intensive care units (icu) - regina qu'appelle health · pdf file1 when someone you care...
TRANSCRIPT

Intensive Care Units (ICU)
CEAC 0876 June 2015

1
When someone you care for is critically ill or injured and requires admission to an Intensive Care Unit (ICU), it can be an anxious and confusing experience for you. Please know that we appreciate how worried and concerned you are. Be assured that we are taking the very best care of your family member. Our units are state-of-the-art. Our staff are educated, experienced, committed, and compassionate. Our number one priority is caring for our patients and helping them recover. This booklet is to help you understand how our ICU’s work. Information is provided about:
what to expect when you are here what we need from you what you can count on from us.
There are 3 ICUs in the Regina Qu’Appelle Health Region:
Pasqua Hospital: Intensive Care Unit (ICU)
Regina General Hospital: Medical Intensive Care Unit (MICU) Surgical Intensive Care Unit (SICU)
Important Numbers
Pasqua Hospital
Intensive Care Unit (306) 766-8555 Patient Advocate Services (306) 766-3232 Native Health Services (306) 766-2298 Spiritual Care (306) 766-3341 Security Services (306) 766-2900 Social Worker (306) 766-2402 Regina General Hospital
Medical Intensive Care Unit (306) 766-4291 Surgical Intensive Care Unit (306) 766-3990 Patient Advocate Services (306) 766-3232 Native Health Services (306) 766-4808 Spiritual Care (306) 766-3341 Security Services (306) 766-3900 Social Worker (306) 766-4631

2
Our Vision: The Critical Care Program at the RQHR is committed to the provision of family centred care initiatives. We promote an interdisciplinary approach to family care that will embrace the principles of respect, confidentiality, accountability, and professionalism. Our Mission: We shall achieve this vision by building collaborative partnerships with families through: Caring: Providing high quality family centred care in the ICU. Learning: We are an innovative academic health care centre dedicated to enhancing our knowledge, research and program development that will positively impact on the health and well-being of our patients and families. Advocacy: Through advocacy, partnership and respect we will campaign for the improvement of services and resource allocation that will foster making and goal setting. Leadership: The Critical Care Program is committed to inspiring and supporting the healthcare provider and the families understanding of quality end of life care in the ICU.
Family Centred Care
Family Centred Care recognizes the family as a constant in the patient’s life and promotes family participation and involvement in health care and decision making. Some important components of family centred care include: The promotion of collaborative relationships between the patient, their family and the Critical Care Team. We view families as allies who contribute to the well being of patients, especially the very young, the elderly, and the chronically ill. The recognition of the individual strengths and coping strategies of the family in crisis, coming to terms with critical illness, death, and dying. The recognition and respect for the diversity among families. The establishment of policies and programs that are responsive to the needs of the family and facilitate a supportive environment. The value of respect for the cultural diversity of families within Critical Care. The advocacy and support for informed decision making pertaining to end of life care, organ and tissue donation. The belief that quality, satisfaction, and value are improved when patients and families are involved in health care planning, implementation, and evaluation.

3
Family Rights and Responsibilities
Staff are committed to family centred care and to supporting the rights and responsibilities of patients and families. Patients and their families have the right to: the most appropriate, planned, and coordinated care that can be provided be treated with dignity, respect, and courtesy receive all information necessary to make informed decisions be told the names of the members of the Critical Care Team involved in their care receive clear answers to questions and full explanations about all aspects of care confidentiality. While your family member is in the ICU, you have the responsibility to:
comfort and support the patient to the extent other responsibilities allow, in the special way that only families can provide
join with the Critical Care Team to ensure the best possible treatment provide accurate information and to be available to the Critical Care Team either personally
or by telephone voice any concerns regarding your family member’s care to the Critical Care Team or to the
Patient Advocate recognize that the needs of other patients and their families may sometimes be more urgent
than your needs treat staff and other families in a considerate, courteous, and cooperative manner.
When Your Family Member Arrives to the ICU
The first hour after a patient is admitted to the ICU is a busy time for staff and can be challenging for the family. It takes time for the ICU Team to safely settle a critically ill/injured patient. You are asked to stay in the ICU waiting room/visitor’s lounge during this time. The ICU staff will keep you informed about your family member’s condition and facilitates your visit as soon as possible. Members of the Critical Care Team: social worker, Native Health Services educator, or Spiritual Care practitioner may visit you during this time.

4
Spending Time in the ICU To ensure the privacy of all patients and that the care they are receiving be maintained, we ask that you call in from the Waiting Room/Visitor’s Lounge before entering the unit. The direct phone line to the ICU Nursing Desk is located in the Waiting Room. When you enter the ICU, you hear a variety of noises from the machines surrounding your family member. What you see and hear is the latest technology that helps the Critical Care Team provide the best possible care to your family member. All ICU machines have alarms. These are safety devices to alert staff if your family member’s condition changes. The Critical Care Team can tell which alarms are emergencies and which ones are not. The alarms may surprise you at first but they are there to help with patient care. If you have a concern about an alarm, please ask the ICU staff about it. The frequency and length of your visits may be limited due to the very unpredictable nature of critical care. Things may not always go as planned. This can be frustrating, but we ask for your understanding. We ask that you limit visitors to immediate family members or people your family member would most want to see at this time. Patients who are in ICU are highly susceptible to infectious illnesses. Please do not visit if you are feeling sick. To avoid germs and infections, visitors must wash their hands before entering and before leaving the ICU. Please ask if you are unsure as to where to wash your hands. Sleep and rest are very important for recovery - short frequent visits are less tiring for your family member. You may be asked to delay your visit if your family member is resting or is receiving care at the time. To avoid overwhelming your family member and to allow adequate space to perform patient care, we ask that you limit visitors to no more than 2 at a time. You may be asked to take your family member’s personal belongings home. Toiletries and items such as glasses, hearing aides, and dentures may stay with the patient. Please ensure that these items are clearly labeled with your family member’s name.

5
Communicating with Your Family Member If your family member has an endotracheal tube (breathing tube) or a tracheostomy to help in breathing, he or she is unable to speak. The Critical Care Team uses other ways to communicate with your family member by: asking them to nod “yes” or “no” to questions asking them to squeeze hands or blink eyes in response to questions writing notes. Asking “yes” or “no” questions helps to relieve the frustration of your family member when they are unable to speak. We encourage you to communicate with your family member in this way as well. There may be times that the Critical Care Team requests that you sit quietly at the bedside and that you do not speak to or stimulate your family member. There are certain medical conditions such as a head injury, where stimulation can be harmful to your family member. Please know that if the Critical Care Team makes this request of you, it is in the very best interests of your family member.
Children’s Visits to the ICU Children who are close to someone who is critically ill may wish to visit. Usually a child who is ready to spend time in ICU will ask. It is natural to try to protect children from painful situations. As much as we might want to shield them from sad experiences, children know when something is wrong. Be open and honest and encourage children to talk about their feelings and their fears. Please speak to the bedside nurse or the social worker so that the visit can be planned and the child can be given support and prepared for the visit.
For Patient Safety and Infection Control
Balloons, flowers, and fruit baskets are not allowed in ICU. The ICUs are “scent free zones”. Please avoid using scented products such as perfume, cologne, aftershave, body spray, and hair products.

6
Note: The use of cellphones, DVD players, laptop computer equipment, iPads®, or any other electronic recording equipment is strictly prohibited while in the ICUs to ensure the privacy and confidentiality of all of our patients. If a recording device is found to be on or in use, you are asked to turn it off and leave the unit immediately. Cellular phones and other transmitting devices post great risk to patients in the ICUs who are dependent on monitoring and/or life support devices. Please restrict the use of electronic devices to the Waiting Room area. Please speak with the unit staff if you have any questions. Your cooperation is appreciated.
Learning the ICU Routines
The Critical Care nurses work 12 hour shifts. Shift changes happen at 7:30 a.m. and 7:30 p.m. every day. At this time nurses starting their shift receive a detailed report about their patient(s). Visiting may be limited during this time. The Critical Care Team holds rounds each day which may last for 2 or 3 hours. Rounds allow for the Critical Care Team to assess each patient and develop the plan of care for the day. More detailed information regarding rounds is provided in a section of this booklet. There may be specialized tests that require the movement of your family member to an area outside the ICU - a nurse always goes with the patient. Sometimes patients are gone for long-er than expected due to the nature of the tests. Please note that when patients come back to ICU, it takes 15 to 30 minutes to settle them back. We must ensure that all our equipment and monitoring devices are in place to ensure safe patient care. Patients are monitored very closely in the ICUs. They are repositioned, if their condition permits, every 2 hours or as needed. Our rooms have ceiling track lifts to help the safe movement of our patients. Mobility is a very important component to recovery. Your family member may be mobilized to a specialized chair or be assisted with walking by the nursing staff and the physiotherapists.

7
Research
Research is part of quality care. Research benefits patients by helping the Critical Care Team keep up to date in their professions. A Research Ethics Board screens all research studies to make sure they have scientific value and are ethical. A research study that involves critically ill patients is carefully reviewed before it is approved. You may be asked if you wish to volunteer your family member to take part in a research study to determine how well new treatments work for ICU patients. Allowing your family member to take part in a study is voluntary and does not affect his or her care. You can change your mind about allowing your family member to take part in a study at any time. If you have any concerns, please let the members of the Critical Care Team know.
Family Presence on Rounds (Family Rounds)
The family’s role in the care of a critically ill/injured patient is well respected and recognized. One of your greatest needs is the need for information. The Critical Care Team members of the answer your questions to the best of their knowledge. We understand and ap-preciate that you are receiving a lot of information that can be difficult to understand and deal with. 2 family members are welcome to participate in the multi disciplinary rounds in the Critical Care Units on Mondays, Wednesdays, and Fridays.
Pasqua Hospital
10:30 a.m. in the ICU
Regina General Hospital
10:30 a.m. in the SICU 1:15 p.m. in the MICU
Please note that the decision for family members to attend rounds is dependent upon the patient giving permission, if they are able to. If the patient is able to communicate they are asked: if they want their family members to attend rounds which family members they want to attend rounds. Please note that arrangements can be made to speak to a doctor at times outside of family rounds. The consistency of information sharing is key to keeping everyone well informed and up to date.

8
When You Participate in Family Rounds You Have the Opportunity to: share information about your family member learn about the plan of care for your family member ask questions, seek clarification, and to be updated regarding your family member.
Please Note:
You may hear a variety of opinions from the Critical Care Team as they discuss the treatment options for your family member. Teaching discussions for members of the Critical Care Team may occur during rounds. Please note that the discussion may not be directly about your family member.
Family Rounds
The Critical Care Team welcomes 2 family members to participate in family rounds on Mon-days, Wednesdays, and Fridays. The Critical Care Team respectfully requests that the 2 family members who participate in family rounds are the:
legal next of kin and the decision makers for the patient. same people each day to ensure consistency of communication. These family
members are to be the “family spokespersons”. It is the responsibility of the family members attending rounds to ensure that the rest of the family is kept well informed and updated.
The Critical Care Team is obligated to ensure and safeguard our patient’s privacy and confidentiality. Information is only given to immediate family and/or spokesperson. Please let the Critical Care Team know if you have any concerns about discussions of certain information. The family spokesperson(s) are the designated contact person for the Critical Care Team. They are asked to provide their phone number(s) to the Critical Care Team so that they can be contacted if there are any major changes in your family member’s condition.
At times, the ICU staff may call or page the family spokesperson in the hospital. This does not always mean there is an emergency. Please note that this is only done if we are unable to reach you by calling the phone number that has been provided to us.

9
Note: Any type of recording devices are prohibited on family rounds to ensure the privacy and confidentiality of all of our patients. If a recording device is found to be on or in use, you are be asked to turn it off and leave the unit immediately. If you are unable to attend and have requested someone else to attend family rounds in your absence, please ensure that you have updated them with your family member’s condition and have sent any questions to be answered. Medical words can be hard to understand and staff may say something that sounds confusing. You may feel that the ICU staff are giving you different information about your family member. If this happens, let them know and ask questions. ICU staff do their best to answer them because they want you to fully understand the situation. Discussion can include information that may be difficult for you to hear. Please tell the staff if you need some extra support or explanations of what has been said during family rounds. We suggest that you write down your questions/concerns to ensure that they are answered/addressed. To ensure the timeliness of rounds, the Critical Care Team may arrange for a separate meeting to facilitate further discussion with you. Sometimes there are unexpected situations that may delay a scheduled family meeting. We ask for your understanding if this occurs. Please note that you are asked to leave the unit when rounds have been completed on your family member to ensure the privacy and confidentiality of the other patients in the unit. If members of the family are disrespectful, verbally, or physically abusive to a patient or a staff member, they are be asked to leave immediately and are not be allowed to participate in rounds in the future. If you require a translator, one can be provided for you.

10
Critical Care Team Members
Doctors
Intensivist - is the doctor who specializes in critical care medicine and is responsible for directing patient care. He/she is your family member’s primary doctor in the ICU. Critical Care Associate (CCA) - is a doctor who manages patient care in the unit on a 24 hour basis under the direction of the Intensivist. Resident - is a doctor in training who works under the direction of the Intensivist and CCA. One or more of them may be present in the ICU 24 hours a day. JURSI - is a medical student. Manager - is responsible for the overall functioning of the unit. Nurses Registered Nurses (RNs) - have specialized education to prepare them to care for critically ill patients. They discuss your concerns with you and answer your questions. Charge Nurse - directs patient care and unit activities during their 12 hour shifts. Bedside RNs - care for 1 or 2 patients during their 12 hour shifts. Registered Respiratory Therapists (RRT)
They are responsible for airway management and breathing support, the breathing machines (ventilators) which most ICU patients need.
Physiotherapists (PT)
They assess patients upon a doctor’s request. They are involved in specific patient positioning, suctioning, mobilization, including ambulation, strengthening and balance exercises, passive range of motion exercises, and airway clearance techniques.
Occupational Therapists (OT)
They assess patients at a doctor’s request. They are involved in promoting function and independence through specialized seating, positioning equipment, splinting to prevent loss of joint movement, prevent skin breakdown, and screening for cognitive impairments.
11
Speech Language Pathologists (SLP) They assess and treat patients upon a doctor’s request. They assess how well a patient is swallowing and decide the best treatment for swallowing problems. They assist the ICU staff and families communicate with patients who are having difficulty speaking. Clinical Dietitian They assess the patient’s nutritional needs and recommend an appropriate diet. This diet may be given by mouth, by a tube through the stomach /small bowel, or by intravenous. Clinical Pharmacists They provide the Critical Care Team with information on drug selection, dosing, interactions and side effects, and provide recommendations for adjustments as required. Social Workers They provide support for family members. They may be involved in assisting with family conferences, providing supportive counselling, crisis intervention, bereavement counselling, advocacy, and mediation. They may assist with discharge plans to other community agencies. Native Health Services Educator They assist with communication issues, families wishing to include traditional care elder support, as well as providing end of life support for patients and families. They assist with patients and families mental, physical, emotional and spiritual needs. Spiritual Care Practitioners They help make possible healing wholeness by tending to the soul and facilitating soul work. They may be certified Spiritual Health Therapists, Denominational Chaplains, or Community Faith Leaders. Health Care Students
We provide on site teaching opportunities and clinical experiences for students who are training for any of the above professions. Students work under the direct supervision of senior staff. To deal with some of the pressure of working in an ICU, staff sometimes use humour as a way to cope. This helps to reduce stress and anxiety in the environment. Please understand that this does not reflect a lack of caring or compassion for your family member.
12
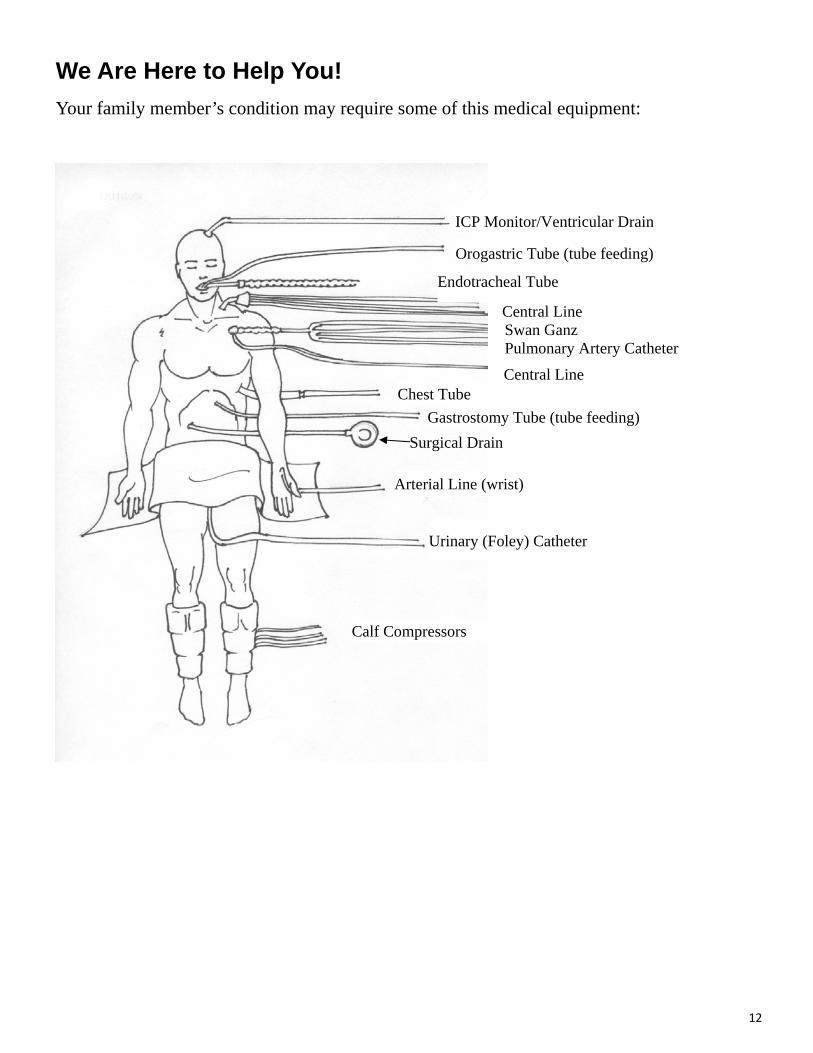
We Are Here to Help You!
Your family member’s condition may require some of this medical equipment:
ICP Monitor/Ventricular Drain
Orogastric Tube (tube feeding)
Endotracheal Tube
Central Line Swan Ganz Pulmonary Artery Catheter
Central Line Chest Tube
Gastrostomy Tube (tube feeding)
Surgical Drain
Arterial Line (wrist)
Urinary (Foley) Catheter
Calf Compressors

13
Medical Words:
Analgesics: Medications used to reduce and control pain. Angiogram: X-rays taken during the injection of dye into a blood vessel. Arterial line/art line: A small plastic tube placed in an artery (usually in the wrist but sometimes in the groin or foot) for painless blood samples and monitoring blood pressure. Blood gases: A blood sample that measures oxygen and carbon dioxide. Calf Compressors: Inflatable cuffs that go around the legs to prevent blood clots. Continuous Renal Replacement Therapy (CRRT): a form of dialysis. Blood is removed from the body through a special catheter/tube and passes through the CRRT machine to remove fluids and toxins from the body on a 24 hour basis when the kidneys are not working properly. CT (CAT) Scan: An x-ray used to show detailed pictures of the body. Central Line: A catheter (tube) placed in a large central vein to facilitate the administration of intravenous fluids and medications. Chest Tube: A tube placed in the chest to drain air or fluid from the cavity around the lung. Dialysis Catheter: A tube placed in a large vein to facilitate hemodialysis or CRRT. Electrocardiogram (ECG): A test to measure the heart’s electrical function. Edema: Swelling in an arm, leg, or face. EEG (Electroencephalogram): A test that measures brain activity. It is used to help diagnose seizures or brain abnormalities. Endotracheal Tube (E-tube) or Breathing Tube: A tube that goes through the nose or mouth and into the airway. It connects the patient to a (ventilator) breathing machine. Extubation: Removal of the endotracheal tube by a respiratory therapist. Gastrostomy Tube: A special tube placed in the stomach by a doctor to allow feeding. Hemodialysis: A catheter/tube placed in a large vein for the continuous slow removal of blood which can then pass through a dialysis machine to remove body wastes or poisons when the kidneys are not working properly.

14
Infection Control Precautions: Sometimes patients’ health conditions require their family members and the members of the Critical Care Team to wear gowns, masks, and gloves in their rooms to prevent the spread of certain types of infections. Intracranial Pressure Monitor (ICP): A small catheter (tube) placed in the brain to monitor pressure, especially when swelling is a concern. Intubation: Insertion of an endotracheal tube by a doctor or a respiratory therapist. Sepsis/Septic Shock: Overwhelming infection that causes organ dysfunction. Spinal Precautions: Instructions to the Critical Care Team to maintain the position of a patient’s spine until certain x-rays have been performed and interpreted by a specialist. Suctioning: Secretions are removed from the mouth, throat, or lungs by inserting a small tube and applying suction. Surgical Drains: A soft tube placed in various body cavities to allow fluids to drain. Swan Ganz or Pulmonary Artery Catheter: A special catheter (tube) that is inserted by a doctor through a central line into a major blood vessel in the lungs to provide information about a patient’s heart and lung function. Tracheostomy: A tracheostomy is the hole created though the skin into the trachea or windpipe; the hole is held open by a tube to keep a clear passage to the lungs. A tracheostomy is required if a patient cannot protect their airway, if they require a ventilator, or if there are too many secretions to be coughed up effectively and suctioning is needed. Tube Feeds: This is a way to meet some or all of the patient’s nutritional needs and is provid-ed by a special liquid formula containing protein, fats, carbohydrates, vitamins, minerals, fibre, and water. This formula is given through a tube into the stomach or small intestine. Urinary Catheter: A soft tube placed in the bladder to allow continuous drainage of urine. Ventilator: A machine to help a patient breathe. Ventricular Drain: A small catheter/tube placed in the brain that monitors pressure and removes extra fluid in the brain. Weaning: The gradual process of lessening the support of a ventilator and allowing the patient to breathe on their own.
15
Taking Care of Yourself When a family member is ill, it can be easy to forget that you need to take care of yourself as well. You are an important member of the Critical Care Team and part of your role is to stay healthy to best help your family. Suggestions for Coping and Staying Healthy Try to keep a positive outlook. You may see signs of progress, then setbacks. You may hope for a complete cure, a successful treatment or a painless end to suffering. It often helps to discuss your feelings with someone and the ICU staff can help you in this way. Sleep is very important to maintain your good health. Overnight stays in the visitor lounge are not encouraged. You are not be at your best for your family member if you are not well rested. We encourage you to leave the hospital to get a good night’s sleep. If you are from out of town, please ask staff for help finding a place to stay. Your family member may have a long recovery and will rely on your strength as he or she starts to feel better. You can call the ICU anytime to ask about your family member’s condition. Staff always call you if there is a significant change. Eat balanced meals even though you may not feel Hungry. Proper nutrition is important to maintain strength. Going for walks and fresh air helps to reduce stress.
Any medical conditions you have can get worse during this stressful time. Let the ICU staff know if this is happening. Try to maintain your normal routines as much as possible. You can bring your own clergy to the hospital at any time. Most religious associations have spiritual support available 24 hours a day. You can contact someone from the Spiritual Care Department. If you would like to do this, tell the nurse caring for your family member. Each hospital has a chapel and a healing lodge to provide a quiet environment for thought and reflection. Visitor’s Lounge/Waiting Rooms
Pasqua Hospital: located on the 2nd floor across from the ICU. Regina General Hospital: located on the 2nd floor - 1 directly across the hall from the SICU and 1located beside the MICU. We cannot be responsible for your personal belongings. Please do not leave valuables unattended in the lounge.
We ask that everyone is respectful of these areas and keep them as tidy as possible. If problems arise, please contact the ICU staff for assistance.

16
For Your Comfort
Pasqua Hospital
Cafeteria is located on level 0. Robin’s Donuts is located on the main floor just inside the main entrance doors.
Regina General Hospital
Cafeteria located on level 0. Robin’s Donuts is located on the main floor down from the 14th Avenue entrance or
from the 15th Avenue entrance to the hospital.
Keeping You Informed
Your family member may be transferred between the 3 ICU’s. The Intensivist makes the decision in the best interests of your family member. The transfer may be necessitated by a variety of reasons. The Critical Care Team explains the need for the transfer to you. Please ask for clarification if needed. Your family member is cared for by a RN and a RRT during the transfer. The Intensivist decides when your family member should be transferred from the ICU to a nursing unit. When you learn that your family member is leaving the ICU, it can cause mixed emotions. For some it may be a time of celebration and for others a time of increased anxiety and stress. It is normal to feel this way and the ICU team helps you and your family member as you make the transition. Family rounds are one avenue that you can utilize to discuss your concerns with the doctor.
If you have any questions, please discuss them with ICU staff.
Photos are courtesy of RQHR Medical Media Department.
Acknowledgement to the Calgary Health Region Intensive Care: A Support Guide for Families.

CEAC 0876 June 2015