introduction to transcranial magnetic stimulation …gestaltrevision.be/pdfs/lss2014/tms lecture...
TRANSCRIPT

INTRODUCTION TO
TRANSCRANIAL MAGNETIC
STIMULATION FOR THE STUDY OF
BRAIN-BEHAVIOUR
RELATIONSHIPS
CAITLIN MULLIN
PERCEPTUAL ORGANIZATION SUMMER
SCHOOL 2014
*This presentation contains images taken from the internet for which I do
not hold the copyright.

OUTLINE
• History
• Nuts and bolts
• Aspects of the technique
• Experimental design
• Parameter selection
• Safety and ethical considerations
• [TMS with neuroimaging]

WHAT IS TMS?
TMS is a non-invasive tool for the electrical stimulation of
neural tissue.

TECHNIQUE ON THE RISE
Rossi., Hallett, Rossini, & Pascual-Leone (2009)

d’Arsonval(1896/1911)
Thompson, 1910
Magnusson &
Stevens, 1911
FUNNY PICTURES
Faraday, 1831

TRUST ME, I’M A DOCTOR

Barker, 1984
MODERN STIMULATOR

NUTS AND BOLTS

TMS coil current
8kA
Magnetic field pulse 2.5T
Rate of change of
magnetic field
30kT/s
Induced tissue current
15mA/cm2
Induced electric field
500v/m
HOW IT WORKS:
SEQUENCE OF EVENTS

WHAT CAN TMS DO FOR YOU
AS A RESEARCHER?
• Virtual Patients: causal link between brain activity and
behavior
Occipital TMS disrupts braille reading
in early blind, but not control subjects
Cohen et al., 1997.

WHAT CAN TMS DO FOR YOU
AS A RESEARCHER?
• Chronometry: timing the contribution of focal brain
activity to behavior
Hamilton & Pascual-Leone, 1998
Role of “visual” cortex in tactile information processing in early
blind subjects

WHAT CAN TMS DO FOR YOU
AS A RESEARCHER?
• Functional connectivity: relate behavior to the
interaction between elements of a neural network

TELL US WHAT WE REALLY
WANT TO KNOW ABOUT
TMS
• How are the neurons activated?
• How precise does the localization get?
• How deep can you stimulate?
• How long does the effect last?
It depends...

• Biophysical mechanisms influenced by TMS are still not fully understood.
• Prevailing hypothesis: Axons!
• The flow of ions brought about by the electric field induced in the brain alters the electric charge stored on both sides of cell membranes
• Any part of the cell membrane interrupting this motion of the charges becomes depolarised or hyperpolarised.
HOW NEURONS ARE
STIMULATED?
uniform current along the axon,
no change from the resting state gradient activation due to non uniform field
across the axon, resulting in action potential
bent axon in uniform electric field
causes action potential
depolarization caused by transverse activation of the neuron change in activation at the axon terminal

EXCITATION? INHIBITION?
IT’S ALL NOISE TO ME!
Hmmm?

NEUROPHYSIOLOGICAL
MECHANISMS?
Pa
ire
d a
sso
cia
tion
stim
ula
tion (
PA
S)
LTP
LTD
Increase in synaptic strength
Decrease in synaptic efficacy

STATE/RHYTHMIC TMS
EFFECTS
Romei, Driver, Schyns, & Thut, 2011 Dugué, Marque, & VanRullen, 2011

SUMMARY: SO HOW DOES
TMS EFFECT NEURONS?
Depends on:
•The spatial derivations of neurons underlying the coil
•The kind of stimulation protocol used (high vs. low
frequency)
•The preliminary state of the activity in the region

SPATIAL RESOLUTION
OF TMS
• Exact resolution cannot be measured in cm or mm
• The geometry of the coil determines the focality of the
magnetic field and of the induced current - hence also of
the targeted brain area.

SPATIAL RESOLUTION
OF TMS
Phosphenes can be elicited with a resolution
of 1-2 degrees of visual angle
Muscles that are segregated by as
little as 1 to 2 cm on the cortex can
be selectively stimulated in motor
cortex
Behavioural dissociations in spatially adjacent regions in the cortex

DEPTH OF
STIMULATION

SUMMARY: SPATIAL
RESOLUTION OF TMS
• Resolution depends on parameters of stimulation, coil
type, etc.
• But we can infer resolution from a number of observations
• Evidence from studies using these kinds of inferences
correspond with an effective spatial resolution of 1-2cm

THE TEMPORAL
RESOLUTION OF TMS
cycle of a single pulse of TMS is approximately 1ms
The duration of
the effect in the
cortex is difficult
to determine
because the
neurons
stimulated by the
field may take
time to recover
their normal
functional state
Thus the most important
consideration when
designing TMS experiments
is the duration of the
impairment to the
behavioural performance
being measured

KINDS OF PULSES
Single pulse TMS
• single stimulus every 5-10 sec
Repetitive TMS (rTMS)
• trains of stimuli to one brain area
Patterned TMS
• Theta-burst
• E.g. 100 triple-pulses at a
frequency of 5Hz with the
triple-pulse frequency of
50Hz

EXPERIMENTAL
DESIGN FOR TMS

THE QUESTION
CHOOSING PARAMETERS
• Where to stimulate
• Task/Dependent variables
• Methods for identifying your target site
• Coil localization
• Control conditions
• Choosing the best stimulation parameters
• - Intensity
• - Frequency
• - Type of stimulation
• - Duration

WHERE TO STIMULATE?
• Informed by:
• Patient studies
• Neuroimaging literature
• Do your own neuroimaging

WHERE TO STIMULATE?
THE BRAIN REGIONS
Zaretskaya, Anstis & Bartels, 2013

DEPENDENT VARIABLES
Zaretskaya, Anstis & Bartels, 2013
Percent of time in global vs. local percept
global local
Eye movement maps under both percepts
How to measure the effects of TMS

IDENTIFYING TMS
TARGET SITES
Find functional effect
- hand twitch (MEP)
- moving phosphenes
Find anatomical landmark
inion/nasion-ear/ear vertex
EEG 10/20 system
MRI/fMRI co-registration

IDENTIFYING TMS
TARGET SITES
Sack, Kadosh, Schuhmann, Moerel, Walsh, & Goebel, (2009)
IT’S ALL ABOUT THE POWER!
n = 5 fMRI
n = 9 MRI
n = 13 Tal coordinates
n = 47 EEG
10-20 system

IDENTIFYING TMS TARGET
SITES IN REAL TIME

IDENTIFYING TMS TARGET
SITES IN REAL TIME
Zaretskaya, Anstis & Bartels, 2013

Real
Sham
Different hemisphere
Different site
Different
effect or
no effect
Or interleave TMS with no TMS trials
CONTROL CONDITIONS

CONTROL CONDITIONS
Zaretskaya, Anstis & Bartels, 2013

Motor Threshold
INTENSITY
Phosphene Threshold
Bartels uses 80% of each individuals active motor threshold

FREQUENCY AND TYPES
OF STIMULATION
On-line:
Stimulation occurs while the subject
performs a task and the effects last for
approximately the duration of
stimulation.
• Good for chronometrics
• How many pulses?
Off-line:
Stimulation occurs without a task and
the length of effect is typically
measured in minutes.
• Low frequency stimulation
• Theta burst

FREQUENCY AND TYPES
OF STIMULATION
Dayan, Censor, Buch, Sandrini, & Cohen, (2013)

RECAP SO FAR?
• Where to stimulate:
• Task/Dependent variables:
• Methods for identifying your target site:
• Coil localization:
• Control conditions:
• Choosing the best stimulation parameters
- Intensity
- Frequency
- Type of stimulation
- Duration
RH aIPS & SPL – based on individual fMRI
Percent of time spent in each
local/global percept
fMRI localizer
Individual fMRI with stereotaxy
Vertex stimulation & baseline performance
80% active motor threshold
Continuous thetaburst stimulation: 48 s of
three pulses at 50 Hz repeated
every 0.2 s, resulting in 600 pulses in total
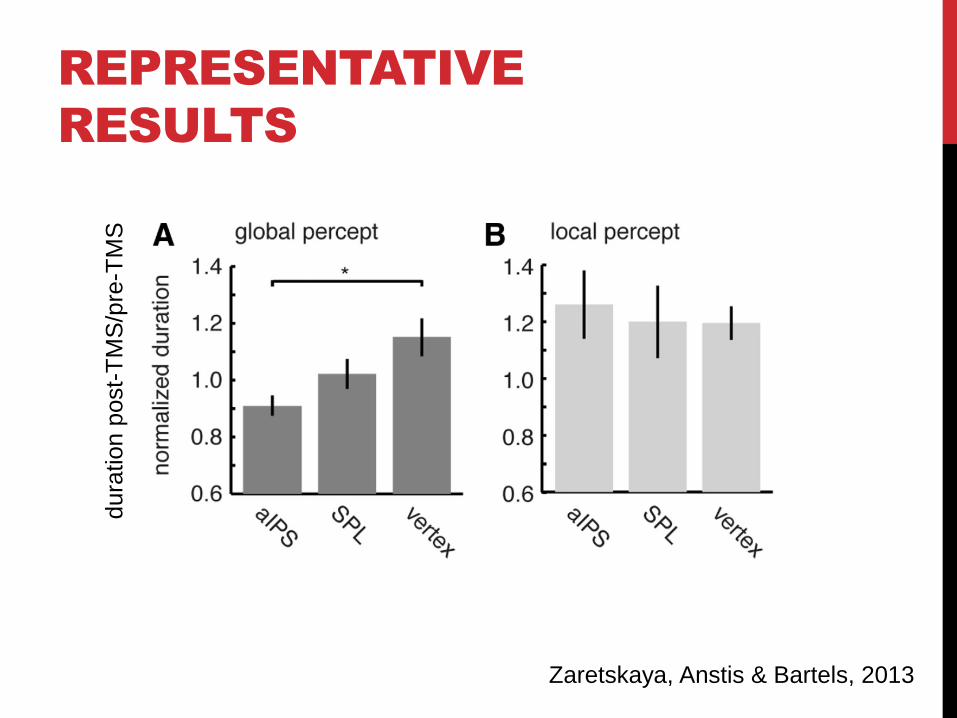
REPRESENTATIVE
RESULTS dura
tion p
ost-
TM
S/p
re-T
MS
Zaretskaya, Anstis & Bartels, 2013
CAUSAL
CONCLUSIONS
“Our results point to aIPS as a potential source of this high-level
grouping signal because it was most strongly activated during the
“global” compared with “local” perceptual state and because it
was causally involved in forming the global percept.”

WHAT ABOUT
TIMING?
We just walked through a virtual lesion study
- TMS protocol – straight forward
What about the chronometrics?
- Many of the decisions will remain the same

• Pascual-Leone et al. (1993), Safety of transcranial magnetic stimulation in normal volunteers.
Electroencephalogr Clin Neurophysiol, 89(2):120-130
• Chen et al. (1997), Safety of different inter-train intervals for repetitive transcranial magnetic
stimulation and recommendations for safe rages of stimulation parameters.
Electroencephalogr Clin Neurophysiol 105(6):415-421
• Wassermann. (1998), Risk and safety of repetitive transcranial magnetic stimulation: report
and suggested guidelines from the International Workshop on the Safety of Repetitive
Transcranial Magnetic Stimulation. June-5-7, 1996. Electroencephalogr Clin Neurophysiol
108(1):1-16
• Machii, et al. (2006). Safety of rTMS to non-motor cortical areas in healthy participants and
patients. Clinical Neurophysiology. 117, 455-471.
• Rossi, S., Hallett, M., Rossini, P. M., & Pascual-Leone, A. (2009). Safety, ethical
considerations, and application guidelines for the use of transcranial magnetic stimulation in
clinical practice and research. Clinical neurophysiology,120(12), 2008-2039.
SAFETY AND SIDE
EFFECTS

Side effect Single-pulse TMS
Paired-pulse TMS
Low frequency
rTMS
High frequency rTMS
Theta burst
Seizure induction Occasional Not reported Occasional (usually
protective effect)
Possible (1.4% crude risk
estimate in epileptic patients;
less than 1% in normals)
Not reported
Transient acute hypomania induction
No No Rare Possible following left prefrontal stimulation
Not known
Syncope Possible as epiphenomenon (i.e, not related to direct brain effect) Not reported
Transient headache, local pain, neck pain, toothache, paresthesia
Possible Likely possible, but not
reported/addressed
Frequent (see para. 3.3)
Frequent (see para. 3.3)
Not reported
Transient hearing changes or tinnitus
Possible Likely possible, but not reported
Possible Possible (avoid rTMS in
cochlear implants)
Not known
Transient cognitive/ neuropsychologial changes
Not reported No reported Overall negligible
(see para. 3.5)
Overall negligible (see para. 3.5)
Not known
Burns from scalp electrodes
No No Not reported Occasionally reported
Not known, but likely possible
Induced currents in electrical circuits
Theoretically possible, but described malfunction only if TMS is delivered in close proximity with the electric device
(pace-makers, brain stimulators, pumps, intacardiac lines)
Structural brain changes
Not reported Nor reported Inconsistent Inconsistent Not known
Histoxicity No No Inconsistent Inconsistent Not known
Other biological transient effects
Not reported Not reported Not reported Transient hormone changes
(Prolactine, TSH)
Not known
Rossi., Hallett, Rossini, & Pascual-Leone (2009)

SEIZURES
• Hypersynchronized discharges of groups of neurons in
gray matter
• -Imbalance between inhibitory and excitatory activity
• -Alterations of ion gradients in nerve cells
• -Factors leading to spread between cortical areas
• Two factors to take into consideration:
• -Parameters used
• -Individual receiving TMS stimulation
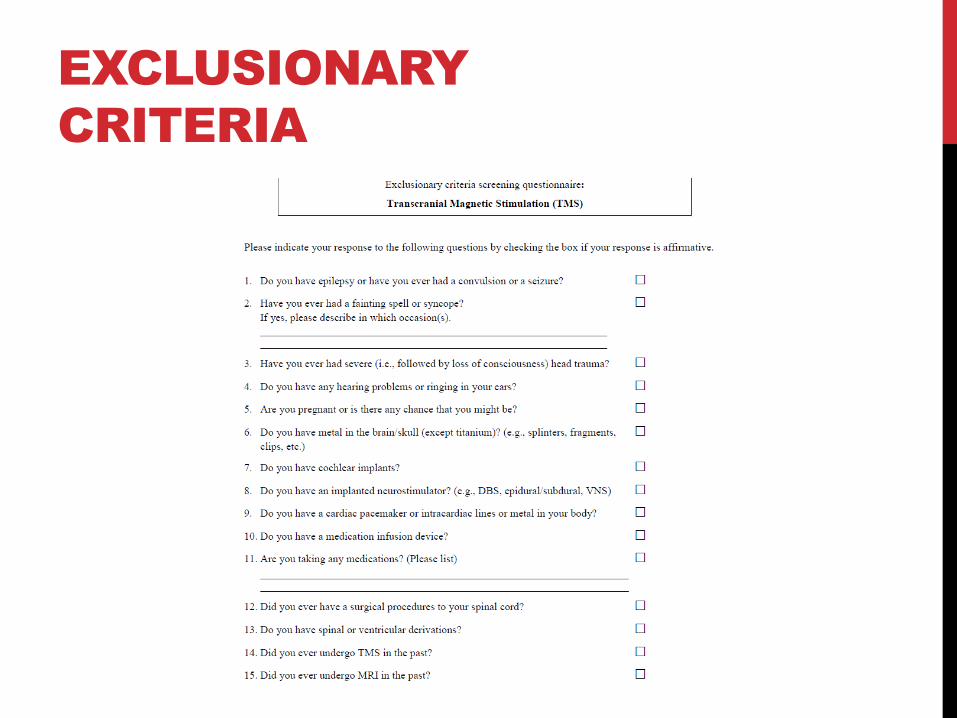
EXCLUSIONARY
CRITERIA

SAFETY GUIDELINES
Rossi., Hallett, Rossini, & Pascual-Leone (2009)

SIDE EFFECTS
• Most common adverse effects reported, and more common with rTMS (Loo et al 2007):
• -Headache: ~20% with single pulse; ~29% with rTMS
• -Neck pain or discomfort: up to 39% in rTMS
• Factors other than TMS also important!!: Headband, Swim cap, Neck posturing
• Prophylaxis and Treatment measures
• -Responds well to analgesics
• -Topical anesthetics have been tried
• -shorter blocks; frequent breaks

ETHICAL
CONSIDERATIONS
Although the risk is small, it is always present, so there is
an obligation on the experimenter to always consider the
value of a given experiment
• How can you minimize risk & discomfort?
• What is the minimal stimulation necessary?
• Is the TMS information clear and consent
informed?
• Are subjects always screened?
• Are the experimenters safety trained?
• Are emergency procedures clear & in place?
• Would YOU do this experiment?

Major limitations summary • Only regions on cortical surface can be stimulated
• Can be unpleasant for subjects
• Risks to subjects and esp. patients
• Stringent ethics required (can’t be used by some institutions)
• Localisation uncertainty
• Stimulation level uncertainty
Major advantages summary • Reversible lesions without plasticity changes
• Repeatable
• High spatial and temporal resolution
• Can establish causal link between brain activation and behaviour
• Can measure cortical plasticity
• Can modulate cortical plasticity
• Therapeutic benefits
TMS: YAY OR NE?