio
n of
nov
el
psy
chol
ogic
al c
risis
in
terv
entio
n in
res
pon
se t
o th
e C
OV
ID-1
9 p
and
emic
in
Tun
isia
Pro
toco
l of i
nter
vent
ion
Clin
ical
:
►Im
ple
men
ting
a w
ell-
defi
ned
tria
ge a
lgor
ithm
to
asse
ss a
ny p
sych
olog
ical
cris
is p
rovi
de
a co
rrec
t re
ferr
al t
o he
alth
care
pro
vid
ers.
Ser
vice
:
►P
rovi
din
g p
sych
olog
ical
cou
nsel
ling
via
a ca
ll- ce
ntre
bas
ed h
elp
line.
Func
tio
nal:
►
Trai
ning
of v
olun
teer
stu
den
ts o
n th
e ca
ll ce
ntre
pla
tfor
m a
nd m
etho
d o
f co
mm
unic
atio
n d
urin
g th
e co
unse
lling
pro
cess
.O
rgan
isat
iona
l:
►C
oord
inat
ion
bet
wee
n th
e S
trat
egic
Hea
lth O
per
atio
ns C
entr
e (S
hoc
room
) of t
he
Min
istr
y of
Hea
lth, t
he p
sych
olog
ical
sup
por
t un
it (C
AP
) and
the
nat
iona
l tel
epho
ne
oper
ator
dur
ing
the
dev
elop
men
t of
the
inte
rven
tion
stra
tegy
.
►C
olla
bor
atio
n am
ong
the
Sho
c ro
om, t
he C
AP,
Tun
isia
n M
edic
al S
tud
ent’s
Ass
ocia
tion
(Ass
ocia
- Med
) and
the
Tun
isia
n R
ed C
resc
ent
to b
uild
a p
ool o
f psy
chol
ogic
al
coun
sello
r.
18 s
tud
ies
wer
e in
clud
ed in
the
sco
pin
g re
view
, whi
ch m
et t
he in
clus
ion
crite
ria, A
yurv
eda
is o
ne o
f the
tra
diti
onal
/com
ple
men
tary
med
icin
e sy
stem
s p
ract
iced
in In
dia
.G
IS, G
lob
al P
ositi
onin
g S
yste
m.
Tab
le 3
C
ontin
ued
was integrated with service delivery systems by forming mobile health teams to ensure data monitoring and surveillance activities.52
Another country in the Asian region, Nepal, imple-mented IHSD during the alert phase and demonstrated a normative mechanism of integration.44 In their study, Piryani et al44 found that Nepal’s integrated response to the COVID-19 included all typologies of integration. Their study highlighted integration between service provision and technology to enable surveillance activ-ities and inter- organisational coordination to ensure strong governance and continuity of routine service delivery.44 L- LMICs from the East Mediterranean region (Egypt, Morocco, Sudan and Tunisia) and South America (Bolivia) adopted a systematic approach for integration.38 40 Their response to COVID-19 involved three building blocks of health systems in IHSD imple-mentation, with service delivery and governance as a common component to both. The countries from the East Mediterranean region heavily focused their effort on the alert phase. In this region, several L- LMICs (such as Egypt, Morocco, Sudan and Tunisia) coordinated with upper- middle- income (Iraq and Jordan) and high- income (Saudi Arabia) economies through the Eastern Mediterranean Public Health Network, and the Field Epidemiology Training Programmes. This multi- country coordinated effort supported a unique IHSD system to enable screening and surveillance activities, exchange information among Public Health Emergency Manage-ment Centres (PHEMC), and harmonise protocols, case definitions and public messaging strategies in the East Mediterranean region countries.
opportunities, challenges and recommendations to implement the IHsd system during CoVId-19Based on the review of the selected studies, we have summarised the opportunities and challenges for implementing the IHSD system in the L- LMICs during COVID-19 in table 4. We have also organised some crit-ical recommendations that emerged from the evidence while conducting the review process.
In the alert and pandemic phase, existing robust health system governance structures appear to be the essential component of implementing an IHSD system in responding to the COVID-19 pandemic. Strong stew-ardship of the central government and confidence in the local institutions and governing bodies to take appro-priate measures by understanding the context appears to be the critical factor in several studies.37 38 42 44 52 This type of decentralisation of the decision- making power and information needs to flow from the health systems struc-ture down to the community level to effectively engage everyone in the pandemic preparation and response effort.38 52
Simultaneously, upstreaming of multisectoral collab-oration within the country, and among regional and international development partners can be a vital source of sharing the most updated knowledge and resources
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

14 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
Tab
le 4
S
umm
ary
of o
pp
ortu
nitie
s an
d c
halle
nges
iden
tified
for
imp
lem
enta
tion
of t
he in
tegr
ated
hea
lth s
ervi
ce d
eliv
ery
syst
em a
nd p
rosp
ectiv
e re
com
men
dat
ions
Pha
ses
Inte
gra
ted
hea
lth
serv
ice
del
iver
y im
ple
men
tati
on
dur
ing
CO
VID
-19
Rec
om
men
dat
ions
Op
po
rtun
itie
sC
halle
nges
CO
VID
-19
spec
ific
Ro
utin
e he
alth
sys
tem
sp
ecifi
c
Ale
rtp
hase
►
Cha
nge
in c
omm
unity
beh
avio
ur d
riven
b
y tr
ansp
aren
cy in
info
rmat
ion
and
cle
ar
com
mun
icat
ion
thro
ugh
offic
ial a
nd s
ocia
l m
edia
pla
tfor
ms.
►
Ste
war
dsh
ip o
f the
cen
tral
gov
ernm
ent
and
dec
entr
alis
atio
n of
dec
isio
n- m
akin
g ca
pac
ity t
o th
e lo
cal a
utho
ritie
s.
►E
xist
ing
lab
orat
ory
netw
orks
.
►E
stab
lishe
d t
elec
omm
unic
atio
n in
fras
truc
ture
with
a h
igh
inte
rnet
p
enet
ratio
n ra
te.
►
Cha
lleng
es r
elat
ed t
o in
vent
ory
cont
rol o
f per
sona
l pro
tect
ive
equi
pm
ent
(PP
E) a
nd
med
icat
ions
.
►A
lim
ited
sup
ply
of m
edic
al
equi
pm
ent
such
as
vent
ilato
rs
and
PP
E.
►
.CO
VID
-19
rela
ted
rum
ours
and
fa
ke n
ews.
►
Str
engt
heni
ng o
f co
ord
inat
ion
bet
wee
n va
rious
hea
lthca
re b
odie
s at
bot
h lo
cal,
natio
nal a
nd
glob
al le
vel.
►
Up
dat
ing
the
‘Pan
dem
ic
Pla
yboo
k’ w
ith t
he t
estin
g,
trai
ning
and
qua
rant
inin
g st
rate
gies
for
bet
ter
dis
ease
m
anag
emen
t.
►
Est
ablis
hing
inte
grat
ed p
latf
orm
s su
ch a
s te
stin
g la
bor
ator
ies
and
ele
ctro
nic
med
ical
rec
ord
sy
stem
with
in r
outin
e he
alth
in
fras
truc
ture
, whi
ch c
an im
pro
ve
utili
satio
n d
urin
g p
ublic
hea
lth
emer
genc
ies.
Pan
dem
ic
pha
se
►C
oord
inat
ion
bet
wee
n go
vern
men
t m
inis
trie
s, p
ublic
hea
lth in
stitu
tions
and
na
tiona
l and
inte
rnat
iona
l reg
ulat
ory
agen
cies
.
►In
ters
ecto
ral c
olla
bor
atio
n b
etw
een
gove
rnm
ent,
priv
ate
sect
or, m
edia
and
ar
med
forc
es.
►
Syn
ergi
es b
etw
een
vario
us c
adre
s w
ithin
th
e he
alth
sys
tem
s su
ch a
s co
mm
unity
he
alth
wor
kers
and
prim
ary
care
pro
vid
ers.
►
Larg
e sc
ale
app
licat
ion
of d
igita
l hea
lth
tech
nolo
gies
suc
h as
tel
econ
sulta
tion,
sc
hed
ulin
g, p
aym
ent
por
tal a
nd
smar
tpho
ne a
pp
licat
ion
for
cont
act
trac
ing.
►
A p
auci
ty o
f tra
ined
pub
lic
heal
th p
rofe
ssio
nals
, esp
ecia
lly
in e
pid
emio
logy
and
out
bre
ak
inve
stig
atio
n.
►Fr
agm
ente
d s
ervi
ce d
eliv
ery
stru
ctur
e w
ith p
oorly
man
aged
he
alth
info
rmat
ion
syst
em.
►
Hig
h b
urd
en o
f mal
nutr
ition
, m
alar
ia, H
IV/A
IDS
and
tu
ber
culo
sis
whi
ch a
lread
y ov
erw
helm
the
hea
lth s
yste
ms.
►
Unp
rep
ared
inte
rnat
iona
l tra
vel
infr
astr
uctu
res
such
as
airp
orts
an
d la
nd b
ord
ers.
►
Tech
nolo
gica
l lim
itatio
ns r
elat
ed
to s
mar
tpho
nes
of t
he e
nd- u
ser
such
as
inte
r net
con
nect
ivity
an
d a
vaila
bili
ty o
f the
req
uire
d
app
licat
ion.
►
Priv
acy
and
dat
a ow
ners
hip
is
sues
.
►
Em
pow
erin
g co
mm
uniti
es
by
enga
ging
the
m
in d
isea
se o
utb
reak
p
reve
ntio
n an
d c
onta
inm
ent
stra
tegi
es.
►
Trai
ning
and
eng
agin
g th
e in
form
al s
ervi
ce
pro
vid
ers
such
as
AYU
SH
an
d c
omm
unity
- bas
ed
pha
rmac
y p
rofe
ssio
nals
for
pan
dem
ic p
reve
ntio
n an
d
resp
onse
.
►E
xpan
sion
of d
igita
l hea
lth
tech
nolo
gies
for
cont
act
trac
ing,
inve
ntor
y, a
nd
sup
ply
cha
in m
anag
emen
t fo
r m
edic
atio
n, e
qui
pm
ent
and
vac
cine
s.
►E
thic
al u
se o
f dat
a an
d
pat
ient
info
rmat
ion.
►
Dev
elop
ing
serv
ice
del
iver
y in
fras
truc
ture
usi
ng d
igita
l hea
lth
tech
nolo
gies
for
pre
vent
ion,
tr
eatm
ent
and
follo
w- u
p o
f non
- co
mm
unic
able
dis
ease
s an
d
men
tal h
ealth
.
►E
xpan
din
g in
vent
ory
and
st
reng
then
ing
of t
he s
upp
ly c
hain
to
ena
ble
tim
ely
avai
lab
ility
of
med
icat
ion
and
eq
uip
men
t.
Con
tinue
d
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 15
BMJ Global Health
Pha
ses
Inte
gra
ted
hea
lth
serv
ice
del
iver
y im
ple
men
tati
on
dur
ing
CO
VID
-19
Rec
om
men
dat
ions
Op
po
rtun
itie
sC
halle
nges
CO
VID
-19
spec
ific
Ro
utin
e he
alth
sys
tem
sp
ecifi
c
Inte
r- p
and
emic
►
Wel
l est
ablis
hed
net
wor
k of
prim
ary
heal
th
cent
res
that
ens
ured
pro
per
pat
ient
- ce
ntre
d c
are.
►
Wea
k p
ublic
hea
lth in
fras
truc
ture
th
at c
an le
arn
and
ad
apt
usin
g p
revi
ous
exp
erie
nce.
►
Pot
entia
l del
ays
in d
eliv
erin
g ca
re t
o ot
her
esse
ntia
l ser
vice
s (s
uch
as m
ater
nal a
nd c
hild
he
alth
, non
- com
mun
icab
le
dis
ease
s an
d e
lect
ive
surg
ical
p
roce
dur
es) d
ue t
o th
e d
isp
ersi
on
of h
uman
res
ourc
e an
d p
hysi
cal
infr
astr
uctu
re.
►
Dev
elop
ing
rob
ust
dis
ease
su
rvei
llanc
e an
d r
epor
ting
mec
hani
sm.
►
Bui
ldin
g tr
ust
of t
he
pop
ulat
ion
in t
he h
ealth
sy
stem
.
►D
evel
opin
g a
heal
th
wor
kfor
ce w
ith a
n ap
pro
pria
te s
kill-
mix
tha
t in
clud
es s
pec
ialis
t, c
linic
al
and
par
a- cl
inic
al w
orke
rs,
fron
tline
hea
lth w
orke
rs
and
tra
ined
info
rmal
ser
vice
p
rovi
der
s.
►
Bui
ldin
g re
silie
nce
of t
he r
outin
e he
alth
sys
tem
s b
y in
crea
sing
in
vest
men
t in
prim
ary
heal
thca
re
and
inte
grat
ed c
are
syst
em
infr
astr
uctu
re.
They
are
the
six
typ
es o
f tra
diti
onal
/com
ple
men
tary
med
icin
e sy
stem
s p
ract
iced
in In
dia
; Ayu
rved
a is
one
of t
he t
rad
ition
al/c
omp
lem
enta
ry m
edic
ine
syst
ems
pra
ctic
ed in
Ind
ia.
AYU
SH
, Ayu
rved
a, Y
oga
and
Nat
urop
athy
, Una
ni, S
idd
ha, H
omeo
pat
hy.
Tab
le 4
C
ontin
ued
related to COVID-19.39–41 43 On the other hand, poorly resourced health system with weak service delivery struc-ture,39 46 52 53 fragmented supply chain,37–39 43 46 51 low diag-nostic capacity39 43 44 and insufficient health workforce46 51 create bottlenecks to implement a well- coordinated IHSD system in L- LMICs. The key recommendation that emerged from the evidence while conducting the review process is discussed in the next section.
dIsCussIonThis review aimed to explore the published evidence of the IHSD system implemented during the COVID-19 pandemic to further our understanding of the struc-tures, mechanisms and features of integrated care models in L- LMICs. We have identified 18 articles that met our inclusion and exclusion criteria and explained the reported integrated service delivery structure as part of pandemic preparedness, response and recovery.
Most of the articles focused on the pandemic phase, with some providing perspectives on the pandemic continuum’s alert phase. None of the included arti-cles used the term ‘Integrated Health Service Delivery’ explicitly in their papers, although the authors identi-fied aspects of integration and categorised the structure, mechanism and typologies of integration. This could indi-cate that the definition and nomenclature of integration adopted to synthesise the evidence in the scoping review apply to L- LMIC health systems, but the specific termi-nologies are not widely used in the articles. Three- fourth of the studies implemented IHSD systems that crosscut multiple typologies of the integrated model. While implementing the IHSD model, all articles reported inte-grating more than one health system building block for service provision, and none of them reported integrating health financing strategy as part of their IHSD approach. Health financing, as compared with other health systems building blocks, was also the least- integrated building block in a 2019 review on integrated care systems.34 This points to a possible evidence gap warranting further exploration.
The majority of the study systemically implemented the IHSD systems, with almost all the studies (17/18) included some type of horizontal integration, while less than half (8/18) provided examples of vertical integra-tion. This raises some critical questions, such as—are horizontal approaches easier, or are they better suited to any healthcare emergencies, or are they more in line with pre- existing efforts at integration? While all these are important queries, the scope of this review was not designed to answer these questions, nor the articles included in this review elaborated on the result of the adopted IHSD systems in detail.
Fragmentation of health systems remains a global challenge. During the COVID-19 pandemic, the lack of integration within service delivery mechanisms became a critical factor when countries of all income levels are trying to meet the dual goal of pandemic management
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

16 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
and routine service delivery.54 In L- LMICs specifically, historically verticalised and disease- oriented approaches have created additional fragmentation, which may have posed further challenges for COVID-19 pandemic preparedness and response.30 54 55 We have found evidence of a range of opportunities in the L- LMICs towards intro-ducing IHSD innovations in response to the COVID-19 pandemic. The importance of existing primary health-care and public health infrastructure was emphasised in several studies,37 43 and existing networks/infrastructure was identified as an enabler to integration. For example, the existing countrywide network of Virus Research and Diagnostic Laboratories in India was pivotal for scaling up testing capacity for SARS- CoV-2 by coordinating with other public health agencies at the state and national level.43 Similarly, in Vietnam, activation of the existing Emergency Public health Operation Centres ensured an effective integration with the Centers for Disease Control and Prevention and Department of Preventive medicine in health workers and medical supplies management.37 Conversely, poor existing infrastructure, weak supply chains and human resource gaps were highlighted as barriers to integration. Whether this indicates an actual pattern of pandemic response in different countries or is merely a representation of differential access to or deci-sion to publish emerging experiences could be an area for further inquiry.
strengths and limitationsThis review has synthesised a rapidly changing evidence based on IHSD in L- LMICs during phases during the COVID-19 pandemic. To our knowledge, this is the first review to precisely apply the definition of IHSD for COVID-19 response in the settings of L- LMICs. Much of the existing evidence on IHSD during health emergen-cies is conceptual in nature. This includes recommen-dations to strengthen national health systems vis a vis the International Health Regulations,56 57 emphasising an integrated approach to resilient health systems,58 and improving overall systems coordination.14 Specific evidence on IHSDs from previous health emergen-cies also remains sparse, possibly due to the ambiguity of conceptualising IHSD in the past. After many of the world’s most recent pandemics (eg, West Africa Ebola, MERS, SARS and H1N1), there was a rapid expansion of IHSD evidence occurred around 2015. However, there was a lack of conceptual clarity and a common definition of health service integration,59–61 making it particularly challenging to identify integration evidence from past pandemics, even though integration approaches could have been used. Our review contributes to this body of knowledge by synthesising the evidence of IHSD during COVID-19, which will be immensely valuable for any future pandemic response.
We also recognise that the challenges of health systems fragmentation are not specific to L- LMIC health systems17; however, the unique nature of IHSD reforms in L- LMICs compared with upper- middle- income and high- income
settings require detailed exploration as to whether or not these approaches are being applied during COVID-19. Given the potential promise of IHSD in strengthening health systems’ resilience during health emergencies,62 63 an early view into IHSD approaches—or lack thereof—in L- LMICs was warranted. With a systematic approach for identifying evidence, selecting the study and analysing data, we have successfully answered our postulated research questions.
Among the eligible articles, 12 out of 18 were from India, representing an increasing focus on IHSD in the Indian health system. This may result from a higher prev-alence of COVID-19 in India and a greater concentra-tion of research institutions rapidly publishing insights from the Indian response. Besides, we have specified the inclusion criteria only for publications in English, which may have resulted in less evidence from non- Anglophone L- LMIC countries. However, due to the limited capacity of our research team, expanding the inclusion criteria to other languages (such as French and Portuguese) was not possible. The relatively sparse literature may also not represent the actual presence of IHSD approaches being used in the routine health service delivery system in L- LMICs. A significant portion of health system expe-riences and innovations are never documented in the peer- reviewed literature.64 Thus, additional research and analysis of grey literature can help to contribute additional evidence on the IHSD system in pandemic response.
Finally, the pandemic’s trajectory and a predetermined focus on L- LMICs may have limited the total number of articles identified during the early phase of the COVID-19 pandemic, as we have explored the published evidence between 1 December 2019 and 12 June 2020. We acknowledge that with the evolution of COVID-19 over the last year, new studies and evidence on the later part of the pandemic are becoming available. Thus, we are encouraging future reviews to synthesise the evidence of IHSD on the later phases of the pandemic, taking this study as a source of baseline evidence.
Policy recommendationsAlthough the review did not highlight any specific patterns or characteristics of IHSD appearing in the COVID-19 literature from L- LMICs, it did indicate a range of opera-tional approaches deployed in the early days of pandemic preparedness and response. As part of synthesising the evidence on IHSD systems, we have also identified some emerging recommendations for L- LMICs, which are crit-ical to sustain the integrity and further build the health system’s resilience (table 4).
Specific to COVID-19 or any future pandemic, it is necessary to strengthen intersectoral coordination via organisational integration—including the private sector, laboratories and non- biomedical systems such as Ayurveda (one of the traditional medicine systems prac-ticed in India)—while integrating the levels and building blocks of the health system. Other than supporting
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 17
BMJ Global Health
broader governance structure for screening, isolation and curative care provision at the health systems- level, organisational integration seems to have also played an essential role in overcoming health workforce gaps, mobilising rapid response teams, enriching technical inputs, establishing necessary infrastructures such as isolation units, quarantine centres, strengthening collab-oration between surveillance units and viral research labs. Organisational integration possibly is a vital strategy to augment pandemic response in the context of L- LMICs that otherwise face health systems deficits and need addi-tional resources from allied sectors.
Our result suggested that while implementing the IHSD system, some healthcare facilities reduced the provision of elective procedures.43 45 However, a similar strategy cannot be implemented for some routine service delivery systems such as obstetrics care,65 immunisation of children66 and cardiovascular emergencies.67 Thus, the integrated care delivery application during pandemic also needs to ensure the undisrupted provision of these critical routine care services. Alternative service delivery mechanisms such as community- based care, task- shifting using community pharmacists and volunteers for contact tracing and counselling functions, and use digital health technologies for prevention, treatment and follow- up of non- communicable diseases and mental health can spur innovations as a part of the IHSD models in L- LMICs. Finally, governments in L- LMICs need to ensure the ethical use of data and patient information,68 develop a transparent communication strategy to convey scien-tific evidence and empower the communities to be active agents for COVID-19 prevention, surveillance and containment strategies.69
The policy recommendations drawn in this review emerged from the analysis of the selected 18 studies representing a smaller number of L- LMICs. While we acknowledge the limited generalisability of the recom-mendations, they certainly are forward- looking strate-gies that are potential value additions to the limited pool of evidence for implementation of IHSD during COVID-19. It is essential that we refer to them as solid starting points to advocate the IHSD system and build the necessary evidence base to inform policies that can be further modified based on the country’s context, demo-graphics and healthcare needs. Moreover, although the findings and policy recommendations were identified from COVID-19 experiences, we argue that they are not limited to the pandemic response. Barriers and facil-itators to integration represent challenges for health systems strengthening more broadly,70 while policy recommendations to strengthen coordination, empow-ering communities, building trust and developing the right skills- mix for the health workforce can be equally applied to non- pandemic times.58 The recommenda-tions from this study are all reflective of adaptive and resilience approaches, mirroring broader recommenda-tions for health systems strengthening and resilience in the literature.71
ConClusIonThe COVID-19 pandemic was a significant shock to the health systems of L- LMICs,5 72 and an integrated model of health service delivery can assist the care provision of COVID-19 related illness and support the currently overwhelmed routine health service delivery struc-ture.25 26 73 Using a robust—yet flexible—methodology of a scoping review, this study was able to systematically organise and report the use of an integrated care system during COVID-19, which to date was not available. We believe the evidence of IHSD presented in this review has emerged organically in response to the COVID-19 emer-gency that is often not documented in the literature. The results demonstrated the crux of the issue with the poten-tial of organisational innovation capability of the health systems in the L- LMICs despite the fragmented structure and dearth of resources. However, the lack of published evidence on IHSD from L- LMICs indicates a significant gap in the original research. We hope the result of our synthesis will encourage more primary research on the integrated care system. Furthermore, we recommend future reviews to revisit the emerging evidence base on IHSD at the later phases of the COVID-19 response and recovery in L- LMICs and beyond to explore how the nascent approaches highlighted here evolve over time.
Author affiliations1School of Population and Public Health, The University of British Columbia, Vancouver, British Columbia, Canada2Department of International Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA3Department of Health and Family Welfare, Government of Gujarat, Gandhinagar, India4Department of Population, Family and Reproductive Health, Johns Hopkins University Bloomberg School of Public Health, Baltimore, Maryland, USA5Deutsche Gesellschaft für Internationale Zusammenarbeit GmbH India Office, New Delhi, India
Twitter Md Zabir Hasan @zabirhasan and Priyanka Das @priyanka0805
Acknowledgements The authors thank the Welch Medical Library of Johns Hopkins University, specifically Informationist Donna Hesson, to assist in this review and develop the search terms.
Contributors MZH, RN and PD developed the first draft of this review. MZH, SG, DA, DB and NJ conceptualised the review. MZH developed the search strategy, conducted the search and compiled the studies. RN, PD and VV performed the study selection by completing the title, abstract and full- text screening. RN, PD and VV completed the data extraction with the supervision of SG and MZH. All authors contributed to manuscript revision and read and approved the article for publication.
Funding This work was supported by the Indo- German Social Security Programme, GIZ India Grant Number #81251835.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study. No additional data are available. This study is developed from publicly available secondary data. The scoping review is registered on OSF. io with the Registration DOI 10.17605/OSF.IO/KY9PX ( osf. io/ yk7gu).
supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer- reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

18 Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667
BMJ Global Health
responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
open access This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https:// creativecommons. org/ licenses/ by/ 4. 0/.
orCId idMd Zabir Hasan http:// orcid. org/ 0000- 0001- 8730- 0054
REFERENCES 1 Johns Hopkins University. Coronavirus COVID-19 global cases.
Johns Hopkins coronavirus resource center, 2020. Available: https:// coronavirus. jhu. edu/ map. html
2 Fitzgerald DA, Wong GWK. COVID-19: a tale of two pandemics across the Asia Pacific region. Paediatr Respir Rev 2020;35:75–80.
3 Anjorin AA, Abioye AI, Asowata OE, et al. Comorbidities and the COVID-19 pandemic dynamics in Africa. Trop Med Int Health 2021;26:2–13.
4 Kaur S, Sonali S. India fights COVID-19. Psychol Trauma 2020;12:579–81.
5 Hopman J, Allegranzi B, Mehtar S. Managing COVID-19 in low- and middle- income countries. JAMA 2020;323:1549–50.
6 Bong C- L, Brasher C, Chikumba E, et al. The COVID-19 pandemic: effects on low- and middle- income countries. Anesth Analg 2020;131:86–92.
7 Thayer WM, Hasan MZ, Sankhla P, et al. An interrupted time series analysis of the lockdown policies in India: a national- level analysis of COVID-19 incidence. Health Policy Plan 2021. doi:10.1093/heapol/czab027. [Epub ahead of print: 26 Apr 2021].
8 Spicer N, Agyepong I, Ottersen T, et al. 'It's far too complicated': why fragmentation persists in global health. Global Health 2020;16:60.
9 World Health Organization Secretariat. Framework on integrated, people- centred health services, 2016. Available: https:// apps. who. int/ gb/ ebwha/ pdf_ files/ WHA69/ A69_ 39- en. pdf? ua=1
10 World Health Organization, Regional Office for Europe. Integrated care models: an overview. Copenhagen, Denmark: WHO Regional Office for Europe, 2016. http://www. euro. who. int/__ data/ assets/ pdf_ file/ 0005/ 322475/ Integrated- care- models- overview. pdf
11 Lewis RQ, Rosen R, Goodwin N. Where next for integrated care organisations in the English NHS? London: The Nuffield Trust, 2010. https://www. nuffieldtrust. org. uk/ files/ 2017- 01/ where- next- integrated- care- english- nhs- web- final. pdf
12 Hasan MZ, Singh S, Arora D, et al. Evidence of integrated primary- secondary health care in low- and middle- income countries: protocol for a scoping review. Syst Rev 2020;9:260.
13 Staňková P, Dvorský J, Dvorský J. The reducing hospital costs through horizontal integration. Iran J Public Health 2019;48:2016–24.
14 World Health Organization. Pandemic influenza risk management: a who guide to inform and harmonize national and international pandemic preparedness and response. Geneva: World Health Organization, 2017. https:// apps. who. int/ iris/ bitstream/ handle/ 10665/ 259893/ WHO- WHE- IHM- GIP- 2017. 1- eng. pdf; jsessionid= FF0E 44DE 342C CEF9 F0A3 1E1E FB14C8E8? sequence=1
15 Ehrlich H, McKenney M, Elkbuli A. Protecting our healthcare workers during the COVID-19 pandemic. Am J Emerg Med 2020;38:1527–8.
16 Farrell TW, Francis L, Brown T, et al. Rationing limited healthcare resources in the COVID-19 era and beyond: ethical considerations regarding older adults. J Am Geriatr Soc 2020;68:1143–9.
17 Mounier- Jack S, Mayhew SH, Mays N. Integrated care: learning between high- income, and low- and middle- income country health systems. Health Policy Plan 2017;32:iv6–12.
18 Lê G, Morgan R, Bestall J, et al. Can service integration work for universal health coverage? Evidence from around the globe. Health Policy 2016;120:406–19.
19 Dudley L, Garner P. Strategies for integrating primary health services in low- and middle- income countries at the point of delivery. Cochrane Database Syst Rev 2011:CD003318.
20 Topp SM, Abimbola S, Joshi R, et al. How to assess and prepare health systems in low- and middle- income countries for
integration of services- a systematic review. Health Policy Plan 2018;33:298–312.
21 Atun R, de Jongh T, Secci F, et al. Integration of targeted health interventions into health systems: a conceptual framework for analysis. Health Policy Plan 2010;25:104–11.
22 Amon JJ. Preventing HIV infections in children and adolescents in sub- Saharan Africa through integrated care and support activities: a review of the literature. Afr J AIDS Res 2002;1:143–9.
23 Lurie N, Dausey DJ, Knighton T, et al. Community planning for pandemic influenza: lessons from the Va health care system. Disaster Med Public Health Prep 2008;2:251–7.
24 Gray R, Sanders C. A reflection on the impact of COVID-19 on primary care in the United Kingdom. J Interprof Care 2020;34:672–8.
25 Capalbo C, Aceti A, Simmaco M, et al. The exponential phase of the Covid-19 pandemic in central Italy: an integrated care pathway. Int J Environ Res Public Health 2020;17. doi:10.3390/ijerph17113792. [Epub ahead of print: 27 May 2020].
26 Lindner S, Kubitschke L, Lionis C, et al. Can integrated care help in meeting the challenges posed on our health care systems by COVID-19? some preliminary lessons learned from the European vigour project. Int J Integr Care 2020;20:4.
27 Neill R, Hasan MZ, Das P, et al. Evidence of integrated health service delivery during COVID-19 in low and lower- middle- income countries: protocol for a scoping review. BMJ Open 2021;11:e042872.
28 The Global Health Security Index. GHS index, 2019. Available: https://www. ghsindex. org/
29 The University of Oxford. COVID-19 government response tracker, 2020. Available: https://www. bsg. ox. ac. uk/ research/ research- projects/ covid- 19- government- response- tracker
30 Pham QD, Stuart RM, Nguyen TV. Lessons learned from Vietnam’s COVID-19 response: the role of adaptive behavior change and testing in epidemic control. medRxiv 2020.
31 Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol 2005;8:19–32.
32 Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA- ScR): checklist and explanation. Ann Intern Med 2018;169:467–73.
33 Peters MDJ, Godfrey C, McInerney P. Chapter 11: scoping reviews. In: Aromataris E, Munn Z, eds. Joanna briggs institute reviewer’s manual. Adelaide, Australia: JBI, 2020. https:// reviewersmanual. joannabriggs. org/
34 Salam RA, Das JK, Bhutta ZA. Integrating nutrition into health systems: what the evidence advocates. Matern Child Nutr 2019;15 Suppl 1:e12738.
35 Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta- analyses: the PRISMA statement. PLoS Med 2009;6:e1000097.
36 Zgueb Y, Bourgou S, Neffeti A, et al. Psychological crisis intervention response to the COVID 19 pandemic: a Tunisian centralised protocol. Psychiatry Res 2020;289:113042.
37 Ha BTT, Ngoc Quang L, Mirzoev T, et al. Combating the COVID-19 epidemic: experiences from Vietnam. Int J Environ Res Public Health 2020;17:3125.
38 Kaplan HS, Trumble BC, Stieglitz J, et al. Voluntary collective isolation as a best response to COVID-19 for Indigenous populations? A case study and protocol from the Bolivian Amazon. The Lancet 2020;395:1727–34.
39 Lucero- Prisno DE, Adebisi YA, Lin X. Current efforts and challenges facing responses to 2019- nCoV in Africa. Glob Health Res Policy 2020;5:1–3.
40 Al Nsour M, Bashier H, Al Serouri A, et al. The role of the global health development/eastern Mediterranean public health network and the eastern Mediterranean field epidemiology training programs in preparedness for COVID-19. JMIR Public Health Surveill 2020;6:e18503.
41 Banerji A. The armed forces medical services response to COVID-19. Indian J Public Health 2020;64:S94–5.
42 Gupta P, Goyal K, Kanta P, et al. Novel 2019- coronavirus on new year's Eve. Indian J Med Microbiol 2019;37:459–77.
43 Gupta N, Potdar V, Praharaj I, et al. Laboratory preparedness for SARS- CoV-2 testing in India: Harnessing a network of virus research & diagnostic laboratories. Indian J Med Res 2020;151:216–25.
44 Piryani RM, Piryani S, Shah JN. Nepal's response to contain COVID-19 infection. J Nepal Health Res Counc 2020;18:128–34.
45 Chellamuthu G, Muthu S. Pandemic response protocol of a non- frontline specialty in a Multispecialty tertiary health care centre- a pilot model in orthopaedics. Int Orthop 2020;44:1481–7.
46 Garg S, Basu S, Rustagi R, et al. Primary health care facility preparedness for outpatient service provision during the COVID-19 pandemic in India: cross- sectional study. JMIR Public Health Surveill 2020;6:e19927.
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from

Hasan MZ, et al. BMJ Global Health 2021;6:e005667. doi:10.1136/bmjgh-2021-005667 19
BMJ Global Health
47 Iyengar K, Upadhyaya GK, Vaishya R, et al. COVID-19 and applications of smartphone technology in the current pandemic. Diabetes Metab Syndr 2020;14:733–7.
48 Rastogi S, Pandey DN, Singh RH. COVID-19 pandemic: a pragmatic plan for ayurveda intervention. J Ayurveda Integr Med 2020. doi:10.1016/j.jaim.2020.04.002. [Epub ahead of print: 23 04 2020].
49 Rastogi S, Singh N, Pandey P. Telemedicine for ayurveda consultation: devising collateral methods during the COVID-19 lockdown impasse. J Ayurveda Integr Med 2020;395.
50 Lal H, Sharma DK, Patralekh MK, et al. Out patient department practices in orthopaedics amidst COVID-19: the evolving model. J Clin Orthop Trauma 2020;11:700–12.
51 Meghana A, Aparna Y, Chandra SM, et al. Emergency preparedness and response (EP&R) by pharmacy professionals in India: Lessons from the COVID-19 pandemic and the way forward. Res Social Adm Pharm 2021;17:2018-2022.
52 Meghwal B, Behera S, Dhariwal AC, et al. Insights from COVID-19 cluster containment in Bhilwara district, Rajasthan. Indian J Public Health 2020;64:S177–82.
53 Shinde RS, Naik MD, Shinde SR, et al. To do or not to do?—a review of cancer surgery triage guidelines in COVID-19 pandemic. Indian J Surg Oncol 2020;11:175–81.
54 Lal A, Erondu NA, Heymann DL, et al. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet 2021;397:61–7.
55 Cook P. Expanding social health protection to reach universal health coverage - health policy watch. health policy watch, 2020. Available: https:// healthpolicy- watch. news/ expanding- social- health- protection- to- reach- universal- health- coverage/
56 Kluge H, Martín- Moreno JM, Emiroglu N, et al. Strengthening global health security by embedding the International health regulations requirements into National health systems. BMJ Glob Health 2018;3:e000656.
57 Gostin LO, Mundaca- Shah CC, Kelley PW. Neglected dimensions of global security: the global health risk framework Commission. JAMA 2016;315:1451–2.
58 Blanchet K, Nam SL, Ramalingam B, et al. Governance and capacity to manage resilience of health systems: towards a new conceptual framework. Int J Health Policy Manag 2017;6:431–5.
59 Suter E, Oelke ND, da Silva Lima MAD, et al. Indicators and measurement tools for health systems integration: a knowledge synthesis. Int J Integr Care 2017;17:4.
60 Strandberg- Larsen M, Krasnik A. Measurement of integrated healthcare delivery: a systematic review of methods and future research directions. Int J Integr Care 2009;9:e01.
61 Bautista MAC, Nurjono M, Lim YW, et al. Instruments measuring integrated care: a systematic review of measurement properties. Milbank Q 2016;94:862–917.
62 Kruk ME, Myers M, Varpilah ST, et al. What is a resilient health system? Lessons from Ebola. The Lancet 2015;385:1910–2.
63 Nuzzo JB, Meyer D, Snyder M, et al. What makes health systems resilient against infectious disease outbreaks and natural hazards? results from a scoping review. BMC Public Health 2019;19:1310.
64 Usuzaki T, Chiba S, Shimoyama M, et al. A disparity in the number of studies related to COVID-19 and SARS- CoV-2 between low- and middle- income countries and high- income countries. Int Health 2020. doi:10.1093/inthealth/ihaa088. [Epub ahead of print: 31 Oct 2020].
65 Alfieri N, Manodoro S, Marconi AM. COVID-19 does not stop obstetrics: what we need to change to go on safely birthing. The experience of a university obstetrics and gynecology department in Milan. J Perinat Med 2020;48:997–1000.
66 Abbas K, Procter SR, van Zandvoort K, et al. Routine childhood immunisation during the COVID-19 pandemic in Africa: a benefit- risk analysis of health benefits versus excess risk of SARS- CoV-2 infection. Lancet Glob Health 2020;8:e1264–72.
67 Wosik J, Clowse MEB, Overton R, et al. Impact of the COVID-19 pandemic on patterns of outpatient cardiovascular care. Am Heart J 2021;231:1–5.
68 Kaplan B. Revisiting health information technology ethical, legal, and social issues and evaluation: TELEHEALTH/TELEMEDICINE and COVID-19. Int J Med Inform 2020;143:104239.
69 Gilmore B, Ndejjo R, Tchetchia A, et al. Community engagement for COVID-19 prevention and control: a rapid evidence synthesis. BMJ Glob Health 2020;5.
70 Kutzin J, Sparkes SP. Health systems strengthening, universal health coverage, health security and resilience. Bull World Health Organ 2016;94:2.
71 Balabanova D, Mills A, Conteh L, et al. Good health at low cost 25 years on: lessons for the future of health systems strengthening. Lancet 2013;381:2118–33.
72 Okereke M, Ukor NA, Adebisi YA, et al. Impact of COVID-19 on access to healthcare in low- and middle- income countries: current evidence and future recommendations. Int J Health Plann Manage 2021;36:13–17.
73 Jaywant A, Vanderlind WM, Boas SJ, et al. Behavioral interventions in acute COVID-19 recovery: a new opportunity for integrated care. Gen Hosp Psychiatry 2021;69:113–4.
on March 23, 2022 by guest. P
rotected by copyright.http://gh.bm
j.com/
BM
J Glob H
ealth: first published as 10.1136/bmjgh-2021-005667 on 16 June 2021. D
ownloaded from