intravenous sedation monitoring 59 amdg/dental squadron technician orientation module
TRANSCRIPT
Intravenous Sedation Monitoring
59 AMDG/Dental Squadron
Technician Orientation Module
Training Objectives
• Verification of current BLS training
• Use of automated monitoring equipment
• Physiologic norms and overview of medications
• Overview of medical emergencies
• “Code Blue” procedures and “Crash Cart” familiarization

Levels of Anesthesia
• Local anesthesia
• Conscious Sedation
• Deep Sedation
• General Anesthesia

Local Anesthesia
• Elimination of sensations, particularly pain, by the administration of a topical application or regional administration or injection of a drug

Conscious Sedation
• A minimally depressed level of consciousness which allows the patient to independently and continuously maintain a patent airway and respond appropriately to verbal commands– Anxiolysis– Moderate Sedation

Deep Sedation
• A controlled state of depressed consciousness accompanied by a partial loss of protective reflexes and the ability to respond appropriately to verbal commands

General Anesthesia
• The elimination of all sensation accompanied by the loss of consciousness

Stages of General Anesthesia
• Stage I– Analgesia
• Stage II– Delirium
• Stage III– Surgical anesthesia
• 4 planes of surgical anesthesia

Stages of General Anesthesia
• Stage IV– Medullary paralysis

Level of Anesthesia
• In the OMFS clinic, Dunn Dental Clinic and MacKown Dental Clinic …..– Stage I
• Otherwise known as “Conscious Sedation”
• In the Wilford Hall Medical Center OSOR– Stage III
• “Deep Sedation”
• General Anesthesia
Provider Training
• Must be able to safely manage 1 level of anesthesia beyond plane to be achieved– If practicing Deep Sedation you must be able to
manage general anesthesia
Technician Responsibilities
• Pre-Procedure – Equipment
• Instruments
• Venipuncture
• Monitors
• Emergency Supplies– “Crash Cart”
– Cardiac Monitor
– Medications

Technician Responsibilities
• Pre-Procedure Patient Assessment– Vital Signs– Allergies– Contacts/Dentures– NPO status– Changes in medical history
• URI• Hospitalizations• Sick family members
Special Considerations
• Pediatric patients– Not “little adults”
• Geriatric patients– Unique subclass of patients with physiological
changes complicating treatment
“Show Stoppers”
• Food or fluid intake 6 hours prior to surgery• Clear fluid intake within 2 hours of surgery
– Can read newspaper print when looking through liquid
• Recent alcohol ingestion• Recreational drug use• Pregnancy• Thyroid Dysfunction

“Show Stoppers”
• Recent asthma attack or respiratory failure
• Treatment with MAO inhibitors
• Tricyclic Antidepressants
• Adrenal Dysfunction
• Renal Dysfunction

Technician Responsibilities
• Pre-Procedure Patient Assessment– Informed Consent– Escort Present– Establishes patient’s mental status
• Under the influence of alcohol or drugs
• Oriented to person, place, time
– Document on AF 1417• Clinical Sedation record


Technician Responsibilities
• Pre-Procedure Patient Assessment– Supplemental oxygen applied– Suction functioning

Technician Responsibilities
• Intraoperative Responsibilities – “Float”– Informed consent signed prior to sedation– Name, dose, route and time of all medications
documented– Procedure begin and end times– Prior adverse reactions– Pre-medication time and effect

Technician Responsibilities
• Intraoperative Responsibilities – “Float”– Vital Signs
• BP
• Heart Rate
• Respiratory Rate
• Oxygen Saturation
• Level of Consciousness
Technician Responsibilities
• Post-operative Responsibilities – “Float”– Vital Signs at least every 5 minutes
• BP • Heart Rate• Respiratory Rate• Oxygen Saturation• Level of Consciousness
• Sedated patients must be continuously monitored until discharged
The following values are indicative of the “normal” adult patient. Pediatric and Geriatric
patients have different values and unique characteristics for which
the anesthesiologist/surgeon must be aware

Blood Pressure
• Specifically mean arterial pressure (MAP)– MAP
• Systolic BP – Diastolic BP/3 + Diastolic BP
• Also written as Diastolic BP + 1/3 Pulse Pressure
• Normal 80-100
• Body loses autoregulatory capacity at a MAP less than 50 or greater than 150
Heart Rate
• Normal range 60-90

Respiratory Rate
• Normal range 10-16 per minute

Oxygen Saturation
• Must be greater than 90%
• Supplemental oxygen via nasal cannula is required in the OMFS clinic during sedation– Initially 2-3 liters/minute
• In the OSOR supplemental oxygen is supplied by nasal cannula or endotracheal tube
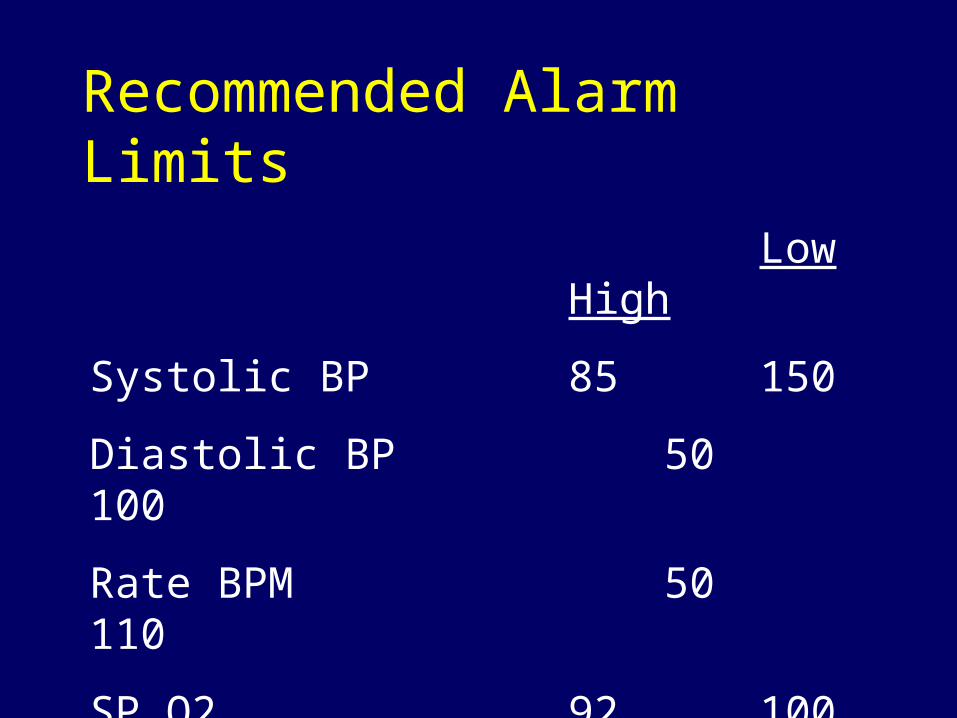
Recommended Alarm Limits
LowHigh
Systolic BP 85 150
Diastolic BP 50 100
Rate BPM 50110
SP O2 92 100
Level of Consciousness
• Must be able to respond to verbal stimuli by the surgeon in the clinic
• May be greatly sedated or unable to arouse by verbal stimuli in the operating room
Technician Responsibilities
• Post-operative Responsibilities – “Float”– ALDRETE Post-Operative Scoring System
• A cumulative score of 8 or above is necessary for discontinuation of monitoring– We generally use a goal of 10 as necessary for
dismissal from clinic– Sum of standardized measurements of
movement, respiration, circulation, color and level of consciousness

Movement
• Move all 4 extremities 2
• Move 2 extremities 1
• No control 0
Respiration
• Breathe deep and cough 2
• Dyspnea 1
• No respirations 0
Circulation
• BP +/- 20% pre-sedation level 2
• BP +/- 21-50% pre-sedation level1
• BP +/- > 50% pre-sedation level 0
Consciousness
• Fully alert 2
• Arousable 1
• No response 0
Color
• Pink 2
• Pale, Dusky, Blotchy 1
• Cardboard 0
The Key to Sedation
• Local Anesthesia– If a poor local
anesthetic block has been given, the patient will continue to feel pain throughout the procedure

Valium (Diazepam)
• Benzodiazepine• Produces sleepiness and relief of apprehension• Onset of action 1-5 minutes• Half-life
– 30 hours
– Active metabolites
• Average sedative dose– 10-12 mg

Versed (Midazolam)
• Short acting benzodiazepine– 4 times more potent than Valium
• Produces sleepiness and relief of apprehension• Onset of action 3-5 minutes• Half-life
– 1.2-12.3 hours
• Average sedative dose– 2.5-7.5 mg

Demerol (Meperidine)
• Narcotic• Pain attenuation and some sedation• Onset of action
– 3-5 minutes• Half-life
– 30-45 minutes• Average dose
– 20-50 mg
Fentanyl (Sublimaze)
• Narcotic/Opiod agonist– 100 times more potent than Morphine
• Pain attenuation and some sedation• Onset of action around 1 minute• Half-life
– 30-60 minutes
• Average dose– 0.05 – 0.06 mg

Additional Medications
• Likely to be seen in scenarios where deeper levels of sedation are being performed– Propofol (Diprivan)– Robinul (Glycopyrrolate)
Propofol (Diprivan)
• Intravenous anesthetic/sedative hypnotic• Sedative, anesthetic and some antiemetic
properties• Onset of action within 30 seconds• Half-life
– 2-4 minutes
• Average sedative dose– Varies
Robinul (Glycopyrrolate)
• Anticholinergic– Heart rate increases– Salivary secretions decrease
• Dose 0.1-0.2 mg
• Onset of action within 1 minute

Medical Emergency
• Syncope• Hypoglycemia• Hypotension• Hypertension• Bronchospasm
• Laryngospasm• Apnea• Myocardial infarction• Stroke

Medical Emergency
• Know when and how to activate a “Code Blue”• Location of Crash Cart
– Medications– Monitors
• Location of emergency medications• BLS
Medical Emergency
• Know how to prevent, recognize, and treat syncope (fainting)– Supplemental O2– Elevation of lower extremities– Trendelenburg
• Be prepared to assist in airway management

Emergency Drugs
• These are included for reference only
• Technicians should not be administering medications to patients without advanced training in ACLS and direct provider supervision

Emergency Drugs
• Flumazenil (Romazicon)
• Naloxone (Narcan)
• Esmolol (Brevibloc)
• Ephedrine
• Epinephrine
• Atropine
Flumazenil (Romazicon)
• Benzodiazepine antagonist– Versed reversal agent
• Initial dose – 0.2mg– May repeat at 1 minute intervals to dose of 1mg
• Onset of action within 1-2 minutes• Must monitor for re-sedation
– May be repeated at 20 minute intervals as needed
Naloxone (Narcan)
• Narcotic antagonist– Fentanyl reversal agent
• Initial dose – 0.4mg– May repeat every 2-3 minutes at doses of 0.4-
2mg
• Monitor for re-sedation
Esmolol (Brevibloc)
• Antihypertensive
• Beta blocker
• Initial dose 0.25 –1.0 mg/kg over 30 seconds– Short half-life of approximately 10 minutes

Ephedrine
• Used for hypotension
• Sympathomimetic
• Initial dose 5-10mg
• Action may not be seen for several minutes

Atropine
• Significant bradycardia or asystole– Slow heart beat or NO heartbeat
• Anticholinergic
• Initial dose 0.25 – 1.0 mg– May repeat every 3-5 minutes– Maximum total dose .03 mg/kg
Epinephrine
• True emergency medication
• Administration should be preceded by activation of the 911 emergency response system

Questions