isbn 978-1-85433-764-1 - bps.org.uk of... · engagement with services. ... ‘the diagnosis of...
TRANSCRIPT

April 2018
Communicating a diagnosis of dementiaSusan Watts, Rose McCabe & Reinhard Guss
Faculty of the Psychology of Older People
Incorporated by Royal Charter Registered Charity No 229642 REP117/03.18
The British Psychological SocietySt Andrews House, 48 Princess Road East, Leicester LE1 7DR, UKTel: 0116 254 9568 Fax 0116 247 0787 E-mail: [email protected] Website: www.bps.org.uk
9 781854 337641
ISBN 978-1-85433-764-1

ii
If you have problems reading this document and would like it in a different format, please contact us with your specific requirements.
Tel: 0116 252 9523; E-mail: [email protected].
© The British Psychological Society 2018
All rights reserved. No part of this report may be reprinted or reproduced or utilised in any form or by any electronic, mechanical, or other means, now known or hereafter invented, including photocopying and recording, or in any information storage or retrieval system, without permission in writing from the publishers. Enquiries in this regard should be directed to the British Psychological Society.
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library.
ISBN 978-1-85433-764-1
Printed and published by The British Psychological Society St Andrews House 48 Princess Road East Leicester LE1 7DR www.bps.org.uk

1
Contents
Authors ................................................................................................................................. 2
Key messages ........................................................................................................................ 3
Introduction ......................................................................................................................... 5
Context ................................................................................................................................. 7
Sharing the diagnosis ........................................................................................................... 9
Best practice in communicating a dementia diagnosis ...................................................... 15
Conclusions .......................................................................................................................... 21
References ............................................................................................................................ 27

2
Authors
Susan Watts, Clinical Psychologist, Former Head of Psychology for Older People, Greater Manchester West Mental Health Foundation Trust.
Rose McCabe, Professor of Clinical Communication, University of Exeter Medical School.
Reinhard Guss, Consultant Clinical Psychologist, Kent & Medway NHS and Social Care Trust.
The front cover of this document features artwork by John Williams. John is an artist living in Liverpool. He has painted all of his life; it has been a passion for him and forms a big part of his self- identity. He was diagnosed with Alzheimer’s type dementia in 2014 but continued painting. John feels that his painting style changed after his diagnosis and that the dementia increased his creativity and ability to express himself freely

3
Key messages
■ There has been substantial progress across the UK in increasing the numbers of people receiving a diagnosis of dementia and reducing the time this takes, but less attention has been paid to some other aspects of the process.
‘The government drive to get everybody diagnosed emphasises quantity over quality. It’s like getting people through a sausage maker!’
(FPOP Consultation with people living with dementia in the UK: Guss et al.; 2014)
■ Communicating about a dementia diagnosis is only one aspect of a communicating strategy which needs to span the entire process from referral through assessment, post-diagnostic support and treatment.
■ People have the right to choose whether or not they receive a diagnosis, some people make an informed choice ‘not to know’.
■ Sharing a life-altering diagnosis is inevitably difficult for the person with dementia and the family, so communicating the diagnosis well is very important. Health care professionals (HCPs) can underestimate the difficulties people experience and should be aware that:
– Bad communication can be distressing and impact on subsequent wellbeing and engagement with services.
– Needs at diagnosis sharing differ, requiring personalisation of sessions and information materials appropriate to the person’s needs.
– Recall of any medical consultation is limited. People with dementia can manage less information dependent on the extent of problems, but also on the degree of their distress.
– People may not express the extent of their distress during a consultation about the diagnosis.
– A sensitive balance is needed between excessively optimistic information with use of euphemisms in place of diagnostic terms and too much negative information about longer-term prognosis.
– The language should be sensitive, non-stigmatising and jargon free.– Whilst individuals with a learning disability should be consistently supported
to make sense of the changes they are experiencing, this may not necessarily involve using the word dementia but should instead be tailored to individual understanding.
– The presence of a familiar HCP during diagnosis sharing is important for most people.
■ An individualised process of diagnosis sharing over a period of time, may seem problematic in the context of limited resources, but may be more efficient through avoidance of distress, improvement in engagement and longer-term outcomes.
■ Diagnosis can be straightforward, and be arrived at swiftly. However, it may be complex and involve periods of uncertainty for the individual and family, despite a thorough memory clinic assessment. This uncertainty about diagnosis also has the potential to be very stressful for the person and family/carers.

4
■ Whether for idiosyncratic reasons, or as a direct result of the nature of the person’s dementia, some people may not be willing to take part in the process of investigation and diagnosis at an early or mid-stage of the condition. Consideration should also be given to the support, communication and information needs of the family and carers.
■ Clinical psychologists have specialist knowledge around the communication, understanding, emotional and family process which impact on sharing a diagnosis. These include direct clinical work, clinical advice, skills development and supervision.
■ The task of sharing a diagnosis is also difficult for staff. Skills training, including in the understanding of the psychological impact of diagnosis, together with supportive supervision are needed, to which clinical psychology can make an important contribution.
■ Clinical psychologists have evaluation and research skills which can help services monitor the effectiveness of communication processes but also develop models to research and understand the process of sharing a diagnosis.
■ This document offers practical suggestions about good practice guidelines and updates existing guidance with a checklist to help support a personalised approach to sharing the diagnosis.

5
Introduction
This paper is part of a suite of documents: Clinical Psychology in the Early Stage Dementia Care Pathway (2014), which has been produced by the Faculty of the Psychology of Older People (FPOP), Division of Clinical Psychology (DCP), British Psychological Society (BPS). These papers address issues around the early stages of dementia in adults and focus on the following specific topics: Pre-assessment Counselling, Cognitive Assessment, and Post-diagnostic Support, and are accompanied by a paper summarising the views of people living with dementia (FPOP Consultation).
The focus of this paper is on issues around sharing a diagnosis of dementia with the person with dementia and the family. However, communicating the diagnosis cannot be viewed in isolation from more general communication about the entire assessment process, so this paper is best understood in conjunction with the rest of the suite of documents. It is part of the wider communication, commencing from the first stages of discussion with Primary Care Practitioners and other referral agents.
‘The diagnosis of dementia is a shared responsibility between generalist and specialist disciplines. Primary care physicians should explore patients’ ideas and concerns around their symptoms prior to referral and tentatively discuss possible diagnoses.’
Iliffe et al. (2009).
Diagnosis sharing is also influenced by any pre-diagnostic counselling (La Fontaine et al., 2014) and is dependent upon clarity about the assessment and the consequences of diagnosis at each stage of the process. Neither can communication about a dementia diagnosis be separated from any subsequent pharmacological and non-pharmacological treatment and support processes. This is not only because mutual communication and understanding is essential to support engagement with treatment and long-term management (Husband, 2009; Moniz-Cook, 2009), but also because diagnosis without a meaningful treatment or management strategy may be counter-productive and distressing (Iliffe & Manthorpe, 2004; Manthorpe et al., 2010). Thus, it may be helpful for readers to review this information in conjunction with guidance around other stages of diagnosis (Clinical Psychology in the Early Stage Dementia Care Pathway, Guss & colleagues, 2014).
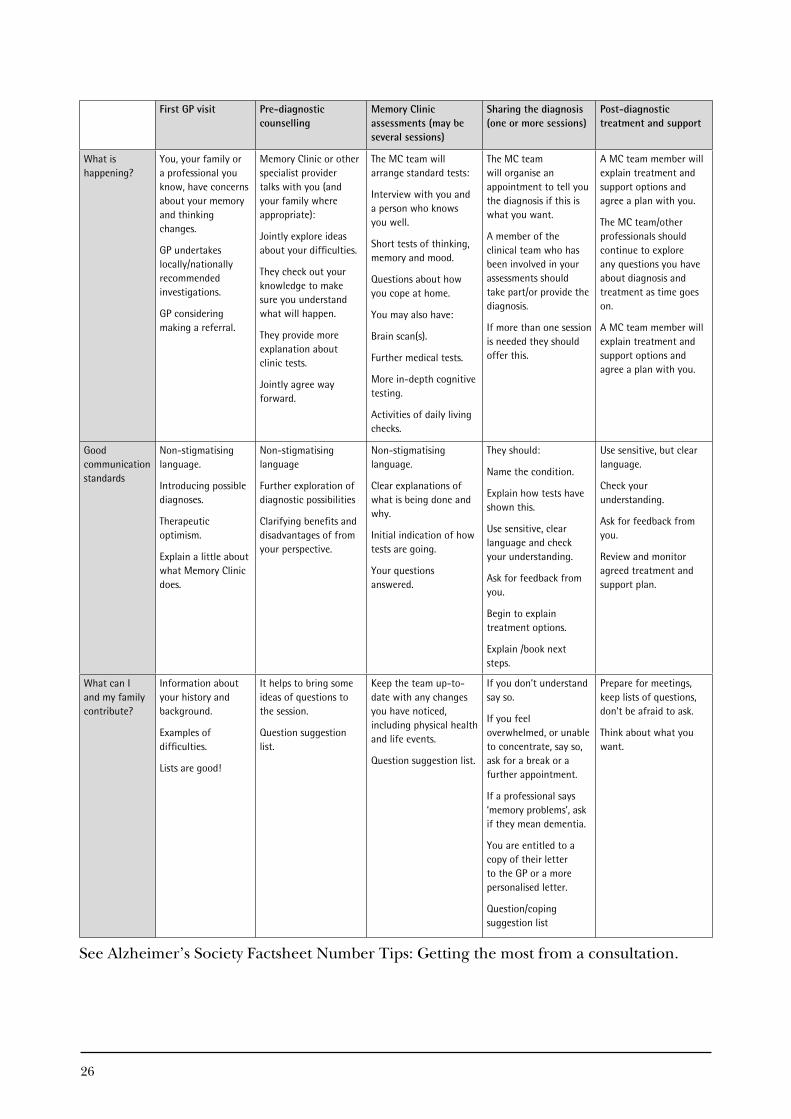
Communication about the diagnosis is often described as though it is a single event. Whilst in most cases there will be an initial meeting between professional(s) and the person with dementia (often together with family or friends) to share the diagnosis, continued understanding and transitional adjustment will continue over a period of time and needs informed, skilled support. See Table opposite for a brief illustration of the communication issues throughout the typical dementia care pathway which will impact on effective diagnosis sharing. A recognition of this communication as an ongoing process is particularly important when sharing the diagnosis with a person who has a learning disability, for whom this typical pathway opposite may be less applicable.

A number of specific issues around diagnosis sharing are not covered here. The document does not address issues related to diagnosis sharing where there is a major genetic component (e.g. Huntington’s disease, genetic frontotemporal dementia), where health implications for other family members will be extremely important (see Antoine & Pasquier, 2013).
The focus of this paper and the associated suite is on early stages of dementia. As such it is outside the scope of this paper to cover issues around Mental Capacity, Safeguarding and Best Interests as they relate to the communication of dementia diagnoses, although these will inform practice where appropriate.
6
Point of referral(GP or other)
Pre-diagnostic counselling
Assessmentby Memory Clinic or related service
Diagnosis-sharing session
Post-diagnostic treatment and support
Initial introduction and discussions about possible diagnoses
Pre-diagnostic counselling (see paper)
Effective explanation of investigations and findings during course of assessment
Well planned and skillful session(s) covering diagnosis, taking account of perspective of person with dementia and family context
Follow-up support to develop understanding and engagement with treatment and management options
Table: Typical Early Stage Dementia Care Pathway: Factors which increase the likelihood of successful diagnosis sharing.

7
Context
There is a current emphasis on the importance of making and sharing an early diagnosis with people with dementia and, where appropriate, their families. The Alzheimer’s Society (2014) campaign: the ‘Right to Know’ promotes this approach. However, it is also the case that people have an equal right not to know a diagnosis, if that is their choice (Nuffield Council on Bioethics, 2009). This emphasis on diagnosis sharing is explicit in the policy documents of the four UK Nations. These include:
England: Prime Minister’s Challenge on Dementia (DH, 2012, 2013); Unlocking Diagnosis (All-Party Parliamentary Group on Dementia, 2012) Case
for change – memory services for people with dementia: evidence (DH, 2011). Northern Ireland: Improving Dementia Services in Northern Ireland – A Regional Strategy,
(Department of Health, Social Services and Public Safety, 2011) Scotland: Scotland’s National Dementia Strategy (The Scottish Government 2013) Charter of Rights for People with Dementia and their Carers in Scotland (Cross
Party Group on Alzheimer’s 2009) Wales: The National Dementia Vision for Wales, Dementia Supportive Communities
(Welsh Assembly Government 2011)
The Scottish Dementia Charter of Rights explicitly addresses empowerment and the enablement of participation for people with dementia and their carers, for which high quality communication about a dementia diagnosis is fundamental.
There is a widespread consensus within much of the literature, that early diagnosis is the way forward (e.g.Waldemar et al., 2007; Prince et al., 2011), though there is also an acknowledgement that public knowledge of the condition needs to increase, and the stigma of dementia also needs to be addressed. Nevertheless, this approach is still contentious, with some commentators raising continuing concerns for a number of reasons. Firstly, the benefits, disadvantages and potential risks for the individual are queried, (see Le Couteur et al.; 2013; Benbow et al.; 2013, for a riposte; and Antoine & Pasquier, 2013). Secondly, the quality of the process of sharing the diagnosis, providing follow-up and post-diagnostic support has been queried, raising concerns about the potential negative impact on the person with dementia and the family (see: Iliffe & Manthorpe, 2004; Milne, 2010; Manthorpe et al 2010; 2013; Samsi et al., 2014).
The UK has seen a major growth in memory clinics and associated services over recent years, and the percentages of people with a dementia diagnosis have been increasing in line with National targets for the identification of people with dementia by health district. Commissioning guidance (e.g. Department of Health, 2011), and clinical standards (Royal College of Psychiatrists, 2014; Memory Services National Accreditation Programme) specify tight time frames for the process from referral by the GP to the stage of sharing the diagnosis with the person and/or family and carers. Specific guidance to inform the

8
process with people with a learning disability is also available BPS/RCPsych (2015). Whilst it is acknowledged in these key documents that the diagnosis should be communicated well, there is little guidance about how this should be done or by whom, nor what training, skills and support are required. Given the numbers of people with possible dementia and the volume of work the investigation and diagnosis process represents, it is particularly pertinent to address these issues. All the more so, as the life-changing nature of the diagnosis combined with the cognitive problems inherent in the condition, mean that sensitivity and clarity are essential. Moreover, particular attention needs to be paid to situations where the individual with the diagnosis may not communicate verbally, or may have a pre-existing cognitive impairment for example due to a learning disability (Tuffrey-Wijne & Watchman, 2014).
Historically, most dementia diagnosis has been undertaken by specialist services. However, health and social care provision for dementia are evolving and options for dementia diagnosis in primary care are also being explored and developed at present. The staffing and specialist skills mix required to undertake this work will need to be considered to ensure good quality communication of the diagnosis.

9
Sharing the diagnosis
Definitive research about the experience of diagnosis sharing in dementia is problematic. In-depth interview studies have involved fairly small numbers of participants, and self-report by professionals, individuals with dementia and their families in questionnaires and surveys may be affected by recall, social desirability and other factors. Ongoing research in the ShareD (Shared Decision Making in Mild to Moderate Dementia) Study by McCabe et al. (2015) has used video-recorded psychiatrists and geriatricians sharing a diagnosis of dementia with individuals and their family members in memory clinics. This methodology has the potential to increase our understanding of a difficult area of clinical practice, although there may be some limitations as participants who have volunteered may not be fully representative of people with dementia or of professionals working in these services. To date, 81 diagnostic interviews have been micro-analysed using conversation analysis. In this study, the doctors always named dementia, addressed the person with dementia and attempted to elicit people’s understanding of the diagnosis (Dooley et al., 2015). In focus groups, doctors working in memory clinics have identified some of the challenges in delivering a diagnosis of dementia (Bailey et al., 2016). They highlight the delicate balance between honesty and hope in delivering diagnostic and prognostic information, together with difficulties providing personalised care and continuity within systemic constraints. For example, many doctors may be meeting the person for the first time when they share the diagnosis.
Skilled and sensitive practice in sharing a diagnosis is important. Unfortunately, people with dementia and their families, report mixed experiences, from very positive through to very negative, in how well this is done, including problems with how the communication of the diagnosis is undertaken. (Lecouturier et al., 2008; Manthorpe et al., 2010; 2013; Samsi et al., 2014; Memory Services National Accreditation Programme – MSNAP Third National Report, 2013–14; 2015). A survey of 400 people affected by dementia by the Alzheimer’s Society (2014) was widely reported in the media, as 90 per cent of those surveyed described dissatisfaction with the amount of information and support available post diagnosis and there were many reports of insensitive consultations. So it is particularly pertinent to review the research evidence, together with other accounts of the experience of diagnosis sharing from the perspective of people with dementia and families.
Generic guidance on sharing a diagnosis:Communication about the diagnosis of any life changing illness has long been recognised as difficult for both the person with dementia and the clinical practitioner. This process has often been called ‘breaking bad news’. However, this term itself has become controversial due to concerns that it colours the nature of the communication. It has been suggested that the term implies a single event, rather than a process, does not reflect the reciprocal nature of communication between the person with dementia, the family and the professional, and sets an overly pessimistic tone. Equally, it needs to be recognised that communication about a dementia diagnosis needs to use language in a way that conveys the serious nature of the condition in an effective way, to avoid any misunderstanding. Generally, the terms sharing the diagnosis and communicating a diagnosis have been used in this document.

10
Generic guidelines and models suggest the following: identifying the person’s knowledge and wishes; addressing the communication skills needed by professionals; and the importance of integrating the diagnosis sharing with subsequent planning and support (e.g. Buckman, 1992; Silverman et al., 1998; Baile et al., 2000). However, these models were principally designed for use in physical health conditions, such as oncology, where the contextual issues are very different. There is much less involvement of family and friends in the assessment process and additional needs to adapt communication to cognitive needs are usually more minor. Some progress has been made in adapting these models for the transition to a diagnosis of dementia (e.g. Pratt & Wilkinson, 2003; Steeman et al., 2006) and include recognising the impact of social and family context and cognitive changes on the person’s ability to engage with diagnosis sharing. These models still have some limitations, which affect their utility to direct the practice of the Health Care Professionals (HCPs) tasked with sharing diagnoses, but research, described later, has identified a range of more specific issues to consider in preparing for, and sharing, a diagnosis.
Issues affecting recall of any medical consultationThere is a well-established literature documenting a gap between the information that HCPs have or think they have covered during a medical appointment about any kind of condition and the amount and type of information actually recalled by patients and families. A range of studies of different treatment groups have found that 40–80 per cent of what is said is forgotten. Ley’s research and publications (e.g. Ley, 1979; 1985; 1988) initially documented the scale of this problem. He proposed a simple model describing the relationship between patients’ memory and understanding of a medical consultation and subsequent treatment adherence and satisfaction with care.
Kessels (2003) provided a useful review, which has more applicability to sharing a dementia diagnosis. This combines the general literature on recall of medical consultations with cognitive and psychological research investigating the impact on memory of factors such as ageing, stress and anxiety, and the nature of the diagnosis and treatment message itself. Examples of the factors he identified include:
■ Cognitive changes associated with ‘normal’ ageing impact on recall, with some aspects of memory better preserved than others.
■ Attentional narrowing – when the patient focuses on a central message, such as the name of the diagnosis, limiting capacity to concentrate on other information, (which may be about important treatment options or next appointments).
■ State dependent learning – for example, when the person learns something whilst in an anxious state in a clinic consultation, but the recall for this at home, when more relaxed, is likely to be poor.
■ Both high and low levels of anxiety have adverse effects on memory, with moderate anxiety being associated with optimal recall.
■ A ‘worried’ demeanour on the part of the HCP can foster anxiety and mean that patients recall less. This is also consistent with views expressed by people taking part in the FPOP consultation with people living with dementia in the UK (Guss et al., 2014) that language use needs to be considerate and sensitive when sharing the diagnosis.
11
‘Be sensitive. Never be dramatic. For example, do not use terms like “I am afraid to tell you…”’(FPOP Consultation, 2014)
■ Research has also explored the effect of using different media to support the session. Generally, a traditional spoken consultation is not recalled well. Written information can be helpful for people with reasonable literacy, if it is their first/preferred language and specific to their circumstances. Using the exact language used in the session in the written information will avoid confusion.
‘I got a long letter from my psychologist. It was very personal and human. This is what I needed.’(FPOP Consultation, 2014)
■ For others, visual representations of information may help. For example, there is some evidence that pictographs and cartoons can improve correct recall of medical information. (see Kessels, 2003, for details.)
Research and a variety of guidance covering good practice in communicating with patients has been available for more than 20 years, but there is continuing evidence that the practice of HCPs in all medical specialties still underestimates the gap between information offered by the professional and the amount recalled and understood by patients. Clearly, there are particular problems when the patient is a person with a dementia, and will have some combination of specific memory, language or reasoning changes for which the HCP needs to adapt communication skills further.
Issues specific to sharing a diagnosis of dementiaThe diagnosis of dementia covers a range of conditions, with different symptoms. Investigation is complex, especially in the early stages of the condition. It differs from many other illnesses for which guidance on diagnosis sharing was originally developed for a number of reasons:
1. The information gathering process involves collecting a detailed clinical history from the person and from family, friends or other carers. As Manthorpe et al., (2010) noted, there are often differences between the perceptions of the person with dementia and their family about the nature and extent of memory, cognitive and other problems. How these discrepancies are handled by professionals during joint meetings can impact on acceptance, adjustment and ongoing family relationships.
2. A variety of cognitive and physical health investigations are involved. However, none of these are fully definitive tests for dementia, so diagnosis always involves a degree of clinical judgement.
3. Sharing a diagnosis of dementia should also be understood to mean sharing the subtype diagnosed, wherever appropriate to the person’s level of understanding. Differential diagnoses can be important in explaining the problems the person is experiencing and the different longer-term implications. Without this information it would be difficult for the person to make informed choices about their future.
4. In early stages, the clinical team may be able to identify cognitive impairment, but be unable to tell whether this will progress to dementia. Depending on how this communication is managed, it may be an opportunity for the person to take active steps to improve their prognosis, for example by following healthy living advice. It may also leave the person with both a protracted period of uncertainty and

12
continuing problems with memory and cognition. Some people may feel relieved and re-assured, but experience distress if problems progress and a later diagnosis is made.
5. The developing cognitive impairment of the person with dementia may impact at some level on his or her engagement with diagnosis sharing, either due to problems recalling and processing information, or because the condition is directly affecting insight or behaviour. Manthorpe et al. (2010) found that participants in the Transitions study, (which followed people from memory clinic assessment through to dementia diagnosis) reported significant problems with recall of consultation sessions.
6. Acceptance and adjustment to diagnosis can be particularly difficult for the person and family in those dementias which lead to early symptoms not widely associated with dementia, such as personality and behavioural changes, which may also affect insight.
7. Individuals’ and families’ expectations of early diagnosis may not be realistic; for example, some people believe that early medical treatment can prevent or cure dementia while others may be overly pessimistic about the potential of early intervention (Manthorpe et al., 2013). Even if this has been addressed during pre-diagnostic counselling, it needs to be re-visited with care during any session sharing a diagnosis.
Experiences of diagnosis sharing Whilst the MSNAP reviews and other sources are identifying much good practice in dementia diagnosis sharing, recent research continues to highlight some gaps and deficiencies in the practice of memory clinics and other services tasked with dementia assessment (e.g. Alzheimer’s Society Survey, 2014; Transitions project: Manthorpe et al., 2010; Samsi et al., 2014). Likewise the FPOP consultation with people living with dementia in the UK (Guss et al: 2014) reported continuing concerns around gaps in good practice.
Experiences of people with dementia and carersA diagnosis of dementia is now the most feared disease in over fifties in the UK (Alzheimer’s Society and Saga Homecare Poll, 2014), both due to the nature of the condition, the limited treatment options currently available, and widespread stigmatisation of the condition. Historically, evidence showed that people with dementia have often not been told the diagnosis themselves (e.g. Bamford et al., 2004). However, studies report that a large majority of people, prior to receiving a diagnosis, report wanting to know whether the cause is dementia (Pinner & Bouman, 2003; Elson, 2006; Robinson et al., 2011).
In their review of 34 papers addressing the transition process from initial referral through to a diagnosis of dementia, Robinson et al. (2011) reported that, at that time, only one study had actually followed people through the process of sharing the diagnosis, and few looked at the effect on the health of the person with dementia. These suggested that diagnosis had a short-term negative impact but that this resolved in the longer-term (Carpenter et al., 2008; Pinner & Bouman, 2003).
More recently, the ShareD study (McCabe et al., 2015; Bailey et al., 2016), which analysed videos of actual consultations, found that, on the whole, people with dementia and their carers were stoic in their reactions to the diagnosis in the meeting. Preliminary findings

13
suggest that there appears to be some reluctance to discuss prognosis – in 13 per cent of diagnostic feedback consultations it was not discussed, and in a further 25 per cent, it was discussed in the context of the effects of medication (e.g. slowing down memory decline). Doctors report that it is difficult to broach this issue at the same time as giving the diagnosis.
Evidence from people with dementia and families indicates that their responses to diagnosis can be complex, with reactions which can include shock, anger, sadness and fear, but also feelings of relief. These reactions vary from person to person and are affected by the family situation, general circumstances, and support available from services (e.g. Connell, 2004; Ducharme et al., 2011; Wald et al., 2003). There can be significant disparities between the various family members and the person with the diagnosis in their response and adjustment to the diagnosis.
The Transitions study (Manthorpe et al., 2010) undertook detailed interviews with people being assessed by Memory Clinics and their carers, to investigate their actual experiences of being referred to services and of receiving a dementia diagnosis. This qualitative evidence showed that people often did not understand the significance of different tests and found some of these distressing to undertake. They were often poorly informed about the assessment procedures used, with a lack of continuing communication with professional teams during any delays in the process. In common with the views of people taking part in the FPOP Consultation (2014), the Transitions study identified a range of different experiences, but significant problems in some Memory Clinic systems and the skills of some staff in communicating the diagnosis.
There is also evidence to support the contention that a protracted or ‘uncertain’ diagnosis, (such as mild cognitive impairment or possible dementia), with a continuing period of uncertainty is particularly difficult and stressful for the person and their family. (Smith & Beattie, 2001; Samsi et al., 2014; Manthorpe et al., 2013).
Even when the diagnosis is shared in an appropriate manner, there are some concerns about the quality and amount of information provided. For example, the Alzheimer’s Society (2014) survey found that 90 per cent of people were ‘dissatisfied’ with the amount of information they were given, with 20 per cent reporting no information or support following diagnosis. There are similar results from the USA with Gibson and Anderson (2011) reporting research with carers indicating that they had not received sufficient information about Alzheimer’s or other dementias either at the time of diagnosis or at one year follow-up.
Experiences of ProfessionalsResearch in the UK and abroad has consistently indicated that professionals find making and disclosing a dementia diagnosis challenging. Historically, studies have shown that diagnosis has been shared with family and carers in almost all cases, but with only about half of the people living with dementia, especially if the clinician considered the degree of dementia to be ‘moderate’ or ‘severe’. (Audit Commission, 2002; Downs et al., 2002; Holroyd et al., 2002).
14
Sharing a diagnosis can be complicated by the current pattern in many services of multidisciplinary assessment and diagnosis, particularly if the diagnosis is then provided by a doctor who does not know or has had little contact with the person. Initial findings from Bailey et al., (2016) suggest that doctors (psychiatrists and geriatricians) find it difficult to communicate a diagnosis of dementia to a person they are often meeting for the first time and with whom they have no established relationship, e.g. ‘I think it’s very difficult. I actually really hate going in cold and giving a diagnosis… You know how do they want to know?’ Doctors often deal with this by reviewing the information they have received from the prior assessment and history-taking meetings with the patients and their families, before delivering the diagnosis. Additionally, many doctors either ask the person about their understanding and expectation of being in the clinic directly, or work to elicit the patient’s orientation to the process in more subtle ways (for example discussing the patient’s recollection of the assessment stage), before delivering the diagnosis (Dooley et al., 2015). These strategies facilitate clinicians in tailoring their delivery to the individual.
Zaleta et al. (2012) undertook a prospective study with people being investigated for dementia which showed that, even when professionals thought they had communicated the diagnosis clearly, subsequent interviews found low levels of agreement about diagnosis between the person and the professional. Also, 20 per cent of the family or carers attending with them had either not understood the diagnosis or disagreed with it. Professionals may also resort to the use of euphemisms (e.g. ‘memory problems’) and technical terms without clarifying shared understanding (Manthorpe et al., 2010: Chapter 7).
Social conventions and constraints often mean that people may not express their emotional reactions during the course of a clinical consultation. There is evidence to suggest that HCPs underestimate the extent of the emotional impact of the diagnosis on the person with dementia and the family. For example, Connell et al. (2004) undertook focus groups with both caregivers and doctors. The family caregivers often recounted highly negative emotional responses to the session(s) in which the diagnosis was shared, whereas many physicians reported that families coped well.
Research has identified various factors which impact on HCPs practice in sharing diagnosis. These included: the emotional challenges for the professional of sharing and containing the impact of diagnosis; practical health service constraints due to pressure from waiting lists and the length of the assessment process (Murphy & Gair, 2014; Milby & Murphy, unpublished thesis, 2013); and local conditions, for example in rural communities (Scymczynska et al., 2011) where access to specialist services is more problematic.

15
Best practice in communicating a dementia diagnosis
Lecouturier et al. (2008) sought to identify what actions and behaviours by clinical staff are integral to the effective sharing of a diagnosis of dementia. They used interviews with a small sample of people with dementia and informal carers, in combination with literature review and a consensus panel of health and social care staff to identify these. They commented that the research identified areas of current clinical practice which needed improvement, but also that there were some contradictory findings, which emphasised the need for a personalised approach to diagnosis sharing and for care in balancing the needs of the person with dementia with that of family or other informal carers. This research also influenced the work of Grossberg et al. (2010) who used a panel of expert physicians and representatives from voluntary sector advocacy organisations for people with dementia and carers, to develop a similar range of guidance for use by primary care physicians in the USA. See also Antoine and Pasquier (2013) for reflections and guidelines on early Alzheimer’s disease diagnosis.
The findings of Lecouturier et al. (2008) provide a valuable description of the components of diagnosis sharing which has the potential to inform service design and training needs. There have also been major advances in clinical practice in recent years, supported by the Memory Services National Accreditation Programme (MSNAP), Royal College of Psychiatrists (2012). This has established standards for memory services, including many covering aspects of communication.
This literature has been reviewed by FPOP representatives in conjunction with the views of people with dementia (FPOP Consultation, 2014) to identify key areas of practice (see below). An extended checklist has also been developed to inform good practice and a short guide covering communication issues throughout the dementia assessment and diagnosis pathway. See appendices.
Summary of key areas of practice
Organisation and preparationThe location of the Memory Clinic itself can present a problem. Some Transitions Project participants reported that the Memory Clinic to which they had been referred was co-located with services for people with late stages of dementia and challenging behaviour. This increased the anxiety of people with possible dementia about longer-term prognosis and future needs (Manthorpe et al., 2010). It was suggested that Primary Care venues were more appropriate. Irrespective of location, any venue needs to offer appropriate privacy.
Adequate time for the session has been reported as a concern.
‘You have an incurable brain disease… Didn’t even say sorry. I was in the room for two minutes.’
The pressure for efficient use of clinical spaces should be balanced with flexible timings to meet individual needs.
Older people referred for dementia assessment who also live alone and have no close relatives or other carers need particular consideration in terms of planning diagnosis
16
sharing and follow-up, to ensure they receive adequate support during adjustment. (Waugh, 2009).
Communication and informationSharing a life-altering diagnosis is inevitably difficult for the person with dementia and the family, so communicating the diagnosis well is very important.
■ Bad communication can be traumatic and distressing for service users and carers, and impact on subsequent wellbeing and engagement with services.
‘My Doctor’s first words were, “it’s dementia, it’s progressive, you can’t drive now”. I asked him “what kind of dementia” he said “does it matter?” I went into denial after that… I think it was because of the way it was conveyed…’
‘I left and wouldn’t come out of the house for three weeks. I became withdrawn.’ (FPOP Consultation, 2014)
■ Good communication throughout assessment helps prepare people for diagnosis. Byszewski et al. (2007) advocate a progressive approach of sharing interim results and possible diagnoses throughout assessment to allow the person and family to prepare for diagnosis.
‘The delivery wasn’t a problem as we’d built up to it.’(FPOP Consultation, 2014)
■ People’s needs and preferences around diagnosis differ markedly, requiring personalisation of assessment and communication, which can be at odds with the drive for efficient use of limited resources. Manthorpe et al. (2010) reported that people with dementia and families found that the information provided by HCPs was often generic, and not specific to their needs.
■ In any medical consultation, patients recall only a small percentage of the information provided. The amount of information people with dementia can process varies depending on the extent of their problems and degree of distress, but is often much less than assumed by clinical staff.
‘I can’t remember my diagnosis.’
‘We also need information on our condition… someone to help… someone to explain it to us perhaps two or three times, and to our families as well. We need information in writing as well as in person, it just doesn’t go in otherwise.’
(FPOP Consultation, 2014)
It can be important to consider slowing down the pace of communication and to avoid an overly complicated conversation referring to multiple possible causative factors and scenarios.
■ Information that is specific to the individual is more easily recalled, so embedding the information about the diagnosis within an explanation of findings from the investigations was experienced as helpful in terms of understanding, acceptance and recall. The Transitions study also noted many favourable reports of consultations which included clear descriptions of test results and explanations of their significance (Manthorpe et al., 2010: Chapter 7.2).

17
‘The psychiatrist gave a rationale for why he came to his conclusion.’(FPOP Consultation, 2014)
■ Some guidance on sharing diagnosis recommends providing time during the session for questions, but as Manthorpe et al., (2013) found, people often did not know what to ask. Nevertheless, a structured opportunity for questions, with suggested question topics from other service users might be helpful.
■ The immediate response of a person with dementia and their family in the formal setting of the clinic may be a poor guide to the extent of psychological distress experienced. Research (Manthorpe et al. 2010) and anecdotal reports demonstrate this with some people reporting being overwhelmed by the diagnosis and unable to cope with lots of information being provided in session.
‘If you have a nervous breakdown, have a follow up, however long it takes, to bring you back to the surface.’
(FPOP Consultation, 2014)
There is no pain free way to undertake dementia assessment or to share the diagnosis. The professional(s) involved must achieve a difficult balance between an over-emphasis on negative aspects of longer-term prognosis, and the risk of colluding with avoidance of adjustment through use of euphemisms and minimisation of potential impact.
‘It was very neutral, not bad or positive. Many people would like positivity, but not false positivity.’
(FPOP Consultation, 2014)
■ The language used throughout is important. Bailey et al., 2016 report that the doctors in the ShareD study (McCabe et al., 2015) were very aware of the importance of the language they use. The doctors attempted to forecast the dementia diagnosis in the test feedback stage, for example saying the cognitive test results ‘are below what we would expect for someone of your age’. There was no evidence that doctors in the study avoided the word ‘dementia’.
■ Doctors from the ShareD study also reported that increasing public awareness of dementia is helpful in addressing the associated stigma: ‘I have to say it’s getting a lot easier to use the word dementia’.
■ Emotional distress caused by stigmatising and insensitive language is acute and impairs the person’s ability to engage with diagnosis sharing and treatment choices. Terms such as ‘sufferers’, ‘demented’ and ‘pre-senile dementia’ are experienced very negatively, and can be readily substituted with alternatives: ‘person with dementia’; ‘young onset dementia’. Many of the FPOP Consultation group expressed a preference for the term ‘sharing the diagnosis’ in place of ‘disclosure’ or ‘breaking bad news’, to emphasize collaboration and the role of the person with dementia in engaging with treatment and management choices. Information about this can be accessed from the Dementia Engagement and Empowerment Project (DEEP) website (http://www.dementiaaction.org.uk/dementiawords). The Deep Guide (2014), Dementia words matter: Guidelines on Language about Dementia provides further details and examples of language options for use in consultations.
■ Language use also needs to accommodate different understanding and awareness of dementia in BME groups. The All-Party Parliamentary Group on dementia (2013)
18
reported on the low levels of awareness and lack of provision of culturally sensitive services.
■ A lack of shared understanding about medical terminology can cause further confusion. Many clinicians have had experience of later conversations illustrating this (e.g. ‘I was so glad it was Alzheimer’s disease – I thought it might be dementia’). Terminology can be a further obstacle to effective communication, both in a diagnosis-sharing session and written correspondence. Copies of letters primarily designed for other HCPs can contain medical jargon that is not understandable for a lay person: ‘dyspraxia’, ‘aphasia’, ‘euthymic’ etc. In other instances there may be a dependency by the HCP on the use of euphemisms which may obscure the message.
‘People are often in shock on diagnosis. Having something in writing to reflect back on is good as shock causes difficulty in remembering what was said.’
(FPOP Consultation, 2014)
■ Similar principles to those described above can be applied to the specific needs of people with learning disability. See Tuffrey-Wijne and Watchman (2015) for a four-step approach to this communication with people who have a learning disability. Also, Watchman et al., (2015) have developed a pictorial guide to talking about dementia with people who have a learning disability; this can be used with both the person who has the diagnosis and any friends and peers who may struggle with understanding the changes they are observing.
■ Bailey et al. (2016) report that doctors found that it can be challenging to communicate with the person with dementia and their carer ‘You’ve got the two people in the room as well, you are sort of playing to two audiences I find’.
Who should communicate a diagnosis?As indicated earlier, assessment and diagnosis within Memory Clinics is a multidisciplinary process. A variety of professionals may be involved, depending upon complexity and the need for any specialised assessments. A diagnosis is then agreed by the team with medical personnel. The clinician responsible for sharing the diagnosis will depend on the particular Memory Clinic’s practices, which may be based on a combination of traditional medical hierarchies, and pragmatic approaches to maximise staff activity and throughput. The clinician sharing the diagnosis with the person with dementia and their family may be a doctor or another member of staff. They may or may not have been actively involved in the assessment. A member of the team who knows the person may be present. These processes can work effectively and good practice is reported by many people with dementia and their families. However, some of these arrangements may not help service users. A selection of quotes are listed below to illustrate some of the difficulties which can arise:
‘For a collaborative diagnosis, can we have someone, a professional, who we know come to the diagnosis with us?’
‘I had a good relationship with my CPN, but they weren’t allowed to be there. I would have liked him to be a part of the process.’
‘I wasn’t given a diagnosis by the one who did all the tests.’(FPOP Consultation, 2014)

19
Staff tasked with this work should have well-developed communication skills, both verbal and non-verbal. In addition specific training around the use of language and awareness of the complex dynamics affecting families are essential. They should also receive supervision focused on diagnosis sharing, which should incorporate feedback from people who use the service.
‘He didn’t introduce himself. He turned halfway round in his seat. No name, he didn’t call me by my name. “I’ve been looking at your notes and you have got Alzheimer’s disease and you will never work again.” He still didn’t look at me. I thought, ‘should I say something or should you?’ He just showed us the door, there was no one else waiting, no information.’
(FPOP Consultation, 2014)
‘Staff knew I was going to be told by a doctor I had never met before. They didn’t seem to realise how serious this was. It was horrific.’
(FPOP Consultation, 2014)
Much of the discussion on this topic has focused on the effective use of clinical resources, and on traditions and conventions around professional responsibilities. However, a memory clinic assessment involves a person with possible dementia seeing a range of different professionals and undergoing a number of specialist assessments. It is critical here also to address the experience and wishes of those on the receiving end of services, and to consider how memory clinics can respond to these. The FPOP consultation showed that most people would like the diagnosis to be shared by a HCP with whom they have built up a relationship or for that person to be involved in the process. In many cases this is likely to be a community psychiatric nurse, but might be another professional if they had a key role in the assessment process – for example a psychologist undertaking neuropsychological testing.
Support for progressive transitional adjustmentResearch (e.g. Zaleta et al., 2012), on user and carer feedback, and clinical experience confirm that communication about a diagnosis should not be seen as a single event. It should be embedded as part of the overall early stage dementia care pathway. The pattern and rate of transition and adjustment are individual to each person with dementia and his or her family. The nature and stage of the dementia, the person’s background, social circumstances and current context all influence adjustment. It is critical to the immediate and long-term wellbeing of people with dementia, possible dementia and the carers of both groups that communication about the diagnosis is done well in all respects. Pressure on resources, volume of work and time frame targets, should not impact on the quality of this communication.
This transitional adjustment is also affected by longer-term treatment and follow-up arrangements, which vary considerably between Nations within the UK and between individual health and social care districts. In some areas, the Memory Clinic responsible for investigations and diagnosis may not be the provider for subsequent follow up, which may be a different NHS Team or a voluntary sector or private agency. However, people for whom medication is appropriate are likely to have access to a HCP monitoring medication and although the primary focus of the session is not follow-up of diagnostic information, it does offer a secondary opportunity to address any issues surrounding understanding of the diagnosis. For other groups of people with dementia who are not deemed suitable for

20
medication, there may be a significant gap, follow-up from a non-health professional or volunteer, or no follow up at all. Lack of continuity and clarity about what to expect from whom, will also add to problems with understanding and adjustment.
This year, the Alzheimer’s Society (2015) commissioned a survey of GPs which found that 50 per cent and 67 per cent respectively had significant concerns about NHS and social services support for people with dementia. Over 70 per cent of GPs felt that people with dementia were having to rely on families and unpaid carers to bridge these gaps in support services. Clearly, families and informal carers cannot substitute for skilled staff in supporting continuing adjustment to diagnosis for people with dementia: they are likely to remain in need of this type of support themselves.

21
Conclusions
Across the UK there has been a focus on improving technical aspects of dementia diagnosis and improving the promptness and speed with which this is achieved. Many memory clinics and other services tasked with this work have undertaken a major process of staff recruitment and skills building for this assessment pathway in a short period of time, whilst also seeking to maximise use of available resources.
Clearly, there are examples of good communication practice in many places, and many people with dementia and carers speak warmly of their experiences of sensitive diagnosis sharing which supported their needs. However, research and feedback from people with dementia and carers shows clearly that good practice in technical diagnosis is not always matched by an integrated communication strategy throughout the process from referral to post-diagnostic support. Skillful, person-centred communication is not always a feature of consultations where the diagnosis is being shared.
A number of sources of information are already available to improve practice in sharing a dementia diagnosis:
1. Well-established knowledge about communication and memory for clinical consultations (Ley, 1979, 1985; Kessels, 2003).
2. Key behaviours that result in high quality diagnosis sharing have been identified, including the use of personalised approaches, specific to the needs, preferences and circumstances of each individual, (see attached checklist and research by Lecouturier et al., 2008; Grossberg et al., 2010; Dooley et al., 2015; Bailey et al., 2016).
3. Research evidence and feedback from people with dementia and carers about good and bad aspects of practice is available and summarised in the preceding sections. See specific recommendations below.
It is also essential for those designing and implementing local services to seek ways to embed good communication practices within their clinical pathways. Active engagement with people with dementia and families can assist this process. Collaboration between service users and professionals around language use, development and implementation of question guides to help people engage more effectively during consultations, and templates for good, personalised written or pictorial communication could all contribute to improved practice.
Clinical and other practitioner psychologists can assist this process by contributing directly to diagnosis sharing in complex cases, and by helping colleagues understand and plan the strategies they will use with particular individuals. Psychologists can also develop and support training approaches and supervision for other staff, focused on the dynamics of diagnostic consultations or offer debriefing when a consultation has been challenging. Further research and evaluation can support continuing development of models of good communication practice and skills. For information about the role and skills of psychologists, see a range of guidance from the Division of Clinical Psychology and the British Psychological Society including: Toogood, (2010), Lavender & Hope, (2007) and Prescott et al. (2014).

22
There are multiple reasons to improve the way a dementia diagnosis is communicated. We all hope for, and should receive, a humane experience at the point of diagnosis of a life-altering condition. Poor practice can cause acute distress, reduces understanding and impacts on collaborative engagement with treatment, support and follow-up. In addition to the human costs, this can have a further impact on the work pressures on the NHS. As one person with dementia contributing to the FPOP Consultation commented:
‘If you [HCP] communicate this wrong, and the person goes on a downward spiral, [the] resources are more to get them back to the surface. This cost would be greater to the individual and to society.’
(FPOP Consultation, 2014)

23
Specific recommendations ■ Sharing of assessment information and interim results throughout. ■ Preparation time for the first formal sharing of a new diagnosis. ■ A formulation of the current understanding and needs of the person with dementia and family should inform preparation for diagnosis sharing.
■ A key clinician, who has become known to the person and their family during assessment, should be present during communication about diagnosis and negotiation of treatment and support options.
■ Results and rationale for diagnosis should be explained clearly and integrated into a framework with is meaningful for the person.
■ Dementia diagnosis should include information about the subtype identified wherever possible.
■ Language use should be appropriate to the persons and reflect people’s understanding and use aids such as pictorial guides when required.
■ Language should also be sensitive and reflect people’s expressed preferences: if a diagnosis has been requested, this should be named explicitly and explained.
■ Service and staff time for multiple appointments where needed. ■ Follow-up to establish the extent to which the person has been affected by the diagnosis and associated information is needed. (Verbal discussions, questionnaires and self-rating scales can encourage frank responses).
■ Follow-up appointments over a longer time period should revisit aspects of diagnosis and prognosis as the team’s understanding of the individual develops over time.
■ Clinical psychology has a range of specialist skills which can support the staff of memory clinic teams who are sharing diagnoses with the person and families:
– Understanding of the full range of factors which impact on communication processes.
– Specialist knowledge of memory, reasoning, language and thinking, and ways to adapt communication to accommodate these.
– Understanding of the emotional impact of diagnosis on people with dementia and their families.
– Offer supervision and support reflective practice in Memory Clinic staff undertaking this work.
■ For people who need specialist cognitive assessment for very early stages, rarer dementias or unusual combinations of symptoms, (e.g. frontotemporal dementias, atypical Alzheimer’s disease) and for very complex family dynamics, clinical psychologists are likely to offer an important contribution or be best placed to undertake diagnosis sharing.

24
Checklist for process of communicating a new dementia diagnosis
Organisational issues ■ Ensure clinicians have training and regular clinical supervision/debriefing to support this work.
■ Conduct regular audits of satisfaction with diagnosis sharing and consider research options.
Preparation for clinicians ■ Identify appropriate clinician(s) based on expertise, relationship with client and family. Where follow-up appointments will be undertaken by a different clinician, undertake first session jointly.
■ Clarify diagnosis and any degree of uncertainty using current guidelines. ■ Review and understand assessment information, including scans and cognitive tests. ■ Review information from pre-diagnostic counselling and choices around diagnosis (see La Fontaine et al., 2014).
■ In context of patient’s understanding and preferences develop a plan to explain key diagnostic information.
■ Where patient’s communication needs or context are complex, consider involving team psychologist.
■ Do not try to fit too much into a single session. ■ Does the person want family or carers to be involved? ■ Identify sufficient time for initial appointment. ■ Meet at patient’s preferred venue if possible and ensure appropriate privacy. ■ Anticipate follow-up needs and make initial plan to meet these. ■ Identify appropriate written/pictorial/electronic information, copies of assessments, in line with pre-diagnostic preferences.
Sharing diagnostic information ■ Avoid interruptions. ■ Check for updates or changes in personal circumstances which may affect the session.
■ Adapt to the patient’s level of vocabulary, comprehension and processing speed. ■ Maintain eye contact and avoid speaking solely to the relative or carer. ■ Subject to person’s preference, social and cultural issues, name the diagnosis explicitly, do not avoid the words.
■ Check for understanding, encourage and answer questions. ■ After each step of the session, summarise, repeat information as needed. ■ Acknowledge emotions arising during the session and allow time for patient and family to express feelings.
■ Actively counter stigma and nihilism by identifying remaining abilities. Focus on strategies to live well with the disease.
Clinical options and post-diagnostic care ■ Set realistic expectations for treatment. ■ Explain all treatment options (including no treatment).
25
■ Initiate prompt, comprehensive treatment, including pharmacotherapy and psychosocial interventions/support, (see Watts et al; 2014).
■ Provide education about dementia appropriate to stage of condition and needs of individual.
■ Inform the person and family of available services, encourage utilization; provide information and websites.
■ Acknowledge importance of caregiver’s emotional and health care needs and facilitate access to resources.
■ Review and address any risks, need for support and encourage feedback about session.
■ Book follow-up appointment with named clinician. ■ Review. ■ Review progress made with communication of diagnosis. ■ Consider further assessment of psychological impact on person/family – refer to psychology when needed.
■ Plan next stages. ■ Review feedback, employ reflective practice and take to clinical supervision.
Acknowledgments: derived from FPOP Consultation(2014); Le Couturier et al. (2008); Grossberg et al. (2010); Murphy & Gair (2014).
26
First GP visit Pre-diagnostic
counsellingMemory Clinic assessments (may be several sessions)
Sharing the diagnosis(one or more sessions)
Post-diagnostic treatment and support
What is happening?
You, your family or a professional you know, have concerns about your memory and thinking changes.
GP undertakes locally/nationally recommended investigations.
GP considering making a referral.
Memory Clinic or other specialist provider talks with you (and your family where appropriate):
Jointly explore ideas about your difficulties.
They check out your knowledge to make sure you understand what will happen.
They provide more explanation about clinic tests.
Jointly agree way forward.
The MC team will arrange standard tests:
Interview with you and a person who knows you well.
Short tests of thinking, memory and mood.
Questions about how you cope at home.
You may also have:
Brain scan(s).
Further medical tests.
More in-depth cognitive testing.
Activities of daily living checks.
The MC team will organise an appointment to tell you the diagnosis if this is what you want.
A member of the clinical team who has been involved in your assessments should take part/or provide the diagnosis.
If more than one session is needed they should offer this.
A MC team member will explain treatment and support options and agree a plan with you.
The MC team/other professionals should continue to explore any questions you have about diagnosis and treatment as time goes on.
A MC team member will explain treatment and support options and agree a plan with you.
Good communication standards
Non-stigmatising language.
Introducing possible diagnoses.
Therapeutic optimism.
Explain a little about what Memory Clinic does.
Non-stigmatising language
Further exploration of diagnostic possibilities
Clarifying benefits and disadvantages of from your perspective.
Non-stigmatising language.
Clear explanations of what is being done and why.
Initial indication of how tests are going.
Your questions answered.
They should:
Name the condition.
Explain how tests have shown this.
Use sensitive, clear language and check your understanding.
Ask for feedback from you.
Begin to explain treatment options.
Explain /book next steps.
Use sensitive, but clear language.
Check your understanding.
Ask for feedback from you.
Review and monitor agreed treatment and support plan.
What can I and my family contribute?
Information about your history and background.
Examples of difficulties.
Lists are good!
It helps to bring some ideas of questions to the session.
Question suggestion list.
Keep the team up-to-date with any changes you have noticed, including physical health and life events.
Question suggestion list.
If you don’t understand say so.
If you feel overwhelmed, or unable to concentrate, say so, ask for a break or a further appointment.
If a professional says ‘memory problems’, ask if they mean dementia.
You are entitled to a copy of their letter to the GP or a more personalised letter.
Question/coping suggestion list
Prepare for meetings, keep lists of questions, don’t be afraid to ask.
Think about what you want.
See Alzheimer’s Society Factsheet Number Tips: Getting the most from a consultation.
27
References
All-Party Parliamentary Group on Dementia, (2012). Unlocking Diagnosis: The key to improving the lives of people with dementia. London: HMSO.
All Party Parliamentary Group (2013). Dementia does not discriminate: The experiences of black, Asian and minority ethnic communities. London: HMSO.
Alzheimer’s Society, (2014). Dementia 2014: Opportunity for change. London: Alzheimer’s Society.
Alzheimer’s Society, (2014). Alzheimer’s Society and Saga Homecare Poll. https://www.alzheimers.org.uk/site/scripts/news_article.php?newsID=2038
Alzheimer’s Society (2015). Alzheimer’s Society Early Diagnosis campaign: GP Evaluation Summary. https://www.alzheimers.org.uk/site/scripts/download_info.php?fileID=1476
Aminzadeh, F., Byszewski, A., Molnar, F. & Eisner, M. (2007). Emotional impact of dementia diagnosis: Exploring persons with dementia and caregivers’ perspectives. Aging & Mental Health, 11(3), 281–290.
Antoine, P. & Pasquier, F. (2013). Emotional and psychological implications of early AD diagnosis. Medical Clinics of North America, 97, 459–475. http://dx.doi.org/10.1016/j.mcna.2012.12.015 medical.theclinics.com
Audit Commission, (2002). Forget-me-not: Developing mental health services for older people. London: Author.
Baile, W.F., Buckman, R., Lenzi, R. et al. (2000) SPIKES – A six-step protocol for delivering bad news: Application to the patient with cancer. The Oncologist, 5, 302–311. doi:10.1634/theoncologist.5-4-302
Bailey, C., Dooley, J. & McCabe, R. (2016). The Little Dance: Delicate Deliveries of Dementia Diagnoses: Emerging findings from the ShareD study focus groups with doctors. The ShareD Study Team, Royal College of Psychiatrists Old Age Faculty Scientific Meeting, Nottingham, UK March 9–11 2016.
Bamford, C., Lamont, S., Eccles, M. et al. (2004). Disclosing a diagnosis of dementia: A systematic review. International Journal of Geriatric Psychiatry, 19(2), 151–169.
Banerjee, S., Willis, R., Matthews, D. et al. (2007) Improving the quality of care for mild to moderate dementia: An evaluation of the Croydon Memory Service Model. International Journal of Geriatric Psychiatry, 22(8), 782–788.
Benbow, S.M., Greaves , I. & Jolley, D. (2013) All people with dementia need accurate assessment and ongoing support, BMJ 2013;347:f6108 doi: 10.1136/bmj.f6108
British Psychological Society/Royal College of Psychiatrists Working Group (2015). Dementia and people with intellectual disabilities: Guidance on the assessment, diagnosis, interventions and support of people with intellectual disabilities who develop dementia. Leicester: British Psychological Society.

28
Buckman, R. (1992). How to break bad news: A guide for health-care professionals. London: Papermac.
Buckman, R. (2005). Breaking bad news: The SPIKES strategy. Community Oncology, 2, 138–142.
Byszewski, A.M., Molnar, F.J., Aminzadeh, F. et al. (2007) Dementia diagnosis disclosure: A study of patient and caregiver perspectives. Alzheimer Disease and Associated Disorders, 21, 107–114.
Cahill, S., Clark, M., O’Connell, H. et al. (2008). The attitudes and practices of general practitioners regarding dementia diagnosis in Ireland. International Journal of Geriatric Psychiatry, 23, 663–669.
Carpenter, B.D., Xiong, C., Porensky, E.K. et al. (2008). Reaction to a dementia diagnosis in individuals with Alzheimer’s disease and mild cognitive impairment. Journal of American Geriatric Society, 56(3), 405–12.
Clare, L. (2003). Managing threats to self: Awareness in early stage Alzheimer’s disease. Social Science and Medicine, 57(6), 1017–1029.
Clark, M., Moreland, N., Greaves, I., Greaves, N. & Jolley, D. (2013) Putting personalisation and integration into practice in primary care. Journal of Integrated Care, 21, 105–20.
Collerton, D. & Domone, R. (2014). Cognitive assessment of people who may be developing dementia. In R. Guss et al. Clinical psychology in the early stage dementia care pathway. Leicester: British Psychological Society.
Connell, C., Boise, L., Stucky, J., Holmes, S. & Hudson, M. (2004). Attitudes toward the diagnosis and disclosure of dementia among family caregivers and primary care physicians. The Gerontologist, 44(4), 500–507.
Connelly, P.J. & Perera, N. (2013). Developing an ideal old age service. London: Royal College of Psychiatry.
Cross Party Group on Alzheimer’s (2009). Charter of Rights for People with Dementia and their Carers in Scotland. Retrieved from: http://www.scottishhumanrights.com/application/resources/documents/FINALCharterofRights.pdf
Cutler, S.J. & Hodgson, L.G. (1996). Anticipatory dementia: A link between memory appraisals and concerns about developing Alzheimer’s disease. Gerontologist, 36(5), 657–664.
Dementia Engagement and Empowerment Project – DEEP. (2014). Dementia words matter: Guidance on language about dementia. Available at: http://dementiavoices.org.uk/wp-content/uploads/2015/03/DEEP-Guide-Language.pdf
Department of Health. (2009). Living well with dementia: A national dementia strategy. London: Author.
Department of Health. (2010). Quality outcomes for people with dementia: Building on the work of the National Dementia Strategy. London: Author.
Department of Health. (2011). Case for change – memory services for people with dementia: Evidence. London: Author.

29
Department of Health. (2011). Service specification for dementia: Memory services for early diagnosis and intervention. London: Author.
Department of Health (2012). Prime Minister’s challenge on dementia: Delivering major improvements in dementia care and research by 2015. London: Author.
Department of Health (2013). Prime Minister’s challenge on dementia: Annual report of progress. London: Author.
Department of Health and Royal College of General Practitioners. (2003). Guidelines for the appointment of general practitioners with special interests in the delivery of clinical services: Care of older people. London: Department of Health.
Department of Health, Social Services & Public Safety (DHSSPS). (2003). Breaking bad news: Regional guidelines. Belfast: Author.
Department of Health, Social Services and Public Safety (2011). Improving Dementia Services in Northern Ireland- A Regional Strategy. Retrieved from: https://www.dhsspsni.gov.uk/sites/default/files/publications/dhssps/improving-dementia-services-2011.pdf
Derksen, E., Vernooij-Dassen, M., Gillissen, F., Olde Rikkert, M. & Scheltens, P. (2006). Impact of diagnostic disclosure in dementia on patients and carers: Qualitative case series analysis. Aging & Mental Health, 10(5), 525–531.
Dexter-Smith, S. (2010). Integrating psychological formulations into older people’s services – three years on (Part 1). PSIGE Newsletter, 112, 8–11.
Division of Clinical Psychology (2007). Marketing strategy for clinical psychologists. Retrieved from dcp.bps.org.uk/document-download-area/document- download$.cfm?file_uuid=AC0686B5-1143-DFD0-7E06-1EA51AB27AEA&ext=pdf
Dooley, J., Bailey, C. & McCabe, R. (2015). Communication in healthcare interactions in dementia: A systematic review of observational studies. International Psychogeriatrics, 27(8), 1277–1300.
Dooley, J., McCabe, R., Bass, N. & ShareD Study Team, (2015). Communicating a diagnosis of dementia. Memory Services National Accreditation Program (MSNAP), Liverpool UK, 29 September 2015.
Downs, M., Clibbens, R., Rae, C., Cook, A. & Woods, R. (2002). What do general practitioners tell people with dementia and their families about the condition? Dementia, 1(1), 47–58.
Ducharme, F., Lèvesque, L., Lachance, L., Kergoat, M-K. & Coulombe, R. (2011). Challenges associated with transition to caregiver role following diagnostic of Alzheimer disease: A descriptive study. International Journal of Nursing Studies, 48, 1109–1119.
Elson, P. (2006). Do older adults presenting with memory complaints wish to be told if later diagnosed with Alzheimer’s disease? International Journal of Geriatric Psychiatry, 21, 419–425.
Fisk, J.D., Beattie, B.L., Donnelly, M., Byszewski, A. & Molnar, F. (2007). Disclosure of the diagnosis of dementia. Alzheimer’s & Dementia, 3, 404–410.

30
Gibson, A.K. & Anderson, K.A. (2011). Difficult diagnoses: family caregivers’ experiences during and following the diagnostic process for dementia. American Journal of Alzheimers Disease and Other Dementias, 26(3), 212–217.
Goodwin, N., Curry, N., Nayloy, C., Ross, S. & Duldig, W. (2010). Managing people with long-term conditions. London: The King’s Fund.
Grossberg, G.T., Christensen, D.D., Griffith, P.A. et al. (2010). The art of sharing the diagnosis and management of Alzheimer’s disease with patients and caregivers: Recommendations of an expert consensus panel. Primary Care Companion to the Journal of Clinical Psychiatry, 12(1), PCC.09cs00833. doi:10.4088/PCC.09cs00833oli PMCID: PMC2882814
Guss, R. & colleagues from the Faculty of the Psychology of Older People (2014). Clinical Psychology in the Early Stage Dementia Care Pathway. Leicester: British Psychological Society.
Guss, R., Slade, L. & Litherland, R. (2014). FPOP consultation with people living with dementia in the UK: A position paper. In R. Guss et al. Clinical Psychology in the Early Stage Dementia Care Pathway. Leicester: British Psychological Society.
Hansen, E.C., Hughes, C., Routely, G. & Robinson, A.L. (2008). General practitioners’ experiences and understandings of diagnosing dementia: Factors impacting on early diagnosis. Social Science & Medicine, 67, 1776–1783.
Hodge, S. & Hailey, E. (Eds.). (2015). MSNAP Third National Report, 2013–14. Royal College of Psychiatrists.
Hodgson, L.G. & Cutler, S.J. (2004). Help seeking for personal concerns about developing Alzheimer’s disease. Journal of Applied Gerontology, 23(4), 385–410.
Holroyd, S., Turnbull, Q. & Wolf, A. (2002). What are patients and their families told about the diagnosis of dementia? Results of a family survey. International Journal of Geriatric Psychiatry, 17, 218–221.
Husband, H.J. (2009). What do we tell people with dementia about their diagnosis and how do we tell them? In E. Moniz-Cook & J. Manthorpe (Eds.) Early psychosocial interventions in dementia: Evidence-based practice. London: Jessica Kingsley.
IIiffe, S., Eden, A., Downs, M. & Rae, C. (1999). The diagnosis and management of dementia in primary care: Development, implementation and evaluation of a national training programme. Aging and Mental Health, 3(2), 129–135.
Iliffe, S., Manthrope, J. & Eden, A. (2003). Sooner or later? Issues in the early diagnosis of dementia in general practice: A qualitative study. Family Practice, 20(4), 376–381.
Iliffe, S. & Manthorpe, J. (2004). The hazards of early recognition of dementia: A risk assessment. Aging Mental Health, 8(2), 99–105.
Iliffe, S., Robinson, L., Brayne, C., Goodman, C., Rait, G., Manthorpe, J., Ashley, P. & the DeNDRoN Primary Care Clinical Studies Group (2009). Primary care and dementia: 1. diagnosis, screening and disclosure. International Journal of Geriatric Psychiatry, 24, 895–901. Published online 18 February 2009 in Wiley InterScience (www.interscience.wiley.com) doi:10.1002/gps.2204

31
Jha, A., Tabet, N. & Orrell, M. (2001). To tell or not to tell – comparison of older patients reactions to their diagnosis of dementia and depression. International Journal of Geriatric Psychiatry, 16, 979–885.
Kaduszkievwicz, H., Bachman, C. & van den Busscle, H. (2008). Telling ‘the truth’ in dementia – Do attitude and approach of general practitioners and specialists differ? Patient Education and Counselling, 70, 220–226.
Kaplan, M. (2010). SPIKES: A framework for breaking bad news to patients with cancer. Clinical Journal of Oncology Nursing, 14(4), 514–516.
Karnieli-Miller, O., Werner, P., Aharon-Peretz, J. & Eidelman, S. (2007). Dilemmas in the (un)veiling of the diagnosis of Alzheimer’s disease: Walking an ethical and professional tight rope. Patient Education and Counselling, 67, 307–314.
Kessels, R.P.(2003). Patients’ memory for medical information. Journal of the Royal Society of Medicine, 96(5), 219–222.
Koch, T. & Iliffe, S. (2011). Dementia diagnosis and management: a narrative review of changing practice. The British Journal of General Practice. doi:10.3399/bjgp11X588493.
Lackkonen, M-L., Raivio, M.M., Eloriemi-Sulkava, V. et al. (2008). How do elderly spouse caregivers of people with Alzheimer’s disease experience the disclosure of dementia diagnosis and subsequent care? Journal of Medical Ethics, 34, 427–430.
La Fontaine, J., Buckell, A., Knibbs, T. & Palfrey, M. (2014). Early and timely intervention in dementia: Pre-assessment counselling. In R. Guss et al. Clinical psychology in the early stage dementia care pathway. Leicester: British Psychological Society.
Lavender, T. & Hope, R. (2007) New ways of working for applied psychologists in health and social care. Care Services Improvement Partnership/British Psychological Society. Leicester: British Psychological Society.
Le Couteur, D.G, Doust J., Creasey H. & Brayne, C. (2013). Political drive to screen for pre-dementia: Not evidence based and ignores the harms of diagnosis. BMJ, 347, f5125. doi: 10.1136/bmj.f5125
Lecouturier, J., Bamford, C., Hughes, J.C. et al. (2008). Appropriate disclosure of a diagnosis of dementia: Identifying the key behaviours of ‘best practice’. BMC Health Services Research, 8(95).
Lee, L., Hillier, L.M., Stolee, P. et al. (2010). Enhancing dementia care: A primary care based memory clinic. Journal of the American Geriatrics Society, 58(11), 2197–2204.
Lee, L. & Weston, W.W. (2011). Disclosing a diagnosis of dementia: Helping learners to break bad news. Canadian Family Physician: Teaching Moment, 57, 851–852.
Leung, K.K., Finlay, J., Silvius, J.L. et al. (2011). Pathways to diagnosis: Exploring the experiences of problem recognition and obtaining a dementia diagnosis among Anglo-Canadians. Health & Social Care in the Community, 19(4), 372–381.
Ley, P. (1979). Memory for medical information. British Journal of Social and Clinical Psychology, 18(2), 245–255.
Ley, P. (1985). Doctor-patient communication: some quantitative estimates of the role of cognitive factors in non-compliance. Journal of Hypertension Supplement, 3(1), S51–S55.

32
Ley, P. (1988). Communicating with patients. New York: Croom Helm.
McCabe, R., Priebe, S., Dooley, J. et al. (2015). The ShareD Study, retrieved from: http://medicine.exeter.ac.uk/research/healthserv/shared/
Manthorpe, J., Samsi, K., Campbell, S., et al. (2010). The transition from cognitive impairment to dementia: older people’s experiences. Final report. Southampton: NIHR Service Delivery and Organisation programme.
Manthorpe, J., Samsi, K., Campbell, S. et al. (2013). From forgetfulness to dementia: Clinical and commissioning implications of diagnostic experiences. British Journal of General Practice. Published online, 2012, 19 December. doi:10.3399/bjgp13X660805
Marzanski M. (2000) On telling the truth to patients with dementia. Journal of Medical Ethics, 26, 108–113.
Milby, E. & Murphy, G.L. (unpublished thesis, 2013). Diagnosis disclosure in dementia: Understanding the experiences of people who have recently given or received a diagnosis.
Milne, A. (2010). Dementia screening and early diagnosis: The case for and against. Health, Risk & Society, 12, 1, 65–76. doi:10.1080/13698570903509497
Moniz-Cook, E. (2009). Timely psychosocial interventions in a memory clinic. In E. Moniz-Cook & J. Manthorpe (Eds.) Early psychosocial interventions in dementia: Evidence-based practice. London: Jessica Kingsley.
Moniz-Cook, E. & J Manthorpe. (2009). Early psychosocial interventions in dementia: Evidence based practice. London: Jessica Kingsley Publications.
Murphy, G.L (unpublished, 2013). Post-diagnostic transition groups for individuals who have received a diagnosis of dementia and their carers.
Murphy, G. & Gair, E. (2014) Communicating a diagnosis of dementia. FPOP Newsletter, 127, 58–62.
Nuffield Council on Bioethics, (2009). Dementia: Ethical issues. London: Author.
Pinner, G. & Bouman, W.P. (2003). Attitudes of patients with mild dementia and their carers towards disclosure of the diagnosis. International Psychogeriatrics, 15(3), 279–288.
Pratt, R. & Wilkinson, H. (2003). A psychosocial model of understanding the experience of receiving a diagnosis of dementia. Dementia, 2(2), 181–199.
Prescott, T., Aris, S., Dale, N. et al. (2014). National mental health, well-being and psychological therapies – the role of clinical psychology: A briefing paper for NHS Commissioners. Leicester: British Psychological Society.
Prince, M., Bryce, R. & Ferri, C. World Alzheimer Report 2011: The benefits of early diagnosis and intervention. London: Alzheimer’s Disease International, 2011.
Rae, C., McIntosh, I. & Colles, S. (2001). The primary care team, dementia and management: A research report. Stirling: University of Sterling.
Rice, K. & Warner, N. (1994). Breaking the bad news: What do psychiatrists tell patients with dementia about their illness? International Journal of Geriatric Psychiatry, 9, 467–471.

33
Robinson, L., Gemski, A., Abley, C. et al. (2011). The transition to dementia – individual and family experiences of receiving a diagnosis: a review. International Psychogeriatrics, 23(7), 1–18, 1026–43. doi:10.1017/S1041610210002437
Royal College of Psychiatrists (2014). Memory services national accreditation programme (3rd edn). London: Author.
Samsi, K., Abley, C., Campbell, S. et al. (2014). Negotiating a labyrinth: Experiences of assessment and diagnostic journey in cognitive impairment and dementia. International Journal of Geriatric Psychiatry, 29, 58–67.
The Scottish Government (2013). Scotland’s National Dementia Strategy 2013–2016, Edinburgh: Author. Retrieved from: http://www.gov.scot/Topics/Health/Services/Mental-Health/Dementia/DementiaStrategy1316
Silverman, J., Kutz, S.M. & Draper, J. (1998). Skills for community with patients. Oxford: Radcliffe Medical Press.
Smith, A. & Beattie, B. (2001). Disclosing a diagnosis of Alzheimer’s disease: Patient and family experiences. The Canadian Journal of Neurological Sciences, 28(1), 67–71.
Spector, A. & Orrell, M. (2010). Using a biopsychosocial model of dementia as a tool to guide clinical practice. International Psychogeriatrics, 22(6), 957–965.
Steeman, E., Casterlè, B., Godderis, J. & Grypolonck, M. (2006). Living with early-stage dementia: A review of qualitative studies. Journal of Advanced Nursing, 54(6), 722–738.
Szymczynska, P., Imes, A., Marson, A. & Stark, C. (2011). A review of diagnostic process and post diagnostic support for people with dementia in rural areas. Journal of primary Care & Community Health, 2(4), 262–276.
Toogood, R. (Ed.). (2010). The core purpose and philosophy of the profession. Division of Clinical Psychology. Leicester: British Psychological Society.
Tuffrey-Wijne, I. (2012). Breaking bad news tool. http://www.breakingbadnews.org/tool
Tuffrey-Wijne, I. & Watchman, K. (2015). Breaking bad news to people with learning disabilities and dementia. Learning Disability Practice, 18(7), 16–23.
Turner, S., Iliffe, S., Downs, M. et al. (2004). General practitioners’ knowledge, confidence and attitudes in the diagnosis and management of dementia. Age and Ageing, 33, 461–467.
Wald, C., Fahy, M., Walker, Z. & Livingston, G. (2003). What to tell dementia caregivers – the rule of three. International Journal of Geriatric Psychiatry, 19, 313–317.
Waldemar, G., Phung, K.T.T., Burns, A. et al. (2007). Access to diagnostic evaluation and treatment for dementia in Europe. International Journal of Geriatric Psychiatry, 22(1), 47–54.
Watchman, K. (Ed.). (2015). Intellectual disability and dementia research into practice. Dementia, 14, 137–138.
Watts, S., Cheston, R., Moniz-Cook, E. Burley, C. & Guss, R. (2014). Post-diagnostic support for people living with dementia. In R. Guss et al. Clinical Psychology in the early stage dementia care pathway. Leicester: British Psychological Society.

34
Waugh F. (2009). Where does risk feature in community care practice for older people with dementia who live alone? Dementia, 8(2), 205–22.
Welsh Assembly Government (2011). The national dementia vision for Wales, dementia supportive communities. Retrieved from: http://gov.wales/docs/dhss/publications/110302dementiaen.pdf
Werner, P., Karnieli-Miller, O. & Eidelman, S. (2013). Current knowledge and future directions about the disclosure of dementia: A systematic review of the first decade of the 21st century. Alzheimer’s and Dementia, 9, 74–88.
Zaleta, A.K. & Carpenter, B.D. (2010) Patient-centered communication during the disclosure of a dementia diagnosis. American Journal of Alzheimer’s Disease and other Dementias, 25(6), 513–520. doi:10.1177/1533317510372924
Zaleta, A.K., Carpenter, B.D., Porensky, E.K., Xiong, C. & Morris, J.C. (2012). Agreement on diagnosis among patients, companions, and professionals after a dementia evaluation. Alzheimer Disease and Associated Disorders, 26(3), 232–7.

April 2018
Communicating a diagnosis of dementiaSusan Watts, Rose McCabe & Reinhard Guss
Faculty of the Psychology of Older People
Incorporated by Royal Charter Registered Charity No 229642 REP117/03.18
The British Psychological SocietySt Andrews House, 48 Princess Road East, Leicester LE1 7DR, UKTel: 0116 254 9568 Fax 0116 247 0787 E-mail: [email protected] Website: www.bps.org.uk
9 781854 337641
ISBN 978-1-85433-764-1