introduction clinical and morphological spectrum...
TRANSCRIPT
02/06/2015
1
Melanocytic Tumours: Update on Epidemiology andUpdate on Epidemiology and
Molecular Biology
Thomas Brenn
Cutaneous Melanocytic Tumours‐Introduction‐
• Wide clinical and morphological spectrum
• Ranging from benign naevi to melanoma
• Majority benignMajority benign
• Separating benign from malignant poses significant clinical and histological challenge
• Most important: identification of predictors of outcome
Melanocytic Tumours
Naevi
• Common acquired naevi
• Congenital naevi
• Special site naevi
Melanoma
• SSM
• Nodular M
• Acral lentiginous M
• Dysplastic naevi
• Sclerosing naevi
• Blue Naevi
• DPN
• Lentigo maligna M
• Desmoplastic M
• Mucosal M
• Lentiginous M
• Blue naevus like M
• Uveal M
Cutaneous Melanocytic Tumours
Intermediate Malignancy
• Spitzoid melanoctic tumours
• Pigmented epithelioid melanocytoma(Pigment synthesising melanoma)

02/06/2015
2
The 10 Most Commonly Diagnosed Cancers: 2012 Estimates
Total Number and Percentage of New Cases Diagnosed per Year, Worldwide
Melanoma Epidemiology The 20 Most Common Cancers in 2011Number of New Cases, UK
Malignant Melanoma (C43): 2009-2011 Average Number of New Cases Per Year and Age-Specific Incidence Rates per 100,000 Population, UK
Malignant Melanoma (C43)Percentage Distribution of Cases Diagnosed on Parts of the Body, by Sex, UK, 2008-2010
Anatomical Distribution
02/06/2015
3
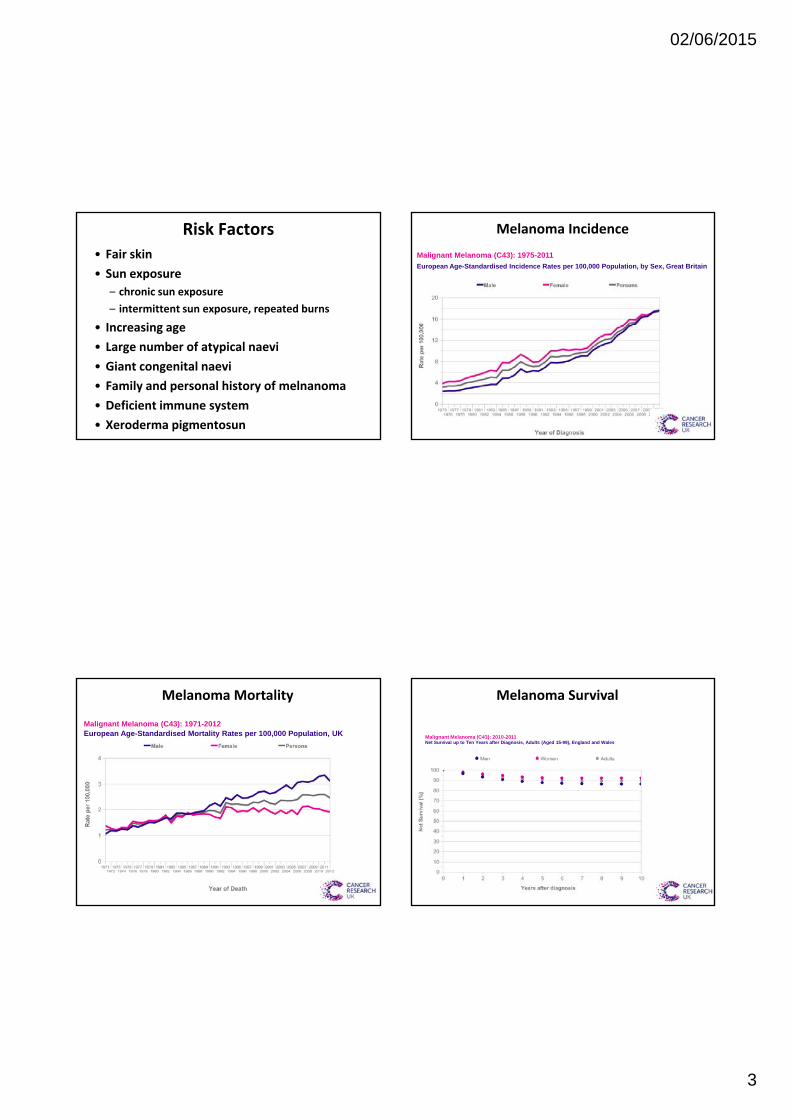
Risk Factors
• Fair skin
• Sun exposure
– chronic sun exposure
– intermittent sun exposure, repeated burns
• Increasing age• Increasing age
• Large number of atypical naevi
• Giant congenital naevi
• Family and personal history of melnanoma
• Deficient immune system
• Xeroderma pigmentosun
Malignant Melanoma (C43): 1975-2011
European Age-Standardised Incidence Rates per 100,000 Population, by Sex, Great Britain
Melanoma Incidence
Malignant Melanoma (C43): 1971-2012European Age-Standardised Mortality Rates per 100,000 Population, UK
Melanoma Mortality
Malignant Melanoma (C43): 2010-2011Net Survival up to Ten Years after Diagnosis, Adults (Aged 15-99), England and Wales
Melanoma Survival

02/06/2015
4
Malignant Melanoma (C43): 1971-2011
Age-Standardised Five-Year Net Survival, England and Wales
Melanoma SurvivalMalignant Melanoma (C43): 2002-2006
Five-Year Relative Survival (%) by Stage, Adults Aged 15-99, Former Anglia Cancer Network
Melanoma Survival
Malignant Melanoma (C43): 2006-2010Proportion of Cases Diagnosed at Each Stage, Adults 15-99, Former Anglia Cancer Network
Stage Men Women Adults
Stage I 61.4% 71.3% 66.4%
Stage II 21.0% 17.1% 19.1%
Stage III 13.7% 8.5% 11.1%
Stage IV 2.0% 0.7% 1.3%
Stage not known 1.9% 2.4% 2.1%
All stages 100.0% 100.0% 100.0%
02/06/2015
5
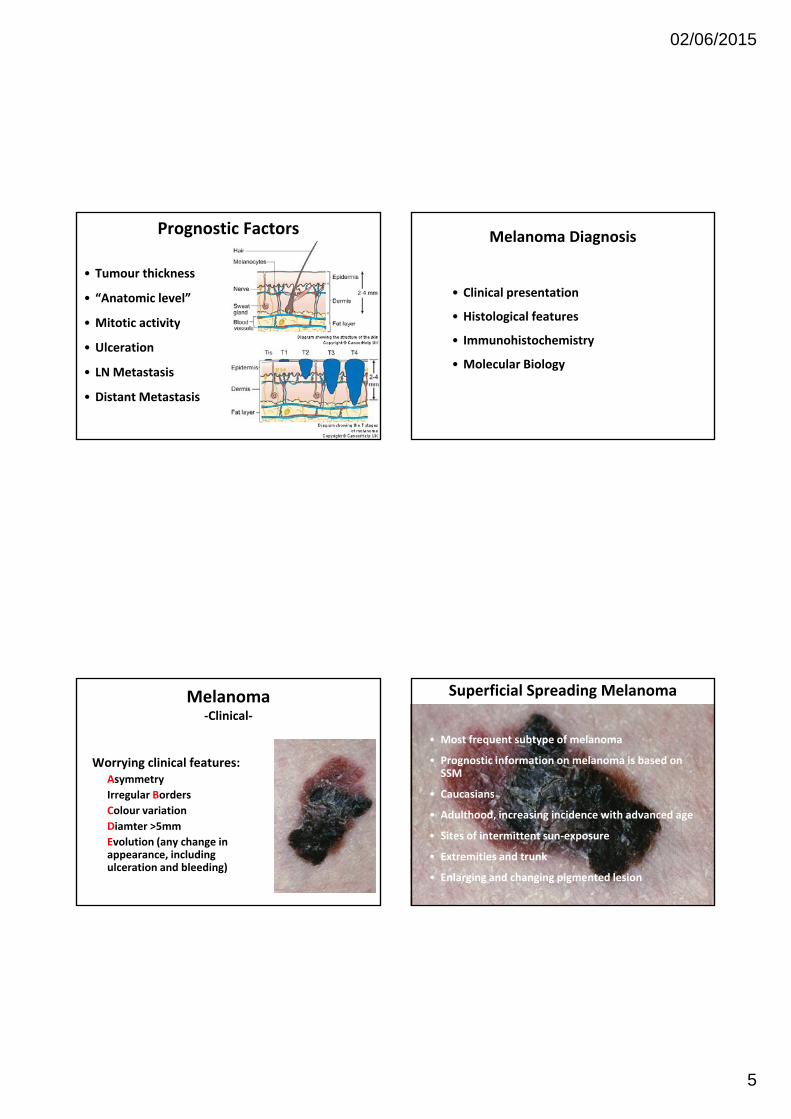
Prognostic Factors
• Tumour thickness
• “Anatomic level”
• Mitotic activityMitotic activity
• Ulceration
• LN Metastasis
• Distant Metastasis
Melanoma Diagnosis
• Clinical presentation
• Histological features
• Immunohistochemistry
• Molecular Biology
Melanoma‐Clinical‐
Worrying clinical features:Asymmetry
I l B dIrregular Borders
Colour variation
Diamter >5mm
Evolution (any change in appearance, including ulceration and bleeding)
Superficial Spreading Melanoma
• Most frequent subtype of melanoma
• Prognostic information on melanoma is based on SSM
Ca casians• Caucasians
• Adulthood, increasing incidence with advanced age
• Sites of intermittent sun‐exposure
• Extremities and trunk
• Enlarging and changing pigmented lesion
02/06/2015
6
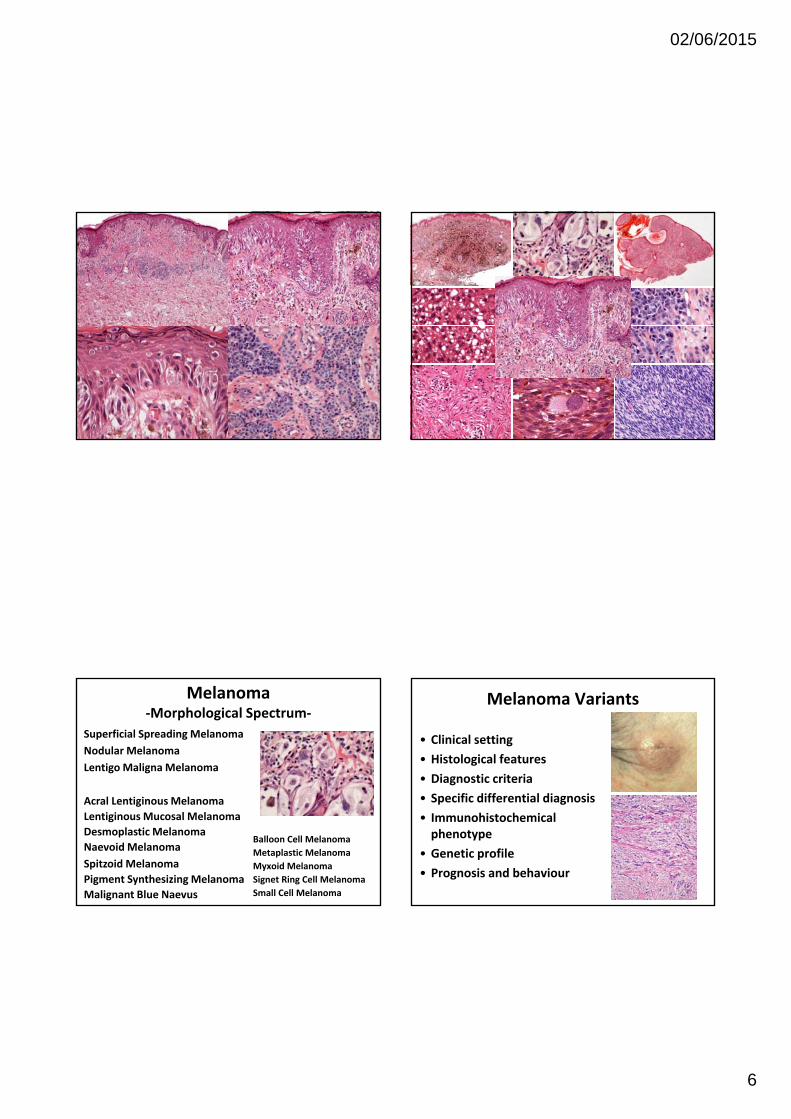
Melanoma‐Morphological Spectrum‐
Superficial Spreading Melanoma
Nodular Melanoma
LentigoMaligna Melanoma
Balloon Cell Melanoma
Metaplastic Melanoma
Myxoid Melanoma
Signet Ring Cell Melanoma
Small Cell Melanoma
Acral LentiginousMelanoma
LentiginousMucosal Melanoma
Desmoplastic Melanoma
Naevoid Melanoma
Spitzoid Melanoma
Pigment Synthesizing Melanoma
Malignant Blue Naevus
Melanoma Variants
• Clinical setting
• Histological features
• Diagnostic criteria
• Specific differential diagnosis
• Immunohistochemicalphenotype
• Genetic profile
• Prognosis and behaviour

02/06/2015
7
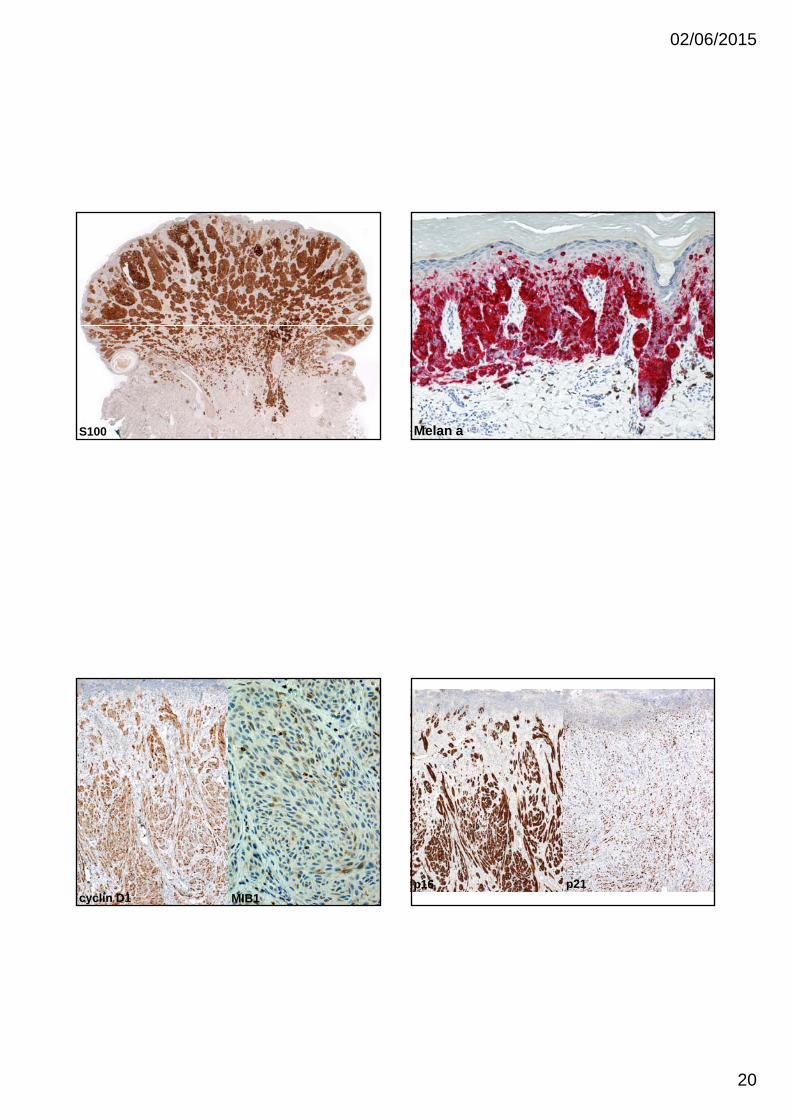
Melanoma‐Immunohistochemistry‐
S100
Sox10
MIB1
cyclin D1
p53
Melan A/Mart‐1
HMB45
MITF
bcl2
p16
p21
BRAF, NRAS, CKIT, ALK, ROS, BAP1 S100
S100/SOX10
First line melanocytic marker:
• High Sensitivity for melanocytic tumours
• Expressed in Naevi and Melanoma
• Low specificity, also seen in neural and myoepithelial neoplasms
• Best marker in desmoplasticmelanoma
• May be weak and focal in benign and malignant blue naevi
S100
Melan ASecond line melanocytic marker:
• Good sensitivity for epithelioidmelanocytic tumours
• But often lost in spindle cell melanoctic neoplasms
• Expressed in Naevi and Melanoma
• Relatively high specificity, but also seen in PECOMA
• Useful for evaluation of junctionalcomponent
• Often strong and diffuse in benign and malignant blue naevi
Melan A
02/06/2015
8
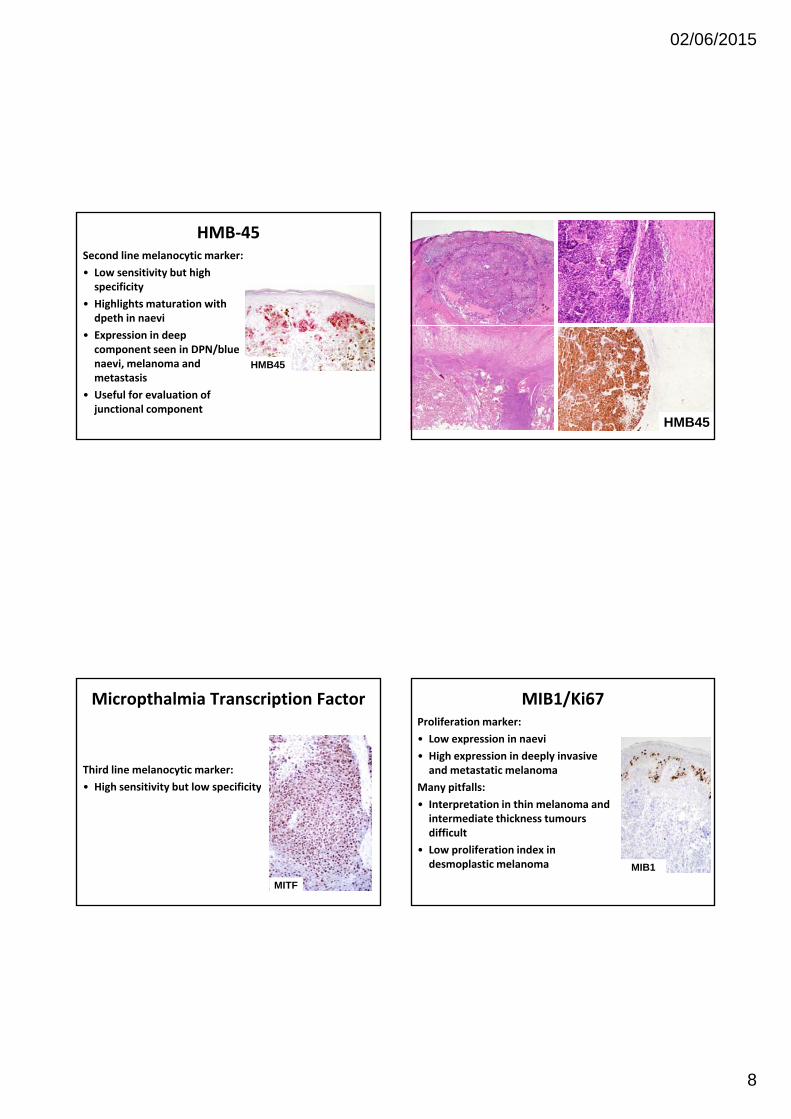
HMB‐45Second line melanocytic marker:
• Low sensitivity but high specificity
• Highlights maturation with dpeth in naevi
• Expression in deep component seen in DPN/blue naevi, melanoma and metastasis
• Useful for evaluation of junctional component
HMB45
HMB45
Micropthalmia Transcription Factor
Third line melanocytic marker:
• High sensitivity but low specificityg y p y
MITF
MIB1/Ki67Proliferation marker:
• Low expression in naevi
• High expression in deeply invasive and metastatic melanoma
Many pitfalls:y p
• Interpretation in thin melanoma and intermediate thickness tumours difficult
• Low proliferation index in desmoplastic melanoma MIB1
02/06/2015
9
MIB1
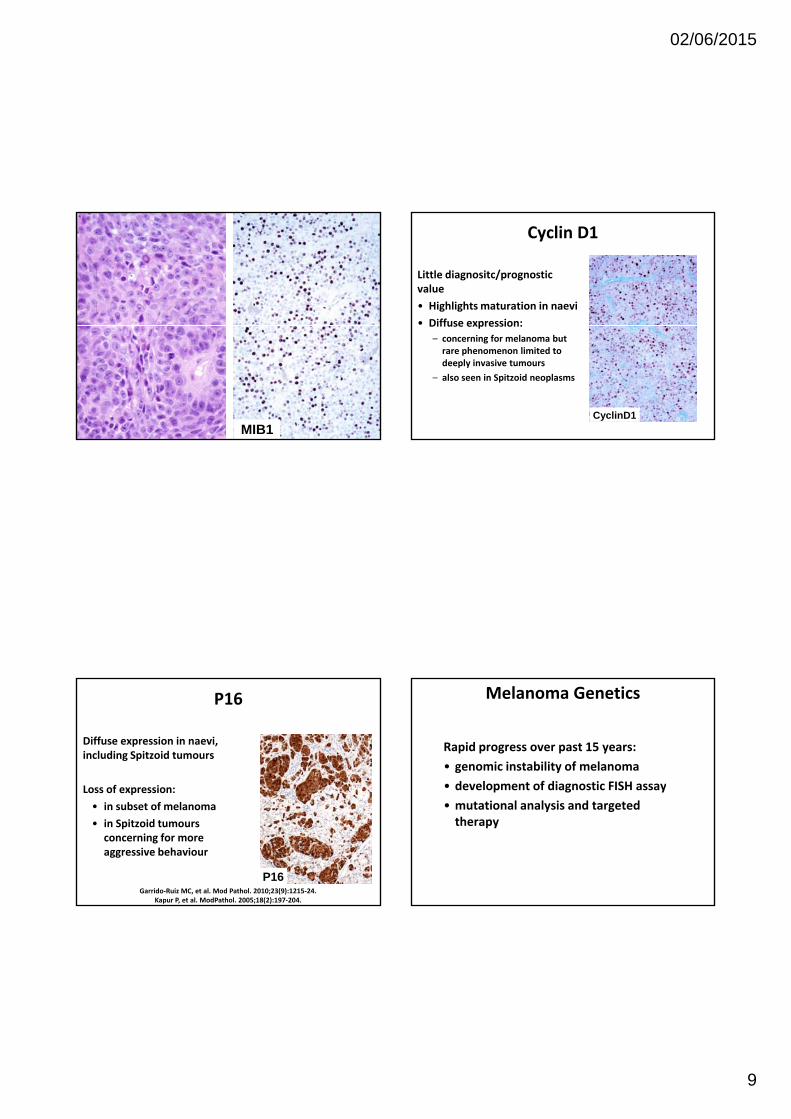
Cyclin D1
Little diagnositc/prognostic value
• Highlights maturation in naevi
• Diffuse expression:Diffuse expression:
– concerning for melanoma but rare phenomenon limited to deeply invasive tumours
– also seen in Spitzoid neoplasms
CyclinD1
P16
Diffuse expression in naevi, including Spitzoid tumours
Loss of expression:Loss of expression:
• in subset of melanoma
• in Spitzoid tumours concerning for more aggressive behaviour
P16Garrido‐Ruiz MC, et al. Mod Pathol. 2010;23(9):1215‐24.
Kapur P, et al. ModPathol. 2005;18(2):197‐204.
Melanoma Genetics
Rapid progress over past 15 years:
• genomic instability of melanoma
• development of diagnostic FISH assayp g y
• mutational analysis and targeted therapy

02/06/2015
10
Melanoma Genetics
Comparative Genomic Hybridisation
• Frequent chromosomal aberrations in melanoma (>95%) in contrast to benign naevi
• 13 regions on 8 chromosomes
Bastian BC, et al. Am J Pathol 2003;163(5):1765‐70.
Melanoma Genetics
Melanoma FISH
Using CGH data a panel of 4 probes was found most informative:
• Centromere chromosome 6
• Gain of CCND1 (11q13)( q )
• Gain of RREB1 (6p25)
• Loss of MYB (6q23)
Sensitivity of 87% and specificity of 96%
Recent inclusion of probe for 9p21 as marker of prognosis
Technically demanding and expensive
Fluorescence In Situ Hybridization as an Ancillary Tool in the Diagnosis of Ambiguous Melanocytic Neoplasms: A Review of 804 Cases.
North, Jeffrey; Garrido, Maria; Kolaitis, Nicholas; LeBoit, Philip; McCalmont, Timothy; Bastian, Boris
American Journal of Surgical Pathology. 38(6):824‐831, June 2014.DOI: 10.1097/PAS.0000000000000189
© 2014 by Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
FIGURE 9 . Polyploidy in FISH. All 4 FISH probes showing >2 signals. Red‐6p25, Green‐11q13, Yellow‐6q23, Aqua‐centr omere 6.
Mutational Spectrum in Melanoma
Whole exome sequencing: numerous (>1,000) gene mutations
Challenge: Driver vsbystander mutations
Inactivating mutations inCDKN2a (40‐80%)PTEN (30‐70%)
Promoter mutations inTERT gene
High rate of mutations inBRAF in 50% (vemurafenib)NRAS in 20% (MEK inhibitor MEK162)CKIT in 10% (imatinib)GNAQ/GNA11

02/06/2015
11
Lentigo Maligna
Vulval Melanoma
AcralMelanoma
Uveal Melanoma
Mutations in GNAQ and GNA11 gene mutations
Additional BAP1 mutations may predict more aggressive behaviour
GANQ and GNA11 gene mutations also observed in blue naevi and blue naevus‐like melanoma (“malignant blue naevus”)
Van Raamsdonk CD, et al. Nature. 2009;457(7229):599‐602.Van Raamsdonk CD, et al. N Engl J Med. 2010;363(23):2191‐9.
Familial Melanoma
CDKN2a
Familial atypical multiple mole melanoma (FAMM)/Dysplastic nevus syndromenevus syndrome
40% of familial melanoma
Autosomal dominant
Multiple atypical naevi and melanoma
Superficial spreading and nodular melanoma
Familial Melanoma
POT‐1
Recently described
Loss of function mutations in the Protection of telomers‐1 (POT‐1) gene on chromosome 7q31
4% of familial melanoma
Also linked to chronic lymphocytic leukemia (CLL)
Robles‐Espinoza CD, et al. Nat Genet. 2014;46(5):478‐81. Shi J, et al. Nat Genet. 2014;46(5):482‐6.
02/06/2015
12
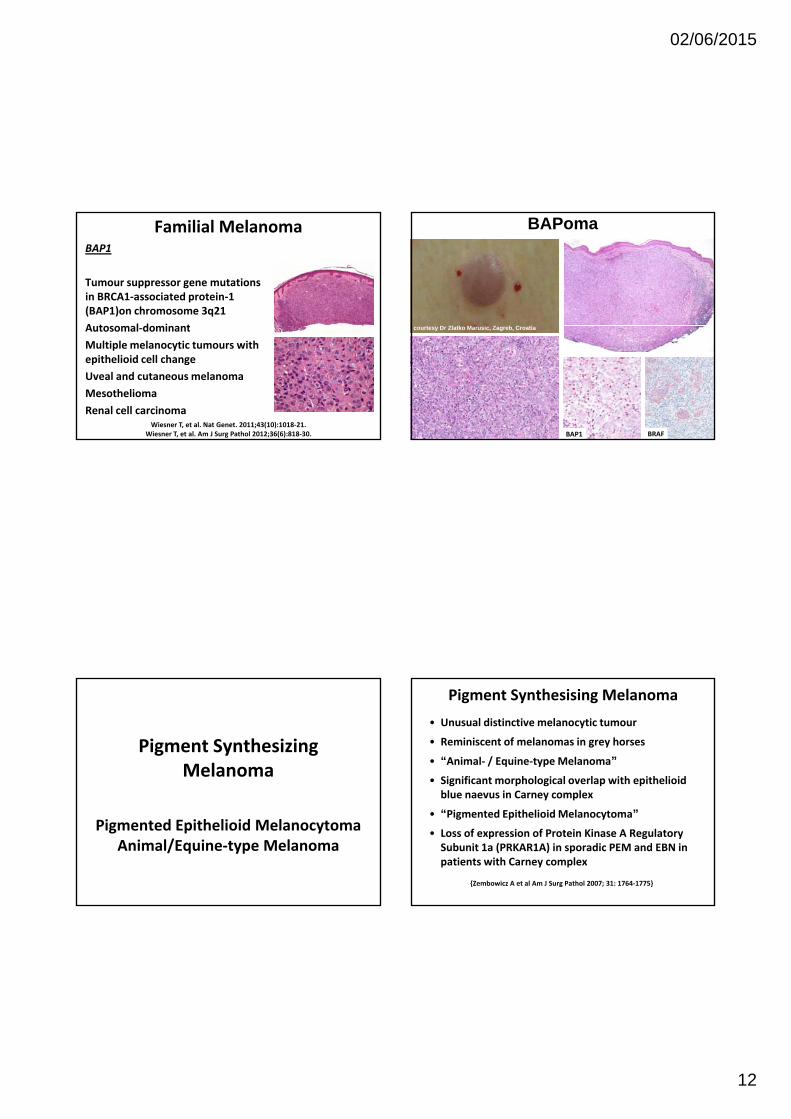
Familial MelanomaBAP1
Tumour suppressor gene mutations in BRCA1‐associated protein‐1 (BAP1)on chromosome 3q21
A t l d i tAutosomal‐dominant
Multiple melanocytic tumours with epithelioid cell change
Uveal and cutaneous melanoma
Mesothelioma
Renal cell carcinomaWiesner T, et al. Nat Genet. 2011;43(10):1018‐21.
Wiesner T, et al. Am J Surg Pathol 2012;36(6):818‐30.
C
BAPoma
courtesy Dr Zlatko Marusic, Zagreb, Croatia
BAP1 BRAF
Pigment Synthesizing Melanoma
Pigmented Epithelioid MelanocytomaAnimal/Equine‐type Melanoma
Pigment Synthesising Melanoma
• Unusual distinctive melanocytic tumour
• Reminiscent of melanomas in grey horses
• “Animal‐ / Equine‐type Melanoma”
• Significant morphological overlap with epithelioid bl i C lblue naevus in Carney complex
• “Pigmented Epithelioid Melanocytoma”
• Loss of expression of Protein Kinase A Regulatory Subunit 1a (PRKAR1A) in sporadic PEM and EBN in patients with Carney complex
{Zembowicz A et al Am J Surg Pathol 2007; 31: 1764‐1775}

02/06/2015
13
Pigment Synthesising Melanoma‐Clinical Presentation‐
• Deeply pigmented tumours
• Extremities, head & neck, trunk
M it l it• Mucosa, genital sites
• Young adults (20‐30 yrs)
• Wide age range including congenital onset
• M=F

02/06/2015
14
9 year old boy with a pigmented lesion on the left superior deltoid area

02/06/2015
15
02/06/2015
16
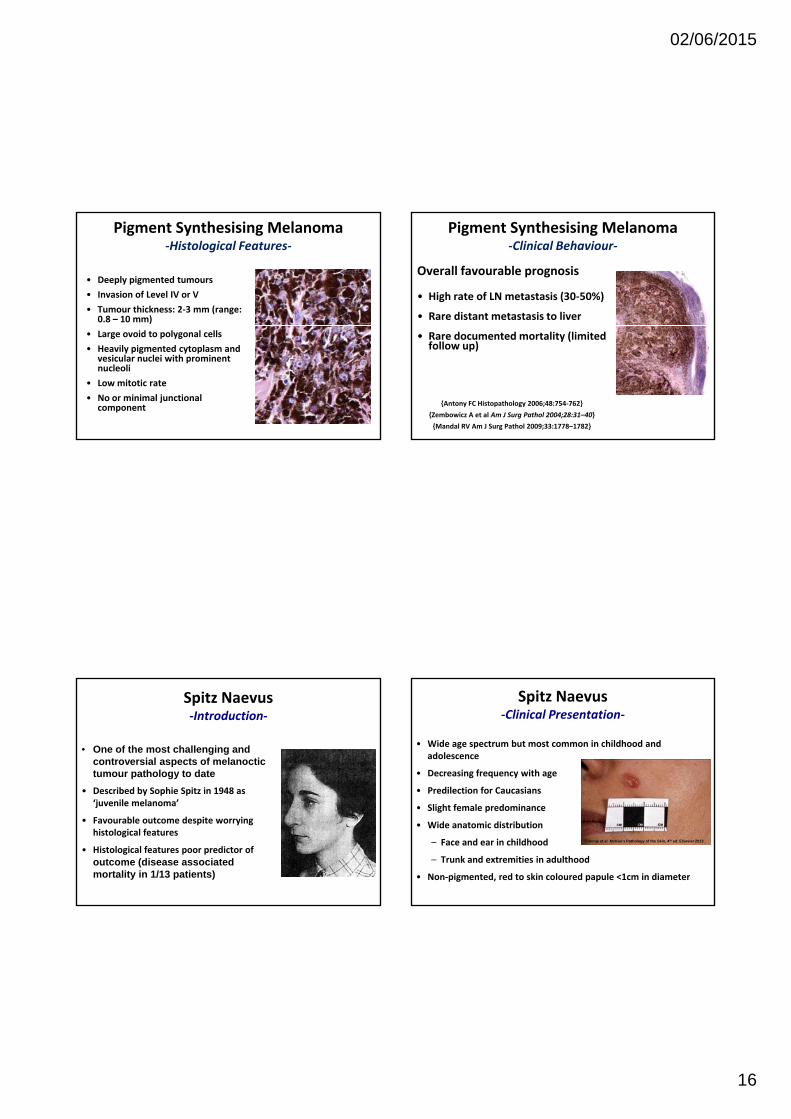
Pigment Synthesising Melanoma‐Histological Features‐
• Deeply pigmented tumours
• Invasion of Level IV or V
• Tumour thickness: 2‐3 mm (range: 0.8 – 10 mm)
• Large ovoid to polygonal cells
• Heavily pigmented cytoplasm and vesicular nuclei with prominent nucleoli
• Low mitotic rate
• No or minimal junctionalcomponent
Pigment Synthesising Melanoma‐Clinical Behaviour‐
Overall favourable prognosis
• High rate of LN metastasis (30‐50%)
• Rare distant metastasis to liver
• Rare documented mortality (limited follow up)
{Antony FC Histopathology 2006;48:754‐762}
{Zembowicz A et al Am J Surg Pathol 2004;28:31–40}
{Mandal RV Am J Surg Pathol 2009;33:1778–1782}
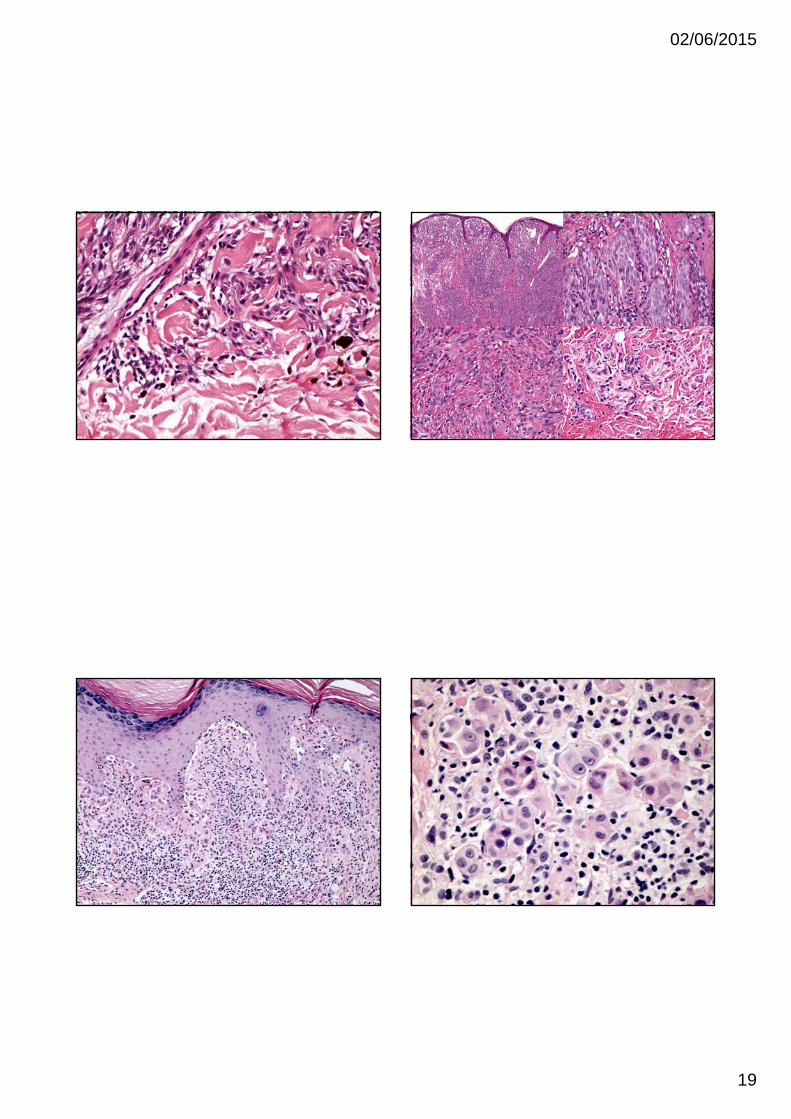
Spitz Naevus‐Introduction‐
• One of the most challenging and controversial aspects of melanoctictumour pathology to date
• Described by Sophie Spitz in 1948 as• Described by Sophie Spitz in 1948 as ‘juvenile melanoma’
• Favourable outcome despite worrying histological features
• Histological features poor predictor of outcome (disease associated mortality in 1/13 patients)
Spitz Naevus‐Clinical Presentation‐
• Wide age spectrum but most common in childhood and adolescence
• Decreasing frequency with age
• Predilection for CaucasiansPredilection for Caucasians
• Slight female predominance
• Wide anatomic distribution
– Face and ear in childhood
– Trunk and extremities in adulthood
• Non‐pigmented, red to skin coloured papule <1cm in diameter
Calonje et al. McKee’s Pathology of the Skin, 4th ed. Elsevier 2013

02/06/2015
17
Spitz Naevus‐Problems‐
65 years after Sophie Spitz’ publication
– Poor insight into the biology of Spitz tumours
– Difficult to predict behaviour
Classification into
– Spitz Naevus
– Atypical Spitz Tumour/Spitz Tumour of Uncertain Malignant Potential
– Spitzoid Melanoma
Spitz Naevus‐Genetics‐
• Lack of mutation in NRAS, KIT, GNAQ, GNA11
• HRAS mutations in ~10% (desmoplastic SN)
H l f BAP1 d BRAF t ti• Homozygous loss of BAP1 and BRAF mutation
• Kinase fusions involving ROS1, NTRK1, ALK, BRAF, RET in ~50% Spitz Tumours
Busam KJ, et al. Clinical and pathologic findings of Spitz nevi and atypical Spitz tumors with ALK fusions. Am J SurgPathol. 2014;38(7):925-33.Wiesner T, et al. Kinase fusions are frequent in Spitz tumours and spitzoid melanomas. Nat Commun. 2014;5:3116.Wiesner T, et al. A distinct subset of atypical Spitz tumors is characterized by BRAF mutation and loss of BAP1 expression. Am J Surg Pathol. 2012;36:818–30.Wiesner T, et al. Germline mutations in BAP1 predispose to melanocytic tumors. Nat Genet. 2011;43:1018–21.Bastian BC, LeBoit PE, Pinkel D. Mutations and copy number increase of HRAS in Spitz nevi with distinctive histopathological features. Am J Pathol. 2000;157:967–72.

02/06/2015
18
02/06/2015
19
02/06/2015
20
S100 Melan a
cyclin D1 MIB1p16 p21

02/06/2015
21
Morphological Spectrum of Spitz Naevi
• Pagetoid Spitz
• Acral Spitz
• Desmoplastic Spitz
• Pigmented Spitz and Spindle Cell Naevus (Reed)• Pigmented Spitz and Spindle Cell Naevus (Reed)
• Deep Penetrating Naevus
Atypical Spitz Naevus/Tumour/Stump
Spitzoid Melanoma
Desmoplastic Spitz Naevus
• Brown/erythematous papules
• <1cm
• Adulthood
• F>M
• Extremities
• HRAS mutations

02/06/2015
22
Kiuru M, Patel RM, Busam KJ. J Cutan Pathol. 2012;39(10):940-4.
02/06/2015
23
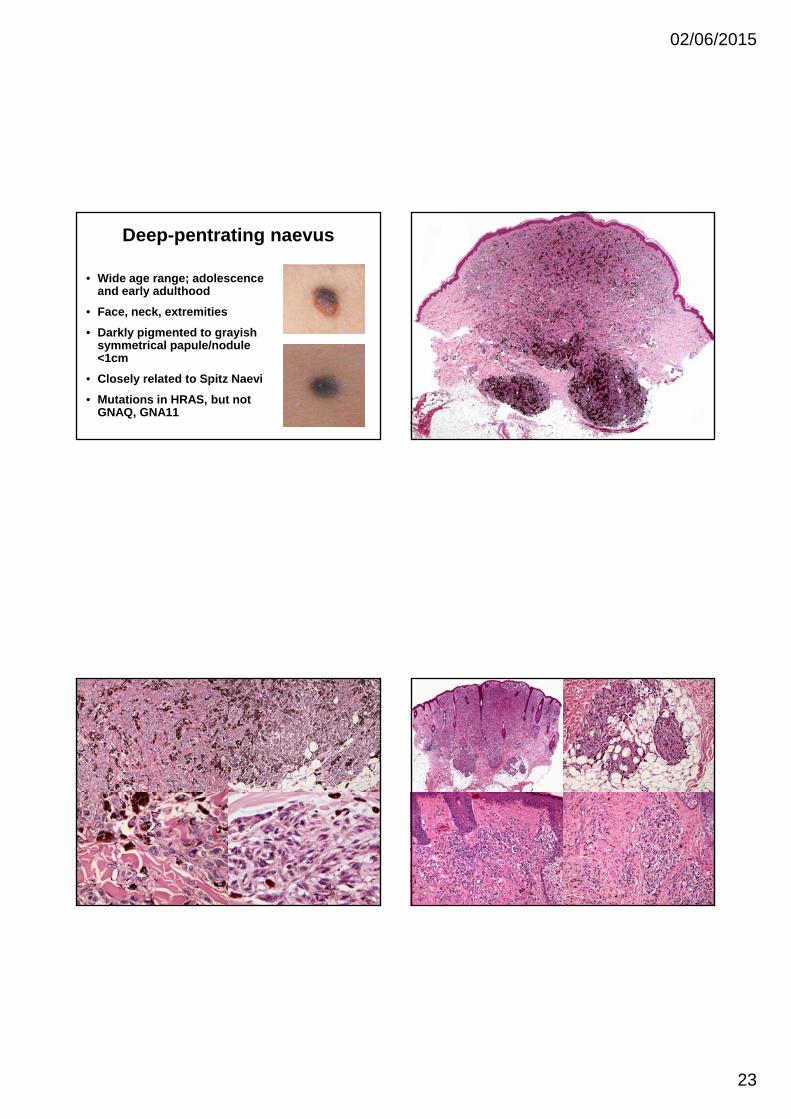
Deep-pentrating naevus
• Wide age range; adolescence and early adulthood
• Face, neck, extremities
• Darkly pigmented to grayish symmetrical papule/nodule <1cm
• Closely related to Spitz Naevi
• Mutations in HRAS, but not GNAQ, GNA11

02/06/2015
24
Characteristic epithelioidmelanocytic tumours with Spitzoid features
Loss of BAP1 expression
BAPoma
courtesy Dr Zlatko Marusic, Zagreb, Croatia
Additional BRAF mutation
Familial or sporadic
Also seen in AST and cutaneous and uvealmelanoma
Wiesner T, et al. Am J Surg Pathol. 2012; 36: 818-30.Wiesner T, et al. Nat Genet. 2011 28; 43: 1018-21.
courtesy Dr Zlatko Marusic, Zagreb, Croatia
M, 28 Jahre, Gesicht
BRAF BAP1

02/06/2015
25
Spitz Naevus with Kinase Fusion
ALK1
Yeh I, et al. Am J Surg Pathol. 2015;39(5):581‐91.Busam KJ, et al. Am J Surg Pathol. 2014;38(7):925‐33.
Clinical, Histopathologic, and Genomic Features of Spitz Tumors With ALK Fusions.Yeh, Iwei; MD, PhD; de la Fouchardiere, Arnaud; MD, PhD; Pissaloux, Daniel; Mully, Thaddeus; Garrido, Maria; MD, PhD; Vemula, Swapna; Busam, Klaus; LeBoit, Philip; McCalmont, Timothy; Bastian, Boris; MD, PhD
American Journal of Surgical Pathology. 39(5):581‐591, May 2015.DOI: 10.1097/PAS.0000000000000387
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved. Published by Lippincott Williams & Wilkins, Inc.2
FIGURE 2 . Disruption of ALK identified by FISH. A, Unbalanced rearrangement of the ALK gene, with preservation of the 3' signal (red) and the remaining intact ALK gene (1 juxtaposed green and orange signal). B, Balanced rearrangement of the ALK gene with separated orange and green signals compared with the remaining intact locus. C, Amplification of the 3' oncogenic signal (1 or 2 fusion signals + numerous clustered orange signals).
Atypical Spitz Tumour/Spitzoid Melanoma
• Poorly defined criteria with poor i t binterobserveragreement
• Constellation of features
Atypical Spitz Tumour/Spitzoid Melanoma-Concerning Features-
Architecture:
Diameter in mm (>10 mm)
Depth in mm (involvement of subcutaneous fat)
Ulceration
Cytology:
High nuclear to cytoplasmic ratios
Loss of delicate or dispersedchromatin patterns
Thickening of nuclear membranes
Poor circumscription
Diffuse Pagetoid spread
High cellular density
Lack of zonation and maturation
Asymmetry
Few or no dull pink (Kamino) bodies
Hyperchromatism
Large nucleoli
Proliferation:
Significant mitotic rate
Deep/marginal mitoses
Increased mib-1 proliferation index
Modified from: Barnhill RL. Modern Pathology. 2006; 19: S21-S33

02/06/2015
26

02/06/2015
27
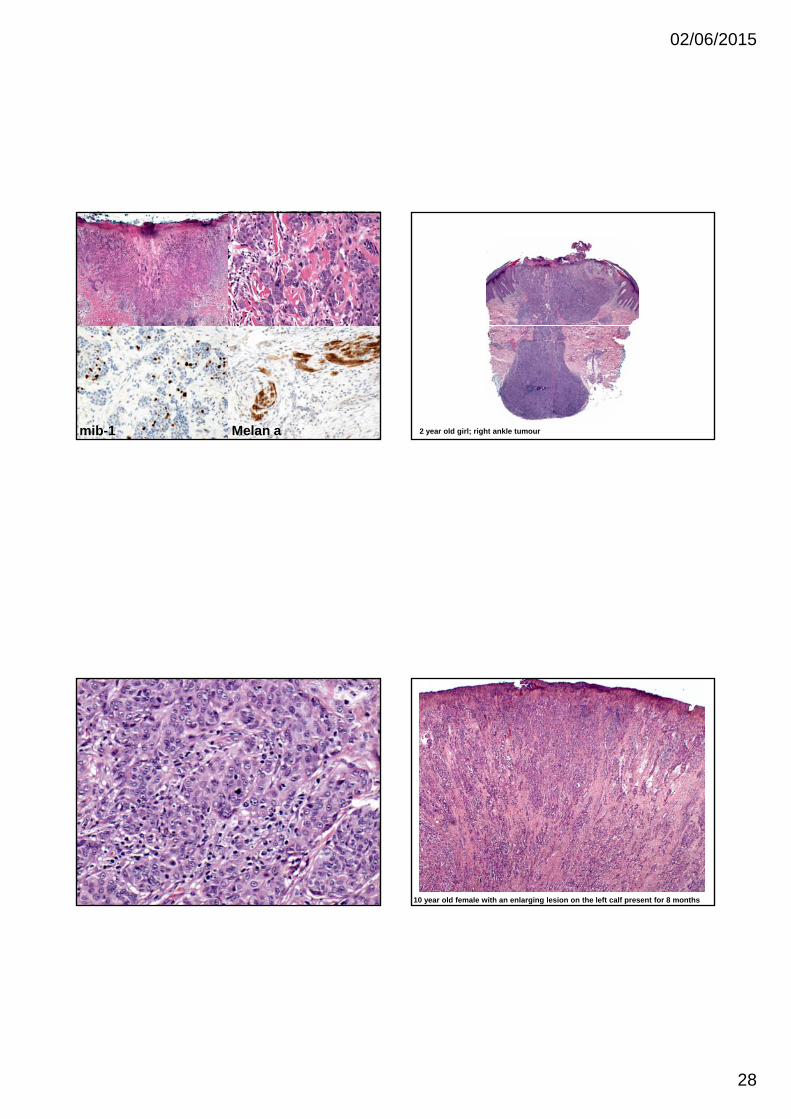
mib-1
02/06/2015
28
mib-1 Melan a 2 year old girl; right ankle tumour
10 year old female with an enlarging lesion on the left calf present for 8 months

02/06/2015
29
Nodular M Sp M PSM SSM Nevoid M
n 21 21 3 12 4
age (yrs) 11 10 9 16 16
site H&N>E>T E>H&N>T H&N E>T E>T
thick (mm) 4 0 3 7 3 4 1 0 1 1
Melanoma in Children and Adolescents
thick (mm) 4.0 3.7 3.4 1.0 1.1
ulceration 50% 24% nil 0.8% nil
necrosis 25% nil nil nil nil
mitoses 6.5/mm2 5/mm2 1/mm2 1/mm2 2.5/mm2
LN met 57% 24% 100% nil 30%
Dist met 50% nil nil nil nil
mortality 40% nil nil nil nil

02/06/2015
30
AST/Spitzoid Melanoma-Prognose-
In young children (<10 years):
• Favourable behaviour
• Risk for involvement of loco-regional lymph nodes
• Rare disseminated disease and mortality
• Sentinel lymph node biopsynot helpful and should beavoided
Lallas A, eta l. Lancet Oncol. 2014;15(4):e178‐83. doi: 10.1016/S1470‐2045(13)70608‐9.Duncan LM. Lancet Oncol. 2014;15(4):377‐8.
Spitzoid Melanoma
• No firm established diagnostic criteria
• Distinction from Atypical Spitz Tumour largely arbitrary
• Best avoided in young patients
AST/Spitzoid Melanoma-Genetics-
Homozygous but not heterozygous 9p21 deletion associated with more aggressive behaviourbe a ou
Yazdan P, et al. Comparative analysis of atypical spitz tumors with heterozygous versus homozygous 9p21 deletions for clinical outcomes, histomorphology, BRAF mutation, and p16 expression. Am J Surg Pathol. 2014May;38(5):638-45.Gerami P, Cooper C, Bajaj S, Wagner A, Fullen D, Busam K, Scolyer RA, Xu X,Elder DE, et al. Outcomes of atypical spitz tumors with chromosomal copy number aberrations and conventional melanomas in children. Am J Surg Pathol. 2013 Sep;37(9):1387-94.Gerami P, et al. Risk assessment for atypical spitzoid melanocytic neoplasms using FISH to identify chromosomal copy number aberrations. Am J Surg Pathol. 2013;37(5):676-84.