international journal of physiotherapy and research, … · int j physiother res 2014;2(6):815-23....
TRANSCRIPT

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 815
Original Article
DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERALEPICONDYLITISG Saroja 1, Antony Leo Aseer P *2, Venkata Sai P M 3.1 Faculty of physiotherapy, Sri Ramachandra University, Chennai, Tamil Nadu, India.2 Reader in physiotherapy, Sri Ramachandra University, Chennai, Tamil Nadu, India.3 Professor & Head in Radiology, Sri Ramachandra University, Chennai, Tamil Nadu, India.
The aim of the present study was to analyze the diagnostic accuracy of the commonly used provocative tests inthe diagnosis of lateral epicondylitis (LE). Cozen’s test, Mills test and Maudsley test are most widely used. Tilldate no studies have been reported on the diagnostic accuracy of these tests. Musculoskeletal ultrasonographyserves as a gold standard tool in the diagnosis of LE. Thirty subjects participated in the study. Baselinemeasurements of pain severity, elbow joint mobility, hand grip strength and three provocative tests wererecorded by the principal investigator. A second investigator accompanied the subjects for musculoskeletalultrasonography who was blinded of the test results. The thickness of common extensor tendon, echo textureand lateral epicondyle bony contour was measured. The test results of the three provocative tests withultrasonographic findings were analyzed. The sensitivity for Cozen’s test, Maudsley test and Mills test wasfound to be 84%, 88% and 53% respectively. The specificity for Cozen’s Maudsley and Mills test was found to be0%, 0% and 100% respectively. Mills test showed significant area under receiver operator curve (ROC) i.e.(0.769), which explains that the test has good diagnostic accuracy. This validation study, concludes that Millstest has an excellent diagnostic value for ruling in LE.KEYWORDS: Lateral epicondylitis, Tennis elbow, Provocative tests, Diagnostic accuracy.
ABSTRACT
INTRODUCTION
Address for correspondence: P. Antony Leo Aseer, Reader in Physiotherapy, Sri RamachandraUniversity, Chennai-600 116. Tamil Nadu, India. E-Mail: [email protected]
International Journal of Physiotherapy and Research,Int J Physiother Res 2014, Vol 2(6):815-23. ISSN 2321-1822
DOI: 10.16965/ijpr.2014.699
The elbow complex comprises of threearticulations, namely humeroradial, humero-ulnar and superior radioulnar joints. Even thoughelbow joint is not a weight bearing joint, but itis subjected to various stresses and loads duringexplosive activities of the upper limb. A cycleof excessive loading, overuse and repetitiveactivities leads to elbow pathologies. Lateralepicondylitis (LE) is known colloquially as tenniselbow, shooter’s elbow, archer’s elbow or simplylateral elbow pain. Runge was the first todescribe this condition in 1873. The term tennis
elbow exhibits its link to racquet sports. Theincidence of lateral epicondylitis varies from 1%to 3% in general population and in tennis playersit only accounts for about 5% between 30-50years of age.1
As the name suggests the primary site ofpathology in LE is at the common extensor origin.Extensor carpi radialis brevis (ECRB) tendon ismost commonly involved and less frequentlyExtensor carpi radialis longus (ECRL) tendon. Insome cases the anterior portion of EDC has alsobeen reported to be involved. The injury occursat the tenoperiosteal junction but scar tissue
Quick Response code
Access this Article online
International Journal of Physiotherapy and ResearchISSN 2321- 1822
www.ijmhr.org/ijpr.htmlAccepted : 24-11-2014Published (O): 11-12-2014Published (P): 11-12-2014
Received: 08-11-2014Peer Review: 08-11-2014Revised: 15-11-2014DOI: 10.16965/ijpr.2014.699

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 816
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.
may form over the tendon itself or at themusculotendinous junction. The cyclic loadingof stresses causes micro tears with formationof granulation tissue under the tendon and atthe tenoperiosteal junction.LE is most common among athletes over 30years with a history of repetitive movements ofwrist extension combined with forearmsupination. Occupational activities such ashammering, painting, using heavy spanners areconsidered to be the causative factors. Painincreases while gripping small objects as thishand position places additional stretch on theforearm extensors. However in LE the patho-physiology involves microscopic as well asmacroscopic changes at the common extensororigin.Biomechanically the ECRB is under maximumtension when it contracts during forearmpronation, wrist flexion and ulnar deviation. Thisis the typical position for a backhand shot inracquet sports. Repeated movement causeshypertrophy of this muscle and often results inloss of flexibility. In addition an imbalance existsbetween the forearm flexors and extensors.2
Tennis elbow is a troublesome disorder whichusually presents as pain over the lateralepicondyle extending distally. The pain graduallyincreases with overuse or may result from asingle incident (trauma). Pain may furtheraggravate by adding forearm supination andradial deviation. Wasting of the affectedmuscles and weak grip strength may also beseen in long standing cases.3
Most of the LE cases are diagnosed based onthe subjective history and physical examination.Findings such as history of pain over lateralelbow on occupational activities and ADL’s, pointtenderness over common extensor origin,reduced grip strength, range of motion and wristextensor strength testing help in the diagnosis.But very few studies are available on thereliability of these measures for the diagnosisof LE. The reliability of hand grip testing using adynamometer in lateral epicondylitis wasassessed in 2002.The inter examiner reliabilitywas found to be .98, inferring maximum painperception while gripping the dynamometer.4
Later, a preliminary clinical prediction rule (CPR)
was postulated to identify those with lateralepicondylitis who were likely to benefit frommobilization with movement (MVM) for whichexercises were devised in 2009. The variableswere based on history taking and physicalexamination findings. The CPR was formed usingthree variables namely age < 49 years, affectedpain less grip strength > 112N and unaffectedpain less grip strength < 336N. If all the threevariables were present, the diagnostic accuracy(i.e.) specificity was shown to be 100% andsensitivity 1%.5 Chair test and Coffee cup test(Coonrad,1986) was also suggested to confirmthe diagnosis.6 The most widely accepted andused tests are Cozens test, Mill’s test andMaudsley test.7
Provocative tests are typically used to pin pointor isolate specific tissues with pathology.Reliability and Validity remains the mostimportant element of a provocative test.Compared to the other regions, physicalexamination tests used in upper extremity lacksreliability and validity.8 With extensive search,there were no psychometric properties availablefor lateral epicondylitis .9 Joshua Cleland anextensive researcher on evidence basedorthopedic special tests, in his recent text editedin 2011, and reported no diagnostic accuracy ofthe commonly used provocative tests in lateralepicondylitis.10
Mohamed Waseema et al in 2012 in a reviewreported that physical examination of LEincludes palpation, use of special tests such asCozen’s and mills and grip strength measure.They also reported that by far the validity i.e.specificity and sensitivity of Cozen’s test andmills test has not been studied. All of the aboverecent studies highlight the lacunae in thecurrently available tests and paves way forevaluating the diagnostic accuracy of the testsemployed in LE.To measure the diagnostic accuracy of the abovementioned tests, a gold standard method is theneed of the hour. Musculoskeletal ultra-sonography has been proven to have highsensitivity but low specificity in the diagnosisof LE and is the most useful tool in the diagnosisof a disorder based on pathological tissuechanges.11

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 817
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.
MATERIALS AND METHODS
Physical examination tests/ Provocation tests:Mill’s test: The Subject was positioned in asitting posture with the shoulder slightlyabducted, elbow flexed to 90°, forearm pronatedand wrist flexed so that the palm of the handwould face downwards. The therapist stoodbehind the subject’s affected side, with one handgrasping the upper arm for support and thesubject’s arm was elevated to 70° of abduction.The thumb of the other hand was then placed inthe patient’s palm between the index finger andthumb and the fingers wrapped around thedorsum of the wrist, to maintain the forearmposition in full pronation and wrist in flexion.While maintaining this position, the elbow wasextended slowly. Pain over the lateral aspect ofthe elbow joint indicated a positive test.Cozen’s test: The subject stood with the affectedelbow fully extended and forearm pronated. Thetherapist stabilized the subject with one handby placing his/her thumb over lateral epicondyle.Instruction was given to make a full fist withwrist extension against resistance followed bypronation and passive radial deviation. Pain overthe lateral aspect of elbow joint indicated apositive test.Maudsley test: The Subject sat with the elbowflexed to 90° and forearm pronated. He was thenasked to extend the middle finger against resi-
Ultrasonography is advantageous as it is themost simple and cost effective method ofmusculoskeletal system imaging with portabilityand real-time dynamic examination.12
Overall, Musculoskeletal Ultrasonography canbe considered as a tool of reference in thediagnosis of LE. The various parameters that canbe assessed include tendon thickness,echotexture, fluid content and appearance ofcortical surfaces. Increase in tendon thicknessis a significant feature of LE. Echo texture oftendon in fibrillar pattern depicts normalcywhereas hyper echoic pattern signifiesinflammation, hypo echoic pattern is seen in casefluid loss in tendon and anechoic patternsignifies presence of fluid. Specks of hyperechoicpattern are seen in case of calcification andcortical irregularities which are evident in chroniccases.Hence, this study is the first of its kind thatfocuses on the psychometric properties ofCozen’s, Mills and Maudsley tests in thediagnosis of LE.
This validation study was approved by the ethicscommittee for student ’s proposal of SriRamachandra University (CSP/12/SEP/25/139).Study participants: All patients diagnosed withLE referred to physiotherapy outpatientdepartment of Sri Ramachandra Hospital whomet the inclusion criteria were included in thestudy.Subjects with lateral elbow pain, age group of30 to 45 years of both genders and medicaldiagnosis of lateral epicondylitis / tennis elbowwere included and those presenting withdiagnosis of cervical radiculopathy ormyelopathy, neurological disorders, fractures inand around elbow joint and othermusculoskeletal disorders related to lateralelbow pain were excluded.Study design: Validation studySample size: The sample size was estimatedusing data taken from a study done in 2008 inwhich 28 subjects were recruited.13
Instrumentation: Universal Goniometer JammarDynamometer Musculoskeletal UltrasonographyImaging – LOGIQ P5
Procedure: 30 subjects who were referred forLE participated in the study, 10 males and 20females. Hand dominance was checked for allthe subjects of whom 28 subjects were righthanded while 2 subjects were left handed. Allsubjects underwent a physical examination ofelbow and wrist joint by the principal investigatorto confirm the presence of LE.History and physical examination: Painlocation, characteristics, behavior, severity,nature of lesion, history of overuse, repetitivestresses were examined. Pain severity wasmeasured using visual analog scale.14 Thelocation of pain and tissue integrity wasanalyzed by palpation of bony contours andsurrounding soft tissues. The elbow joint motionof the involved elbow was measured using aplastic Goniometer. The Jammar dynamometerwith third spacing was used to measure gripstrength.

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 818
-stance.Pain over the lateral aspect elbow jointindicated a positive test.The test results of the three provocative testswere correlated with the gold standard methodi.e. musculoskeletal ultrasonography. The testresults of physical examination were keptconfidential with the principal investigator. Thesecond examiner, who accompanied thesubjects for Musculoskeletal Ultrasonographywas blinded to the test results. Allmusculoskeletal ultrasonic examination wasdone by the same examiner who has anexperience of 7years in musculoskeletal imaging.Ultrasound machine of LOGIQ P5 of GE Companywas used in which a linear transducer is usedwith a high frequency probe of 12MHz frequency.The subject was comfortably seated with elbowsupported and flexed at 90 degrees. The scanwas performed in a longitudinal fashion with thetransducer over the lateral epicondyle and withthe linear array parallel to the radius. Thecommon extensor origin (CEO) was looked fortendon thickness which was compared to theuninvolved side, echotexture, presence of fluidand bony contour of lateral epicondyle forcortical irregularity.
MSUS report- (i) Normal tendon thickness
(ii)-Increase in tendon thickness(involved)
(iii) Common extensor tendon showinghyperechogenecity
(iv) Common extensor tendon showinghypoechogenicity.
Finally, the principal investigator compared thetest results of physical examination with theultrasonographic findings for diagnostic accu-racy of the three provocative tests. The sensi-tivity, specificity, positive and negative likelihoodratios of cozen’s, mills and maudsley tests wereanalyzed.
RESULTSDuring Musculoskeletal ultrasonographysubjects had a thorough examination for lateralepicondylitis by considering the parameters. Theultrasonograhic findings were then comparedwith physical examination findings to determinethe diagnostic accuracy of Cozen’s,Mill’s andMaudsley test in LE.A total of 30 subjects underwent physicalexamination for lateral elbow pain and alsomusculoskeletal ultrasonography. Out of 30subjects, males accounted for 33% and female’s67%.The mean age was 43 years. Thepercentage of dominant side involved was 80%and non dominant side is 20%. The mean valueof pain severity was 3.6 and elbow flexion ROM
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.
Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 819
was 133 degrees and elbow extension was 0degrees. The mean grip strength of the involvedextremity was 14.5 kg. degrees and elbowextension is 0 degrees.The Mean grip strengthof involved extremity is 14.5 kg.Musculoskeletal Ultrasonography findings:Line diagram: Comparison of tendon thicknessof uninvolved and elbows with LE.
On ultrasonography, the tendon thicknessvaried significantly in patients who were posi-tive for LE with a mean of .46cm of uninvolvedtendon and .57cm for the involved tendon.
Graph 1: Distribution of tissue texture.
When considering the texture of the tendon, outof 30 patients 20 showed normal echotexturewhile 10 patients showed altered echogenecity.
Graph 2: Distribution of fluid.
Graph 3: Distribution of bony irregularity.
Out of 30 subjects, only one exhibited fluidcontent and bony irregularity which denotes lessnumber of subject’s exhibit chronicity of thecondition.
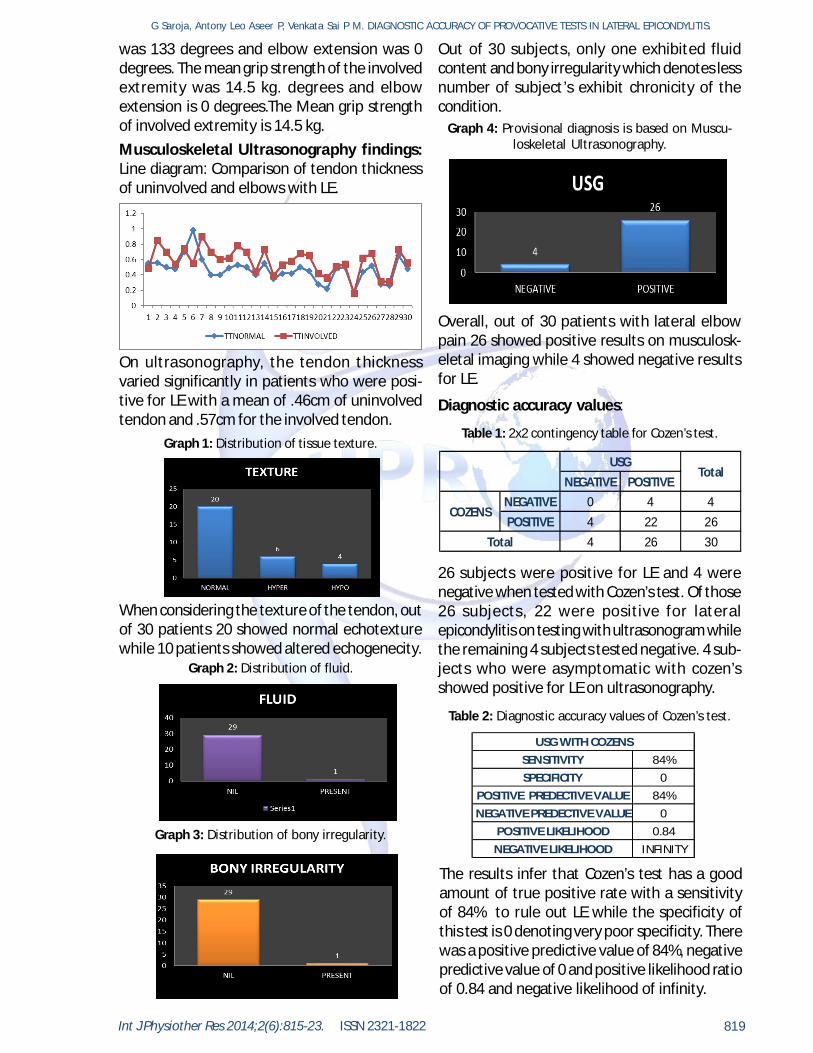
Graph 4: Provisional diagnosis is based on Muscu-loskeletal Ultrasonography.
Overall, out of 30 patients with lateral elbowpain 26 showed positive results on musculosk-eletal imaging while 4 showed negative resultsfor LE.
Diagnostic accuracy values:
Table 1: 2x2 contingency table for Cozen’s test.
NEGATIVE POSITIVE
NEGATIVE 0 4 4POSITIVE 4 22 26
4 26 30
USGTotal
COZENS
Total
26 subjects were positive for LE and 4 werenegative when tested with Cozen’s test. Of those26 subjects, 22 were positive for lateralepicondylitis on testing with ultrasonogram whilethe remaining 4 subjects tested negative. 4 sub-jects who were asymptomatic with cozen’sshowed positive for LE on ultrasonography.
Table 2: Diagnostic accuracy values of Cozen’s test.
SENSITIVITY 84%SPECIFICITY 0
POSITIVE PREDECTIVE VALUE 84%NEGATIVE PREDECTIVE VALUE 0
POSITIVE LIKELIHOOD 0.84NEGATIVE LIKELIHOOD INFINITY
USG WITH COZENS
The results infer that Cozen’s test has a goodamount of true positive rate with a sensitivityof 84% to rule out LE while the specificity ofthis test is 0 denoting very poor specificity. Therewas a positive predictive value of 84%, negativepredictive value of 0 and positive likelihood ratioof 0.84 and negative likelihood of infinity.
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 820
Table 3: 2x2 contingency table for Maudsley test.
NEGATIVE POSITIVE
NEGATIVE 0 3 3POSITIVE 4 23 27
4 26 30
USGTotal
MAUDSLEY
Total
27 subjects tested positive for lateral epicondyli-tis and 3 tested negative .Out of 27 subjects, 23were positive and 4 were negative for LE onultrasonographic examination .Remaining 3 sub-jects who were negative with maudsley, testedpositive for LE on ultrasonography.
Table 4: Diagnostic accuracy values of Maudsley test.
SENSITIVITY 88%SPECIFICITY 0
POSITIVE PREDECTIVE VALUE 85%NEGATIVE PREDECTIVE VALUE 0
POSITIVE LIKELIHOOD 0.88NEGATIVE LIKELIHOOD INFINITY
USG WITH MAUDSLEY
The results infer that the Maudsley test has agood true positive rate with a sensitivity of 88%whereas it is a poorly specific test. It showedpositive predictive value of 85%, negativepredictive value of 0 and positive likelihood ratioof 0.88 and negative likelihood of infinity.
Table 5: 2x2 contingency table for Mill’s test.
NEGATIVE POSITIVE
NEGATIVE 4 12 16POSITIVE 0 14 14
4 26 30
USGTotal
MILLS
Total
14 subjects were tested positive and 16 subjectstested negative for lateral epicondylitis onexamination with Mills test. The 14 subjects whowere positive for Mills test showed a positivecorrelation for LE on ultrasonography. Out of the16 negative subjects on physical examination,4 tested positive on ultrasonic examination.
Table 6: Diagnostic accuracy values of Mill’s test.
SENSITIVITY 53%SPECIFICITY 100%
POSITIVE PREDECTIVE VALUE 100%NEGATIVE PREDECTIVE VALUE 25%
POSITIVE LIKELIHOOD INIFINITYNEGATIVE LIKELIHOOD 0.47
USG WITH MILLS
The results infer that Mills test has an averagetrue positive rate with sensitivity of 53% to ruleout LE but a very good true negative rate to rulein LE with 100% specificity. Positive predictivevalue of 100% and negative predictive value of25% was seen. A positive likelihood ratio ofinfinity and 0.47 negative likelihood ratio. Outof the three provocative tests, Mills test showedgood specificity and partial sensitivity, whereasCozen’s and Maudsley exhibited good sensitivityand poor specificity.Receiver operator characteristic (ROC) curve:A good test results in a ROC curve that rises tothe upper left hand corner in a rapid manner.Therefore the area under the curve is themeasure of the quality of the diagnostic test.Hence, larger the area, better the diagnosticvalue.
ROC curve for Cozen’s testGraph 5: ROC curve for Cozen’s test.
Since, the area under the curve is very less of0.423, the cozen’s test is found to have lessaccuracy value.
ROC curve for Maudsley testGraph 6: ROC curve for Maudsley test.
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 821
The area under the curve is0.442 which is veryless and hence the Maudsley test has loweraccuracy for LE.
ROC curve for Mill’s testGraph 10: ROC curve for Mill’s test.
The ROC curve for Mill’s test shows significantarea under curve i.e 0.769 which indicates thetest has a good diagnostic accuracy for lateralepicondylitis.
DISCUSSION
Although the positive predictive value forCozen’s is 84% and 85% for Maudsley test. Thenegative predictive value is 0% which impliesthat an individual is truly disease free whenCozen’s and Maudsley show clinically negativeresults. In the present study, Cozen’s andMaudsley failed to produce negative clinicalresults in 4 subjects, indicating 0% poorprobability of detecting disease free.The most valuable data was the likelihood ratio(LR). In this study the positive LR for Cozen’swas 0.84 indicating that Cozen’s test is .84 timesmore likely to be positive in the presence ofdisease the than in the absence of disease. Thenegative LR for Cozen’s and Maudsley is foundas infinity. This suggests subjects with LE hada negative cozen’s and maudsley is infinite timesas often as those who did not have LE.Considering the test results, Mills test shows100% specificity which is a good reliable toolfor identifying individuals who do not have thedisease as really not having it. It also has a 50%chance of correctly identifying individuals whohave the disease as positive as it has 53%sensitivity. The positive predictive value of Millstest is 100%, so the probability that the diseaseis present when the test result is positive is100%.Out of 30 subjects, 14 subjects weresymptomatic on Mills test and all 14 of themwere diagnosed with lateral epicondylitis onmusculoskeletal ultrasonography. It has 25%negative predictor value which shows that thereis a 25% probability that the disease is notpresent when the test result is negative. Out of16 subjects with negative Mills test only 4showed negative results for lateral epicondylitison ultrasonography while 12 were positive forthe condition.On the analysis of LR values, positive LR ofinfinity for Mills test indicates that it is infinitetimes more likely to be positive in the presenceof disease than in its absence. It can also bestated in another way that individuals who trulyhave LE were infinite times as likely to have apositive Mills as those who did not have LE. Withnegative likelihood ratio 0.47, the negative testis .47 times less likely to be made in thepresence of disease than in the absence of it.The individuals who actually have LE hadnegative mills examination 47% as often as
The purpose of this study was to ascertain thediagnostic value of the most widely usedprovocative tests i.e Cozen’s test, Mills test andMaudsley test in the diagnosis of lateralepicondylitis.The study results with Cozen’s test andMaudsley test indicate 84% sensitivity and 88%sensitivity respectively and 0% specificity .Thisinfers the ability of Cozen’s and Maudsley testto correctly identify subjects who do not havethe disease.Out of 30 subjects, 4 tested to benegative for lateral epicondylitis onmusculoskeletal ultrasonography and the abovetwo tests were unable to identify these 4 patientsas not having the disease but instead producedpositive results on testing. Whereas ,the abilityof the test to correctly identify subjects whohave the disease is 84% and 88% with respectto Cozen’s and Maudsley test. Out of the 26subjects who were diagnosed to have LE,Cozen’s test showed positive result for 22subjects and Maudsley showed positive for 23subjects.The diagnostic predictive value of Cozen’s andMaudsley failed to show a strong tendency.
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 822
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.
CONCLUSIONThe validation study on finding the diagnosticaccuracy of provocative tests in lateralepicondylitis highlighted that Cozen’s test andMaudsley test are better tests for ruling outlateral epicondylitis whereas Mills test is anexcellent diagnostic test for ruling in lateralepicondylitis.
1. Mohamed Waseem, S. Nuhmanib, C.S. Ramc andYadav Sachind.Lateral epicondylitis: A review of theLiterature. Journal of Back and MusculoskeletalRehabilitation 2012;25:131–142.
2. Christopher M Norris, Sports Injuries: Diagnosisand Management. 3rd edition, 2004.
3. Halle JS,Franklin RJ,Karalfa BL.Comparision of fourtreatment approaches for lateral epiocondylitis ofthe elbow.J Ortho Sports Phys Ther 1986;8(2):62-69.
4. Smidt N,Vander Windt DA,Assendelfl WJ,MouritsAJ,Devi l le WL,de Winter AF,BouterLM.Interaobserver reproducibil ity of theassessment of severity of complaints,gripstrength,and pressure pain threshold in patientswith Lateral Epicondylitis,Arch Phys Med Rehabil2002 Aug:83(8) :1145 – 50.
5. Vicenzino.B,Smith D,Cleland J,Bisset L.Developmentof cclinical prediction rule to identify intialresponders to movement with mobilisation andexercise for lateral epicondylalgis.Manualtherapy.220.oct;14(5):550-4.
6. Coonrad RW, Hooper WR. Tennis elbow: its course,natural history, conservative and surgicalmanagement.J Bone Joint Surg Am1973; 55-A: 1177-82.
7. Tuomo Pienimaki, Tuula Tarvainen,Pertti Siira, P,Antti Malmivaara,and Heikki Vanharanta.Associations Between Pain, Grip Strength, andManual Tests in the Treatment Evaluation ofChronic Tennis Elbow. The Clinical Journal of Pain18:164–170.
8. Robert G Max,Claire Bombardier, JamesG.Wright.What do we know about the reliability andvalidity of physical examination tests used toexamine the upper limb? The Journal of HandSurgery;1999Vol 24(1):185-193.
9. Joy C Mac Dermid, Susan L,Micholovitz. Examinationof the elbow: Linking diagnosis,prognosis andoutcomes as a framework for maximizing therapyinterventions.Journal of Hand Therapy; Apr 2006vol.19(2)82-97.
10. Joshua Cleland, Orthopaedic clinical examination:An evidence-based approach for physicaltherapist.2nd edition,2011.
11. Dayna Levin, Levon N. Nazarian, Theodore T. Miller,Patrick L. O’Kane, Rick I. Feld, Laurence Parker, JohnM. McShane.Lateral Epicondylitis of the Elbow: USFindings. Radiology 2005; 237:230–234.
12. Pravin Pati l and Bhaskar Dasgupta. Role ofdiagnostic ultrasound in the assessment ofmusculoskeletal diseases. Ther Adv MusculoskeletDis. 2012 October; 4(5): 341–355.
13. Serdar Tarhan, Zeliha Ünlü, Gülgün Yýlmaz Ovalý,Yüksel Pabuºçu. Value of Ultrasonography onDiagnosis and Assessment of Pain and GripStrength in Patients with Lateral Epicondylitis, TurkJ Rheumatol 2009; 24: 123-30.
those who did not have.The commonly used provocative tests in clinicalpractice are those that have both high sensitivityand specificity. A shoulder test with highpsychometric properties i.e Crank test, has 83%sensitivity and 100% specificity is reported tobe the most valid special test available indetermining shoulder labrum pathologies. Astudy in 2008 analyzed diagnostic accuracy ofClarke’s test in the diagnosis of chondromalaciapatella assigned sensitivity of 0.39, specificityof 0.67, likelihood ratio for a positive test was1.18, likelihood ratio for a negative test was0.91, positive predictive value was 0.25, andnegative predictive value was 0.80 was notrecommended for use as a diagnostic test forany patellofemoral syndromes as its diagnosticvalue deemed highly suspectible.15
Hence, the above study shows that Mills test ishighly significant for ruling in LE. If Mills test ispositive there are 100 % chances for theindividual of having the disease and therebyCozen’s and Maudsley have a high sensitivity ofruling out the lateral epicondylitis. But in thediagnosis of LE other variables such astenderness over lateral elbow, reduced painfulgrip strength are also significant measures forthe therspist for ruling in LE.The limitation of the study was a limited samplesize, pretest probability and post test probabilitywas not carried out. Further, a more precise toollike MRI can be used as a gold standard in thediagnosis of LE while musculoskeletalultrasonography could be used as an efficienttool in evaluating the efficacy of a therapeuticprogram.
Conflicts of interest: None
REFERENCES

Int J Physiother Res 2014;2(6):815-23. ISSN 2321-1822 823
G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACY OF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS.
How to cite this article:G Saroja, Antony Leo Aseer P, Venkata Sai P M. DIAGNOSTIC ACCURACYOF PROVOCATIVE TESTS IN LATERAL EPICONDYLITIS. Int J Physiother Res2014;2(6): 815-823. DOI: 10.16965/ijpr.2014.699
14. Donald D.Price,Pratricia A.McGrath,Amir Rafii andBarbara Buckingham(2003).The validation of visualanalogue scales as ratio scale measures for chronicand experimental pain.Pain;Volume 17,Issue 1,pp45-56.
15. Scott T. Doberstein; Richard L. Romeyn;David M.Reineke.The Diagnostic Value of the Clarke Sign inAssessing Chondromalacia Patella, Journal ofAthletic Training2008; 43(2):190–196.