ipf treatment update › media › ... · 2% 9% 10. insipre cohort (n=438) chicago cohort (n=148)...
TRANSCRIPT

IPF treatment update
Ulrich Costabel
Professor of Medicine
University of Duisburg-Essen
Ruhrlandklinik
University Hospital
Essen, GermanyRuhrlandklinik
Disclosure StatementDr. Costabel has served on a Scientific
Advisory Board for the following companies:
• Actelion
• Bayer
• Boehringer Ingelheim
• Centocor
• Gilead
• GSK
• InterMune
• Roche
• Wyeth

Overview of Idiopathic Pulmonary Fibrosis (IPF)
• IPF: a progressive and fatal lung disease
– HRCT and pathology: ‘Usual Interstitial Pneumonia’ (UIP) – Age of onset 50-80 years– Incidence: 10.7/100,000 Males; 7.4/100,000 Females– 70 % smokers/exsmokers
• Natural History of IPF
– Rate of decline in lung function appears to predict mortality– Median survival only 3 years after diagnosis
• Limited therapeutic options, but hope for the future
– Corticosteroids and cytotoxic therapies: side effects– Antifibrotic drugs: 2 drugs have shown efficacy
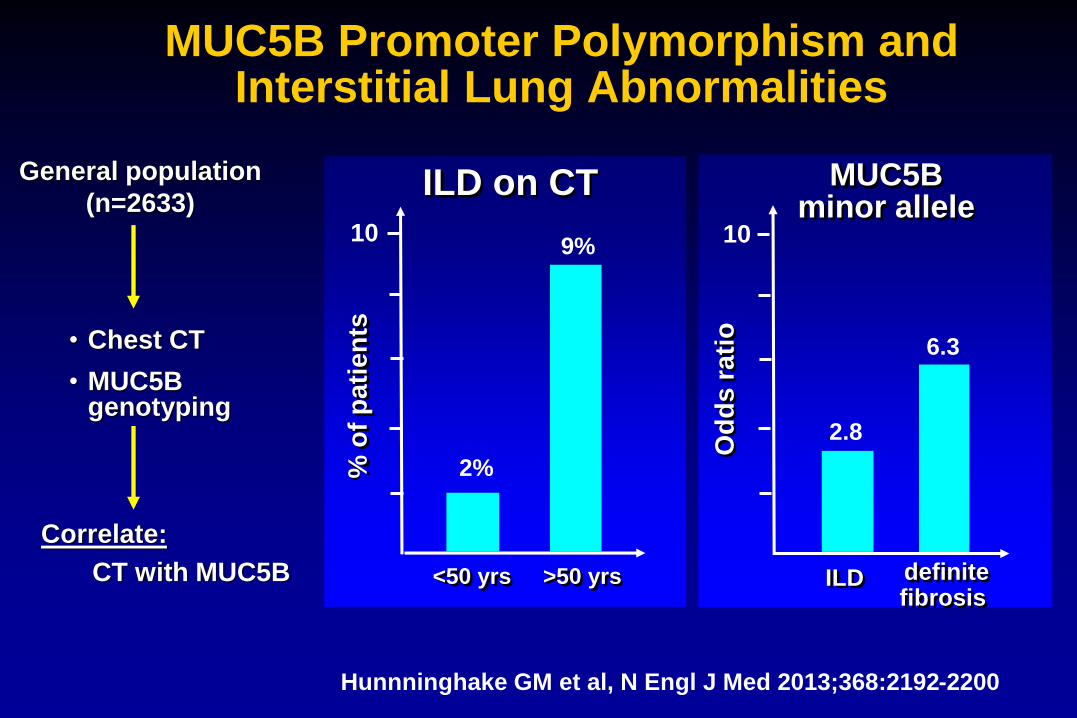
MUC5B Promoter Polymorphism and Interstitial Lung Abnormalities
Hunnninghake GM et al, N Engl J Med 2013;368:2192-2200
General population
(n=2633)
• Chest CT
• MUC5B genotyping
Correlate:
CT with MUC5B
Od
ds
ra
tio
MUC5Bminor allele
ILD
2.8
6.3
definite fibrosis
% o
f p
ati
en
ts
ILD on CT
<50 yrs >50 yrs
2%
9%10 10
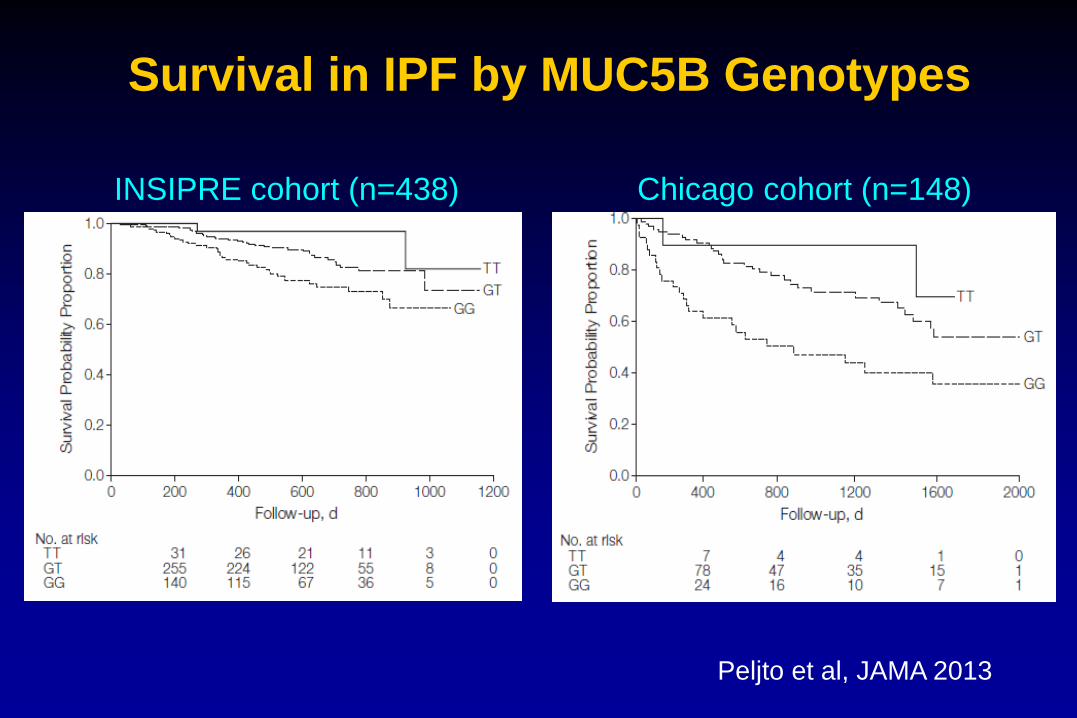
INSIPRE cohort (n=438) Chicago cohort (n=148)
Peljto et al, JAMA 2013
Survival in IPF by MUC5B Genotypes
IPF: Goals of Treatment
• Stop disease progression
• Prolong survival
• Prevent acute exacerbations
• Reduce symptoms
Treatment of IPF:
a dynamic field since 2011
• 2011:
– Pirfenidone in
– Triple therapy out
– Anticoagulants out
• 2014 :
– Nintedanib, a tyrosine kinase inhibitor of the FGF, PDGF and VEGF
receptors, has shown consistent positive effects in 2 phase III trials
(INPULSIS trials)
– Pirfenidone: evidence on efficacy and safety observed in previous
studies reinforced (ASCEND trial)
– NAC monotherapy out (PANTHER trial)
Raghu et al., ATS, 19.5.2015
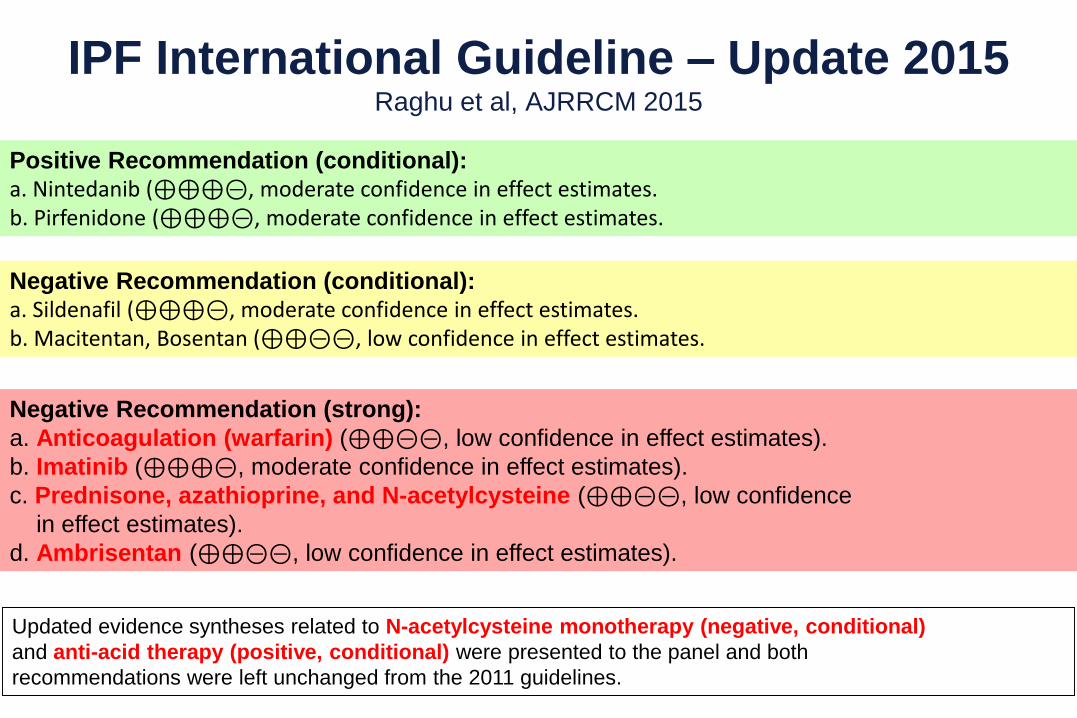
Negative Recommendation (strong):
a. Anticoagulation (warfarin) (⊕⊕⊝⊝, low confidence in effect estimates).
b. Imatinib (⊕⊕⊕⊝, moderate confidence in effect estimates).
c. Prednisone, azathioprine, and N-acetylcysteine (⊕⊕⊝⊝, low confidence
in effect estimates).
d. Ambrisentan (⊕⊕⊝⊝, low confidence in effect estimates).
Negative Recommendation (conditional):
a. Sildenafil (⊕⊕⊕⊝, moderate confidence in effect estimates.b. Macitentan, Bosentan (⊕⊕⊝⊝, low confidence in effect estimates.
Positive Recommendation (conditional):
a. Nintedanib (⊕⊕⊕⊝, moderate confidence in effect estimates.b. Pirfenidone (⊕⊕⊕⊝, moderate confidence in effect estimates.
Updated evidence syntheses related to N-acetylcysteine monotherapy (negative, conditional)
and anti-acid therapy (positive, conditional) were presented to the panel and both
recommendations were left unchanged from the 2011 guidelines.
IPF International Guideline – Update 2015Raghu et al, AJRRCM 2015
Natural History of IPF and
Prognostic Factors
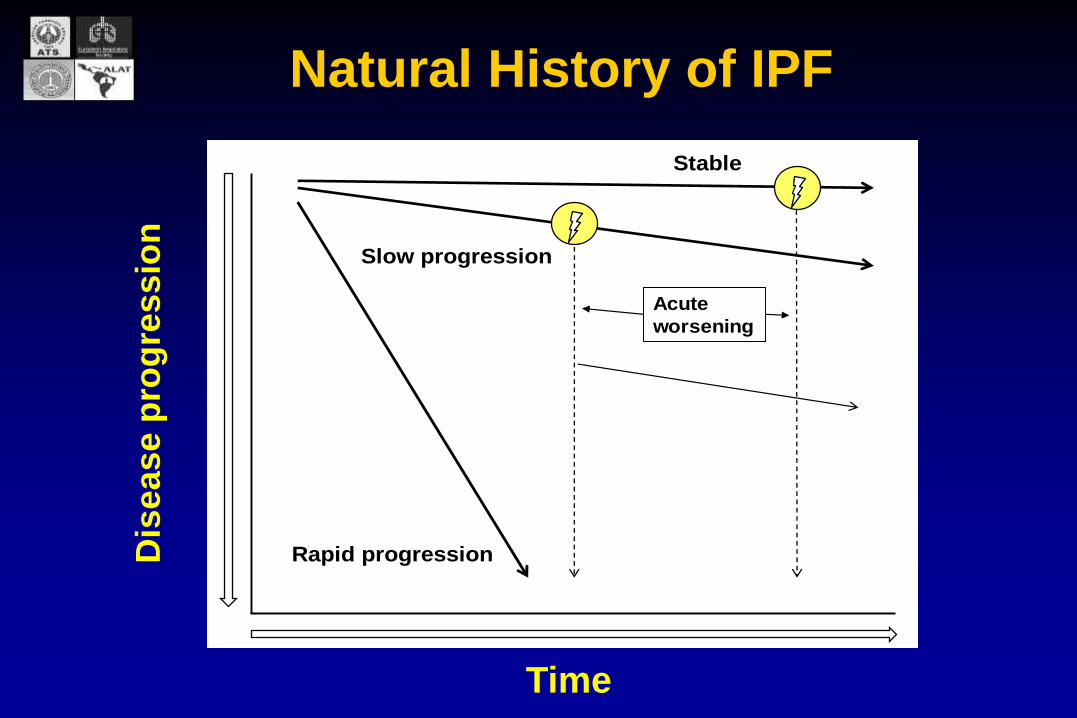
Natural History of IPF
Acute
worsening
Rapid progression
Slow progression
Dis
ea
se
pro
gre
ssio
n
Time
StableD
ise
as
e p
rog
res
sio
n
Time
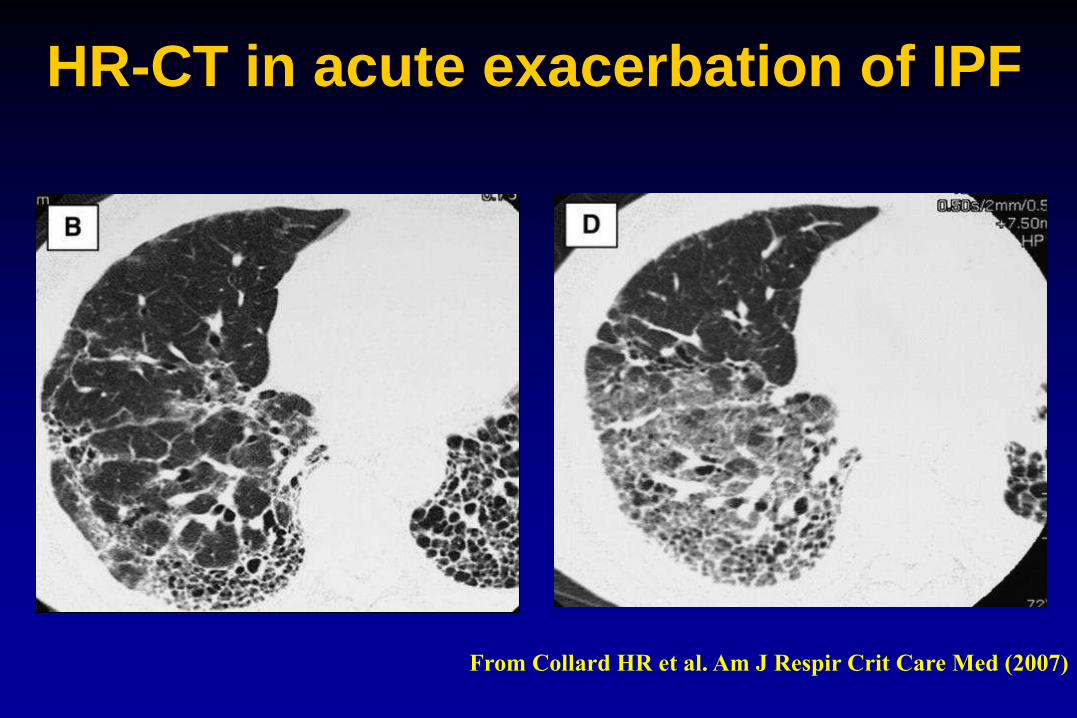
From Collard HR et al. Am J Respir Crit Care Med (2007)
HR-CT in acute exacerbation of IPF

IPF: Acute Exacerbation
• Incidence: 5 % per year
• Mortality: 70-90 %
Kim 2006, Okamoto 2006, Kondoh 2006
FVC as
Prognostic Factor
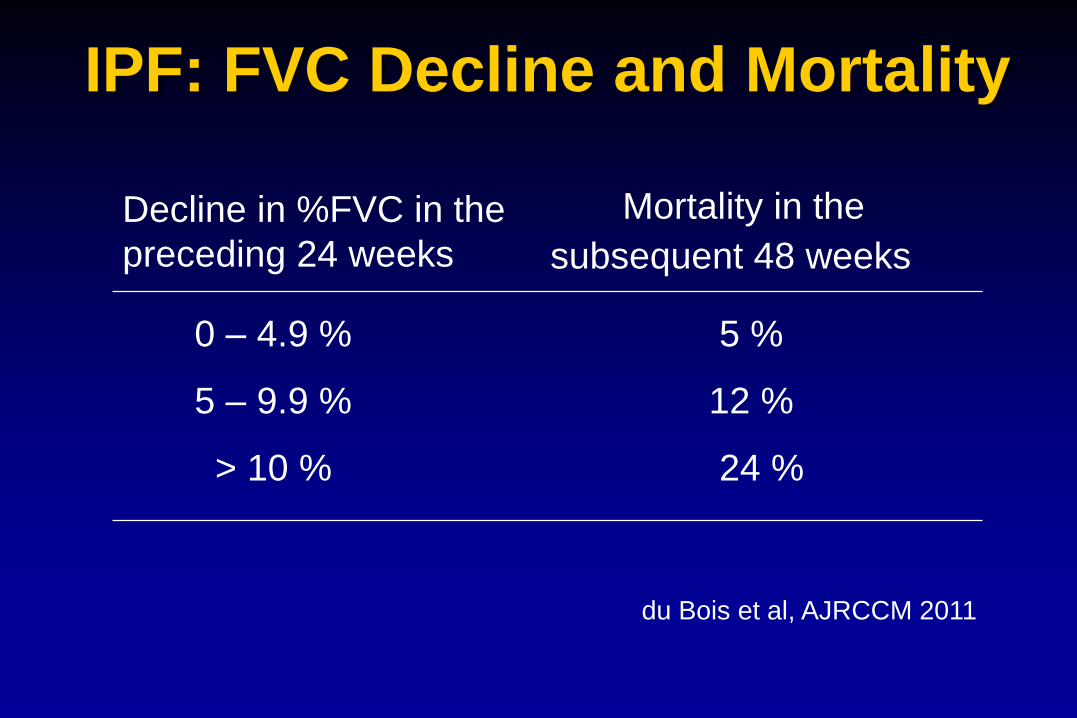
IPF: FVC Decline and Mortality
Decline in %FVC in the
preceding 24 weeks
Mortality in the
subsequent 48 weeks
0 – 4.9 %
5 – 9.9 %
> 10 %
5 %
12 %
24 %
du Bois et al, AJRCCM 2011

The New Era
of IPF Treatment:
Two Approved Drugs
• Pirfenidone is an orally-available small molecule
• Pirfenidone is active in cell cultures and several animal models of fibrosis– Including lung, liver, heart, and kidney– Active at clinically relevant exposures– ~40 peer reviewed preclinical publications
• Inhibits TGF- and TNF-a
Pirfenidone: key points

Pirfenidone:The first approved IPF drug
Pirfenidone (Pirespa ) approved for IPF patients in Japan (October 2008)
Pirfenidone (Esbriet ) approved for IPF patients in Europe (February 2011)
Pirfenidone (Esbriet ) approved for IPF patients in USA (October 2014)
Therapeutic indications: for mild- to moderate IPF in adults (in Europe)
Should be initiated and supervised by a physician specialized in treatment of IPF

18
Mean Change in % Predicted FVC Progression-free Survival Time
Mean Change in 6MWT Distance
Week
0
-10
-20
-30
-40
-50
-60
-70
-80
-900 12 24 36 48 60 72
Week
Mean
Ch
an
ge i
n 6
MW
D (
m)
Perc
en
t o
f P
ati
en
tsPFD 2403 (n=345)
Placebo (n=347)
100
80
60
40
20
00 12 24 36 48 60 72 84 96 108 120
Week
PFD 2403 (n=345)
Placebo (n=347)
Categorical Decline in FVC and 6MWD
60
40
20
0% FVC ≥ 10% 6MWD ≥ 50 m
CAPACITY Pirfenidone trials: Pooled Efficacy Results
Perc
en
t o
f P
ati
en
ts
PFD 2403 mg/d (n=345)
Placebo (n=347)
PFD 2403 (n=345)
Placebo (n=347)
P=0.005
P=0.001
P=0.003
P=0.001
P=0.025
HR 0.74
720
0
-5
-10
-15 12 24 36 48 60
Mean
Ch
an
ge f
rom
Baselin
e (
%)
Noble et al, Lancet 2011
ASCEND Trial
NEJM 2014;370:2083
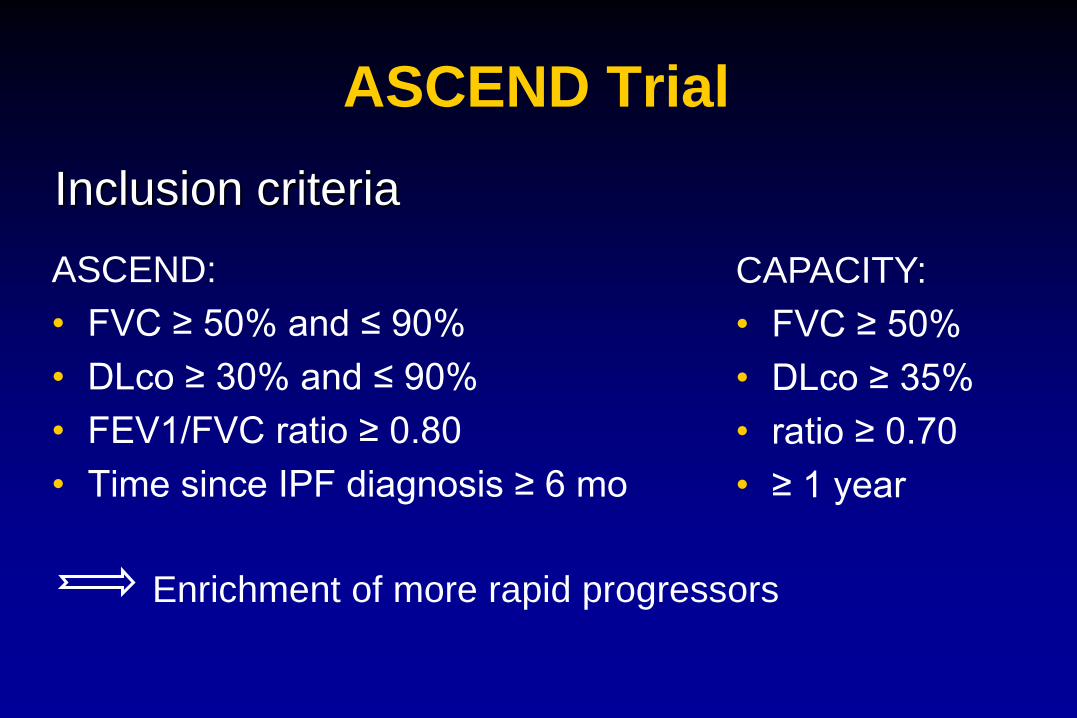
ASCEND Trial
ASCEND:
• FVC ≥ 50% and ≤ 90%
• DLco ≥ 30% and ≤ 90%
• FEV1/FVC ratio ≥ 0.80
• Time since IPF diagnosis ≥ 6 mo
Enrichment of more rapid progressors
CAPACITY:
• FVC ≥ 50%
• DLco ≥ 35%
• ratio ≥ 0.70
• ≥ 1 year
Inclusion criteria

Primary Efficacy Analysis: Treatment with pirfenidone resulted in
a significant between-group difference in the rank ANCOVA
analysis (P<0.000001)
Proportion of Patients
with ≥10% Decline in
FVC or Death (%)
Absolute Difference 2.5% 7.9% 12.3% 15.3%
Relative Difference 54.0% 58.0% 57.8% 47.9%
Rank ANCOVA p-value <0.000001 <0.000001 0.000002 <0.000001
King et al. N Engl J Med 2014;370:2083–92

Absolute Difference, 116 mL/yr
Relative reduction: 41.5%
P<0.0001*
* Linear slope analysis: Mixed model with linear time effect adjusted for age, height, and sex
Annual Rate of FVC
Change (mL/yr)
Supportive Analysis of the primary endpoint:
Annual rate of FVC decline at week 52 favored Pirfenidone
(Linear Slope Analysis)
-164 mL/yr
Figures corrected
as per NEJM
erratum Aug 2014
King et al. N Engl J Med 2014;370:2083–92
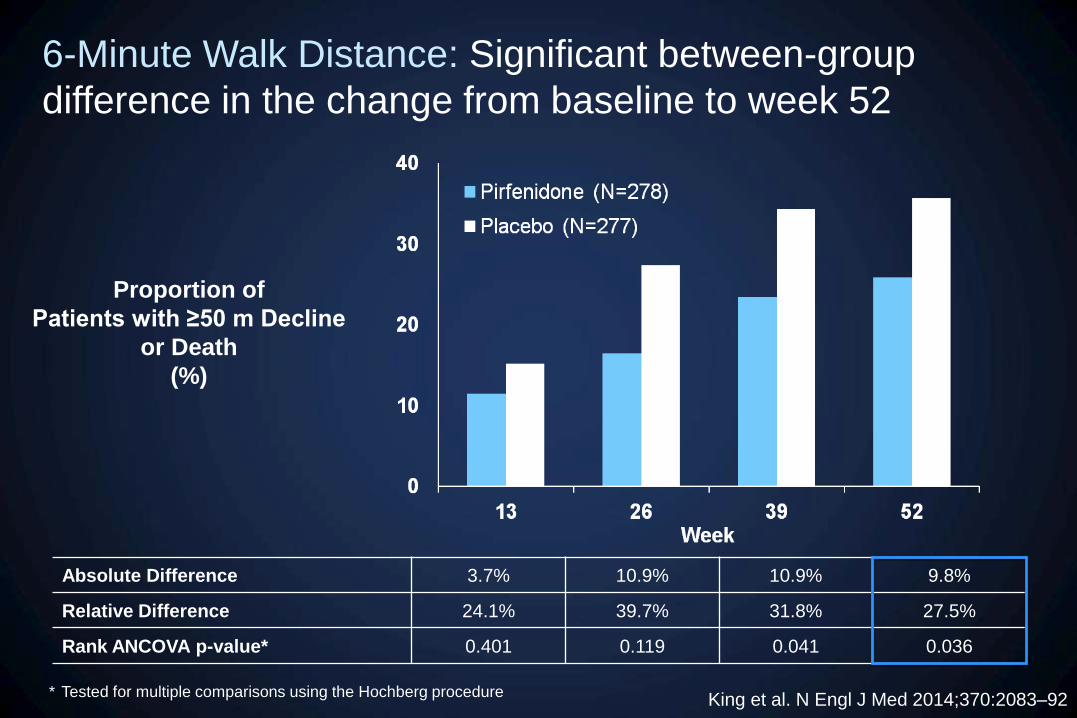
6-Minute Walk Distance: Significant between-group
difference in the change from baseline to week 52
Absolute Difference 3.7% 10.9% 10.9% 9.8%
Relative Difference 24.1% 39.7% 31.8% 27.5%
Rank ANCOVA p-value* 0.401 0.119 0.041 0.036
* Tested for multiple comparisons using the Hochberg procedure
Proportion of
Patients with ≥50 m Decline
or Death
(%)
King et al. N Engl J Med 2014;370:2083–92
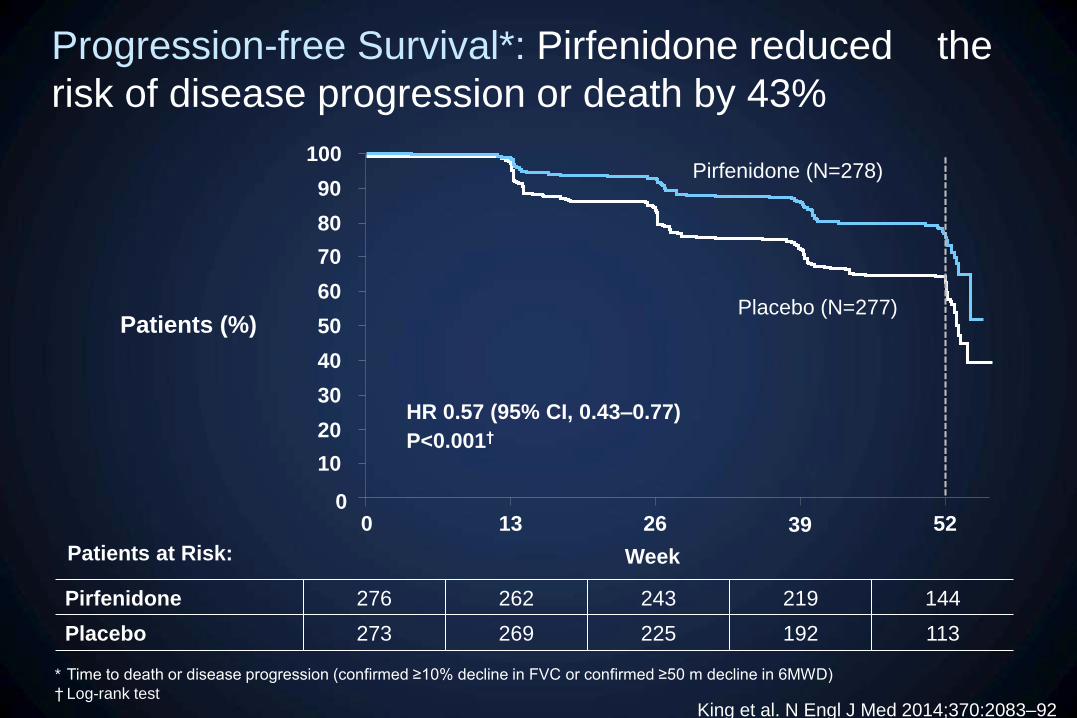
Progression-free Survival*: Pirfenidone reduced the
risk of disease progression or death by 43%
* Time to death or disease progression (confirmed ≥10% decline in FVC or confirmed ≥50 m decline in 6MWD)
† Log-rank test
Pirfenidone 276 262 243 219 144
Placebo 273 269 225 192 113
Patients at Risk:
0 13 26 39 52
Week
0
10
20
30
40
50
60
70
80
90
100
Placebo (N=277)
Pirfenidone (N=278)
P<0.001†
HR 0.57 (95% CI, 0.43–0.77)
Patients (%)
King et al. N Engl J Med 2014;370:2083–92

Pooled All-cause Mortality (Week 52): Treatment group
curves diverge early and continue separating throughout the
study period
Month
Cumulative Risk of
Death
(%)
Placebo (N=624)
Pirfenidone (N=623)
Patients at Risk, n
Pirfenidone
Placebo
623
624
HR 0.52 (95% CI 0.31–0.87)*
P=0.011†
* Cox proportional hazards model
† Log-rank test
618 609 596 509
619 603 586 490
King et al. N Engl J Med 2014;370:2083–92

Adverse events occuring in >10% of patients
in CAPACITY
Pirfenidone (n=345)
%
Placebo (n=347)
%
Nausea 36 17
Rash 32 12
Dyspepsia 19 7
Dizziness 18 10
Vomiting 14 4
Photosensitivity 12 2
Anorexia 11 4
Noble et al, Lancet 2011
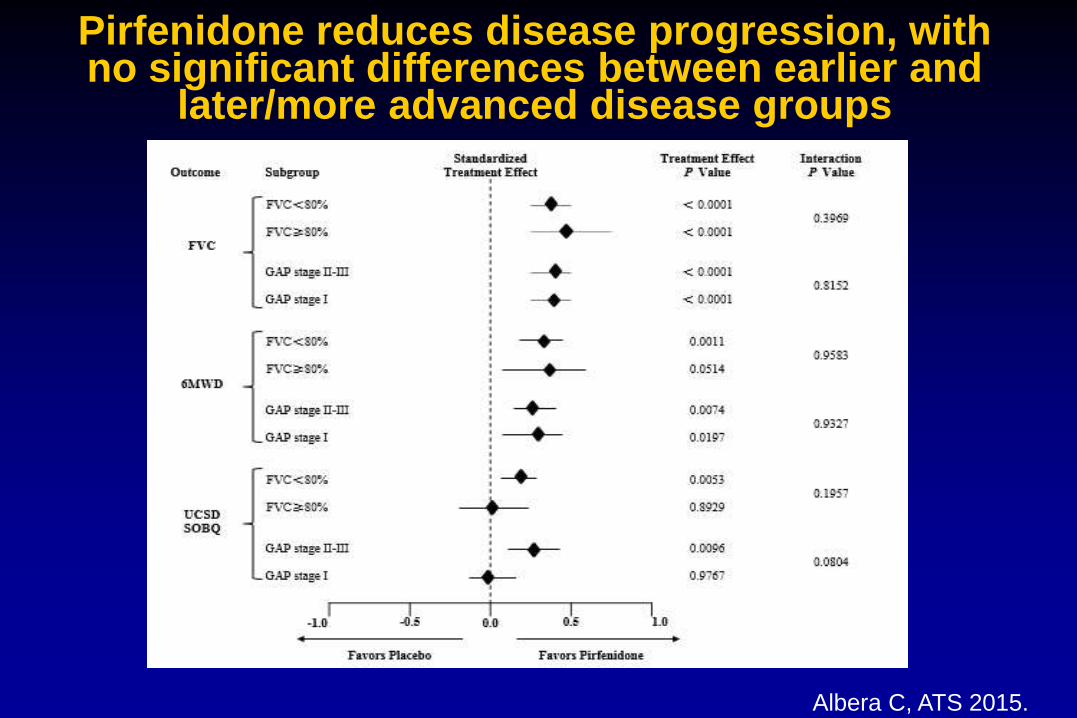
Albera C, ATS 2015.
Pirfenidone reduces disease progression, with no significant differences between earlier and
later/more advanced disease groups

Pirfenidone: Summary
• Pirfenidone was the first approved drug for treatment of IPF
• Pirfenidone was tested in 5 randomized placebo-controlled trials including more than 1.600 IPF patients
• Pirfenidone reduced disease progression and 1-year-
mortality.
• The adverse events support a favourable risk-benefit ratio
- increased GI und photosensitivity/skin reactions
- only few leading to withdrawal

New Approved Therapy for IPF
Nintedanib:
Tyrosine kinase inhibitor
(PDGF, FGF, VEGF)

Nintedanib: a potent intracellular tyrosine kinase inhibitor
• Nintedanib targets the VEGF, FGF and PDGF receptors
• Nintedanib acts by blocking the intracellular ATP binding site of the receptors and with it activation and signalling
Hilberg et al. Cancer Res 2008;68:4774–82; Wollin et al. J Pharmacol Exp Ther 2014;349:209–20.
Richeldi et al, N Engl J Med 2011;365:1079–87.
TOMORROW
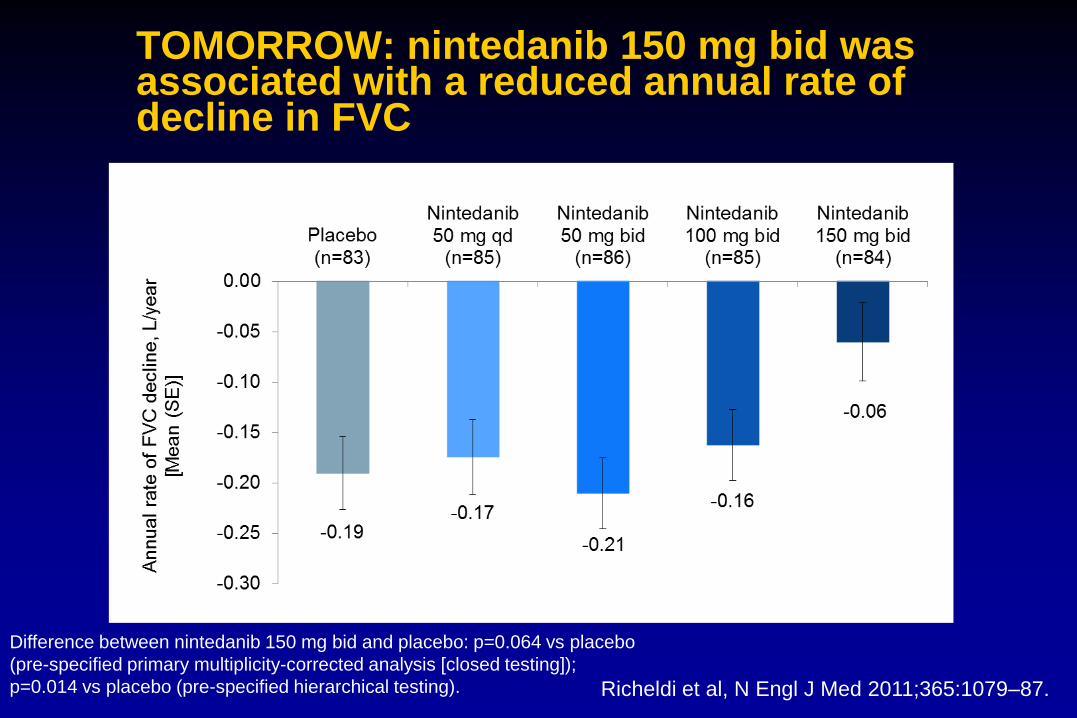
TOMORROW: nintedanib 150 mg bid was associated with a reduced annual rate of decline in FVC
Richeldi et al, N Engl J Med 2011;365:1079–87.
Difference between nintedanib 150 mg bid and placebo: p=0.064 vs placebo
(pre-specified primary multiplicity-corrected analysis [closed testing]);
p=0.014 vs placebo (pre-specified hierarchical testing).
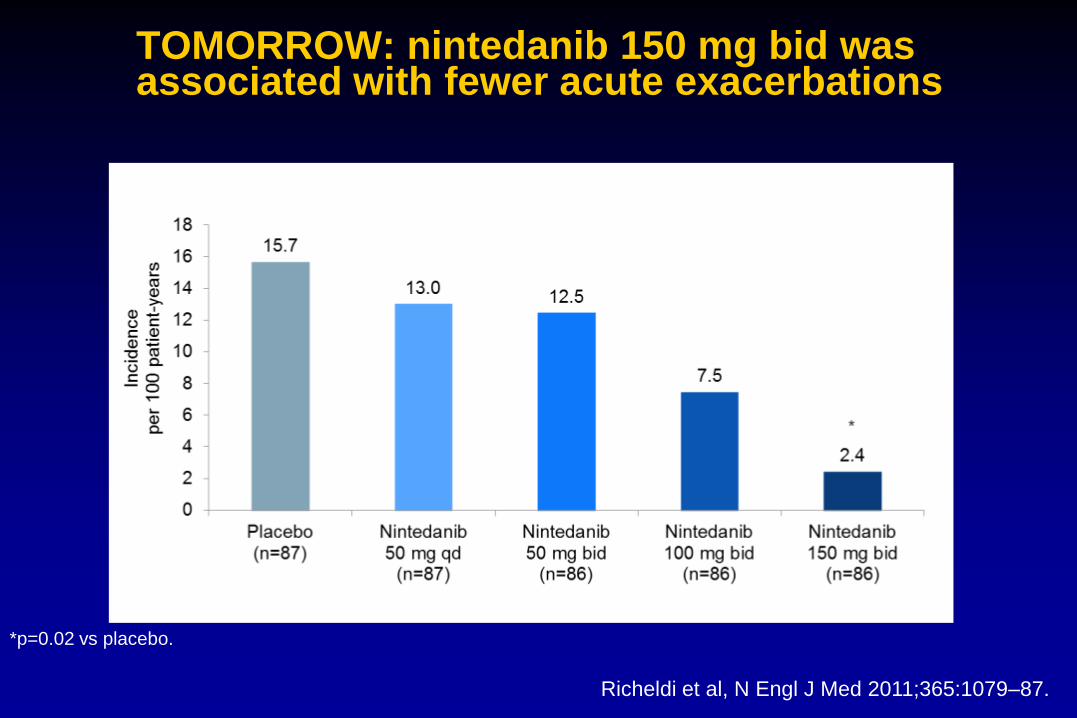
TOMORROW: nintedanib 150 mg bid was associated with fewer acute exacerbations
Richeldi et al, N Engl J Med 2011;365:1079–87.
*p=0.02 vs placebo.

Richeldi et al. N Engl J Med 2014;370:2071–82.
INPULSIS®-1 and INPULSIS®-2
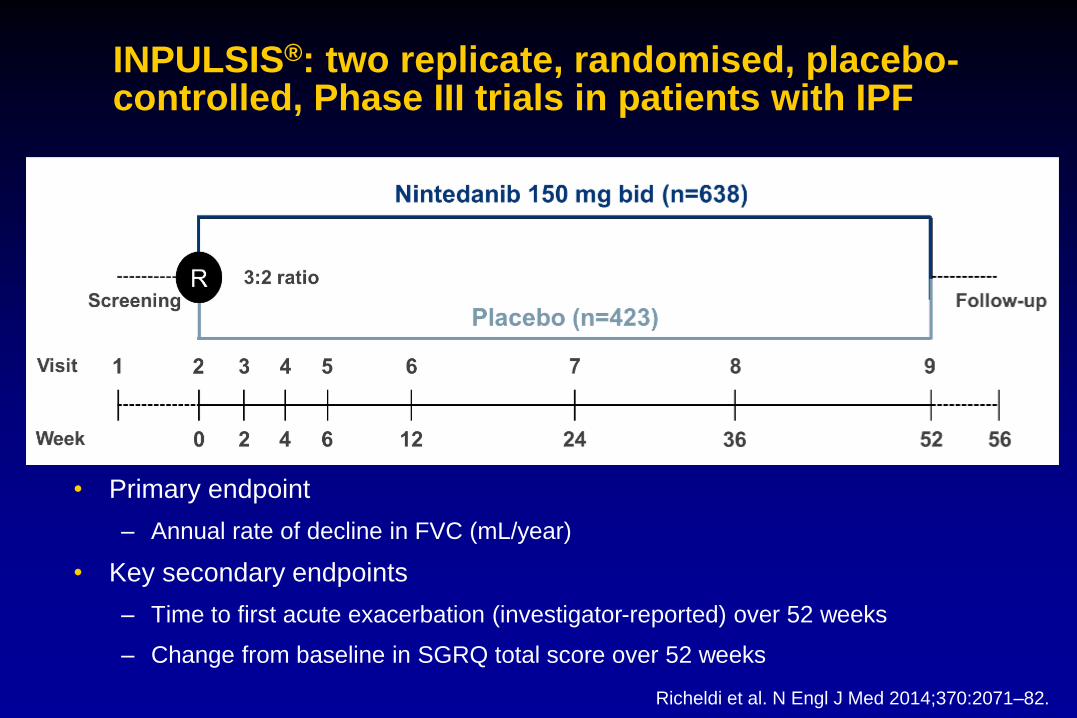
INPULSIS®: two replicate, randomised, placebo-controlled, Phase III trials in patients with IPF
• Primary endpoint
– Annual rate of decline in FVC (mL/year)
• Key secondary endpoints
– Time to first acute exacerbation (investigator-reported) over 52 weeks
– Change from baseline in SGRQ total score over 52 weeks
Richeldi et al. N Engl J Med 2014;370:2071–82.

Key inclusion criteria
• Age ≥40 years
• Diagnosis of IPF within 5 years of randomisation
• Chest HRCT performed within 12 months of screening
• HRCT pattern and, if available, surgical lung biopsy pattern, consistent with diagnosis of IPF as assessed by central review
• FVC ≥50% of predicted value
• DLCO 30–79% predicted
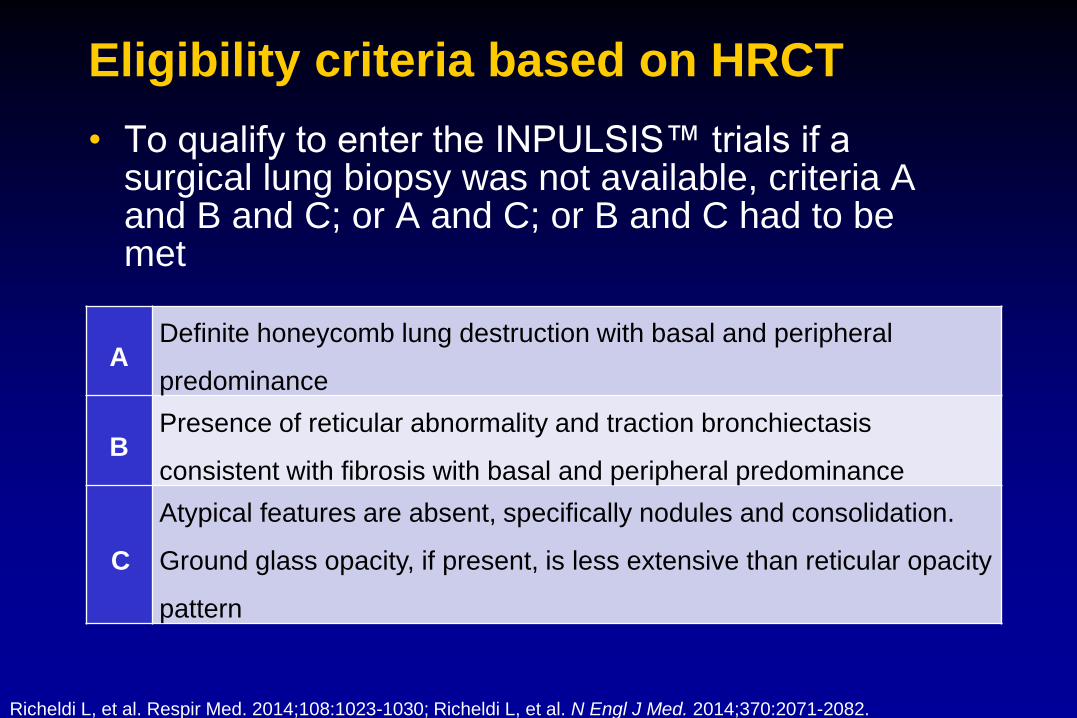
Eligibility criteria based on HRCT
• To qualify to enter the INPULSIS™ trials if a surgical lung biopsy was not available, criteria A and B and C; or A and C; or B and C had to be met
ADefinite honeycomb lung destruction with basal and peripheral
predominance
BPresence of reticular abnormality and traction bronchiectasis
consistent with fibrosis with basal and peripheral predominance
C
Atypical features are absent, specifically nodules and consolidation.
Ground glass opacity, if present, is less extensive than reticular opacity
pattern
Richeldi L, et al. Respir Med. 2014;108:1023-1030; Richeldi L, et al. N Engl J Med. 2014;370:2071-2082.
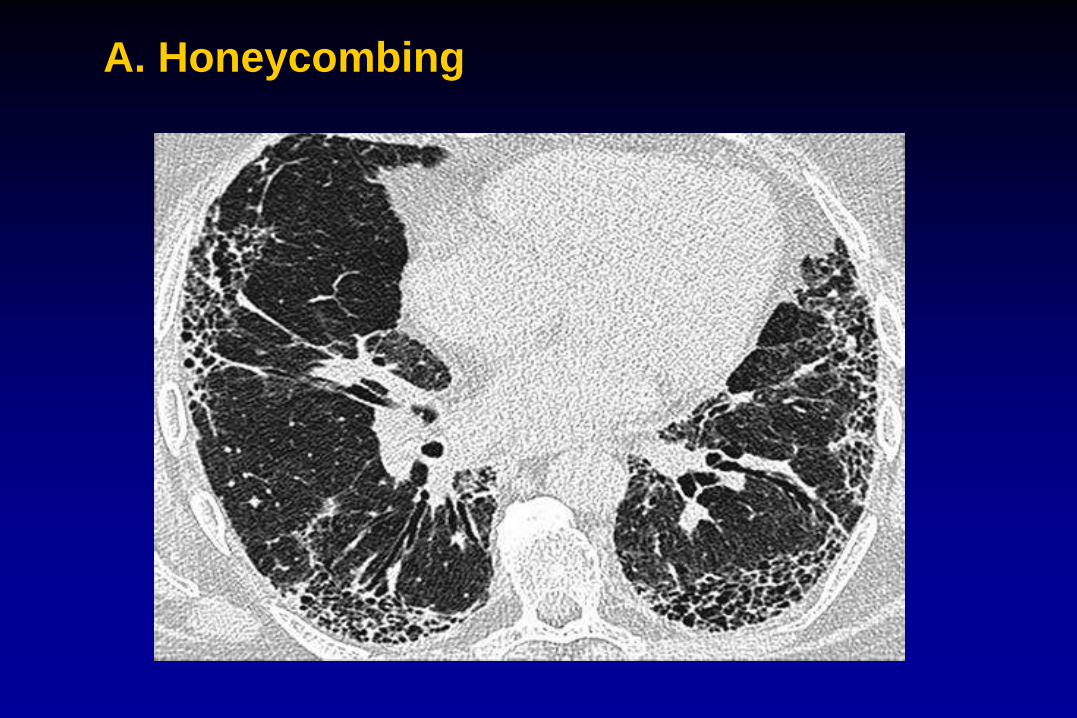
A. Honeycombing

B. No honeycombing –but reticulation and traction bronchiectasis

Annual Rate of Decline and Change from Baseline
in FVC in INPULSIS-1
Richeldi et al, NEJM 2014
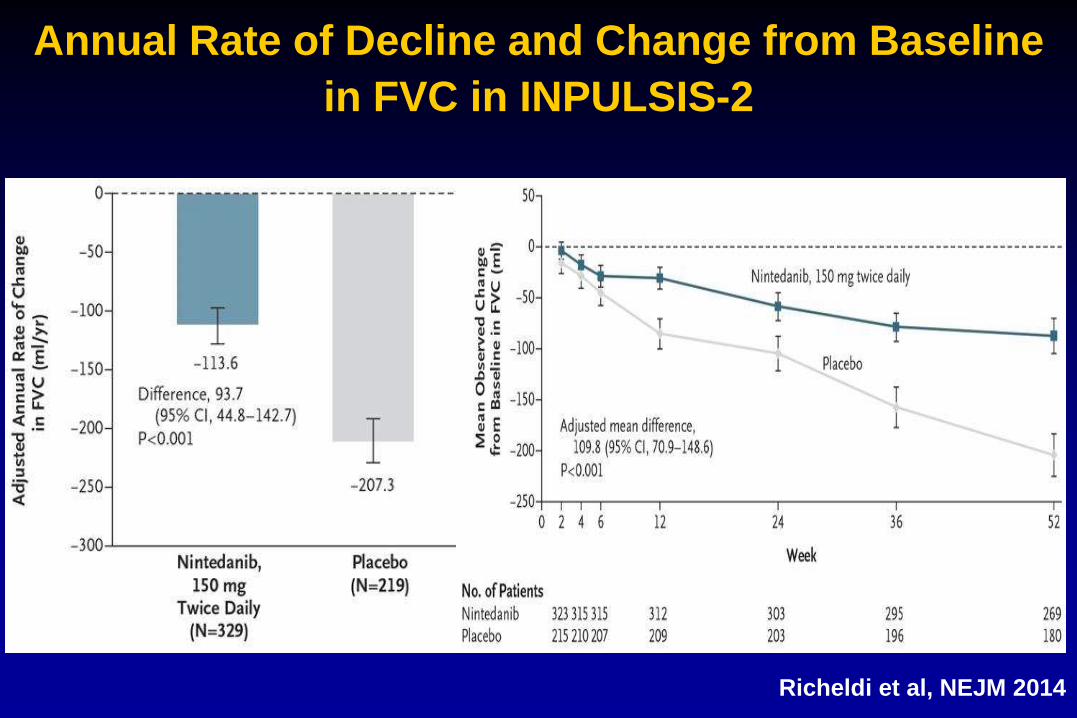
Annual Rate of Decline and Change from Baseline
in FVC in INPULSIS-2
Richeldi et al, NEJM 2014
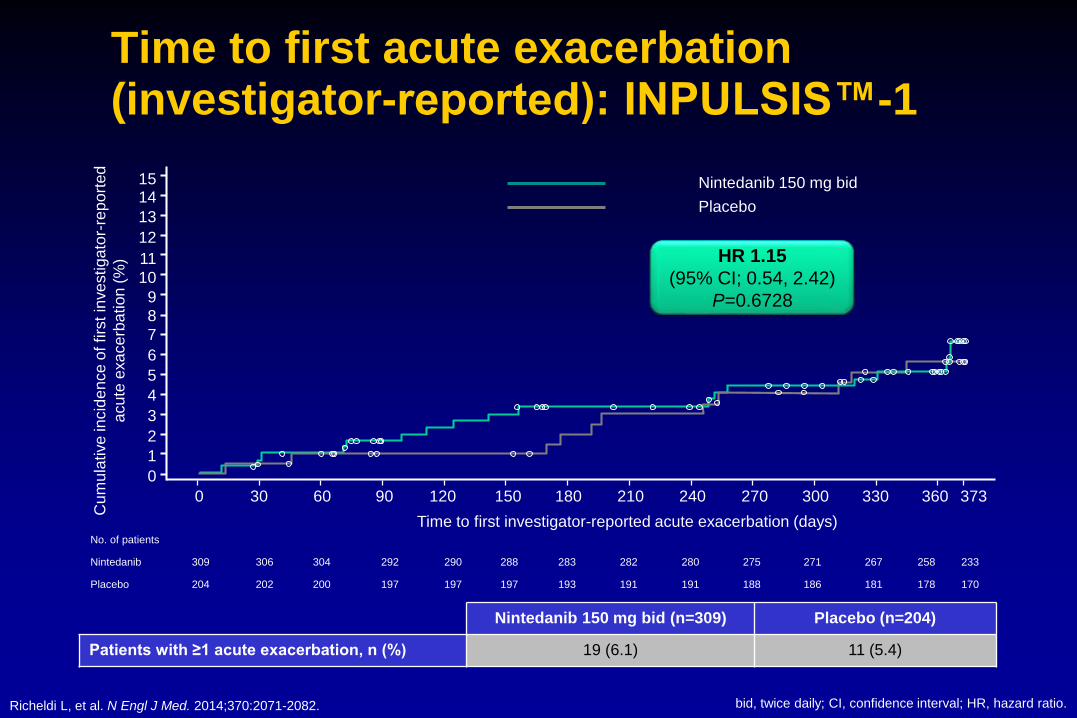
Time to first acute exacerbation (investigator-reported): INPULSIS™-1
bid, twice daily; CI, confidence interval; HR, hazard ratio.
Nintedanib 150 mg bid (n=309) Placebo (n=204)
Patients with ≥1 acute exacerbation, n (%) 19 (6.1) 11 (5.4)
HR 1.15
(95% CI; 0.54, 2.42)
P=0.6728
0 30 60 90 120 150 180 210 240 270 300 330 360 373
Time to first investigator-reported acute exacerbation (days)
0
1
2
3
4
5
6
7
8
9
10
11
12
13
1415
Cum
ula
tive
incid
en
ce o
f firs
t in
ve
stiga
tor-
rep
ort
ed
acu
te e
xa
ce
rba
tion
(%
)
No. of patients
Nintedanib 309 306 304 292 290 288 283 282 280 275 271 267 258 233
Placebo 204 202 200 197 197 197 193 191 191 188 186 181 178 170
Placebo
Nintedanib 150 mg bid
Richeldi L, et al. N Engl J Med. 2014;370:2071-2082.
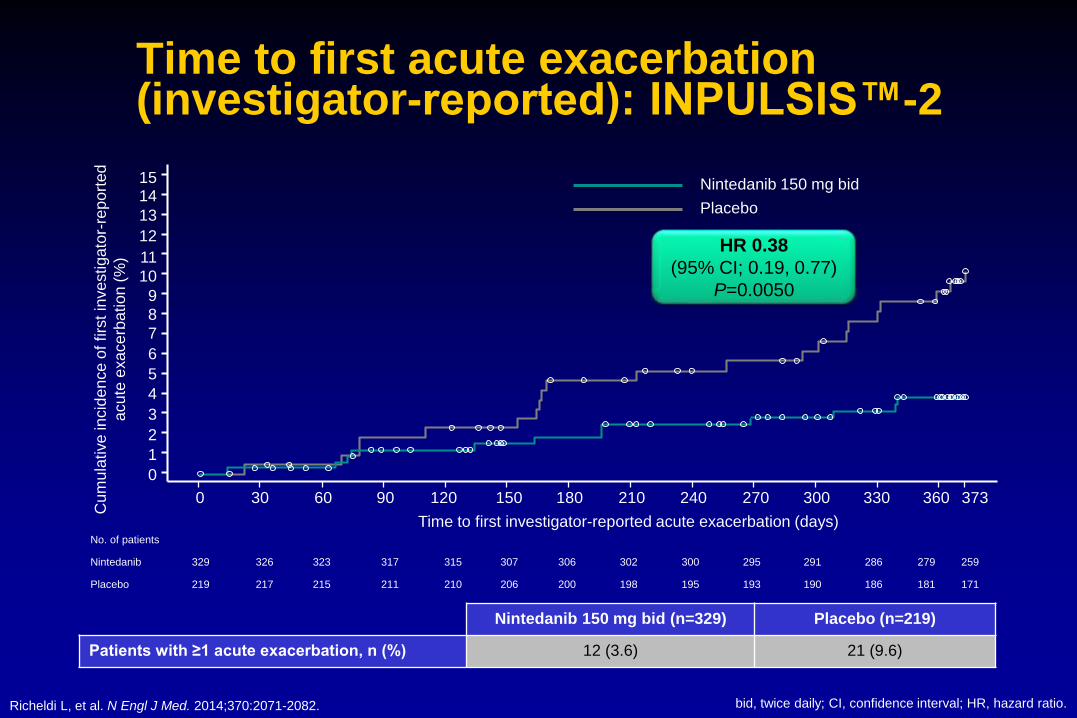
No. of patients
Nintedanib 329 326 323 317 315 307 306 302 300 295 291 286 279 259
Placebo 219 217 215 211 210 206 200 198 195 193 190 186 181 171
Time to first acute exacerbation (investigator-reported): INPULSIS™-2
Nintedanib 150 mg bid (n=329) Placebo (n=219)
Patients with ≥1 acute exacerbation, n (%) 12 (3.6) 21 (9.6)
HR 0.38
(95% CI; 0.19, 0.77)
P=0.0050
Placebo
Nintedanib 150 mg bid
0
1
2
3
4
5
6
7
8
9
10
11
12
13
1415
Cum
ula
tive
incid
en
ce o
f firs
t in
ve
stiga
tor-
rep
ort
ed
acu
te e
xa
ce
rba
tion
(%
)
0 30 60 90 120 150 180 210 240 270 300 330 360 373
Time to first investigator-reported acute exacerbation (days)
bid, twice daily; CI, confidence interval; HR, hazard ratio.Richeldi L, et al. N Engl J Med. 2014;370:2071-2082.

Time to first acute exacerbation (investigator-reported): pooled data
Nintedanib 150 mg bid (n=638) Placebo (n=423)
Patients with ≥1 acute exacerbation, n (%) 31 (4.9) 32 (7.6)
HR 0.64
(95% CI; 0.39, 1.05)
P=0.0823
Placebo
Nintedanib 150 mg bid
0
1
2
3
4
5
6
7
8
9
10
11
12
13
1415
Cum
ula
tive
incid
en
ce o
f firs
t in
ve
stiga
tor-
rep
ort
ed
acu
te e
xa
ce
rba
tion
(%
)
0 30 60 90 120 150 180 210 240 270 300 330 360 373
Time to first investigator-reported acute exacerbation (days)No. of patients
Nintedanib 638 632 627 609 605 595 589 584 580 570 562 553 537 492
Placebo 423 419 415 408 407 403 393 389 386 381 376 367 359 341
bid, twice daily; CI, confidence interval; HR, hazard ratio.Richeldi L, et al. N Engl J Med. 2014;370:2071-2082.

Time to first confirmed or suspected acute
exacerbation per adjudication (pooled data)
Patients with ≥ 1AE:
-N= 12 (1.9%) in Nindetanib arm (N=638)
-N= 24 (5.7%) in placebo arm (N=423)
Richeldi et al, NEJM 2014
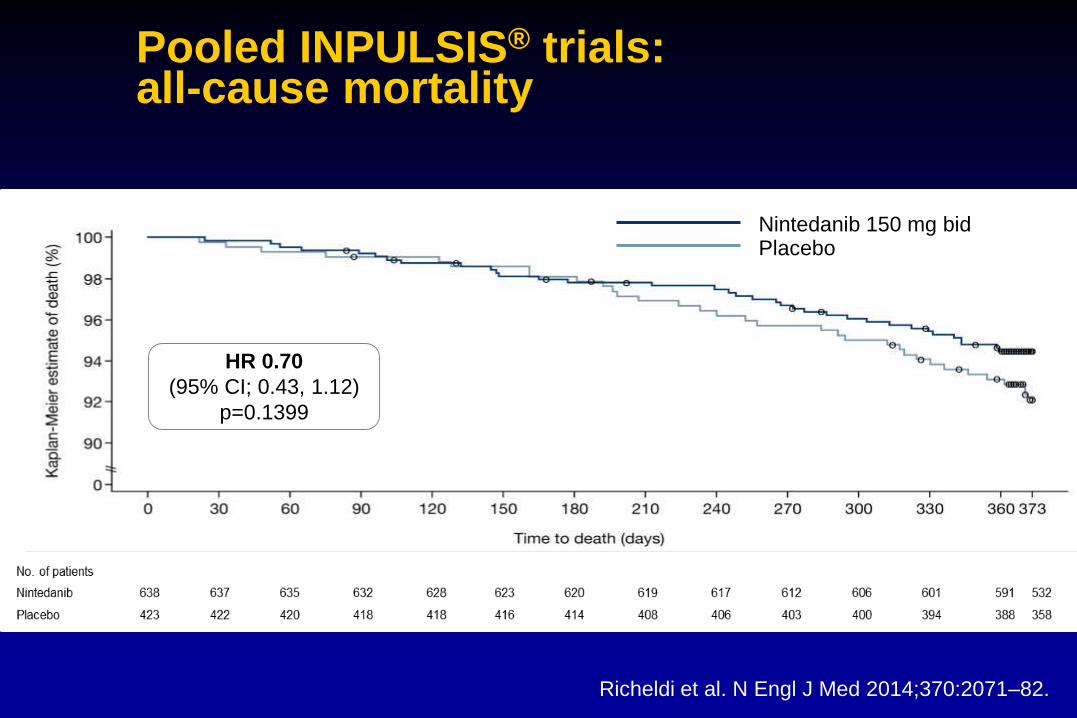
Pooled INPULSIS® trials:all-cause mortality
Richeldi et al. N Engl J Med 2014;370:2071–82.
PlaceboNintedanib 150 mg bid
HR 0.70
(95% CI; 0.43, 1.12)
p=0.1399
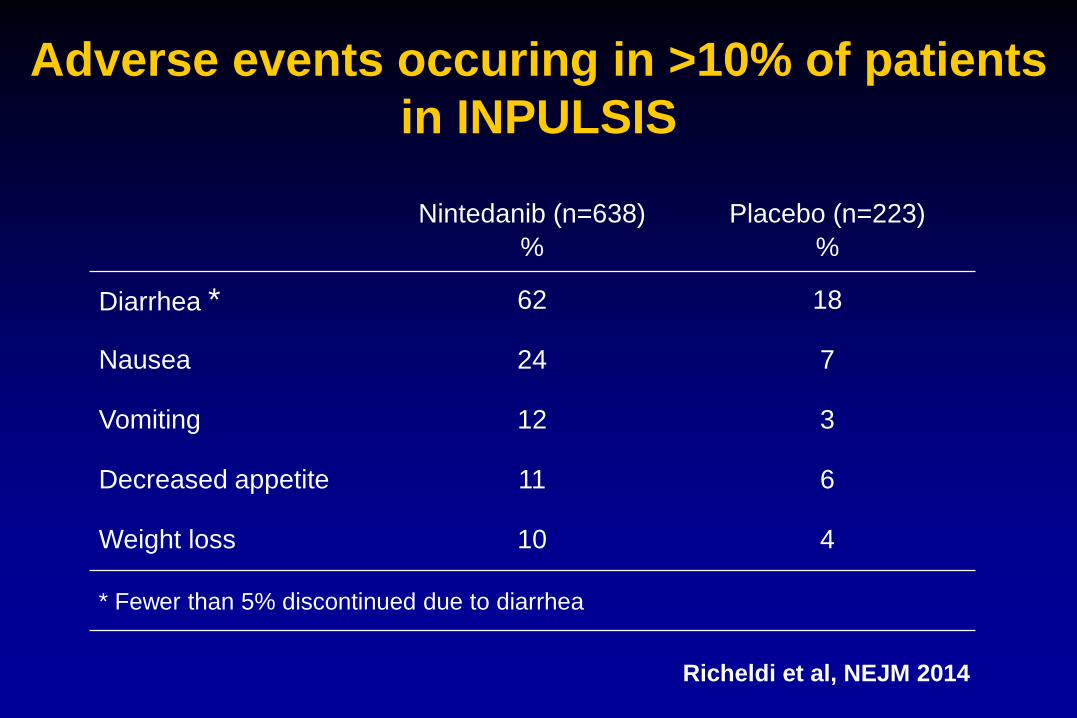
Adverse events occuring in >10% of patients
in INPULSIS
Nintedanib (n=638)
%
Placebo (n=223)
%
Diarrhea * 62 18
Nausea 24 7
Vomiting 12 3
Decreased appetite 11 6
Weight loss 10 4
* Fewer than 5% discontinued due to diarrhea
Richeldi et al, NEJM 2014

Nintedanib: summary
• This clinically relevant effect of nintedanib on disease progression is further supported by:
– A numerical reduction in the risk of acute exacerbations
– A significantly reduced risk of adjudicated confirmed or suspected exacerbations
– A numerical reduction in all-cause mortality (pooled INPULSIS®)
– Consistent positive results across a range of lung function endpoints and sensitivity analyses
• Nintedanib was associated with a manageable safety profile
Nintedanib consistently slows disease progression in IPF
by significantly reducing the annual decline in lung
function by approximately 50%
Richeldi et al. N Engl J Med 2014;370:2071–82.

Subgroup analyses of rate of
decline in FVC

Nintedanib demonstrated a consistent effect on the annual
rate of decline in FVC across all pre-specified subgroups
Costabel U et al. Am J Respir Crit Care Med 2016.

Costabel U et al. Am J Respir Crit Care Med 2015; epub ahead of print.
Pre-specified subgroup analysis by baseline FVC ≤70% vs
>70% predicted
Ad
juste
d a
nn
ua
l ra
te (
SE
) o
f d
eclin
e in
FV
C (
mL
/ye
ar)
Nintedanib Placebo
Treatment-by-time-by-
subgroup interaction
p=0.9505
∆113.5 mL
(95% CI: 51.3, 175.7)
FVC ≤70% predicted
∆109.0 mL
(95% CI: 68.2, 149.9)
n=207 n=154 n=431 n=269
FVC >70% predicted
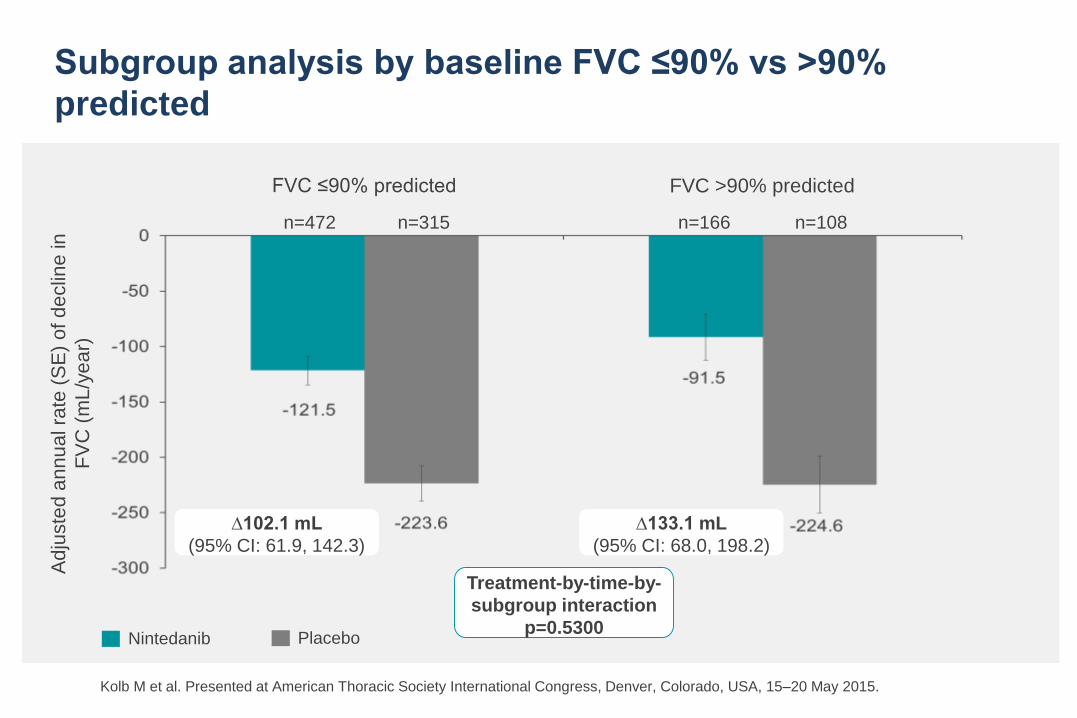
Kolb M et al. Presented at American Thoracic Society International Congress, Denver, Colorado, USA, 15–20 May 2015.
Subgroup analysis by baseline FVC ≤90% vs >90%
predicted
Ad
juste
d a
nn
ua
l ra
te (
SE
) o
f d
eclin
e in
FV
C (
mL
/ye
ar)
Nintedanib Placebo
FVC ≤90% predicted
n=472 n=315 n=166 n=108
FVC >90% predicted
Treatment-by-time-by-
subgroup interaction
p=0.5300
∆102.1 mL
(95% CI: 61.9, 142.3)
∆133.1 mL
(95% CI: 68.0, 198.2)
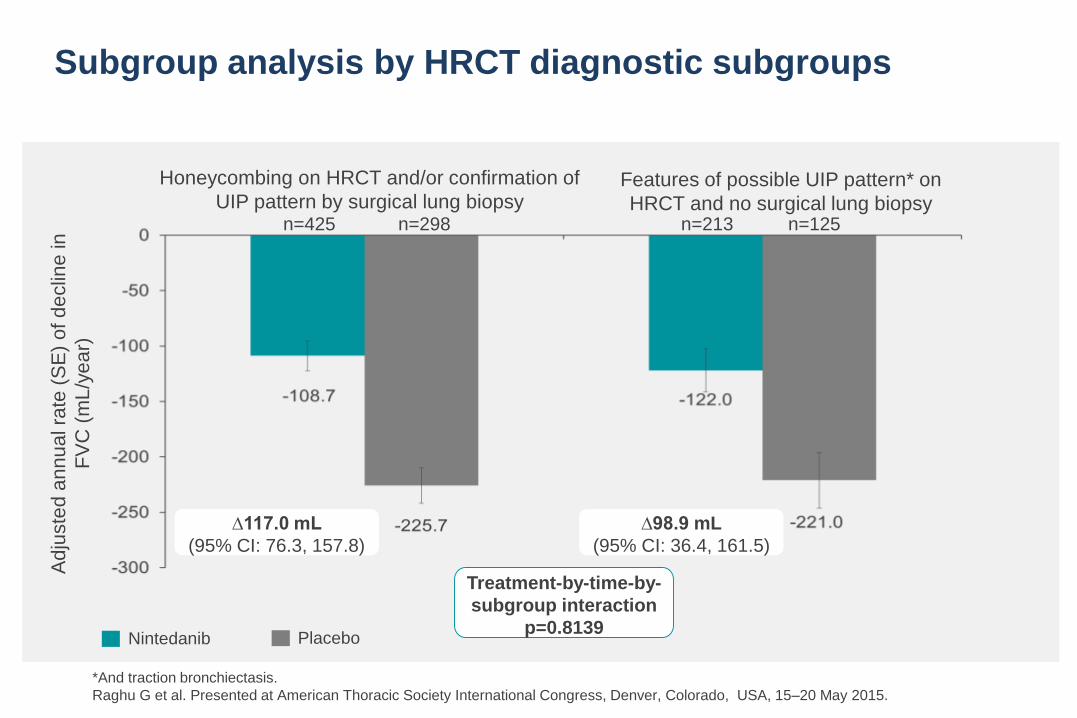
*And traction bronchiectasis.
Raghu G et al. Presented at American Thoracic Society International Congress, Denver, Colorado, USA, 15–20 May 2015.
Subgroup analysis by HRCT diagnostic subgroups
n=425 n=298 n=213 n=125
Honeycombing on HRCT and/or confirmation of
UIP pattern by surgical lung biopsyFeatures of possible UIP pattern* on
HRCT and no surgical lung biopsy
Nintedanib Placebo
Ad
juste
d a
nn
ua
l ra
te (
SE
) o
f d
eclin
e in
FV
C (
mL
/ye
ar)
Treatment-by-time-by-
subgroup interaction
p=0.8139
∆117.0 mL
(95% CI: 76.3, 157.8)
∆98.9 mL
(95% CI: 36.4, 161.5)
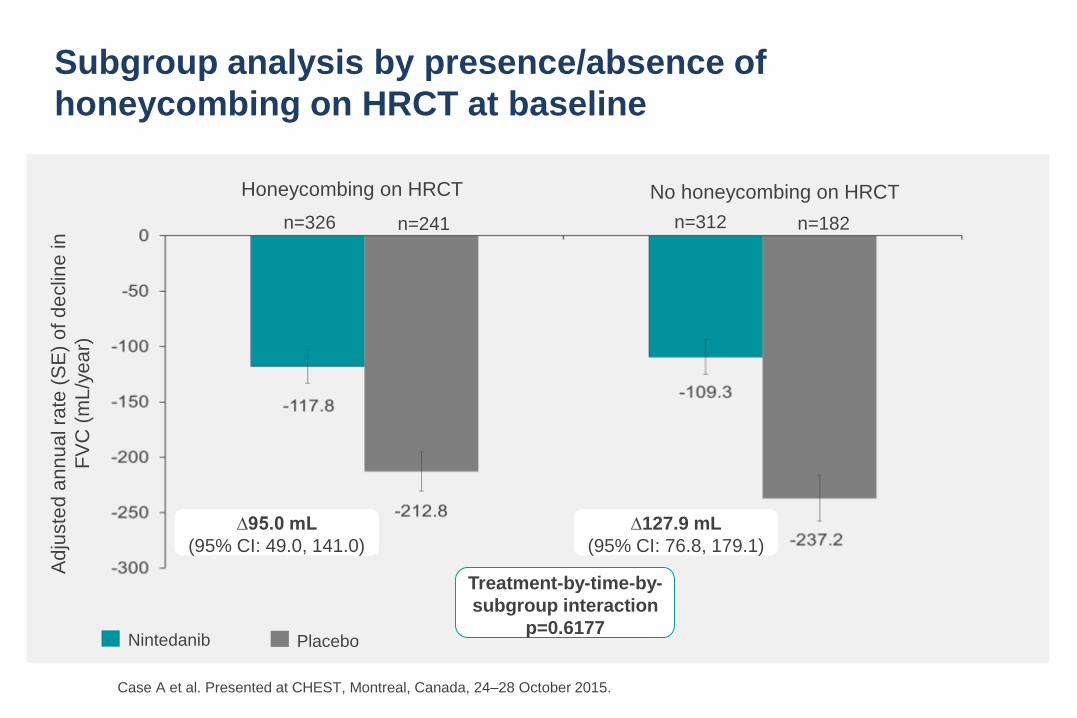
Subgroup analysis by presence/absence of
honeycombing on HRCT at baseline
Ad
juste
d a
nn
ua
l ra
te (
SE
) o
f d
eclin
e in
FV
C (
mL
/ye
ar)
Nintedanib Placebo
Treatment-by-time-by-
subgroup interaction
p=0.6177
∆95.0 mL
(95% CI: 49.0, 141.0)
Honeycombing on HRCT
∆127.9 mL
(95% CI: 76.8, 179.1)
n=326 n=241 n=312 n=182
No honeycombing on HRCT
Case A et al. Presented at CHEST, Montreal, Canada, 24–28 October 2015.
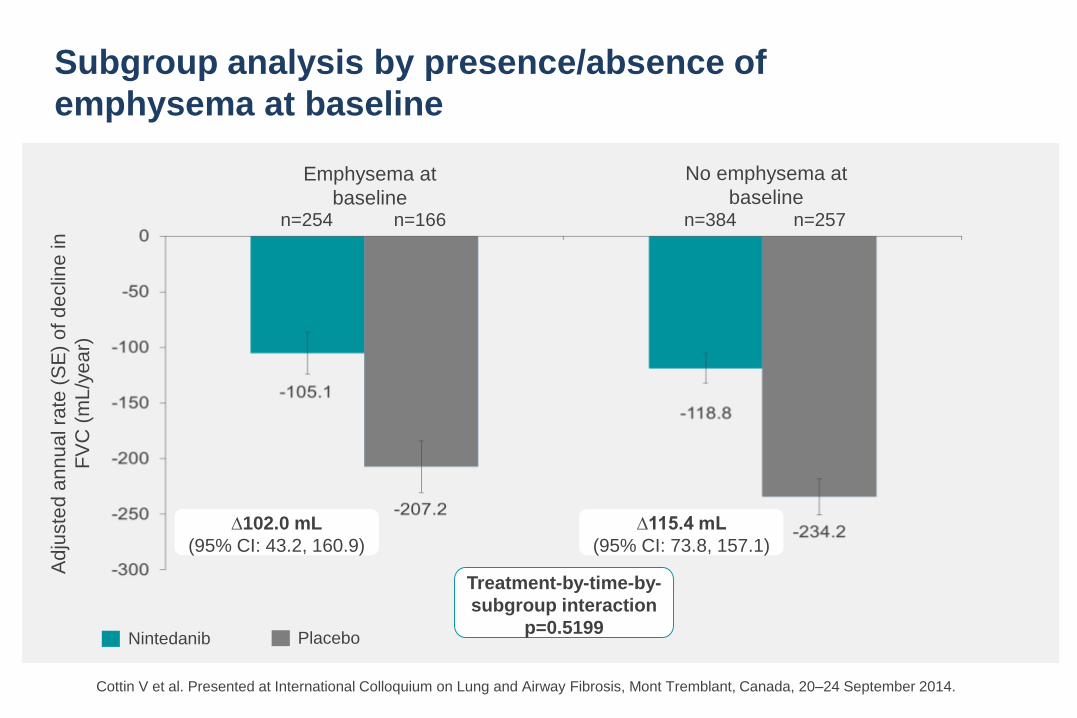
Cottin V et al. Presented at International Colloquium on Lung and Airway Fibrosis, Mont Tremblant, Canada, 20–24 September 2014.
Subgroup analysis by presence/absence of
emphysema at baseline
Emphysema at
baseline
No emphysema at
baselinen=254 n=166 n=384 n=257
Nintedanib Placebo
Ad
juste
d a
nn
ua
l ra
te (
SE
) o
f d
eclin
e in
FV
C (
mL
/ye
ar)
Treatment-by-time-by-
subgroup interaction
p=0.5199
∆102.0 mL
(95% CI: 43.2, 160.9)
∆115.4 mL
(95% CI: 73.8, 157.1)
Subgroup analyses of time to
first acute exacerbation
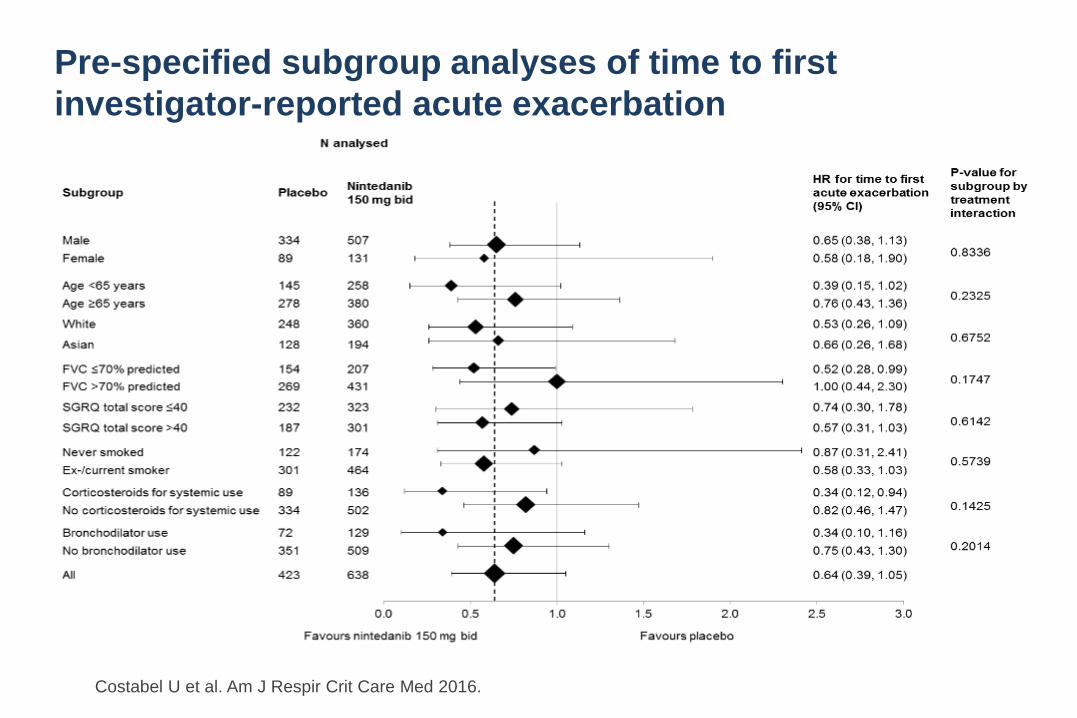
Pre-specified subgroup analyses of time to first
investigator-reported acute exacerbation
Costabel U et al. Am J Respir Crit Care Med 2016.
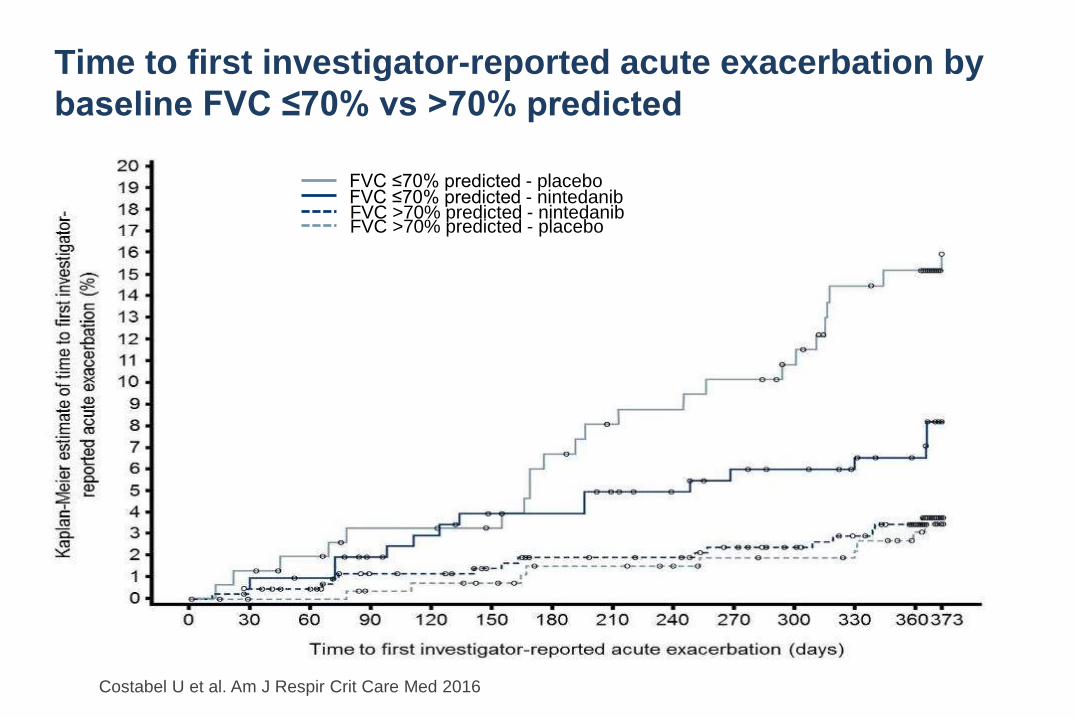
Time to first investigator-reported acute exacerbation by
baseline FVC ≤70% vs >70% predicted
Costabel U et al. Am J Respir Crit Care Med 2016
FVC ≤70% predicted - nintedanibFVC ≤70% predicted - placebo
FVC >70% predicted - nintedanibFVC >70% predicted - placebo

IPF Phase III Trials in Comparison
ASCEND INPULSIS
68 yr, 79% men, 64% smokers 67 yr, 79% men, 72% smokers
95% definite UIP pattern on
HRCT
97% UIP pattern on HRCT
40% emphysema on HRCT
FEV1/FVC ≥0.8 FEV1/FVC ≥0.7
30% SLB performed 21% SLB performed
FVC 68% pred.
DLCO 44% pred.
FVC 82% pred.
DLCO 47% pred.
35% pts screened enrolled 70% pts screened enrolled
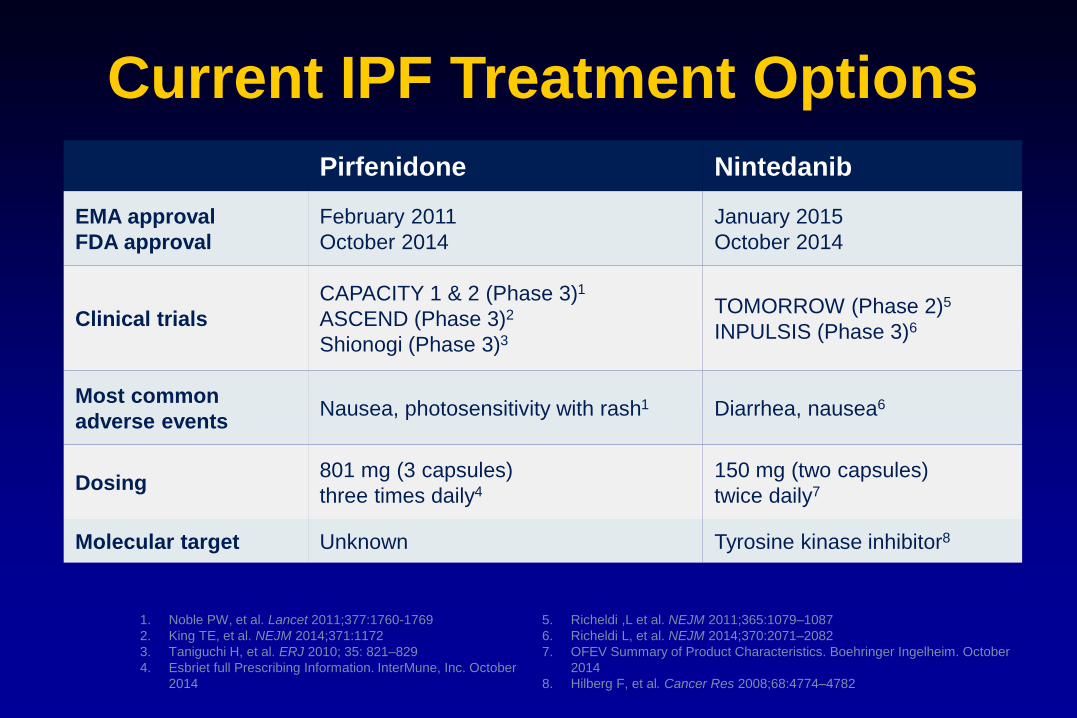
Current IPF Treatment Options
Pirfenidone Nintedanib
EMA approval
FDA approval
February 2011
October 2014
January 2015
October 2014
Clinical trials
CAPACITY 1 & 2 (Phase 3)1
ASCEND (Phase 3)2
Shionogi (Phase 3)3
TOMORROW (Phase 2)5
INPULSIS (Phase 3)6
Most common
adverse eventsNausea, photosensitivity with rash1 Diarrhea, nausea6
Dosing801 mg (3 capsules)
three times daily4
150 mg (two capsules)
twice daily7
Molecular target Unknown Tyrosine kinase inhibitor8
5. Richeldi ,L et al. NEJM 2011;365:1079–1087
6. Richeldi L, et al. NEJM 2014;370:2071–2082
7. OFEV Summary of Product Characteristics. Boehringer Ingelheim. October
2014
8. Hilberg F, et al. Cancer Res 2008;68:4774–4782
1. Noble PW, et al. Lancet 2011;377:1760-1769
2. King TE, et al. NEJM 2014;371:1172
3. Taniguchi H, et al. ERJ 2010; 35: 821–829
4. Esbriet full Prescribing Information. InterMune, Inc. October
2014
Key Challenges and Questions 2016
• How to ensure prompt and correct diagnosis?
• Combination therapy?
• Which drug first?
• When should treatment be started?
• When should treatment be stopped?
• Current antifibrotic drugs cannot cure IPF
• They have shown to slow disease progression by 50%,
on average, in clinical trial populations but not in every
patient
• Some patients will not respond to treatment
• Should a stable patient with mild disease
be treated?
The problem
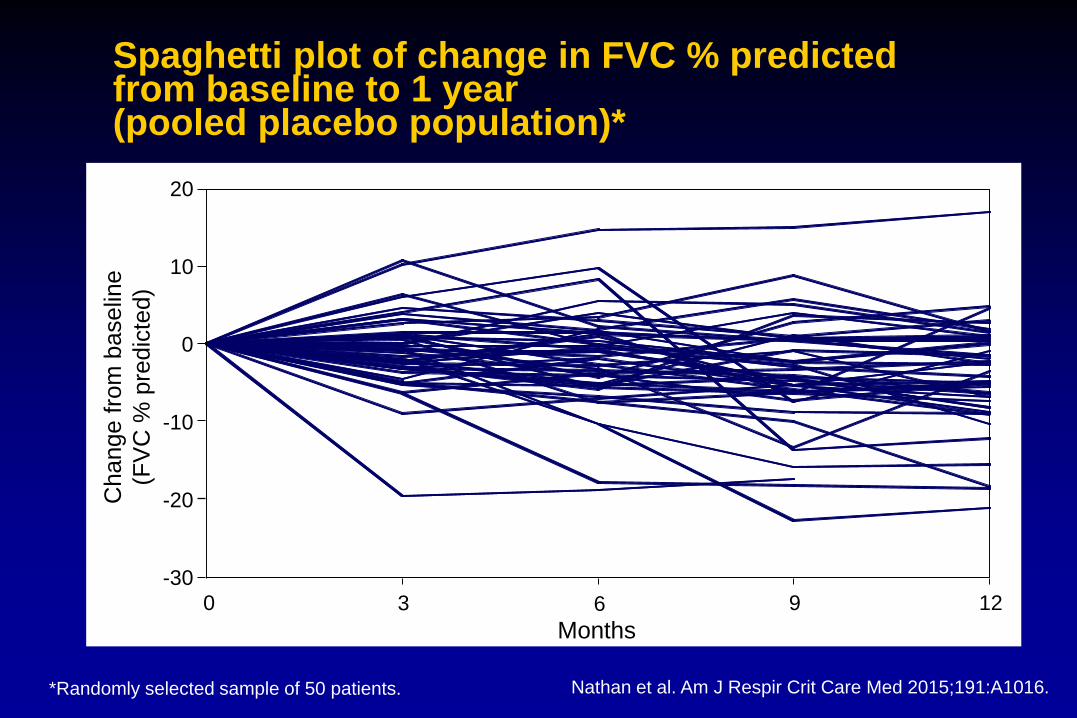
Spaghetti plot of change in FVC % predicted from baseline to 1 year (pooled placebo population)*
Change f
rom
baselin
e
(FV
C %
pre
dic
ted)
-30
-20
-10
0
10
20
Months
0 3 6 9 12
*Randomly selected sample of 50 patients. Nathan et al. Am J Respir Crit Care Med 2015;191:A1016.
How many patients with IPF
are stable or improve?
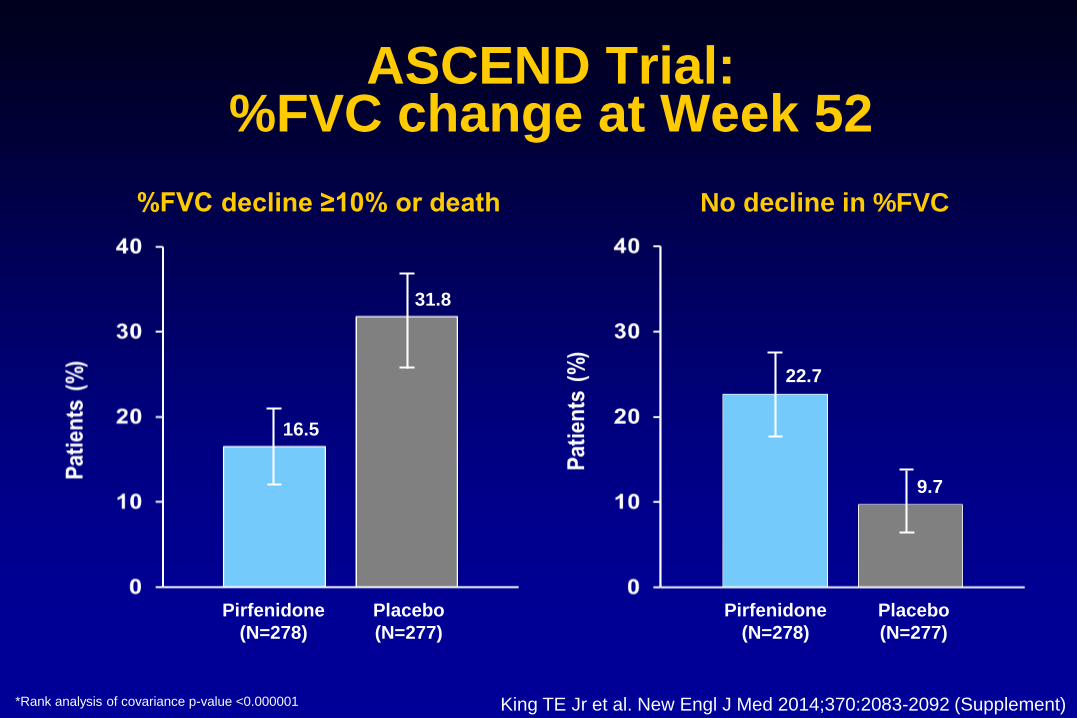
%FVC decline ≥10% or death No decline in %FVC
22.7
9.7
16.5
31.8
*Rank analysis of covariance p-value <0.000001
ASCEND Trial: %FVC change at Week 52
Pirfenidone
(N=278)
Placebo
(N=277)
Pirfenidone
(N=278)
Placebo
(N=277)
King TE Jr et al. New Engl J Med 2014;370:2083-2092 (Supplement)

INPULSIS®: patients with no absolute decline of FVC >5% predicted at week 52
OR 1.85(95% CI: 1.28, 2.66)
p=0.0010
OR 1.79(95% CI: 1.26, 2.55)
p=0.0011
OR 1.84(95% CI: 1.43, 2.36)
p<0.0001
Nintedanib 150 mg bid Placebo
INPULSIS®-1 INPULSIS®-2 Pooled data
n=309 n=204 n=329 n=219 n=638 n=423
Resp
on
ders
(%
)
Patients with missing data at week 52 were considered to be non-
respondersRicheldi et al. N Engl J Med 2014;370:2071–82.

Is antifibrotic therapy effective
in stable IPF?

Intraindividual response to pirfenidone
Annual FVC decline >10%
N=76
Loeh B et al. Am J Respir Crit Care Med 2015;191:110-113

N=71
Intraindividual response to pirfenidone
Annual FVC decline 10%
Loeh B et al. Am J Respir Crit Care Med 2015;191:110-113
How frequent is early ILD
in the elderly?

• Consecutive computed tomography study in
asymptomatic volunteers aged >75 years
• Subpleural, basal, reticular ILD in 24 / 40 (60%)
• Do they all have IPF?
• Should they all be treated prophylactically?
Lung morphology in the elderly
Copley SJ et al. Radiology 2009;251:566-573ILD, interstitial lung disease
Key Challenges and Questions 2016
• How to manage side effects?
• Long term treatment effective?
• What are realistic treatment expectations?
• Can we predict response to therapy?
Long-term efficacy?

INPULSIS® and INPULSIS®-ON: study designs
• Patients who completed the 52-week treatment period and follow-up visit 4 weeks later in an INPULSIS® trial were eligible to enter INPULSIS®-ON
• Dose reduction to 100 mg bid and treatment interruption were allowed to manage adverse events; dose re-escalation to 150 mg bid was permitted
Continuing nintedanib (n=430)
Open-label extension
INPULSIS®-ON
Double-blind, placebo-controlled
INPULSIS®
Nintedanib 150 mg bid (n=638)
No treatment*
Placebo (n=423)
ScreeningR 3:2 ratio
Week 52
Initiating nintedanib (n=304)
*Per protocol, the off-treatment period between INPULSIS® and INPULSIS®-ON could be between 4 and 12 weeks.
Crestani et. al. Presented at the European Respiratory Society International Congress, Amsterdam, The Netherlands,
September 26–30, 2015
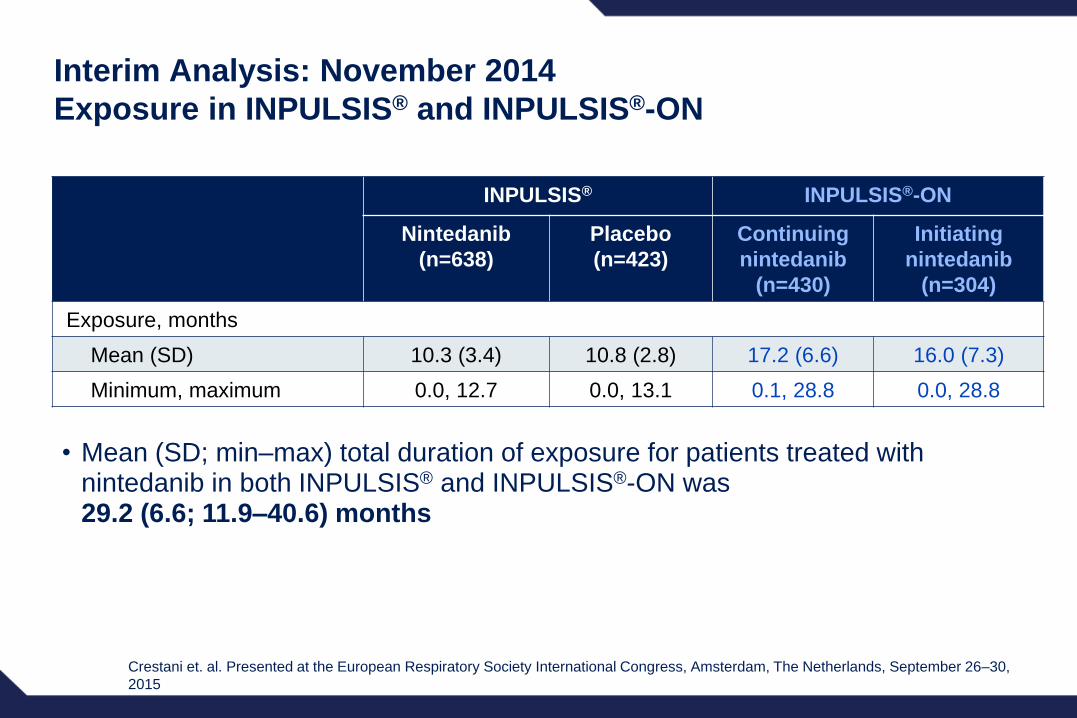
Interim Analysis: November 2014
Exposure in INPULSIS® and INPULSIS®-ON
• Mean (SD; min–max) total duration of exposure for patients treated with nintedanib in both INPULSIS® and INPULSIS®-ON was 29.2 (6.6; 11.9–40.6) months
INPULSIS® INPULSIS®-ON
Nintedanib
(n=638)
Placebo
(n=423)
Continuing
nintedanib
(n=430)
Initiating
nintedanib
(n=304)
Exposure, months
Mean (SD) 10.3 (3.4) 10.8 (2.8) 17.2 (6.6) 16.0 (7.3)
Minimum, maximum 0.0, 12.7 0.0, 13.1 0.1, 28.8 0.0, 28.8
Crestani et. al. Presented at the European Respiratory Society International Congress, Amsterdam, The Netherlands, September 26–30,
2015

Change from baseline in FVC at week 52 in INPULSIS®
and at week 48 in INPULSIS®-ONM
ea
n (
SE
M)
ob
se
rve
d c
ha
ng
e fro
m b
ase
line
in
FV
C (
mL
)
INPULSIS®-ONINPULSIS®
Nintedanib
n=519
Placebo
n=345
Continuing
nintedanibn=352
Initiating
nintedanibn=233
Crestani et al. ERS 2015

Real-life experience with
antifibrotic therapy

Pirfenidone for IPF in the real world
– Number of patients: 45
– Average duration of treatment: 48 weeks
Safety and tolerance
– Side effects: 58%
– Dose adjustment: 18%
Discontinuation
– Total: 33%
– Due to progression: 20%
– Due to side effects: 13%
Real-world scenario
Bonella F et al. Dtsch Med Wochenschr 2013;138:518-523
Is response to IPF therapy
predictable?
TOLLIP, MUC5B and the Response to
N-acetylcysteine among Individuals with
Idiopathic Pulmonary Fibrosis
Justin M. Oldham , MD 1,2 , Shwu-Fan Ma , PhD 1 , Rekha Vij , MD 1 , Yong Huang , MD 1 ,
Ganesh Raghu , MD 3 , Kevin J. Anstrom , MD, PhD 4 , Fernando J. Martinez , MD, MS 5 ,
Imre Noth , MD 1
1. Department of Medicine, Section of Pulmonary and Critical Care Medicine; The
University of Chicago
2. Department of Internal Medicine, Weill Cornell Medical School
3. Duke Clinical Research Institute; Duke University
4. Department of Medicine, Division of Pulmonary and Critical Care Medicine; The
University of Washington Medical Center
5. Department of Medicine, The University of Colorado
Am J Respir Crit Care Med 2015; 192: 1475-82

• 154 PANTHER participants genotyped for 5 SNPs on Chr11:
rs35705950 in MUC5B and rs5743890, rs5744034, rs3750920 and
rs5743854 in TOLLIP
• Minor allele frequency (MAF) of each SNP compared to that of 868
IPF GWAS patients.
• Minor allele counts compared between the prednisone/azathioprine/N-
acetylcysteine, N-acetylcysteine (NAC) and placebo arms
Genetic Heterogeneity Among Patients
Enrolled In The PANTHER-IPF Clinical Trial
Oldham et al, AJRRCM 2015

Composite endpoint-free survival between NAC and
Placebo groups after stratification by
rs3750920 (TOLLIP) genotype
Oldham et al, AJRRCM 2015
HR 3.23
p=0.10
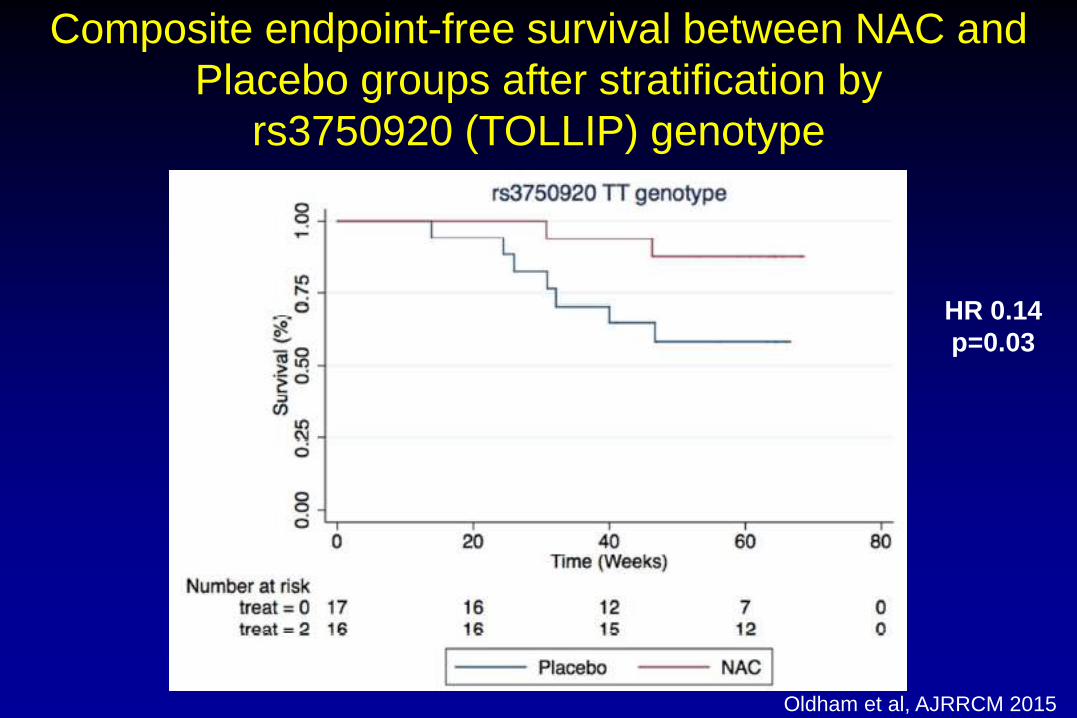
Composite endpoint-free survival between NAC and
Placebo groups after stratification by
rs3750920 (TOLLIP) genotype
Oldham et al, AJRRCM 2015
HR 0.14
p=0.03
Interstitial and Rare Lung Disease Unit
Prof. U. Costabel
Dr. F. Bonella
Dr. T.E. Wessendorf
Dr. E. Börner
Dr. M. Cuyas
Dr. X. Long
Prof. J. Guzman
Dr. S. Ohshimo
Prof. D. Theegarten
Mrs. L. Ngoc Tran
Thank you for your attention