interventional cardiology pre-procedure … do not use abbreviations: u, iu, ... admit as inpatient...
TRANSCRIPT

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME Baptist Cardiac & Vascular Institute Interventional Services
INTERVENTIONAL CARDIOLOGY PRE-PROCEDURE ORDERSReminder: Date, time all orders. Print name & ID # under signature.
1. Patient for procedure on (date): by Dr.: ______________________________________
2. Out-patient In-patient morning admit
3. Obtain the following consent(s) for:
Cardiac Catheterization
Percutaneous Coronary Intervention by Dr.: ____________________________________________
Transesophageal Echocardiogram
Patent Foramen Ovale Closure and/or Atrial Septal Defect Closure
Atrial Appendage Closure
Percutaneous Mitral Valve Repair
Blood or Blood Derivatives
Moderate Sedation (use consent form # 4446)4. The following to be obtained the day of the procedure: PT/INR aPTT BUN Creatinine Potassium BMP CBC EKG CXR PA/LAT Type and Screen Urine HCG if indicated Blood HCG if indicated Finger stick Glucose if indicated5. Start IV with 20 gauge catheter in left arm, unless left radial approach is involved and start fl uids of 0.9% NaCl at 100 ml/hour or choose from below.
IV fl uids: (Choose one and complete IP or OP times) 0.9% NaCl @75 ml/hour 0.9% NaCl @150 ml/hour 0.9% NaCl @200 ml/hour 0.9% NaCl @250 ml/hour
2nd IV with saline loc
IV fl uids not indicated
Inpatient: To start at ___________ AM / PM
6. NPO, continue all oral medications unless otherwise directed
7. Notify procedural physician with any concerns related to scheduled procedure.
8. Midazolam (Versed) 0.5 mg IV every 5 minutes, up to a total of 2 mg, as needed for anxiety, once patient is in procedure room. Hold midazolam dose(s) if Respiration Rate less than 12/minute, Systolic Blood Pressure less than 100 mmHg, or O2 Saturation less than 92%.
9. Premedicate with:
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
DO #43 Rev. 2/1307600BDO043
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Use black ballpoint pen. RM#

*02700B5140*
LEFT HEART CATHETERIZATION INDICATIONS
Page 1 of 3 ! Form #5140 (Rev. 6/12)
All patients must have a detailed written or transcribed history and note on the chart prior to procedure detailing the need for a cardiac catheterization.
Previous diagnosti c catheterizati on within 3 months? Yes Provide documentati on to support second procedure No Complete indicati ons worksheet below
ASY
MTO
MAT
IC
Rest or exercise-induced ECG abnormaliti es suggesti ng myocardial ischemia associated with other risk factors:
ST segment depression
Exercise-induced ST elevati on in leads other than aVr
Blunted SBP response during progressive exercise
Exercise-induced ventricular tachycardia
Stress Test
Abnormal myocardial perfusion study includes radiopharmaceuti cal distributi on compati ble with coronary ischemia:
Decreased distributi on in one or more vascular regions at rest or with exercise
Evidence of transient ischemic dilati on
Abnormal distributi on associated with increased lung uptake produced by exercise in the absence of severely depressed LVF at rest
Nuclear Stress Test
Abnormal radionuclide ventriculography where the LV EF falls during exercise or rest, and the fi ndings are suggesti ve of CAD.
Nuclear Stress Test
Abnormal echo global or regional LVF at rest or in response to pharmacologic or exercise stress testi ng.
Stress Echo Echo
SYM
PTO
MAT
IC
Post successful resuscitati on from cardiac arrest with reasonable suspicion of CAD.
Pati ent Record
Presence of atypical chest pain due to coronary spasm, or signs and symptoms of abnormal LVF.
H & P Pati ent Record
Angina associated with abnormal results of noninvasive cardiac testi ng suggesti ve of CAD.
Stress Test Stress Echo CTA
Angina inadequately responsive to medical treatment or prior interventi on (PTCA, thrombolyti c therapy, CABG).
H & P Pati ent Record
ACS including unstable angina, NSTEMI, and STEMI.
H & P Pati ent Record EKG Labs

LEFT HEART CATHETERIZATION INDICATIONS
Page 2 of 3 ! Form #5140 (Rev. 6/12)
SYM
PTO
MAT
IC
Complicated MI, with:
Ischemic chest pain, parti cularly when accompanied with ECG changes.
H & P EKG Labs
Suspected mitral regurgitati on or ruptured interventricular septum, parti cularly when accompanied with heart failure or shock.
Echo H & P Pati ent Record
Suspected sub-acute cardiac rupture (pseudoaneurysm).
Echo CT/MRI H & P Pati ent Record
Hemodynamic compromise or clinical heart failure.
H & P Pati ent Record
Post-MI angina, parti cularly when there is evidence of post-MI ischemia.
EKG H & P Pati ent Record Labs
Recurrent, potenti ally malignant ventricular arrhythmias.
EKG Pati ent Record Telemetry
Evidence of myocardial ischemia:
Abnormal blood pressure response or ventricular tachycardia on pre-discharge exercise stress testi ng
Abnormal lab testi ng or non-invasive cardiac tests
Pati ent Record Stress Test EKG Labs
Heart failure or signifi cantly decreased left ventricular EF associated with manifestati on of recurrent myocardial ischemia or signifi cant ventricular arrhythmias.
H & P Echo
Evaluati on for multi -vessel disease for prognosis and management.
Pati ent Record
PAST
MED
ICA
L H
ISTO
RYor
SUR
GIC
AL
CLE
AR
AN
CE
Prior to a high-risk surgery (major emergency surgery, aorti c and other major vascular surgery, peripheral vascular surgery) and anti cipated prolonged procedures associated with large fl uid shift s and/or blood loss.
Pati ent Record MD Notes
Considerati on for valve surgery, or existence of other valvular pathology in adult pati ent with chest discomfort or ECG changes, and at risk for CAD.
EKG Echo CT/MRI MD Notes
Planned correcti ve open heart surgery for congenital heart disease, and pati ent at risk for CAD.
Echo CT/MRI MD Notes Pati ent Record H & P
*02700B5140*

LEFT HEART CATHETERIZATION INDICATIONS
Page 3 of 3 ! Form #5140 (Rev. 6/12)
In Patient Only:
Justifi cation for procedure during this hospital admission:________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
_____________________________________________________________________________________________________
Physician Signature: ______________________________________________________________ Date: ________________
Print Name: _____________________________________________________________________ Time: ________________
PAST
MED
ICA
L H
ISTO
RY o
rSU
RG
ICA
L C
LEA
RA
NC
E
Evaluati on of pati ents with congenital heart disease who have signs or symptoms suggesti ng associated CAD.
EKG CT/MRI Echo Labs MD Notes
Suspected congenital coronary anomalies (congenital coronary artery stenosis, coronary arteriovenous fi stula, anomalous origin of left coronary aft ery) provided aortography is not diagnosti c.
CT/MRI Echo/TEE Previous aortography results
Diseases of aorta when knowledge of presence or extent of coronary artery involvement is necessary for management.
CT/MRI
Left ventricular failure without obvious cause.
Echo Stress Test CT/MRI
Pati ents with hypertrophic cardiomyopathy being evaluated for therapy of outf low tract obstructi on.
Echo
Presence or suspicion of heart neoplasms.
Chest X-ray Echo CT MR
Hemodynamic evaluati on of pulmonary hypertension.
MD Notes
*02700B5140*

DRAFT
DO NOT PLACE
IN CHART
*02700B5139*
RIGHT HEART CATHETERIZATION INDICATIONS
*02700B5139*Form #5139 (Rev. 8/12/14)
All patients must have a detailed written or transcribed history and note on the chart prior to procedure detailing the need for a cardiac catheterization.
Previous diagnostic catheterization within 3 months? Yes Provide documentation to support second procedure No Complete indications worksheet below
RIG
HT
HE
AR
T
£ Abnormal right ventricular function (right ventricular infarction, tricuspid regurgitation, ventricular septal defect).
Echo CT
£ Suspected pulmonary artery disease (e.g. pulmonary hypertension, pulmonary emboli, pulmonary vascular abnormalities).
CT VQ Scan Echo Chest X-ray H&P
£ Unexplained congestive heart failure, or right heart failure due to pulmonary hypertension or pulmonary interstitial disease.
CT Echo Chest X-ray
£ Suspected intracardiac shunt (e.g. atrial septal defect), ventricular septal defect, papillary muscle rupture, or pseudo aneurysms complicating an acute MI.
Echo CT
£ Abnormal findings from cardiac testing (e.g. echocardiogram) indicating right heart disease.
Echo
£ Cardiomyopathy.
Chest X-ray EKG Echo Stress Test
£ Clinically suspected or known valvular heart disease.
Echo
£ Known or suspected significant pericardial disease, myocarditis, or endocarditis.
Echo EKG Labs
£ Congenital heart disease affecting right heart.
Echo
In Patient Only: Justification for procedure during this hospital admission:__________________________________________
_____________________________________________________________________________________________________
Physician Signature: ______________________________________________________________ Date: ________________
Print Name: _____________________________________________________________________ Time: ________________

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TimE ACUTE mYOCARDiAL iNFARCTiON / UNSTABLE ANGiNA ACUTE CORONARY SYNDROmE ORDERS
Reminder: Date, time all orders. Print name & ID # under signature.1. Admit as inpatient to £ ICU £ CVS £ 4 CLARKE/4BCVI Telemetry
Attending: Place on the service of: ___________________________________________________
2. ACS Diagnosis: £ STEMI £ NON STEMI £ UNSTABLE ANGINA
3. Code status: (Complete the stratification order sheet as indicated) Please obtain advance directive if not previously done
4. Attach completed and signed “Telemetry and Arrhythmia Standing Orders” (DO # 111).
5. Cardiac telemetry monitor6. Vital signs as per unit protocol7. Height and weight on admission and daily weights before breakfast8. Oxygen to maintain O2 sat greater than 92%: £ 2 L /Nasal Cannula £ NRB Mask £ 4 L/NC
£ Simple Face mask £ Venturi Mask @ ______% £ Room Air
£ BIPAP settings _______________________________________________________________ £ Initiate Critical Care Mechanical Ventilation Protocol £ Initiate Critical Care Admission orders
9. £ Strict I & O every shift10. Diet: Keep NPO except meds until cleared by Cardiologist. £ NPO except meds £ Low saturated fat/ Low Cholesterol £ Calories: ________
£ 2 Gm Sodium £ Fluid restricted _____ ml per day £ Other: ___________ £ Dietician Consult11. IV Fluids: £ 0.45% NaCl £ D5W/0.45% NaCl £ IV 0.9% NaCl at _______ ml per hour
£ Saline Lock
£ Other: __________________________________________________________________
12. Activity: £ Bed Rest £ BSC £ BRP with assist as needed £ Ambulate as tolerated13. Notify Attending if: Chest pain, Heart rate greater than 120 bpm or less than 50 bpm, SBP greater than 170 mmHg or less than 90 mmHg, respiratory rate greater than 30 bpm or O2 Saturation less than 92%14. Labs: If NOT done in the ED: £ BMP or £ CMP £ CBC w'diff and Plts £ Troponin day 2 and day 3 £ Iron
£ Mg £ Ca £ Fasting Lipid Profile (within 24 hours of admission) £ TIBC £ PT/INR (if patient receiving warfarin) £ PTT (if patient treated with heparin/LMWH)
£ Other: __________________________________________________________________15. Diagnostic tests: £ ECG daily x 2 days for ACS £ ECG Stat for complaint of chest pain
Others: _______________________________ INDICATION: _______________________________
Others: _______________________________ INDICATION: _______________________________
*07600BDO400A*
p
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
SCANNED DATE: _______ TimE: _______ iNiTiALS: _______
Use black ballpoint pen. RM#
Page 1 of 3DO #400-A Rev. 6/12
07600BDO400A
STAT PHARmACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
SCANNED DATE: _______ TimE: _______ iNiTiALS: _______
p p
p pp

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TimE ACUTE mYOCARDiAL iNFARCTiON / UNSTABLE ANGiNA ACUTE CORONARY SYNDROmE ORDERS
Reminder: Date, time all orders. Print name & ID # under signature.mEDiCATiONS: ACC/AHA Guideline Class I Recommendations Indicated in Bold16. Beta blockers: £ metoprolol Tartrate (Lopressor) £ 12.5 mg £ 25 mg £ 50 mg PO every ___________________ (Hold for SBP less than ________ mmHg, heart rate less than ________) £ Carvedilol (Coreg) £ 3.125 mg £ 6.25 mg £ 12.5 mg £ 25 mg PO every 12 hours. (Hold for SBP less than _______ mmHg, heart rate less than _______.) Preferred if EF less than 40% £ Other: ____________________________________________________ £ Beta blocker not indicated or contraindicated. Please document reason in Progress Notes.
17. ACEi / ARB: Should be prescribed w/EF less than 40%. £ Lisinopril (Zestril): £ 5 mg £ 10 mg £ 20 mg £ 40 mg PO daily £ Losartan (Cozaar): £ 25 mg £ 50 mg £ 100 mg PO daily £ Other: _______________________________________________________________________ £ ACEI / ARB not indicated or contraindicated. Please document reason in Progress Notes.
18. Antiplatelet Therapy: £ Aspirin 81 mg x 4 PO if not previously given in ED/CATH-LAB £ Aspirin 81 mg PO daily £ coated £ non-coated £ Aspirin 325 mg PO daily £ coated £ non-coatedAND £ Clopidogrel (Plavix) 300 mg PO one time dose £ Clopidogrel (Plavix) 600 mg PO one time dose £ Clopidogrel (Plavix) 75 mg PO daily to start on _________ (Date)OR £ Prasugrel (Effient) 60 mg PO one time dose (Prescribed only by interventional cardiologists) £ Prasugrel (Effient) 10 mg PO daily. (Continue only if patient was taking at home)OR £ Ticagrelor (Brilinta) 180 mg PO one time dose £ Ticagrelor (Brilinta) 90 mg PO twice daily (Note: Maximum aspirin daily dose 81 mg)OR £ Other: ___________________________________
19. Anticoagulation Therapy: (check one) £ Heparin ACS Protocol: Complete order form DO #438 £ Enoxaparin (Lovenox) _____ mg (1 mg/kg) subcutaneous twice daily, if CrCl greater than 30 ml/min If CrCl less than 30 ml/min Lovenox _____ mg (1 mg/kg) subcutaneous daily £ Therapeutic anticoagulation not indicated. Complete VTE Prophylaxis Orders form DO #520
Use black ballpoint pen. RM#
Page 2 of 3DO #400-A Rev. 6/12
07600BDO400A
*07600BDO400A*
STAT PHARmACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
SCANNED DATE: _______ TimE: _______ iNiTiALS: _______

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TimE ACUTE mYOCARDiAL iNFARCTiON / UNSTABLE ANGiNA ACUTE CORONARY SYNDROmE ORDERS
Reminder: Date, time all orders. Print name & ID # under signature.21. Statin Therapy: £ Simvastatin (Zocor): £ 10 mg £ 20 mg £ 40 mg PO daily at bedtime £ Atorvastatin (Lipitor) 80 mg PO daily £ Rosuvastatin (Crestor): £ 5 mg £ 10 mg £ 20 mg £ 40 mg PO daily
22. Nitrates: £ Nitroglycerin 2% topical ointment __________ inch(es) applied topically four times daily. £ Nitroglycerin 0.4 mg SL every 5 min x 3 doses PRN for chest pain (Hold for SBP less than 100) £ Nitroglycerin ________ mcg / min IV
23. Analgesics: Morphine Sulfate: £ 1 mg £ 2 mg £ 3 mg £ 4 mg IVP x one for chest pain. Hold for SBP less than 100 mmHg. Call MD if pain is not relieved or returns within 4 hours.
24. Other Medications: __________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
_________________________________________________________________________________
25. £ Care Management: Indication ________________________________________________________
26. Consult:
£ Cardiology: Indication _____________________________ Doctor: _________________________
£ Nephrology: Indication ____________________________ Doctor: _________________________
£ Pulmonary: Indication _____________________________ Doctor: _________________________
£ Endocrinologist: Indication _________________________ Doctor: _________________________
£ Other:_______________________________________________________________________
27. Cardiac Rehab for patient and family education
28. Smoking cessation counseling
29. Please include detailed instructions on discharge.
Use black ballpoint pen. RM#
Page 3 of 3DO #400-A Rev. 6/12
07600BDO400A
*07600BDO400A*
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
STAT PHARmACYORDER(Place X in Box)
SCANNED DATE: _______ TimE: _______ iNiTiALS: _______

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TimE OrDErs fOr sT-sEgmENT ElEvATiON myOcArDiAl iNfArcTiON (sTEmi)
Reminder: Date, time all orders. Print name & ID # under signature.1. Admit as inpatient to £ ICU £ CVS £ 4 CLARKE/4BCVI Telemetry Attending: Place on the service of: ___________________________________________________
Activate STEMI Team by calling hospital operator.Start two (2) 18 gauge IV’s preferably in left arm, one with 0.9% NaCl to infuse at KVO and one saline lock, and avoid starting an IV in the right wrist and right hand.
Stat Labs/diagnostics: CBC, Chem 18, Total CPK, CPK MB, Troponin, PT/INR, aPTT, Lipid panel, EKG
Oxygen:
No arterial sticks
Medications: G clopidogrel (Plavix) 600 mg PO x 1.
OR G Ticagrelor (Brilinta) 180 mg PO x 1.
OR G Prasugrel (Effient) 60 mg PO x 1
G Aspirin 81mg x 4 PO chew and swallow if not administered by EMS.
G Only Heparin bolus 60 units / kilogram (Maximum dose: 4,000 units)*
Heparin IV bolus = _________ units * Note this is the only option
G Nitroglycerin drip 25 mg/250 ml D5W, start at 5 mcg/min and titrate as needed for relief of chest pain. Hold for Systolic BP less than 100. G morphine sulfate 2 mg IV every 5 - 15 minutes for a total of 10 mg as needed for chest pain. G Ondansetron (Zofran) 4 mg IV PRN x 1 for nausea/vomitingfor patients not immediately going for cardiac catheterization: G Tenectaplase (TNKase) IV over 5 seconds, based upon patient’s weight (see chart below). Max dose = 50 mg. After administration flush IV line with 10 mL of Normal Saline 0.9%.
*From one vial of TNKase reconstituted with 10 mL Sterile Water for Injection G Heparin Infusion Regimen A per Adult Intravenous Heparin Physicians Orders DO#438
DO #589 Rev. 12/1207600BDO589
*07600BDO589*
sTAT PHArmAcyOrDEr(Place X in Box)
scANNEDDATE: _______ TimE: _______ iNiTiAls: _______
Physician’s signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Use black ball point pen. RM#
Patient Weight (kg) Heparin Bolus50 kg or less 3000 units
51 - 60 3,300 units61 - 70 3,900 units
71 kg or more 4000 units
Cardiologist Signature: _____________________
Print Name: ______________________________
Date: _____________ Time: _________
Patient Weight (kg) TNKase® dose (mg) Volume TNKase*® to be adminstered (mL)Less than 60 30 6
60 to 69 35 770 to 79 40 880 to 89 45 9
90 and above 50 10

Absolute contraindications for use of Tenectaplase (TNKase): • Active internal bleeding • History of cerebrovascular accident • Intracranial or intraspinal surgery or trauma within past 2 months • Intracranial neoplasm, arteriovenous malformation, or aneurysm • Known bleeding diathesis • Severe uncontrolled hypertension
relative contraindications for use of Tenectaplase (TNKase): • Recent major surgery within the past two months.(e.g. coronary artery bypass graft, obstetrical delivery, organ biopsy, previous puncture of noncompressible vessels) • Cerebrovascular disease • Recent gastrointestinal or genitourinary bleeding • Recent trauma within the past two months • Hypertension (SBP above 180 mm Hg and/or DBP above 110 mm Hg) • High likelyhood of left heart thrombus • Acute pericarditis • Subacute bacterial endocarditis • Hemostatic heart defects, including those secondary to severe hepatic or renal disease • Severe hepatic dysfunction • Diabetic hemorrhagic retinopathy or other hemorrhagic opthalmic conditions • Septic thrombophlebitis or occluded AV cannula at seriously infected site • Advanced age • Patients currently receiving oral anticoagulants • Recent administration of GP IIb/IIIa inhibitors within the past 12 hours

*07600BDO400D*
DATE/TIME DOCTOR’S ORDERS
SUPPLEMENTAL DISCHARGE ORDERS: ACUTE MYOCARDIAL INFARCTION
1. Discharge patient:
2. Cardiac rehab for outpatient phase II:
3. Smoking counseling by Cardiac Rehab
4. Give patient discharge instructions from Micromedix: Acute Myocardial Infarctionor Acute Coronary Syndrome to patient
5. Follow up cholesterol testing with primary MD
ACC/AHA Recommended Medications:
ORDERED NOT indicated or(see Physician Contraindicated
Discharge Orders)
ASA G G
Beta Blocker G G
ACEI OR ARB G G
Statin G G
TRANSCRIBEDBY @ TIME
DOCTOR: PLEASE USE BALL POINT PEN - PRESS FIRMLY
STAT PHARMACYORDER(Place X in Box)
DO #400d (Rev. 1/06)
*07600BDO400d*
SCANNEDDATE: _______ TIME: _______ INITIALS: _______
Physician’s Signature _________________________________
Print Name: ________________________ I.D. #: _____________

STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME IMPELLA VENTRICULAR ASSIST DEVICE ORDER
Reminder: Date, time all orders. Print name & ID # under signature.INSTRUCTIONS:1. Admit to ICU
2. See post cath PCI orders for additional MD orders
3. Call ___________________________ for Impella problems. Call Abiomed clinical support (24/7) for help troubleshooting at: 1-888-215-8666
ACTIVITY:4. Complete bedrest. May logroll from side to side. May have HOB elevated up to 30 degrees only.DIET:5. Diet: £ NPO £ Clear liquids to cardiac diet advance as toleratedMONITORING:6. On arrival to Unit, assess vital signs, device assessment, and patient hemodynamic every 15 minutes X 4, every 30 minutes X 2, and then hourly while on Impella support.
7. Maintain Impella purge pressure between 300 and 700 mm Hg
8. Maintain pump performance (p-perf) to keep flow above _____ L/min
9. Document on Impella flow sheet every 1 hour: Performance level, Flow, Placement signal, Motor current, Pump position, Purge pressure, Infusion rate, and power source
10. Assess and document arterial access site and distal pulses every one hour while on Impella support.
LABS/DIAGNOSTIC STUDIES:11. On arrival to ICU: Plasma free hemoglobin, Creatnine, ABGs with ionized calcium, and CK, CKMB,
Troponin x 3 every 8 hours.12. Every 8 hours while on Impella support: plasma free hemoglobin, CBC, CMP, PT, PTT ABGs with
ionized calcium.
13. PTT per Heparin Protocol
14. Daily Portable chest x-ray while on support
15. Daily ECG while on Impella support
MEDICATIONS:16. Heparin Drip per DO #438: Regimen _______. Start drip @ _______ units/hour and titrate per protocol17. Purge fluid to Impella: 20% dextrose 500 ml with heparin 25,000 units. Change purge fluid and tubing
every 24 hours.18. SEDATION and PARALYSIS: Initiate DO #354 Sedation, Analgesic and Paralytic Order Form when
transferred to the ICU.
Use black ballpoint pen. RM#
*07600BDO759* DO #759 Rev. 5/1207600BDO759

*02400B5231*
TAVR PRE-PROCEDURE REVIEW
*02400B5231*Form #5231 (Rev. 4/13)
Patient Name: ____________________________________________ Outpatient / Inpatient: Room# ____________
Scheduled TAVR Date: ___________________________ Date Patient seen by: IC___________ CTS __________
Clinical Indication:______________________ STS Score: Risk of Mortality________ Morbidity or Mortality_______
Access Site: __________ Common femoral ___________ Common iliac ___________ External Iliac ____________
Anticipated Valve Size: _____________ Anticipated Sheath Size:_____________ Coronary Height:_____________
Annulus Measurement by: TTE__________ TEE__________ CT__________ Echo/CT Reader:________________
Transfemoral patient with Conduction Defect? Yes________ No________ If Yes, will require Pacing Swan_______
Transapical patient? Yes____________ No____________ If yes, will require Epicardial wires:_________________
Interventional Cardiologist:__________________________ Cardio-thoracic Surgeon: _______________________
Anesthesiologist:__________________________________ IVR/Vascular Surgeon: _________________________
Will patient be put on Cardiopulmonary bypass in the event of a complication? Yes__________ No _____________
Will patient undergo emergent Cardiac Surgery in the event of a complication? Yes__________No _____________
Unresolved issues/Anticipated problems: (i.e.: Aortic annulus size, difficulty expected in iliacs, horizontal aorta/heart)
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________________________________
Reviewed & Approved by TAVR Team: Interventional Cardiology: ____________________ ____________________
Cardio-thoracic Surgery: ____________________ ____________________
Anesthesia: ____________________
IVR/Vascular Surgery: ____________________ Date: _______________

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME PRE-PROCEDURE TRANSCATHETER AORTIC VALVE REPLACEMENT (TAVR) ORDERS
Reminder: Date, time all orders. Print name & ID # under signature.1. Patient for procedure on (date): by Drs.:
2. Out-patient In-patient morning admit
3. Obtain the following consent(s) for: Transcatheter Aortic Valve Replacement
Blood or Blood Derivatives Other: __________________________________________4. The following to be obtained day before procedure or day of procedure: PT/INR aPTT BUN Creatinine Potassium CBC BMP EKG CXR PA/LAT Type and Crossmatch 4 units of PRBC, 2 units of FFP and 2 adult doses of platelets
5. Urine HCG the day of procedure, if patient meets criteria
6. Fingerstick glucose the day of procedure if patient is diabetic
7. Start IV with a 20 gauge catheter and begin: Lactated Ringers or 0.9% NaCI at _______ mL/hr.
8. Patient instructed to be NPO after midnight and continue all oral medications unless otherwise directed.
9. Patient instructed to take clear liquids until ________ (time), then NPO. Continue all other oral medications unless otherwise directed.
10. Hold diuretics and metformin day of procedure.
11. Notify procedural physician with any concerns related to scheduled procedure.
12. • First dose of antibiotic to be given within 60 minutes prior to incision or within 120 minutes for vancomycin. • Prophylactic antibiotics continued for more than 24 hours after surgery end time must have a justifi cation noted in the medical record.
Surgery Type Recommended Pre-Operative Antimicrobials Penicillin Allergy
CARDIAC HIGH RISK CABG, prosthetic valve
Less than or equal to 100 kg: Cefazolin (Ancef) 2 gm IV x 1 dose + Vancomycin 1 gm IV x 1 dose
Greater than 100 kg: Cefazolin (Ancef) 2 gm IV x 1 dose + Vancomycin 1.5 gm IV x 1 dose
Less than or equal to 100 kg: Vancomycin 1 gm IV x 1 dose + Gentamicin 4 mg/kg IV (max dose 400 mg)
Greater than 100 kg: Vancomycin 1.5 gm IV x 1 dose + Gentamicin 4 mg/kg IV (max dose 400 mg)
13. Premedicate with:
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Use black ballpoint pen. RM#
DO #895 Rev. 2/1307600BDO895
SCANNED DATE: _______ TIME: _______ INITIALS: _______

*07600BDO868*
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME POST STRUCTURAL HEART PROCEDURE ORDERS
Reminder: Date, time all orders. Print name & ID # under signature. (please check all which apply): G Atrial Septal Defect Closure G Patent Foramen Ovale Closure G Ventricular Septal Defect Closure G Atrial Appendage Closure G Percutaneous Mitral Valve Repair G Perivalvular Leak Closure
G Other: ___________________________________________________________________________
1. £ Outpatient procedure, discharge home when stable
£ Outpatient procedure with planned overnight recovery, transfer to: £ Women’s services 2 EM/1EL £ Med/Surg floor £ Short Stay £ 3 Main £ 2 Clarke £ Peds £ Other:_______________________________________________
£ Inpatient procedure or emergency procedure performed. Admit as inpatient to:_____________________________________
£ Return to pre-procedure level of care ______________________________________________________________________
£ Place in observation—unexpected need for extended monitoring following outpatient procedure.
Reason: _________________________________________________ Attending physician: _________________________
£ Admit as inpatient for complication of outpatient procedure.
Diagnosis: ______________ _______________________________ Admitting physician: ___________________________
2. Diagnosis/Procedure:
3. Diet: G NPO, except Medications G Advance as tolerated to: _______________________________ G Clear Liquids
4. CLOSURE METHOD HEMOSTASIS INSTRUCTIONS: G Vascular Hemostasis Device: Bedrest for ___________ hours with accessed leg straight then ambulate patient with assistance and monitor access site for any signs of bleeding/hematoma. OR G Manual Pressure: Bedrest for ______ hours with accessed leg straight after femoral sheath is removed. Ambulate patient with assistance and monitor access site for any signs of bleeding/hematoma. OR G Figure-of-Eight Stitch: Remove figure-of-eight stitch with a sterile suture removal kit from: G Right and/or G Left groin in __________ hours and apply a sterile band-aid to site. Bedrest for ___________ hours after stitch is removed and then ambulate patient with assistance Monitor access site for any signs of bleeding/hematoma.(please check all which apply):
5. G Post-procedure assessment: Vital signs to include extremity pulses and puncture site check every 15 minutes x 1 hour, every 30 minutes x 2 hours, every 1 hour x _______ hour(s) , then routine for unit.
6. G Call Dr. ______________________________ and gallery if any sign of bleeding (BCVI ext. 56991).
Use black ball point pen. RM#
Page 1 of 4DO #868 Rev. 1/14
07600BDO868

STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 2 of 4DO #868 Rev. 1/14
07600BDO868
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME POST STRUCTURAL HEART PROCEDURE ORDERS
(please check all which apply):
7. G IV Fluids: ________________ at __________ mL/hour x _______hours, then convert to saline lock.
8. G Sequential compression device to lower extremities while patient is in bed.
9. G EKG now and the morning.
10. G Daily weights in the morning.
11. G CXR PA & LAT by 8:00 am.
12. G 2D Echo/Doppler by 8:00 am. G Bedside.
13. G Notify Dr. ___________________________ if pericardial drainage is greater than 30 mL/hr. Best rest while pericardial catheter in place. (Atrial Appendage Closure Procedures. 2D Echo must be done prior to catheter removal.)
Time of lastpre-op/intra-op dose:
______________
MEDICATIONS:14. Antibiotics: Last dose not to exceed 24 hours from pre-op/intra-op dose G Cefazolin (Ancef) 1 gm IVPB every 8 hours for a total of 2 doses if the patient is not allergic to Penicillin. OR G Clindamycin (Cleocin) 600 mg IVPB every 8 hours for a total of 2 doses if the patient is allergic to Penicillin.15. Antiplatelet therapy G Aspirin _______ mg PO x 1 dose now G Aspirin _______ mg PO daily G coated G non-coated to start on _________________ (Date) G Clopidogrel (Plavix) _______ mg PO x 1 dose now G Clopidogrel (Plavix) 75 mg PO daily to start on _________________ (Date)
16. G Antiemetic: G Metoclopramide (Reglan) 10 mg IV every 6 hours PRN nausea and vomiting if CrCl is greater than 40 mL/min. G Ondansetron (Zofran) 4 mg IV every 6 hours PRN nausea and vomiting.17. G Pain medication: G Acetaminophen (Tylenol) 650 mg PO every 6 hours PRN pain (Maximum 3 grams per day). G Hydromorphone (Dilaudid) 0.5 mg – 1 mg IV every 4 hours PRN moderate to severe pain.
18. G Additional Medications: _______________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
__________________________________________________________________________________
Use black ball point pen. RM#
*07600BDO868*

STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 3 of 4DO #868 Rev. 1/14
07600BDO868
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME POST STRUCTURAL HEART PROCEDURE ORDERS
(please check all which apply):
19. G Labs: G aPTT, K+, Total CPK and CPK MB, CBC, at ____ am/pm. Call interventionalist if Platelets less than 100,000. G K+, Total CPK and CPK MB, CBC, BUN and Creatinine in AM at 0600.
20. G Fingerstick blood sugar post procedure if patient is diabetic.
21. G Call Hospitalist for medication orders.
22. G Other: ____________________________________________________________________________
23. Consult Cardiothoracic surgeon Dr.__________________________. Patient to be seen prior to discharge.
24. Discontinue urinary catheter 6 hours post procedure
Use black ball point pen. RM#
*07600BDO868*

STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 4 of 4DO #868 Rev. 1/14
07600BDO868
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME VTE PROPHYLAXIS FOR MEDICAL AND SURGICAL PATIENTSFor medical patients must start within 24 hours of admission.For surgical patients must start within 24 hours post-op or reason documented.
£ Early ambulation for all patients when possible, with assistance if necessary. See activity order.
£ No Chemical VTE Prophylaxis needed Reason:______________________________ £ No Mechanical VTE Prophylaxis needed Reason:______________________________
Chemical Prophylaxis:
£ Already on therapeutic anticoagulation or secondary VTE prophylaxis£ Chemical prophylaxis contraindicated. £ Active bleeding/Risk of bleeding £ Other:____________________________Start Anticoagulation: £ 8 hours post op £ 12 hours post op Surgery end time:____________ £ 24 hours post rt-PA (Activase) if no blood seen on 24 hours follow-up CT Brain – confirm with physician£ Fondaparinux (Arixtra) 2.5 mg SubQ every 24 hours (Contraindicated in Patient with CrCl less than 30 mL/min or Actual Body Weight less than 50 kg)£ Enoxaparin (Lovenox) 40 mg SubQ every 24 hours£ Enoxaparin (Lovenox) 30 mg SubQ every 24 hours (for CrCl 15- 30 mL/min)£ Heparin 5000 units SubQ every £ 8 hours £ 12 hoursMay use one of the following alternative regimens if applicable. £ Post op hip or knee replacement patients ONLY: Rivaroxaban (Xarelto) 10 mg PO once daily (Do not use in patients with CrCl less than 30 mL/min)£ Post op knee replacement patients: Enoxaparin (Lovenox) 30 mg SubQ every 12 hours.£ Post op Bariatric Surgical patients: Enoxaparin (Lovenox) 40 mg SubQ every 12 hours
Monitoring orders for patients on chemical prophylaxis:
Baseline CBC, Serum Creatinine, aPTT and PT/INR CBC every 48 hours x 5 days or until discharged, if soonerBleeding precautions
Mechanical Prophylaxis:
Intermittent Pneumatic Compression Devices:£ Calf £ Above Knee£ Both legs £ Left only £ Right only£ VFP (Venous Foot Pumps) £ Right foot £ Left foot £ Both feet£ Mechanical prophylaxis contraindicated. Reason_________________________________________.
*07600BDO868*

NOT A PART OF THE PERMANENT MEDICAL RECORD
CONTRAINDICATIONS TO PHARMACOLOGIC PROPHYLAXISRelative• History of cerebral hemorrhage • Craniotomy within 2 weeks • GI, GU hemorrhage within the last 6 months • Thrombocytopenia (symptomatic) • Coagulopathy • Active intracranial lesions and Intracranial/
spinal lesion /neoplasms/monitoring devices • Diabetic Retinopathy • Vascular access/biopsy sites inaccessible to hemostatic control • Spine Surgery
Absolute• Active hemorrhage • Heparin or Enoxaparin (Lovenox) use in patients
with heparin- induced thrombocytopenia • Severe trauma to head, spinal cord or extremities with hemorrhage within the last 4 weeks • Thrombocytopenia (platelets less than 20 K/
microliter) • Coagulopathy (INR greater than 2)• Presence of an epidural catheter

ADULT INTERVENTIONAL SERVICES CONTRAST INDUCED NEPHROPATHY RISK ASSESSMENT TOOL
*01200B5104*Form #5104 (Rev. 6/12)
Elective Add-On Emergent NA-Dialysis Pt Scheduled Procedure: ________________________ Date of Service: ___________Contrast Allergy: No Yes If yes, Pre-Med Orders (DO #638) obtained: Yes No If No, rationale: ____________________________________________________________________________________________________ Current Meds include: NSAIDS ACE Inhibitor Metformin NA Contrast within 72 hours: Yes No Pre- Procedure Assessment:
Creatinine:___________ mg/dL eGFR:________ ml/min/1.73 m2 (eGFR calculator @ www.kidney.org)
eGFR less than or equal to 50 ml/min/1.73 m2; Cr greater than 1.5 in diabetic; greater than 1.7 non-diabetic: CIN Prophylaxis Orders (DO#540): Yes No If No, rationale: ________________________________________
Maximum Contrast Volume = Weight (kg): ______ x 5 ÷ Creatinine: ______ mg/dL = ______ Max Contrast Volume (Not to exceed 300 ml) (In patients with eGFR less than 60 ml/min/1.73 m2 a contrast volume less than 100 ml is preferred)
Post Procedure Assessment:
RISK FACTORS √ SCORE
Age greater than 75 years ______ 4
Diabetes ______ 3
CHF III/IV ______ 5
Anemia (HCT less than 39 men / less than 36 women) ______ 3
Serum Creatinine greater than 1.5 mg/dL ______ 4 OReGFR less than 60 ML/min/1.73 m2 ______ 2 for 40 - 60
______ 4 for 20 - 39
______ 6 for less than 20
Hypotension SBP less than 80 mmHg (current) ______ 5
IABP ______ 5
Contrast Volume ______ 1 for every 100 ML
SCORE ______ greater than 6 Post-proc hydration orders Yes No
If No, rationale: ________________________________________ (Recommend 0.9 NS @ 1 ml/kg x 12 hour or 3 ml/kg x 6 hours if patient can tolerate)
SCORE RISK OF CIN % RISK OF DIALYSIS %
less than or equal to 5 7.50 % 0.04 %
6 - 10 14.00 % 0.12 %
11 - 15 26.10 % 1.09 %
greater than or equal to 16 57.30 % 12.60 %
Follow-up instructions for repeat Creatinine and hold meds indicated: Yes No
RN Signature: __________________________________ Print Name:____________________________ Date:__________ Time:________
RN Signature: __________________________________ Print Name:____________________________ Date:__________ Time:________
RN Signature: __________________________________ Print Name:____________________________ Date:__________ Time:________

DRAFT
DO NOT PLACE
IN CHART
*07600BDO540*
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
DO #540 Rev. 9/1407600BDO540
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04DATE TIME CONTRAST NEPHROPATHY PROPHYLAXIS ORDER
Reminder: Date, time all orders. Print name & ID # under signature.ü Check all that apply
G A. NaCL IV Hydration Patient’s weight _________ kg G Infuse 0.9% NaCl, 1 mL/kg/hr IV X ______ hours prior to procedure and continue for 12 hours post-procedure. (recommend to begin infusion 12 hours prior to procedure) OR G Infuse 0.9 % NaCl IV bolus of 250 mL over 30 minutes, immediately prior to procedure and immediately after contrast medium given, infuse 0.9% NaCl at 3 mL/kg/hr IV X 6 hours.
G B. Sodium Bicarbonate IV Therapy Patient’s weight _________ kg • Pharmacy to prepare Na Bicarbonate 154 mEq/L in 846 mL D5W (total volume 1000 mL) • Infuse at the following rates into a dedicated IV site. • Bolus with 3 mL/kg/hour 1 hour prior to procedure. See table below • Then start infusion at 1 mL/kg/hr intra procedure and 6 hours post procedure, then discontinue.
G C. Acetylcysteine (Mucomyst): Use in conjunction with either choice A or B above 600 mg PO BID x 4 doses – Starting on Date: _____________ Time:__________
G D. Other: ____________________________________________________________________ __________________________________________________________________________Discontinue any metformin or metformin containing medications post contrast administration. � For inpatients, verify with attending physician if metformin or metformin containing medication can be restarted 48 hours post contrast after renal function has been re-evaluated. � For outpatients: G Instruct patient to restart metformin or metformin containing medication 48 hours post contrast administration G Instruct patient to contact: G Surgeon G Endocrinologist G Primary Care Physician G Other physician: _________________________________ in 48 hours post contrast administration to verify if metformin or metformin containing medication can be restarted.
Use black ballpoint pen. RM#
Patient’s weight 3 mL/kg IV Bolusover 1 hour
1 mL/kg/hr X 6 hourinfusion
less than 65 kg 180 mL 360 mL (60 mL/hr)65 – 69 kg 200 mL 390 mL (65 mL/hr)70 – 74 kg 215 mL 420 mL (70 mL/hr)75 – 79 kg 230 mL 450 mL (75 mL/hr)80 – 84 kg 245 mL 480 mL (80 mL/hr)85 – 89 kg 260 mL 510 mL (85 mL/hr)90 – 94 kg 275 mL 540 mL (90 mL/hr)95 – 99 kg 290 mL 570 mL (95 mL/hr)
100 – 104 kg 305 mL 600 mL (100 mL/hr)105 – 110 kg 320 mL 630 mL (105 mL/hr)
greater than 110 kg 330 mL 660 mL (110 mL/hr)
APPROVED BY BHSF P&T
DO #723 Rev. 4/09
07600BDO723
*07600BDO723*
STAT PHARMACYORDER(Place X in Box)
SCANNEDDATE: _______ TIME: _______ INITIALS: _______
Physician’s Signature: _________________________________________________ Date:____________ Time:__________
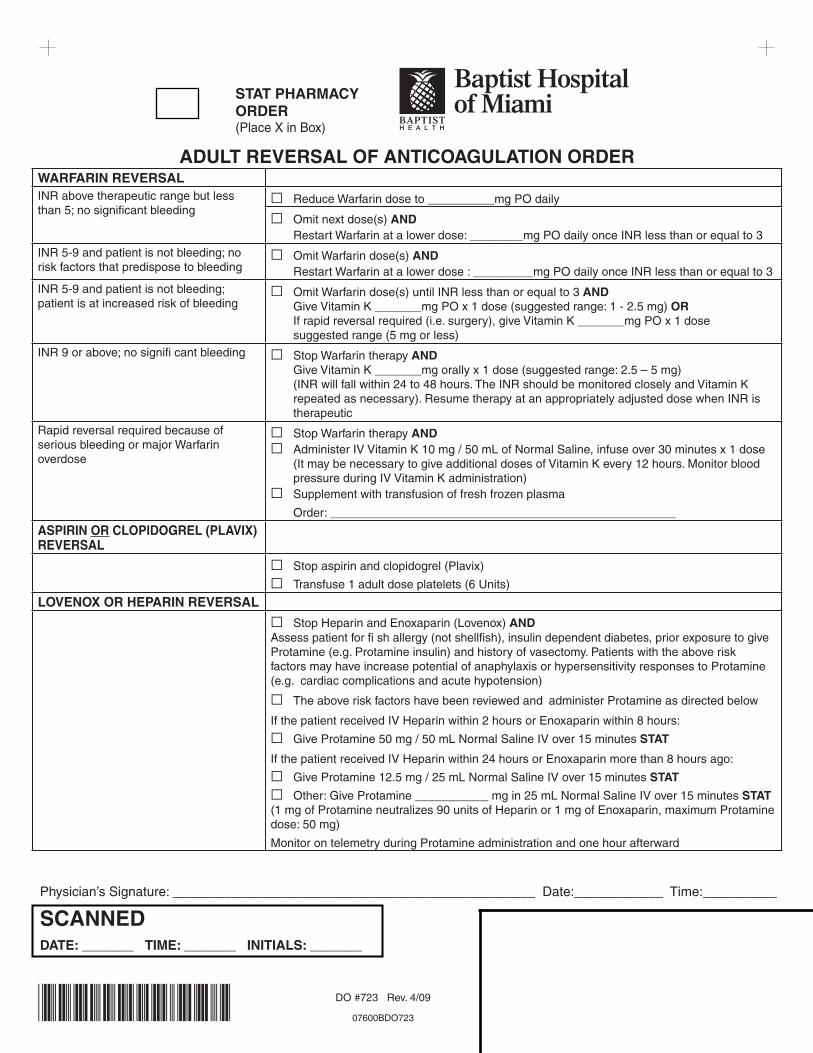
ADULT REVERSAL OF ANTICOAGULATION ORDERWARFARIN REVERSALINR above therapeutic range but lessthan 5; no significant bleeding
G Reduce Warfarin dose to __________mg PO daily
G Omit next dose(s) AND Restart Warfarin at a lower dose: ________mg PO daily once INR less than or equal to 3
INR 5-9 and patient is not bleeding; norisk factors that predispose to bleeding
G Omit Warfarin dose(s) AND Restart Warfarin at a lower dose : _________mg PO daily once INR less than or equal to 3
INR 5-9 and patient is not bleeding;patient is at increased risk of bleeding
G Omit Warfarin dose(s) until INR less than or equal to 3 AND Give Vitamin K _______mg PO x 1 dose (suggested range: 1 - 2.5 mg) OR If rapid reversal required (i.e. surgery), give Vitamin K _______mg PO x 1 dose suggested range (5 mg or less)
INR 9 or above; no signifi cant bleeding G Stop Warfarin therapy AND Give Vitamin K _______mg orally x 1 dose (suggested range: 2.5 – 5 mg) (INR will fall within 24 to 48 hours. The INR should be monitored closely and Vitamin K repeated as necessary). Resume therapy at an appropriately adjusted dose when INR is therapeutic
Rapid reversal required because ofserious bleeding or major Warfarinoverdose
G Stop Warfarin therapy ANDG Administer IV Vitamin K 10 mg / 50 mL of Normal Saline, infuse over 30 minutes x 1 dose (It may be necessary to give additional doses of Vitamin K every 12 hours. Monitor blood pressure during IV Vitamin K administration)G Supplement with transfusion of fresh frozen plasma
Order: ____________________________________________________
ASPIRIN OR CLOPIDOGREL (PLAVIX)REVERSAL
G Stop aspirin and clopidogrel (Plavix)
G Transfuse 1 adult dose platelets (6 Units)
LOVENOX OR HEPARIN REVERSAL
G Stop Heparin and Enoxaparin (Lovenox) ANDAssess patient for fi sh allergy (not shellfish), insulin dependent diabetes, prior exposure to giveProtamine (e.g. Protamine insulin) and history of vasectomy. Patients with the above riskfactors may have increase potential of anaphylaxis or hypersensitivity responses to Protamine (e.g. cardiac complications and acute hypotension)
G The above risk factors have been reviewed and administer Protamine as directed below
If the patient received IV Heparin within 2 hours or Enoxaparin within 8 hours:
G Give Protamine 50 mg / 50 mL Normal Saline IV over 15 minutes STAT
If the patient received IV Heparin within 24 hours or Enoxaparin more than 8 hours ago:
G Give Protamine 12.5 mg / 25 mL Normal Saline IV over 15 minutes STAT
G Other: Give Protamine ___________ mg in 25 mL Normal Saline IV over 15 minutes STAT(1 mg of Protamine neutralizes 90 units of Heparin or 1 mg of Enoxaparin, maximum Protaminedose: 50 mg)
Monitor on telemetry during Protamine administration and one hour afterward

DO #638 Rev. 6/11
07600BDO638
*07600BDO638*
DATE TIME
STAT PHARMACYORDER(Place X in Box)
SCANNEDDATE: _______ TIME: _______ INITIALS: _______
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
DOCTOR’S ORDER SHEET RM#(PLEASE USE BLACK
BALL POINT PEN)
Physician’s Signature ________________________________
Print Name: ________________________ I.D. #: ___________
Pre-medication for allergy to: IODINATED CONTRAST MEDIA GADOLINIUM BASED CONTRAST MEDIA
If patient can tolerate oral intake:1. ___ Methylprednisolone (Medrol) 32 mg PO 12 hours and 2 hours prior to contrast injection
2. ___ Diphenhydramine (Benadryl) 50 mg PO 1 hour prior to contrast injection
If patient cannot take oral medications:1. ___ Hydrocortisone (Solu-Cortef) 200 mg IV 12 hours and 2 hours prior to contrast injection
OR ___ Methylprednisolone (Solu-Medrol) 40 mg IV 12 hours and 2 hours prior to contrast injection
2. ___ Diphenhydramine (Benadryl) 50 mg IV 1 hour prior to contrast injection
Emergent:1. ___ Hydrocortisone (Solu-Cortef) 200 mg IV every 4 hours prior to contrast injection
OR ___ Methylprednisolone (Solu-Medrol) 40 mg IV every 4 hours prior to contrast injection
2. ___ Diphenhydramine (Benadryl) 50 mg IV 1 hour prior to contrast
Other medications as per ordering physician:
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04

DO #640 Rev. 9/1007600BDO640
STAT PHARMACYORDER(Place X in Box)
SCANNEDDATE: _______ TIME: _______ INITIALS: _______
CODE:C = CONSULT CALLEDMAK/MAR = MEDICATION ADMINISTRATION RECORDSS = SLIP SENTMS = MESSAGE SENT
ALLERGIES:G SCANNED
Print Physician’s Name: ___________________________________________________
Physician’s Signature: ____________________________ Date:_________ Time:______
Day INR Dosage (PO)
Starting Date (Day 1) less than 1.51.5 – 1.9
greater than 1.9
5 mg2.5 mgCall MD
2 less than 1.51.5 – 1.92 – 2.5
greater than 2.5
5 mg2.5 mg1 mg
Hold dose, notify MD, discontinue protocol
3 less than 1.51.5 – 1.9
2 – 3greater than 3
7.5 mg5 mg
2.5 mgHold dose, notify MD, discontinue protocol
4 to 7 days until INR 2-3for 2 consecutive days
less than 1.51.5 – 1.9
2 – 3greater than 3
10 mg7.5 mg5 mg
Hold dose, notify MD, discontinue protocol
DATE TIME ADULT WARFARIN (COUMADIN®) INITIATION ORDER INR GOAL = 2-3
Warfarin Nomogram
1. Do not use this form if goal INR is greater than 3 or if patient is on Argatroban.
2. If patient has epidural catheter contact Anesthesia prior to initiation of therapy for approval
3. Place patient on bleeding precautions
4. Indication for Warfarin _________________________________________________ Goal INR 2 – 3 (Deep venous thrombosis, Pulmonary Embolism, Atrial Fibrillation, Tissue Heart Valve, Valvular Heart Disease, Mechanical Valve in aortic position)
5. Baseline CBC with platelets, PT/INR, within previous 48 hours prior to Warfarin administration. Call MD if INR greater than 1.9.
6. Obtain PT/INR daily, draw labs in AM.
7. Obtain CBC every 48 hours x 3.
8. Day 1: Initiate Warfarin Nomogram below. Administration of Warfarin should be at 14:00 each day as directed. If after 14:00, give now then follow up doses at 14:00 next day thereafter.
9. Initiate Warfarin teaching.
10. When INR 2 – 3 for two consecutive days: a. Contact prescribing physician for further labs and maintenance Warfarin dosing b. Contact physician to discontinue Heparin, Lovenox, Arixtra or Refl udan if patient is receiving these medications concurrently.
11. Discharge plans: G Refer to anticoagulation clinic G Plan for out-patient transition to primary care physician for daily monitoring G Arrange for post hospital discharge lab monitoring.

DRAFT
DO NOT PLACE
IN CHART
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME ADULT INTRAVENOUS HEPARIN PHYSICIANS ORDERDo not use this form for ischemic stroke unless specified by physician (see DO #401)
Reminder: Date, time all orders. Print name & ID # under signature.Allergies: _________________________________ Current Actual Weight: ___________ kg (2.2 pounds = 1 kg)
1. Discontinue all previous orders for heparin, low molecular weight heparin (i.e. enoxaparin (Lovenox®)), fondaparinux (Arixtra®). Contact physician if patient is on dabigatran (Pradaxa®), rivaroxaban (Xarelto®), apixaban (Eliquis®) or warfarin (Coumadin® or Jantoven®).2. BASELINE LABS: Obtain baseline CBC AND PTT if not already done within previous 48 hours prior to IV heparin administration. 3. Place patient on bleeding precautions. Monitor for signs and symptoms of bleeding. Please see Bleeding Precautions Policy (GPR 78).
4. Avoid intramuscular (IM) injections during heparin infusion.
5. Notify anesthesia if epidural catheter is present.
6. Epidural catheter removal must occur greater than 6 hours after last dose of heparin.
7. Administer heparin IV bolus and initial infusion using the table on page 2.
8. Use only a premixed preparation of heparin (25,000 units in 500 mL = 50 units/mL).
9. Notify physician if platelet count drops by more than 50% from baseline or is less than 100,000/mm3.
Follow-up LAB orders: 10. Obtain PTT at baseline & at 6 hours after initiation of heparin and when specified in dosing adjustment algorithm tables.11. Continue to check PTT every 6 hours (adjusting rate using tables provided) until TWO consecutive values are between 47 – 62 seconds for Regimen A or between 63 – 102 seconds for regimens B & C.
12. Obtain once daily PTT when dosage no longer requires adjusting.
13. Obtain daily CBC while on heparin infusion.
14. Heparin orders (please choose appropriate regimen below), and indicate if no loading dose is desired:
£ Regimen A - Acute Coronary Syndrome WITH Thrombolytics or GP IIb/IIIa inhibitors Loading dose: 60 units/kg (Maximum dose: 4,000 units) £ No Loading dose Initial Infusion dose: 12 units/kg/hour (Maximum initial infusion dose: 1,000 units/hour)
£ Regimen B - Acute Coronary Syndrome WITHOUT Thrombolytics or GP IIb/IIIa inhibitors Loading dose: 70 units/kg (Maximum dose: 5,000 units) £ No Loading dose Initial Infusion dose: 15 units/kg/hour (Maximum initial infusion dose: 1,000 units/hour)
£ Regimen C - Deep Venous Thrombosis (DVT), Pulmonary Embolism (PE) or any indication requiring full anticoagulation (i.e. Atrial Fibrillation) Loading dose: 80 units/kg (Maximum dose: 5,000 units) £ No Loading dose Initial Infusion dose: 18 units/kg/hour (Maximum initial infusion dose: 1,300 units/hour)
*07600BDO438*
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Use black ballpoint pen.
RM#
Page 1 of 2DO #438 Rev. 6/14
07600BDO438
SCANNED DATE: _______ TIME: _______ INITIALS: _______
APPROVED BY BHSF P&T

DRAFT
DO NOT PLACE
IN CHART
Use the following dose adjustment algorithm as per the PTT value after the initial infusion above: Dosing Adjustment Algorithm (Regimen A) Dosing Adjustment Algorithm (Regimen B & C)
PTT(seconds)
Re-BolusIVP (units)
Hold Drip(minutes)
ChangeDrip
RepeatPTT
PTT(seconds)
Re-BolusIVP (units)
Hold Drip(minutes) Change Drip Repeat PTT
46 or less 0 0
+ 100 units/hour (+ 2 mL/hour)
6 hours 46 or lessRepeatinitial
loading dose**
0 + 200 units/hour(+4 mL/hour) 6 hours
47 – 62 0 0 No changeSee order
#11 OR #12on page 1***
47 – 62 0 0 + 100 units/hour(+2 mL/hour) 6 hours
63 – 102 0 30 minutes
- 100 units/hour (- 2 mL/hour)
6 hours 63 – 102 0 0 No changeSee order
#11 OR #12on page 1***
103 orgreater 0 60
minutes-200 units/hour (- 4 mL/hour)
6 hours 103 – 125 0 30 minutes - 100 units/hour(- 2 mL/hour) 6 hours
* indicates maximum bolus or infusion rate regardless of weight** If no initial bolus ordered, contact physician*** Repeat PTT in 6 hours if 1st PTT level within goal range; repeat PTT next day if 2 consecutive PTT levels within goal range
126 or greater 0 60 minutes - 200 units/hour
(- 4 mL/hour) 6 hours
*07600BDO438*
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 2 of 2DO #438 Rev. 6/14
07600BDO438
SCANNED DATE: _______ TIME: _______ INITIALS: _______
APPROVED BY BHSF P&T
STAT PHARMACYORDER(Place X in Box)
REGIMEN A REGIMEN B REGIMEN C
PATIENTWEIGHT
(kgs)
Acute Coronary SyndromeWITH
Thrombolytics or GP llb/llla inhibitors
Acute Coronary SyndromeWITHOUT
Thrombolytics or GP llb/llla inhibitors
Any Indication RequiringFull Anticoagulation
(i.e. DVT, PE, and Atrial Fibrillation)
Initial Loading Dose: 60 units/kgMaximum Initial Loading Dose:
4,000 units
Initial Loading Dose: 70 units/kgMaximum Initial Loading Dose:
5,000 units
Initial Loading Dose: 80 units/kgMaximum Initial Loading Dose:
5,000 units
Initial Infusion Dose: 12 units/kg/hourMaximum Initial Infusion Dose:
1,000 units/hour
Initial Infusion Dose: 15 units/kg/hourMaximum Initial Infusion Dose:
1,000 units/hour
Initial Infusion Dose: 18 units/kg/hourMaximum Initial Infusion Dose:
1,300 units/hour
Heparin Bolus Heparin Infusion Heparin Bolus Heparin Infusion Heparin Bolus Heparin Infusion50 or less 3,000 600 units/hour 3,500 750 units/hour 4,000 900 units/hour
51 - 60 3,300 650 units/hour 3,800 800 units/hour 4,400 1,000 units/hour
61 - 70 3,900 750 units/hour 4,500 950 units/hour 5,000* 1,100 units/hour
71 - 80 4,000* 900 units/hour 5,000* 1,000 units/hour* 5,000* 1,300 units/hour*
81 - greater 4,000* 1,000 units/hour* 5,000* 1,000 units/hour* 5,000* 1,300 units/hour*

POLICY NO.: BCVI-200-4020-200.328 TYPE: Departmental
All references to Policies must go to the BHSF Master Copy on the BHSF Intranet; do not rely on other versions / copies of the Policy.
Page 1 of 2
POLICY TITLE: Management of Acute Reactions to Iodinated Contrast Media Responsible Department: Interventional Services Creation Date: 1/95 Review Date: 12/04/14 Revision Date: 12/04/14 SUBMITTED BY (AUTHOR): Debra Denny, MS, RN Title: Patient Care Manager APPROVED BY: Alex Powell, MD Title: Medical Director of Interventional Services APPROVED BY: Ramon Quesada, MD Title: Medical Director, Interventional Cardiology APPROVED BY: Efrain Gonzalez, MD Title: Medical Director, Electrophysiology Lab APPROVED BY: Jane Kiah, MS, RN Title: Director of Invasive Services APPROVED (Released): 12/04/2014
SUMMARY & PURPOSE: This policy is intended to provide guidance on the appropriate management of a patient exhibiting signs and symptoms of a contrast agent reaction. POLICY: This policy serves as a guideline for the management of a patient with a reaction to iodinated contrast agents. Supportive Data: There are three types of contrast allergies:
Cutaneous and mucosal manifestations.
Smooth muscle and minor anaphylactoid responses.
Cardiovascular and major anaphylactoid responses. All patients will be interviewed by the physician and nurse pre-procedure for history of iodinated contrast agent allergies which will be documented in the medical record. If the patient verbalizes a history of allergic reaction to contrast, the physician will order the appropriate medication and or hydration to be completed before the procedure if indicated. Confirmation of pre-treatment will be performed and documented before the start of the procedure. Full emergency resuscitation equipment, as well as trained personnel should be available during the procedure. SCOPE/APPLICABILITY: All IVS Registered Nurse personnel are expected to adhere to this policy.
POLICY NO.: BCVI-200-4020-200.328 TYPE: Departmental
All references to Policies must go to the BHSF Master Copy on the BHSF Intranet; do not rely on other versions / copies of the Policy.
Page 2 of 2
PROCEDURES TO ENSURE COMPLIANCE: The Registered Nurse will continuously assess the patient during and after the procedure in the recovery phase for signs and symptoms of contrast allergy including the following: 1. Mild to Moderate Reaction:
a. Nausea, Vomiting: i. Observe the patient and give assurance that this reaction is transient. ii. Assess for patent IV site. iii. Administer anti-emetic under direction of Physician. iv. Continuous hemodynamic monitoring.
b. Urticaria: i. Observe the patient and give assurance that this reaction is transient. The urticaria may be localized
or generalized. ii. Assess for a patent IV site. iii. Administer Dipenhydramine 25-50mg IM/IV under the direction of the Physician. iv. Continuous hemodynamic monitoring. Oxygen may be ordered by Physician.
2. Moderate to Severe Anaphylactic Reaction:
a. Bronchospasm: i. Observe the patient and give assurance. ii. Wheezing is usually present in this reaction. iii. May administer oxygen at 2-3L/ nasal cannula. iv. May administer Epinepherine 1:1000 subcutaneously or for an accelerating severe reaction,
Epinepherine 1:10,000, 1-3ml intravenously under the direction of a Physician. v. May administer corticosteroids under the direction of the Physician. vi. Prepare for potential intubation. vii. Continuous hemodynamic monitoring.
b. Hypotension: i. Observe the patient and give assurance. ii. Normal sinus rhythm or compensatory tachycardia may be present. iii. May administer oxygen at 2-3L/ nasal cannula. iv. May open up the IV fluids. v. May elevate the patient’s legs. vi. If bradycardia is present, the Registered Nurse may administer Atropine 0.5-1.0mg IV under the
direction of the Physician. vii. Continuous hemodynamic monitoring.
The Registered Nurse will complete a Reportable Incident Report on line. The patient’s chart will reflect an allergy to contrast and the type of contrast. The patient, when stable, will be informed that he/she has had a contrast media reaction. Instruct the patient to report this reaction when questioned about allergies. Apply an allergy band to the patient. SUPPORTING/REFERENCE DOCUMENTATION: Kern, Morton J., 1999. The Cardiac Catheterization Handbook. 3rd Ed. Mosby, St. Louis. Pg. 560 RELATED POLICIES, PROCEDURES, AND ASSOCIATED FORMS: N/A ENFORCEMENT & SANCTIONS: Violations of this policy may lead to revocation of system privileges and/or disciplinary action including termination. Anyone willfully violating this policy will be subject to disciplinary action up to and including termination.








DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
PATIENT LABEL
DATE/TIME TRANSCRIBEDBY @ TIME POST-CORONARY INTERVENTION ORDERS
(Please check all orders which apply):
1. £ Outpatient procedure, discharge home when stable
£ Outpatient procedure with planned overnight recovery, transfer to:
£ Short Stay £ 4 Clarke £ Other: ________________________________________
£ Place in observation—unexpected need for extended monitoring following outpatient procedure.
Reason: _____________________________ Attending physician: ___________________
£ Return to pre-procedure nursing unit
£ Admit as inpatient for complication of outpatient procedure to: £ ICU £ CVS
£ 4 Clarke £ 4 BCVI £ Other___________________________________________
Diagnosis: ___________________________ Admitting physician: ___________________
£ Inpatient procedure or emergency procedure performed. Admit as inpatient to: £ ICU
£ CVS £ 4 Clarke £ 4 BCVI £ Other__________________________________
2. £ Telemetry (Complete “Adult Telemetry Arrhythmia Orders” DO #111)
3. £ Pressure lines to continuous monitor.
4. £ Check vital signs, access site and extremity pulses, every 15 minutes x 4, every 30 minutes x 4, every 1 hour x 4, then every 4 hours and PRN.
5. £ EKG now and in A.M.
6. £ Monitor lead __________________________________________________________
7. £ EKG STAT for chest pain and call Interventional Cardiologist on the case and
_______________________________ .
8. £ Notify procedure physician & BCVI (BCVI ext. 56991) of any signs of bleeding.
9. £ Maintain femoral venous line KVO.
10. £ IV Fluids of ______________________________ at __________ mL/hr x ________ hrs., then convert to saline lock or remove if being discharged home.
11. £ Obtain ACT and/or PTT at ____________. Trained personnel to remove lines when ACT less than 200 or PTT less than 40. Repeat ACT or PTT every 1 hour until above parameters are achieved.
£ Medication for sheath removal: Fentanyl (Sublimaze) 25 mcg IV every 5 minutes up to 50 mcg prior to sheath removal
12. £ FemoStop to £ RIGHT or £ LEFT groin at __________ mm Hg x __________ after hemostasis obtained with hand held pressure.
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 1 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
DATE/TIME TRANSCRIBEDBY @ TIME POST-CORONARY INTERVENTION ORDERS
(Please check all orders which apply):
13. CLOSURE METHOD HEMOSTASIS INSTRUCTIONS: £VASCULAR HEMOSTASIS DEVICE: Bedrest for: _______ hours. Then immediately ambulate patient with assistance and monitor access site for any signs of bleeding/hematoma. OR £MANUAL PRESSURE: Bedrest for: _______ hours after femoral sheath is removed. Then immediately ambulate patient with assistance and monitor access site for any signs of bleeding/hematoma. OR £RADIAL APPROACH: Bedrest for: _______ hours. Compression band to £ RIGHT or £ LEFT wrist at present tension x _______ hours then slowly release and wean off band over the next ____ hours. Monitor thumb of accessed wrist with pulse oximetry until hemostasis achieved, if no bleeding/hematoma remove band. Check wrist for bleeding/hematoma and capillary refill with vital signs. Discontinue pulse oximetry when hemostasis has been achieved. Apply band-aid to access site when the band is removed. Then immediately ambulate patient with assistance and monitor access site for any signs of bleeding/hematoma.
14. £ If indwelling urinary catheter is present post procedure, remove on: _____________________ before POD#2. (DATE/TIME)
15. £ Bedrest, may have head of bed elevated 30 degrees-may increase to 45 degrees for meals.
16. £Patient may be discharged SAME DAY 1 hour after bedrest hours are complete and if: • Vital signs are stable • No hematoma; no bleeding from access site • Labs within baseline range for patient • Patient ambulates without difficulty • Smoking cessation counseling completed • Patient received invasive cardiac procedure discharge instructions
OR
17. £Patient may be discharged in AM if: • Vital signs are stable • No hematoma; no bleeding from access site • Labs within baseline range for patient • Patient ambulates without difficulty • Smoking cessation counseling completed • Patient received invasive cardiac procedure discharge instructions
PATIENT LABEL
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 2 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
DATE/TIME TRANSCRIBEDBY @ TIME POST-CORONARY INTERVENTION ORDERS
(Please check all orders which apply):
MEDICATIONS:18. £ Do not restart Nitroglycerin drip £ Nitroglycerin drip 25 mg in 250 mL (0.1mg/mL) D5W at _____ micrograms/min, titrate to keep systolic blood pressure (BP) less than _____ greater than ______ £ Begin to wean Nitroglycerin drip 5 - 10 micrograms every 10 minutes at _______ (time) until Nitroglycerin is off and patient is chest pain free and systolic BP less than _______.
19. GP IIb/IIIa inhibitors £ Eptifibatide (Integrilin) Bolus dosing: (2 mg/mL vial) £ 180 microgram/kg IV bolus (Max: 11.3 mL) Dose: _________ £ Percutaneous Coronary Intervention (PCI) Repeat bolus dose ten minute after first bolus dose Continuous infusion: (0.75 mg/mL vial) **CrCl: _________ (mL/min) **Patients with CrCl equal to or greater than 50 mL/min £ 2 microgram/kg/min (Max: 20 mL / hr) X ________ (hrs) **Non-dialysis dependent patients with CrCl less than 50 mL/min £ 1 microgram/kg/min (Max: 10 mL / hr) X ________ (hrs) **Cockcroft-Gault equation: CrCl = {(140 – Age) x (IBW in Kg) / 72 x (SCr)} x 0.85 for females OR £ Abciximab (Reopro) Bolus dosing: (2 mg/mL vial) £ 0.25 mg/kg IV bolus x 1 (Max: 18.5 mL) Dose: _________ Continuous infusion: (9 mg in 250 mL 0.9% NACL or D5W) £ 0.125 microgram/kg/min (Max: 17 mL / hr) X ______ (hrs)
20. Antiplatelet therapy: £ Discontinue all previous antiplatelet therapy £ Regimen A Aspirin ______ mg PO X 1 dose now Aspirin ______ mg PO daily £ coated £ non-coated to start on _________ (Date) Clopidogrel (Plavix) ______ mg PO X 1 dose now Clopidogrel (Plavix) 75 mg PO daily to start on _________ (Date) OR £ Regimen B: Aspirin ______ mg PO one time dose Aspirin ______ mg PO daily £ coated £ non-coated to start on ___________ (Date) Prasugrel (Effient) ______ mg PO one time dose Prasugrel (Effient) ______ mg PO daily to start on __________ (Date)continued on next page
PATIENT LABEL
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 3 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
DATE/TIME TRANSCRIBEDBY @ TIME POST-CORONARY INTERVENTION ORDERS
(Please check all orders which apply):
OR £ Regimen C: Aspirin ______ mg PO X 1 dose now Aspirin 81 mg PO daily £ coated £ non-coated to start on _____________ (Date) Ticagrelor (Brilinta) ______ mg PO one time dose Ticagrelor (Brilinta) 90 mg PO twice daily start __________ (Date/Time) (Note: Maximum aspirin daily dose 81 mg)21.£ Do not restart heparin drip. £ Restart heparin drip at _________ (time). (Complete “Intravenous Heparin Order Form”- DO# 438)
22. £ Do not restart enoxaparin (Lovenox) £ Restart enoxaparin (Lovenox) on ___________________ (date) ______________ (time) at ______ mg/kg subQ every ______ hours for ______ days23. Oral pain medications: £Acetaminophen (Tylenol) 650 mg PO every 6 hours PRN for Pain. (Maximum 3 grams per day).
£Other: __________________________________________________ PRN for Pain.24. Antiemetic £Metoclopramide (Reglan) 10 mg IV every 6 hours PRN for nausea and vomiting if CrCl is greater than 40 mL/min £Ondansetron (Zofran) 4 mg IV every 6 hours PRN for nausea and vomiting
25. £ For patients with CrCl greater than or equal to 30 mL/min.
IF K+ is 3.5 – 3.8 mmol/L, give KCL 20 mEq IV X 2 doses. If venous sheath is discontinued, give KCL 20 mEq PO X 2 doses.
IF K+ is less than 3.5, give KCL 20 mEq IV X 3 doses. If venous sheath is discontinued, give KCL 20 mEQ PO X 3 doses. £ For patients with CrCl less than 30 mL/min or if urine output is less than 20 mL/hr
IF K+ is 3.5 – 3.8 mmol/L, give KCL 10 mEq IV X 2 doses. If venous sheath is discontinued, give KCL 10 mEq PO X 2 doses.
IF K+ is less than 3.5, give KCL 10 mEq IV X 3 doses. If venous sheath is discontinued, give KCL 10 mEQ PO X 3 doses
26. £ Other medication(s): _____________________________________________________ ______________________________________________________________________ ______________________________________________________________________27. £ K+, Total CPK, CPK MB and CBC at ______ a.m./p.m.
Call £ Interventional cardiologist OR £ Dr. ___________________ if platelets less than 100 K/ul.
PATIENT LABEL
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 4 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
DATE/TIME TRANSCRIBEDBY @ TIME POST-CORONARY INTERVENTION ORDERS
(Please check all orders which apply):
28. £ K+, Total CPK, CPK MB, CBC, BUN and Creatinine in A.M. at 0600.29. Post PCI cardiac enzymes / troponin reporting criteria:
£ Please call interventional cardiologist with abnormal cardiac enzymes / troponin results.
OR £ Please do NOT call interventional cardiologist with abnormal and / or critical cardiac enzymes / troponin results, as this is expected.
30.£ Fingerstick blood sugar post procedure if patient is diabetic. (Complete “Subcutaneous Insulin Order Form”-DO #512).31. Oxygen via NC at ______ l/min. £ Other:______________________________________
32. Diet: £ NPO except medications £ Clear liquids
£ Advance as tolerated to: ___________________. £ Encourage PO fluids
33. £ Cardiac Rehabilitation Consult (call EXT. 66564 and place order in Net Access)
34. Add PCI interventional cardiologist as a consulting physician
PATIENT LABEL
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 5 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
STAT PHARMACYORDER(Place X in Box)
PATIENT LABEL
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Page 6 of 6DO #141 Rev. 6/17/14
07600BDO141
SCANNED DATE: _______ TIME: _______ INITIALS: _______
Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME POST-CORONARY INTERVENTION ORDERSFor medical patients must start within 24 hours of admission.For surgical patients must start within 24 hours post-op or reason documented.
VTE PROPHYLAXIS FOR MEDICAL AND SURGICAL PATIENTS£ Early ambulation for all patients when possible, with assistance if necessary. See activity order.
£ No Chemical VTE Prophylaxis needed Reason:______________________________ £ No Mechanical VTE Prophylaxis needed Reason:______________________________
Chemical Prophylaxis:
£ Already on therapeutic anticoagulation or secondary VTE prophylaxis£ Chemical prophylaxis contraindicated. £ Active bleeding/Risk of bleeding £ Other:_____________________Start Anticoagulation: £ 8 hours post op £ 12 hours post op Surgery end time:____________ £ 24 hours post rt-PA (Activase) if no blood seen on 24 hours follow-up CT Brain – confirm with physician£ Fondaparinux (Arixtra) 2.5 mg SubQ every 24 hours (Contraindicated in Patient with CrCl less than 30 mL/min or Actual Body Weight less than 50 kg)£ Enoxaparin (Lovenox) 40 mg SubQ every 24 hours£ Enoxaparin (Lovenox) 30 mg SubQ every 24 hours (for CrCl 15- 30 mL/min)£ Heparin 5000 units SubQ every £ 8 hours £ 12 hoursMay use one of the following alternative regimens if applicable. £ Post op hip or knee replacement patients ONLY: Rivaroxaban (Xarelto) 10 mg PO once daily (Do not use in patients with CrCl less than 30 mL/min)£ Post op knee replacement patients: Enoxaparin (Lovenox) 30 mg SubQ every 12 hours.£ Post op Bariatric Surgical patients: Enoxaparin (Lovenox) 40 mg SubQ every 12 hours
Monitoring orders for patients on chemical prophylaxis:
Baseline CBC, Serum Creatinine, aPTT and PT/INR CBC every 48 hours x 5 days or until discharged, if soonerBleeding precautions
Mechanical Prophylaxis:
Intermittent Pneumatic Compression Devices:£ Calf £ Above Knee£ Both legs £ Left only £ Right only£ VFP (Venous Foot Pumps) £ Right foot £ Left foot £ Both feet£ Mechanical prophylaxis contraindicated. Reason_________________________________________.
Use black ballpoint pen. RM#
*07600BDO141*

DRAFT
DO NOT PLACE
IN CHART
NOT A PART OF THE PERMANENT MEDICAL RECORD
CONTRAINDICATIONS TO PHARMACOLOGIC PROPHYLAXISRelative• History of cerebral hemorrhage• Craniotomy within 2 weeks• GI, GU hemorrhage within the last 6 months• Thrombocytopenia (symptomatic)• Coagulopathy• Active intracranial lesions and Intracranial/
spinal lesion /neoplasms/monitoring devices• Diabetic Retinopathy• Vascular access/biopsy sites inaccessible to
hemostatic control• Spine Surgery
Absolute• Active hemorrhage• Heparin or Enoxaparin (Lovenox) use in patients
with heparin- induced thrombocytopenia• Severe trauma to head, spinal cord or extremities with hemorrhage within the last 4 weeks • Thrombocytopenia (platelets less than 20 K/
microliter)• Coagulopathy (INR greater than 2)• Presence of an epidural catheter

INTERVENTIONAL SERVICES
Radial Access Protocol
Contraindications:
Contraindication to radial access for interventional procedures includes single artery circulation to the hand determined by an Allen test. An abnormal Allen test is blood flow return to the hand delayed more than 7 seconds.
Procedure:
1. Operator to perform an Allen test assessment. Determine if normal or abnormal. If normal, proceed to the next step. If abnormal, cancel radial access procedure.
2. May perform ultrasound to assess artery diameter for sheath.
3. Operator to enter artery with a 21-gauge thin wall needle.
4. After the artery is cannulated, advance a 0.025 inch guidewire through the needle
5. A 4-, 5-, 6-, 7-, or 8-Fr introducer sheath is inserted.
6. Administer the “Radial Access Cocktail” as follows;
► Without Nitroglycerin:
1. In a 10 ml syringe prepare: Verapamil 2.5 mg (1 ml) 0.9% Normal Saline 9 ml
2. Heparin Sodium, 50 units/kg IV bolus
► With Nitroglycerin:
1. In a 10 ml syringe prepare: Verapamil 2.5 mg (1 ml) Nitroglycerin 200 mcg (2 ml) 0.9% Normal Saline 2 ml
2. Heparin Sodium, 50 units/kg IV bolus
3. Nitroglycerin 0.4 mg sublingual x 1 tab.
7. Apply radial artery compression band with 12-15 ml of air x 30 to 60 minutes.
8. Wean compression band by decreasing pressure in small increments over 30 minutes. Check for signs of bleeding or hematoma. Reapply if indicated.

M
Dosing Guidelines for Moderate Sedation -ADULTS
Drug Dose Onset/Duration Monitoring/Comments Diazepam (Valium)
IV: 2.5 mg in increments, (not to exceed 5 mg per single dose over 60 seconds). (individual response is variable.) Do not dilute with saline or H20 Do not mix with other drugs Reduce dose of narcotic by a third
when used with diazepam; reduce diazepam dose by 30-50% in elderly.
Onset: 30 seconds to 2 minutes (may take up to 5 min) Duration: 60 – 180 mins (may last up to 4 hours); sedative effects usually last for 3 hours
Administer into a large vein; monitor airway, 02 sats and HR. Titrate to slurring of speech. Contraindicated in untreated narrow-angle glaucoma; irritating to veins-may cause phlebitis, thrombosis, and local inflammation. Avoid in pregnant women, esp. during first trimester.
Midazolam (Versed) Healthy, Adults < 60
IV: 0.5 to 2.5 mg over at least 2 minutes. Repeat in 2 minutes, if needed, in small increments of initial dose over at least 2 minutes to achieve desired effect. Overall dose 2.5-5 mg. Elderly: Initial dose 0.5 mg slow IV, give no more than 1.5 mg over 1 minute period, waiting another 2 minutes to evaluate sedative effect. Total dose >3.5 mg is rarely necessary. Titrate with small increments allowing 2 minutes after each dose to evaluate effect. Once sedation is achieved, additional doses should be 25% of the dose required to produce the sedative endpoint; for maintenance, use 0.25 mg to 1 mg. Total dose: usually < = 5 mg Reduce dose by 30% if patient was premedicated with a narcotic or other CNS depressant.
Onset: 1.5 to 5 minutes Duration: 2 to 6 hours. Recovery usually occurs within 2 hours, but effects may last as long as 6 hours.
Titrate to slurred speech. Monitor airway, oxygen saturation, HR. Contraindicated in acute narrow-angle glaucoma. May potentiate adverse effects of opioids - including respiratory depression - when used in combination. Reduce dose in patients with compromised renal or hepatic dysfunction. Avoid use with alcohol, St. John’s Wort, Valerian, Kava-Kava, and gotukola. May increase CNS depression BP monitoring required during IV administration.
Midazolam (Versed) Adults > 60; debilitated or chronically ill
IV: Initial dose 0.5 mg slow IV, give no more than 1.5 mg over 1 minute period, waiting another 2 minutes to evaluate sedative effect. Total dose >3.5 mg is rarely necessary. Usual max total dose: 3.5 mg Reduce dose by 50% if patient was premedicated with a narcotic or other CNS depressant.
Onset: 1.5 to 5 minutes Duration: 2 to 6 hours. Recovery usually occurs within 2 hours, but effects may last as long as 6 hours.
Titrate to slurred speech. Monitor airway, oxygen saturation, HR. Contraindicated in acute narrow-angle glaucoma. May potentiate adverse effects of opioids - including respiratory depression - when used in combination. Reduce dose in patients with renal or hepatic dysfunction.
Pentobarbital (Nembutal) Alternative for benzodiazepine Allergy
IV: 50 – 100 mg at a rate no greater than 50mg/min to prevent hypotension and respiratory depression. May repeat in 2 minutes to achieve sedation endpoint. PO: 150 – 200 mg in divided doses. If desire repeat, consider IV to titrate effect.
Onset: PO = 20 mins; IV = 15 sec Duration: PO = 1-4 H; IV = 15 min
Titrate to slurred speech. Contraindicated in patients with hypersensitivity to barbiturates or porphyria or with severe respiratory disease when dyspnea or obstruction is evident. Use cautiously in geriatric or debilitated patients.

Moderate Sedation Self Study Packet 16
Dosing Guidelines for Moderate Sedation - ADULTS
Drug Dose Onset/Duration Monitoring/Comments Meperidine (Demerol) Pure opioid agonist
IV: Dilute to achieve concentration of 10mg/mL and administer 12.5 – 25 mg over 2 minutes. May repeat incremental dose at 2 minute intervals to achieve desired endpoint for sedation. Do not exceed 200 mg in 1 H. Do not exceed 600 mg. over 24 hour period. (It’s 1/10 as potent as morphine) Reduce dose in elderly or debilitated patients.
Onset: 5 min Duration: 2 – 4 H
Titrate to slurred speech. Contraindicated in patients with hypersensitivity to the drug and in those who have received an MAO inhibitor within the past 14 days. Use cautiously in geriatric or debilitated patients and in those with respiratory conditions (COPD, asthma). More nausea/vomiting versus morphine. Normeperidine, a metabolite of meperidine is a CNS endotoxin. Patients with compromised renal function are particularly at risk. Meperidine should not be used for more than 48 hours for acute pain or at a dose greater than 600 mg/ 24 hours.
Morphine Pure opioid Agonist
IV: Dilute to achieve concentration of 1mg/mL. Administer 1 or 2 mg over 1 to 2 min. May repeat incremental dose at 5 minute intervals to achieve desired endpoint for sedation. Usual max total dose: 10 mg/24 hours. Reduce dose in elderly or debilitated patients.
Onset: 5 min Duration: 4 – 5 H
Titrate to slurred speech and Ramsay Score of 3. Monitor respiratory rate and depth continuously; respiratory depression may occur. Be prepared to assist ventilation. Contraindicated if drug allergy; use cautiously in elderly and debilitated patient. Hypotension is possible especially if the patient is hypovolemic. Nausea and vomiting may occur. Less nausea/vomiting versus meperidine.
Fentanyl (Sublimaze) Opioid Analgesic
IV: 25 mcg to 50 mcg up to 150 mcg .
Slow IV administration over 2 minutes.
Onset: 1 – 2 min Duration: 30 – 60 min
Titrate to slurred speech. Monitor respiratory rate and depth continuously; respiratory depression may occur. Crosses the blood brain barrier quickly. With rapid administration, can cause skeletal muscle and chest wall rigidity impairing ventilation. More sedative effects when compared with morphine. Shorter acting when compared to morphine. Less hypotension compared to morphine and Demerol.

Moderate Sedation Self Study Packet 17
Dosing Guidelines for Moderate Sedation - PEDIATRICS
Drug Dose Onset/Duration Monitoring/Comments Diazepam (Valium)
IV: 0.1 to 0.15 mg/kg over 60 seconds. May repeat incremental doses to achieve desired sedation endpoint. Do not exceed 1-2 mg per minute IV. Do not exceed 0.25mg/kg Do not dilute with saline or H20 Do not mix with other drugs Reduce narcotic dose by a third when
used with diazepam;
Onset: 30 seconds to 2 minutes (may take up to 5 min) Duration: 60 – 180 mins (may last up to 4 hours); sedative effects usually last for 3 hours
Administer into a large vein; monitor airway, 02 sats and HR. Titrate to slurring of speech. Contraindicated in untreated narrow-angle glaucoma; irritating to veins-may cause phlebitis, thrombosis, and local inflammation.
Midazolam (Versed)
PO: Syrup, age > 6 months: 0.25 – 0.5 mg/kg as a SINGLE DOSE given 30-45 minutes before a procedure. IV - Dilute to 0.1 mg/ml < 6 months old: 0.025 – 0.05 mg/kg over at least 2 minutes. Higher risk for airway obstruction and aspiration. 6 months to 5 years: 0.05 to 0.1 mg/kg over at least 2 min. Titrate carefully, usual max dose 6 mg. 6 – 12 years: 0.025 – 0.05 mg/kg over at least 2 min. Titrate carefully, usual max dose 10 mg. 12 – 16 years: Same as adult, but use incremental dosing. Titrate carefully, usual max dose 10 mg. IV Only: Repeat doses in 2 minutes, if needed, in small increments of initial dose over at least 2 minutes to achieve desired endpoint. Titrate with small increments allowing 2 minutes after each dose to evaluate effect. Once sedation is achieved, additional doses should be 25% of the dose required to produce the endpoint Reduce dose by 30% if patient was pre-medicated with a narcotic or other CNS depressant.
Onset: 1.5 to 5 minutes Duration: 2 to 6 hours. Recovery usually occurs within 2 hours, but effects may last as long as 6 hours.
Titrate to slurred speech. Monitor airway, oxygen saturation, HR. Contraindicated in acute narrow-angle glaucoma. May potentiate adverse effects of opioids - including respiratory depression - when used in combination. Reduce dose in patients with renal or hepatic dysfunction. Avoid use with alcohol, St. John’s Wort, Valerian, Kava-Kava, and gotukola. May increase CNS depression
Chloral Hydrate Moderate Sedation Dose Oral or Rectally: 50-75 mg/kg/dose 30 to 60 minutes prior to a procedure. May repeat dose in 30 mins to a total max dose of 120 mg/kg or 1000 mg total.
Onset: 30 to 60 min Duration: 4-8 hours
May cause disorientation, excitement, delirium drowsiness, ataxia, “hangover” Contraindicated in patients with marked hepatic or renal impairment; severe cardiac disease; gastritis; hypersensitivity or idiosyncrasy to chloral derivatives.

Moderate Sedation Self Study Packet 18
Dosing Guidelines for Moderate Sedation - PEDIATRICS Drug Dose Onset/Duration Monitoring/Comments
Meperidine (Demerol)
Pure opioid agonist
IV: Dilute with NS or H20 to a concentration of 5 mg/ml Administer 1 to 1.5 mg/kg over 2 to 3 minutes. May repeat dose to achieve desired endpoint.
IM/SC: 1 to 2 mg/kg 30-90 minutes prior to a procedure.
Max dose: 100 mg.
Onset: 5 min
Duration: 2 – 4 H
Onset: 10-15 min
Titrate to slurred speech.
Contraindicated in patients with hypersensitivity to the drug and in those who have received an MAO inhibitor within the past 14 days.
Use cautiously in patients with respiratory conditions (COPD, asthma). More nausea/vomiting versus morphine.
Not for long term use or with renal failure due to accumulation of normeperidine (metabolite).
Morphine
Pure opioid Agonist
IV: Dilute with NS or H20 to achieve concentration of 0.5 mg/ml. Administer 0.05 – 0.1 mg/kg over 3 to 5 min. May repeat incremental dose at 5 minute intervals to achieve desired endpoint for sedation.
PO: 0.3 mg/kg
Reduce dose if used with a benzodiazepine.
Onset: 5 min
Duration: 4 – 5 H
Onset and duration may be longer in PO
Titrate to slurred speech. Monitor respiratory rate and depth continuously; respiratory depression may occur. Be prepared to assist ventilation.
Contraindicated if drug allergy; use cautiously in debilitated patient.
Hypotension is possible especially if patient is hypovolemic. Nausea and vomiting may occur. Less nausea/vomiting versus meperidine.

Moderate Sedation Self Study Packet 19
Dosing Guidelines for Moderate Sedation REVERSAL AGENTS - ADULT AND PEDIATRICS
Drug Dose Onset/Duration Monitoring/Comments Flumazenil
(Romazicon)
For Benzodiazepine
Reversal
ADULT IV: 0.2 mg over 15 seconds. If patient does not reach desired level of consciousness after 45 sec, repeat dose. Dose may be repeated at 1 min intervals until a cumulative dose of 1 mg has been given. Dose may be repeated after 20 minutes if re-sedation occurs, but no more than 1 mg should be given at one time. Do not exceed 3 mg in 1 hour.
0.1 to 0.2 mg increments in opioid dependent patients and in post op patients to avoid large cardiovascular changes.
PEDIATRIC IV: 0.01 mg/kg given IV over 15 seconds (up to 0.2 mg total dose). May repeat the dose at 1 minute intervals until desired endpoint is reach or up to 5 total doses of 0.01 mg/kg. Maximum dose is 0.05 mg/kg or 1 mg, whichever is lower.
Onset: immediate
Duration:
Initial half-life: 7 – 15 min
Terminal half-life: 41 – 79 min
Benzodiazepine antagonist.
Use has been associated with occurrence of seizures. Monitor for recurrence of sedation. Monitor ventilation, HR, O2 sats.
NOTE: The effects of Flumazenil may wear off before the effects of the benzodiazepine. Repeat doses may be required.
Flumazenil is not generally recommended for use in children.
Naloxone (Narcan)
Narcotic Antagonist
ADULTS IV: 0.4 to 2 mg over 2 minutes with repeated doses at 2 to 3 minute intervals. Max total dose = 10 mg
PEDIATRIC IV: 0.01 mg/kg over 2 minutes and may repeat with a dose of 0.1 mg/kg if needed.
Onset: 2 – 3 min
Duration: 45 min to 4 H
Half-life Adults - 30-80 min Neonate: 2.5-3.5H
Narcotic antagonist. Contraindicated in patients with hypersensitivity to Naloxone.
NOTE: The effects of Naloxone may wear off before the effects of the narcotic. Repeat doses may be required.
Naloxone does not reverse and may even exacerbate hyperexcitability response associated with normeperidine toxicity.
References: Drug Facts and Comparisons, Facts and Comparisons, Inc: St. Louis, MO: 2000 Micromedex, Volume 107, expires 3/31/2001. McEvoy, GK. Pharmacist’s Drug Handbook, American Society of Health-System Pharmacists; Springhouse Corp: Hudson, Ohio: 2001. Lacy, et. Al., Drug Information Handbook, American Pharmaceutical Association, LexiComp, Inc: Hudson, Ohio: 2003. Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain, American Pain Society: 1999

Do Not Use Abbreviations: U, IU, Q.D., Q.O.D., Trailing zero (X.0 mg), Lack of leading zero (.X mg), MS, MSO4 and MgS04
DATE TIME LONG-TERM ANTICOAGULATION ORDERS FOR ATRIAL FIBRILLATION
Reminder: Date, time all orders. Print name & ID # under signature.Warfarin (COUMADIN): Follow Warfarin (COUMADIN) Therapy Initiation Protocol (DO 640)
Warfarin (COUMADIN) _______ mg PO once daily
Dabigatran (PRADAXA): 150 mg PO twice daily 75 mg PO twice daily (CrCl 15 - 30 mL/min)
Rivaroxaban (XARELTO): 20 mg PO daily 15 mg PO daily (CrCl 15 - 30 mL/min)
Apixaban (ELIQUIS): 5 mg PO twice daily 2.5 mg PO twice daily
(If patient has 2 out of 3 criteria: Age greater than 80, Weight less than 60 kg, Creatinine greater than 1.5 mg/dL)
STAT PHARMACYORDER(Place X in Box)
ONE SET OF ORDERS PER PAGE /MARK THROUGH BLANK LINES / SCAN ALL ORDERS
Physician’s Signature ______________________________________ I.D. #: ______________ ANDPrint Name: _______________________________________ Date: ___________ Time: _______
Use black ballpoint pen. RM#
DO #1003 Rev. 7/23/1407600BD1003
SCANNED DATE: _______ TIME: _______ INITIALS: _______
APPROVED BY BHSF P&T