integrating imaging of the shoulder in msk practice the
TRANSCRIPT
Integrating Imaging of the
Shoulder in MSK practice
The Role of MRI
Cathy Barrett MCSP MPhty.st MMACP FACP
Sharon Morgans MCSP MMACP
Lecturer UCL, KCL, Coventry UniveristyCentral Health [email protected]
Radiology and Orthopaedic Colleagues Imperial Healthcare NHS Trust.
.
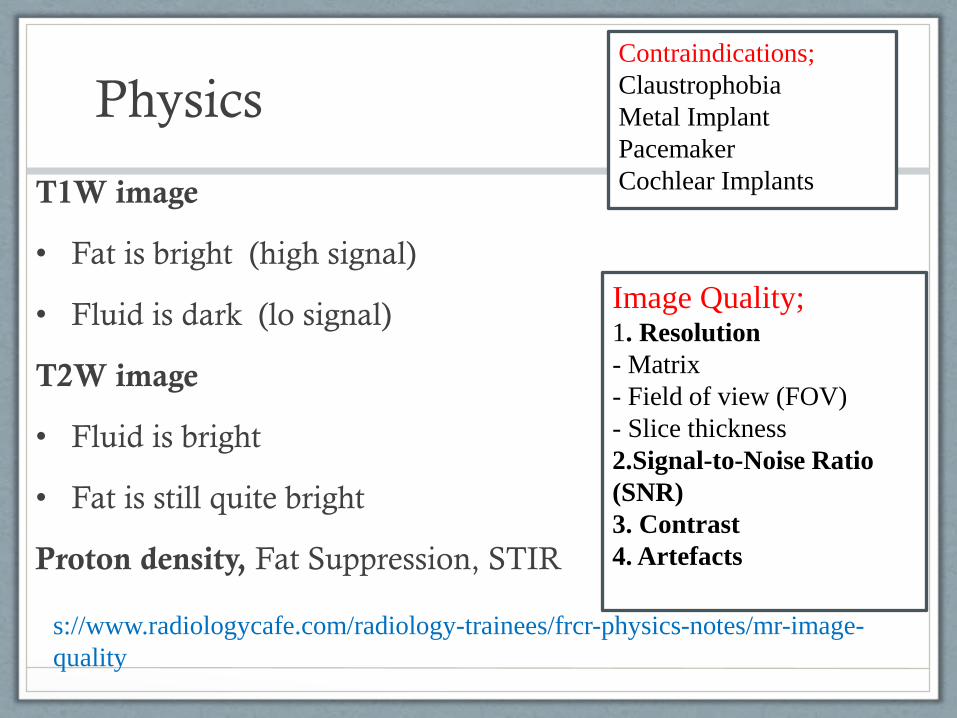
Physics
T1W image
• Fat is bright (high signal)
• Fluid is dark (lo signal)
T2W image
• Fluid is bright
• Fat is still quite bright
Proton density, Fat Suppression, STIR
Contraindications;
Claustrophobia
Metal Implant
Pacemaker
Cochlear Implants
Image Quality;1. Resolution
- Matrix
- Field of view (FOV)
- Slice thickness
2.Signal-to-Noise Ratio
(SNR)
3. Contrast
4. Artefacts
s://www.radiologycafe.com/radiology-trainees/frcr-physics-notes/mr-image-
quality
MRI VIEWS
• Coronal Views (front to back through Coronal plane)
• Saggital Views (side to side through saggital plane)
• Axial Views (Top down through horizontal plane)
• REQUESTING: Clinical information is required on your
request form for Imaging team to set up most appropriate
contrast
• REVIEWING; Need to know which sequences to view for
the anatomical tissue/pathology you are examining.
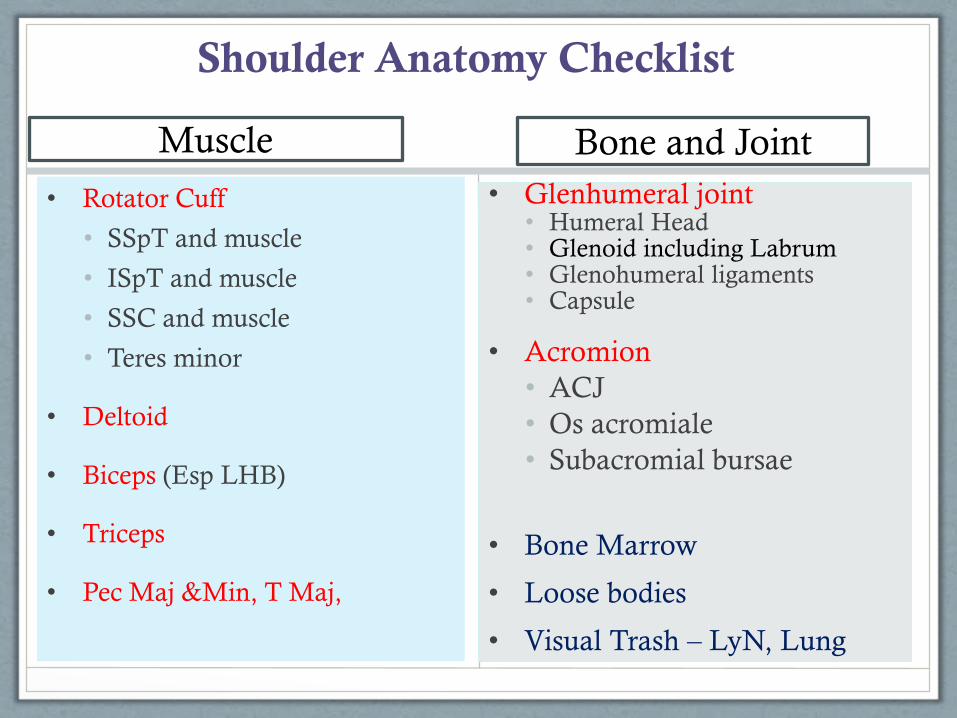
Shoulder Anatomy Checklist
Muscle
• Rotator Cuff
• SSpT and muscle
• ISpT and muscle
• SSC and muscle
• Teres minor
• Deltoid
• Biceps (Esp LHB)
• Triceps
• Pec Maj &Min, T Maj,
Bone and Joint
• Glenhumeral joint• Humeral Head• Glenoid including Labrum• Glenohumeral ligaments• Capsule
• Acromion
• ACJ
• Os acromiale
• Subacromial bursae
• Bone Marrow
• Loose bodies
• Visual Trash – LyN, Lung
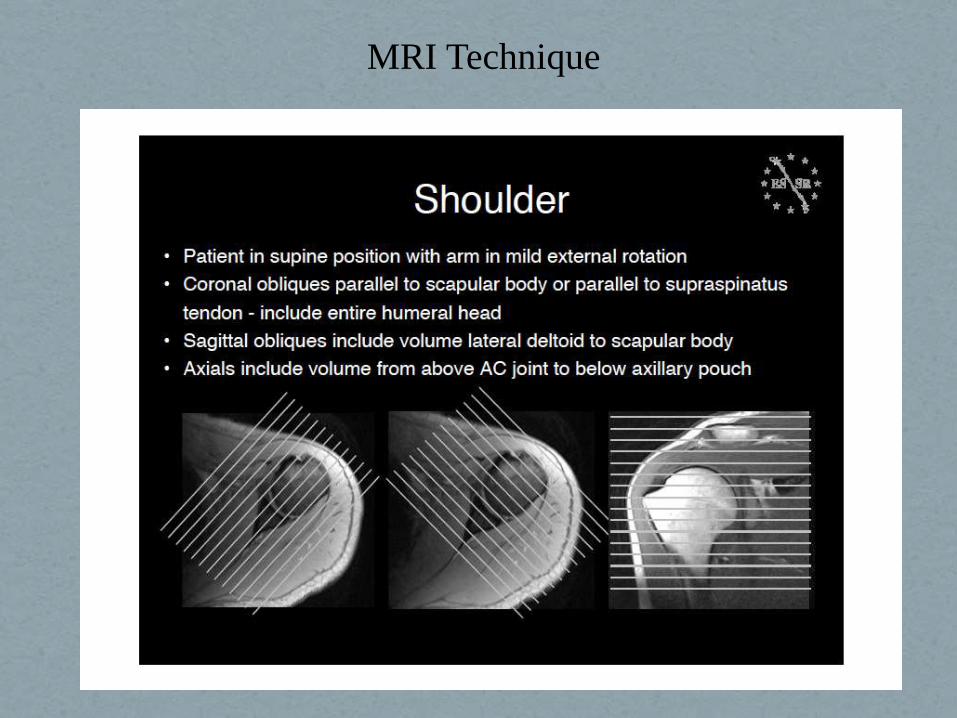
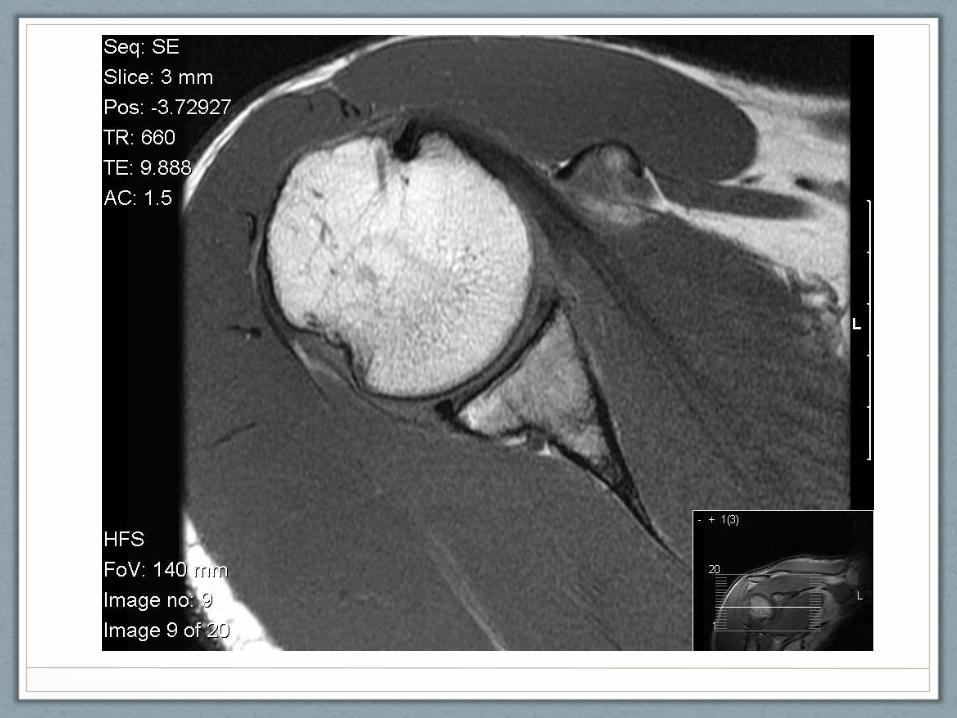
MRI Technique

Normal Shoulder
MRI.coronal view

Sagittal View.
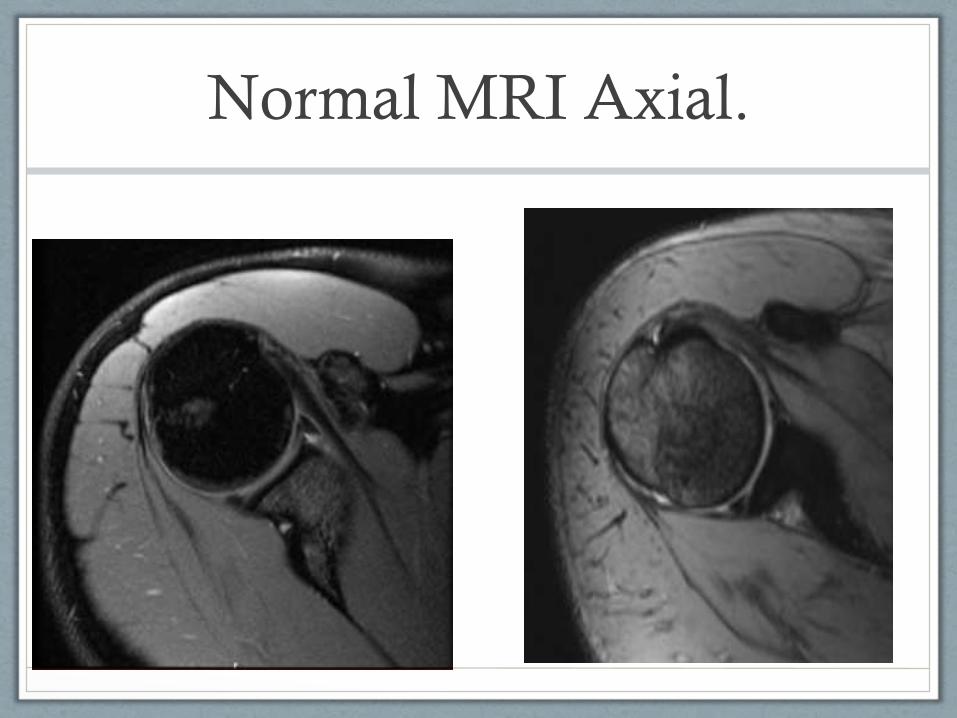
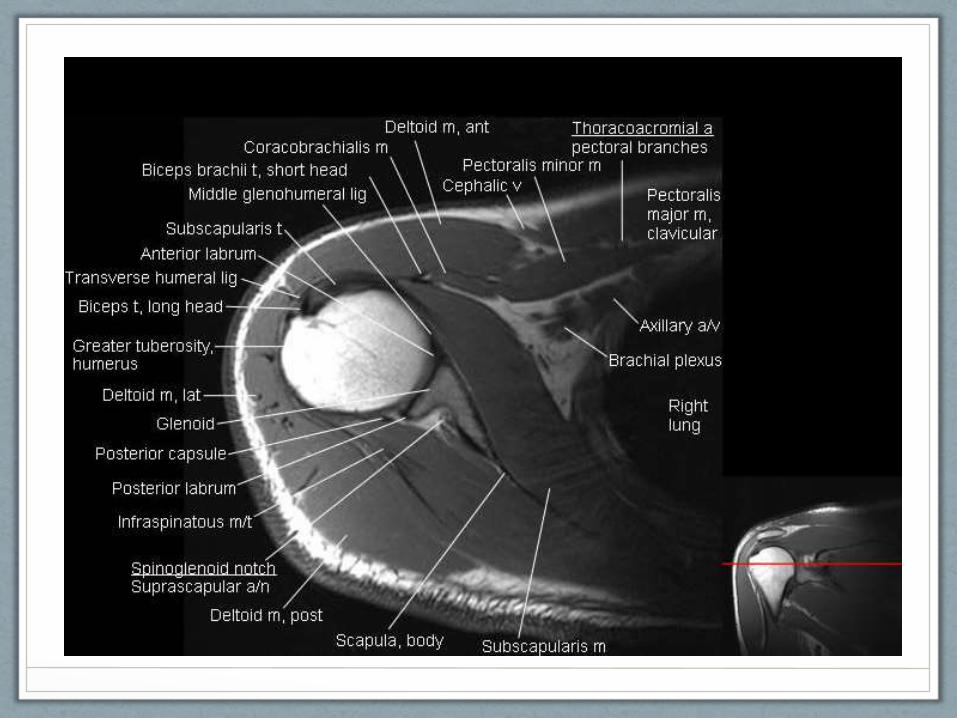
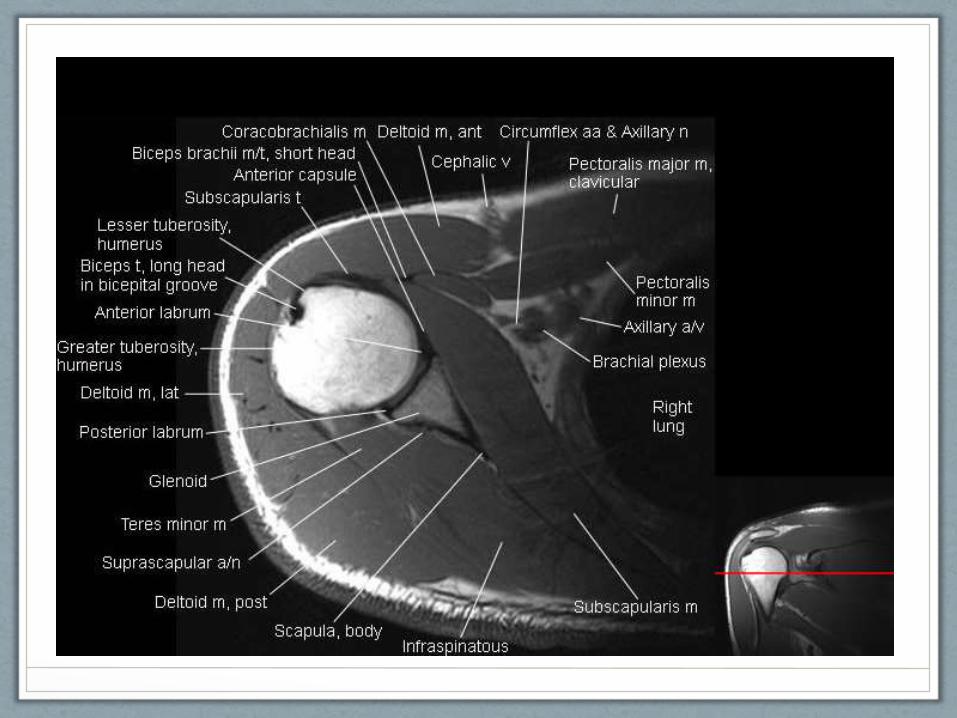
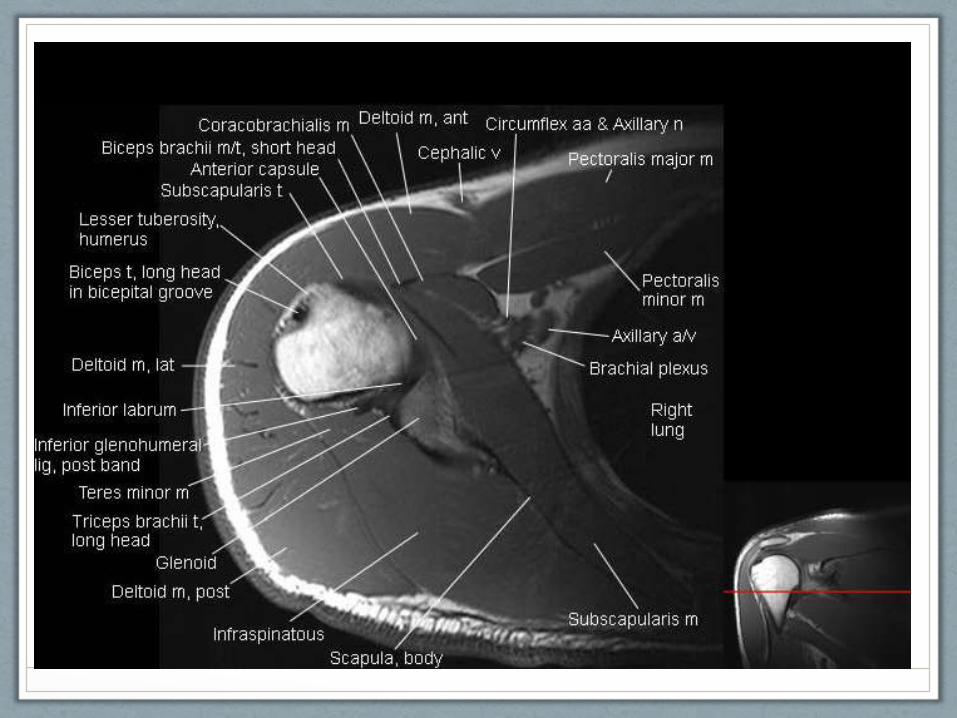
Normal MRI Axial.
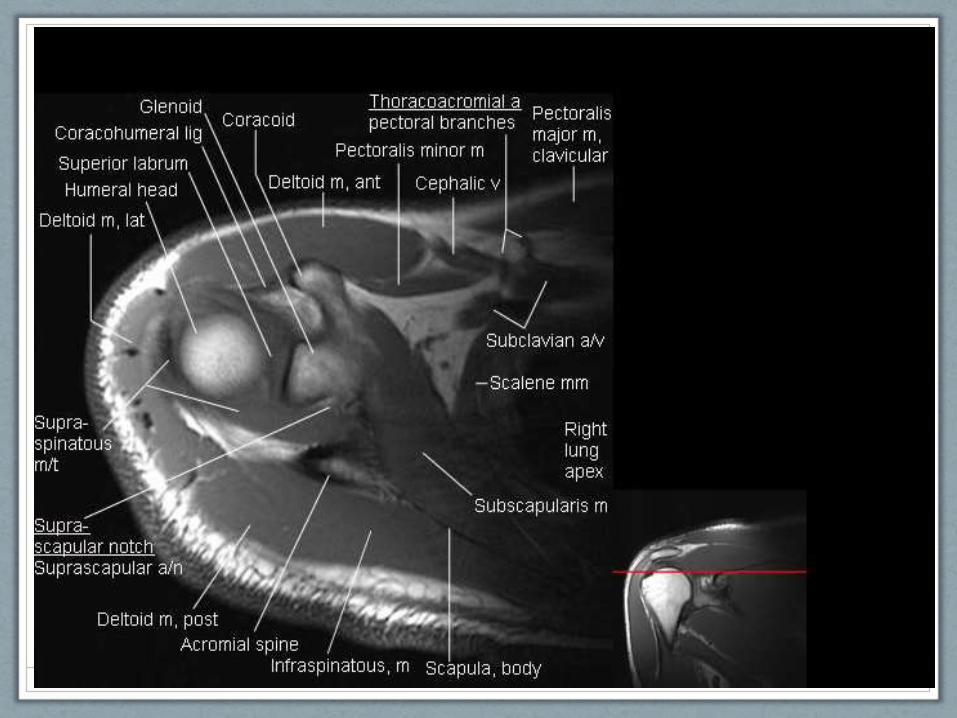
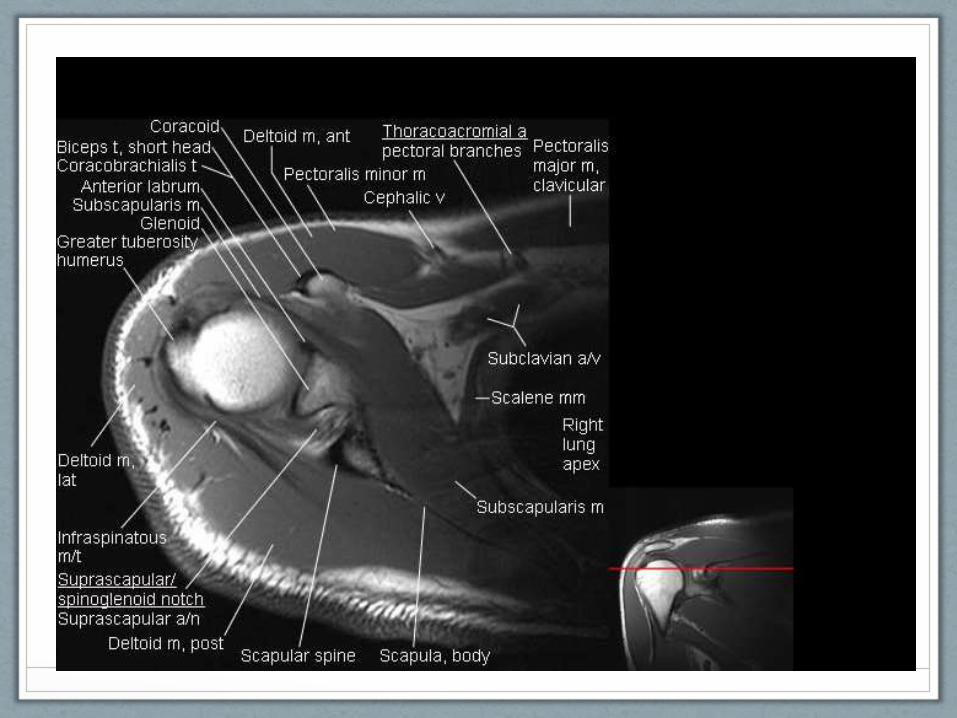
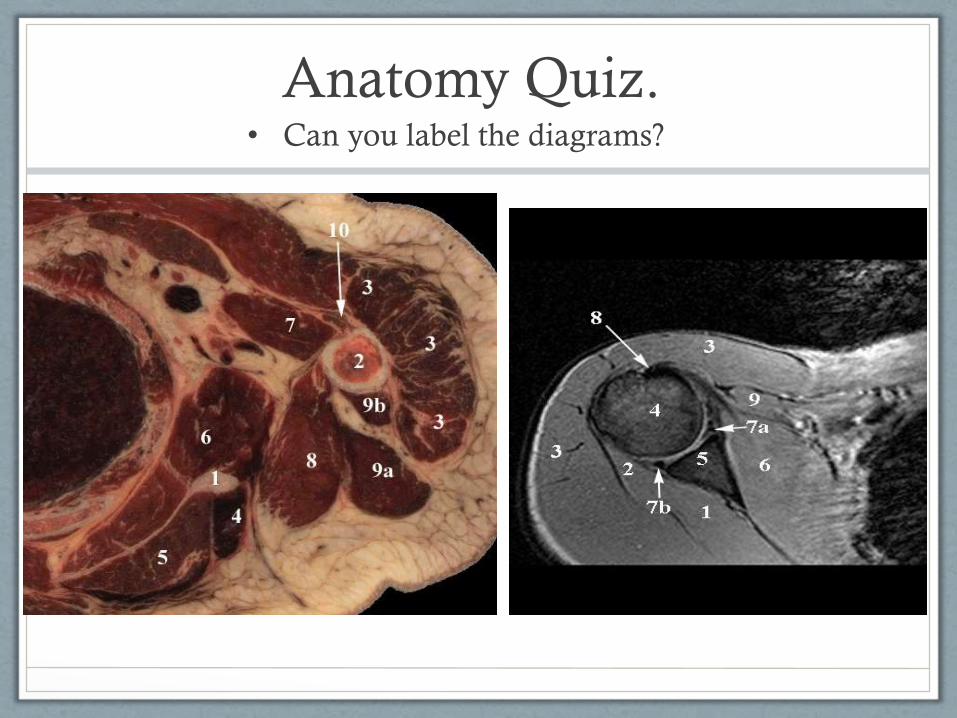
Anatomy Quiz.• Can you label the diagrams?

MRI: The Rotator Cuff
• Normal Cuff
• Abnormal Cuff
• What is relevant to symptoms?
Normal Anatomy
• SST, IST, SSC, Teres Minor
• All cylindrical then flat, fan out and interdigitate at insertion on greater tuberosity of humerus, none have synovial sheath
• SST inserts onto fibrocartilage at top of gter tuberosity
• IST attaches to sup-post gter tuberosity
• Teres minor attaches to inf-post gter tuberosity
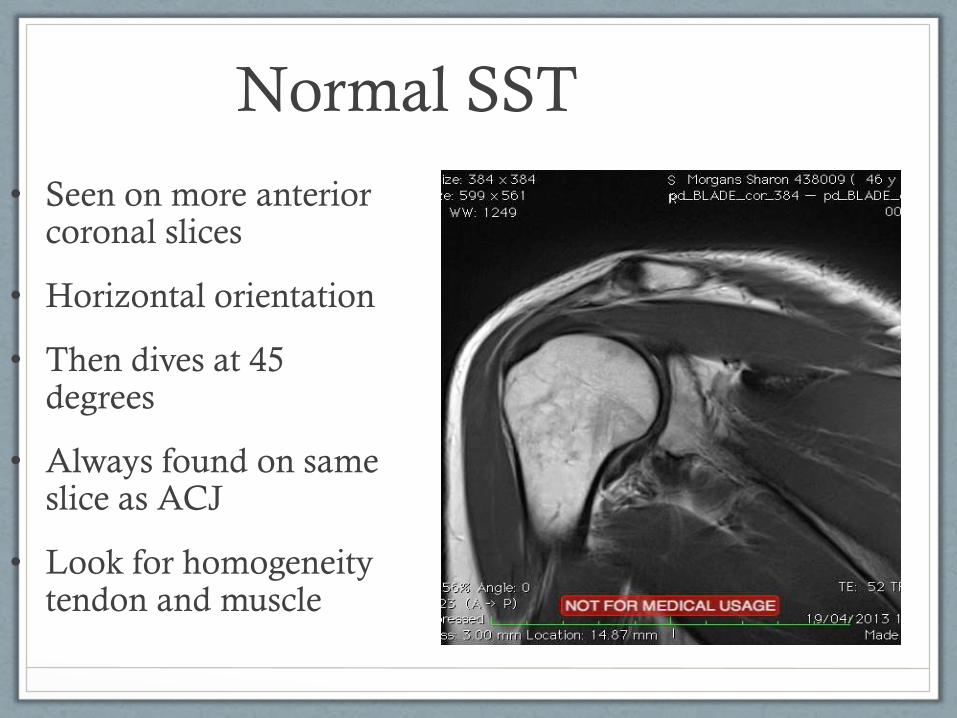
Normal SST
• Seen on more anterior coronal slices
• Horizontal orientation
• Then dives at 45 degrees
• Always found on same slice as ACJ
• Look for homogeneity tendon and muscle
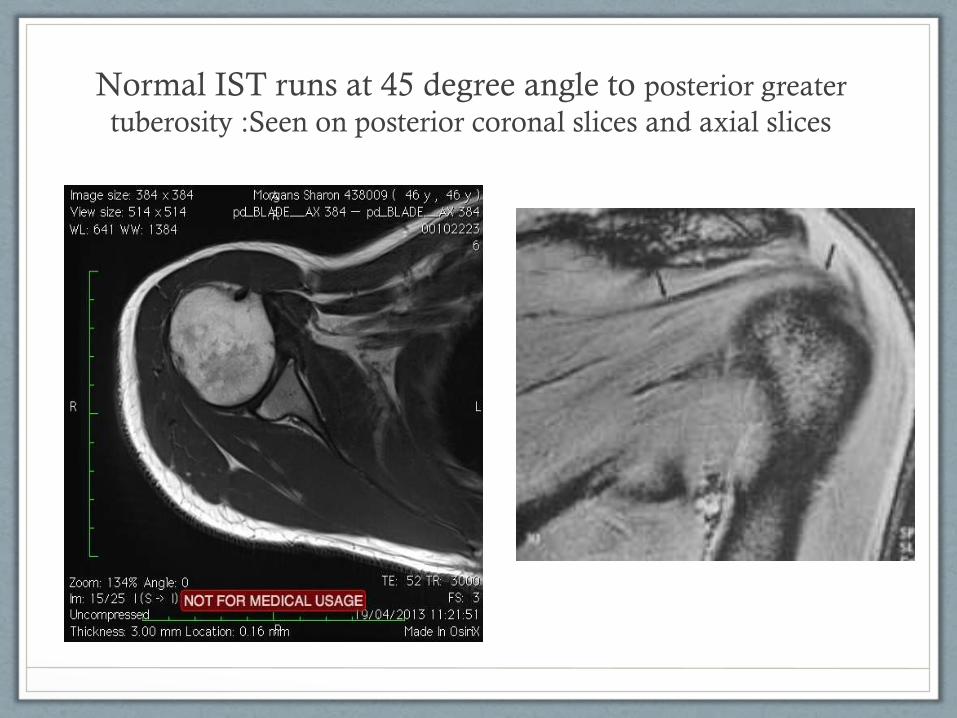
Normal IST runs at 45 degree angle to posterior greater
tuberosity :Seen on posterior coronal slices and axial slices
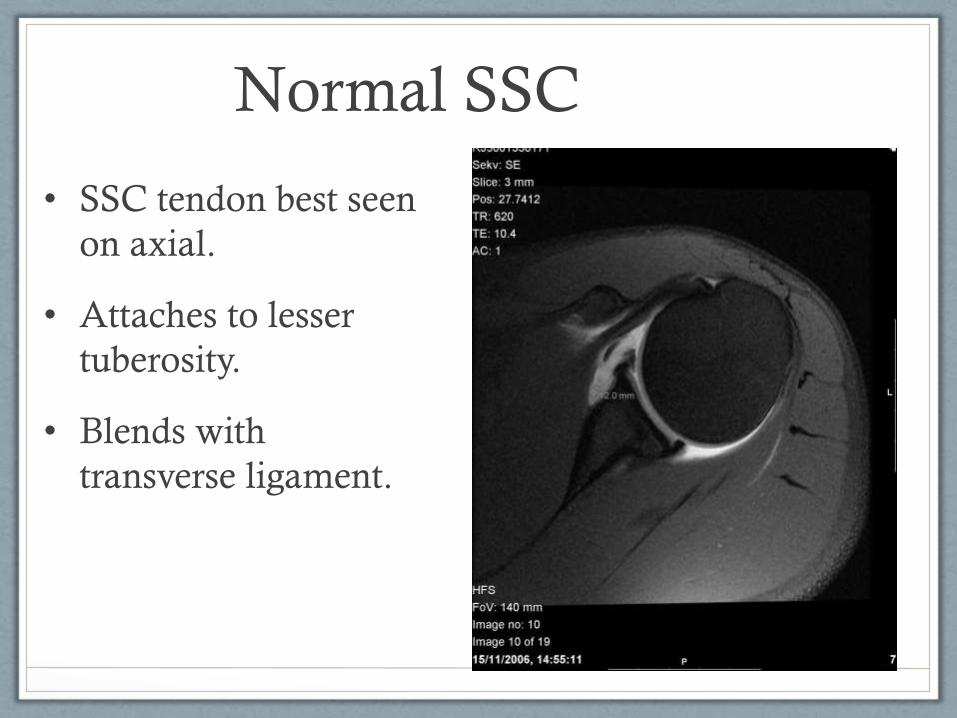
Normal SSC
• SSC tendon best seen
on axial.
• Attaches to lesser
tuberosity.
• Blends with
transverse ligament.
Indicators Rotator Cuff
Pathology
• Bursal fluid
• Heterogeneity vs homogeneity
• Retraction of tendon
• Fatty changes in muscle belly (infiltration)
• Cystic changes at bony insertion
• Bony outlet changes
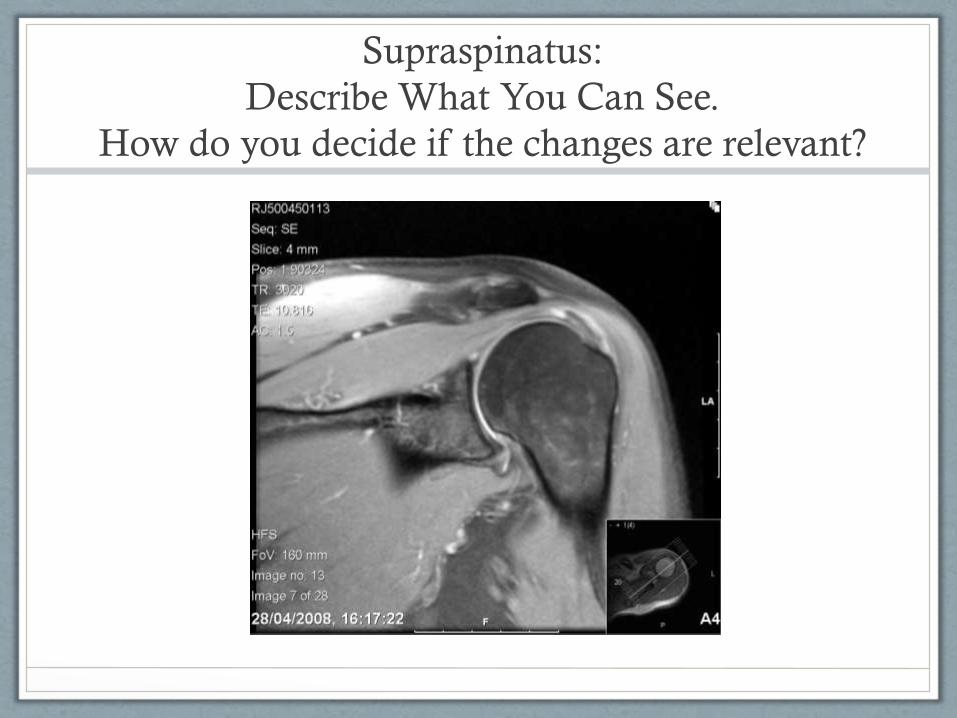
Supraspinatus:
Describe What You Can See.
How do you decide if the changes are relevant?

Same patient. What do you see?
Where are you compared to last slice?
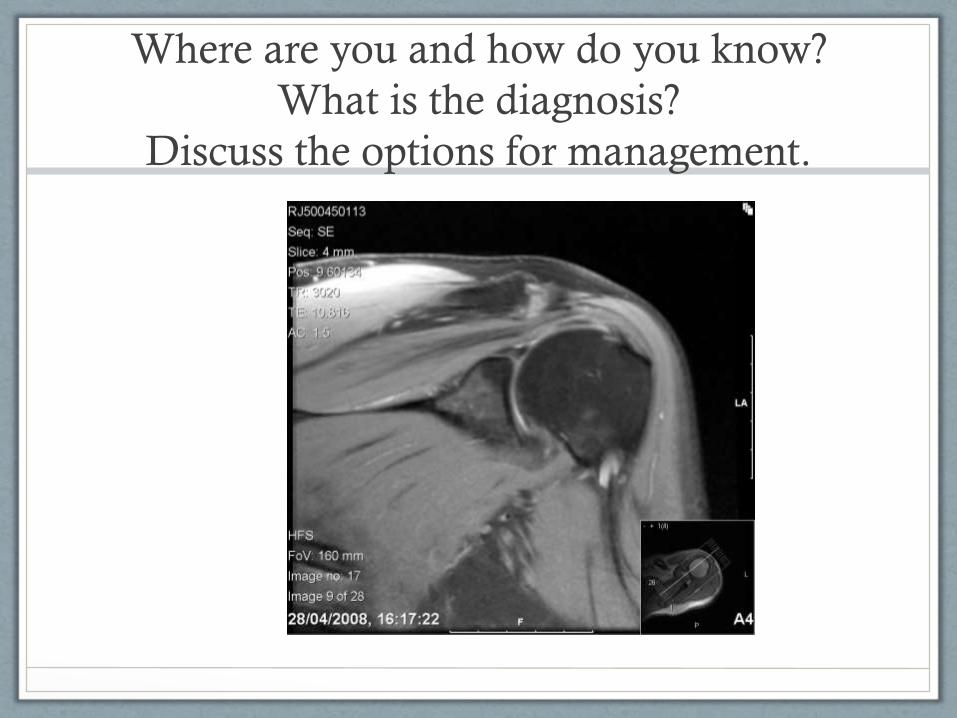
Where are you and how do you know?
What is the diagnosis?
Discuss the options for management.
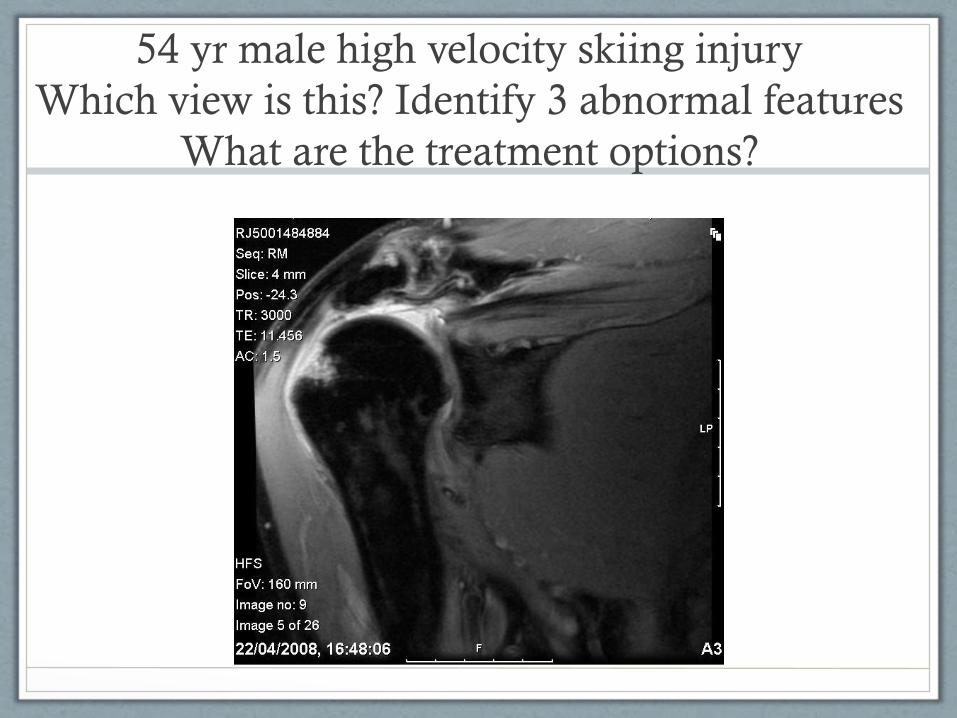
54 yr male high velocity skiing injury
Which view is this? Identify 3 abnormal features
What are the treatment options?
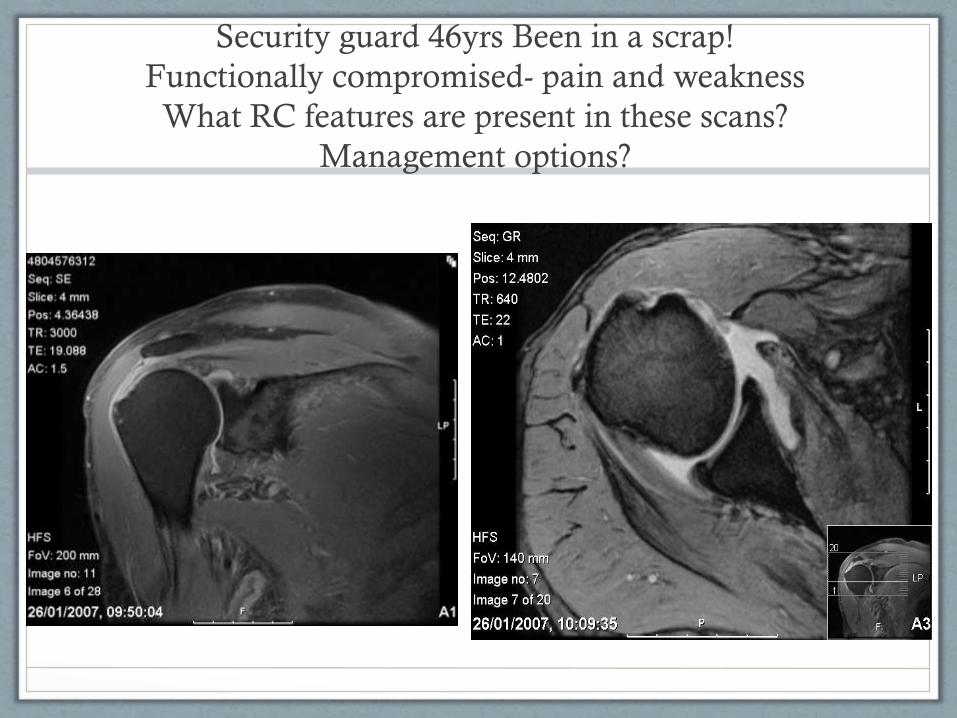
Security guard 46yrs Been in a scrap!
Functionally compromised- pain and weakness
What RC features are present in these scans?
Management options?
Use of Ultrasound vs MRI
• Dynamic
• Operator dependent and machine dependent
• Cheaper, faster
• Option to inject bursa, suck up soft calcium or babbotagehard calcification
• Good view:
• R cuff, bursa, muscle belly, biceps, calcification
Ultrasound;
Diagnosis and Therapeutic Intervention
• ACJ Pathology
• Capsule Hypertrophy/Intra-articular view/Ultrasound guided injection
• Lumps
• Eg Lipoma
• SCJ Pathology
• Lumps and fluid collections (Xray required; CT may be indicated)
• Sub Acromial Pain
• Rotator Cuff Pathology
• Bursal inflammation
• Calcification
US disadvantages
• Operator and machine dependent
• If inject then require MR, the MRI will be distorted
• MRI better for planning surgical intervention
Sub-Acromial and intra-articular Injection
Complications; Steroid Flare and Infection
Steroid Flare;
• Significant increase in Pain within 24-48 hours (once local
worn off)
• Can last 4 days. 20% of these will have facial flushing
• >30% incidence Fawi et al 2017
Infection; RARE
Occurs minimum several days post injection
Hot, swollen locally BUT NOT necessarily generally unwell
Degenerative Joint Disease /
Rotator Cuff pathology.
MRI Informing Management.
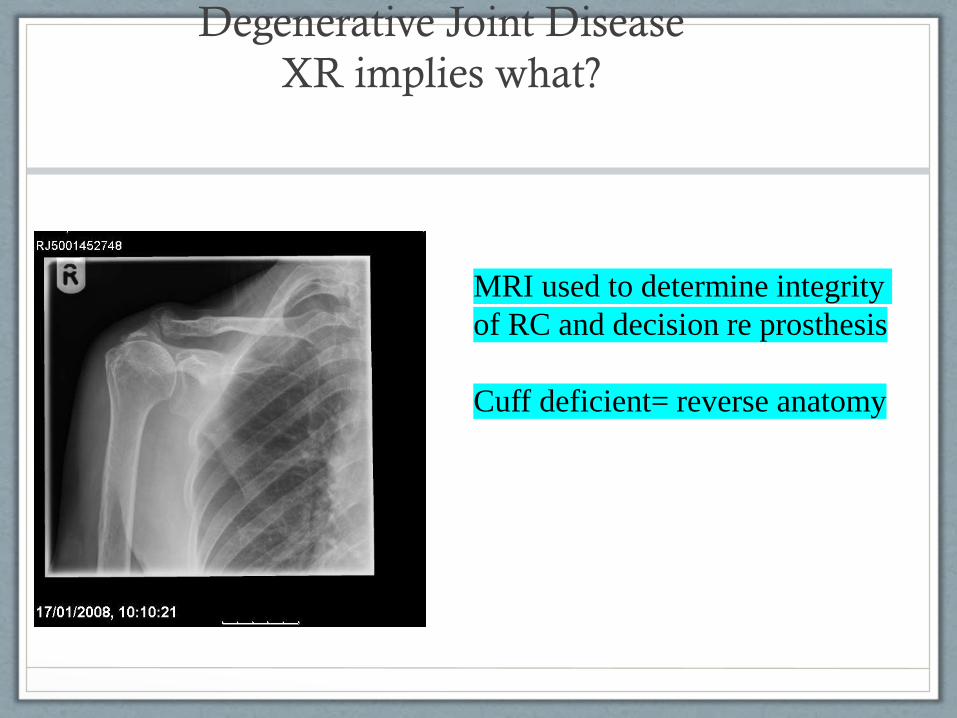
Degenerative Joint Disease
XR implies what?
MRI used to determine integrity
of RC and decision re prosthesis
Cuff deficient= reverse anatomy
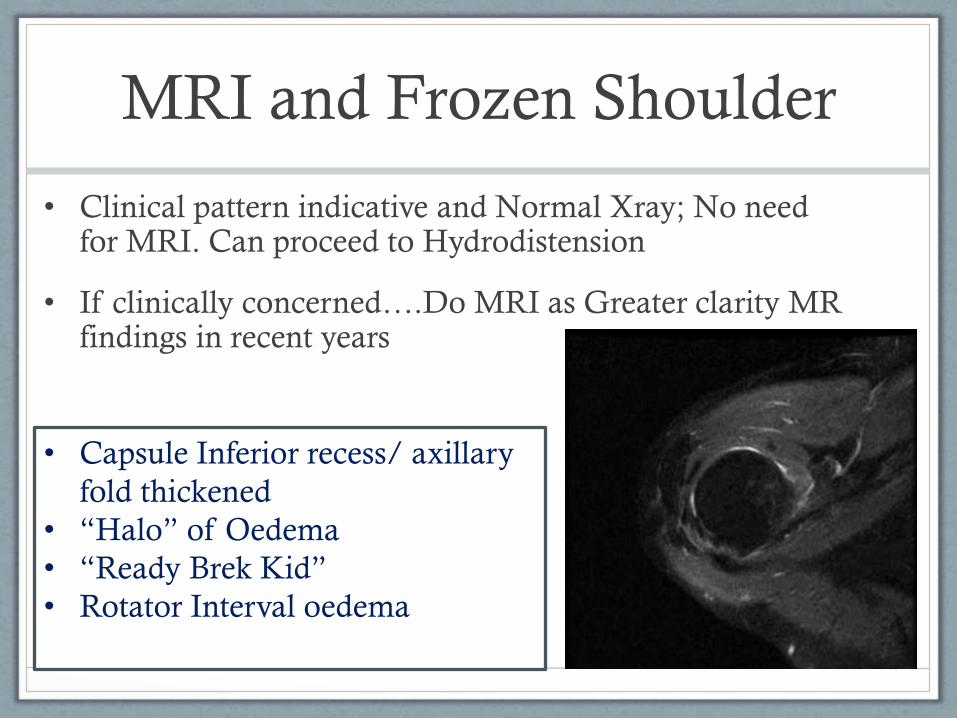
MRI and Frozen Shoulder
• Clinical pattern indicative and Normal Xray; No need for MRI. Can proceed to Hydrodistension
• If clinically concerned….Do MRI as Greater clarity MR findings in recent years
• Capsule Inferior recess/ axillary
fold thickened
• “Halo” of Oedema
• “Ready Brek Kid”
• Rotator Interval oedema
MRI and Instability

Normal GH ligs – MGHL behind SSC
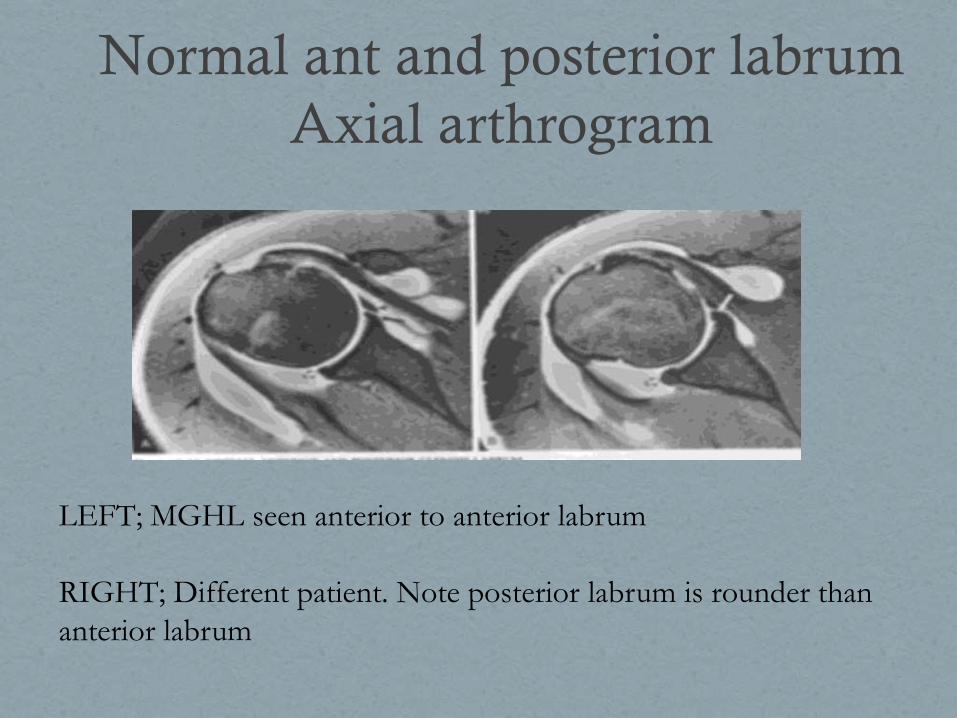
Normal ant and posterior labrum
Axial arthrogram
LEFT; MGHL seen anterior to anterior labrum
RIGHT; Different patient. Note posterior labrum is rounder than
anterior labrum
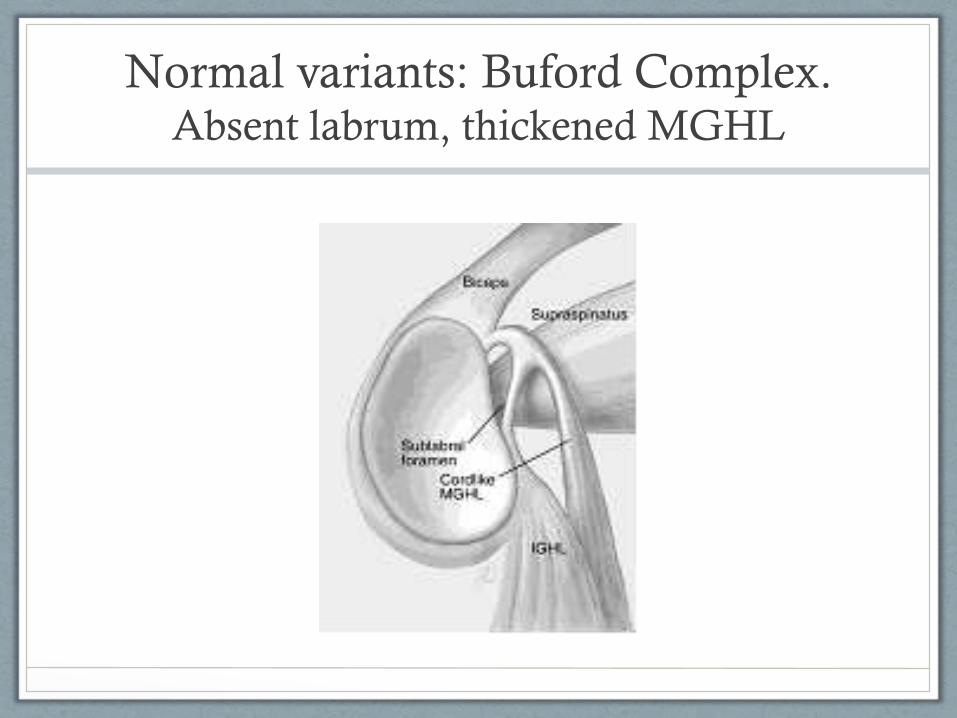
Normal variants: Buford Complex. Absent labrum, thickened MGHL
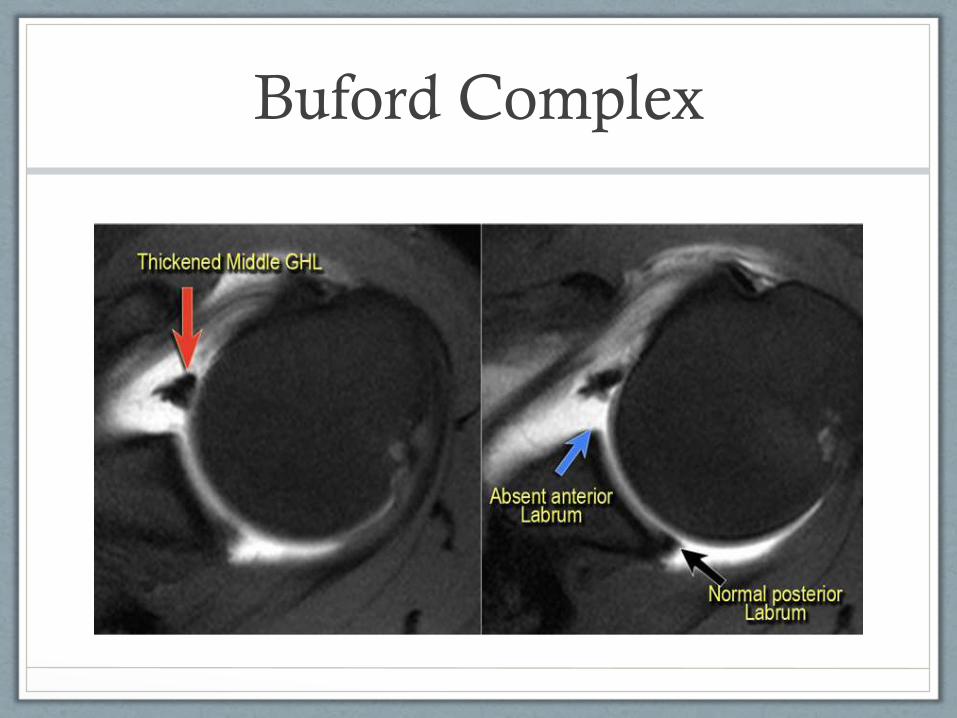
Buford Complex

Most common lesions
• BANKART
Anterior labrum torn/absent
• HILL SACHS
Posterior humeral head fracture
• BONY BANKART
Glenoid fracture antero-inferior
ANTERIOR INSTABILITY POSTERIOR INSTABILITY
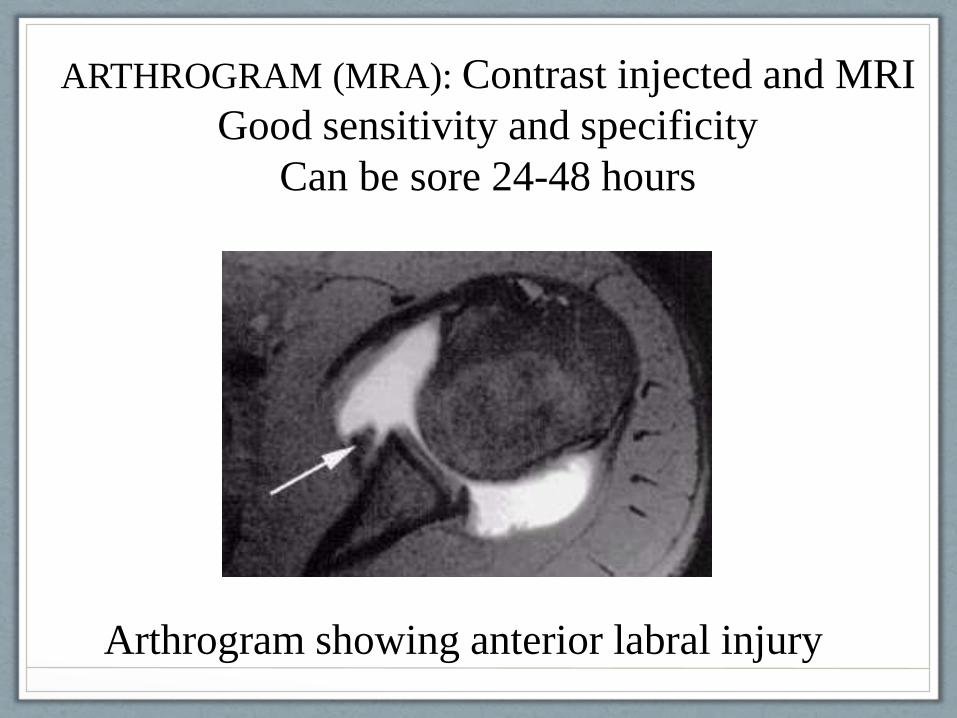
Arthrogram showing anterior labral injury
ARTHROGRAM (MRA): Contrast injected and MRI
Good sensitivity and specificity
Can be sore 24-48 hours

Instability Lesions – axial MRA
• Bankart (labral bankart on arthrogram)
• Left; Anterior labral tear plus ?tear anterior periosteum. Hill Sachs defect
• Right; Tissue lying in medial joint space (completely detached) Could be labral or bone from HS defect
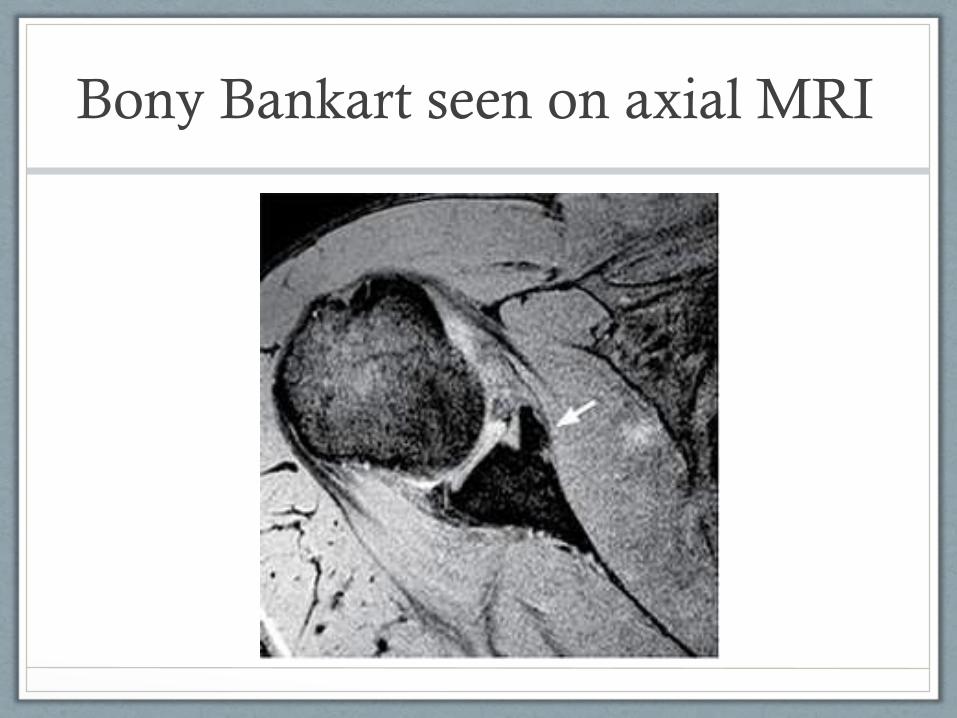
Bony Bankart seen on axial MRI
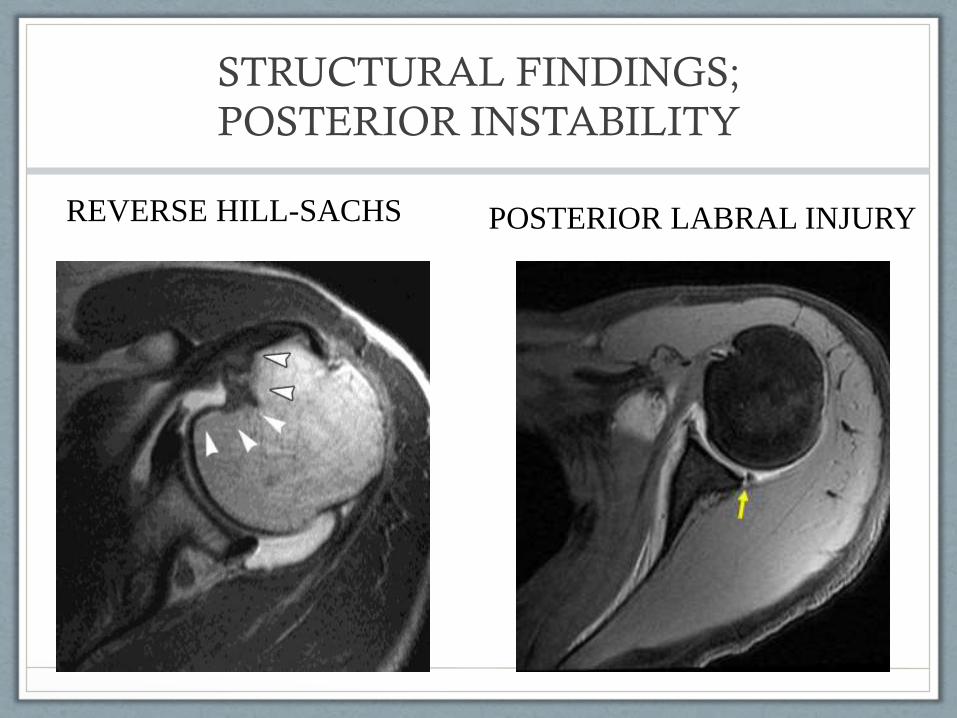
STRUCTURAL FINDINGS;
POSTERIOR INSTABILITY
POSTERIOR LABRAL INJURY REVERSE HILL-SACHS
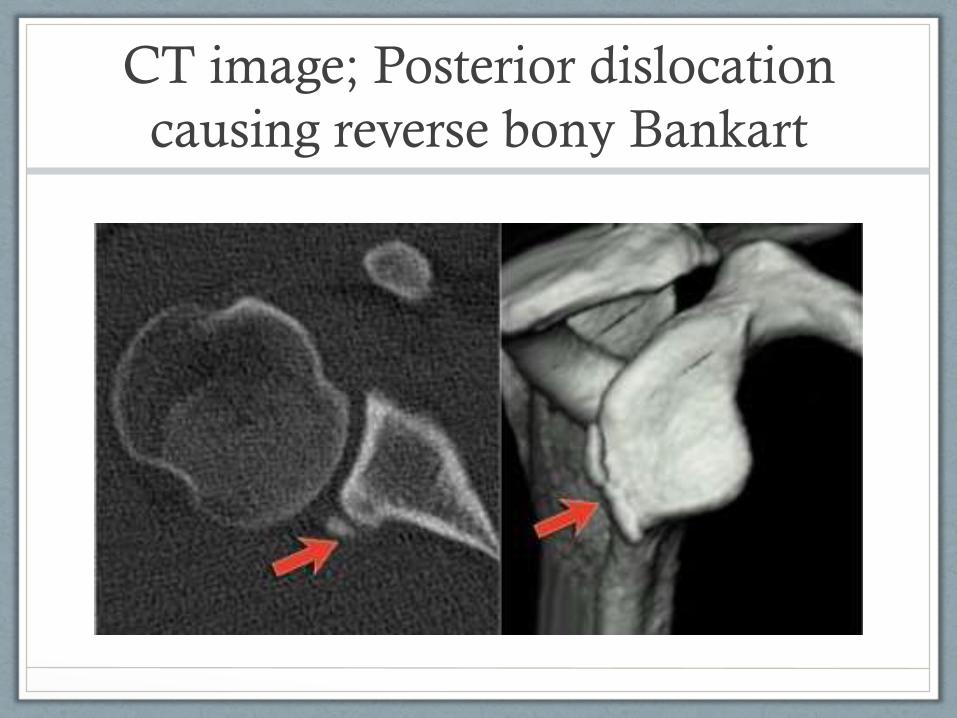
CT image; Posterior dislocation
causing reverse bony Bankart
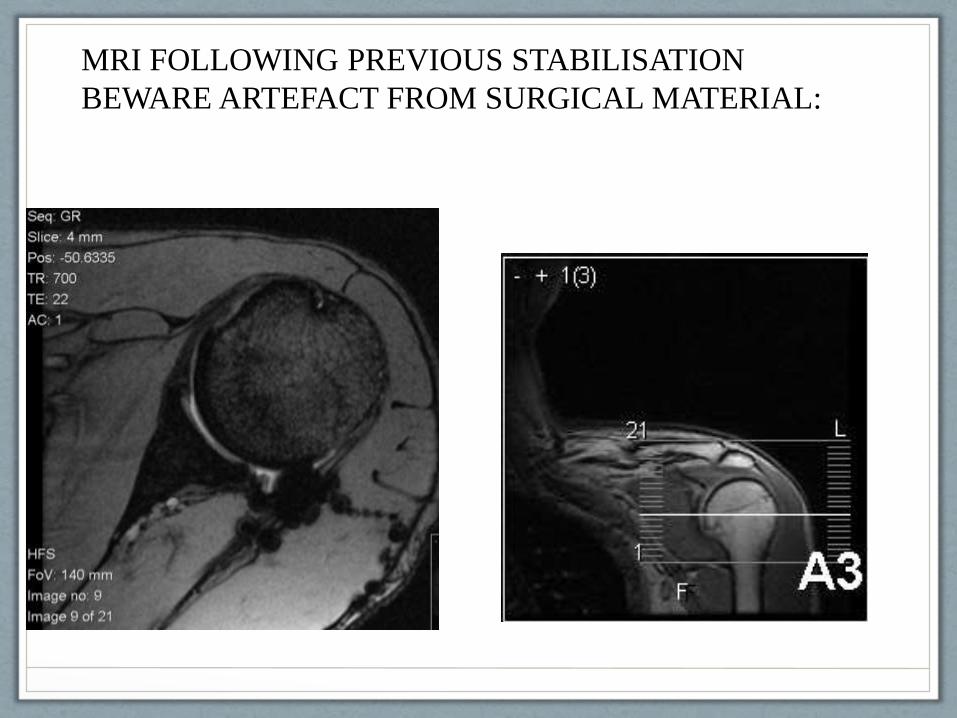
MRI FOLLOWING PREVIOUS STABILISATION
BEWARE ARTEFACT FROM SURGICAL MATERIAL:
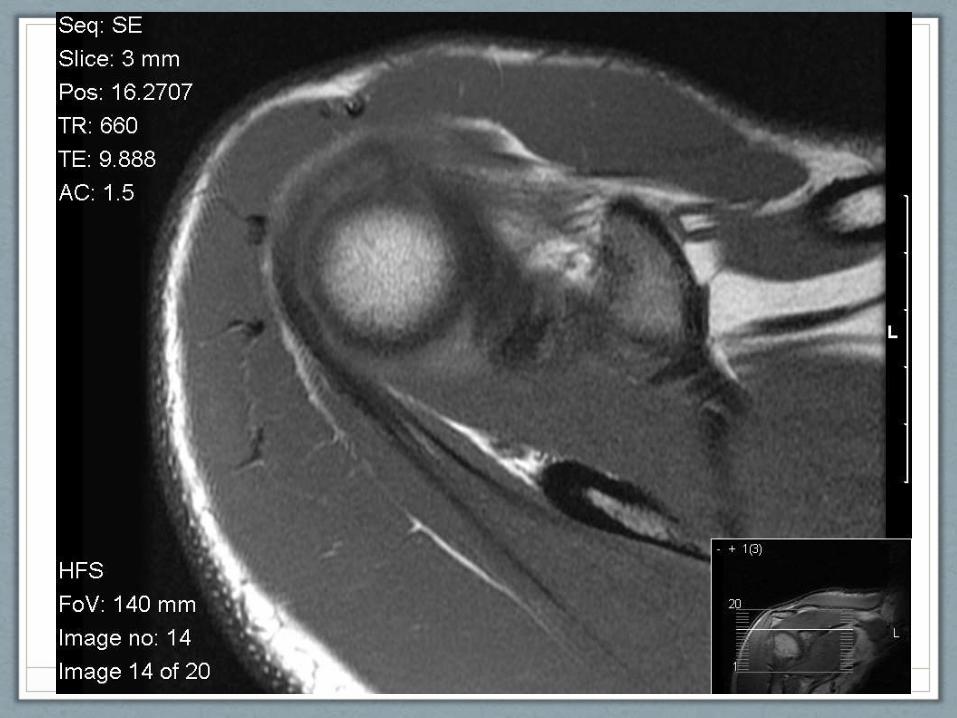
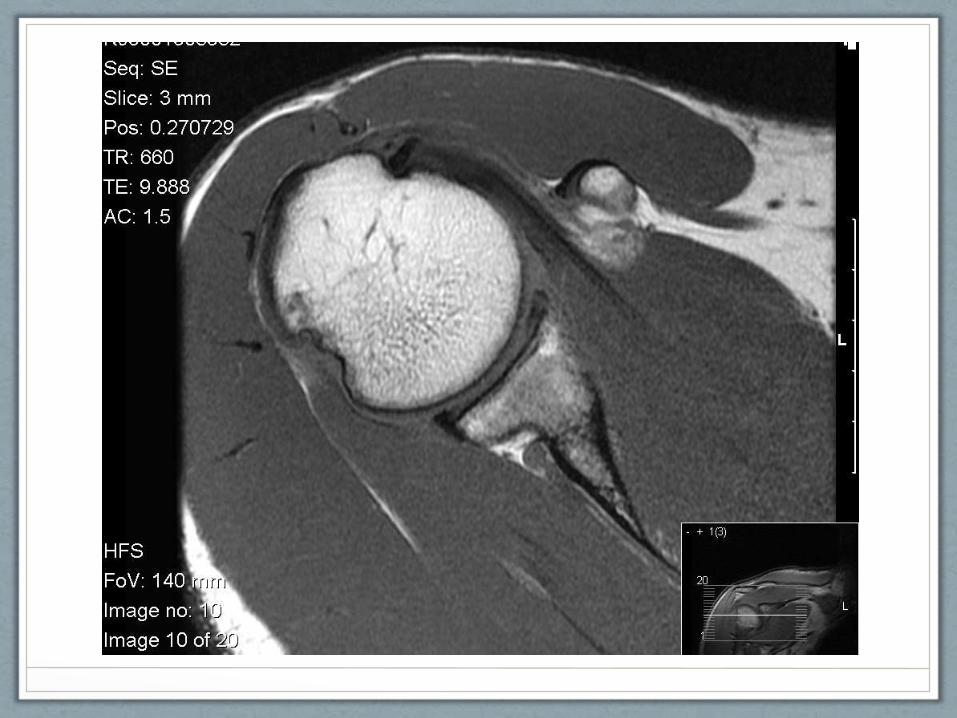
Axial views of a patient with recurrent
instability and anterior apprehension
Orientate yourself and look for any signs
of labral pathology










Investigation Selection
Instability
MRI Good for Labral pathology if quality machine and
slices. Axial views most helpful
Good muscle differentiation
Arthrogram Better for Labral specificity and sensitivity.
Slightly increased risk infection
CT: Excellent bony construct. High Ionising radiation
dose
Arthroscopy Gold standard

WITH SPECIAL THANKS TO
OUR COLLEAGUES AT
St Marys and Imperial College
[email protected]@central-health.com
Cathy Barrett BSc MSc MCSP MACP FACPMember of the British Elbow and Shoulder Society
Lecturer University College Londonhttps://www.ucl.ac.uk/prospective-students/graduate/taught-
degrees/physiotherapy-studies-musculoskeletal-msc