interindividual and intraindividual pharmacokinetic...
TRANSCRIPT
Interindividual and intraindividual
pharmacokinetic variability
Mark J. Ratain, M.D.
University of Chicago
2nd International Workshop on Clinical
Pharmacology of Anticancer Drugs
Madrid, Spain
September 13, 2017




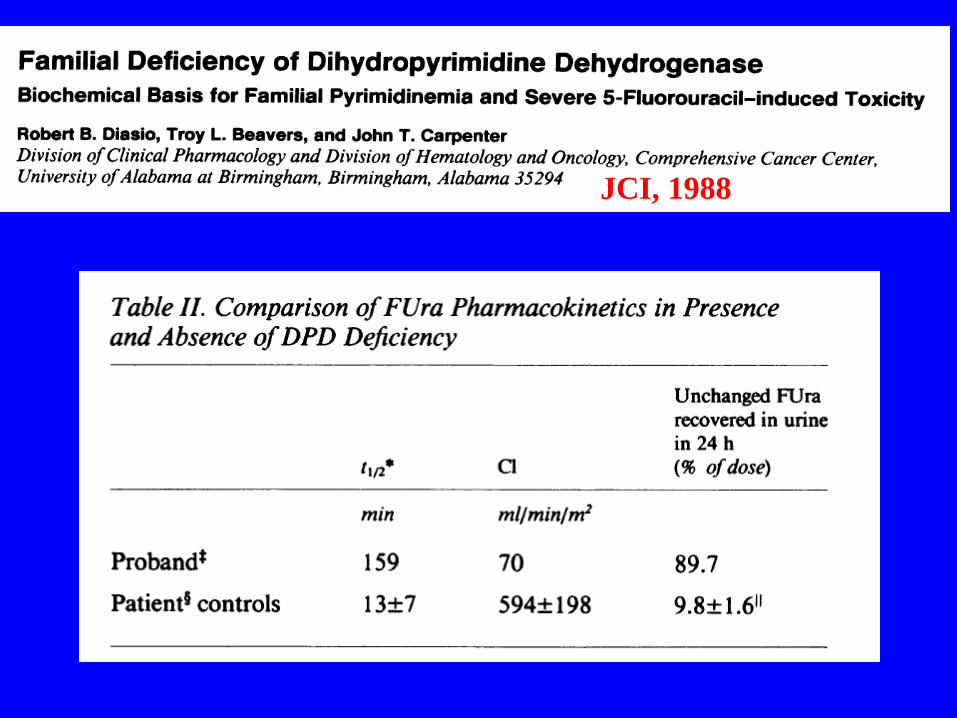
JCI, 1988

Jin et al., J. Natl. Cancer Inst. 97:20-39, 2005.
Tamoxifen Biotransformation
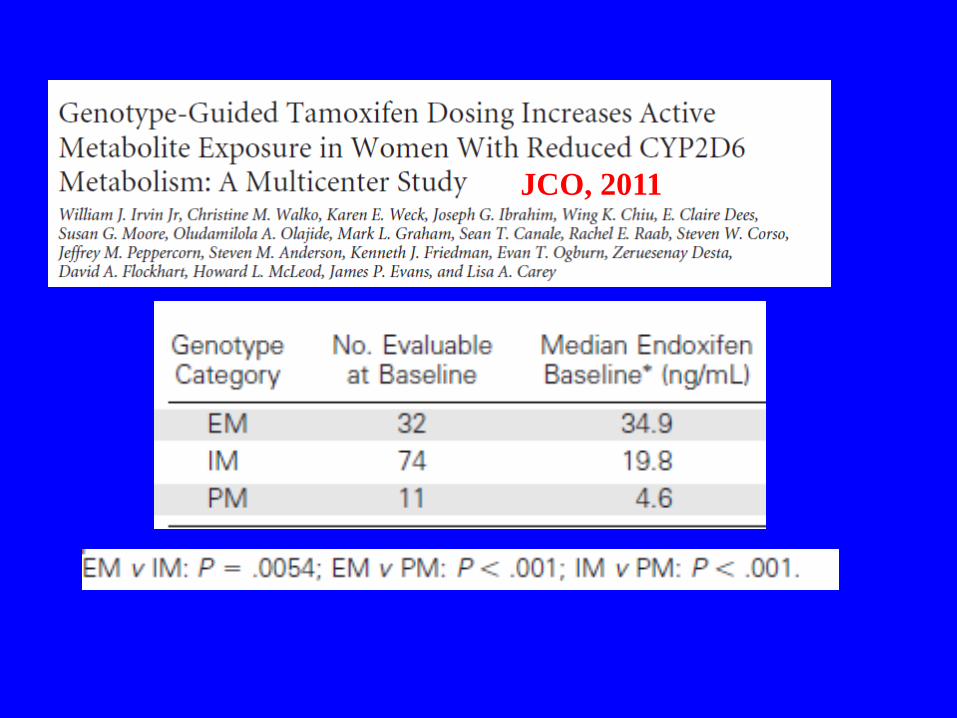
JCO, 2011

Metabolism of Irinotecan (CPT-11)
CPT-11
APC
SN-38G
SN-38
CYP3A4
CE
UGT1A1
N N
O
O
NN
O
O
OH O
C2H5
NN
O
O
OH O
C2H5
H O
N
O
O
NN
O
O
OH OC2H5
HNH O
O
O
NN
O
O
OHO
C2H5
O
C O O H
O HHO
0302_Irinotecan (CPT-11)
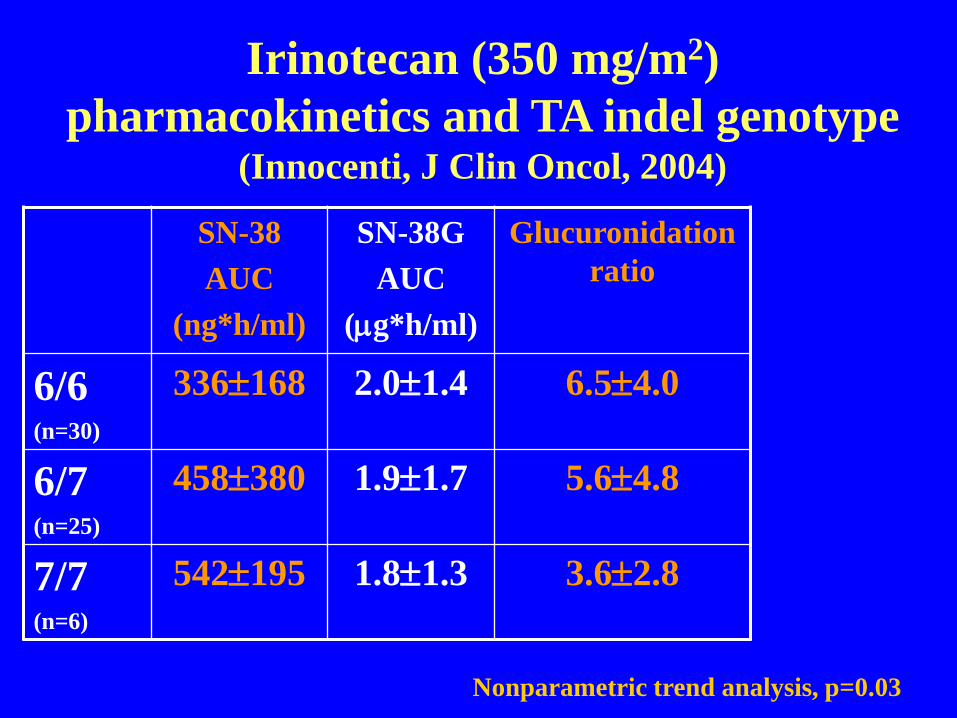
Irinotecan (350 mg/m2)
pharmacokinetics and TA indel genotype (Innocenti, J Clin Oncol, 2004)
SN-38
AUC
(ng*h/ml)
SN-38G
AUC
(g*h/ml)
Glucuronidation
ratio
6/6(n=30)
336168 2.01.4 6.54.0
6/7(n=25)
458380 1.91.7 5.64.8
7/7(n=6)
542195 1.81.3 3.62.8
Nonparametric trend analysis, p=0.03

Relationship between CL and phenotypic measurement of CYP3A4.
JoAnn Hirth et al. Clin Cancer Res 2000;6:1255-1258
©2000 by American Association for Cancer Research


Intraindividual variability of
antiretrovirals
(Nettles, Clin Inf Dis, 2006)
• Lopinavir/ritonavir 24-92%
• Nelfinavir/M8 metabolite 30-54%
• Ritonavir 34-43%
• Saquinavir 52-55%

Why is intraindividual variability of
increasing importance in oncology?
• Increasing use of oral drugs
– Often with low bioavailability
– Substrates for CYP3A
• Increasing use of expensive drugs
– Financial incentive to increase
bioavailability
• Increasing use of monoclonal antibiodies
– May have time-dependent clearance

Erlotinib concentrations versus time following the 150 mg erlotinib dose (A) and the 300 mg erlotinib dose (B).
Marta Hamilton et al. Clin Cancer Res 2006;12:2166-2171
©2006 by American Association for Cancer Research
CCR, 2010
Focus on 23 drugs with marked (+50%) food effect
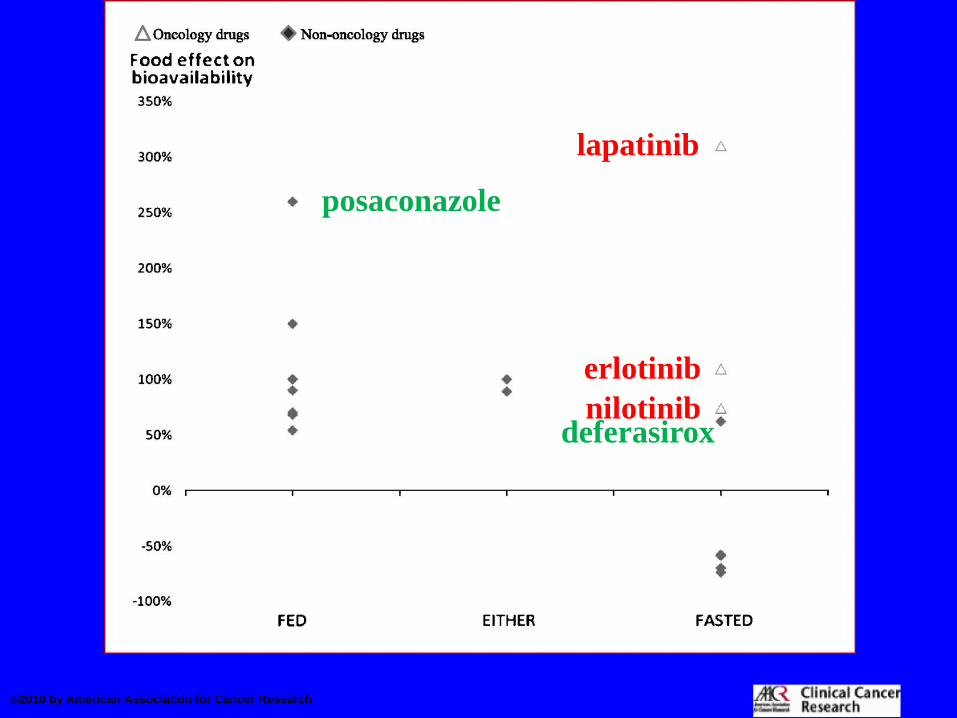
©2010 by American Association for Cancer Research
lapatinib
nilotinib
erlotinib
deferasirox
posaconazole


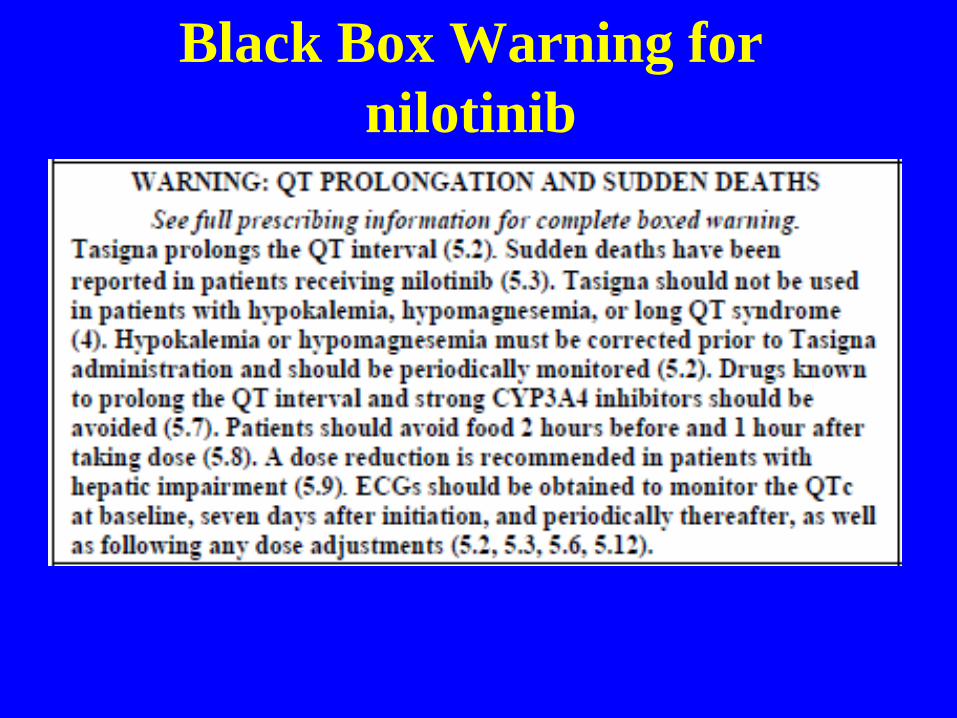
Black Box Warning for
nilotinib

Nilotinib labeled to be taken
fasting
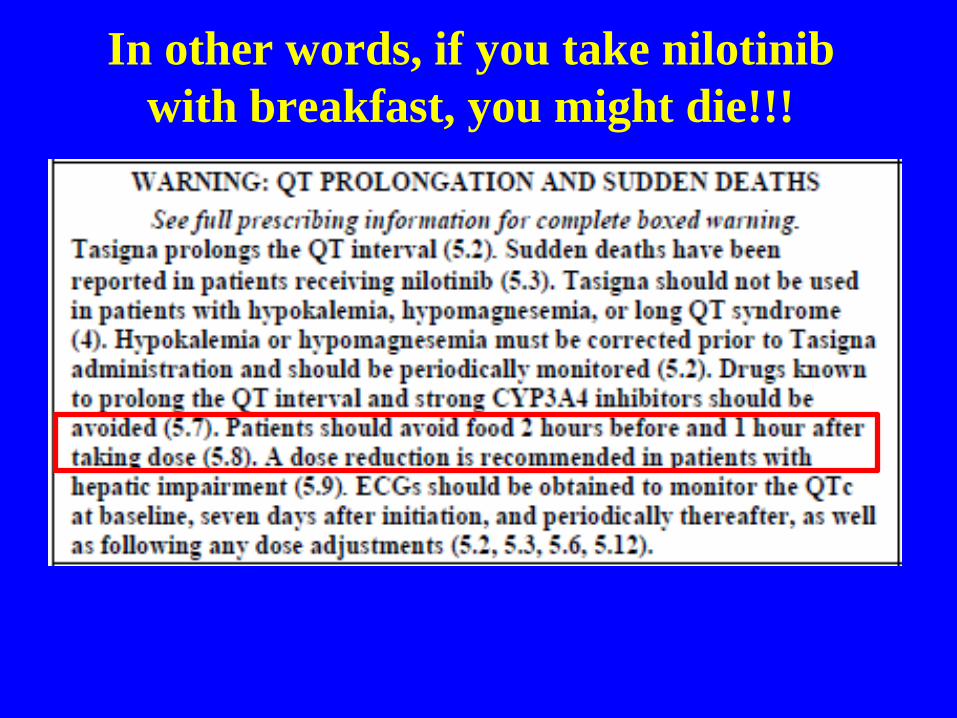
In other words, if you take nilotinib
with breakfast, you might die!!!

Abiraterone
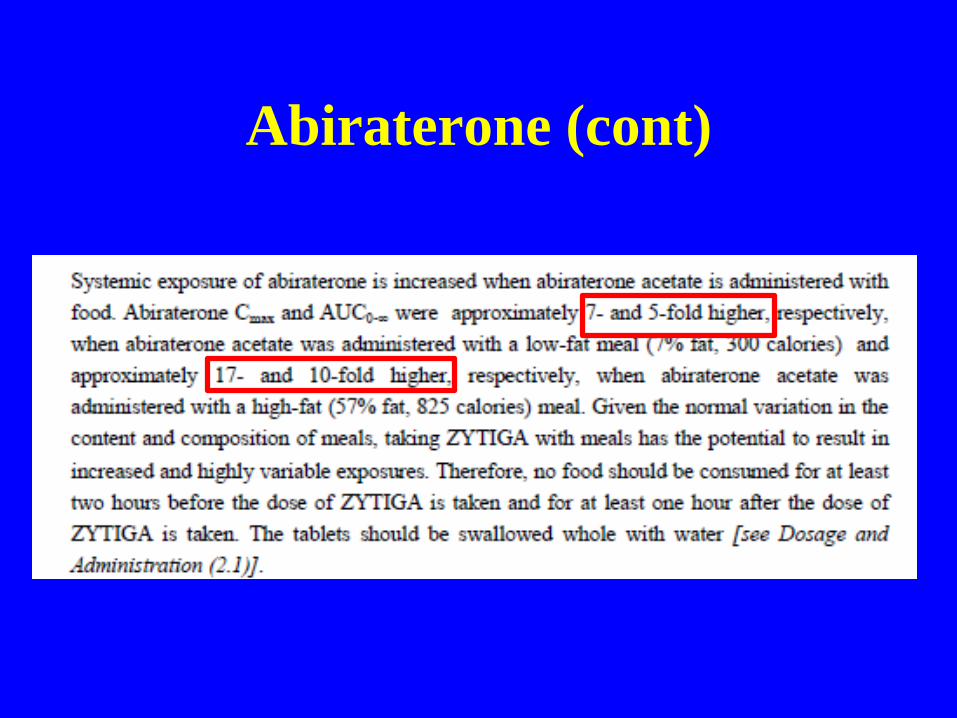
Abiraterone (cont)


A prospective international randomized
phase II study evaluating the food effect
on the pharmacokinetics (PK) and
pharmacodynamics (PD) of abiraterone
acetate (AA) in men with castrate
resistant prostate cancer (CRPC)
Russell Szmulewitz, MD

Hypothesis and Design
• Hypothesis: Lower-dose abiraterone taken
with food will have a similar effect on CRPC as
full-dose taken fasting. We will use serum PSA
as a pharmacodynamic marker of abiraterone
effect.
Progressive CRPC• PS 0-2• Prior keto
stratification
R
STD: Abiraterone 1000mg/day fasting+ prednisone 5mg BID
LOW: Abiraterone 250mg/day with low fat meal+ prednisone 5mg BID
Primary Objective: PSA response at 12 weeks

Study demographics• 72 patients across 7 centers (6 US, 1 Singapore)
Characteristics STD (n=36) LOW (n=36)
Age
Median (range)- year 71(49-83) 69(53-83)
>75 years- no of patients /total no 10(27%) 11(31%)
Disease location, n(%)
Bone 25(69%) 25(69%)
Visceral 5(14%) 5(14%)
Prior systemic treatment for CRPC, n(%)
0 14(39%) 12(33%)
2-Jan 14(39%) 16(44%)
3 or more 2(6%) 1(3%)
Prior chemotherapy, n(%)
0 21/36(58%) 19(53%)
1 9(25%) 9(25%)
2 or more 0(0%) 1(3%)
ECOG performance status, n(%)
0 or 1 33(92%) 33(92%)
2 2(6%) 3(8%)
Prostate- specific antigen
Median (range) 48.4(0.73-1789) 48.4(1.01-1768)
Race, n(%)
White 26(72%) 17(47%)
African American 5(14%) 11(31%)
Asian 5(14%) 7(19%)

Primary endpoint: PSA response-Nadir
STD (1000mg fasting) LOW (250mg fed)
PSA50%-Nadir: STD=61%,LOW=69%, **PSA50% on COU-302=62%

Understanding intraindividual
variability may create
opportunities to monetize clinical
pharmacology knowledge
• Clearance of oral small molecules can be
decreased with food or CYP3A4
inhibitors
• Modulation of clearance of monoclonal
antibodies may also be feasible
• High drug prices have created new
“targets” for pharmacokinetic
modulation