investigation and management of the patient with delirium
TRANSCRIPT

Excellence in Health putting People first
Investigation and management of the patient with delirium
Dr Lesley Young
Consultant geriatrician, Sunderland royal Hospital

Excellence in Health putting People first
Mary
• 83 year old lady from a care home presents to A&E
• Unwell for ~2/52
• “just not right”
• Reduced oral intake
• Drowsy
• More muddled

Excellence in Health putting People first
• “poor historian” - Appears confused,
• Background from medical records:
– Hypertension
– IHD
– OA
• From care home:
Normally “pleasantly confused”
1/12 ago Blood pressure tablets changed
1/52 ago treated for “presumed” UTI
Much more confused over past few days
Excellence in Health putting People first
• Medications:
– Bendroflumethiazide 5mg od
– Bisoprolol 5mg od
– Lisinopril 5mg od
– Simvastatin 20mg od
– Aspirin75mg od
– Codeine 30mg qds
– Trimethoprim for 5 days
• NEWS = 1 (sats 95% on air)
• Awake, but confused, apyrexial
• CVS – NAD BP 134/78
• Chest- NAD
• Abdo – NAD
– PR – hard stool
• No focal neurology
• Incontinent of urine

Excellence in Health putting People first
Initial investigations
• Hb N
• WBC 9
• CRP 14
• Na 122
• Urea 14
• Creat 161
• Urinalyisis - NAD
• CXR – NAD

Excellence in Health putting People first
Question 1?
Does she have a delirium?
YES?
NO?

Excellence in Health putting People first
What is delirium – DSM V
1. disturbance in attention (ie, reduced ability to direct, focus, sustain & shift attention) and orientation to the environment;
2. disturbance develops over a short period of time and represents an acute change from baseline, not solely attributable to another neurocognitive disorder and tends to fluctuate in severity during the course of a day;
3. a change in an additional cognitive domain, e.g. memory deficit, disorientation, or language disturbance, or perceptual disturbance not better accounted for by a pre-existing, established, or evolving other neurocognitive disorder
4. disturbances in 1 & 3 must not occur in the context of a severely reduced level of arousal, such as coma.

Excellence in Health putting People first
Types of delirium
Hypoactive

Excellence in Health putting People first
Question 2
• What proportion of adults in an acute hospital will have delirium?
1. 2%
2. 5%
3. 10%
4. 15%
5. 20%
6. 30%

Excellence in Health putting People first
How common is delirium?
• Most hospital beds occupied by older people
• Dementia v common in hospital population
• Dementia and age biggest risk factors for delirium
• Cork point prevalence study (Ryan BMJ Open 2013)
– 52% inattentive or “confused” – 20.7% delirium + 8.6% subsyndromal delirium
• 50.9% had pre-existing dementia (only 1 in 5 noted) • 64% recognised as “confused” by nurses • only 44% noted in medical case notes

Excellence in Health putting People first
But… Delirium is under-recognised:
• NHS coding data: Prevalence 0.7% (2013-14 data)
• In published studies only 20-50% of delirium noted in medical records(Foreman 2004)
• Hypoactive more easily overlooked (Inouye Arch Int Med 2001)
• In dementia patients with delirium (Fick J Geront Nurs 2000):
– Family members report change in cognition but not identified by clinical staff
“If they are known to have Alzheimer's then I usually don’t even try to ask the questions”

Excellence in Health putting People first
Failure to recognise
Risk factors for missing delirium:
• Hypoactive delirium
• Delirium superimposed on dementia
• Lack of staff knowledge
• Lack of tools
• Impaired vision
• Age >80years
Factors associated with poor outcome:
• Hypoactive delirium
• Delirium superimposed on dementia
• Prolonged duration of delirium
Failure to
recognise
Excellence in Health putting People first
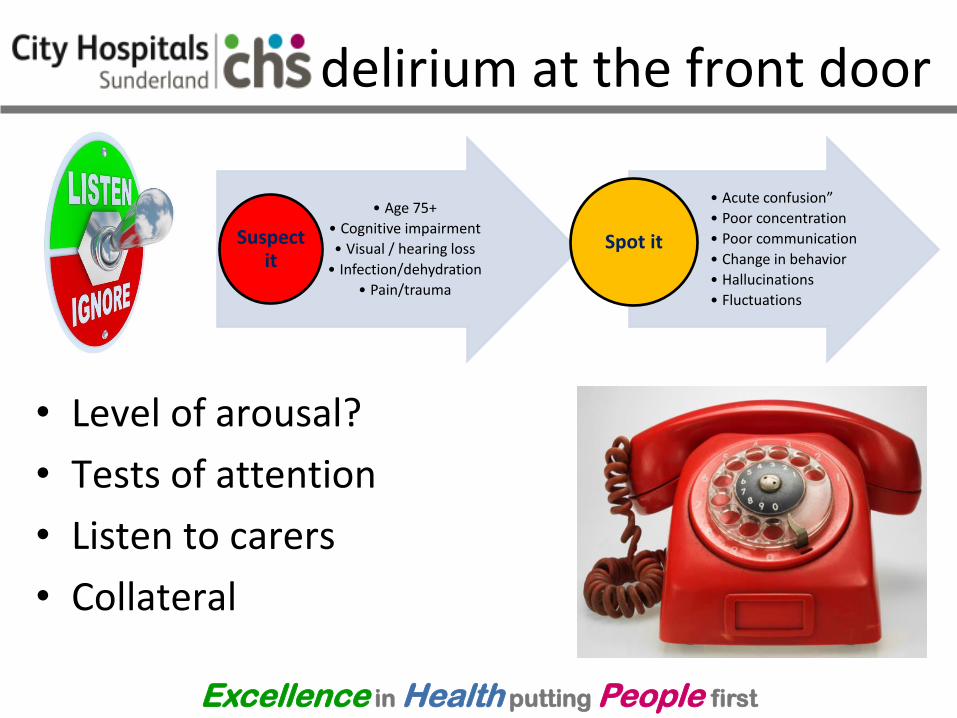
delirium at the front door
• Level of arousal?
• Tests of attention
• Listen to carers
• Collateral
• Age 75+
• Cognitive impairment
• Visual / hearing loss
• Infection/dehydration
• Pain/trauma
Suspect it
• Acute confusion”
• Poor concentration
• Poor communication
• Change in behavior
• Hallucinations
• Fluctuations
Spot it

Excellence in Health putting People first
For Delirium detection(Chester J
Hosp med 2012)
M-RASS 0
For delirium superimposed on dementia (morandi JAMDA 2016)
Sens Spec
Single 64% 93%
Serial 85% 92%
Arousal
mRASS Sens Spec
0 70.5% 84.8%
>+1 or <-1 30.6% 95.5%
mRASS
Excellence in Health putting People first
Question 3
• Which of the following are measures of attention (chose 2)?
1. Recalling an address
2. Recalling current date / time
3. Giving own date of birth / address
4. Serial 7`s
5. Months of the year backwards

Excellence in Health putting People first
Attention
• Ability to follow a conversation
• Serial 7`s or WORLD backwards in MMSE
• 20-1
• MOYB
• Months Of the Year Backwards:
• 83.3% sensitivity
• 90% specificity

Excellence in Health putting People first
4AT www.the4AT.com [1] ALERTNESS
Normal (fully alert, but not agitated, throughout assessment) 0
Mild sleepiness for <10 seconds after waking, then normal 0
Clearly abnormal 4
[2] AMT4 Age, date of birth, place (name of the hospital or building), current year.
No mistakes 0
1 mistake 1
2 or more mistakes/untestable 2
[3] ATTENTION Months of the year backwards
Achieves 7 months or more correctly 0
Starts but scores <7 months / refuses to start 1
Untestable (cannot start because unwell, drowsy, inattentive) 2
[4] ACUTE CHANGE OR FLUCTUATING COURSE Evidence of significant change or fluctuation in: alertness, cognition, other mental function (eg. paranoia, hallucinations) arising over the last 2 weeks and still evident in last 24hrs
No 0
Yes 4

Excellence in Health putting People first
Validity of delirium screening tools
Sensitivity Specificity
4AT >3 92.7% 89.7% 100%
53.7% 84.1% 82%
Hendry Age and ageing 2016 (V specialist) Bellelli Age and Ageing 2014 (v specialist) Lees Stroke 2013 (v CAM)
AMT 10 <4/10
73% 65% Lees Stroke 2013 (v CAM)
SQiD 58% 80%
85% 71%
Lees Stroke 2013 (v CAM) Sands Palliat Med 2010 (v specialist)
BCam 70.3% 40% (untrained)
91.4% Hendry Age and ageing 20162016 (V specialist) Sands Palliat Med 2010 (v specialist)

Excellence in Health putting People first
If you don’t look for it you wont find it!
Failure to recognise delirium is associated
with worse outcomes (Young, Age and Ageing 2003)
For each 48 hours of active delirium
mortality increases by 11% (Gonzales 2009)

Excellence in Health putting People first
What next?
Does she have a delirium? YES
How can we test for this at the front door? YES
simple tests of:
arousal (mRASS)
attention (MOYB)
What is the cause?
What are her risk factors?
How should we manage her?

Excellence in Health putting People first
Mary • 83 year old lady from a
care home
• Unwell for ~2/52, recent change in medication
• Drowsy, “just not right”, More muddled
• Reduced oral intake
• Hyponatraemia, AKI
• Constipation
– Bendroflumethiazide 5mg od
– Bisoprolol 5mg od
– Lisinopril 5mg od
– Simvastatin 20mg od
– Aspirin75mg od
– Codeine 30mg qds
– Trimethoprim for 5 days

Excellence in Health putting People first
Question 4
• What is the most likely cause(s) of the delirium? (chose up to 3)
1. Urinary tract infection
2. Dementia
3. Hyponatraemia
4. Constipation
5. Hyponatraemia due to drugs
6. Acute Kidney injury
7. Old age

Excellence in Health putting People first
Mary – causes of delirium
Triggers (causes)
• Hyponatraemia: – Trimethoprim
– Bendrofluamethiazide
• AKI – Bendroflumethiazide
– ACE
• Constipation – Codeine
• Drugs – Codeine
Risk factors (vulnerability)
• Age
• Cognitive impairment
• ?poor hearing / vision??
• frailty
Not all delirium is a
UTI

Excellence in Health putting People first
Causes of delirium
• Infections
• Drugs, especially opiates and anticholinergics
• Organ failure
• Biochemical disturbances
• Constipation
• Surgery
• Pain
• Infection
• Constipation
• Hydration
• Medication
• Environment & Electrolyte
Multiple causes

Excellence in Health putting People first
Drugs causing delirium
Consistent association
• Opiates OR 2.5
• Benzodiazepines OR 3
• Dihydropyradines OR 2.4
• Antihistamines OR 1.8 (Clegg Age and Ageing 2011)
Anticholinergic burden
• polypharmacy
Uncertain - individual
• H2 antagonists
• Tricyclic antidepressants
• Parkinson's med
• Steroids
• NSAID
• Anitmuscarinics

Excellence in Health putting People first
Other tests?
CT head
• Commonly abnormal
• Rarely diagnostic
• Work up for ? Underlying dementia
• Falls/ head injury
• Focal neurological symptoms
EEG
• Second line test
• Abnormal in delirium – Diffuse irregular theta
slowing
• Delirium v psychiatric illness
• ? Non-convulsive status
LP
• Consider if encephalitis suspected

Excellence in Health putting People first
What now? TIME
HIS/SDA TIME Bundle
Think exclude and treat triggers
Investigate and intervene to correct underlying
causes
Management plan
Engage and explore

Excellence in Health putting People first
“Icanpreventdelirium”
Suspect it
• Age 75+ Cognitive impairment
• Visual / hearing loss Infection/dehydration
• Pain/trauma
Spot it
• “Acute confusion” Poor concentration
• Poor communication Change in behavior
• Hallucinations Fluctuations
Stop it
• Treat cause Explain and reassure
• Environment Physical needs
• Psychological needs Social needs
(Krishnan&Fixter TEWV)

Excellence in Health putting People first
Targeted multi-component interventions in delirium
Risk factor Intervention
Cognitive impairment Reality orientation
Therapeutic activities
Vision/hearing impairment Vision/hearing aids
Adaptive equipment
Immobilisation Early mobilisation
Minimising immobilising equipment
Psychoactive medication use Non-pharmacological approaches to sleep/anxiety
Restricted use of sleeping tablets
Dehydration Early recognition
Volume repletion
Sleep deprivation Noise reduction strategies
Sleep enhancement program
Hospital elder life programme, Inouye NEJM 1999
Excellence in Health putting People first
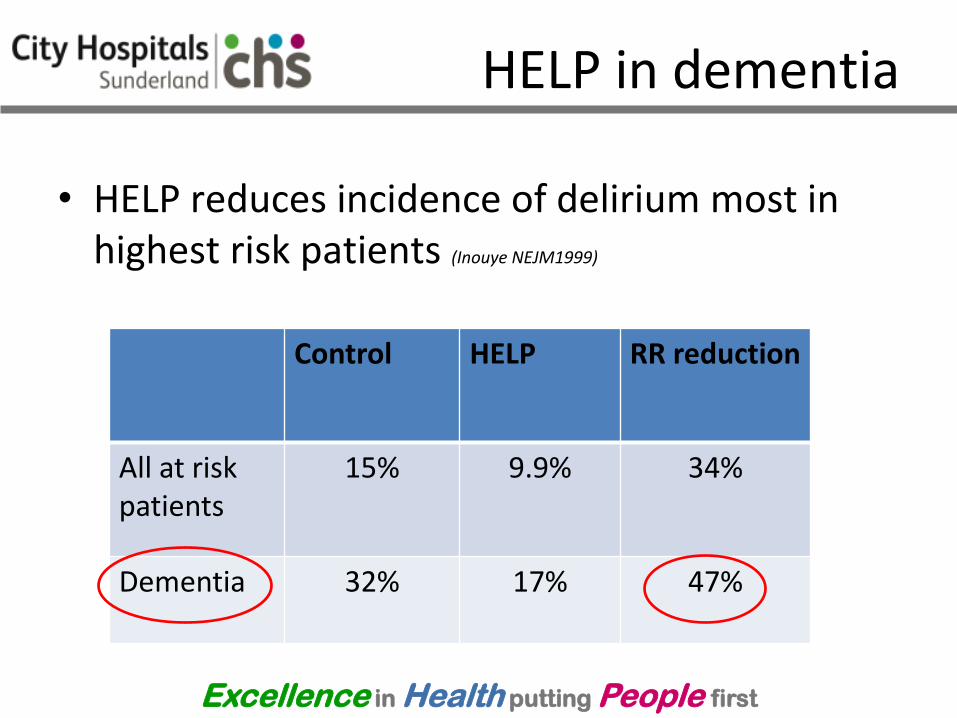
HELP in dementia
• HELP reduces incidence of delirium most in highest risk patients (Inouye NEJM1999)
Control HELP RR reduction
All at risk patients
15% 9.9% 34%
Dementia 32%
17% 47%

Excellence in Health putting People first
Delirium Toolbox study Rudolph JAMDA 2014
• Patient safety outcomes in patients at risk of delirium
• Intervention:
– Delirium tool box
• Identify risk (3 risk factors)
• Modify risk (using tool box)
• Monitor for delirium

Excellence in Health putting People first
Delirium tool box
Tool box
Sensory impairment
Pocket amplifier
Reading glasses
Magnifying glass
Stress ball
Cognition
Puzzles
Cards
dominos
Sleep promotion
Ear plugs
Eye mask
Head phones

Excellence in Health putting People first
Outcomes (Rudolph 2015)

Excellence in Health putting People first
Prevention is better than cure
• Up to 40% incident delirium is preventable:
• targeted multi-component intervention (Inouye NEJM 1999)
• Delirium toolbox study (Rudolph JAMDA
2014)
• But little evidence for improved 6/12 outcomes in prevalent delirium with non-pharmacological interventions
(Laurila, Helsinki study J Geront 2006)
Vu
lnera
bil
ity
insult
Age
Dem
entia
low risk, severe insult
High risk, small insult

Excellence in Health putting People first
Managing delirious patients
• Medical /nursing
– Document / explain diagnosis
– Assess/treat pain
– Ensure O2 sats maintained
– Avoid/treat constipation
– Avoid catheterisation
– Person centred care tool
– Consider if swallow is safe
• Environment & general
measures
– Sensory aids
– Sleep chart
– Encourage to mobilise
– Encourage diet and fluids (maintain charts)
– Reduced stress to patient
– Minimise ward moves (right ward first time)
– Avoid unnecessary interventions

Excellence in Health putting People first
• Drugs NICE Guidelines CG103 (2010).
– Limited evidence base
– Low dose antipsychotics safe
• Haloperidol 0.5mg
• Olanzapine
– Benzodiazepines not recommended (Cochrane
review 2009)
• Unless PD / LBD
• Treatment of symptoms
– Encourage family visits • Johns campaign
– Consider additional staff
– Assess for psychotic symptoms
• Treat if distressing
– Inform/explain to next of kin
– Assess capacity

Excellence in Health putting People first
What about outcomes?
• Delirium is an independent risk factor for poor outcomes:
– Mortality
• at discharge
• 12 months OR 1.95 (witlox JAMA 2010)
– Length of stay
– Institutionalisation OR 2.41-3.19 (witlox JAMA 2010, Siddiqi Age and ageing 2006)
– ADL decline
– Cognitive decline

Excellence in Health putting People first
Mary
• 83 year old lady from a care home
• Delirium due to AKI / Hyponatraemia / drugs
• “pleasantly confused”
– Consider formal diagnosis ? Dementia
• Follow up to ensure full resolution of delirium
• “at risk” of future delirium
– Delirium prevention advice to care home
Excellence in Health putting People first
Take home messages
• Delirium is common
• Delirium is a serious problem with poor outcomes
• Delirium can be prevented
– Prevention is better than cure
• If you don’t look for it, you wont find it
– Use a tool: arousal + attention
• Failure to recognise is associated with worse outcomes
