introduction to rls
DESCRIPTION
bahanTRANSCRIPT
Introduction to RLSHistoryThe term Restless Leg Syndrome was coined by Professor Karl-Axel Ekbom in 1944 and is therefore also known as "Ekbom's disease". Ekbom studied medicine at the Karolinska Institute and later became the first Professor and head of the department of neurology at Uppsala university hospital. In his 1945 publication entitled "Restless Legs", Ekbom described the disease and presented eight cases.
Ekbom was not the first to describe the disease. The earliest documentation was appears to be by Thomas Willis, a 17th century English physician of Charles II. Willis studied at the private school of Edward Sylvester in Oxford and is probably most famous for his publication Cerebri anatome, published in 1664, a foundational text on the anatomy of the cerebral system. This book was the first to describe the term reflex action and the Circle of Willis was outlined and understood.
In 1672 described what may have been RLS. Willis wrote in a chapter entitled "Instructions for curing the Watching evil":
.......Wherefore to some, when being in bed they betake themselves to sleep, presently in the arms and legs. Leaping and contractions of the tendons and so great a restlessness and tossing of the members ensure, that the diseased are no more able to sleep, than if they were in the place of the greatest torture!....
Willis went on to think that the diseases originated in the spinal cord and was a product of spinal irritation and used opiates as his therapy of choice.
Sometimes since I was advised with for a lady of quality, who in the night was hindered from sleep by reason of these spasmodic effects which came upon her only twice a week; she took afterward daily for almost three months, receiving no injury thereby, either on the brain or about any other function, and
when while by the use of other remedies; the dyscrasia of the blood and nervous juice being corrected, the animal spirits became more benign and mild. She afterward leaving wholly the opium was able to sleep indifferently well!!
What is restless legs?Restless legs syndrome (RLS) is a neurological disorder with unpleasant sensations in the legs and an uncontrollable urge to move when at rest to try to relieve these feelings. RLS sensations are often described by people as burning, creeping, tugging, or like insects crawling inside the legs, and a wide variety of descriptions is included in diagnostic criteria. Often called paresthesias (abnormal sensations) or dysesthesias (unpleasant abnormal sensations), the sensations range in severity from uncomfortable to irritating to painful.
Lying down and trying to relax activates the symptoms or makes them worse. Most people with RLS have difficulty falling asleep and staying asleep. People are exhausted with daytime fatigue and sleepiness. Many people with RLS report that job, personal relations, and activities of daily living are strongly affected as a result of this exhaustion, because they are unable to concentrate, or have impaired memory.
RLS probably affects 5-10% of people, but may be underdiagnosed and, in some cases, misdiagnosed. Some people with RLS will not seek medical attention, believing that they will not be taken seriously, that their symptoms are too mild, or that their condition is not treatable. Some physicians wrongly attribute the symptoms to nervousness, insomnia, stress, arthritis, muscle cramps, or aging.
RLS occurs in women and men, probably slightly more often in women. Although the syndrome may begin at any age, even as early as infancy, most patients who are severely affected are middle-aged or older. In addition, severity appears to increase with age. Older patients experience symptoms more frequently and for longer.
Most people with RLS also experience a more common condition known as periodic limb movement disorder (PLMD). PLMD is involuntary leg twitching or jerking movements during sleep that typically occur every 10 to 60 seconds, in periods or throughout the night. The symptoms cause repeated awakening and disrupted sleep. Unlike RLS, the movements caused by PLMD are involuntary-people have no control over them. Although many patients with RLS also develop PLMD, most people with PLMD do not experience RLS. Like RLS, the cause of PLMD is unknown.
What are the symptoms of restless legs?People with RLS feel uncomfortable sensations in their legs, especially when sitting or lying down, often more in the evening than the day, with an irresistible urge to move about. Although the sensations can occur on just one side of the body, most often they affect both sides.
Because moving the legs (or other affected parts of the body) relieves the discomfort, people with RLS often keep their legs moving to reduce the unpleasant sensations. They may pace the floor, constantly move their legs while sitting, and toss and turn in bed.
Most people find the symptoms to be less noticeable during the day and more pronounced in the evening or at night, especially going to sleep. For many people, the symptoms disappear by early morning, allowing for more refreshing sleep at that time. Other triggering situations are periods of inactivity such as long journeys, or other behaviours that reduce movement.
The symptoms of RLS vary in severity and duration from person to person. Mild RLS occurs episodically, with only mild disruption of sleep onset, and causes little distress. In moderately severe cases, symptoms occur only once or twice a week but result in significant delay of sleep onset, with some disruption of daytime function. In severe cases of RLS, the symptoms occur more than twice a week and result in burdensome interruption of sleep and impairment of daytime function. There is a standard symptom scoring system.
What causes RLS?In most cases, the cause of RLS is unknown (and then doctors call it idiopathic RLS). Family history of the condition is common, perhaps in half the sufferers. People with familial RLS tend to be younger when symptoms start and have a slower progression of the condition.
In other cases, RLS appears to be related to the following factors or conditions, although researchers do not yet know if these factors actually cause RLS.
People with low iron levels or anaemia may be prone to developing RLS. Once iron levels or anaemia is corrected, patients may see a reduction in symptoms.
Chronic diseases such as kidney failure, diabetes, Parkinson's disease, and peripheral neuropathy are associated with RLS. Treating the underlying condition often provides relief from RLS symptoms.
Some pregnant women experience RLS, especially in their last trimester. For most of these women, symptoms usually disappear within four weeks after delivery.
Certain medications-such as antinausea drugs (prochlorperazine or metoclopramide), antiseizure drugs (phenytoin or droperidol), antipsychotic drugs (haloperidol or phenothiazine derivatives), and some cold and allergy medications-may aggravate symptoms. Patients can talk with their physicians about the possibility of changing medications.
How is RLS diagnosed?
Currently, there is no single diagnostic test for RLS. The disorder is diagnosed clinically by evaluating the patient's history and symptoms. In 1995, the International Restless Legs Syndrome Study Group identified four basic criteria for diagnosing RLS:
1. a desire to move the limbs, often associated with paresthesias or dysesthesias,
2. symptoms that are worse or present only during rest and are partially or temporarily relieved by activity,
3. motor restlessness, and4. nocturnal worsening of symptoms.
A 10-question scoring system is available for RLS diagnosis and severity scoring.
A more detailed description of diagnostic criteria in adults, children, and cognitively impaired adults is available.
How is RLS treated?Relief on movement is generally only temporary. However, RLS can be controlled by finding any possible underlying disorder. Often, treating the associated medical condition, like anaemia, peripheral neuropathy or diabetes, will alleviate many symptoms. For patients with idiopathic RLS, treatment is directed toward relieving symptoms.
For those with mild to moderate symptoms, prevention is key, and many physicians suggest certain lifestyle changes and activities to reduce or eliminate symptoms. Decreased use of caffeine, alcohol, and tobacco may provide some relief. Doctors may suggest the use of supplements to correct deficiencies in iron, folate, and magnesium. Studies also have shown that maintaining a regular sleep pattern can reduce symptoms. Some individuals, finding that RLS symptoms are lower in the early morning, change their sleep patterns. Others have found that a program of regular moderate exercise helps them sleep better. Taking a hot bath, massaging the legs, or using a heating pad or ice pack can help relieve symptoms in some patients. Although many patients find some relief with such measures, rarely do these efforts completely eliminate symptoms, and for many of these measures there is only anecdotal evidence that they work.
A variety of drugs have been tried, often not in large or long trials. Some seem to work well in reducing periodic leg movements, or daytime
tiredness, or improving sleep, or reducing RLS symptom severity, but there is no magic bullet as yet.
http://www.medicine.ox.ac.uk/bandolier/booth/RLS/RLSintro.html
Restless legs syndrome and related disorders
DescriptionAn in-depth report on the causes, diagnosis, treatment, and prevention of RLS.
Alternative NamesEkbom's syndrome
HighlightsOverview
Restless leg syndrome (RLS) can be a temporary problem (such as during pregnancy) or a chronic, long-term issue. It can develop from several medical conditions and genetic risk factors.
The condition involves a feeling of "pulling, searing, drawing, tingling, bubbling, or crawling" beneath the skin, usually in the calf area. This causes an irresistible urge to move the legs. These sensations can sometimesaffect the thighs, feet, and sometimes even the arms. Treatment often includes over-the-counter remedies and lifestyle changes. Iron supplements may be recommended in cases where a lack of iron has been identified. Prescription medications can provide good relief of symptoms.
RLS and PLMD: Periodic limb movement disorder (PLMD) is a condition where leg muscles contract and jerk every
20 - 40 seconds during sleep. These movements may last less than 1 second, or as long as 10 seconds.
Unlike RLS, contractions in PLMD usually do not wake patients.
Four out of five people who have of RLS sufferers also report having PLMD, but only about a third of people with PLMD also have RLS.
New Treatment: An antiseizure agent, gabapentin enacarbil (Horizant), was approved by the Food and Drug
Administration (FDA) in 2011 for moderate-to-severe RLS. Common side effects included mild sleepiness and dizziness.
The drug rotigotine (Neupro) was withdrawn from the US in 2008 because of concerns about absorption of the medication from the skin patch. The issue has since been corrected and the drug was approved in April 2012 for treatment of moderate-to-severe RLS.
IntroductionRestless legs syndrome (RLS) is a poorly understood movement disorder that affects 3 - 15% of the general population. The problem can occur in both children and adults. Although effective treatments are available, RLS often goes undiagnosed.
Symptoms of RLS. The core symptom of RLS is an irresistible urge to move the legs (medically known as akathisia). Some people describe this symptom as a sense of unease and weariness in the lower leg. The sensations are aggravated by rest and relieved by movement. Specific characteristics of RLS include:
"Pulling, searing, drawing, tingling, bubbling, or crawling" beneath the skin, usually in the calf area, causing an irresistible urge to move the legs. These sensations can occur mostly in the lower legs, but they can sometimes affect the thighs, feet, and even the upper body. RLS-type symptoms may also occur in the arms. These may be the first symptoms of RLS in some people.
About 4 out of 5 patients with RLS also have semi-rhythmic movements during sleep, a condition called periodic limb movement disorder (PLMD). (See description below.)
Itching and pain, particularly aching pain, may be present.
Patients experience symptoms when they feel most relaxed and their legs are at rest. Symptoms usually occur at night when lying down. In more severe cases,symptoms also occur during the day while sitting.
Episodes of RLS usually develop between 10 p.m. and 4 a.m. Symptoms are often worse shortly after midnight and disappear by morning. If the condition becomes more severe, people may begin to have symptoms during the day, but the problem is always worse at night.
The unpleasant sensations and uncontrollable urge to move the legs often disturbs nighttime sleep. When the person tries to ignore the urge to move the legs, tension builds up until the legs jerk uncontrollably. Individuals who experience daytime symptoms may find it difficult to sit during air or car travel, or through classes or meetings.
Late-onset and Early-onset Forms. There appear to be two forms of RL -- early-onset and late-onset. Each form may have different characteristics:
People with early-onset RLS (occurring in the teenage years or earlier) tend to have a family history of the disorder. They usually have RLS without accompanying pain.
People with late-onset RLS usually do not have a family history of RLS. The condition is more likely to result from a problem with the nervous system. Symptoms may also include pain in the lower legs.
Periodic Limb Movement DisorderPeriodic limb movement disorder (PLMD) is also known as nocturnal myoclonus. PLMD symptoms include:
Nighttime episodes that usually peak near midnight (similar to the pattern in restless legs syndrome).
Contractions and jerking of the leg muscles every 20 - 40 seconds during sleep. These movements may last less than 1 second, or as long as 10 seconds.
PLMD usually does not wake patients. This condition is distinct from the brief and sudden movements that occur just as people are falling asleep; these brief jerking movements may interrupt sleep.
Four out of five people who have RLS also report having PLMD, but only a third of people with PLMD report having RLS.
While treatments for the two conditions are similar, PLMD is a separate syndrome. PLMD is also very common in narcolepsy, a sleep disorder that causes people to fall asleep suddenly and uncontrollably.
CausesThe main cause of RLS is unknown. Scientists are researching nervous system problems that may arise in either the spinal cord or the brain. One theory suggests that low levels of the brain chemical dopamine causes restless legs syndrome.
RLS may often have a genetic basis, particularly in those who develop it before age 40. Restless legs syndrome in older adults is less likely to be inherited.
The central nervous system includes the brain and spinal cord. The peripheral nervous system includes all peripheral nerves.
Genetic FactorsPeople with RLS often have a family history of the disorder. Researchers have detected at least six genetic factors that may play a part. Two of the genes are linked to spinal cord development. Although none of the genes has been associated
with dopamine or iron-regulating systems, these factors are considered likely causes of the condition.
Neurological AbnormalitiesDopamine and Neurologic Abnormalities in the Brain. Several studies support the theory that an imbalance in neurotransmitters (chemical messengers in the brain), notably dopamine, may play a part in RLS. Dopamine triggers numerous nerve impulses that affect muscle movement. The effect is similar to that seen in Parkinson's disease. In addition, drugs that increase dopamine levels treat both disorders. However, Parkinson's disease itself does not seem to increase the risk for RLS and RLS early in life does not increase the risk of Parkinson's later on.Neurologic Abnormalities in the Spine. Other research suggests that restless legs syndrome may be due to nerve impairment in the spinal cord. Researchers had thought that such abnormalities began in nerve pathways in the lower spine. However, some patients with RLS have symptoms in the arms, which indicates that the upper spine may also be involved.Neuropathy. Some experts suggest that RLS, particularly if it occurs in older adults, may be a form of neuropathy, which is an abnormality in the nervous system outside the spine and brain. So far, there is no evidence to support a cause and effect relationship between neuropathy and RLS.
Abnormalities of Iron MetabolismIron deficiency, even at a level too mild to cause anemia, has been linked to RLS in some people. Some research suggest that RLS in some people may be due to a problem with getting iron into cells that regulate dopamine in the brain. Some studies have reported RLS in a quarter to a third of people with low iron levels.
Deficiencies in CortisolOther research suggests that low levels of the hormone cortisol in the evening and early night hours may be related to restless leg
symptoms. Low-dose cortisol injections have reduced symptoms in some people. Causes of Periodic Limb Movement DisorderThe causes of PLMD are not clear. Some research suggests that it may be due to abnormalities in the autonomic nervous system, which regulates the involuntary actions of the smooth muscles, heart, and glands.
Risk FactorsRLS may affect 3 - 15% of the general population. It is more common in women than in men, and its frequency increases with age. The disorder affects an estimated 10 - 28% of adults older than age 65, however 4 in 10 patients have their first symptoms of RLS as teenagers.
An international study showed that 2% of children ages 8 - 17 have RLS symptoms. RLS may be more common than epilepsy and diabetes in children and teens.
Family HistoryAs many as two-thirds of people with restless legs syndrome (RLS) have a family history of the disorder. In people with a family history of the condition, RLS is more likely to occur before they turn 40. People who develop the condition at a later age are less likely to have a family history of RLS. RLS is also more common in people from northern and western Europe, adding support for the theory that some cases have a genetic basis.
Attention Deficit Hyperactivity DisorderRLS and PLMD in children are strongly associated with inattention and hyperactivity. Up to a quarter of children diagnosed with attention-deficit hyperactivity disorder (ADHD) may also have RLS, sleep apnea, and PLMD. These conditions may actually contribute to inattentiveness and hyperactivity. The disorders have much in common, including poor sleep habits, twitching, and the need to get up suddenly and
walk about frequently. Some evidence suggests that the link between the diseases may be a deficiency in the brain chemical dopamine.
PregnancyAbout 1 in 5 pregnant women report having RLS. The condition usually goes away within a month of delivery. RLS in pregnancy has been linked to deficiencies in iron and the B vitamin folate.
DialysisRestless legs syndrome is relatively common in people undergoing kidney dialysis. Up to two-thirds of patients report this problem. Symptoms often disappear after a kidney transplant.
Anxiety DisordersAnxiety can cause restlessness and agitation at night. These symptoms can cause restless legs syndrome or strongly resemble the condition.
Other Conditions Associated with Restless Legs SyndromeThe following medical conditions are also associated with restless legs syndrome, although the relationships are not clear. In some cases, these conditions may contribute to RLS. Others may have a common cause. In some cases, they may coexist due to other risk factors:
Osteoarthritis (degenerative joint disease). About three-quarters of patients with RLS also have osteoarthritis, a common condition affecting older adults.
Varicose veins. Varicose veins occur in about 1 in 7 patients with RLS.
Obesity
Diabetes. People with type 2 diabetes may have higher rates of secondary RLS. Nerve pain (neuropathy) related to their diabetes cannot fully explain the higher rate of RLS.
Hypertension
Hypothyroidism (a condition in which the thyroid gland does not make enough hormones)
Fibromyalgia (chronic pain of unknown cause)
Rheumatoid arthritis
Emphysema (a lung disease usually caused by smoking)
Chronic alcoholism
Sleep apnea (pauses in breathing during sleep) and snoring
Chronic headaches
Brain or spinal injuries
Many muscle and nerve disorders. Of particular interest is hereditary ataxia, a group of genetic diseases that affects the central nervous system and causes loss of motor control. Researchers believe that hereditary ataxia may supply clues to the genetic causes of RLS.
Osteoarthritis is a chronic disease of the joint cartilage and bone, once thought to result from "wear and tear" on a joint, although there are other causes such as trauma, and metabolic disorders. Joints appear swollen, are stiff and painful, and usually feel worse the more they are used throughout the day.
Click the icon to see an image of hypothyroidism.
Click the icon to see an image detailing fibromyalgia.
Click the icon to see an image detailing rheumatoid arthritis.
Click the icon to see an image detailing emphysema.
Environmental and Dietary FactorsSeveral environmental and dietary factors can trigger or worsen restless legs syndrome:
Iron deficiencies. People who are deficient in iron are at risk for restless legs syndrome, even if they do not have anemia
Folic acid or magnesium deficiencies
Smoking
Alcohol abuse
Caffeine (coffee drinking is specifically associated with PLMD)
Stress
Fatigue
Prolonged exposure to cold
MedicationsDrugs that worsen or provoke RLS include:
Antidepressants
Antipsychotic drugs
Anti-nausea drugs
Calcium channel blockers (mostly used to treat high blood pressure)
Metoclopramide (used to treat various digestive diseases)
Antihistamines
Oral decongestants
Diuretics
Asthma drugs
Spinal anesthesia (anesthesia-induced restless legs syndrome typically disappears on its own within several months)
Risk Factors for Periodic Limb Movement DisorderAbout 6% of the general population has PLMD. However, the prevalence in older adults is much higher, reaching almost 60%. Studies suggest that PLMD may be especially common in elderly women. As with RLS, there are many conditions are associated with PLMD. They include sleep apnea, spinal cord injuries, stroke, narcolepsy, and diseases that destroy nerves or the brain over time. Certain drugs, including some antidepressants and anti-seizure medications, may also contribute to PLMD.
ComplicationsRLS rarely results in any serious consequences. However, recurring severe symptoms may cause considerable mental
distress, loss of sleep, and daytime sleepiness. Because the condition is worse while resting, people with severe RLS may avoid activities that involve extended periods of sitting, such as attending movies or traveling long distances.
Sleep DeprivationInability to sleep during the night due to RLS symptoms and subsequent daytime sleepiness can cause mood changes. Lack of sleep can also contribute to workplace errors and car crashes.
Effect on Daily Performance and Activities. Studies suggest that sleeplessness has a negative effect on the ability to function while awake. Areas that can be affected include:
Concentration. Loss of deep sleep appears to impair the brain's ability to process information.
Task performance. Missing several hours of sleep every night over the course of a week can negatively affect a person's ability to function. It also affects mood. In fact, people deprived of sleep show lowered performance levels on a par with those of people who are intoxicated.
Learning. The extent to which sleeplessness impairs learning is unclear. Some studies have reported problems in memorization. Other studies, however, have found no differences in test scores between people with temporary sleep loss and those with regular sleep cycles.
Psychiatric EffectsPeople with restless legs syndrome are more apt to suffer problems such as social isolation, frequent daytime headaches, and depression. The also complain of lower sex drive and other problems related to insufficient sleep.
RLS can contribute to insomnia. Insomnia itself can increase the activity of hormones and pathways in the brain that produce emotional problems. Even modest changes in waking and sleeping patterns can have significant effects on a person's mood. In some cases, ongoing insomnia may even predict mood disorders in the future.
It is not clear if RLS is responsible for mood problems or if anxiety or depression contributes to RLS. Anxiety can cause agitation and leg restlessness that resemble RLS. Depression and RLS symptoms also overlap. In addition, certain types of antidepressant drugs, such as seratonin reuptake inhibitors, can increase periodic limb movements during sleep.
DiagnosisA diagnosis of restless legs syndrome often relies mainly on the patient's description of symptoms. The first step in diagnosis is usually to gather information on a person's sleep and personal history. The doctor may ask the following questions:
How would you describe your sleep problem?
How long have you had this sleep problem? How long does it take you to fall asleep?
How many times a week does the problem occur?
How restful is your sleep?
What do your leg problems feel like (such as cramps, twitching, and crawling feelings)?
What is your sleep environment like? Noisy? Not dark enough?
What medications are you taking (including the use of antidepressants and self-medications -- such as herbs, alcohol, and over-the-counter or prescription drugs)?
Are you taking or withdrawing from stimulants, such as coffee or tobacco? How much alcohol do you drink per day?
What stresses or emotional factors may be present in your life? Have you experienced any significant life changes?
Do you snore or gasp during sleep? (This may be an indication of sleep apnea. Sleep apnea is a condition in which breathing stops for short periods many times during the night. It may worsen symptoms of restless legs syndrome or insomnia.)
If you have a bed partner, does he or she notice that you have jerking legs, interrupted breathing, or thrashing while you sleep?
Are you a shift worker?
Do you have a family history of RLS or periodic movement limb disorder, "growing pains" at night, or night walking?
Keeping a Record of Sleep. To help answer these questions, the patient may need to keep a sleep diary for 2 weeks. The patient should record all sleep-related information, including responses to the questions listed above described on a daily basis. Using an extended-play audio or videotape to record sleep behavior can be very helpful in diagnosing sleep apnea. A bed partner can help provide information based on observations of the patient's sleep behavior.
Sleep Disorders CentersSome patients may need to consult a sleep specialist or go to a sleep disorders center in order for the problem to be diagnosed. At most centers, patients undergo in-depth testing supervised by a team of consultants from various specialties, who can provide both physical and psychiatric evaluations. Centers should be accredited by the American Academy of Sleep Medicine.
Signs that may indicate the need for a sleep disorders center are: Insomnia due to psychological disorders
Sleeping problems due to substance abuse
Snoring and sudden awakening with gasping for breath (possible sleep apnea)
Severe restless legs syndrome
Persistent daytime sleepiness
Sudden episodes of falling asleep during the day (possible narcolepsy)
PolysomnographyOvernight polysomnography involves a series of tests to measure different functions during sleep. This type of evaluation is typically performed in a sleep center. It can help rule out sleep apnea or evaluate the effectiveness of RLS treatments.
To undergo the test, the patient arrives about 2 hours before bedtime without having made any changes in daily habits. Polysomnography electronically monitors the patient through the various sleep stages. Polysomnography tracks the following:
Brain waves
Body movements
Breathing
Heart rate
Eye movements
Changes in breathing and blood levels of oxygen
ActigraphyActigraphy uses a small wristwatch-like device (such as Actiwatch) worn on the wrist or ankle. The device monitors or sleep quality in people suspected of having RLS, PLMD, insomnia, sleep apnea, and other sleep-related conditions. It measures and records muscle movements during sleep. For example, with PLMD, actigraphy can provide information on how long movements last and the number of times they occur. It can also track whether PLMD occurs in both legs at the same time, and the effect it has on sleep. Actigraphy is not as accurate as polysomnography because it cannot measure all the biological effects of sleep. It is more accurate than a sleep log, however, and very helpful for recording long periods of sleep.
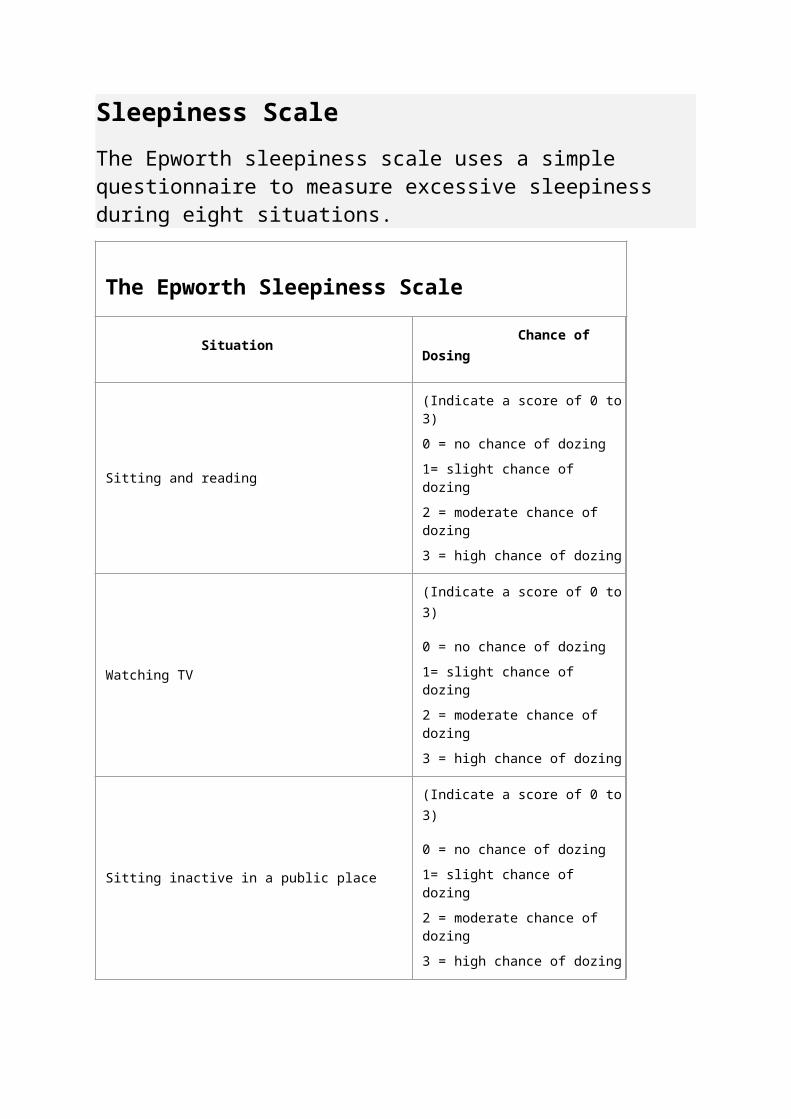
Sleepiness ScaleThe Epworth sleepiness scale uses a simple questionnaire to measure excessive sleepiness during eight situations.
The Epworth Sleepiness Scale
Situation Chance of Dosing
Sitting and reading
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Watching TV
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Sitting inactive in a public place (Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
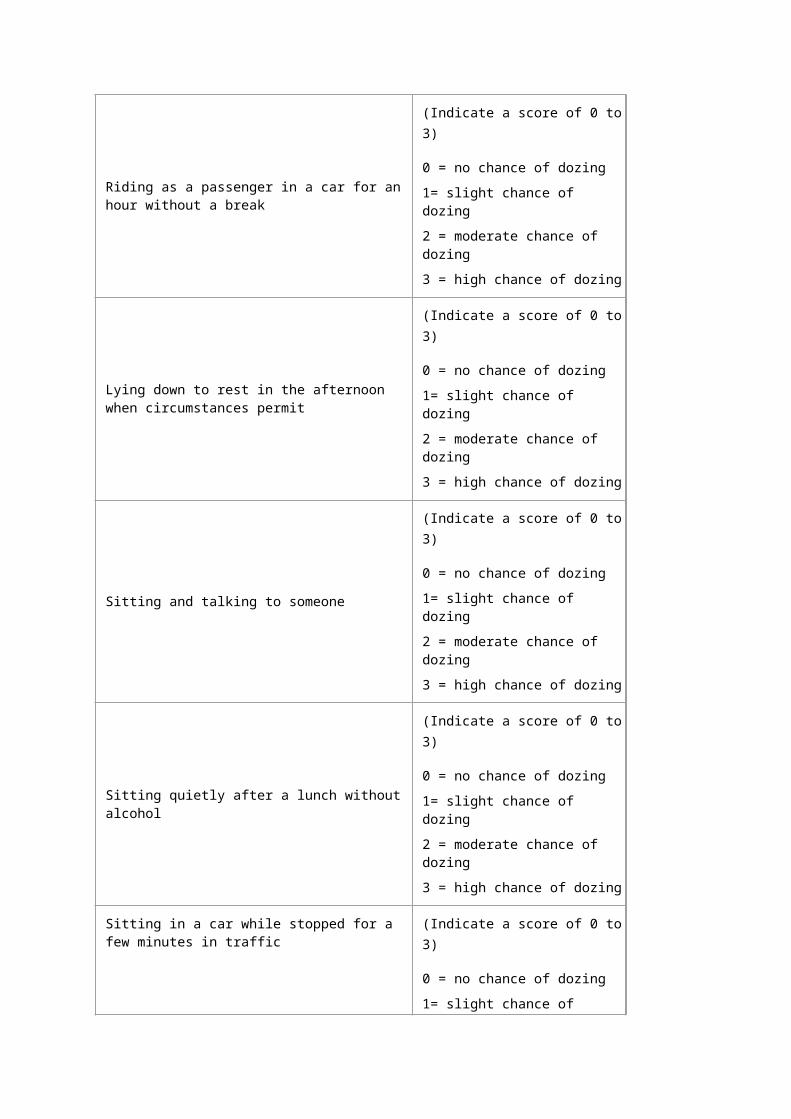
Riding as a passenger in a car for an hour without a break
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Lying down to rest in the afternoon when circumstances permit
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Sitting and talking to someone
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Sitting quietly after a lunch without alcohol
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
Sitting in a car while stopped for a few minutes in traffic
(Indicate a score of 0 to 3)
0 = no chance of dozing
1= slight chance of dozing
2 = moderate chance of dozing
3 = high chance of dozing
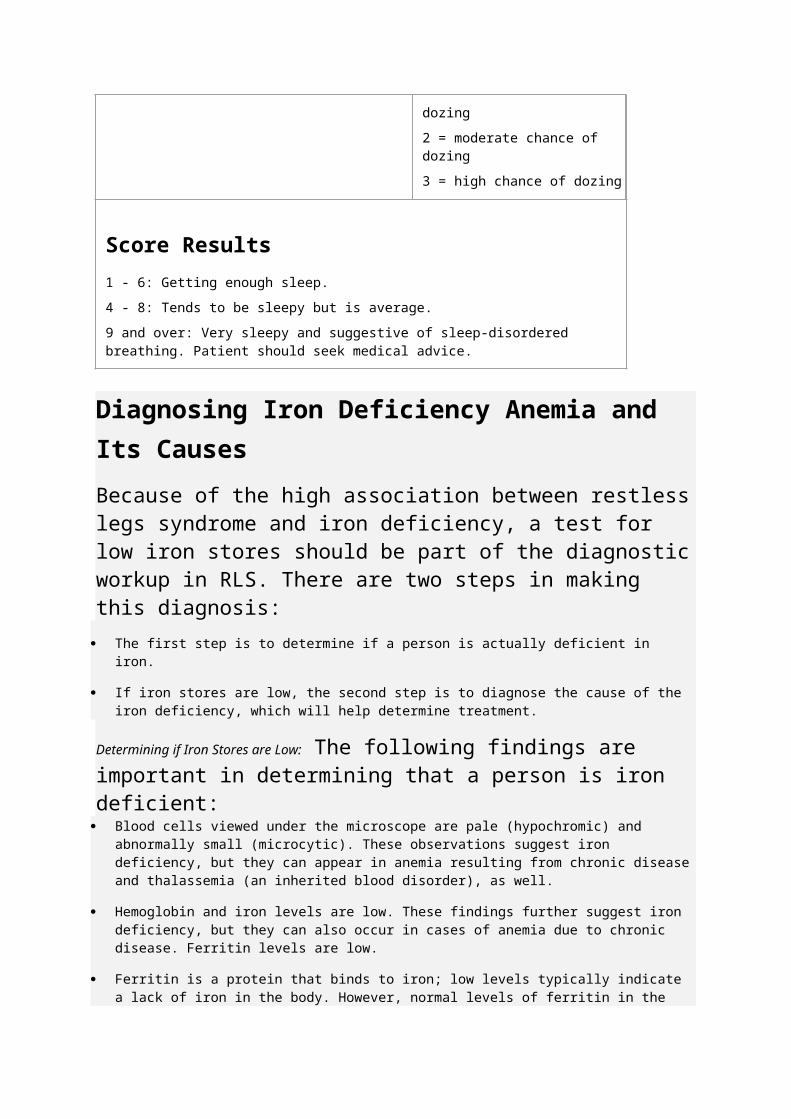
Score Results1 - 6: Getting enough sleep.
4 - 8: Tends to be sleepy but is average.
9 and over: Very sleepy and suggestive of sleep-disordered breathing. Patient should seek medical advice.
Diagnosing Iron Deficiency Anemia and Its CausesBecause of the high association between restless legs syndrome and iron deficiency, a test for low iron stores should be part of the diagnostic workup in RLS. There are two steps in making this diagnosis:
The first step is to determine if a person is actually deficient in iron.
If iron stores are low, the second step is to diagnose the cause of the iron deficiency, which will help determine treatment.
Determining if Iron Stores are Low: The following findings are important in determining that a person is iron deficient:
Blood cells viewed under the microscope are pale (hypochromic) and abnormally small (microcytic). These observations suggest iron deficiency, but they can appear in anemia resulting from chronic disease and thalassemia (an inherited blood disorder), as well.
Hemoglobin and iron levels are low. These findings further suggest iron deficiency, but they can also occur in cases of anemia due to chronic disease. Ferritin levels are low.
Ferritin is a protein that binds to iron; low levels typically indicate a lack of iron in the body. However, normal levels of ferritin in the blood do not always mean a patient has enough iron. For example, pregnant women in their third trimester or patients with a chronic disease may not have enough iron even with normal or high ferritin levels.
A test that measures a factor called serum transferrin receptor (TfR) is proving to be very sensitive in identifying iron deficiency in some patients, including the elderly with chronic diseases and possibly pregnant women. When iron deficiency anemia is diagnosed, the next step is to determine the cause of the iron deficiency itself. Menstrual blood loss is a common cause of iron deficiencyin women of reproductive age. Tests to check for an underlying cause of iron deficiency, such as gastrointestinal (digestive tract) bleeding, are particularly important in men, postmenopausal women, and children. [See In-Depth Report #57: Anemia.]
Other Laboratory TestsThe following laboratory tests may be helpful in determining causes of restless legs syndrome (RLS) or identifying conditions that rule it out.
Blood glucose tests for diabetes
Tests for kidney problems
In certain cases, tests for thyroid hormone, magnesium, and folate levels
Electromyography (recording the electrical activity of muscles) for neuropathy, radiculopathy (problem with the nerve roots), myelopathy (problem with the spinal cord)
Central nervous system MRI for myelopathy or stroke
Ruling Out Other Leg DisordersIn addition to other sleep-related leg disorders, many other medical conditions may have features that resemble restless legs syndrome (RLS). The doctor will need to consider these disorders in making a diagnosis.
Peripheral Neuropathies. Peripheral neuropathies are nerve disorders in the hands or feet, which can produce pain, burning, tingling, or shooting sensations in the arms and legs. Several conditions can cause these disorders; diabetes is a very common cause of painful peripheral neuropathies. Other causes include alcoholism, rheumatoid arthritis, systemic lupus erythematosus, amyloidosis, HIV infection, kidney failure, and certain vitamin deficiencies. Symptoms of peripheral neuropathies may mimic RLS. However, unlike RLS, these disorders ar not usually associated with restlessness. Also, movement does not relieve the discomfort, and the the problem does not worsen at bedtime.Akathisia. Akathisia is a state of restlessness or agitation, and feelings of muscle quivering. A condition called hypotensive akathisia is caused by failure in the autonomic nervous system. Unlike RLS, it occurs at any time of the day. Also, it usually happens only when the patient is sitting -- not lying down. Anti-nausea drugs and drugs used to treat schizophrenia and other psychoses can cause akathisia. The condition also occurs when drugs to treat Parkinson's disease are stopped.Painful Legs and Moving Toes Syndrome. This is a rare disorder that affects one or both legs. Painful legs and moving toes syndrome is marked by a constant, deep, throbbing ache in the limbs and involuntary toe movements. The discomfort may be mild or severe. The problem gets worse with activity and usually stops during sleep. Most of the time, the cause is unknown, although it may arise from spinal injuries or herpes zoster infection. The condition is difficult to treat, but the drug baclofen, combined with either clonazepam or carbamazepine, has shown some success. Other treatments that may help include orthotic shoe inserts and transcutaneous electrical nerve stimulation (TENS).Meralgia Paresthetica. An uncommon nerve condition, meralgia paresthetica causes numbness, pain, tingling, or burning on the
front and side of the thigh. It usually occurs on one side of the body. The condition may be caused by compression of the thigh nerve as it passes through the pelvis. The problem typically occurs in people aged 30 to 60 years, but it can affect people of all ages. It often goes away on its own.
Nocturnal (Nighttime) Leg CrampsCramps that awaken people during sleep are very common, but they are not part of restless legs syndrome or periodic limb movement disorder. Nocturnal leg cramps can be very painful and may cause the person jump out of bed in the middle of the night. They typically affect a specific area of the calf or the sole of the foot.
What Are Nocturnal Leg Cramps?Benign nocturnal leg cramps ("charley horse") are muscle spasms in the calf. They can occur one or many times during the night. Cramping may also occur in the soles of the feet. Typically, cramps last from a few seconds to a few minutes. Some people experience them regularly, others rarely.
Causes of Nocturnal Leg Cramps. In most cases, the cause of nocturnal leg cramps remains unknown. Among the conditions that might cause leg cramps are:
Calcium and phosphorus imbalances, particularly during pregnancy
Low potassium or sodium levels
Overexertion, standing on hard surfaces for long periods, or prolonged sitting (especially with the legs contorted)
Having structural disorders in the legs or feet (such as flat feet)
Medical causes of muscle cramping include hypothyroidism, Addison's disease, uremia, hypoglycemia, anemia, and certain medications. Various diseases that affect nerves and muscles, such as Parkinson's, cause leg cramps. Peripheral neuropathy, a complication of diabetes, can cause cramp-like pain, numbness, or tingling in the legs. Patients with kidney disease undergoing dialysis are also prone to leg cramps.
Individuals at Higher Risk for Nocturnal Leg Cramps. Nocturnal leg cramps occur at all ages but peak at different times. They are particularly common in adolescence, during pregnancy, and in older age, affecting up to 70% of adults over age 50 at some point.
Pregnant women and those taking diuretics are also at risk for leg cramps because of low calcium levels and an imbalance in calcium and phosphorus.
Consequences of Nocturnal Leg Cramps. Nocturnal leg cramps, like restless legs syndrome, rarely have serious consequences. However, they can be extremely painful and long lasting. Severe symptoms that occur often can cause chronic insomnia and considerable mental distress.
Managing Nocturnal Leg CrampsWays to relieve a cramp once it has begun include:
Straightening the leg, flexing the foot upward toward the knee, or grabbing the toes and pulling them toward the knee.
Walking, or shaking the affected leg then elevating it.
If soreness persists, a warm bath or shower or an ice pack may bring relief.
Lifestyle Tips for Preventing Nocturnal Leg Cramps. Nighttime leg cramps are generally treated with lifestyle changes.
People with leg cramps should drink plenty of water (at least 6 to 8 glasses daily) to maintain adequate fluid levels. Nightly stretching exercises may help prevent leg cramps from occuring. (This are generally recommended for RLS, as well).
To stretch leg muscles: Stand about 30 inches from a wall. Keeping heels flat on the floor, lean forward and slowly move hands up the wall to achieve a comfortable stretch.
Alternately, pedal for a few minutes on a stationary bicycle at bedtime.
While in bed, loose covers should be placed over the toes and feet. This prevents the toes and feet from pointing, which causes calf muscles to contract and cramp. Propping the feet up higher than the torso may also help.
Regular swimming and water exercises are a good way to keep muscles stretched.
Wearing supportive footwear may help reduce leg cramps
Quinine. Quinine had been widely used to prevent leg cramping. The U.S. Food and Drug Administration (FDA) banned its sale over the counter because it reportedly caused some serious, although rare, side effects. These side effects include bleeding problems and heart irregularities. Other, less serious side effects include headaches, vision problems, and rashes.The FDA has since banned the marketing of most quinine drugs, cautioning against the off-label (non-approved) use of the drug to
treat nocturnal (nighttime) leg cramps. Only one form of the drug, Qualaquin, is approved for sale. It is used for the treatment of some types of malaria. Pregnant women and people with liver problems should avoid quinine in any form. In July 2010 the FDA issued a warning of serious, potentially life-threatening side effects resulting from the use of Qualaquin for nocturnal leg cramps. These side effects include dangerously low blood platelet counts (platelets help the blood clot) and permanent kidney damage.
Supplements. Some small studies indicate that the mineral magnesium, taken as magnesium citrate or magnesium lactate, may provide some benefit to people with leg cramps, including pregnant women. In one small study, taking vitamin B complex was shown to be helpful. Other supplements tried for leg cramps include vitamin E, calcium, and potassium or sodium chloride, but these do not appear to be very effective.
TreatmentTreatment for complaints of sleeplessness and restless legs syndrome focus on efforts to improve sleep and eliminate possible causes of RLS. Initially, doctors normally try to achieve these goals without the use of drugs. A non-drug approach is a particularly important first step for elderly patients.
The doctor should first try to treat any underlying medical conditions that may be causing restless legs.
If medications may be causing RLS, the doctor should try to prescribe alternatives.
If the cause cannot be determined, measures to improve sleep habits and relaxation techniques are the best first steps. These approaches may help, even if medicines may be needed later on.
Lifestyle ChangesSome people report that making the following changes help control restless legs syndrome:
Taking hot baths or using cold compresses.
Stopping smoking.
Getting enough exercise during the day.
Doing calf stretching exercises at bedtime.
Using Ergonomic measures. For example, working at a high stool where legs can dangle helps some people. Also, sitting on a aisle during meetings or airplane travel can allow for more leg movement.
Changing sleep patterns. Some people report that symptoms do not occur when they sleep in the late morning. Therefore, patients may consider changing their sleep patterns if feasible.
Avoiding caffeine, alcohol, and nicotine also improves some cases of RLS.
Some patients have tried alternative treatments for RLS, such as acupuncture and massage. To date, however, there is not enough data on the effectiveness of these treatments.
Dietary IronRestless legs syndrome is associated with iron deficiency, so people with the condition should get enough iron in their diet. [For more information, see In-Depth Report #57:Anemia.] Iron is found in foods either in the form of heme or non-heme iron:
Foods containing heme iron are the best for increasing or maintaining healthy iron levels. Such foods include clams, oysters, organ meats, beef, pork, poultry, and fish.
Non-heme iron is less well absorbed. Over half the iron in meat is non-heme. Eggs, dairy products, and iron-containing vegetables (including dried beans and peas) have only the non-heme form. Other sources of non-heme iron include iron-fortified cereals, bread, and pasta products, dark green leafy vegetables (such as chard, spinach, mustard greens, and kale), dried fruits, nuts, and seeds.
Iron SupplementsIron supplements may reduce symptoms in people with restless legs syndrome who are also iron deficient. Patients should use them only when dietary measures have failed. Iron supplements do not appear to be useful for RLS patients with normal or above normal iron levels.
Supplement Forms. To replace iron, the preferred forms of iron tablets are ferrous salts, usually ferrous sulfate (Feosol, Fer-In-Sol, Mol-Iron). Other forms include ferrous fumarate (Femiron, FerroSequels, Feostat, Fumerin, Hemocyte, Ircon), ferrous gluconate (Fergon, Ferralet, Simron), polysaccharide-iron complex (Niferex, Nu-Iron), and carbonyl iron (Elemental Iron,
Feosol Caplet, Ferra-Cap). Specific brands and forms may have certain advantages.Regimen. A reasonable approach for patients with RLS is to take 65 mg of iron (or 325 mg of ferrous sulfate) along with 100 mg of vitamin C on an empty stomach, 3 times a day.IMPORTANT: As few as 3 adult iron tablets can poison, and even kill, children. This includes any form of iron pill. No one, not even adults, should take a double dose of iron if they miss one dose.
Tips for taking iron are: For best absorption, take iron between meals. (Iron may cause stomach and intestinal
disturbances, however. Some experts believe that you can take low doses of ferrous sulfate with food and avoid the side effects.)
Always drink a full 8 ounces of fluid with an iron pill.
Keep tablets in a cool place. Bathroom medicine cabinets may be too warm and humid, which may cause the pills to disintegrate.
Side Effects. Common side effects of iron supplements include the following:
Constipation and diarrhea may occur but these side effects are rarely severe. However, iron tablets can aggravate existing digestive problems such as ulcers and ulcerative colitis.
Nausea and vomiting may occur with high doses. You can control this by taking smaller amounts. Switching to ferrous gluconate may help some people with severe digestive problems.
Black stools are normal when taking iron tablets. In fact, if stools do not turn black, the tablets may not be working effectively.
Stools appear tarry or have red streaks may indicate bleeding in the digestive tract, which may be causing iron deficiency. Other warning signs include cramps, sharp pains, or soreness in the stomach. Intestinal bleeding requires immediate medical attention.
Acute iron poisoning is rare in adults, but can be fatal in children who take adult-strength tablets.
Interactions With Other Drugs. Certain medicines, including antacids, can reduce iron absorption.Iron tablets may also reduce the effectiveness of other drugs, including:
Antibiotics -- tetracycline, penicillamine, and ciprofloxacin
Anti-Parkinson's disease drugs -- methyldopa, levodopa, and carbidopa
At least 2 hours should elapse between doses of these drugs and doses of iron supplements.
[For additional information about iron supplements see In-Depth
Report #57: Anemia.]
ExerciseExercise early in the day helps achieve healthy sleep. Vigorous too close to bedtime (1 to 2 hours before) may worsen restless legs syndrome (RLS). A study found that people who walked briskly for 30 minutes, four times a week, improved minor sleep disturbances after 4 months. Regular, moderate exercise may help prevent RLS. However, patients report that either bursts of excessive energy or long sedentary periods can worsen symptoms.
Pneumatic Compression DeviceSmall studies have shown that the use of a pneumatic compression device improves symptoms on RLS in some patients. Pneumatic compression devices wrap an inflatable cuff around the legs. This cuff is attached to a device which then increases pressure around the legs. It is worn for at least an hour, generally around the time symptoms usually begin.
MedicationsThe American Academy of Sleep Medicine recommends medications for RLS or PLMD only for persons who fit strict diagnostic criteria, and who experience excessive daytime sleepiness as a result of these conditions. (Excessive daytime sleepiness results from nighttime sleeplessness due to RLS or PLMD symptoms).
More research and physician training is needed to better diagnose and treat RLS with medications in children and adolescents. Little is known about the best way to treat RLS in general, but some experts suggest the following for adults:
If lifestyle changes do not control the problem, over-the-counter pain relievers should be the first form of treatment.
People with RLS should have a test for iron deficiency. If they are iron deficient, they should start treatment with iron supplements.
Dopaminergic drugs (drugs that increase levels of dopamine) are the standard medicines for treating severe RLS, PLMD, or both.
Other drugs may be helpful if dopaminergic drugs fail, or for patients who have frequent -- but not nightly -- symptoms. These include opiates (pain relievers), benzodiazepines (sedative hypnotic drugs), or anticonvulsants. However, benzodiazepines and opiates can become habit forming and addictive.
Tylenol and Non-Steroidal Anti-Inflammatory DrugsBefore taking stronger medications, people should try over-the-counter pain relievers, such as acetaminophen (Tylenol) or non-steroidal anti-inflammatory drugs (NSAIDs), which include ibuprofen (Advil, Motrin, Rufen), naproxen (Anaprox, Naprosyn, Aleve), and ketoprofen (Orudis KT, Aktron).
Although NSAIDs work well, long-term use can cause stomach problems, such as ulcers, bleeding, and possible heart problems. In April 2005, the FDA asked drug manufacturers of NSAIDs to include a warning label on their product that alerts users of an increased risk for heart-related problems and digestive tract bleeding.
Levodopa and Other Dopaminergic DrugsDopaminergic drugs increase the availability of the chemical messenger dopamine in the brain, and are the first-line treatment for severe RLS and PLMD. These drugs significantly reduce the number of limb movements per hour, and improve the subjective quality of sleep. Patients with either condition who take these drugs have experienced up to 100% reduction in symptoms.
Dopaminergic drugs, however, can have severe side effects (they are ordinarily used for Parkinson's disease). They do not appear to be as helpful for RLS related to dialysis as they do for RLS from other causes.
Dopaminergic drugs include dopamine precursors and dopamine receptor agonists.
Dopamine Receptor Agonists. Dopamine receptor agonists (also called dopamine agonists) mimic the effects of dopamine by acting on dopamine receptors in the brain. They are now generally preferred to L-dopa (see below). Because they have fewer side
effects than L-dopa, including rebound effect and augmentation, these drugs may be used on a daily basis. About 30% of patients who take dopamine receptor agonists have reported augmentations symptoms. As the newer drugs are taken for longer periods and at higher doses, however, their augmentation rates may become closer to those of L-dopa.Dopamine agonists have been shown to relieve symptoms in 70 to 90% of patients. Dopamine agonists can be ergot-derived (such as cabergoline) or non-ergot derived (such as pramipexole and ropinirole). The newer non-ergotamine derivatives may induce fewer side effects than ergot-derived drugs:
Ropinirole (Requip) was the first drug approved specifically for treatment of moderate-to-severe RLS (more than 15 RLS episodes a month). Side effects are generally mild but may include nausea, vomiting, drowsiness, and dizziness.
Pramipexole (Mirapex) is also approved for RLS. However, patients may fall asleep, without warning, while taking this drug, even while performing activities such as driving.
Rotigotine is a patch preparation. Common side effects include back or joint pain, dizziness, decreased appetite, dry mouth, fatigue, sweating, trouble sleeping or upset stomach.
Cabergoline is a dopamine agnoist that should be used only when other medications have been tried and failed; it poses a risk of heart valve damage.
Other Dopamine Agonists. Other dopamine agonists that have shown some promise in small studies include alpha-dihydroergocryptine, or DHEC (Almirid), and piribedil (Trivastal).Dopamine Precursors. The dopamine precursor levodopa (L-dopa) was once a popular drug for severe RLS. Although it can still be useful, most doctors now prefer the newer dopamine agonists (see above). The standard preparations (Sinemet, Atamet) combine levodopa with carbidopa, which improves the action of levodopa and reduces some of its side effects, particularly nausea. Levodopa can also be combined with benserazide (Madopar) with similar results, but Sinemet is almost always used in America. (Levodopa combinations are well tolerated and safe.)Patients typically start with a very low dose taken 1 hour before bedtime. The dosage is increased until the patient finds relief. Patients sometimes need to take an extended-release form or to take it again during the night.
Levodopa acts fast, and the treatment is usually effective within the first few days of therapy.
Serious common side effects of L-dopa treatment (and, to lesser extent, of dopamine receptor agonists) are augmentation and rebound. Many studies report that augmentation (worsening of symptoms that occur earlier in the day) occurs in up to 70% of patients who take L-dopa. The risk is highest for patients who take daily doses, especially doses at high levels (greater than 200 mg/day). For this reason, patients should use L-dopa only intermittently (fewer than 3 times per week). The drug should be immediately discontinued if augmentation does occur. Following withdrawal from L-dopa, patients can switch to a dopamine receptor agonist.
The rebound effect causes increased leg movements at night or in the morning as the dose wears off, or as tolerance to the drug builds up.
Regimens. The effects of L-dopa are apparent in 15 to 30 minutes. Dopamine receptor agonists, meanwhile, take at least 2 hours to start working. Some doctors recommend regular use of dopamine receptor agonists for patients who experience nightly symptoms, and L-dopa for those whose symptoms occur only occasionally.Side Effects. Common side effects of dopaminergic drugs vary but may include feeling faint or dizzy (especially when standing up), headaches, abnormal muscle movements, rapid heartbeat, insomnia, bloating, chest pain, and dry mouth. Nausea may be especially common. Adding the drug domperidone may help to relieve this side effect. In rare cases, dopaminergic drugs can cause hallucinations or lung disease.Because these drugs may cause daytime drowsiness, patients should be extremely careful while driving or performing tasks that require concentration.
Long-term use of dopaminergic drugs can lead tolerance, which results in to loss of effectiveness. Adding a drug called entacapone (Comtan) may prolong the duration of action of carbidopa-levodopa therapy, but it can cause nausea.
Rebound effect, augmentation, and tolerance can reduce the value of dopaminergic drugs in the treatment of RLS. Using the lowest dose possible can minimize these effects.
Withdrawal Symptoms. Patients who withdraw from these drugs typically experience severe RLS symptoms for the first 2 days after stopping. RLS eventually returns to pre-treatment levels after about a week. The longer a patient uses these drugs, the worse their withdrawal symptoms.
BenzodiazepinesBenzodiazepines, such as clonazepam (Klonopin), are known as sedative hypnotics. Doctors prescribe them for insomnia and anxiety. They may be helpful for restless legs syndrome (RLS) that disrupts sleep, especially in younger patients. Clonazepam may be particularly helpful for children with both periodic limb movement disorder and symptoms of attention deficit hyperactivity disorder. The medicine also may be helpful for patients with RLS who are undergoing dialysis.
Side Effects. Elderly people are more susceptible to side effects. They should usually start at half the dose prescribed for younger people, and should not take long-acting forms. Side effects may differ depending on whether the benzodiazepine is long-acting or short-acting.
The drugs may increase depression, a common condition in many people with insomnia.
Breathing problems may occur with overuse or in people with pre-existing respiratory illness.
Long-acting drugs have a very high rate of residual daytime drowsiness compared to others. They have been associated with a significantly increased risk for automobile accidents and falls in the elderly, particularly in the first week after taking them. Shorter-acting benzodiazepines do not appear to pose as high a risk.
There are reports of memory loss (so-called traveler's amnesia), sleepwalking, and odd mood states after taking triazolam (Halcion) and other short-acting benzodiazepines. These effects are rare and probably enhanced by alcohol.
Because benzodiazepines cross the placenta and enter breast milk, pregnant and nursing women should not use them. There are some reports of an association between the use of benzodiazepines in the first trimester of pregnancy and the development of cleft lip in newborns. Studies are conflicting at this point, but other side effects are known to occur in babies exposed to these drugs in the uterus.
In rare cases, overdoses have been fatal.
Interactions. Benzodiazepines are potentially dangerous when used in combination with alcohol. Some drugs, such as the ulcer medication cimetidine, can slow the breakdown of benzodiazepine.
Withdrawal Symptoms. Withdrawal symptoms usually occur after prolonged use and indicate dependence. They can last 1 to 3 weeks after stopping the drug and may include:
Gastrointestinal distress
Sweating
Disturbed heart rhythm
In severe cases, patients might hallucinate or experience seizures, even a week or more after they stop taking the drug.
Rebound Insomnia. Rebound insomnia, which often occurs after withdrawal, typically includes 1 to 2 nights of sleep disturbance, daytime sleepiness, and anxiety. The chances of rebound are higher with the short-acting benzodiazepines than with the longer-acting ones.
Narcotic Pain RelieversNarcotics are pain-relieving drugs that act on the central nervous system. They are sometimes prescribed for severe cases of restless legs syndrome (RLS). They may be a good choice if pain is a prominent feature. Some evidence also suggests that narcotics reduce the frequency of periodic leg movements.
There are two types of narcotics, both of which have been used for severe RLS:
Opiates (such as morphine and codeine) come from natural opium. Some patients report relief with the use of the opiate fentanyl (Duragesic), available in skin patch form. An implanted pump that uses morphine and an anesthetic called bupivacaine is showing promise for patients with severe RLS. The pump delivers the drugs to the fluid surrounding the spinal cord (cerebrospinal fluid).
Opioids are synthetic drugs. The most common example is oxycodone (Percodan, Percocet, Roxicodone, OxyContin, Methadone, and Hydrocodone).
Although the use of narcotics for severe RLS is controversial, some studies have suggested that even when the treatments are long-term, they are rarely addictive for pain sufferers except among patients with a history of substance abuse.
The use of such drugs may be beneficial when included as part of a comprehensive pain management program. Such a program involves screening prospective patients for possible drug abuse, and regularly monitoring those who are taking narcotics. Doses should be adjusted as necessary to achieve an acceptable balance between pain relief and side effects. Patients on long-
term opiate therapy should also be monitored periodically for sleep apnea, a condition that causes breathing to stop for short periods many times during the night. Sleep apnea may worsen symptoms of RLS, insomnia, and other complaints.
Tramadol. Tramadol (Ultram) is a pain reliever that has been used as an alternative to opioids. It has opioid-like properties, but is not as addictive. (However, there are reports of dependence and abuse with this drug as well.) Withdrawal after long-term use (longer than a year) can cause intense symptoms, including diarrhea, insomnia, and even restless legs syndrome itself.
Antiseizure DrugsAntiseizure drugs -- such as gabapentin (Neurontin), valproic acid (valproate, divalproex, Depakote, Depakene), and carbamazepine (Tegretol) are being tested for restless legs syndrome (RLS). In 2011 the FDA approved gabapentin enacarbil, a form of gabapentin, for the once daily treatment of moderate to severe RLS. Gabapentin enacarbil converts to gabapentin in the intestines, and therefore may reduce some of the side effects experienced by patients taking antiseizure medications. (Common side effects included mild sleepiness and dizziness.) The drug is marketed under the name Horizant Extended Release.
Side Effects. All antiseizure drugs have potentially severe side effects. Therefore, patients should try these medications only after non-drug methods have failed. Side effects of many anti-seizure drugs include nausea, vomiting, heartburn, increased appetite with weight gain, hand tremors, irritability, and temporary hair thinning and hair loss (taking zinc and selenium supplements may help reduce this last effect). Some antiseizure drugs can also cause birth defects and, in rare cases, liver toxicity. Gabapentin may have fewer of these side effects than valproic acid or carbamazepine.
Other DrugsAntidepressants. Bupropion (Wellbutrin), a newer antidepressant, may be helpful for restless legs syndrome (RLS). Bupropion is a weak dopamine reuptake inhibitor -- it causes a slight increase in the availability of dopamine in the brain. The drug is not addictive and does not have the severe side effects of other RLS drugs, but more research is needed to determine if it is useful.Clonidine. Clonidine (Catapres), a drug used for high blood pressure, is helpful for some patients and may be an appropriate choice for patients who have RLS accompanied by hypertension. It also may help patients with RLS who are undergoing hemodialysis.Baclofen. The anti-spasm drug baclofen (Lioresal) appears to reduce intensity of RLS (although not frequency of movements).Alpha-2 Delta Blockers. Gabapentin and gabapentin enacarbil appear to help RLS sufferers. Pregabalin is currently under study.
Resources www.aasmnet.org -- American Academy of Sleep Medicine
www.sleepfoundation.org -- National Sleep Foundation
www.ninds.nih.gov -- National Institute of Neurological Disorders and Stroke
www.nhlbi.nih.gov/about/ncsdr/ -- National Center on Sleep Disorders Research
www.rls.org -- Restless Legs Syndrome Foundation
www.wemove.org -- Worldwide Education and Awareness for Movement Disorders
ReferencesAurora RN, Kristo DA, Bista SR, et al. Update to the AASM clinical practice guideline: The treatment of restless legs syndrome and periodic limb movement disorder in addults--an update for 2012: practice paramters with an evidence-based systematic review and meta-anayysis. Sleep. 2012;35(8):1039-1062.Aurora RN, Kristo DA, Bista SR, et al. Letter to the Editor: Update to the AASM clinical practice guideline: The treatment of restless legs syndrome and periodic limb movement disorder in addults--
an update for 2012: practice paramters with an evidence-based systematic review and meta-anayysis. Sleep. 2012;35(8):1037..Bayard M, Avonda T, Wadzinski, J. Restless Legs Syndrome. American Family Physician. 2008;78(2):235-240.Gringas P. When to use drugs to help sleep. Arch Dis Child. 2008;93(11):976-81.Hening WA. Current Guidelines and Standards of Practice for Restless Legs Syndrome.AmJ Med. 2007;120(1A):S22-S27.Hornyak M, Rupp A, Riemann D, et al. Low-dose hydrocortisone in the evening modulates symptom severity in restless leg syndrome. Neurology. 2008;70(18):1620-2.Kushida CA. Clinical Presentation, Diagnosis, and Quality of Life Issues in Restless Legs Syndrome. AmJ Med. 2007;120(1A):S4-S12.Kushida CA, Becker PM, Ellenbogen AL, et al. Randomized, double-blind, placebo-controlled study of XP13512/GSK1838262 in patients with RLS. Neurology. 2009;72(5):439-46.Lettieri CJ, Eliasson AH. Pneumatic compression devices are an effective therapy for restless legs syndrome: a prospective, randomized, double-blind, sham- controlled trial.Chest. 2009;135(1):74-80.Lohmann-Hedrich K, Neumann A, Kleensang A, et al. Evidence for linkage of restless legs syndrome to chromosome 9p: are there two distinct loci? Neurology. 2008;70(9):686-694.Ondo WG. Restless Leg Syndrome. Neurol Clin. 2009;27(3):779-799.Ong KH, Tan HL, Tam LP, et al. Accuracy of serum transferrin receptor levels in the diagnosis of iron deficiency among hospital patients in a population with a high prevalence of thalassaemia trait. Int J Lab Hematol. 2008;30(6):487-493Picchietti D. Restless legs syndrome: prevalence and impact in children and adolescents--the Peds REST study. Pediatrics. 2007; 120(2): 253-66.Restless Leg Syndrome Foundation. RLS Name Change: Willis-Ekbom Disease. Available online. Last accessed: October 1, 2011.Stefansson H, Rye DB, Hicks A, et al. A Genetic Risk Factor for Periodic Limb Movements in Sleep. N Engl J Med. 2007;357:639-47.Trotti LM, Bhadriraju S, Becker LA. Iron for restless legs syndrome. Cochrane Data Base Syst Rev. 2012;16;5:CD007834.
U.S. Food and Drug Administration. FDA approves Horizant to treat restless legs syndrome. FDA News Release, April 7, 2011. Available online. Last accessed September 17, 2011.
U.S. Food and Drug Administration. FDA's MedWatch Safety Alerts: July 2010. Available online. Last Accessed 21 September, 2010.
Version Info Last Reviewed on 01/10/2013
Reviewed by: Harvey Simon, MD, Editor-in-Chief, Associate Professor of Medicine, Harvard Medical School; Physician, Massachusetts General Hospital. Also reviewed by A.D.A.M. Health Solutions, Ebix, Inc., Editorial Team: David Zieve, MD, MHA, David R. Eltz, Stephanie Slon, and Nissi Wang.
A.D.A.M., Inc. is accredited by URAC, also known as the American Accreditation HealthCare Commission (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics and subscribes to the principles of the Health on the Net Foundation (www.hon.ch)
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Call 911 for all medical emergencies. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2013 A.D.A.M., Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
https://umm.edu/health/medical/reports/articles/restless-legs-syndrome-and-related-disorders
Causes of restless legs syndrome In many cases, the exact cause of restless legs syndrome is unknown.When no cause can be found, it's known as "idiopathic" or primary restless legs syndrome.Research has identified specific genes related to restless legs syndrome, and it can run in families. In these cases, symptoms usually occur before the age of 40.
DopamineThere's evidence to suggest restless legs syndrome is related to a problem with part of the brain called the basal ganglia. The basal ganglia uses a chemical (neurotransmitter) called dopamine to help control muscle activity and movement.Dopamine acts as a messenger between the brain and nervous system to help the brain regulate and co-ordinate movement. If nerve cells become damaged, the amount of dopamine in the brain is reduced, which causes muscle spasms and involuntary movements.Dopamine levels naturally fall towards the end of the day, which may explain why the symptoms of
restless legs syndrome are often worse in the evening and during the night.
Underlying health conditionRestless legs syndrome can sometimes occur as a complication of another health condition, or it can be the result of another health-related factor. This is known as secondary restless legs syndrome.You can develop secondary restless legs syndrome if you:
have iron deficiency anaemia – low levels of iron in the blood can lead to a fall in dopamine, triggering restless legs syndrome
have a long-term health condition – such as chronic kidney disease, diabetes, Parkinson's disease, rheumatoid arthritis, anunderactive thyroid gland, or fibromyalgia
are pregnant – particularly from week 27 until birth; in most cases the symptoms disappear within four weeks of giving birth
TriggersThere are a number of triggers that don't cause restless legs syndrome, but can make symptoms worse. These include medications such as:
some antidepressants antipsychotics lithium – used in the treatment of bipolar disorder calcium channel blockers – used in the treatment of high blood pressure some antihistamines metoclopramide – used to relieve nausea
Other possible triggers include: excessive smoking, caffeine or alcohol being overweight or obese
stress lack of exercise
Page last reviewed: 02/09/2015Next review due: 02/09/2017http://www.nhs.uk/Conditions/Restless-leg-syndrome/Pages/Causes.aspx
INTRODUCTION — Restless legs syndrome/Willis-Ekbom disease (RLS/WED) refers to an overwhelming urge to move the legs, usually associated with unpleasant sensations. The urge to move the legs is worse at rest and at night and relieved by movement. RLS/WED is commonly associated with sleep disturbance and with involuntary, jerking movements of the legs during sleep, known as periodic leg movements of sleep (PLMS). When significant sleep disturbances or impaired daytime functioning coexist with PLMS in the absence of RLS/WED or other associated disorders, the term periodic limb movement disorder (PLMD) is used.
RLS/WED is a treatable condition that generally responds well to pharmacologic therapy. A variety of treatments have been studied in randomized, controlled trials; the major classes of drugs used include dopaminergic agents, alpha-2-delta calcium channel ligands, opioids, and benzodiazepines [1-4]. The treatment approach to PLMD is similar to that of RLS/WED, although supported by considerably less data. (See 'Periodic limb movement disorder' below.)
The selection of therapy depends upon a number of factors, including disease severity, patient age, comorbidities (eg, pain, depression, anxiety, history of impulse control behaviors), drug side effects, and patient preferences. The goals of therapy are to reduce or eliminate symptoms of RLS/WED and improve daytime function, sleep, and quality of life.
This topic will review the treatment of RLS/WED and PLMD in adults. The clinical features and diagnosis of RLS/WED and PLMD in adults and treatment of these disorders in children are discussed separately. (See "Clinical features and diagnosis of restless legs syndrome/Willis-Ekbom disease and periodic limb movement disorder in adults" and "Restless legs syndrome/Willis-Ekbom disease and periodic limb movement disorder in children".)
IRON REPLACEMENT — A serum ferritin concentration lower than 45 to 50 mcg/L (ng/mL) has been associated with an increased severity of restless legssyndrome/Willis-Ekbom disease (RLS/WED), and iron replacement is suggested if the serum ferritin level is lower than 75 mcg/L [5]. Iron therapy should not be prescribed empirically because it may result in iron overload, especially in patients with previously unsuspected hemochromatosis.
This recommendation is based on evidence supporting a role for iron deficiency in the pathophysiology of RLS/WED and three small randomized placebo-controlled studies showing a clinical benefit in patients receiving iron replacement therapy: one in adult patients with serum ferritin ≤75 mcg/L treated with oral iron [6], one in patients with end-stage renal disease and functional iron deficiency treated with intravenous iron dextran [7], and a third in patients with moderate to severe RLS/WEDtreated with intravenous ferric carboxymaltose [8].
Two other randomized studies of intravenous iron sucrose, only one of which was limited to iron-deficient patients, failed to show a benefit [9,10]. A meta-analysis that included four out of five of these studies found significant heterogeneity in the formulation of iron used, patient characteristics, and measurement of outcome variables across studies and found insufficient evidence to conclude whether iron is beneficial for treatment of RLS/WED [1].
Iron supplementation can be supplied orally or intravenously. Intravenous delivery has the advantage of replenishing iron stores more quickly than oral therapy but it is less convenient and carries a risk of serious infusion reactions, including anaphylaxis. There are no direct comparisons of intravenous versus oral iron supplementation in patients with RLS/WED, and available data do not show clear superiority of one route of administration over the other. (See "Treatment of the adult with iron deficiency anemia", section on 'Prevention and treatment of adverse drug events'.)
Because oral iron is easier to administer and safer, we suggest initial therapy with an oral regimen such as ferrous sulfate (325 mg orally two to three times a day). Iron should be combined with vitamin C (100 to 200 mg with each dose of ferrous sulfate) or a glass of orange juice to enhance absorption. Iron should not be taken at the same time as calcium supplements or significant amounts of dairy products. (See "Treatment of the adult with iron deficiency anemia".)
Intravenous iron therapy is generally reserved for patients with low iron stores and either a malabsorption state or complete intolerance to oral iron preparations. (See"Treatment of the adult with iron deficiency anemia", section on 'Oral iron therapy'.)
Ferritin levels should be checked after three to four months of therapy and then every three to six months until the serum ferritin level is >75 mcg/L and iron saturation is greater than 20 percent. Monitoring is important to avoid the rare but serious complication of iron overload in patients with hemochromatosis genes [11]. Iron therapy can then be discontinued if an ongoing cause for iron deficiency has not been established. The etiologic evaluation of iron deficiency in adults is reviewed separately. (See "Causes and diagnosis of iron deficiency anemia in the adult", section on 'Search for source of blood and iron loss'.)
NONPHARMACOLOGIC THERAPY — In patients with mild symptoms, nonpharmacologic therapies may be sufficient for symptom relief. In patients with more severe symptoms, nonpharmacologic measures are worth reviewing, as they may limit medication requirements.
Behavioral strategies — Use of the following interventions is supported primarily on the basis of clinical experience and, in some cases, small randomized trials [5,12]:
●Mental alerting activities, such as working on a computer or doing crossword puzzles, at times of rest or boredom●Avoidance of aggravating factors, including consideration of withdrawal of possibly predisposing medications (see 'Avoidance of aggravating factors' below)●Moderate regular exercise [13]●Reduced caffeine intake●For symptomatic relief – walking, bicycling, soaking the affected limbs, and leg massage, including pneumatic compression [14]●Short daily hemodialysis for patients with end-stage renal disease (see "Sleep disorders in end-stage renal disease", section on 'Treatment')
Avoidance of aggravating factors — Sleep deprivation is known to aggravate symptoms of restless legs syndrome/Willis-Ekbom disease (RLS/WED) in many patients, and general principles of sleep hygiene should be reviewed. (See "Treatment of insomnia", section on 'Sleep hygiene'.)
Antidepressants, neuroleptic agents, dopamine-blocking antiemetics such as metoclopramide, and sedating antihistamines (including those found in nonprescription medications) may contribute to emergence of RLS/WED or worsening of prior symptoms (table 1) [15]. Most antidepressant classes have been associated withRLS/WED, including tricyclics, selective serotonin reuptake inhibitors, and serotonin-norepinephrine reuptake inhibitors [16].
Discontinuation of antidepressants, however, may not always be possible without causing patient harm. If antidepressants are necessary, the symptoms of secondaryRLS/WED can usually be treated in the same way as primary RLS/WED. Bupropion is an alternative antidepressant that may be less likely to induce or worsenRLS/WED [17].
Novel devices — A device that provides vibratory stimulation to the legs (Relaxis Pad) was approved by the US Food and Drug Administration (FDA) in May 2014 for use in patients with RLS/WED. We do not find compelling evidence of benefit from the available data, however, and we suggest that patients not use this device until further studies have been performed and reported in peer reviewed publications.
According to a pooled analysis of two randomized trials (156 patients) published in a non-MEDLINE-indexed journal, patients assigned to the vibrating pad experienced improvement in Medical Outcomes Study Sleep Problems Index II (MOS-II) scores compared with those assigned to either a light-emitting or sound-producing sham pad (mean improvement from baseline for active versus sham pad: 13.2 versus 6.2 points, p = 0.02) [18]. In descriptions of the two trials available on the company website, however, the MOS-II was not a primary or secondary outcome measure and was tabulated using 9 out of 12 questions from the MOS sleep scale, which itself was listed as a secondary outcome.
Analysis of primary and secondary outcome measures revealed no differences in International Restless Legs Syndrome Study Group (IRLS) scores (improvement from baseline for active versus sham pad: 6.68 versus 6.39 points, p = 0.81) or RLS quality of life scores (improvement from baseline: 11 versus 7 points, p = 0.14). Changes in the MOS sleep scale score were not reported. The most common adverse effect of the vibratory pad was temporary worsening of RLS/WED symptoms, reported in nine patients in the active group and two patients in the control group.
CHRONIC PERSISTENT SYMPTOMS — Chronic persistent restless legs syndrome/Willis-Ekbom disease (RLS/WED) is defined as RLS/WED that is frequent and troublesome enough to require daily treatment, with symptoms usually occurring at least twice a week on average and resulting in moderate or severe distress [5].
Choice of therapy — In patients who do not respond to nonpharmacologic therapy and correction of iron deficiency, we recommend pharmacologic treatment with a dopamine agonist or an alpha-2-delta calcium channel ligand as first-line therapy. These classes of drugs have been shown to be effective compared with placebo in multiple randomized controlled trials [2-4,19-21].
Head-to-head comparisons between the two classes are limited to a single study [21], and we therefore suggest choosing initial therapy based on consideration of symptom severity, patient age and comorbidities, drug side effect profiles, and patient preferences (table 2) [5].
●For patients with very severe RLS/WED, comorbid depression, or obesity/metabolic syndrome, a dopamine agonist is preferred over other drugs as initial therapy.●For patients with comorbid pain, anxiety, or insomnia or a history of impulse control disorder or addiction associated with use of a dopamine agonist, we suggest starting with an alpha-2-delta calcium channel ligand.●For most other patients, we initially try an alpha-2-delta calcium channel ligand because of the risk of augmentation with dopamine agonists, but other potential side effects of the various drugs should also be considered. In general, older patients are more prone to side effects of alpha-2-delta ligands. If the first drug chosen is ineffective or poorly tolerated, then a drug of the other class should be tried.
Small randomized trials and observational studies also support the use of other agents, including levodopa, benzodiazepines, and opioids, but generally these are reserved for intermittent use or in patients with more refractory symptoms. (See 'Intermittent symptoms' below and 'Refractory RLS' below.)
Drug dosages should be used at the minimum dose required to control symptoms. For dopaminergic agents, the doses required for RLS/WED are lower than those used to treat Parkinson disease and usually are given only in the evening (table 2). Ropinirole and rotigotine should be avoided in patients with hepatic failure, as they are metabolized by the liver.
Patients on continuous therapy should be examined regularly (eg, every 6 to 12 months) and screened for side effects and complications such as augmentation, which is a common complication of long-term dopaminergic therapy [17]. (See 'Augmentation' below.)
Dopamine agonists — Dopamine agonists belong to a class of drugs that directly stimulate dopamine receptors and have a longer half-life (four to six hours) than levodopa (90 minutes). They are generally superior to levodopa for the treatment of daily RLS/WED, because of the lower risk of complications.
In a 2011 meta-analysis of 38 trials evaluating dopamine agonists for the treatment of RLS/WED that included cabergoline, lisuride, pergolide, pramipexole, ropinirole,rotigotine, and sumanirole, all except sumanirole were superior to placebo [2]. In two trials, cabergoline and pramipexole were superior to levodopa for improvement in disease severity as measured by the International Restless Legs Syndrome Study Group (IRLS) rating scale [22,23].
Pramipexole and ropinirole — The non-ergot dopamine agonists, pramipexole and ropinirole, are effective in the treatment of RLS/WED and are less likely to cause side effects than other dopamine agonists (eg, cabergoline and pergolide) and levodopa. These agents, along with rotigotine, are considered to be the dopamine agonists of choice for RLS/WED, and all three have been approved by the US Food and Drug Administration (FDA) for this indication [3,5].
●The benefit of pramipexole was demonstrated in a meta-analysis of seven randomized placebo-controlled trials totalling over 1200 patients [3]. In all of the studies, pramipexole improved RLS/WED symptom severity, with an average improvement in the IRLS rating scale of 6.7 points over placebo (95% CI 4.9-8.5) [3]. For reference, a 6-point difference has been proposed as a clinically meaningful improvement in IRLS scores [24]. Uncontrolled studies with longer-term follow-up (26 to 52 weeks) have reported a mean improvement of 17 points on the IRLS scale [25,26].●The benefit of ropinirole was demonstrated in a meta-analysis of five randomized placebo-controlled trials totalling over 900 patients, in which the average improvement in IRLS score over placebo was 4 points (95% CI 2-6) [3].
The onset of action for pramipexole and ropinirole is typically 90 to 120 minutes after intake. Therefore, these medications should be started two hours beforeRLS/WED symptoms start [5]. The recommended doses are as follows (table 2) [5]:
●Pramipexole 0.125 mg once daily. The dose may be increased by 0.125 mg every two to three days until relief is obtained. In a clinical trial, all three doses of pramipexole (0.25, 0.50, and 0.75 mg daily) were equally effective, and some patients responded to the initial dose of 0.125 mg daily [27]. However, side effects were more common with the 0.50 mg and 0.75 mg daily doses. Therefore, it is expected that 0.25 mg daily has the best therapeutic margin. Most patients require 0.5 mg or less, but doses up to 1 mg may be needed.
●Ropinirole 0.25 mg once daily. The dose may be increased by 0.25 mg every two to three days until relief is obtained. Most patients require at least 2 mg, and doses up to 4 mg may be needed. The maximum recommended dose is 3 mg in patients with end-stage renal disease on hemodialysis. In one large randomized controlled trial, the average daily dose of ropinirole was 1.9 mg [28].
Adverse effects with pramipexole and ropinirole are usually mild, transient, and limited to nausea, lightheadedness, and fatigue; these usually resolve within 10 to 14 days. Less frequent side effects include nasal stuffiness, constipation, insomnia, and leg edema; these are reversible if the medication is stopped. Excessive daytime sleepiness can occur at higher doses and occasionally manifests as sudden, unexpected sleep attacks [29]. These may be less common than in patients with Parkinson disease on higher doses of pramipexole [30].
As first reported in patients with Parkinson disease, dopamine agonist therapy in patients with RLS/WED may be associated with an increased risk of impulse control disorders such as pathologic gambling, compulsive eating and shopping, and compulsive inappropriate hypersexuality [31,32]. (See "Pharmacologic treatment of Parkinson disease", section on 'Impulse control disorders'.)
Augmentation, which refers to a worsening of RLS/WED symptoms with increasing doses of medication, including earlier onset of symptoms, increased intensity of symptoms, shorter duration of drug action, or topographic spread of symptoms to the arms, is a common complication of long-term dopaminergic therapy in RLS/WEDthat is discussed in more detail below. (See 'Augmentation' below.)
Early morning rebound symptoms have also been observed in some patients and should be approached in a manner similar to augmentation. Doses of ropinirole andpramipexole should not generally exceed the limits given above to avoid or reduce the risk of augmentation.
Dopamine withdrawal syndrome can occur with abrupt discontinuation of dopamine agonist therapy. Symptoms include anxiety, panic attacks, depression, sweating, nausea, pain, fatigue, dizziness, and drug craving. (See "Pharmacologic treatment of Parkinson disease", section on 'Dopamine agonist withdrawal syndrome'.)
Rotigotine — Rotigotine is a non-ergot dopamine agonist that is formulated as a 24-hour transdermal patch. Rotigotine was withdrawn from the United States and European markets in 2008 due to problems with the delivery mechanism, but it was reintroduced in 2012.
The benefit of rotigotine for RLS/WED was demonstrated in a meta-analysis of five randomized controlled trials totalling over 600 patients, in which the average improvement in IRLS score over placebo was 7 points (95% CI 5.6-8.4) [3]. Two long-term follow-up studies (52 to 104 weeks) have reported a mean improvement of 15 to 17 points on the IRLS scale [33,34].
Transdermal rotigotine is a once-daily patch that is typically started at 1 mg/24 hours and titrated upwards to a maximum dose of 3 mg/24 hours. Application site reaction is the most common adverse effect of rotigotine, reported by 40 to 50 percent of patients. To decrease the risk of skin reactions, the manufacturer recommends rotating application sites, avoidance of direct sun exposure, and removal of the patch during magnetic resonance imaging. Other side effects are similar to those seen with oral dopamine agonists, including augmentation. (See 'Augmentation' below.)
Alpha-2-delta calcium channel ligands — Gabapentin enacarbil, gabapentin, and pregabalin are alternative choices for patients with chronic persistent RLS, and the FDA has approved gabapentin enacarbil for this indication [5,35,36].
The alpha-2-delta calcium channel ligands may be particularly useful when RLS/WED occurs in the setting of a painful peripheral neuropathy or an unrelated chronic pain syndrome and in patients with
comorbid insomnia or sleep disturbance that is disproportionate to other RLS/WED symptoms [20]. They are preferred over dopamine agonists in patients with impulse control disorders and are probably more helpful than dopamine agonists in patients with comorbid anxiety.
They may also be considered in the treatment of RLS/WED in association with Parkinson disease, since these patients may already be receiving dopaminergic therapy, or as an add-on therapy in patients with a partial response to dopamine agonist therapy but intolerance to higher doses. Unlike the dopamine agonists, they are not associated with augmentation.
As with other antiepileptic drugs (AEDs), the alpha-2-delta calcium channel ligands may be associated with an increased risk of suicidal thoughts and behavior, and patients should be monitored for emergent suicidality and depression. (See "Overview of the management of epilepsy in adults", section on 'Specific adverse reactions'.)
Gabapentin enacarbil — Several randomized, placebo-controlled studies have demonstrated that gabapentin enacarbil is effective in reducing RLS/WEDsymptom severity [3]. In the largest study of 325 patients, gabapentin enacarbil at a dose of 600 or 1200 mg/day was associated with a 3- to 4-point improvement in IRLS scores compared with placebo [37]. In another randomized study, gabapentin enacarbil also showed efficacy in decreasing the polysomnographic parameters of wake time during sleep and number of periodic limb movements with arousals per hour of sleep [38].
The recommended dose of gabapentin enacarbil for RLS/WED is 600 mg, taken in the early evening (eg, at 5 pm). Common adverse effects associated with gabapentin enacarbil include somnolence and dizziness; these are generally mild to moderate and remit with time. In a 52-week open-label study, two-thirds of patients reported mild to moderate side effects, leading to treatment discontinuation in 10 percent [39]. Somnolence, dizziness and weight gain were among the most common reasons for discontinuation. Although not formally assessed with rating scales, augmentation was not recognized in any patients based on retrospective review of adverse events.
Gabapentin — More limited data also suggest that gabapentin may be effective in RLS/WED. Gabapentin, mean dose 733 mg/day, was effective in a four-week open-label study of nine patients with idiopathic RLS [40], and at a much higher mean dose (1855 mg) in a randomized, placebo-controlled trial of 22 patients [41]. Although this trial suggested that mean gabapentin doses of 1800 mg a day are needed, many patients appear to benefit from a lower dose.
We suggest beginning treatment at 100 to 300 mg per dose because of the tendency of the drug to cause somnolence and gait unsteadiness [5]. Among dialysis patients, low-dose gabapentin (200 to 300 mg three times weekly after hemodialysis) was effective in a 12-week, double-blind crossover study [42].
Pregabalin — In a small randomized trial of 58 patients, pregabalin (starting dose 150 mg daily, mean dose 337 mg daily) was superior to placebo for improving symptoms of RLS/WED [43].
In a subsequent larger randomized trial, pregabalin was compared with pramipexole and placebo in 719 patients with RLS/WED [21]. After 12 weeks of therapy, both pregabalin (300 mg daily) and pramipexole (0.5 mg daily) were associated with a significant 3- to 4-point improvement in IRLS scores compared with placebo. Over 40 to 52 weeks of treatment, pregabalin was noninferior to pramipexole on measures of efficacy and was associated with a significantly lower augmentation rate (2.1 percent) compared with pramipexole at a dose of 0.25 mg (5.3 percent) or 0.5 mg (7.7 percent). In contrast, pregabalin was associated with a slightly higher rate of treatment discontinuation due to side effects (28 percent, versus 19 and 24 percent for pramipexole 0.25 mg and 0.5 mg daily, respectively). Suicidal ideation was reported in six patients taking pregabalin and in five patients taking pramipexole.
Similar to gabapentin enacarbil, pregabalin may also improve subjective and objective measures of sleep maintenance and total sleep time in patients with RLS and comorbid insomnia [44].
We suggest starting pregabalin at a dose of 50 to 75 mg per day. The usual effective dose is 150 to 450 mg. The most common side effects reported with pregabalin include dizziness, somnolence, fatigue, headache, peripheral edema, and weight gain [21,43].
Duration of therapy — RLS/WED is often a lifelong disease, but the optimal and safe duration of pharmacologic therapy has not been well established [20]. Most of the supporting data are based on relatively short (≤12-week) randomized trials, with fewer long-term extension studies supporting efficacy for 6 to 12 months of therapy with either a dopamine agonist or gabapentin enacarbil.
In clinical practice, the most common problems that arise with long-term therapy are loss of efficacy and augmentation. (See 'Augmentation' below and 'Refractory RLS' below.)
INTERMITTENT SYMPTOMS
Choice of therapy — In patients with mild or intermittent symptoms, nonpharmacologic therapies may be sufficient for symptom relief. In other patients, clinically significant symptoms do not occur frequently enough to require daily treatment but are nonetheless disabling when they do occur. For such patients, we suggest use of levodopa or a dopamine agonist on an as-needed basis. While this approach has not been systematically studied in clinical trials, clinical experience suggests that it is a reasonable strategy.
The use of dopamine agonists in restless legs syndrome/Willis-Ekbom disease (RLS/WED) is discussed in more detail above (see 'Dopamine agonists' above). Other treatment options include intermittent use of levodopa, a benzodiazepine, or a low-potency opioid [5]. (See 'Levodopa' below and 'Benzodiazepines' below and'Opioids' below.)
Levodopa — Levodopa was the first drug to be formally studied in RLS/WED, and its ability to ameliorate symptoms of RLS/WED has long been recognized. However, use of levodopa for RLS/WED has waned over time as the risk for augmentation has been better characterized, and as other dopaminergic agents that have a lower risk for augmentation have become available. (See 'Augmentation' below.)
Levodopa remains a reasonable "on demand" treatment option for patients with intermittent RLS who do not require daily therapy [3,5].
Several small randomized studies have demonstrated that levodopa improves RLS/WED symptom severity, number of periodic limb movements in sleep (PLMS), self-rated sleep quality, and quality of life compared with placebo [45]. Most studies were performed before the International Restless Leg Syndrome Study Group (IRLS) rating scale became widely used as an outcome measure; in two studies that reported RLS/WED symptom severity on a 10-point scale, levodopa improved symptom severity by a mean of 1.34 points compared with placebo [45]. Levodopa was also effective in a double-blind study of uremic RLS/WED [46].
Short-term therapy with levodopa is generally well tolerated; common adverse effects such as nausea, dizziness, and somnolence are usually mild and improve over time. Other problems that may occur in patients on levodopa include symptom rebound in the early morning (20 to 35 percent) or in the second half of the night [47,48]. Controlled release (CR) carbidopa-levodopa combined with standard carbidopa-levodopa may help sleep quality during the second half of the night for patients who experience recurrence [49].
For best absorption, levodopa should not be taken with high protein foods. Suggested agents include:
●Carbidopa-levodopa 25 mg/100 mg, one-half or one tablet, can be used as a starting dose for intermittent RLS/WED that occurs during the evening, at bedtime, or on waking during the night. Additionally, this medication may be helpful for RLS/WED associated with specific triggers including lengthy travel by auto or airline, or spectator events with prolonged sitting. Levodopa doses greater than 200 mg per day should be avoided.●Carbidopa-levodopa CR, starting at 25 mg/100 mg before bed, may be helpful for RLS/WED symptoms that awaken the patient during the night.
Benzodiazepines — Benzodiazepines can be useful in mild cases of RLS/WED, particularly in younger patients [50,51]. The best-studied benzodiazepine inRLS/WED is clonazepam.
In a small randomized, double-blind, crossover trial, treatment with clonazepam, 1 mg daily, was superior to placebo in six patients with RLS/WED [52]. In an open trial, 14 of 15 patients with RLS/WED due to uremia responded to clonazepam, 1 to 2 mg daily [53]. Clinical experience suggests that clonazepam is useful in some patients at 0.5 mg daily.
Although most trials have been performed with clonazepam, its long duration of action may result in more adverse effects, such as nocturnal unsteadiness, drowsiness or cognitive impairment in the morning, impotence, and exacerbation of sleep apnea [54]. However, at least one study has shown a low rate of adverse effects from clonazepam in older adult patients [50].
Long-term maintenance treatment with benzodiazepines is limited by tolerance in many patients, but abuse appears to be low in this disorder. Because of tolerance and the potential for side effects, use of benzodiazepines for RLS/WED is generally limited to those patients that require only intermittent therapy, or as an add-on agent in patients with refractory symptoms.
Short-acting benzodiazepine receptor agonists such as zolpidem should generally be avoided, as a high frequency of sleepwalking and sleep-related eating disorder has been reported with their use in the setting of RLS/WED (as high as 80 percent in one study of 15 patients) [55-57].
AUGMENTATION — Augmentation is the main complication of long-term dopaminergic therapy for restless legs syndrome/Willis-Ekbom disease (RLS/WED). It refers to an overall increase in RLS/WED symptom severity with increasing doses of medication, including earlier onset of symptoms, increased intensity of symptoms, shorter duration of drug action, or topographic spread of symptoms to other body parts, including the trunk and arms.
Augmentation should be considered a possibility in the following circumstances [58]:
●A maintained increase in symptom severity despite appropriate treatment●A maintained increase in symptom severity following a dose increase, particularly if a dose reduction leads to an improvement in symptoms●Earlier onset of symptoms in the afternoon/evening●Topographic spreading of symptoms to previously unaffected body parts●Shorter latency to symptom onset during the day when at rest●Shorter duration of action of the drug
Augmentation was first recognized in patients taking levodopa. In one study of 23 patients with severe RLS/WED treated with a combination of regular release and sustained-release levodopa (mean total daily dose of levodopa, 388 mg), two-thirds of patients stopped therapy before the end of the planned year of therapy due to increased severity of RLS during the day [59]. In a multicenter open-label study using flexible dosing of levodopa (mean maximum daily dose, 311 mg), 60 percent of patients developed augmentation at a median time of 71 days into therapy, leading to treatment
discontinuation in 12 percent [60]. Augmentation was significantly more common in patients taking greater than or equal to 300 mg of levodopa daily (70 versus 35 percent).
The risk of augmentation with dopamine agonists appears to be lower but not insignificant; it has been reported in 3 to 9 percent of patients taking pramipexole for one year [21], about one-third of patients taking pramipexole for two years [61], and 42 to 68 percent of patients taking pramipexole for 8 to 10 years [29,62]. Fewer studies have been performed on ropinirole, but it appears that the short-term augmentation rate is similar to that of pramipexole. Augmentation has been reported in 2 to 9 percent of patients taking rotigotine for one year [34,63,64] and 38 percent of those using rotigotine for five years (only clinically significant in 13 percent) [65]. The definition of augmentation and the method of assessment (ie, retrospective or prospective) have varied across studies, and therefore direct comparisons are difficult.
The risk of augmentation increases with higher daily doses, longer duration of use, and lower iron stores [21,66]. Other risk factors for augmentation are not well known; in one study, augmentation was significantly more common in patients with a family history of RLS/WED and in those who had no evidence of neuropathy on electromyography or nerve conduction studies [67].
Using dopaminergic drugs on an intermittent basis rather than continuously may lower the risk of augmentation, although this has not been well studied. This is the rationale for use of levodopa in patients with intermittent RLS/WED, despite the high risk of augmentation with continuous use.
Alpha-2-delta calcium channel ligands have not been associated with augmentation.
Management of augmentation has not been systematically studied, but several strategies can be used when it is recognized in patients on dopamine agonists.
●For mild augmentation, the dose of a dopamine agonist can be split between a nighttime dose and a dose earlier in the day. If this is ineffective, the dose can be modestly increased, but caution should be used not to exceed the maximum recommended total daily dosage. In addition, the patient should be carefully followed to ensure that augmentation is not worsening.●For more severe augmentation, switching from pramipexole or ropinirole to the extended release preparation, rotigotine, can sometimes help, as the rate of significant augmentation may be less with rotigotine.●Alternatively, dopamine agonists can be discontinued and replaced with alpha-2-delta calcium channel ligands [5]. We typically introduce the new drug and increase the dose to an effective level before slowly reducing the dopamine agonist and discontinuing if at all possible. Some experts advocate a 10-day wash-out period before introducing the alpha-2-delta ligand in order to establish a baseline measure of disease severity, but this can result in increased RLS/WEDsymptoms and profound insomnia during the wash-out period.●Iron stores should be re-evaluated and iron replacement initiated if stores are low. (See 'Iron replacement' above.)
REFRACTORY RLS — Refractory restless legs syndrome/Willis-Ekbom disease (RLS/WED) is defined as restless legs unresponsive to monotherapy with tolerable doses of a dopamine agonist or alpha-2-delta ligand due to reduced efficacy, augmentation, or adverse effects [5].
In patients with refractory symptoms, iron stores should be re-evaluated and iron replacement initiated if stores are low. Lifestyle practices, concomitant medications, and treatment adherence should also be reviewed. (See 'Iron replacement' above and 'Avoidance of aggravating factors' above.)
Referral to a specialist for RLS/WED management should be considered for these patients [54]. The main pharmacologic treatment options are:
●Use a combination of agents, such as a dopamine agonist, alpha-2 delta ligand, and/or a benzodiazepine. (See 'Dopamine agonists' above and 'Alpha-2-delta calcium channel ligands' above and 'Benzodiazepines' above.)●Change to a high-potency opioid. (See 'Opioids' below.)
Opioids — Opioids can be effective in the treatment of chronic and refractory RLS/WED, particularly for patients who have not responded to other therapies. A variety of opioids, including oxycodone, codeine, propoxyphene, methadone, and tramadol, have been reported to be helpful for RLS/WED, primarily in uncontrolled trials [3,59].
In a double-blind, four-week crossover study of 11 patients, oxycodone (mean dose 16 mg/day) was superior to placebo with regard to number of sleep arousals, periodic leg movement frequency, and sleep efficiency [68]. One long-term retrospective study of 113 patients treated with opioids demonstrated persistent benefit, but a small number of patients developed sleep apnea [69].
In a double-blind, multicenter trial of 276 patients with refractory RLS/WED, controlled release oxycodone-naloxone was significantly more effective than placebo at 12 weeks (mean difference in International Restless Legs Syndrome Study Group [IRLS] scores: 8.15) [70]. The mean daily dose of oxycodone was 22 mg. Benefit was preserved over a 40-week, open-label extension period. Fatigue and constipation were the most common side effects; two patients developed ileus or sub-ileus. No augmentation was seen.
In a 10-year, open-label study of methadone for RLS/WED, 15 percent of 76 patients discontinued methadone treatment in the first year, but the remainder continued to use it with benefit. The mean daily dose after six months was 10 mg, with subsequent increases of no more than 10 mg [62].
Low potency opioids or opioid agonists can be used for intermittent RLS [54]. These drugs are usually taken before bed and include:
●Codeine 30 to 60 mg.●Tramadol 50 to 100 mg before bed or during the night. Of note, tramadol has also been reported to cause augmentation in some patients [15].
Similar to benzodiazepines, tolerance to high potency opioids can develop with long-term maintenance therapy, but opioid abuse potential appears to be low in patients with RLS/WED in the absence of a history of substance abuse. Nevertheless, we typically restrict use to patients with more severe symptoms who fail to respond to other agents. Potential side effects include constipation, nausea, fatigue, itchiness, unsteadiness, and exacerbation of sleep apnea. Agents include [54]:
●Oxycodone 5 to 30 mg●Hydrocodone 5 to 30 mg●Methadone 2.5 to 20 mg
Other drugs — Other drugs that may be useful in RLS/WED but have been reported in only a small number of (mainly open-label) studies include carbamazepine(mean dose 236 mg/day) [71], clonidine (0.05 mg/day) [72], and amantadine (up to 300 mg/day) [73]. There is inadequate evidence to suggest that magnesium supplementation is an effective treatment for RLS/WED.
SPECIAL POPULATIONS
Pregnancy and lactation — Management of restless legs syndrome/Willis-Ekbom disease (RLS/WED) during pregnancy should be individualized based on symptom severity, comorbidities such as depression or anxiety, and patient preferences.
Many patients can be managed successfully with education, reassurance, iron supplementation if indicated, and nonpharmacologic strategies. Pharmacologic therapies such as clonazepam or carbidopa-levodopa may be considered for severe symptoms in women who wish to try medication. (See "Restless legs syndrome/Willis-Ekbom disease during pregnancy and lactation".)
End-stage renal disease — The management of RLS/WED in patients with end-stage renal disease is similar to that in patients with normal renal function. However, medication doses may need to be adjusted, especially if the patient is not yet receiving dialysis, as dopamine agonists and alpha-2-delta ligands are all excreted by the kidneys. Careful attention to iron status is especially important in this group [74]. (See "Sleep disorders in end-stage renal disease", section on 'Treatment'.)
PERIODIC LIMB MOVEMENT DISORDER — Periodic limb movements of sleep (PLMS) accompany many sleep and neurologic disorders, including restless legssyndrome/Willis-Ekbom disease (RLS/WED), obstructive sleep apnea, rapid eye movement (REM) sleep behavior disorder, narcolepsy, and Parkinson disease. PLMS increase in frequency with age. (See "Clinical features and diagnosis of restless legs syndrome/Willis-Ekbom disease and periodic limb movement disorder in adults", section on 'Periodic limb movements of sleep'.)
PLMS do not have a consistent relationship with symptoms (eg, insomnia, excessive daytime sleepiness) or with polysomnographic variables of sleep disruption. They are generally considered to be an age-related phenomenon, a response to arousals, or an epiphenomenon of other disorders. However, occasionally they occur abundantly with frequent electroencephalographic arousals in the absence of other disorders, leading the clinician to suspect that they are directly responsible for complaints of excessive sleepiness or insomnia. The term periodic limb movement disorder (PLMD) should be restricted to this subgroup.
For patients with PLMS associated with RLS/WED, treatment should concentrate on the symptoms of RLS/WED rather than on the leg movements. For PLMS associated with other sleep disorders, independent treatment of PLMS is rarely required.
There are limited data regarding management of PLMD. Polysomnographic studies of PLMS in RLS/WED have shown reduction in the periodic limb movement index with pramipexole, ropinirole, rotigotine, gabapentin, gabapentin enacarbil, and pregabalin [3,38,75]. A comparison study suggested greater reduction with pramipexole compared with pregabalin [44].
Extrapolating from this data, we suggest a trial of dopamine agonist therapy in suspected cases of PLMD. If there are contraindications to dopamine agonist therapy, an alpha-2-delta ligand can be tried. Dosing and safety considerations are the same as for use in RLS/WED. (See 'Dopamine agonists' above and 'Alpha-2-delta calcium channel ligands' above.)
If the primary symptoms of insomnia or sleepiness do not respond to adequate doses of the selected drug, then the patient should be re-evaluated for other causes of insomnia or excessive daytime sleepiness. (See "Clinical features and diagnosis of insomnia" and "Approach to the patient with excessive daytime sleepiness".)
Clonazepam, valproate, and selegiline have been reported to help PLMD in small, uncontrolled studies [3]. It would appear, however, that clonazepam reduces arousals rather than eliminates PLMS.
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and "Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5th to 6th grade reading level, and they answer the four or five key questions a patient might
have about a given condition. These articles are best for patients who want a general overview and who prefer short, easy-to-read materials. Beyond the Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are written at the 10th to 12th grade reading level and are best for patients who want in-depth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or e-mail these topics to your patients. (You can also locate patient education articles on a variety of subjects by searching on "patient info" and the keyword(s) of interest.)
●Basics topic (see "Patient information: Restless legs syndrome (Willis-Ekbom disease) (The Basics)" and "Patient information: Nocturnal (nighttime) leg cramps (The Basics)")
Online information and support is available for patients with RLS/WED through The Restless Legs Syndrome Foundation and the American Academy of Sleep Medicine (yoursleep.aasmnet.org).
SUMMARY AND RECOMMENDATIONS — Restless legs syndrome/Willis-Ekbom disease (RLS/WED) is a treatable condition that generally responds well to pharmacologic therapy. A variety of treatments for RLS/WED have been studied in randomized controlled trials. The goals of therapy are to reduce or eliminate symptoms of RLS/WED and improve daytime function, sleep, and quality of life.
●Iron stores should be evaluated in all patients with suspected or established RLS/WED. We suggest a trial of oral iron therapy for patients with iron deficiency or low-normal ferritin levels (ie, serum ferritin level <75 mcg/mL) (Grade 2C). (See 'Iron replacement' above.)●Nonpharmacologic therapy options include avoidance of aggravating drugs and substances such as caffeine (table 1), mental alerting activities, short daily hemodialysis for patients in renal failure, exercise, leg massage, and applied heat. In patients with mild and/or intermittent symptoms, these therapies may be sufficient for symptom relief. (See 'Nonpharmacologic therapy' above.)●In patients with chronic persistent RLS/WED despite nonpharmacologic therapies, we recommend pharmacologic therapy with a non-ergot dopamine agonist or an alpha-2-delta calcium channel ligand (Grade 1B). The choice between the two classes of drugs is based on symptom severity, patient age and comorbidities, drug side effect profiles, and patient preferences. (See 'Choice of therapy' above.)
•For patients with very severe RLS/WED, comorbid depression, or obesity/metabolic syndrome, we suggest initial therapy with a dopamine agonist (pramipexole, ropinirole, or rotigotine) rather than an alpha-2-delta calcium channel ligand (Grade 2C). (See 'Dopamine agonists' above.)•For patients with comorbid pain, anxiety, or insomnia or a history of impulse control disorder or addiction associated with use of a dopamine agonist, we suggest starting with an alpha-2-delta calcium channel ligand (gabapentin enacarbil, gabapentin, or pregabalin) (Grade 2C). (See 'Alpha-2-delta calcium channel ligands' above.)•For most other patients, we initially try an alpha-2-delta calcium channel ligand because of the risk of augmentation with dopamine agonists, but other potential side effects of the various drugs should also be considered. In general, older patients are more prone to side effects of alpha-2-delta ligands. If the first drug chosen is ineffective or poorly tolerated, then a drug of the other class should be tried.
●In patients with intermittent symptoms that are not frequent enough to require daily therapy but are nonetheless disabling when they do occur, we suggest a trial of a dopamine agonist or
levodopa on an as-needed basis (Grade 2C). Other treatment options for intermittent symptoms include benzodiazepines and opioids. (See 'Intermittent symptoms' above.)●When RLS/WED symptoms are refractory to first-line therapy with a dopamine agonist or an alpha-2-delta calcium channel ligand, treatment options include combination therapy and opioids. (See 'Refractory RLS' above.)●Augmentation, which refers to an overall worsening of RLS/WED symptom severity, with earlier onset of symptoms, shorter symptom latency with rest, shorter duration of action of drugs, or spread of symptoms to trunk or arms, is the most common complication of long-term dopaminergic therapy. Augmentation may be managed by alteration in the treatment regimen. (See 'Augmentation' above.)●RLS/WED is common during pregnancy. Many patients can be managed successfully with education, reassurance, iron supplementation if indicated, and nonpharmacologic strategies. Pharmacologic therapies such as clonazepam and carbidopa-levodopa may be considered for severe symptoms. (See "Restless legs syndrome/Willis-Ekbom disease during pregnancy and lactation".)●Treatment of periodic limb movement disorder (PLMD) as an entity distinct from RLS/WED is not well studied, but the approach is similar to that of RLS/WED. Periodic limb movements of sleep (PLMS) in the absence of insomnia or excessive daytime sleepiness do not require treatment. (See 'Periodic limb movement disorder' above.)
ACKNOWLEDGMENT — The editorial staff at UpToDate would like to acknowledge Robert Sheon, MD, who contributed to an earlier version of this topic review.
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Trotti LM, Bhadriraju S, Becker LA. Iron for restless legs syndrome. Cochrane Database Syst Rev 2012; 5:CD007834.
2. Scholz H, Trenkwalder C, Kohnen R, et al. Dopamine agonists for restless legs syndrome. Cochrane Database Syst Rev 2011; :CD006009.
3. Aurora RN, Kristo DA, Bista SR, et al. The treatment of restless legs syndrome and periodic limb movement disorder in adults--an update for 2012: practice parameters with an evidence-based systematic review and meta-analyses: an American Academy of Sleep Medicine Clinical Practice Guideline. Sleep 2012; 35:1039.
4. Wilt TJ, MacDonald R, Ouellette J, et al. Pharmacologic therapy for primary restless legs syndrome: a systematic review and meta-analysis. JAMA Intern Med 2013; 173:496.
5. Silber MH, Becker PM, Earley C, et al. Willis-Ekbom Disease Foundation revised consensus statement on the management of restless legs syndrome. Mayo Clin Proc 2013; 88:977.
6. Wang J, O'Reilly B, Venkataraman R, et al. Efficacy of oral iron in patients with restless legs syndrome and a low-normal ferritin: A randomized, double-blind, placebo-controlled study. Sleep Med 2009; 10:973.
7. Sloand JA, Shelly MA, Feigin A, et al. A double-blind, placebo-controlled trial of intravenous iron dextran therapy in patients with ESRD and restless legs syndrome. Am J Kidney Dis 2004; 43:663.
8. Allen RP, Adler CH, Du W, et al. Clinical efficacy and safety of IV ferric carboxymaltose (FCM) treatment of RLS: a multi-centred, placebo-controlled preliminary clinical trial. Sleep Med 2011; 12:906.
9. Earley CJ, Horská A, Mohamed MA, et al. A randomized, double-blind, placebo-controlled trial of intravenous iron sucrose in restless legs syndrome. Sleep Med 2009; 10:206.
10. Grote L, Leissner L, Hedner J, Ulfberg J. A randomized, double-blind, placebo controlled, multi-center study of intravenous iron sucrose and placebo in the treatment of restless legs syndrome. Mov Disord 2009; 24:1445.
11. Barton JC, Wooten VD, Acton RT. Hemochromatosis and iron therapy of Restless Legs Syndrome. Sleep Med 2001; 2:249.
12. Mitchell UH. Nondrug-related aspect of treating Ekbom disease, formerly known as restless legs syndrome. Neuropsychiatr Dis Treat 2011; 7:251.
13. Aukerman MM, Aukerman D, Bayard M, et al. Exercise and restless legs syndrome: a randomized controlled trial. J Am Board Fam Med 2006; 19:487.
14. Lettieri CJ, Eliasson AH. Pneumatic compression devices are an effective therapy for restless legs syndrome: a prospective, randomized, double-blinded, sham-controlled trial. Chest 2009; 135:74.
15. Hoque R, Chesson AL Jr. Pharmacologically induced/exacerbated restless legs syndrome, periodic limb movements of sleep, and REM behavior disorder/REM sleep without atonia: literature review, qualitative scoring, and comparative analysis. J Clin Sleep Med 2010; 6:79.
16. Rottach KG, Schaner BM, Kirch MH, et al. Restless legs syndrome as side effect of second generation antidepressants. J Psychiatr Res 2008; 43:70.
17. Nofzinger EA, Fasiczka A, Berman S, Thase ME. Bupropion SR reduces periodic limb movements associated with arousals from sleep in depressed patients with periodic limb movement disorder. J Clin Psychiatry 2000; 61:858.
18. Burbank F, Buchfuhrer M, Kopjar B. Sleep improvement for restless legs syndrome patients. Part I: pooled analysis of two prospective, double-blind, sham-controlled, multi-center, randomized clinical studies of the effects of vibrating pads on RLS symptoms. Journal of Parkinsonism and Restless Legs Syndrome 2013; 3:1.
19. Trenkwalder C, Hening WA, Montagna P, et al. Treatment of restless legs syndrome: an evidence- based review and implications for clinical practice. Mov Disord 2008; 23:2267.
20. Garcia-Borreguero D, Kohnen R, Silber MH, et al. The long-term treatment of restless legs syndrome/Willis-Ekbom disease: evidence-based guidelines and clinical consensus best practice guidance: a report from the International Restless Legs Syndrome Study Group. Sleep Med 2013; 14:675.
21. Allen RP, Chen C, Garcia-Borreguero D, et al. Comparison of pregabalin with pramipexole for restless legs syndrome. N Engl J Med 2014; 370:621.
22. Trenkwalder C, Benes H, Grote L, et al. Cabergoline compared to levodopa in the treatment of patients with severe restless legs syndrome: results from a multi-center, randomized, active controlled trial. Mov Disord 2007; 22:696.
23. Bassetti CL, Bornatico F, Fuhr P, et al. Pramipexole versus dual release levodopa in restless legs syndrome: a double blind, randomised, cross-over trial. Swiss Med Wkly 2011; 141:w13274.
24. Trenkwalder C, Kohnen R, Allen RP, et al. Clinical trials in restless legs syndrome--recommendations of the European RLS Study Group (EURLSSG). Mov Disord 2007; 22 Suppl 18:S495.
25. Inoue Y, Kuroda K, Hirata K, et al. Long-term open-label study of pramipexole in patients with primary restless legs syndrome. J Neurol Sci 2010; 294:62.
26. Partinen M, Hirvonen K, Jama L, et al. Open-label study of the long-term efficacy and safety of pramipexole in patients with Restless Legs Syndrome (extension of the PRELUDE study). Sleep Med 2008; 9:537.
27. Winkelman JW, Sethi KD, Kushida CA, et al. Efficacy and safety of pramipexole in restless legs syndrome. Neurology 2006; 67:1034.
28. Trenkwalder C, Garcia-Borreguero D, Montagna P, et al. Ropinirole in the treatment of restless legs syndrome: results from the TREAT RLS 1 study, a 12 week, randomised, placebo controlled study in 10 European countries. J Neurol Neurosurg Psychiatry 2004; 75:92.
29. Lipford MC, Silber MH. Long-term use of pramipexole in the management of restless legs syndrome. Sleep Med 2012; 13:1280.
30. Stiasny K, Möller JC, Oertel WH. Safety of pramipexole in patients with restless legs syndrome. Neurology 2000; 55:1589.
31. Tippmann-Peikert M, Park JG, Boeve BF, et al. Pathologic gambling in patients with restless legs syndrome treated with dopaminergic agonists. Neurology 2007; 68:301.
32. Cornelius JR, Tippmann-Peikert M, Slocumb NL, et al. Impulse control disorders with the use of dopaminergic agents in restless legs syndrome: a case-control study. Sleep 2010; 33:81.
33. Oertel WH, Benes H, Garcia-Borreguero D, et al. One year open-label safety and efficacy trial with rotigotine transdermal patch in moderate to severe idiopathic restless legs syndrome. Sleep Med 2008; 9:865.
34. Högl B, Oertel WH, Stiasny-Kolster K, et al. Treatment of moderate to severe restless legs syndrome: 2-year safety and efficacy of rotigotine transdermal patch. BMC Neurol 2010; 10:86.
35. Kushida CA, Becker PM, Ellenbogen AL, et al. Randomized, double-blind, placebo-controlled study of XP13512/GSK1838262 in patients with RLS. Neurology 2009; 72:439.
36. Kushida CA, Walters AS, Becker P, et al. A randomized, double-blind, placebo-controlled, crossover study of XP13512/GSK1838262 in the treatment of patients with primary restless legs syndrome. Sleep 2009; 32:159.
37. Lee DO, Ziman RB, Perkins AT, et al. A randomized, double-blind, placebo-controlled study to assess the efficacy and tolerability of gabapentin enacarbil in subjects with restless legs syndrome. J Clin Sleep Med 2011; 7:282.
38. Winkelman JW, Bogan RK, Schmidt MH, et al. Randomized polysomnography study of gabapentin enacarbil in subjects with restless legs syndrome. Mov Disord 2011; 26:2065.
39. Ellenbogen AL, Thein SG, Winslow DH, et al. A 52-week study of gabapentin enacarbil in restless legs syndrome. Clin Neuropharmacol 2011; 34:8.
40. Happe S, Klösch G, Saletu B, Zeitlhofer J. Treatment of idiopathic restless legs syndrome (RLS) with gabapentin. Neurology 2001; 57:1717.
41. Garcia-Borreguero D, Larrosa O, de la Llave Y, et al. Treatment of restless legs syndrome with gabapentin: a double-blind, cross-over study. Neurology 2002; 59:1573.
42. Thorp ML, Morris CD, Bagby SP. A crossover study of gabapentin in treatment of restless legs syndrome among hemodialysis patients. Am J Kidney Dis 2001; 38:104.
43. Garcia-Borreguero D, Larrosa O, Williams AM, et al. Treatment of restless legs syndrome with pregabalin: a double-blind, placebo-controlled study. Neurology 2010; 74:1897.
44. Garcia-Borreguero D, Patrick J, DuBrava S, et al. Pregabalin versus pramipexole: effects on sleep disturbance in restless legs syndrome. Sleep 2014; 37:635.
45. Scholz H, Trenkwalder C, Kohnen R, et al. Levodopa for restless legs syndrome. Cochrane Database Syst Rev 2011; :CD005504.
46. Trenkwalder C, Stiasny K, Pollmächer T, et al. L-dopa therapy of uremic and idiopathic restless legs syndrome: a double-blind, crossover trial. Sleep 1995; 18:681.
47. Earley CJ, Allen RP. Pergolide and carbidopa/levodopa treatment of the restless legs syndrome and periodic leg movements in sleep in a consecutive series of patients. Sleep 1996; 19:801.
48. Guilleminault C, Cetel M, Philip P. Dopaminergic treatment of restless legs and rebound phenomenon. Neurology 1993; 43:445.
49. Collado-Seidel V, Kazenwadel J, Wetter TC, et al. A controlled study of additional sr-L-dopa in L- dopa-responsive restless legs syndrome with late-night symptoms. Neurology 1999; 52:285.
50. Schenck CH, Mahowald MW. Long-term, nightly benzodiazepine treatment of injurious parasomnias and other disorders of disrupted nocturnal sleep in 170 adults. Am J Med 1996; 100:333.
51. Montplaisir J, Godbout R, Boghen D, et al. Familial restless legs with periodic movements in sleep: electrophysiologic, biochemical, and pharmacologic study. Neurology 1985; 35:130.
52. Montagna P, Sassoli de Bianchi L, Zucconi M, et al. Clonazepam and vibration in restless legs syndrome. Acta Neurol Scand 1984; 69:428.
53. Read DJ, Feest TG, Nassim MA. Clonazepam: effective treatment for restless legs syndrome in uraemia. Br Med J (Clin Res Ed) 1981; 283:885.
54. Silber MH, Ehrenberg BL, Allen RP, et al. An algorithm for the management of restless legs syndrome. Mayo Clin Proc 2004; 79:916.
55. Howell MJ, Schenck CH. Restless nocturnal eating: a common feature of Willis-Ekbom Syndrome (RLS). J Clin Sleep Med 2012; 8:413.
56. Lauerma H. Nocturnal wandering caused by restless legs and short-acting benzodiazepines. Acta Psychiatr Scand 1991; 83:492.
57. Morgenthaler TI, Silber MH. Amnestic sleep-related eating disorder associated with zolpidem. Sleep Med 2002; 3:323.
58. Garcia-Borreguero D, Stillman P, Benes H, et al. Algorithms for the diagnosis and treatment of restless legs syndrome in primary care. BMC Neurol 2011; 11:28.
59. Trenkwalder C, Collado Seidel V, Kazenwadel J, et al. One-year treatment with standard and sustained-release levodopa: appropriate long-term treatment of restless legs syndrome? Mov Disord 2003; 18:1184.
60. Högl B, García-Borreguero D, Kohnen R, et al. Progressive development of augmentation during long-term treatment with levodopa in restless legs syndrome: results of a prospective multi-center study. J Neurol 2010; 257:230.
61. Winkelman JW, Johnston L. Augmentation and tolerance with long-term pramipexole treatment of restless legs syndrome (RLS). Sleep Med 2004; 5:9.
62. Silver N, Allen RP, Senerth J, Earley CJ. A 10-year, longitudinal assessment of dopamine agonists and methadone in the treatment of restless legs syndrome. Sleep Med 2011; 12:440.
63. Inoue Y, Hirata K, Hayashida K, et al. Efficacy, safety and risk of augmentation of rotigotine for treating restless legs syndrome. Prog Neuropsychopharmacol Biol Psychiatry 2013; 40:326.
64. Beneš H, García-Borreguero D, Ferini-Strambi L, et al. Augmentation in the treatment of restless legs syndrome with transdermal rotigotine. Sleep Med 2012; 13:589.
65. Oertel W, Trenkwalder C, Beneš H, et al. Long-term safety and efficacy of rotigotine transdermal patch for moderate-to-severe idiopathic restless legs syndrome: a 5-year open-label extension study. Lancet Neurol 2011; 10:710.
66. Frauscher B, Gschliesser V, Brandauer E, et al. The severity range of restless legs syndrome (RLS) and augmentation in a prospective patient cohort: association with ferritin levels. Sleep Med 2009; 10:611.
67. Ondo W, Romanyshyn J, Vuong KD, Lai D. Long-term treatment of restless legs syndrome with dopamine agonists. Arch Neurol 2004; 61:1393.
68. Walters AS, Wagner ML, Hening WA, et al. Successful treatment of the idiopathic restless legs syndrome in a randomized double-blind trial of oxycodone versus placebo. Sleep 1993; 16:327.
69. Walters AS, Winkelmann J, Trenkwalder C, et al. Long-term follow-up on restless legs syndrome patients treated with opioids. Mov Disord 2001; 16:1105.
70. Trenkwalder C, Beneš H, Grote L, et al. Prolonged release oxycodone-naloxone for treatment of severe restless legs syndrome after failure of previous treatment: a double-blind, randomised, placebo-controlled trial with an open-label extension. Lancet Neurol 2013; 12:1141.
71. Telstad W, Sørensen O, Larsen S, et al. Treatment of the restless legs syndrome with carbamazepine: a double blind study. Br Med J (Clin Res Ed) 1984; 288:444.
72. Wagner ML, Walters AS, Coleman RG, et al. Randomized, double-blind, placebo-controlled study of clonidine in restless legs syndrome. Sleep 1996; 19:52.
73. Evidente VG, Adler CH, Caviness JN, et al. Amantadine is beneficial in restless legs syndrome. Mov Disord 2000; 15:324.
74. Giannaki CD, Hadjigeorgiou GM, Karatzaferi C, et al. Epidemiology, impact, and treatment options of restless legs syndrome in end-stage renal disease patients: an evidence-based review. Kidney Int 2014; 85:1275.
75. Oertel WH, Benes H, Garcia-Borreguero D, et al. Rotigotine transdermal patch in moderate to severe idiopathic restless legs syndrome: a randomized, placebo-controlled polysomnographic study. Sleep Med 2010; 11:848.
Topic 88241 Version 19.0http://www.uptodate.com/contents/treatment-of-restless-legs-syndrome-willis-ekbom-disease-and-periodic-limb-movement-disorder-in-adults
Untuk RLS ringan, gejala dapat membaik dengan terapi non-farmakologi, yaitu
dengan program latihan atau olahraga yang dilakukan rutin. Penggunaan mandi air
panas, pijat pada tungkai, dan heating pads dapat mengurangi gejala. Disamping
itu, penting juga untuk menghindari konsumsi alkohol karena dapat mengurangi
dan menurunkan kulaitas tidur sehingga dapat menyebabkan eksaserbasi RLS.
Pemberian preparat besi secara oral maupun intravena dapat mengurangi gejala
pada pasien RLS dengan kadar feritin serum rendah. Terapi pada RLS dapat
meliputi obat-oabt sebagai berikut :
1. Agonis Dopamin
Merupakan first-line teratment untuk RLS.
Memiliki efek terhadap level dopamin otak yang merupakan
neurotransmitter yang berperan penting dalalm sistem saraf pusat.
Contoh : ropinirole (Requip), pramipexole (Mirapex), pergolide (Permax)
Agen dopaminergik lainnya seperti levodopa (Sinemet) dapat digunakan
untuk RLS, tetapi memiliki efektifitas rendah serta efek samping yang lebih
banyak dibandingkan agonis dopamin.
2. Benzodiazepin
Obat golongan ini memiliki efektivitas yang lebih rendah dalam
mengurangi gejala RLS, tetapi memiliki kelebihan dalam meningkatkan
kualitas tidur. Dosis kecil benzodiazepin dapat digunakan untuk menangkal
efek stimulasi dari agonis dopamin.
Contoh : clonazepam (Klonipin)
3. Anti-konvulsan
Dianggap berpotensi rendah dibanding agonis dopamin.
Pilihan efektif untuk RLS ringan atau untuk paien yang tidak toleransi
terhadap agonis dopamin. Juga sangat berguna untuk pasien dengan sensai
nyeri.
Contoh : gabapentin (Neurontin)
4. Opioid
Digunakan pada pasien dengan gejala berat yang tidak respon terhadap
terapi farmakologi lainnya. Terapi ini juga dapat digunakan sebgai anti-
nyeri.
Contoh : kodein, propoxyphene (Darvon)