iron stores and coagulation parameters in patients antônio baddini martinez, celso carlos de...
TRANSCRIPT

José Antônio Baddini Martinez,Celso Carlos de Campos Guerra, Luiz Eduardo Nery,
José Roberto de Brito Jardim
Iron stores and coagulation parameters in patients withhypoxem' c polycythemia secondary to chronic obstructive
pulmonary disease: The effect of phlebotomiesFrom the Respiratory and Hematology Divisions, Universidade Federal de São Paulo/Escola Paulista tle Medicina -
São Paulo, Brazil.
This study was designed to determine the effects of phlebotomy on iron body contents and coagulation tests of COPO patients withpo'ycythemia secondary to hypoxemia. Seventeen patients with COPO and hematocrits higher than 54 percent (mean Hct: 57 :t 0.49percent ), who had not received anti-inflammatory or antiplatelet aggregation agents recently.Their mean forced expiratory volume at1 second (FEV1) was 0.92:t 0.11 L. Intervention: Blood work was collected to evaluate the following: serum iron and ferritin leveis, totaliron binding capacity, transferrin saturation index, fibrinogen plasma leveis, activated partial thromboplastin time, platelet count, plate-let aggregation measurements, and thromboelastography coagulation parameters. The blood samples were obtained before andabout 7 days after the hematocrit correction by 300-400 ml phlebotomies done every other day.The mean number of phlebotomiesdone for each patient was 4.4. Postphlebotomy iron serum leveis decreased from 90.1 :t 14.8 to 59.7:t 9.9 mg/dl and the ferritin serumleveis from 133.8 :t 37.9 to 70.8 :t 32.7 ng/ml (p< 0.05). Regarding the coagulation studies, there were significant increases in theplatelet count, from 227,300 :t 13,900 to 312,500 :t 30,200 per mm3, and in the maximum clot amplitude (a) obtained bythromboelastography ( from 53.6 :t 1.4 percent to 60.4 :t 1.1 percent). The coagulation time (k) of the thromboelastography alsodecreased significantly, from 7.5 :t 0.7mm prephlebotomy to 4.5 :t 0.3mm postphlebotomy. Although the coagulation changes weresmall amount, the observed significant decrease in iron contents may have important clinicai implications.
UNITERMS: Secondary polycythemia; repetitive phlebotomies; iron deficiency; coagulation; chronic obstructive pulmonary disease
INTRODUCTION
B loodlettings, or phlebotomies, are still adyocatedin the care of chronic obstructive pulmonarydisease (COPD) patients with cor pulmonale and
severe secondary polycythemia.1 Several authors haveshown that hematocrit (Hct) reductions in hypoxemicpatients with COPD and polycythemia are followed byimprovement in general symptoms,2-S mental activity2-6 andexercise performance.2-4.7.8
Address for correspondence:José A. B. Martinez MODisciplina de Pneumologia (Lung Division) UNIFESP/EPMRua Botucatu, 740 - Vila ClementinoSão Paulo/SP - Brasil - CEP 04023-900
In a group of patients performing exercise studies inergometer, the maximum workload and oxygenconsumption have increased 31 and 16 percentrespectively, when the mean Htc had decreased from 62to 50 percent,x These effects are not secondary to changesin respiratory mechanics or blood gases.2.4.S.7-10Rather, itseems they result from improvements in hemodynamicconditions related to a better blood viscosity.3.11-13
Although a great deal has been published in this field,no attention has been paid to the potential hematologicalconsequences of phlebotomies. Similarly to what happenswith blood donors and during the treatment ofhemochromatosis, repeated phlebotomies in COPDpatients could lead to reductions in their iron bodycontents.14.1S Iron deficiency states may run withdecrements in work performance secondary to drops in
MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - lron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructivepulmonary disease: The effect of phlebotomies
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997
1396
helTIoglobin leveIs, and disturbances in muscular oxidativemetaboIism.1ó In the case of reductions in iron bodycontents actualIy deveIoping in COPD patients folIowingphlebotomies, the former could act as limiting factors forexpected exercise improvements.
In addition, polycythemia is a welI known risk factorfor thrombosis,17 and lnany studies. suggest that COPDpatients have a higher tendency to have thromboembolicepisodes.IX-20 SOlne studies of thrombotic risk in COPDhave shown an increased tendency towards coagulationwith altered values in the throlnboelastogram,hyperfibrinogemia and increased platelet aggregation.1x'21-23Therefore, we hypothesized that a reduction in Hct leveIsby phlebotolnies could aIso have a favorable effect ondecreasing s'uch thrombotic risk.
The present study investigates the effects of the Hctcorrection by repeated phlebotomies on paralneters ofhemostasis and body iron contents in COPD patients withsevere secondary hypoxemic polycythemia.
PATIENTS AND METHODS
Patient Selection
Seventeen with COPD and polycythelnia ( Hct 54percent or more) patients were studied after signing aninformed consent formo All patients were in stablerespiratory conditions, without clinicaI evidence of right orleft ventricular faiIure. They had not been under anyantiplatelet or anti-inflammatory agent for at least the prior10 days, and.during the study period there were no changesin their daily medications. None of the patients showedclinicaI evidence ofblood loss or were using oxygen at thattime.
Following an initiallaboratory evaIuation, phlebotomiesof 300 to 400 ml were perfonned every other day until avenous Hct value around 45 percent was reached (range: 41-48 percent). A second set of laboratory tests was thenperformed about 7 days after the last phlebotomy 'session.
Iron Stores Measurements
Venous blood samples with no anticoagulant werecollected from fasting patients in the Inorning. Iron serulnleveIs and seruln total iron binding capacity (TIBC) weremeasured using a commercialIy available kit (Iron Roche@)
with readings made with a Colelnan 6/20spectrophotometer. Ferritin serum leveIs were alsoevaluated by a commercially available enzymaticimmunoassay (FerrizYlne TM@- Abbot Laboratories). Thetransferrin saturation index (TSI) was calculated as thepercentile ratio between serum iron leveIs and TIBC.
Coagulation Studies
Coagulation tests were performed on 3.8 percentsodium citrate venous blood samples collectedsimuItaneously with the iron blood work. The followingdeterminations were made:
- Activated paltial thromboplastin time (APTT) usinghuman cephalin.24 The results were expressed as the ratioto the control values for the Iaboratory on that day.
- Fibrinogen plasma leveIs, assessed by the Ratnoff-Menzie Inethocl.25
- PlateIet count, made in an automatic counter ClayAdams modeI Ultra-FIo.
- Platelet aggregation determinations by the Bornlnethod in a Chronolog aggregometer.2ó The aggregationagents ADP in concentrations of 1 mM and 3 mM,epinephrine at 1:1000 dilution, and hUlnan colIagen wereused in salnples froln each patient. The percentage ofaggregated pIatelets was caIculated at a curve pointcorresponding to an interval of 5 minutes from the initial.stimulus for each aggregation agent.
- Throlnboelastography (TEG), using a Hartertthrolnboelastograph lnade by HelIige. This test exalninesthe entire bloocl coaguIation process and the interactionof alI involvecl cOlnponents.27 The reaction tilne r, thecoagulation time k, and the lnaxil11um cIot alnpIitude a ,were lneasured using a special ruIer on the developed filmo
Statistical Methods
All data are expressed as the mean :t standard error.The WiIcoxon test was used in the statistical analysis forthe nonindependent variables. A. leveI of 5 percent wasfixed as the litnit for rejection of the null hypothesis.
RESULTS
Thirteen male and four female patients were studiecl.Most of theln had severe or 1110derateCOPD with arterialhypoxemia (Table 1). The mean Hct fell frol1157 percentbefore phebotolnies to 45 percent at the time of the final
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997 MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - Iron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructive
pulmonary disease: The effect of phlebotomies

1397
Table 1Patient Summary
Age FEV1 FVC/FEV1 Pa02 Hct Pre Hct PostNo. Gender yr L % mmHg % %
1 M 53 1.17 50 47 54 452 M 44 0.82 38 39 55 483 M' 60 0.71 35 44 54 444 M 63 0.59 31 49 57 455 M 44 0.65 38 45 60 456 F 36 0.47 47 42 57 417 M 50 1.46 50 46 63 448 F 72 0.48 45 38 56 469 M 28 0.57 36 42 58 4710 M 75 1.19 45 49 60 4711 M 67 1.41 60 53 58 4412 M 70 1.68 60 51 55 4513 F 42 0.65 32 46 56 4314 F 68 0.44 37 49 58 4415 M 70 0.62 35 53 57 4616 M 35 1.88 49 52 55 4517 M 66 0.93 28 59 55 42Mean 55:t3.6 0.92:t .11 42:t2.4 47:t1.2 57:t.49 45:t.49
TIBC: serum total iron binding capacity; TSI: transferin saturation indexo*p< 0.05
Table 2Iron contents measurements (Mean :!: SE) obtained
pre-and postphlebotomy
There were significant decreases in the serunl leveIsof iron, ferritin and TSI postphlebotolny (Table 2). Twelve
studies. The second set of blood tests were collected 8.7 :t1.3 days after the Iast phlebotomy. The time between bloodcollection and actuaI sample analysis was no longer thantwo hours in every case.
Postphlebotomy
59.7:t 9.9*399.9 :t 20.016.7:t 3.6*
Prephlebotomy
90.1 :t 14.8393.6 :t 27.625.4 :t 4.9
Coagulation Studies
Coagulation studies obtained before and afterphlebotomies are listed in Table 3. Ali the initial Ineanvalues were within the norlnal limits' of the authors'laboratory except for the r paralneter of the TEG, vvhichwas slightly increased. No significant decreases were seenin the Inean APTT and fibrinogen leveIs afterphlebotolnies. The platelet count significantly increasedfronl 227,3001Inln3 to 312,000/mm3 after the procedure.Fifteen patients (88.2 percent) showed an increase in the
Normal Range
50-150200-40020-50
Iron, mg/dlTIBC, mg/dlTSI, %
a decrease i n i ron
Iron Measurements
patients (70 percent) showedconcentrations and in 7 of theseit remained below 50 percent ofthe initial value. Falls in ferritinleveIs were seen in 16 patients(94 percent). Such decreaseswere greater than 50 percentfrom the baseline values in 12(70 percent) of the subjects. In8 patients (47 percent), the finalferritin values were below 10 ng/Inl, indicating severe irondepletion (Fig. 1).
MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - lron stores and coagulationparameters in pa~ients with hypoxemic polycythemia secondary to chronic obstructivepulmonary disease: The effect of phlebotomies
São Paulo Medicai JournallRPM 115(2): 1395-1402, 1997

1398
'OSTPK.EBOTOMY
r-PCO.os -,
PREPHELEBOTOMY
,-- pc 0.05 -,
300 410
400250
1_ 350E
200 .5._I zz t=o ~ 250e: 150 ~
200
100 150
10050
50
PRE 'OSTPHELEBOTOMY PK.EBOTOMY
2). Serum ferritin is a good indicator ofiron body stores, and the drop in its leveIsdenotes that the tissue iron contents28,29were also affected.
Iron deficiency states may haveeffects on red blood cells and solid organtissues. Although it would be expectedthat iron deficiency could have aninhibitory effect on COPD hypoxichemopoietic response, this is not alwaysthe case. Secondary polycythemiaassociated to iron deficiency in COPDpatients has been described.30,31 Someauthors report that iro,n depletion may notbe an impeding factor to increases in redcell mass, and that in such casespolycythemia is associated withhypochromic erythrocytes.32
An iron deficiency state may alsoFigure 1- Iron and ferritin individual values for COPO patients submitted to sequencial di sturb the mu scular oxidati vephlebotomies. metabolism, interfering with the patient's
work performance. 16 The tissue haem ironcompounds include the cytoçhromes, myoglobin, catalaseand peroxidase. In additiQD, muscles harbor non-haemiron-containing enzymes such as NADH dehydrogenase,succinic dehydrogenase and xanthine oxidase. Finally,some enzymes such as aconitase and tryptophan pyrrolaserequire iron or haem as a cofactor.
Experimental studies on rats have found that mildand severe iron deficiency are associated with deficits 9fcytochrome c and mioglobin in skeletal muscle.33 FINCHet a1.34 completed studies of work performance on iron-deficient rats, keeping hemoglobin leveIs constant throughexchange transfusions. It was seen that iron-deficient ratshad a significant shorter running time than çontrols withsimilar hemoglobin leveIs. After 4 days of ironadministration, the iron-deficient group achieved normalrunning times.
Biochemical analysis done at that time suggested thatan increase in the rate of oxidative phosphorylation witha-glycerophosphate as a substrate played a key role in theimprovement of work performance. Non-published datafrom our laboratory have shown small but significantincreases in the maximal work load and oxygenconsumption reached by 15 iron-deficient, anemic wom'4 days after administration ofIV iron-dextran, ev~n thoughtheir hemoglobin leveIs had not changed.
Therefore, we can hypothesize that COPD patientswho show ameIioration of exercise performance afterphIebotomies lnight have this effect attenuated ifsimuItaneous iron deficiency states deveIop. The
DISCUSSION
platelet count, 4 of them with final measurements beyond400,OOO/mm.3 Studies of platelet aggregation made withdifferent stimulant agents did not show any significantpostphlebotomies change.
Adequate thromboelastography studies before andafter phIebotomies could not be obtained in 4 patients dueto technical problems. In the 13 studied subjects, asignificant decrease was noticed in k during the finalstudies. Although r also experienced a decrease, suchchange did not reach statistical significance. Finally, avalues showed a significant postphlebotomies increase.
Phlebotomy may be used in the care of COPDpatients in an attempt to reduce detrimental cardiovasculareffects of blood hyperviscosity due to polycythemia. Thebasis for this procedure is the effect of phIebotomy inimproving hemodynamic conditions and exerciseperformance in such patients.2-4,7,8,11-13 However, the effectsof this kind of therapy on hemostasis and iron reserves ofCOPD patients had not been thoroughIy examined before.
Our present resuIts showed that the normalization ofhematocrits by phlebotomies led to an important reductionin iron body contents. This became apparent by thesignificant decreases in serum iron, ferritin and TSI (Table
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997 MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - Iron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructive
pulmonary disease: The effect of phlebotomies
1399
Table 3Results of coagulation studies (Mean :!: SE) obtained pre-and postphlebotomy
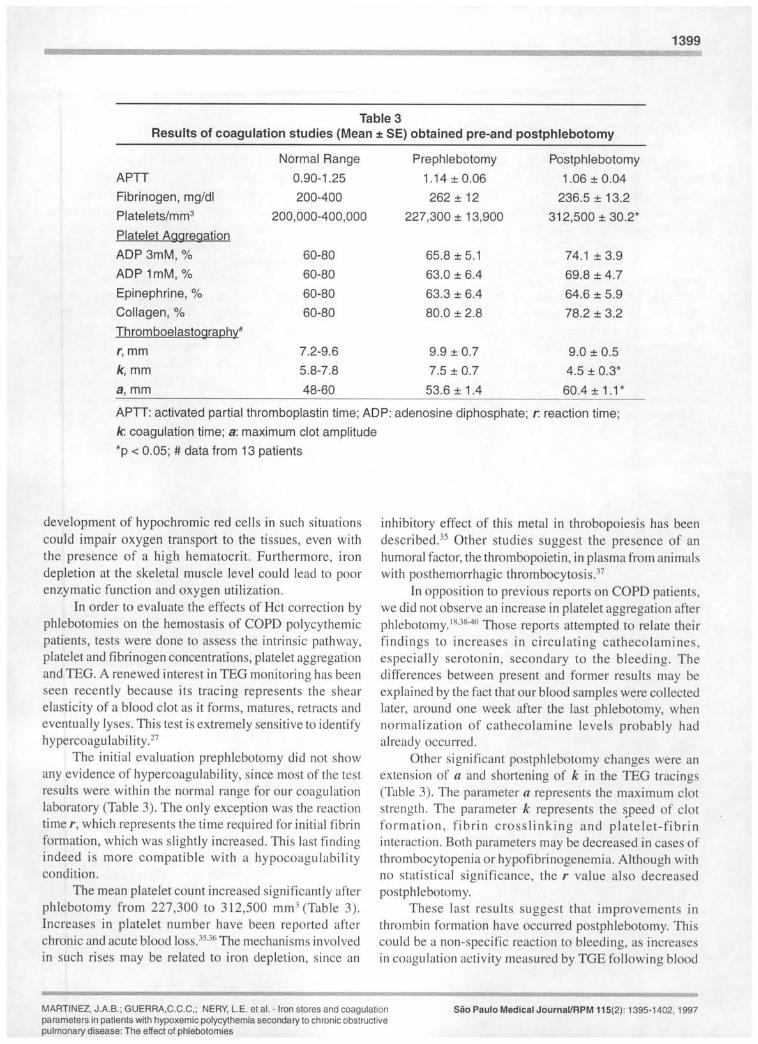
Normal Range Prephlebotomy PostphlebotomyAPTT 0.90-1.25 1.14:t 0.06 1.06 :t 0.04Fibrinogen, mg/dl 200-400 262:t 12 236.5 :t 13.2Platelets/mm3 200,000-400,000 227,300:t 13,900 312,500:t 30.2*Platelet AggregationADP 3mM, % 60-80 65.8 :t 5.1 74.1 :t 3.9ADP 1mM, % 60-80 63.0 :t 6.4 69.8 :t 4.7Epinephrine, % 60-80 63.3 :t 6.4 64.6 :t 5.9Collagen, % 60-80 80.0 :t 2.8 78.2 :t 3.2Thromboelastography#
',mm 7.2-9.6 9.9 :t 0.7 9.0 :t 0.5k,mm 5.8-7.8 7.5 :t 0.7 4.5 :t 0.3*a,mm 48-60 53.6:t 1.4 60.4:t 1.1*
APTT: activated partial thromboplastin time; ADP: adenosine diphosphate; r: reaction time;k coagulation time; a: maximum clot amplitude*p < 0.05; # data from 13 patients
development of hypochromic red ceIls in such situationscould impair oxygen transport to the tissues, even withthe presence of a high hematocrit. Furthermore, irondepletion at the skeletal muscle leveI could lead to poorenzymatic function and oxygen utilization.
In order to evaluate the effects of Het correction byphlebotomies on the hemostasis of COPD polycythemicpatients, tests were done to assess the intrinsic pathway,platelet and fibrinogen concentrations, platelet aggregationand TEG. A renewed interest in TEG monitoring has beenseen recently because its tracing represents the shearelasticity of a blood clot as it forms, matures, retracts andeventuaIIy lyses. This test is extremely sensitive to identifyhypercoagulabi lity. 27
The initial evaluation prephlebotomy did not showany evidence of hypercoagulability, since most of the testresuIts were within the normal range for our coagulationlaboratory (Table 3). The only exception was the reactiontime r, which represents the time required for initiaI fibrinfornlation, which was slightly increased. This last findingindeed is lnore compatible with a hypocoagulabilitycondition.
The mean platelet count increased significantly afterphlebotomy from 227,300 to 312,500 mm3 (Table 3).Increases in platelet number have been reported afterchronic and acute blood 10ss.35.36The lnechanisms involvedin such rises may be related to iron depletion, since an
inhibitory effect of this metal in throbopoiesis has beendescribed.35 Other studies suggest the presence of anhumoral factor, the thrombopoietin, in plasma from animaIswith posthemorrhagic thrombocytosis.37
In opposition to previous reports on COPD patients,we did not observe an increase in platelet aggregation afterphlebotomy.'XJX-40Those reports attempted to relate theirfindings to increases in circulating cathecolamines,especial1y serotonin, secondary to the bleeding. Thedifferences between present and former results lnay beexplained by the fact that our blood samples were collectedlater, around one week after the Iast phlebotomy, whennormalization of cathecolamine leveIs probably hadalready occurred.
Other significant postphlebotomy changes were anextension of a and shortening of k in the TEG tracings(Table 3). The paralneter a represents the lnaximuln clotstrength. The parameter k represents the ~peed of clotforlnation, fibrin crosslinking and platelet-fibrininteraction. Both parameters may be decreased in cases ofthrolnbocytopenia or hypofibrinogenemia. Although withno statistical significance, the r value also decreasedpostphlebotomy.
These last results suggest that improvements inthrombin fonnation have occurred postphlebotomy. Thiscould be a non-specific reaction to bleeding, as increasesin coagulation activity measured by TGE following blood
MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - Iron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructivepulmonary disease: The effect of phlebotomies
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997

1400
losses during surgery have been described.41 Such changeswere documented even 2 hours after surgery and couldhave accounted for cathecolamine releases related to stress,and the entry into circulation of coagulation factors frolnthe hepatic interstitial fluido However, our final coagulationtests were performed about 7 days after the lastphlebotomy, again making this interpretation less probable.Another possibility is that decreased helnatocrits led tofalls in viscosity with better liver perfusion andoxygenation, promoting improvelnent its production ofcoagulation factors.
The increase in a Inay also be related to theen)argement' of the platelet counting. Although thefibrinogen leveIs have not changed, the growth in apostphlebotomy may also be in part secondary to a higheravailability of fibrinogen for the fibrin network making.In high Hct samples, the total alnount of fibrinogen maynot be enough to make a fibrin network capable of stronglycontaining an increased nUlnber of red cells. Low Hctsamples may have proportionally Inore fibrinogen to be
used in the fibrin network, producing clots with greatertexture.
In summary, the coagulation tests made afterphlebotolny have shown slnall changes towards anaugmented coagulability. Such changes could be the resultof an organic reaction to bleeding, especially the increasein platelet counting. Although the precise clinicaI meaningof these findings are unknown, the literature contains areference to a patient with pulmonary artery thrombosisfollowing phlebotomies.42 However, alnong the differenttests done, only k reached a final value out of our normallaboratory range. Therefore, we speculate that the detectedchanges do not represent a harmful thrombotic risk relatedto the phlebotomies
Based in the present results, we do oot think theprophylactic adlninistration of anticoagulant agents afterphlebotomies in COPD patients is necessary. In addition,we recolnmend oral iron supplementation afterphlebotolnies for polycythelnic COPD patients in orderto avoid iron deficiency.
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997 MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - Iron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructive
pulmonary disease: The effect of phlebotomies

REFERENCES
1. Kingler JR, HiU NS. Right ventricular dysfunction in chronicobstructive pulmonary disease. Chest 1991 ;99:715-23.
2. Harrison BDW, Gregory RJ, Clark TJH, ScoU BW. Exchangetransfusion with Dextran 40 in polycythaemia secondary tohypoxic lung disease. Br Med J 1971 ;4:7136.
3. Harrison BDW, Daws J, Madgwick RG, Evans M. The effectsof therapeutic decrease in packed cell volume on theresponses to exercise of patients with polycythaemiasecondary to lung disease. Clin Sci 1973;45:833-47.
4. Wedzicha JA, Rudd RM, Apps MCP, Cotter FE, NewlandAC, Empey DW. Erythrapheresis in patients withpolycythaemia secondary to hypoxic lung disease. Br Med J1983;286:511-4.
5. Dayton LM, McCullough RE, Scheinhorn DJ, Well JV.Symptomatic and pulmonary response to acute phlebotomyin secondary polycythemia. Chest 1975;68:785-90.
6. Bornstein R, Meron D, York E, Sproule B, Zak C. Effects ofvenesection on cerebral function in chronic lung disease. CanJ Neurol Sci 1980;7:293-6.
7. Chetty KG, Brown SE, Light RW. Improved exercisetolerance of the polycythemic lung patient followingphlebotomy. Am J Med 1983;74:415-20.
8. Chetty KO, Light RW, Stansbury DW, Milne N. Exerciseperformance of polycythemic chronic obstructive pulmonarydisease: Effect of phlebotomies. Chest 1990;98: 1073-7.
9. Massaro D, Katz F. Effect of venesection on arterial gasvalues and ventilatory function in patients with chronicbronchitis. Thorax 1965 ;20:441-6.
10. Patakas DA, Christaki PI, Louridas GE, Sproule BJ. Controlof breathing in patients with chronic obstructi ve lung diseaseand secondary polycythemia after venesection. Respiration1986;49:257-62.
11. Rakita L, Gillespie DG, Sancetta SM. The acute and chroniceffects of phlebotomy on general hemodynamics andpulmonary functions of patients with pulmonary elnphysema.Am Heart J ] 965;70:466-75.
12. Segel N, Bishop JM. The circulation in patients with chronicbronchitis and emphysenla at rest and during exercise, withspecial reference to the influence of changes in bloodviscosity and blood volume on the pulmonary circulation. JClin Invest 1966;45: 1555-68.
13. Weisse AB, Moschos CB, Frank MJ, Levinson GE, CannilaJE, Regan T1. Hemodynamic effects of staged helnatocritreduction in patients with stable cor puhnonale and severelelevated hematocrit leveIs. Am J Med 1975;58:92-8.
14. Lieden G. Iron state in regular blood donors. Scand JI-Iaematol.1973;11 :342-9.
15. Propper R, Nathan D. ClinicaI removal of iron. Ann RevMed 1982;33:509-19.
16. Dallman PRo Manifestations of iron deficiency. SeminHematol 1982; 19: 19-30.
17. Schafer AL. The hypercoagulable states. Ann Intern Med1985; 102:814-28.
18. Cordova C, Musca A, Violi F, Perrone F, Alessandri C,Marigliano V, Balsano F. Pathophysiological and clinicaIresearch on the platelet hyperaggregation in patients withchronic respiratory failure. BulI Europ Physiopatol Respir1980;16:113-5.
19. MitchelI RS, Silvers G, Dart GA, Petty TL, Vicent TN, RyanSF, FilIey GF. ClinicaI and morphologic correlations inchronic airway obstruction. Am Rev Respir Dis 1968;97:54-62.
20. Ryan SF. Pulmonary embolism and thrombosis in chronicobstructive emphysema. Am J Pathol 1963;43:767-73.
21. Balsano F, Cordova C, Musca A, Perone A, Violi F. RuolodeI metabolismo pulmonary sull'emocoagulazione infisiologia in clinica ed in terapia. CI Terap 1977;80:513-7.
22. Brun J, Biot N, Perryn-FayolIe M, Sab H. Les troubles de lacoagulation sanguine au cours de I'insuffisance respiratoirecronique: Deductions therapeutiques. Poumon Couer1962;18:181-194.
23. Gaida A, Ghio G. Emocoagulazione e fibrinolisinelI'enfisema polmonare. Minerva Med 1964;55:2122-5.
24. Chanarin L Laboratory haematology: an account of laboratorytechniques, 1st ed. Edinburgh: Churchill Livingstone,1989:274-5.
25. Ratnoff OD, Menzie C. A new method for determination offibrinogen in small samples of plasma. J Lab Clin Med1951 ;37:316-20.
26. Born GVR. Aggregation of blood platelets by adenosinediphosphate and its reversal. Nature 1962; 194:327-9.
27. Spiess BD, DavalIe M. Coagulation monitoring in the surgicalintensive care unit. Crit Care Clin 1988;4:605-20.
28. Milnan N, Pedersen NS, Visfeldt 1. Serum ferritin in healthyDanes: Relation to marrow haemosiderin iron stores. DanMed BulI 1983;30: 116-20.
29. Walters GO, Miller FE, Worwood M. Serum ferritinconcentration and iron stores in normal subjects. J Clin Path1973;26:770-2.
30. Tura S, Pollycove M, Gelpi AP. Erythrocyte and ironkineticsin patients with chronic pulmonary emphysema. J Nucl Med1962;3: 110-25.
31. Shaw DB, Simpson T. Polycythemia in emphysema. Q J Med1961 ;30: 135-52.
32. Stradling JR, Lane DJ. Development of secondarypolycythaemia in chronic airways obstruction. Thorax1981 ;36:321-5.
33. Siimes MA, Refino C, Dallman PRo Manifestations of irondeficiency at various leveIs of dietary iron intake. Am J ClinNutr 1980;33:570-4.
34. Finch CA, Miller LR, Inamdar AR, Person R, Seiler K,Mackler B. Iron deficiency in the rat: Physiological andbiochemical studies of muscle dysfunction .. J Clin Invest1976;58:447-53.
35. Krizsa A. Study on the development of posthaemorrhagicthrombocytosis in rats. Acta Haemat 1971 ;46:228-31.
MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - lron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructivepulmonary disease: The effect of phlebotomies
São Paulo Medicai JournallRPM 115(2): 1395-1402, 1997

1402
36. Karpaktin S, Garg SK, Fredman ML. Role of iron as aregulator of thrombopoiesis.Am J Med 1974;57:521-5.
37. Weintraub A, Khan I, Karpatkin S. A splenie dependentthrombopoietie faetor in ehronie blood loss plaslna. Clin Res1974;22:411A.
38. Cordova C, Musea A, Violi F, Alessandri A, Perrone A,Balsano F. Platelet hyperfunetion in patients with ehronieairways obstruetion. Eur J Respir Dis 1985;66:9-12
39. Musea A, Cordova C, Violi F. The thrombogenie risk inehronie res .ratory failure. Adv Exp Med Bio11984; 164:369-375.
40. Cordova C, Musea A, Perrone A, Violi F, Alessandri C,Marigliano V. Possibile ruolo deIla serotonina neldeterminismo deIla iperaggregazione piastriniea dopo sal assoin pazienti eon insufieienza respiratoria eroniea. CI Terap1979;90:489-501.
41. Tuman KJ, Spiess BD, Me Carthy RJ, Ivankovieh AD. Etfeetsof progressive blood Ioss on eoagulation as measures bythromboelastography. Anesth AnaIg 1987;66:856-63.
42. Chamberlain DA, MilIard FJC. The treatment of polyeythaemiaseeondary to hypoxie lung disease by continuous oxygenadministration. Q J Med 1963;32:341-50.
São Paulo Medicai Journal/RPM 115(2): 1395-1402, 1997 MARTINEZ, J.A.B.; GUERRA,C.C.C,; NERY, L.E. et aI. - lron stores and coagulationparameters in patients with hypoxemic polycythemia secondary to chronic obstructive
nl Jlm()n~ rv rli~A~~A' ThA AffAr.t ()f nhIAh()t()miA~