interventions in the elderly - tri city cardiology · interventions in the elderly. satya reddy...
TRANSCRIPT

FIFTH ANNUAL SYMPOSIUM
Interventions in the Elderly
Satya Reddy Atmakuri MD
I Have No Financial Interest to Disclose

People greater than 65 years of age will increase from 12% of population in 2000 to 20% of population in 2030People greater than 85 years of age will increase from 9.3 million in 2000 to 19.5 million in 2030Average life expectancy in US was 77.3 years in 2002 and risingWe take care of these elderly patients every dayWe are in Mesa !!

Acute coronary syndromes
ST elevation myocardial infarction
Peripheral arterial disease
Structural heart disease
Chest pain (cardiac) greater than 20 minutes
Abnormal cardiac enzymes
ST-T segment changes
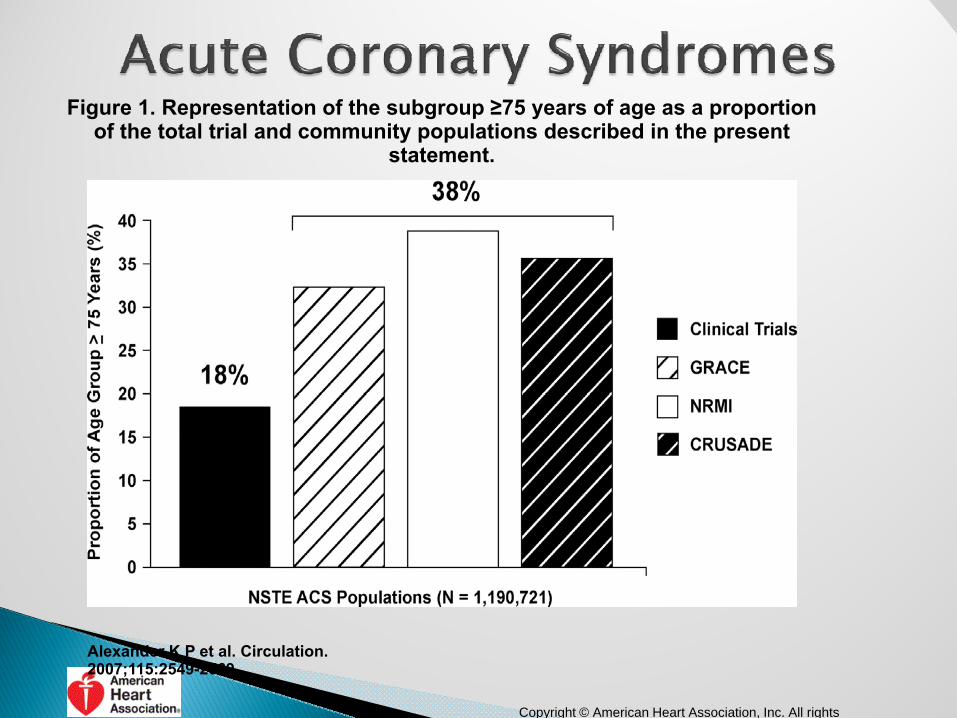
Figure 1. Representation of the subgroup ≥75 years of age as a proportion of the total trial and community populations described in the present
statement.
Alexander K P et al. Circulation. 2007;115:2549-2569
Copyright © American Heart Association, Inc. All rights

Figure 2. Proportion of age subgroups with cardiac risk factors and comorbidity from the CRUSADE Quality Improvement Initiative.
Alexander K P et al. Circulation. 2007;115:2549-2569
Copyright © American Heart Association Inc All rights
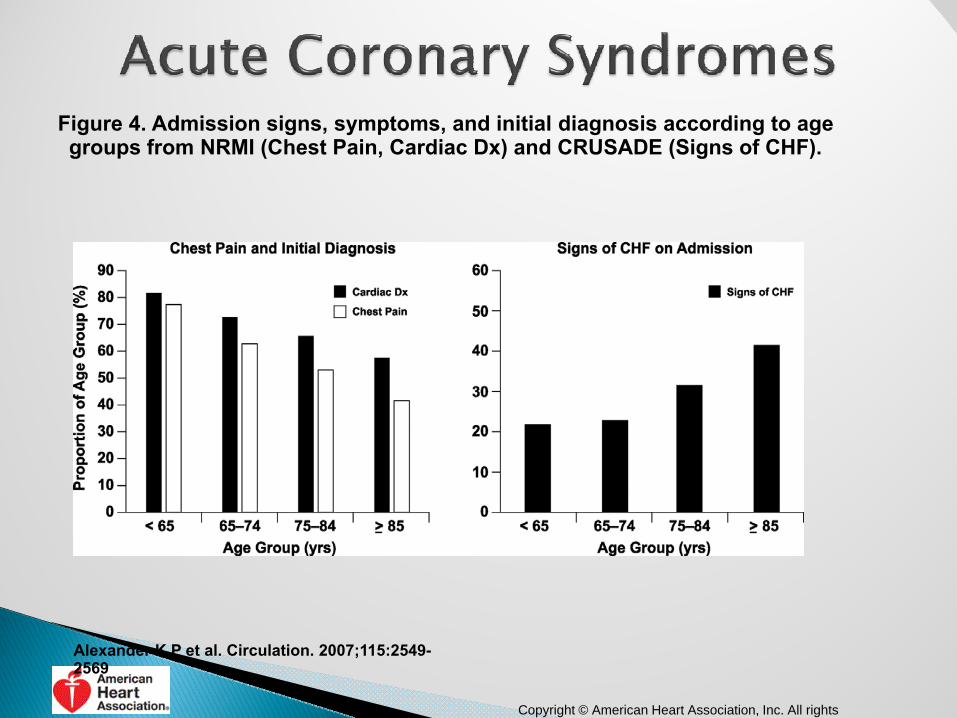
Figure 4. Admission signs, symptoms, and initial diagnosis according to age groups from NRMI (Chest Pain, Cardiac Dx) and CRUSADE (Signs of CHF).
Alexander K P et al. Circulation. 2007;115:2549-2569
Copyright © American Heart Association, Inc. All rights

Figure 5. In-hospital and 30-day death rates according to age groups in trial (VIGOUR) and community (GRACE) populations.
Alexander K P et al. Circulation. 2007;115:2549-2569
Copyright © American Heart Association, Inc. All rights

Figure 7. Benefit of invasive care in older patients in reducing the risk of death or MI combined from the TACTICS-TIMI 18 trial.117.
Alexander K P et al. Circulation. 2007;115:2549-2569
Copyright © American Heart Association, Inc. All rights reserved

Patient Presentation - ACS
91 yo gentleman presents with progressive class III – IV angina Able to walk 1-2 blocks 2 months prior to presentationCardiac risk factors◦ Hypertension◦ HyperlipidemiaSick sinus syndrome◦ s/p PPMRheumatoid arthritis

Stress studyIschemia of anterior/anterolateral walls and apexEF 45%
EchocardiogramEF 40-45%No significant valvular disease
Medical therapyAtenolol 25, Lisinopril 2.5, Imdur30ASA 81, Simvastatin 10
Admitted to the hospital with worsening angina and dyspnea at rest
New onset CHF

Coronary Angiography

PTCA – 3mm balloon at 8 atm
Impella 2.5CO 2.2 L/min at P8
7 Fr EBU 3.5 guide
Runthrough wire in LAD
BMW wire in LCX

Stent – 4x20mm Promus Premier

Final Angiogram
IVUS: LAD 9.4mm2; LM 12.2mm2

Figure 1. Representation of elderly (≥75 years of age) trial versus community populations.
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association Inc All rights

Figure 2. Presentation of STEMI and age (NRMI 2–4).
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association, Inc. All rights

Figure 3. Reperfusion therapy for STEMI (NRMI 2–4).
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association, Inc. All

Figure 4. Death and stroke after fibrinolysis in GUSTO-I, categorized by age.
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association, Inc. All rights reserved

STEMIFigure 5. Fibrinolytic therapy and age (excluding patients presenting beyond 12 hours, with normal ECGs, with only T-wave inversion or ST depression).
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association, Inc. All rights
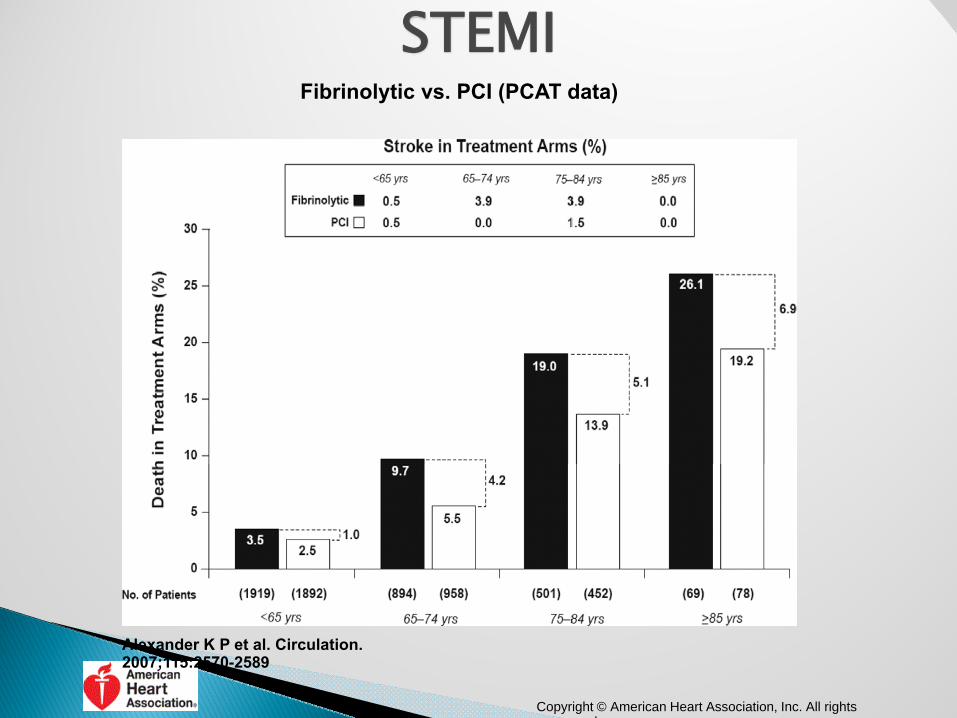
STEMIFibrinolytic vs. PCI (PCAT data)
Alexander K P et al. Circulation. 2007;115:2570-2589
Copyright © American Heart Association, Inc. All rights d

Shock trial◦ Small subset, n=56◦ No benefit from revascularizationShock registry◦ 277 patients > 75 years◦ Benefit with early revascularization
81 year old femaleRisk factors◦ Hypertension◦ Hyperlipidemia◦ Severe COPD – FEV-1 0.7 L◦ Current smokerPresentation◦ 3 hours of chest pain◦ Inferior ST elevation by EKG


Placement of two drug eluting stents

Patient developed COPD exacerbation Intubated on hospital day 3Ventilator associated pneumoniaAtrial fibrillationGI BleedCVATracheostomyPassed away from multi-organ failure after 40 days from presentation
Developed to treat patients ◦ High surgical risk (Partner Cohort-A)◦ In-operable (Partner Cohort-B)◦ Technically difficult
Porcelain AortaRadiationSternal infectionPatent LIMA underneath sternum

Co-morbidities◦ STS◦ Euro-scoreDisability◦ ADLs◦ Dementia◦ Wheel-chair boundFrailty

Frailty - Risk Assessment in ElderlySyndrome of multisystem impairment associated with aging that results in decreased physiologic reserve and increased vulnerability to stressors.
Increasing ageFried J Gerontol A Biol Sci Med Sci. 2001 Mar;56(3)figure modified from Taffert GE: Physiology of aging. 2003.

Objective Frailty Assessment -Physical Frailty in CHS
Self Report Objective Measures• Unintentional
weight loss• Subjective
exhaustion• Low physical
activity
• Slow walking speed• Low grip strength
Fried 2001, Guralnik 2000,Studenski 2011, Afilalo, 2010.
Frailty increases risk for• Death• New disability• Major complications after
cardiac surgery• Resource utilization

Frailty in the general population
Fried, LP. J Geront Med Sci 2001, 56A, 3, M146
3‐year Outcomes (%)Frailty Status at Baseline (n)
Died First Hospitalization
First Fall Worsening ADL Disability
Worsening Mobility Disability
Not Frail (2469) 3 33 15 8 23Intermediate (2480) 7 43 19 20 40
Frail (368) 7% 18 59 28 39 51
p‐value <0.0001 <0.0001 <0.0001 <0.0001 <0.0001
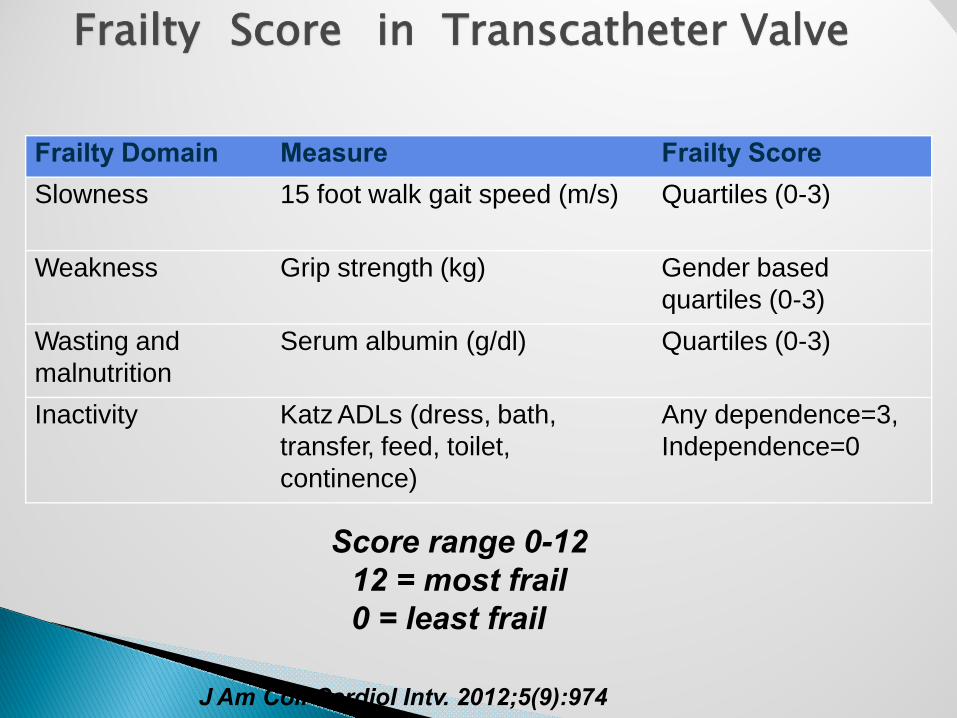
Frailty Score in Transcatheter Valve
Score range 0-12 12 = most frail 0 = least frail
J Am Coll Cardiol Intv. 2012;5(9):974
Frailty Domain Measure Frailty ScoreSlowness 15 foot walk gait speed (m/s) Quartiles (0-3)
Weakness Grip strength (kg) Gender based quartiles (0-3)
Wasting and malnutrition
Serum albumin (g/dl) Quartiles (0-3)
Inactivity Katz ADLs (dress, bath, transfer, feed, toilet, continence)
Any dependence=3, Independence=0
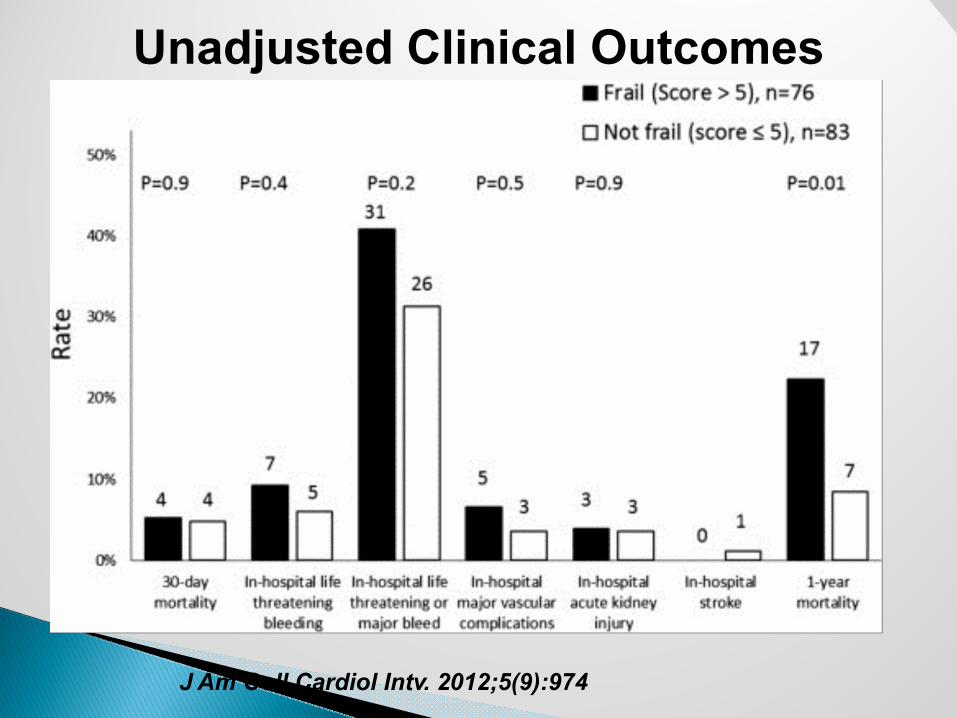
Unadjusted Clinical Outcomes
J Am Coll Cardiol Intv. 2012;5(9):974
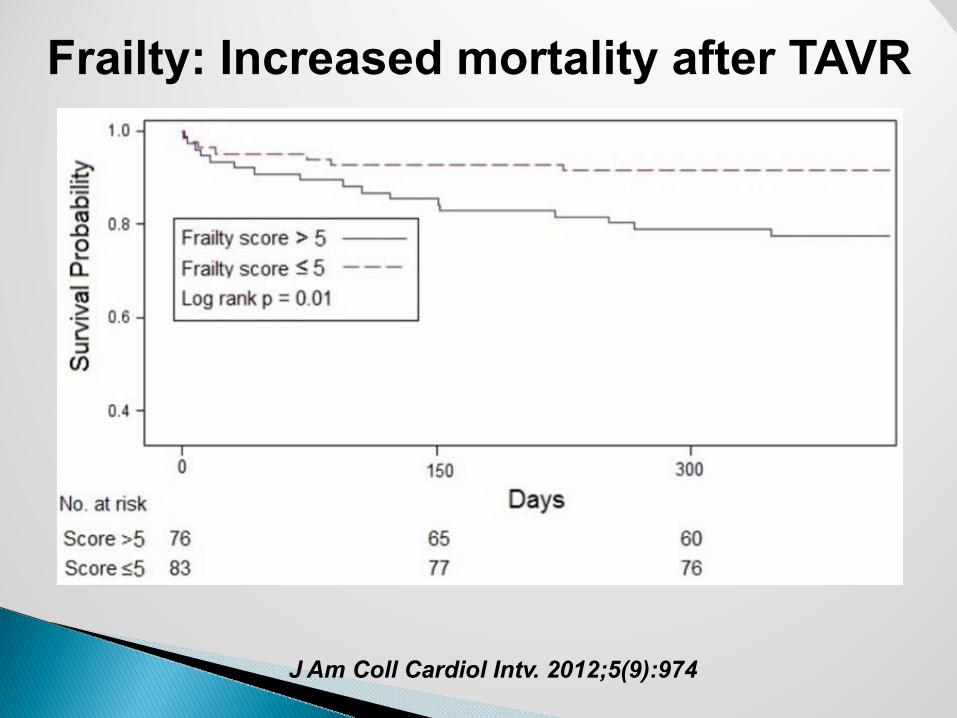
Frailty: Increased mortality after TAVR
J Am Coll Cardiol Intv. 2012;5(9):974

Frailty: Increased mortality after TAVR
Frailty ≠ Futility 78% of frail subjects alive at 1 year
J Am Coll Cardiol Intv. 2012;5(9):974

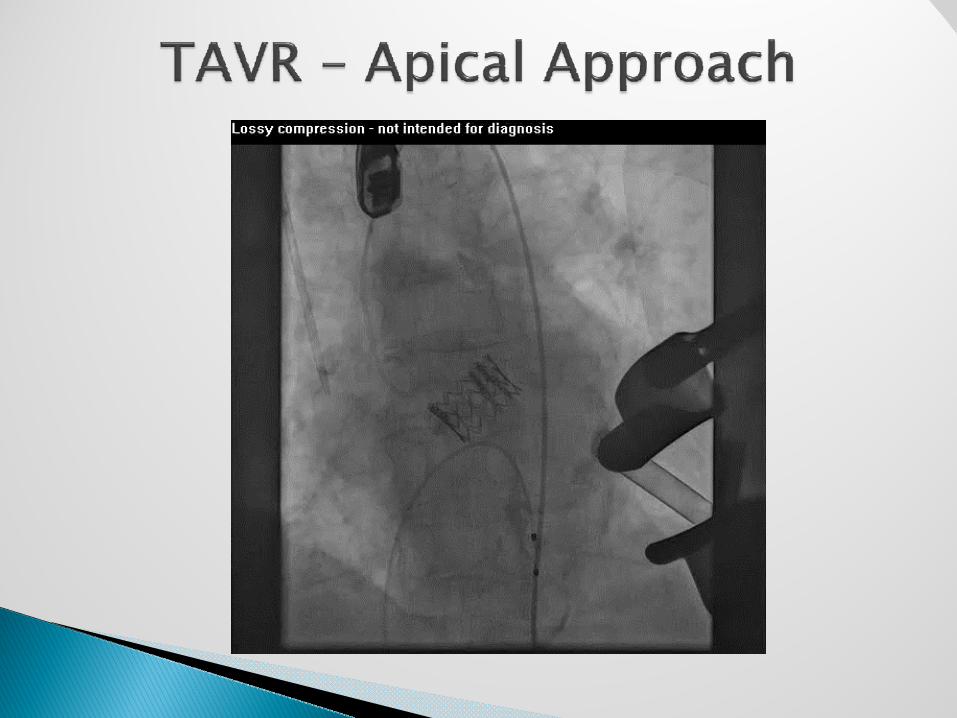
94 year old femalePresents with Class III CHFSTS 11.2%Normal coronariesNormal LV functionPADBalloon Aortic Valvuloplasty 1 year agoFrailty score◦ After valvuloplasty – 3◦ Current presentation - 7

Vmax 3.7m/sec after BAV now back to 4.18m/sec ; mean gradient 45 mm HG Area-0.8cm 2
Heavily calcified valve


Edwards-Sapien 26mm valve
At 6-month follow up◦ NYHA Class II◦ Frailty score back to 3◦ Lives independently

• Procedural success is lower in elderly pts (≥ 80 years) than inyounger groups (70-80 years and < 70 years): 74.2% vs. 78% vs. 81.4%, respectively; P < 0.001)
In multivariate analysis, advanced age predicts increasedvascular access complications
• However, very old age is not associated with significantly higher in-hospital mortality, MI, stroke, or reintervention
•
7,769 pts from the Blue Cross Blue Shield of MichiganCardiovascular Consortium PVI registry.
Plaisance BR, et al. J Am Coll Cardiol Intv.2011;4:694-701.
Safety of Contemporary Percutaneous Peripheral ArterialInterventions in the Elderly
Implications: Contemporary peripheral vascular intervention canbe performed in elderly patients with low rates of periproceduralcomplications.

85 year old practicing attorney presents with chest pain and right foot pain and noted to have troponin 2.4◦ DM◦ HTN◦ Hyperlipidemia◦ CAD s/p CABG in 2000◦ CRI with creatinine in 1.8 to 2.0 rangeInitial medical management◦ NTG, iv heparin◦ ASA, beta blocker, statin
Physical Exam◦ Clear lungs, S4, 1/6 SEM, R carotid bruit◦ Left toe ulcer and non-palpable pulses in left footChest discomfort improved with medical therapyABI◦ Right – 0.72; Left 0.4Carotid ultrasound◦ Right > 80% stenosis; Left < 50% stenosisEcho◦ EF 55-60%, Aortic sclerosis

Placement of two drug eluting stents

Stent placement in the left external iliac artery

Placement of stents in left SFA
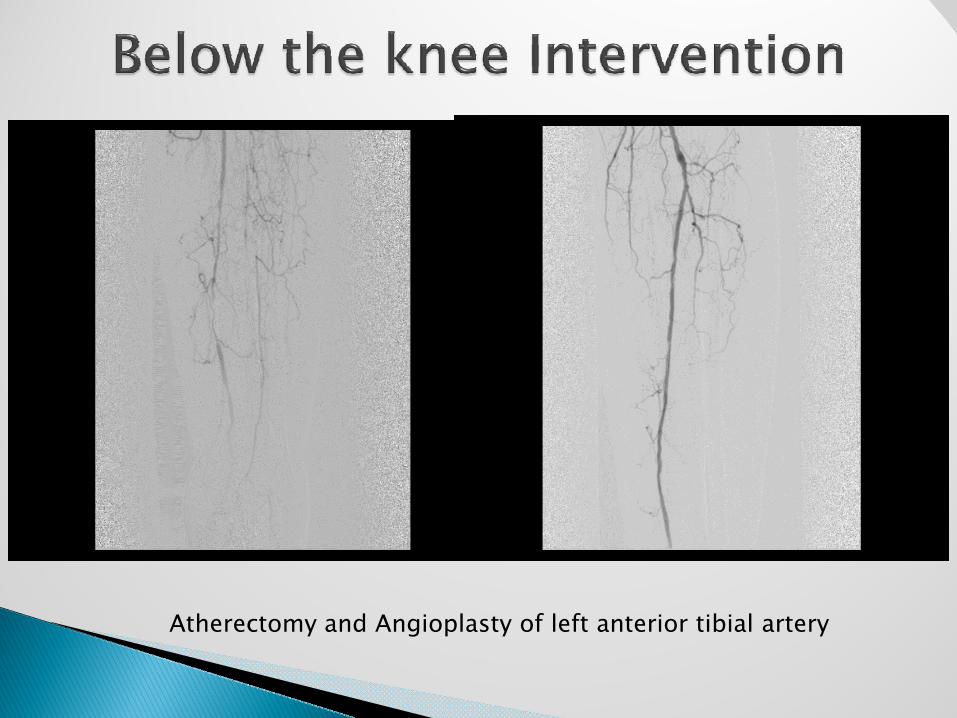
Atherectomy and Angioplasty of left anterior tibial artery

Atherectomy and Angioplasty of left anterior tibial artery


Cardiac◦ No angina◦ Stress study in 2011 – No ischemia, EF 60%Lower extremity◦ No claudication (ABI in 2013: R–0.9, L-0.8) ◦ R toe – partial amputation; healed well◦ No further ischemic sequalaeCarotid◦ Widely patent stent in 2013Renal◦ Creatinine – 2.2
Patients > 75 years :Are usually not enrolled in clinical trialsPresent with atypical symptomsHave more co-morbiditiesHave more risks associated with interventionsHave the greatest benefit

75 year old female presents with severe dyspnea, orthopnea, PNDHypertensionHyperlipidemiaCOPDMultiple admissions for COPD exacerbation over the last three monthsEKG – Diffuse ST depression in anterior leadsCXR – COPD changes, pulmonary edemaLabs – Troponin – 2.69