is medial ridge sign a reliable indicator glenoid bone loss-dr. dhanasekaraprabhu
TRANSCRIPT

Medial Ridge Sign- Is it a reliable indicator of GlenoidBone loss?
Dr. Dhanasekaraprabu, Dr. Aravindh Palaniswamy,
Prof H L Nag, Dr. Vivek Morrey, Dr. Deep Srivastava
All India Institute of Medical Sciences,
New Delhi
Introduction:
• Glenohumeral instability affects approximately 2% of general population and anterior dislocations occuring 95% TO 98% of the time1.Recurrent shoulder instability is a major problem among athletes and the young adult population.
• Anterior shoulder dislocation is more common than the posterior shoulder dislocations and the recurrence of shoulder dislocations is increased in the young adults and also in athletes.
• The recurrence rates following the primary dislocation in patients who were less than 20 years old was almost 90%2.
• The management of recurrent anterior shoulder instability has been mainly surgical and bankart’s repair is the gold standard. Recently the trend towards arthroscopic bankart’s repair is on the rise3
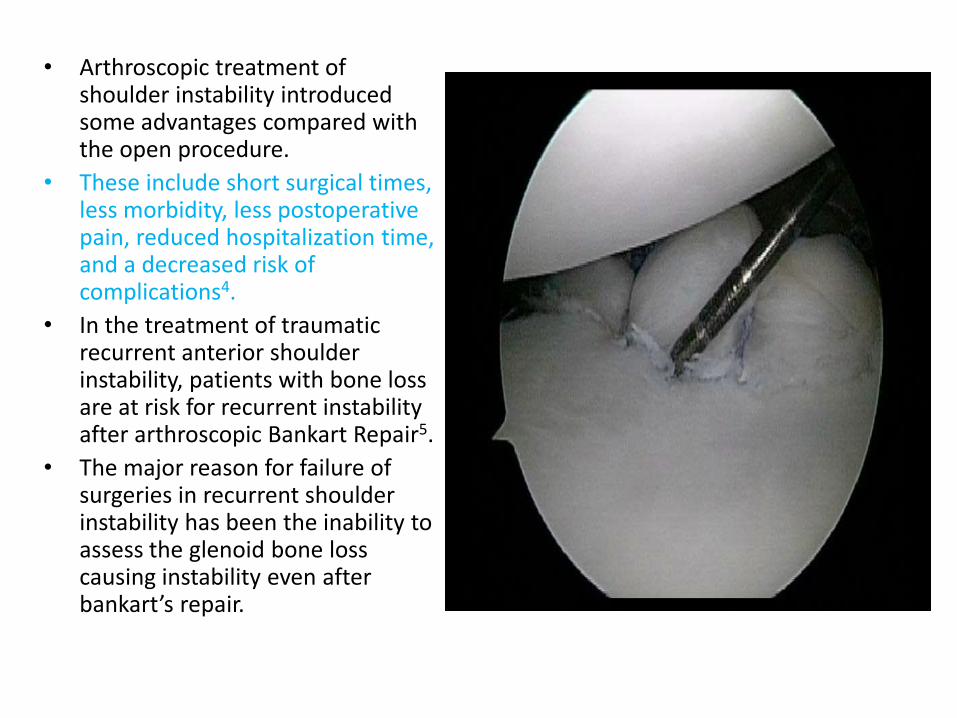
• Arthroscopic treatment of shoulder instability introduced some advantages compared with the open procedure.
• These include short surgical times, less morbidity, less postoperative pain, reduced hospitalization time, and a decreased risk of complications4.
• In the treatment of traumatic recurrent anterior shoulder instability, patients with bone loss are at risk for recurrent instability after arthroscopic Bankart Repair5.
• The major reason for failure of surgeries in recurrent shoulder instability has been the inability to assess the glenoid bone loss causing instability even after bankart’s repair.
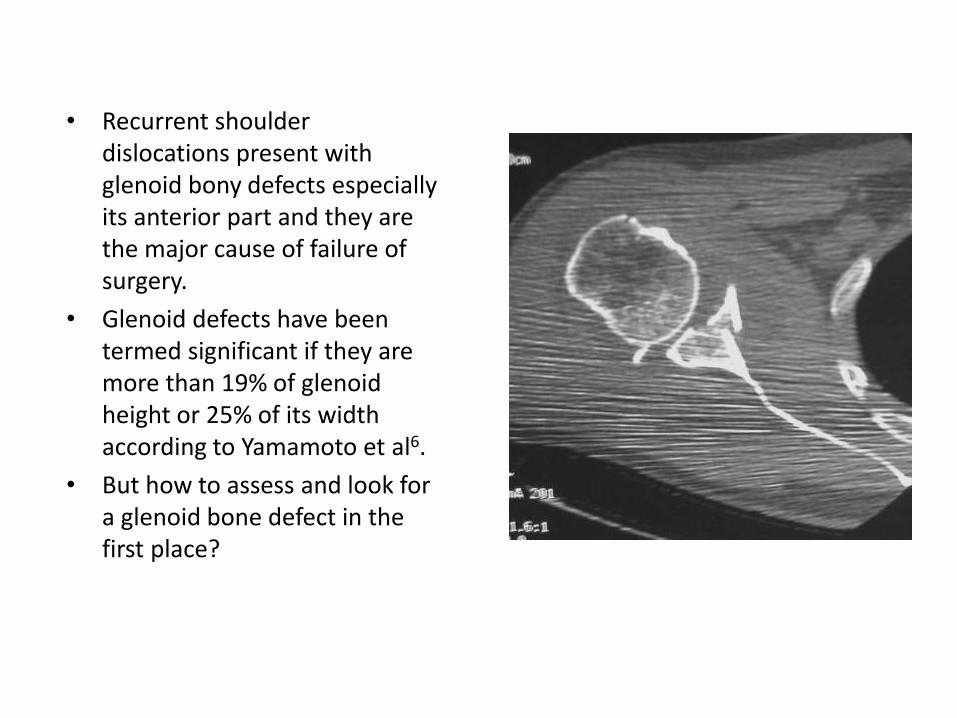
• Recurrent shoulder dislocations present with glenoid bony defects especially its anterior part and they are the major cause of failure of surgery.
• Glenoid defects have been termed significant if they are more than 19% of glenoidheight or 25% of its width according to Yamamoto et al6.
• But how to assess and look for a glenoid bone defect in the first place?
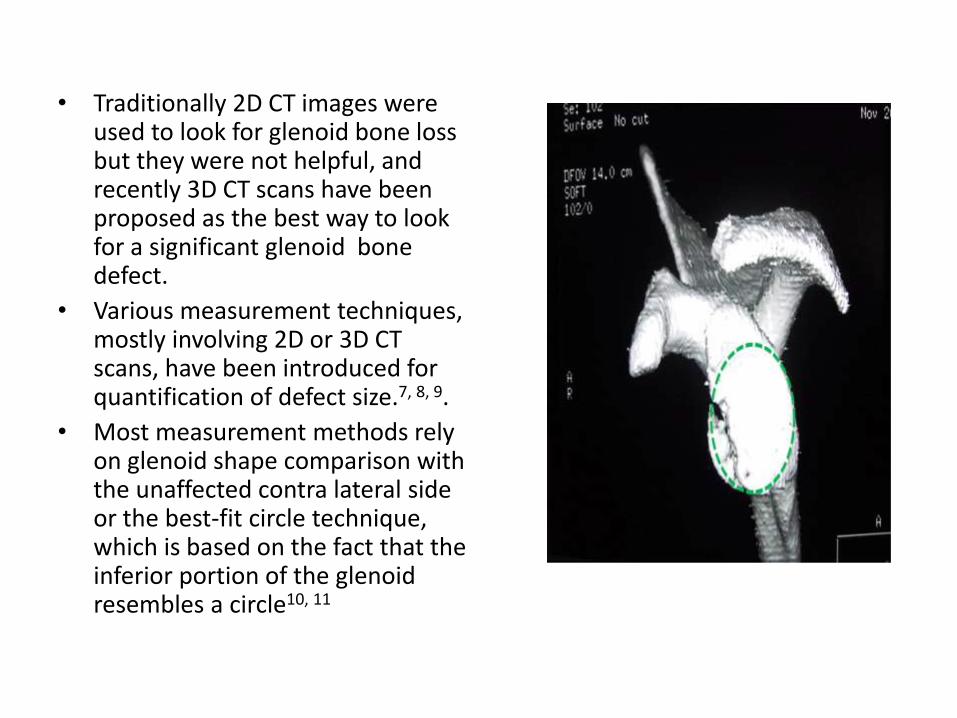
• Traditionally 2D CT images were used to look for glenoid bone loss but they were not helpful, and recently 3D CT scans have been proposed as the best way to look for a significant glenoid bone defect.
• Various measurement techniques, mostly involving 2D or 3D CT scans, have been introduced for quantification of defect size.7, 8, 9.
• Most measurement methods rely on glenoid shape comparison with the unaffected contra lateral side or the best-fit circle technique, which is based on the fact that the inferior portion of the glenoidresembles a circle10, 11
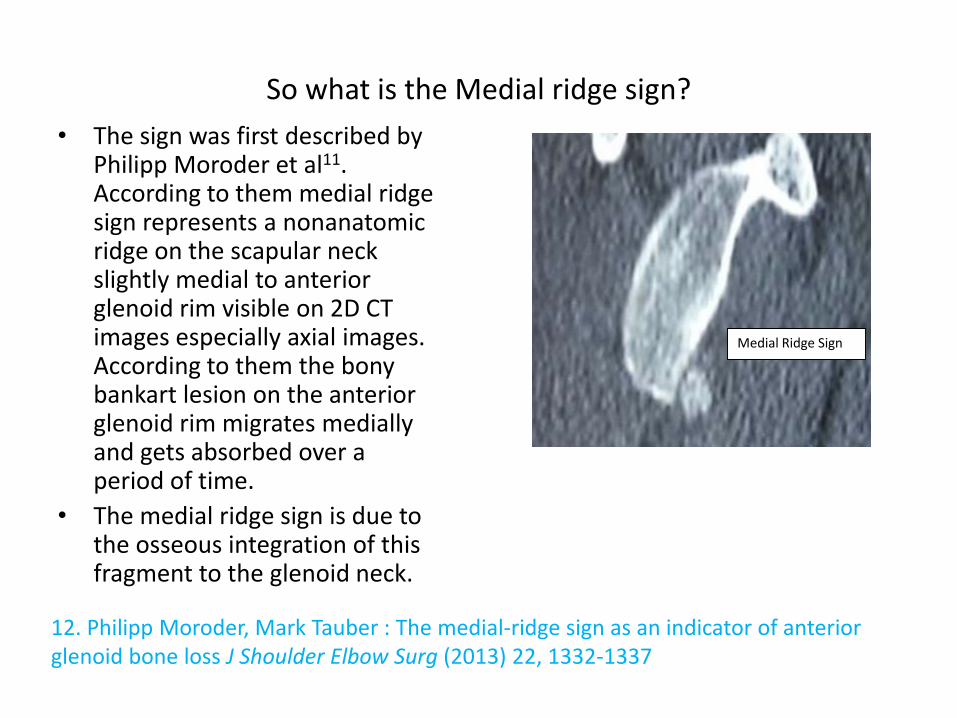
So what is the Medial ridge sign?
• The sign was first described by Philipp Moroder et al11. According to them medial ridge sign represents a nonanatomicridge on the scapular neck slightly medial to anterior glenoid rim visible on 2D CT images especially axial images. According to them the bony bankart lesion on the anterior glenoid rim migrates medially and gets absorbed over a period of time.
• The medial ridge sign is due to the osseous integration of this fragment to the glenoid neck.
Medial Ridge Sign
12. Philipp Moroder, Mark Tauber : The medial-ridge sign as an indicator of anterior glenoid bone loss J Shoulder Elbow Surg (2013) 22, 1332-1337

The Medial Ridge sign demonstrated on a 3D CT scan

• The goal of this study was to look for medial ridge sign in patients with recurrent shoulder dislocations and find out whether the sign was useful in assessing the percentage of bone loss in such patients.
• We wanted to find out if the medial ridge sign was helpful in pointing to patients with significant glenoid bone loss so that a decision for arthroscopic bankart’s vs bone augmentation procedure may be made in these patients.
Goals of our study:

Materials and Methods:
• The study was conducted at our institution. 35 patients with unilateral recurrent anterior instability of shoulder were evaluated with Computer tomography preoperatively before undergoing definitive surgical procedure.
• Study Design : Observational Study
• The patients who were included in the study were 15-40 years old, and had more than one episode of dislocation.
• Patients with habitual dislocation and bilateral dislocations were excluded from the study.
• The patients enrolled in the study were subjected to a 3D CT of bilateral shoulder with arms by the side of the chest wall.

• CT films were acquired in MDCT scanners (Somatom sensation, Siemens, Erlanger, Germany) with a volume data acquisition of 0.6 X 40, slice thickness of 0.6 mm.
• The scanning plane extended from the acromion to just below the glenoid following which 3D volume rendered standardized images were reconstructed and then en face view of the glenoid cavity was obtained after subtracting the humeral head.
• On en face view of the glenoid a line was drawn along the long axis of the glenoid and a second line was drawn perpendicular to the long axis of glenoid at the inferior glenoid from the posterior margin to the anterior margin and was calculated as the width of the glenoid (glenoid index) in millimetres. It was also then calculated in the contralateralnormal side.
• Percentage of bone loss was calculated using the formula [ (D-d)/D] x 100.
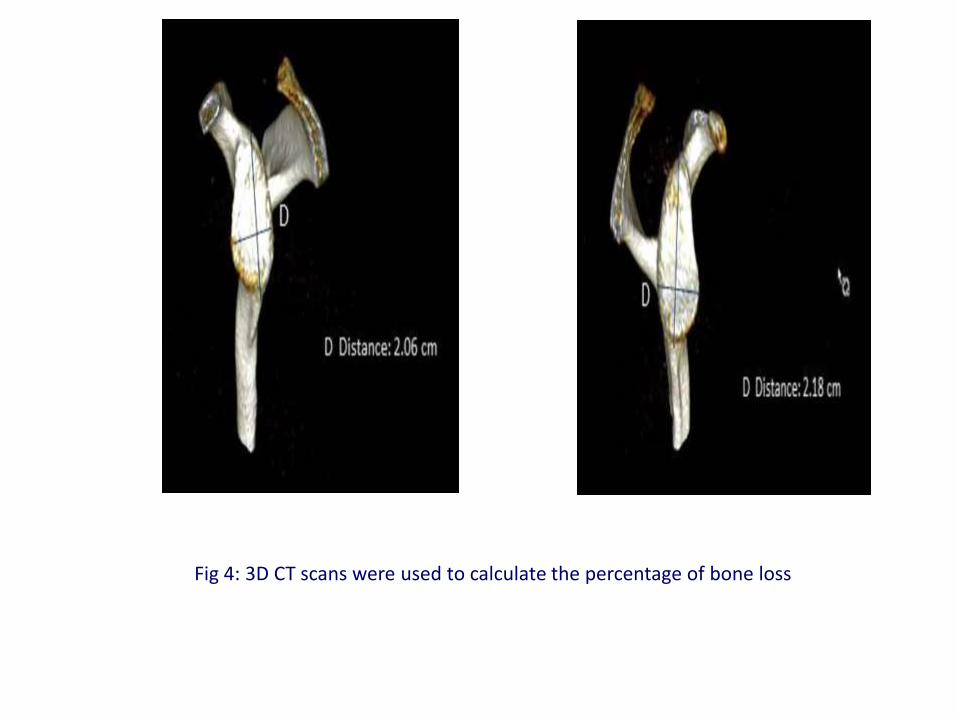
Fig 4: 3D CT scans were used to calculate the percentage of bone loss
Results:
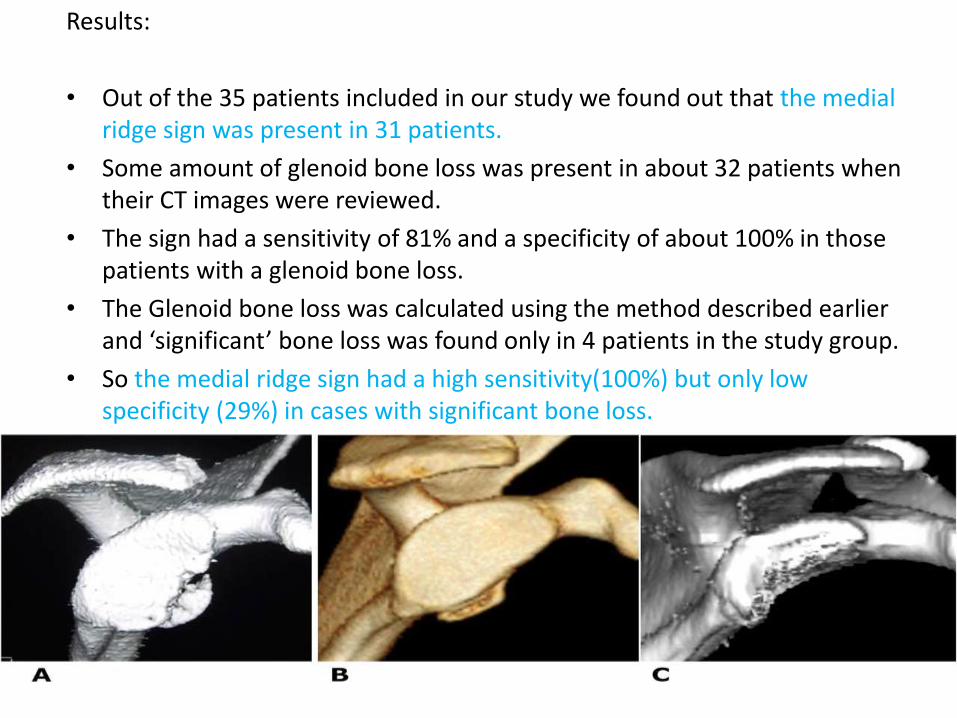
• Out of the 35 patients included in our study we found out that the medial ridge sign was present in 31 patients.
• Some amount of glenoid bone loss was present in about 32 patients when their CT images were reviewed.
• The sign had a sensitivity of 81% and a specificity of about 100% in those patients with a glenoid bone loss.
• The Glenoid bone loss was calculated using the method described earlier and ‘significant’ bone loss was found only in 4 patients in the study group.
• So the medial ridge sign had a high sensitivity(100%) but only low specificity (29%) in cases with significant bone loss.

Discussion:
• One of the most common surgical procedures performed for recurrent shoulder instability is Bankart’s repair and
• An Important cause of failure of arthroscopic surgery in the condition is glenoid bone loss5.
• As we had already mentioned even though various authors differ on the estimates of “significant” glenoid bone loss the consensus seems to be about 25% of the glenoidsurface6.
• CT scans are more sensitive in picking up the bony defects than MRI or routine radiography13.
• 3D CT scans were in fact more accurate in predicting bone loss than 2D CT scans 13
• However the glenoid bone loss is not routinely measured on the CT scans preoperatively leading to underestimating the amount of glenoid loss resulting in failure of surgery.
• Various methods have been developed that estimate the glenoidbone loss on CT scans as we had mentioned earlier including comparing it with the contralateralside and also the best fit technique10,
11

• The medial ridge sign was described by Philipp Moroder et al12 after the analysis of CT scans of patients with recurrent shoulder instability and they propose it as a indicator of anterior glenoid bone loss in their study
• But as our results point out the medial ridge sign even though present in cases with anterior glenoid bone loss was not specific enough to pick up cases with significant bone loss in which there is a difficulty in making a clinical decision

• Hence even though the medial ridge sign may be present in cases of recurrent shoulder instability, it will not help the surgeon in choosing a bone augmentation procedure over the routine bankart’sprocedure.
• The medial ridge sign is just an indicator of glenoid bone loss and eventually 3D CT scans need to be analysed and the loss measured. And when the loss is found to be significant the surgeon may decide upon the need for a bone augmentation procedure lessening the chances of failure in the post op period.
References:
1.Zacchilli MA, Owens BD. Epidemiology of shoulder dislocations presenting to emergency departments in the united states. J Bone Joint SurgAm 2010;92(3):542-9
2. Mclaughlin HL, Cavallaro WU: Primary anterior dislocation of the shoulder, Am J Surg 80:615, 1950
3. Owens BD, Harrast JJ : Surgical trends in Bankart repair: an analysis of data from the American Board of Orthopaedic Surgery certification examination, Am J Sports Med. 2011 Sep;39(9):1865-9
4. Green MR, Christensen KP. Arthroscopic versus open Bankart procedures: a comparison of early morbidity and complications. Arthroscopy 1993;9:371-374.
5. Risk factors for recurrence of shoulder instability after arthroscopic Bankart repair. Boileau P , Villalba M J Bone Joint Surg Am. 2006 Aug;88(8):1755-63.
6. Yamamoto N, Muraki T, Sperling JW, Steinmann SP, Cofield RH, Itoi E, et al. Stabilizing mechanism in bone-grafting of a large glenoid defect. J Bone Joint Surg Am 2010; 92:2059-66. http://dx.doi.org/ 10.2106/JBJS.I.00261
7. Baudi P, Righi P, Bolognesi D, Rivetta S, Rossi Urtoler E, Guicciardi N, et al. How to identify and calculate glenoid bone deficit. Chir OrganiMov 2005; 90:145-52.
8. Chuang TY, Adams CR, Burkhart SS. Use of preoperative three dimensional computed tomography to quantify glenoid bone loss in shoulder instability. Arthroscopy 2008; 24:376-82. http://dx.doi.org/ 10.1016/j.arthro.2007.10.008
9. Dumont GD, Russell RD, Browne MG, Robertson WJ. Area-based determination of bone loss using the glenoid arc angle. Arthroscopy 2012; 28:1030-5. http://dx.doi.org/10.1016/j.arthro.2012.04.147
10. Huysmans PE, Haen PS, Kidd M, Dhert WJ, Willems JW. The shape of the inferior part of the glenoid: a cadaveric study. J Shoulder Elbow Surg 2006; 15:759-63.
11. Jeske HC, Oberthaler M, Klingensmith M, Dallapozza C, Smekal V, Wambacher M, et al. Normal glenoid rim anatomy and the reliability of shoulder instability measurements based on intrasite correlation. Surg Radiol Anat 2009; 31:623-5.
12. Philipp Moroder, Mark Tauber : The medial-ridge sign as an indicator of anterior glenoid bone loss J Shoulder Elbow Surg (2013) 22, 1332-1337
13. Rerko MA, Pan X, Donaldson C, Jones GL, Bishop JY. Comparison of various imaging techniques to quantify glenoid bone loss in shoulder instability. J Shoulder Elbow Surg 2013;22:528-34
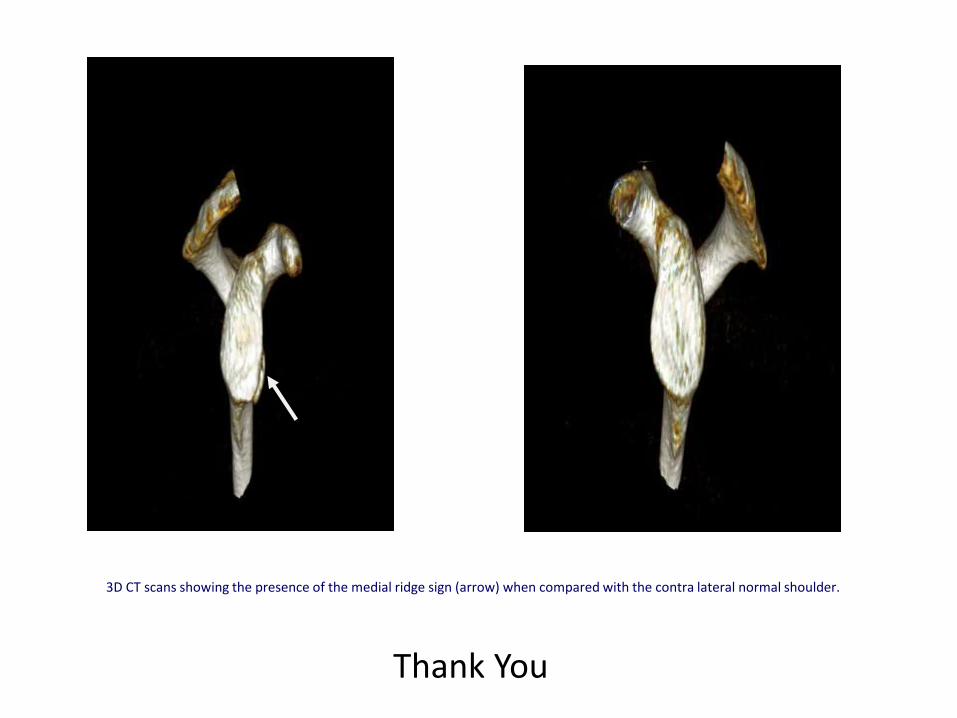
3D CT scans showing the presence of the medial ridge sign (arrow) when compared with the contra lateral normal shoulder.
Thank You