isjm issue #2 september 2013
DESCRIPTION
Imternational Students Journal of Medicine (ISJM), S.D.Asfendiyarov Kazakh National Medical UniversityTRANSCRIPT

THE LATEST MODE OF DIAGNOSIS,
MANAGEMENT AND PREVENTION OF
ACUTE MENINGITIS
By Muhammad Yameen Hamid, AninditaGhosh
THE ETIOLOGICAL STRUCTURE AND
CLINICAL EPIDEMIOLOGICAL FEATURES
OF VIRAL MENINGOENCEPHALITIS IN
CHILDREN
By N.B.Tukhanova
MODULATION OF INTESTINAL TIGHT
JUNCTION PROTEINS BY NUTRIENTS
By Siti Sarah Binti Ahmad Shahidan, Mohammed
Nasimul Islam, Jesmine Khan
IDENTIFICATION OF SYMPTOMS OF A
STRESS AT STUDENTS DURING CARRYING
OUT IN EXAMS
By Akkazhieva N.N., Nuritdinova M.M.
ATRIAL FIBRILLATION AND VEGETATIVE
NERVOUS SYSTEM STATUS: PRE-HOSPITAL
TREATMENT AND MANAGEMENT TACTICS
By V.G. Epifanov, V.T. Dolgikh
INVESTIGATION OF STOMATITIS CAUSES
AMONG THE STUDENTS AND
DEVELOPMENT OF "PHYTOMEDICATION"
FOR THE PREVENTION AND TREATMENT
By D. Sharipov
CHANGING OF SUCCINATE
DEHYDROGENASE’S (SDH’S) ACTIVITY IN
HYPOTHYROIDISM OF NEWBORN AND
PREGNANT WOMEN
By M. Kulmaganbetov
p. 8
p. 16
p. 18
p. 23
p. 25
p. 33
p. 35

Toregeldy Sharmanov Sharmanovich was born on the 19th of
October of 1930, in village Ulytau, Karagandy province. After
excellent graduation of Karagandy State Medical University in
1995 and postgraduate studentship (1958-1962) he worked as a
chief doctor of Ulytau Central District Hospital of Karagandy
Province. Since 1962 till 1968 he was a chair of nutrition
department of research institute of endemic medicine of Health
Ministry of KazSSR. From 1968 to 1971 – vice-chancellor of
Aktyubinsk State Medicine Institute and at the same time a chair
of pharmacology department.
1971-1982 – Minister of Health Ministry of Kazakh SSR
From 1972 to these days – founder and president of Kazakh
Nutrition Academy. The academy is a center of comlplex research
involving a wide spectrum of problems of hygiene, biochemistry,
immunology, nutrition physiology, diet prevention and diet
therapy in the republics of Central Asia. T.S.Sharmanov is a
founder of the School of Nutritionists in Kazakhstan. He is a
director of international scientific and technological projects on
liquidation of iron deficiency anemia, iodine insufficient
condition, breast nutrition supporting, medical-demographic
investigations being lead in cooperation with international
organizations such as UN Children Fund, WHO, UN Development
Programme, USAID, Macro International Inc, Wilstart, etc.
During 1985 through 1988 he was a main editor of All-Soviet
Union magazine “Nutrition issues”, chair of nutrition department
of Central Institute of doctors’ enhancement in Moscow. From
May of 1995, he was a founder and president of the Academy of
Preventative Medicine.
He remains a head editor of the magazine “Health and decease”.
The Center of Children Nutrition that has no analogies on the area
of CIS was created under his direction, just like principally new
products of children nutrition were brought into practice, and a
range of decease-preventive products as well.
Thanks to the initiativity of T.S.Sharmanov and his efforts, in 1979 the nutrition Institute became first in the
world to cooperate with WHO in nutrition field, and since 1997 cooperating center of UN University. Thirty
six doctor and one hundred seventy PhD dissertations were defended under his supervision. T.Sharmanov
is an author of 350 publications including 25 monographs and 37 inventions. He was elected into the
Parliament of Republic of Kazakhstan for three times.
His son Almaz is a PhD in medicine, a citizen of the United States, diplomat, director of USAID Kazakhstan
mission, international health expert and a professor at Johns Hopkins University (USA), vice-president of
Nazarbayev University. He is a grandfather for three: Alua has graduated from Maryland University (USA),
married, living in USA, Torekhan – 19 years old, Askar – 17, and a great grandson Konnor, born in 2006.

Toregeldy Sharmanov Sharmanovich is a man who needs no presentation.
However, he prefers avoing various praises and mentioning his numerous
regalia that might be a subject of jealousy for any academician.
Toregeldy has always openly expressed and keeps expressing his criticizing his
extraordinary position towards not only the topical health-related issues, but
also the ethics of human relationships, social development and political
priorities.
It certainly must be the 12 years of being a health minister, also claimed as a
“golden age of our medicine”, that comprise the most unforgettable part of his
bio for us. Those were the years when he unfolded as a convinced, charismatic,
creative and willful leader. At that time he manages to create a unique
infrastructure of health service and a great human recourse potential that will
withstand the collapse of USSR and the following reforms. These achievements
received international acknowledgement during the historical conference
dedicated to rendering first medical help that was lead in Alma-Ata in 1978 in
presence of health minister from 140 countries. That conference has accepted
the Alma-ata declaration which is now being called a “Bible of world health
service”. For these merits twenty five years later Toregeldy Sharmanov was
entitled for the highest award of World Health Organization – Leon Bernar
medal which has been conferred for only 42 times during the entire history.
Toregeldy has actualized himself not only as a politician and public figure, but
also as a great scientist. His discoveries in the area of nutrition still remain
relevant to our days. He was the first academician from Central Asia who
became a member of the Academy of Medical Sciences of USSR. The science
collectivity of Kazakh Academy of Nutrition that was chaired by him for 35
years received acknowledgments from such reputable organizations as UN
Children Fund, UN Development Programme and many others.
Today Kazakh Academy of Nutrition puts a lot of effort on fighting anemia,
iodine insufficiency and other deceases of children and women.
Several generations of Kazakhstan people grew nourished by unique children
products, created by Toregeldy Sharmanov. Today these inventions are
implemented as a factory producing children nutrition that was constructed by
him in cooperation with foreign investors.
Politicians respect him. He is always at the center of media’s attention.
Colleagues praise him. Youth admires him. Relatives love him. As Toregeldy
Sharmanov says about himself, he feels that he is in a good shape and feels like
40 at his 83 years.
«ALMATY TURNING POINT OF WORLD HEALTH CARE»
Dedicated to the 30th anniversary of Alma-Ata WHO/UNICEF
Conference of 1978 named the most remarkable event in the
history of medicine and then adopted Alma-Ata Declaration –
«The Great Charter of World Health care»
Thirty years ago the Declaration of Alma
Ata articulated Primary Health Care as a
set of guiding values for health
development, a set of principles for the
organization of health services and a range
of approaches for addressing both priority
health needs and the fundamental
determinants of health.
It was conceived as a commitment to
universal access to services for protecting
and improving health status between and
within countries.
On the whole people are healthier today
and live longer than thirty years ago.
However, there is a deepening
dissatisfaction with health services
worldwide. Unprecedented commitment,
funds, technology and expertise have not
resulted in expected health outcomes.
Hundreds of millions of people still remain
without regular access to services.
More and more countries are turning
again to the values of Primary Health Care
as the basis for strengthening their health
systems.
In his capacity as Minister of Health of
the Kazakh Republic Professor Toregeldy
Sharmanov was one of the key organizers
of the Alma Ata conference which was co-
sponsored by the World Health
Organization and UNICEF. As author of
this book he offers readers unique
perspective on both the background and
follow up to the historic Alma Ata
conference.
On the occasion of the Thirtieth
Anniversary of the Declaration of Alma
Ata his insight provides a valuable
reference to today’s members of the
international health community as they
engage in the new worldwide movement to
revitalize Primary Health Care.
Dr Margaret Chan
Director Genera
World Health Organization
«Almaty Turning Point of World Health
Care»

ISJM
8 Issue 01 / September 2013 isjm.kaznmu.kz
THE LATEST MODE OF DIAGNOSIS, MANAGEMENT AND PREVENTION OF
ACUTE MENINGITIS
Prof. Dr. Maliha Hakim, Professors, Neurology Department, ShaheedSuhrawardy Medical College, Dhaka Dr. M TasdikHasan, Research Fellow, ICDDR,B Muhammad Yameen Hamid, 4th year, ShaheedSuhrawardy Medical College, Dhaka, Bangladesh E-mail: [email protected] AninditaGhosh, 4th year, ShaheedSuhrawardy Medical College, Dhaka, Bangladesh
Abstract:
Introduction
Meningitis is an acute inflammation of
leptomeninges and CSF caused by
mainly bacteria, virus and less
commonly fungus which has 50% case
fatality rate if untreated. The most
common symptoms are a stiff neck, high
fever, sensitivity to light, confusion,
headaches and vomiting. Meningitis is
potentially fatal and should always be
viewed as a medical emergency. Thus
early diagnosis and effective
management of suspected cases of
meningitis will lead to significantly
reduction in mortality. In this article the
latest modes of diagnosis and treatment
have been discussed along with
preventive measure.
Method
This study was done by reviewing 15
journals, online clinical articles and
clinical books from June, 2013 to July,
2013.
Result
In laboratory investigation, CSF profile
shows different characteristics in
bacterial and viral etiology. CSF
pressure is elevated with low glucose
level; high protein level and
predominant neutrophil in bacterial
cause. In viral cause pressure is almost
normal, lymphocyte is predominant,
glucose and protein levels are normal.
PCR and ICT detecting bacterial DNA
show 100% specificity. CT or MRI is not
diagnostic usually. The latest treatment
plan includes empiric therapy, specific
therapy, adjunctive therapy by
Dexamethasone, outpatient
antimicrobial therapy & antiviral
therapy and treatment of special
situation. Empiric antimicrobial therapy
should be started as soon as possible
after diagnosis proven or suspected.
Specific therapy depends on Gram’s
staining and culture of CSF.
Ciprofloxacin is used successfully in
multidrug resistant gram-negative
bacilli. In HSV, VZV and CMV
meningitis acyclovir and ganciclovir is
given. Dexamethasone is effective in
bacterial meningitis as adjunctive
therapy. In special situation as in
fulminant meningococcemia
benzylpenicillin is drug of choice, in
increased ICP mannitol is administered
and patient is monitored ICU. Vaccines
that are available to control the disease
are meningococcal A conjugate vaccine,
C conjugate vaccines (MCV4),
tetravalent A, C, Y and W135 conjugate
vaccines and meningococcal
polysaccharide vaccines. Meningococcal
A conjugate vaccineelicited a stronger
response to group A antibody than the
tetravalent vaccine.
Discussion/Conclusion

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 9
Early recognition and initiation of
appropriate empiric therapy can reduce
the mortality to 10%. If rapid and
specific identification of the
etiologicagent is done and adjusting
therapies are given as indicated, it will
efficiently manage a patient with
meningitis. Optimize management is
possible in complicating features.
Prevention can be done in epidemic
areas by proper vaccination mentioning
MCV4 and HIB vaccine.
Key words
acute meningitis, empiric therapy,
adjunctive therapy, meningococcal
vaccine.
Introduction:
Meningitis is an acute inflammation of
leptomeninges and CSF caused by
mainly bacteria, virus and less
commonly fungus which has 50% case
fatality rate if untreated. The most
common symptoms are a stiff neck, high
fever, sensitivity to light, confusion,
headaches and vomiting. This disease
has worldwide distribution. But Sub
Saharan countries are labeled as
‘Meningitis belt’ due to overwhelming
epidemic of meningitis. It has a high
death rate with severe complications
such as mental retardation, difficulty in
hearing, which may disable the person
for life time. Meningitis is potentially
fatal and should always be viewed as a
medical emergency. Thus early
diagnosis and effective management of
suspected cases of meningitis will lead
to significantly reduction in mortality. In
this article the latest modes of diagnosis
and treatment have been discussed
along with preventive measure.[15][1][8]
Methods:This study was done by
reviewing 15 journals, online clinical
articles and clinical books from June,
2013 to July, 2013.
Body of the article:
Epidemiology:
Bacterial meningitis occurs in about 3
people per 100,000 annually in Western
countries. Sub-Saharan Africa
experienced large epidemics of
meningococcal meningitis for over a
century which is labeled the "meningitis
belt". Attack rates of 100–800 cases per
100,000 are encountered in this
area.[8]Regional averages ranged from 1
to 15 per 100,000 population in children
age one to four.[7]
The death rate of about 10% for treated
meningococcal meningitis occurs even
when the public is aware of the disease
and health care is prompt. In sub-
Saharan Africa, death rates as high as
30% have been reported. At least 75 000
children are likely to have sustained
central nervous system injury after cure
of their meningococcal meningitis. [9]
Etiology:
Meningitis usually results from a viral
infection, but the cause may also be a
bacterial infection. Less commonly, a
fungal infection may cause meningitis.

ISJM
10 Issue 01 / September 2013 isjm.kaznmu.kz
Because bacterial infections are the most
serious and can be life-threatening,
identifying the source of the infection is
an important part of developing a
treatment plan.[10]
Clinical assessment:
Classic clinical presentations are fever,
headache, stiff neck & alterations in
mental status.95% of patients with
culture-proven bacterial meningitis
present with at least two of these signs
or symptoms.Nuchal rigidity occurs in
70% of adult cases. There are some
special signs of
meningismincludingKernig’s sign,
Brudzinski’s sign and positive jolt
accentuation test.Other physical
examinations includeseizure activity,
signs of increased ICP, rash of
meningococcemia, signs of Fulminate
meningococcemia[1]
Evidence of severe meningeal irritation
is generallyabsent or minimal in viral
meningitis. Signs of encephalitis often
present in HSV-1. Viral meningitis is
usually self-limiting&
withoutneurological sequelae. [2]
Lab diagnosis:
Blood cultures positive in 50-60% cases
of bacterial meningitis & detect
Arbovirus, Enterovirus, and LCMV.[2]
CSF Analysis:
Gram’s stain demonstrates organisms in
>60% of untreated cases (specificity
>97%).CSF Culture are positive in (70-
85)% of untreated bacterial meningitis &
(30-70)% in viral meningitis.Latex
agglutination test is most useful for
pretreated patients & Gram’s stain &
CSF culture negative cases. Limulus
amebocyte lysate assay detects gram-
negativeendotoxin.[3]
PCR detects bacterial DNA in pretreated
& Gram’s stain & CSF culture negative
cases. PCR detects two-thirds of culture-
negative cases of viral etiology.[2] But
PCR and ICT shows 100% specificity in
detection of bacterial cases.[11]
In bacterial etiology following CSF
profile is found:
1. Elevated opening pressure:
>180 mmH2O in more than 90% of
patients
>400 mmH2Oin 20% of patients
2. Leukocyte count:
10/μL to 10,000/μL, neutrophil are
predominant
3. Glucose level: Low (< 40 mg/dL)
4. CSF/serum glucose ratio:< 0.4 in
60% of patients
5. Protein level: >45 mg/dL in 90% of
patients[2]
In viral etiology following CSF profile is
found:
1. Normal or mildly elevated opening
pressure: 100–350 mmH2O
2. Leukocyte count: <100–1000 cells
per μL, lymphocytes are
predominant
3. Protein level: Normal
4. Glucose level: Normal
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 11
In either bacterial or viral etiology
following CSF profile is found:
1. CSF lactate
concentration:>4.2mmol/L
2. Elevated CSF concentration of CRP
3. Elevated serum concentrations of the
polypeptideprocalcitonin[1]
CT or MRI is not diagnostic. MRI
preferred in demonstrating areas of
edema & ischemia. Meningeal
enhancement often seen [2]
Indication of CT prior to lumbar
puncture:
a. Immunocompromised state
b. History of Mass lesion, stroke, or
focal infection
c. New onset seizure (Within 1 week
of presentation)
d. Papilloedema (Presence of
venous pulsations suggests
absence of increased ICP)
e. Reduced level of consciousness
f. Focal neurologic deficit
g. Patients with coagulopathy &
taking anticoagulants [1]
Differential diagnosis:
Encephalitis
Subarachnoid haemorrhage
Septic thrombosis of the superior
sagittal sinus
Focal infectious intracranial mass
lesions[2]
Treatment plan:
a. Empiric therapy
b. Specific therapy
c. Adjunctive therapy:
Dexamethasone
d. Criteria for outpatient
antimicrobial therapy & antiviral
therapy
e. Treatment of special situation [3]
Empiric therapy:
Antimicrobial therapy is administered
before the patient’s level of
consciousness deteriorated to 10 on the
Glasgow Coma Scale to reduce mortality
& neurologic complication.[3]
Empiric antimicrobial therapy should be
initiated as soon as possible after
diagnosis proven or suspected.
Antimicrobial therapy should not await
CT or MRI or lumbar puncture. Blood
cultures should be obtained. Empiric
therapy should include a combination of
a third- or fourth-generation
cephalosporin plus vancomycin plus
Acyclovir. Ampicillin & gentamicin
should be added to the empiricregimen
in patients in whom L.
monocytogenesmay be the causative
organism. Doxycycline should be added
to the empiric regimen in patients with a
rash. Combination of
vancomycin&ceftazidime, cefepimeor
meropenemshould include in
neurosurgical patients & in hospital-
acquired meningitis. Increased ICP
should be managed emergently.[4]
Specific therapy:
ISJM
12 Issue 01 / September 2013 isjm.kaznmu.kz
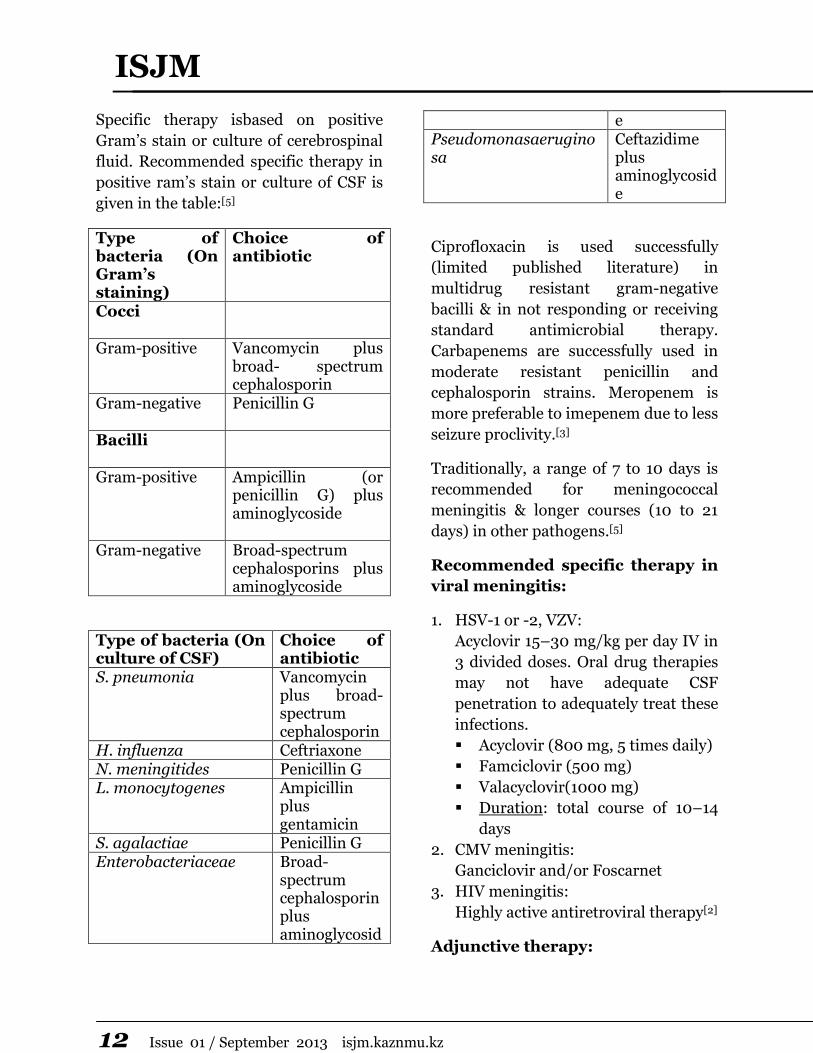
Specific therapy isbased on positive
Gram’s stain or culture of cerebrospinal
fluid. Recommended specific therapy in
positive ram’s stain or culture of CSF is
given in the table:[5]
Type of bacteria (On Gram’s staining)
Choice of antibiotic
Cocci
Gram-positive Vancomycin plus broad- spectrum cephalosporin
Gram-negative
Penicillin G
Bacilli
Gram-positive Ampicillin (or penicillin G) plus aminoglycoside
Gram-negative Broad-spectrum cephalosporins plus aminoglycoside
Type of bacteria (On culture of CSF)
Choice of antibiotic
S. pneumonia Vancomycin plus broad-spectrum cephalosporin
H. influenza Ceftriaxone N. meningitides Penicillin G L. monocytogenes Ampicillin
plus gentamicin
S. agalactiae Penicillin G Enterobacteriaceae Broad-
spectrum cephalosporin plus aminoglycosid
e Pseudomonasaeruginosa
Ceftazidime plus aminoglycoside
Ciprofloxacin is used successfully
(limited published literature) in
multidrug resistant gram-negative
bacilli & in not responding or receiving
standard antimicrobial therapy.
Carbapenems are successfully used in
moderate resistant penicillin and
cephalosporin strains. Meropenem is
more preferable to imepenem due to less
seizure proclivity.[3]
Traditionally, a range of 7 to 10 days is
recommended for meningococcal
meningitis & longer courses (10 to 21
days) in other pathogens.[5]
Recommended specific therapy in
viral meningitis:
1. HSV-1 or -2, VZV:
Acyclovir 15–30 mg/kg per day IV in
3 divided doses. Oral drug therapies
may not have adequate CSF
penetration to adequately treat these
infections.
Acyclovir (800 mg, 5 times daily)
Famciclovir (500 mg)
Valacyclovir(1000 mg)
Duration: total course of 10–14
days
2. CMV meningitis:
Ganciclovir and/or Foscarnet
3. HIV meningitis:
Highly active antiretroviral therapy[2]
Adjunctive therapy:
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 13
Dexamethasone is administered as soon
as possible if lumbar puncture reveals
any of the following:
Frankly purulent CSF
CSF WBC count >1000/microlitre
Raised CSF WBC count with protein
concentration >1 g/litre
Bacteria on Gram stain [2]
Most likely to benefit are those with a
high concentration of bacteria in CSF
(positive Gram’s stain of CSF) and
evidence of increased ICP.[6]
The recommended dose is 0.6
mg/kg/day in 4 divided doses
(0.15mg/kg/dose) given intravenously
for the first 4 days of antibiotic therapy.
The first dose of dexamethasone should
be administered before or at least with
the first dose of antibiotic. Decrease
CNS concentration of vancomycin with
concurrent steroid use. Mortality to
pneumococcal meningitis reduced from
34% to 14%. Reduce fatality, hearing
loss & neurologicalsequelae.[3]
Patients with septic shock & adrenal
insufficiency get benefit from steroid
therapy in physiological doses & longer
duration. [1]
Criteria for outpatient
antimicrobial therapy:
Inpatient antimicrobial therapy for >
6 days
Absence of fever for at least 24 – 48
h prior to initiation of outpatient
therapy
No significant neurologic
dysfunction, focal findings or seizure
activity
Clinical stability or improving
condition
Ability to take fluids by mouth
Reliable intravenous line and
infusion device (if needed)
Availability of physician, nurse,
laboratory monitoring &
emergencies[3]
Criteria for outpatient in antiviral
therapy:
Immunocompetent patient with
presumed viral meningitis
No focal signs or symptoms
No significant alteration in
consciousness
Classic CSF profile
Adequate provision for monitoring at
home and medical follow-up can be
ensured[2]
Treatment of special situation:
1. Acute meningococcaemia:
Cases are isolated (if possible) until
they have had >12 hours antibiotic
treatment. Empiric therapy is
Cefotaxime or Chloramphenicol
alternative. Benzylpenicillin is
specific drug. Often peripheral
perfusion is needed 40 ml/kg or
more in the first hour.
2. Fulminant meningococcemia:
Drug of choice is Benzylpenicillinand
Chloramphenicol is alternative.
Ceftriaxone is commonly employed
today. Hydrocortisone is used for

ISJM
14 Issue 01 / September 2013 isjm.kaznmu.kz
hypoadrenal shock. Plastic surgery
and grafting is done in tissue
necrosis.
3. Increased ICP:
Patient’s head should be elevated at
30° to 45°. Intubation is done in
hyperventilation (PCO2 25–30
mmHg). Mannitolis administered.
Patient is monitored ICU.Use ICP
monitoring device for accurate
monitoring possibly drainage of CSF [2]
Complications:
Bacterial meningitis results in
substantial morbidity and mortality
despite the availability of effective
antimicrobial therapy. Complications
due to bacterial meningitis can be
divided into systemic and neurologic.
Systemic complications such as septic
shock, disseminated intravascular
coagulation, acute respiratory distress
syndrome, and septic or reactive
arthritis, are usually the consequence of
the bacteremia that frequently
accompanies meningitis. The neurologic
complications of bacterial meningitis
include:
Impaired mental status
Increased intracranial pressure and
cerebral edema
Seizures
Focal neurologic deficits (eg, cranial
nerve palsy, hemiparesis)
Cerebrovascular abnormalities
Sensorineural hearing loss
Intellectual impairment[12] [13]
Prevention:
Meningitis typically results from
contagious infections. Common bacteria
or viruses that can cause meningitis can
spread through coughing, sneezing,
kissing, or sharing eating utensils, a
toothbrush or a cigarette. A person is
also at increased risk if he lives or works
with someone who has the disease.
These steps can help prevent meningitis:
Wash your hands
Practice good hygiene
Stay healthy
Cover your mouth during cough or
sneeze
Immunizations:
Some forms of bacterial meningitis are
preventable with the following
vaccinations:
Haemophilusinfluenzae type b
(Hib): vaccine. Children in the
United States routinely receive this
vaccine as part of the recommended
schedule of vaccines.
Pneumococcal conjugate vaccine
(PCV7): This vaccine is part of the
regular immunization schedule for
children younger than 2 years in the
United States
Haemophilusinfluenzae type b and
Neisseria meningitidisserogroups C
and Y vaccine (Hib-MenCY)
Pneumococcal polysaccharide
vaccine (PPSV)
Meningococcal conjugate vaccine
(MCV4)

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 15
This vaccine can also be given to
younger children who are at high risk of
bacterial meningitis or who have been
exposed to someone with the disease.
It's approved for use in children as
young as 9 months old. It's also used to
vaccinate healthy people who have been
exposed in outbreaks but have not been
previously vaccinated. [10]
Meningococcal A conjugate
vaccineelicited a stronger response to
group A antibody than the tetravalent
vaccine.[14]
Conclusion:
Early recognition and initiation of
appropriate empiric therapy can reduce
the mortality to 10%. If rapid and
specific identification of the
etiologicagent is done and adjusting
therapies are given as indicated, it will
efficiently manage a patient with
meningitis. Optimize management is
possible in complicating features.
Prevention can be done in epidemic
areas by proper vaccination mentioning
MCV4 and HIB vaccine.
References:
1. Infection thelancet.com Volume 7,
March 2007
2. Harrison’s Principles of Internal
Medicine, 17th edition
3. Tunkel et al., Practice Guidelines for
Bacterial Meningitis,CID 2004:39 (1
November)
4. Saunders manual of Neurologic
Practice
5. The New England Journal of
Medicine, 712, March 6, 1997
6. The New England Journal of
Medicine; Volume 336 Number 10
7. http://www.ncbi.nlm.nih.gov/books
/NBK11768/
8. http://en.wikipedia.com/meningitis
9. Bulletin of the World Health
Organization 2003, 81 (10)
10. http://www.mayoclinic.com/health/
meningitis/
11. Bangladesh J Microbiol, Volume 24,
Number 1, June 2007, pp 24-29
12. Pfister HW, Feiden W, Einhäupl
KM. Spectrum of complications
during bacterial meningitis in adults.
Results of a prospective clinical
study. Arch Neurol 1993; 50:575.
13. Durand ML, Calderwood SB, Weber
DJ, et al. Acute bacterial meningitis
in adults. A review of 493 episodes.
N Engl J Med 1993; 328:21
14. N Engl J Med 2011; 364:2293-2304
15. http://www.who.int/mediacentre/fa
ctsheets/fs141/en/index.htm

ISJM
16 Issue 01 / September 2013 isjm.kaznmu.kz
THE ETIOLOGICAL STRUCTURE AND CLINICAL EPIDEMIOLOGICAL
FEATURES OF VIRAL MENINGOENCEPHALITIS IN CHILDREN
N.B.Tukhanova E-mail: [email protected] Kazakh National Medical University named after S.D Asfendiyarov, Almaty, Kazakhstan
Keywords: viral meningoencephalitis, children.
Actuality
Viral meningoencephalitis in children are not only life-threatening conditions, but also has social importance as the impact on future child’s devolopment social adaptation. The viral meningoencephalitis are 25-38% in the structure of infections diseases of the nervous system. Many of them are characterized by severe, high probability of gross residual central nervous system and significant mortality. The difficulties in the diagnosis of viral infection of the central nervous system, especially in babies, limited of etiotropic drugs, complications leading to disability and child mortality and responsible for high urgency of the problem of viral encephalitis;
Aim of study
To analyse the etiology structure and epidemiological, clinical viral meningoencephalitis in children period of 2001-2010 year hospitalized in Children Infection Diseases Hospital in Almaty.
Materials and method
We have studied 48 patients since 0 to 14 years old, who had admitted to department Infection Diseases Hospital, is there: herpesmeningoencephalitis – 18,8%, CMV meningoencephalitis –
12,5%,measlesmeningoencephalitis – 8,3%, mixed meningoencephalitis (Herpes+CMV) – 29,2%,unknown etiologymeningoencephalitis – 31,2%.
The majority of cases the children were under 6 months of age 45,8%, the least number of cases were children from 4-6 years – 6,3%.
All children admitted complications premorbid background, mostly anemia 31.2%, pathology of pregnancy and childbirth 22.9%. In the analysis of cerebrospinal fluid in patients with viral meningoencephalitis – 83% of the cases observed lymphocytic pleocytosis and increased protein. The major complications of herpes virus, CMV and mixed meningoencephalitis in children has been the development of edema, hemi-paraparesis and atrophic changes in the brain
Fatalities in viral meningoencephalitis came 1/3 cases, they were mostly children under the age of 6 months. In all cases, death occurred due to the development of edema and swelling of the brain, organ failure
Conclusions:
1. Viral meningoencephalitis occurs in children with complicated background;
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 17
2. The most of the children were of the first six months of life – 45,8%;
3. In the etiological structure of more than met mixed meningoencephalitis29,2%
4. The main complications of viral encephalitis in children has been the development of edema,hemi-paraparesis and atrophic changes in the brain;
The 31,2% of patients had fatal issues.

ISJM
18 Issue 01 / September 2013 isjm.kaznmu.kz
MODULATION OF INTESTINAL TIGHT JUNCTION PROTEINS BY NUTRIENTS
Siti Sarah Binti Ahmad Shahidan, Mohammed Nasimul Islam, Jesmine Khan.
E-mail: [email protected]
Faculty of Medicine, Universiti Teknologi MARA (UiTM)
Sungai Buloh, Selangor, Malaysia
Introduction
Beside its main function of digestion and
absorption, intestinal mucosa acts as an
important barrier to toxic and harmful
materials and protects an individual from
different antigenic and inflammatory
reactions. The intestinal barrier is
composed of a mucin layer covering the
cells, enterocytes and the apical junctional
complex between cells (Nusrat A 2000).
The apical junctional complex consists of a
network of tight junction proteins and the
adherens junction (Mitic LL 1998). They are
anchored in the cell via the filamentous
actin cytoskeleton (Ivanov A 2004). Zonula
occludens proteins (ZO-1, ZO-2 and ZO-3)
are important intracellular tight junction
proteins, linking the cell cytoskeleton to the
transmembrane TJ proteins such as
claudins, occludin and junctional adhesion
molecules (JAM). Whereas occludin and
JAM have a regulatory role, transmembrane
protein claudins, abundantly present
between adjacent healthy intestinal
epithelial cells, are mainly responsible for
the intestinal barrier function (Turksen K
2004). Recently, disruption of the above
mentioned structures during several
physiological or pathological conditions has
been reported, which were associated with
impaired intestinal barrier function and
lead to the passage of intraluminal solutes
into the systemic circulation (Rahner C
2001, Saudi WSW 2009, Suzuki T 2010).
Investigations showed that the changes of
intestinal barrier function were mainly due
to the relaxation of the tight-junction
between intestinal epithelial cells
(Gasbarrini G 1999).
Objective of the study
To review whether intestinal disrupted
TJP can be modified or returned back to
normal by nutrients.
Materials and Methods
We found a total of 112 studies using the key
words, claudin, occludin, junctional
adhesion molecule, intestinal tight junction
proteins and nutrients. Most of the studies
dealt with the effect of probiotics on
intestinal TJP. To include and discuss all the
studies is beyond the scope of this poster.
Hence, we will give an overall idea of the
effects of nutrients on the intestinal TJP.

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 19
Results
Table I: Effect of different nutrients on modulating the tight junction proteins of gastrointestinal barrier.
Nutrients Methods used Findings Author
Glutamine Electron microscopy Prevented total
parenteral nutrition
induced loss of ZO-1
expression along the
apical surface of
intestinal epithelial cells
in rats.
Nose K 2010
Zinc
Electron microscopy Percentage of the
disrupted tight
junctions in
experimental colitis
were reduced by 50%
with zinc in mice.
Sturniolo GC 2002
Vitamin A PCR Treatment with retinoic
acid enhanced the
expression of claudin-2
of intestinal Caco-2
cells.
Baltes S 2004
Probiotics RT PCR Prevented acute colitis
induced decreased
expression and
redistribution of tight
junction proteins
occludin, zonula
occludens-1, and
claudin-1, -3, -4, and -5
in mice.
Mennigen R 2009
Prebiotics
qPCR and
immunohistochemistry
Improved tight-
junction ZO-1 and
occludin in mice.
Schedle K 2008
ISJM
20 Issue 01 / September 2013 isjm.kaznmu.kz
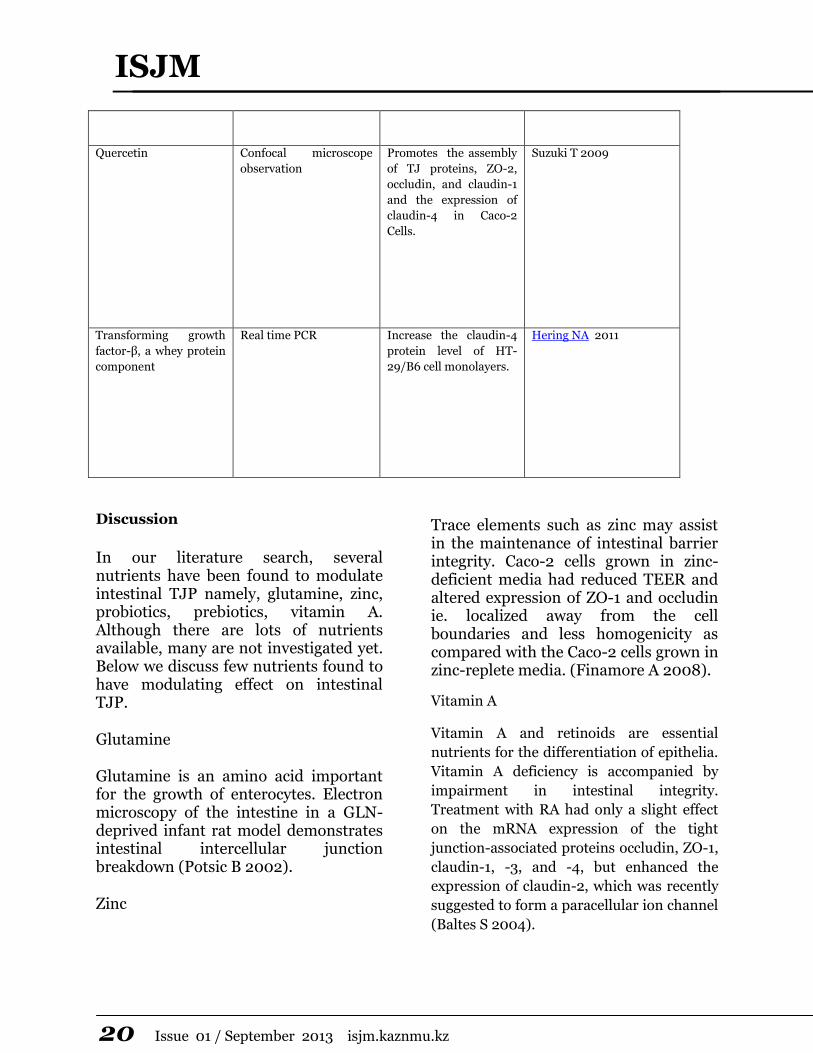
Quercetin
Confocal microscope
observation
Promotes the assembly
of TJ proteins, ZO-2,
occludin, and claudin-1
and the expression of
claudin-4 in Caco-2
Cells.
Suzuki T 2009
Transforming growth
factor-β, a whey protein
component
Real time PCR Increase the claudin-4
protein level of HT-
29/B6 cell monolayers.
Hering NA 2011
Discussion
In our literature search, several nutrients have been found to modulate intestinal TJP namely, glutamine, zinc, probiotics, prebiotics, vitamin A. Although there are lots of nutrients available, many are not investigated yet. Below we discuss few nutrients found to have modulating effect on intestinal TJP.
Glutamine
Glutamine is an amino acid important for the growth of enterocytes. Electron microscopy of the intestine in a GLN-deprived infant rat model demonstrates intestinal intercellular junction breakdown (Potsic B 2002).
Zinc
Trace elements such as zinc may assist in the maintenance of intestinal barrier integrity. Caco-2 cells grown in zinc-deficient media had reduced TEER and altered expression of ZO-1 and occludin ie. localized away from the cell boundaries and less homogenicity as compared with the Caco-2 cells grown in zinc-replete media. (Finamore A 2008).
Vitamin A
Vitamin A and retinoids are essential
nutrients for the differentiation of epithelia.
Vitamin A deficiency is accompanied by
impairment in intestinal integrity.
Treatment with RA had only a slight effect
on the mRNA expression of the tight
junction-associated proteins occludin, ZO-1,
claudin-1, -3, and -4, but enhanced the
expression of claudin-2, which was recently
suggested to form a paracellular ion channel
(Baltes S 2004).

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 21
Probiotic
Probiotics are living bacteria that, when
ingested in sufficient quantity, improve the
health of the host beyond their inherent
basic nutrition. In acute colitis, decreased
expression and redistribution of the tight
junction proteins occludin, zonula
occludens-1, and claudin-1, -3, -4, and -5
were observed, whereas VSL#3, a mixture of
8 probiotic bacterial strains therapy
prevented these changes (Mennigen R
2009).
Prebiotic
Prebiotic treated mice exhibited a decreased
hepatic expression of inflammatory and
oxidative stress markers. This decreased
inflammatory tone was associated with a
lower intestinal permeability and improved
tight-junction ZO-1 and occluding integrity
compared to controls (Schedle K 2008).
Flavonoid
Quercetin is the most common flavonoid in
nature. High amounts of quercetin are
found in onions, kale, and apples.
Flavonoids, quercetin and myricetin,
enhance barrier function in intestinal Caco-
2 cells. (Suzuki T 2009). Kaempferol, a
natural flavonoid present in fruits,
vegetables, and teas, provides beneficial
effects for human health. Confocal
microscopy showed that kaempferol-
induced assembly of occludin and claudin-3
occurred at the TJ of Caco -2 cells at 6 h
post administration (Suzuki T 2011).
Whey protein and casein peptide
Transforming growth factor-β, a whey
protein component, increase in the claudin-
4 protein level of HT-29/B6 cell monolayers
observed by real time PCR method (Hering
NA 2011).Casein peptide up-regulated the
expression of the occludin gene in cells, but
the level of the genes of the claudin family
and zonula occludens-1 (ZO-1) was
unchanged. Increased protein expression of
occludin, but not of claudin-1 or of ZO-1,
was also observed in Caco-2 cells using the
microarray method (Yasumatsu 2010).
Conclusion
Although still at the conceptual level,
evidences are persuasive that use of the
certain compounds, such as zinc, glutamine,
probiotics etc has the potential to attenuate
morphological changes by the above factors
and might represent a simple device to
prevent the occurrence or aggravation of
chronic pathologies caused by intestinal
barrier dysfunction. Future researches are
suggested to deal with the effect of several
other modulating agents on the intestinal
TJP. Therapeutic restoration of barrier
function could improve pathophysiology
and clinical outcomes of different diseases.
References
Nusrat A, Turner JR, Madara JL (2000) Molecular
physiology and pathophysiology of tight junctions. IV.
Regulation of tight junctions by extracellular stimuli:
nutrients, cytokines, and immune cells. Am J Physiol
Gastrointest Liver Physiol 279(5):G851-7.
Mitic LL, Anderson JM (1998) Molecular architecture of
tight junctions. Annu Rev Physiol 60:121-42.
Ivanov AI, McCall IC, Parkos CA, Nusrat A (2004) Role for
actin filament turnover and a myosin II motor in
cytoskeleton-driven disassembly of the epithelial apical

ISJM
22 Issue 01 / September 2013 isjm.kaznmu.kz
junctional complex. Mol Biol Cell 15(6):2639-51. Epub 2004
Mar 26
Turksen K, Troy TC (2004) Barriers built on claudins. J Cell
Sci. 117:2435–2447
Rahner C, Mitic LL, Anderson JM (2001) Heterogeneity in
expression and subcellular localization of claudins 2, 3, 4,
and 5 in the rat liver, pancreas, and gut. Gastroenterology
120(2):411-422
Saudi WSW, Khan J, Islam MN (2009) Small intestinal
morphology and permeability in chronic water avoidance
stress in rats. IMJ16(2), 87-91
Suzuki T, Hara H (2010) Dietary fat and bile juice, but not
obesity, are responsible for the increase in small intestinal
permeability induced through the suppression of tight
junction protein expression in LETO and OLETF rats. Nutr
Metab (Lond) 12;7-19
Gasbarrini G, Montalto M (1999) Structure and function of
tight junctions. Role in intestinal barrier. Ital J Gastroenterol
Hepatol.1999 Aug-Sep;31(6):481-8.
Nose K, Yang H, Sun X, Nose S, Koga H, Feng Y, Miyasaka E,
Teitelbaum DH.Glutamine prevents total parenteral
nutrition-associated changes to intraepithelial lymphocyte
phenotype and function: a potential mechanism for the
preservation of epithelial barrier function. J Interferon
Cytokine Res. 2010 Feb;30(2):67-80.
Sturniolo GC, Fries W, Mazzon E, Di Leo V, Barollo M,
D'inca R (2002) Effect of zinc supplementation on intestinal
permeability in experimental colitis. J Lab Clin Med
139: 311–315.
Baltes S, Nau H, Lampen A. All-trans retinoic acid enhances
differentiation and influences permeability of intestinal
Caco-2 cells under serum-free conditions. Dev Growth
Differ. 2004 Dec;46(6):503-14.
Mennigen R, Nolte K, Rijcken E, Utech M, Loeffler B,
Senninger N, Bruewer M. Probiotic mixture VSL#3 protects
the epithelial barrier by maintaining tight junction protein
expression and preventing apoptosis in a murine model of
colitis. Am J Physiol Gastrointest Liver Physiol. 2009
May;296(5):G1140-9. doi: 10.1152/ajpgi.90534.2008. Epub
2009 Feb 12.
Schedle K, Pfaffl MW, Plitzner C, Meyer HH, Windisch W
(2008) Effect of insoluble fibre on intestinal morphology and
mRNA expression pattern of inflammatory, cell cycle and
growth marker genes in a piglet model. Arch Anim Nutr.
62(6):427-38.
Suzuki T, Hara H (2009) Quercetin Enhances Intestinal
Barrier Function through the Assembly of Zonnula
Occludens-2, Occludin, and Claudin-1 and the Expression of
Claudin-4 in Caco-2 Cells. J Nutr: 139(5), 965-97
Takuya Suzuki, Soichi Tanabe and Hiroshi Hara (2011)
Kaempferol Enhances Intestinal Barrier Function through
the Cytoskeletal Association and Expression of Tight
Junction Proteins in Caco-2 Cells. J Nutr: 141(1), 187-94
Vreeburg RA, van Wezel EE, Ocaña-Calahorro F, Mes JJ.
Apple extract induces increased epithelial resistance and
claudin 4 expression in Caco-2 cells. J Sci Food Agric. 2012
Jan 30;92(2):439-44. doi: 10.1002/jsfa.4598. Epub 2011 Oct
3.
Hering NA, Andres S, Fromm A, van Tol EA, Amasheh M,
Mankertz J, Fromm M, Schulzke JD.Transforming growth
factor-β, a whey protein component, strengthens the
intestinal barrier by upregulating claudin-4 in HT-29/B6
cells. J Nutr. 2011 May;141(5):783-9. doi:
10.3945/jn.110.137588. Epub 2011 Mar 23.
Yasumatsu H, Tanabe S.The casein peptide Asn-Pro-Trp-
Asp-Gln enforces the intestinal tight junction partly by
increasing occludin expression in Caco-2 cells. Br J Nutr.
2010 Oct;104(7):951-6. doi: 10.1017/S0007114510001698.
Epub 2010 May 19.
Finamore A, Massimi M, Conti Devirgiliis L, Mengheri E
(2008) Zinc deficiency induces membrane barrier damage
and increases neutrophil transmigration in Caco-2 cells. J
Nutr 138:1664–70.
Lihua Wang, Yuzhu Tang, Deborah C. Rubin, and Marc S.
Levin (2007) Chronically administered retinoic acid has
trophic effects in the rat small intestine and promotes
adaptation in a resection model of short bowel syndrome.
Am J Physiol Gastrointest Liver Physiol. 292(6):G1559-69.
Epub 2007 Feb 15.
M Zareie, K Johnson Henry, J Jury, PC Yang, BY Ngan, D M
McKay, J D Soderholm, M H Perdue, and P M Sherman
(2006) Probiotics prevent bacterial translocation and
improve intestinal barrier function in rats following chronic
psychological stress. Gut: 55(11): 1553–1560.
Schedle K, Pfaffl MW, Plitzner C, Meyer HH, Windisch W
(2008) Effect of insoluble fibre on intestinal morphology and
mRNA expression pattern of inflammatory, cell cycle and
growth marker genes in a piglet model. Arch Anim Nutr.
62(6):427-38.
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 23
IDENTIFICATION OF SYMPTOMS
OF A STRESS AT STUDENTS
DURING CARRYING OUT IN
EXAMS
Akkazhieva N.N., Nuritdinova M.M.
E-mail: [email protected]
Scientific supervisors: Xasenova K.X., Biserovad
S.D Asfendiyarov Kazakh National Medical
University, Almaty, Kazakhstan
Actuality
It is shown that at a stress various
physiological functions are broken down
in works of foreign scientists. Our
university transited on credit system
from this year, according to which the
greatest attention is given to
independent work at acquisition of
knowledge of students, in this regard the
number of lectures and a practical
training was sharply reduced, duration
of a term made to 15 weeks. As a result,
the emotional and academic loading
increased on students. And to those
students to whom aren't indifferent their
estimates, it is necessary to strain
considerably during exams which we
pass nearly an every week. A revealing
the changes happening at us in our
organism during adaptation to
educational process was aim of our task.
Methods and material of research
The main method of work was to
conduct a two- stage survey of 50
students of 2nd course of the faculty
general medicine during regular
sessions within 15-19 November 2012
and at the time of control with a
landmark 22-29 November 2012 for
the studied subjects physiology and
biochemistry. Determined the
following performance:
1. Pulse rate - per minute;
2. Consentration of attention;
3. Level of memory;
4. Estimate the internal state of the
adapted Coleman test.
Results of research
We observed that majority of students
(93%) has a small increase of frequency
of the pulse in minute till 73-81 during
delivery of exams, whereas:
1. Pulse rate is about 70-77 in rest.
2. Consecration of attention to
extraneous stimuli (tables to determine
attention) during quiz reduced for 16%
than in the rest.
3. The number of students which
showed the excellent level of memory in
rest and during delivery of control is
observed from 46% from 100% to 29%
from 100% .
4. During control among students the
level of irritability is increased from 34%
to 41%, i.e. for 7% is observed.
Conclusion
It is possible on the basis of results
of research to assume that exams
acting as a stressful factor can have
negative impact on an organism of
students. The influence of stress
factor amplifies during session and
we can judge a condition of an
organism of students during this
period. All feel an emotional stress
differently therefore it is necessary
to adapt ourselves for such
influences since continuous
influences such can lead to
ISJM
24 Issue 01 / September 2013 isjm.kaznmu.kz
development of various
pathological conditions gradually.
Thus, planned the exams, carried
out during a semester, adaptations
of an organism of students to the
forthcoming examinations promote.

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 25
ATRIAL FIBRILLATION AND VEGETATIVE NERVOUS SYSTEM STATUS:
PRE-HOSPITAL TREATMENT AND MANAGEMENT TACTICS
V.G. Epifanov, V.T. Dolgikh
Omsk State Medical Academy, Lenin Str. 12, Omsk 644043, Russia
Epifanov V.G. — post-graduate student the Omsk State Medical Academy. Krasnoznamennaya Str. 20, apt. 19, Omsk 644013,
Russia. Phone: (3812) 60-01-14. Mobile phone: 8-904-321-1763. E-mail: [email protected]
Dolgikh V.T. — Honored Science Worker of the Russian Federation, Academician of the Russian Academy of Medical-Technical
Sciences, Doctor of Medical Sciences, Professor, holder of the Chair of Physiopathology with a course in clinical physiopathology at
the Omsk State Medical Academy. Lenin Str. 12, Omsk 644043, Russia. Phone: (3821) 23-03-78
Mobile phone: 8-913-155-28-60. E-mail: [email protected]
Keywords: atrial fibrillation, acute medical care at pre-hospital stage, vegetative tonus.
Abstract
A comparative retrospective study of
1009 cases of acute care rendered to
patients with atrial fibrillation episodes
was made, and tactics of pre-hospital
management of such patients were
evaluated. It was shown that the onset of
atrial fibrillation episode at pre-hospital
stage is accompanied by a pronounced
vegetative imbalance. Antiarrhythmic
therapy of atrial fibrillation with
diazepam rapidly reduces
sympathicotonia at pre-hospital stage
and increases the treatment efficacy in
the first hour of the patient’s follow-up.
Introduction
Atrial fibrillation (AF) is the most
common cardiac arrhythmia
encountered in clinical practice,
particularly in the practice of acute care
doctor. AF accounts nearly for one third
of hospitalizations due to cardiac
rhythm disturbances [5]. In two recent
decades, the admission rate of AF
patients has risen by a factor of 2-3; on
the one hand, this increased the
treatment cost, and on the other hand,
led to the development of novel
therapies for this category of patients
[4].
Among patients with cardiovascular
pathology who appealed for acute
medical care, those with AF episodes
constitute about 10%. The prevalence of
atrial fibrillation in a general population
amounts to 0.5%, increases with age and
in the presence of organic heart
pathology, and exceeds 6% among
persons older than 80. 23.3% of patients
with paroxysmal and 28.4% with
persistent AF show the increased clinical
anxiety and depression as compared to
patients without heart rhythm
disturbances [3]. An important role of
psychovegetative disorders in patients
with paroxysmal AF was proved; in
some paroxysmal AF patients, an
obvious similarity between subjective
symptoms of AF episode and the
symptoms of a panic attack was
demonstrated [6]. The development of
atrial fibrillation and related changes in
the life pattern (disabling,
hospitalization, etc.) may give rise to
pronounced mental troubles in patients
[8].
As early as in the 1950s, a relation
between AF onset and tonus of the
vegetative nervous system was reported
[10]. Further studies proved empirically
that electrophysiological properties of
cardiomyocytes can be impaired under
the action of vegetative nervous system,
and AF paroxysms can be caused by
changes in the vegetative tonus. Vagal

ISJM
26 Issue 01 / September 2013 isjm.kaznmu.kz
and sympathetic effects modulate
electrophysiological characteristics of
the atrial cells (duration of the action
potential, refractoriness, and conduction
velocity). Parasympathetic stimuli
facilitate the re-entry mechanism,
whereas sympathetic stimuli promote
the trigger activity [9].
Psychoneurological disorders aggravate
the course of atrial fibrillation,
complicate the clinical presentation,
increase the rate of emergency calls,
raise the number of unnecessary assays
and hospitalizations, and strongly affect
the patients’ quality of life [8].
Evidently, topicality of the problem of
psychosomatic disorders observed in AF
patients is determined not only by their
prevalence and disadapting effect, but
also by the fact that timely treatment of
these disorders often becomes a crucial
factor in efficacious therapeutic and
particularly acute care. This makes
pathogenetically valid the use of
psychopharmacological preparations
normalizing the tonus of the vegetative
nervous system during pre-hospital
acute care rendered to patients with AF
episodes.
In this connection, taking into account
the current reform of acute care service
and the usual shortage of time at pre-
hospital stage, the problems of acute
therapy and management tactics applied
to atrial fibrillation patients at pre-
hospital stage are very important.
Aim of the study
Using a comparative retrospective
analysis of the therapy data for patients
with atrial fibrillation episodes, to study
the efficacy of combined administration
of antiarrhythmic preparations and
diazepam during acute medical care and
evaluate the tactics of patients’
management and the state of vegetative
nervous system in this category of
patients at pre-hospital stage.
Materials and Methods
The comparative retrospective study
considered the results of acute medical
care rendered to 1009 patients with
uncomplicated atrial fibrillation
episodes lasting up to 24 hours. Of
them, 903 patients (the 1st group)
received only antiarrhythmic
preparations, and 106 patients (the 2nd
group) received a combined therapy
with antiarrhythmics and diazepam. The
duration of a single AF episode ranged
from 30 minutes to 28 hours, the
duration of “arrhythmic anamnesis”
lasted from 2-3 months to 27 years. The
mean age of the patients was 68.3±10.93
years (from 22 to 96). The analysis was
made using the cards of emergency calls,
outpatient cards from polyclinics, and
case histories from hospitals.
The study was performed using the
methods available at pre-hospital stage.
To evaluate the initial and final (after
therapy) vegetative status of patients,
the vegetative Kerdo index (VI) was
calculated, and blood minute volume
(MV) was examined by the Lilye-
Shtrander and Zander indirect method.
The Hildebrand coefficient (Q) was
employed to calculate intersystem
cardiorespiratory ratios [1].
Electrocardiographic control and
recording of arterial pressure (AP) were
performed over the entire follow-up
period.
In all the patients appealed for acute
medical care, the arrhythmia episodes
had no complications that would require
urgent electrical cardioversion.

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 27
In both groups, antiarrhythmic therapy
was performed with the preparations
included in the Standards for Acute
Medical Care [7]. The AF episode was
stopped by intravenous injection of
cordarone (amiodarone, KRKA) in a
single dose of 5 mg/kg, novocainamide
(procainamide, Organics) at a dose of
0.5-1 g, verapamil 5-10 mg (0.1 mg/kg
on the average) (Alkaloid), digoxin
0.25 mg (Nycomed), diazepam 10 mg
(seduxen, Gedeon Richter; relium,
Ciech; sibazon, Organics).
Antiarrhythmics were administered with
preliminary injection of 10 ml panangin
(Gedeon Richter). Action of the
preparations was evaluated for 50-70
minutes (on the average, for 64.1±3.2
min). The entire period of follow-up was
accompanied by ECG control and
recording of arterial pressure.
Check points of the study were as
follows: 1 h (the period of emergency
team work and patient’s follow-up), 12
and 24 h. The values are given as a mean
± standard error (M±σ). The mean time
needed to stop an AF episode and the
values of vegetative Kerdo index are
presented as “lower quartile – median –
upper quartile” (LQ-Me-UQ). Statistical
processing of the data was made using
the Mann-Whitney Test to compare
clinical parameters of the groups,
Wilcoxon Test to compare the
parameters in each group before and
after therapy, Chi-square Test) and
Fisher's Exact Test 2-tailed P to
compare the groups of patients with
respect to the relative rate of
administered antiarrhythmic
preparations. Methods of survival rate
analysis were applied: Cox's F-test and
the Cox’s regression model of
proportional intensities. Interrelations
between samples were analyzed using
the Spearman rank correlation (ρ) with
subsequent comparison of the
correlation coefficients to determine
whether their differences are stochastic.
The confidence interval taken as
statistically significant in this study was
equal to 95% (the significance level of p
was 0.05). Statistical analysis was
performed using the programs XLSTAT
2009 v. 3.02 (Addinsoft) and
STATISTICA v. 8.0 (StatSoft, Inc.) and
tabular processor Microsoft Office Excel
2010.
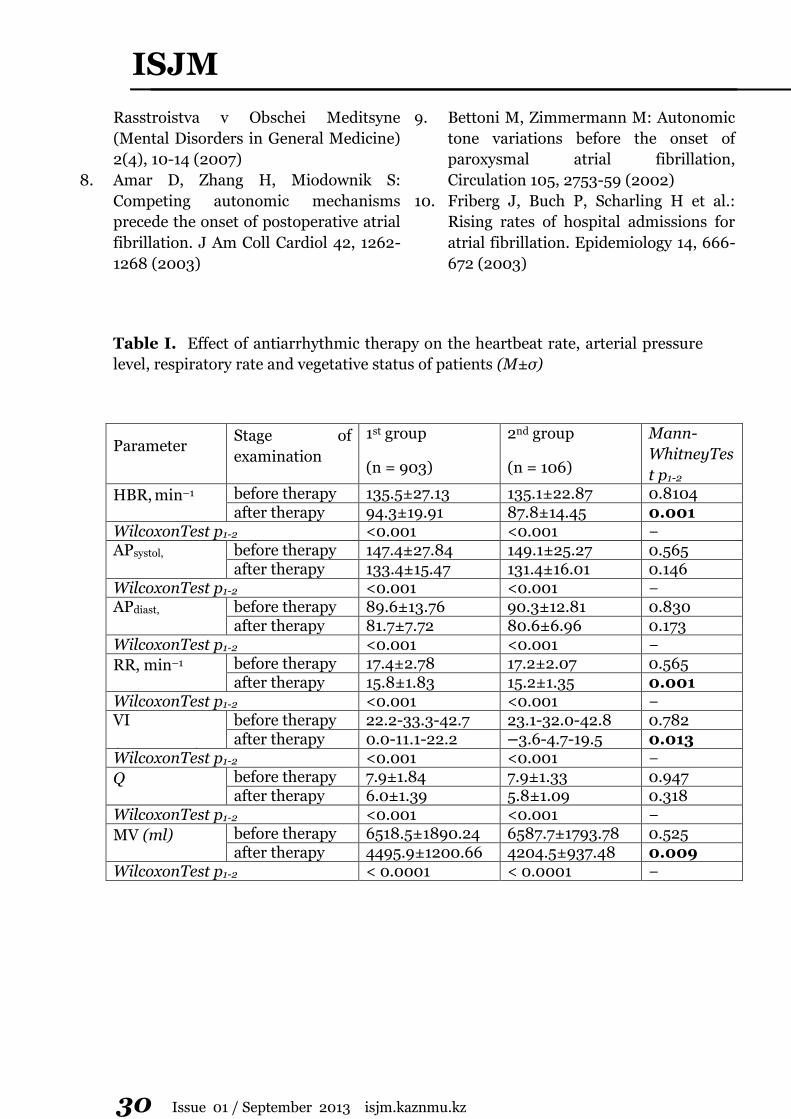
Results
Patients from both groups were found to
be comparable in age (Mann-
WhitneyTestp1-2=0,64), sex, diseases
that caused AF (Fisher'sExactTestp1-
2˃ 0,3), main clinical and hemodynamic
parameters, and antiarrhythmic
preparations used for medical care (Chi-
squaretestp1-4 = 0.27).
During the period of emergency team
work and patient’s follow-up, both
groups showed a marked improvement
in the clinical parameters. A decrease in
the heartbeat rate (HBR) and
respiratory rate (RR) was more
pronounced in the 2nd group of patients,
with statistically significant differences
between the groups (Table 1).
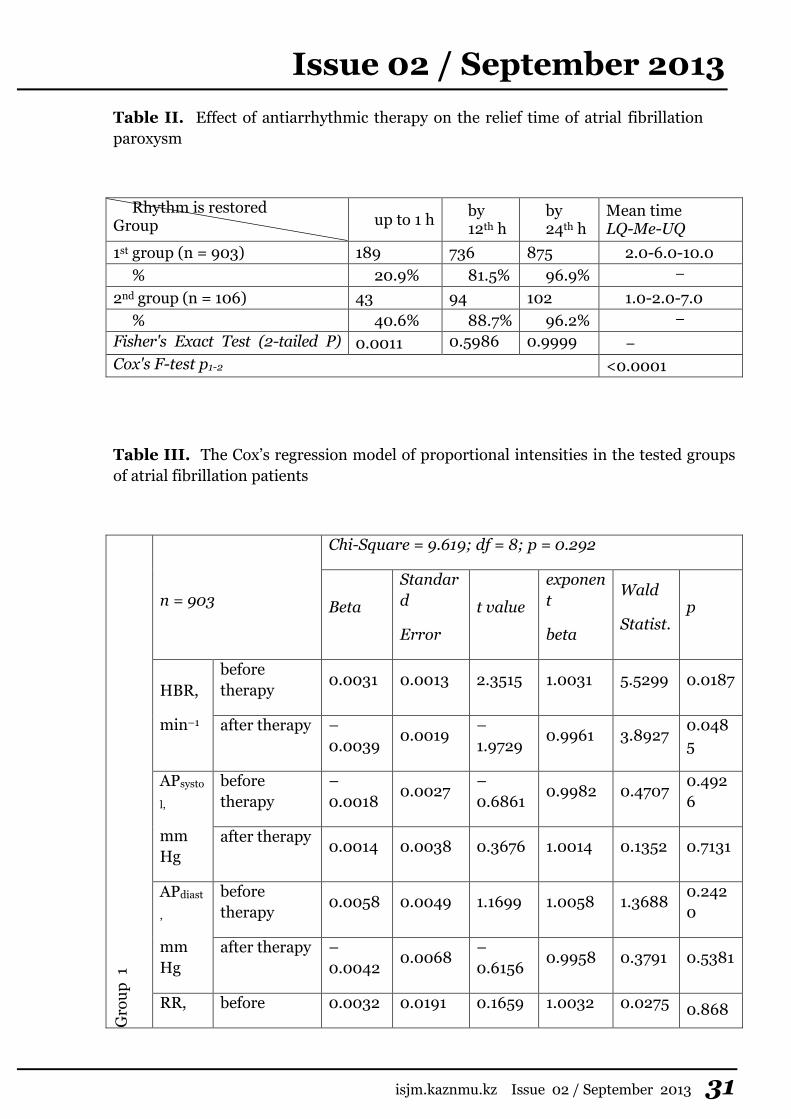
Within the first hour of the patients’
follow-up, the rhythm was restored in
20.9% of cases in the 1st group and in
40.6% cases in the 2nd group
(Fisher'sExactTestp1-2 = 0.0011). High
initial values of the vegetative index and
blood minute volume in both groups
indicated the pronounced
sympathicotonia (Table 1). The
Hildebrand coefficient in AF patients
was beyond the normal values, which

ISJM
28 Issue 01 / September 2013 isjm.kaznmu.kz
testifies to discoordination of vegetative
provision of respiratory and cardial
systems. By the end of the first hour of
follow-up, the improvement in
cardiorespiratory ratio and abatement of
sympathicotonia in the 2nd group, where
antiarrhythmic preparations were
administered in combination with
diazepam, were more pronounced than
in the 1st group. After acute care, the
value of vegetative index in the 2nd
group was 2.4 times lower as compared
to the 1st group (Table 1). In the 2nd
group, a moderate and reliable
(p < 0.0001) direct correlation
(ρVI = 0.4467 and ρMV = 0.4222)
between time of relieving the AF
paroxysm and decreasing the vegetative
index and blood minute volume was
observed. In the 1st group, the
correlation was absent (ρVI = 0.0365 at
p = 0.2617 and ρMV = 0.0315 at
p = 0.3333). The correlation coefficients
were different at a high level of
statistical significance (p < 0.0001). By
the 12th and 24th hours of follow-up, the
samples being compared had identical
characteristics of the AF paroxysm relief
time (Table 2). Such results can be
attributed not only to antiarrhythmic
therapy, but also to the fact that
spontaneous conversion of the paroxysm
may attain 66% in patients within 24 h
after the onset of arrhythmia, and only
in 17% arrhythmia can persist for a
longer period [2].
Relations between therapy and the
results obtained were analyzed using the
Cox’s regression model of proportional
intensities. In the 1st group of patients,
the analysis did not show statistically
significant correlations between therapy
and clinical parameters, between time of
relieving the AF paroxysm and the
administered antiarrhythmic
preparations (p = 0.2928 at a 8.91%
fraction of censored observations). In
the second group of patients, who
received acute care using
antiarrhythmics in combination with
diazepam, the analysis revealed a
statistically significant correlation
between these factors (p = 0.0068 at a
3.37% fraction of censored
observations). The obtained models are
described in Table 3, which shows that
the ultimate heartbeat rate in the 2nd
group is closely associated with the time
elapsed before the outcome under
consideration.
The assumption that antiarrhythmic
therapy and time of AF paroxysm relief
are not directly proportional to each
other was verified by analysis based on
the Cox’s model of proportional
intensities with time-dependent
covariates. As shown by the Chi-square
Test, there is a statistically significant
difference (Chi-square = 18.1783 at
p = 0.0001) between the models. The
model obtained in the 2nd group is
statistically significant (p = 0.0336) —
the time of AF paroxysm relief in this
group depends on the applied acute
therapy (antiarrhythmic preparations in
combination with diazepam).
Thus, the onset of AF paroxysm at pre-
hospital stage is accompanied by a
pronounced sympathicotonia. When
rendering acute care to AF patients at
pre-hospital stage, changes in the
vegetative tonus should be considered
and corrected. The combination of
diazepam with antiarrhythmic
preparations makes it possible to stop
the paroxysm promptly, often within the
first hour of the patient’s follow-up,
which prevents unnecessary

Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 29
hospitalizations and improves the
patients’ quality of life. Since AF tends
to spontaneous restoration of the
rhythm in more than a half of patients
[2] and both the decrease in heartbeat
rate and the restoration of sinus rhythm
at atrial fibrillation equally improve the
patient’s status [5], it is clear that
antiarrhythmic therapy at pre-hospital
stage should be aimed mainly at
lowering the heart’s ventricular rate
rather than reducing the arrhythmia.
In our opinion, the currently accepted
tactics of mandatory hospitalization of
the patients with uncomplicated AF
episode that lasts up to 24 hours and is
not relieved at pre-hospital stage are not
quite correct. Such tactics increase the
number of unreasonable
hospitalizations and irrational use of
hospital resources, extend the work time
of medical emergency team and
decrease the team turnover rate, thus
increasing the wait time in acute care as
well as the delay time and unjustified
financial expenditures.
Conclusions
1. Irrespective of the underlying disease
and administered antiarrhythmic
preparations, the overwhelming
majority of atrial fibrillation cases are
relieved by the end of the first day after
beginning of the treatment.
2. The onset of atrial fibrillation
paroxysm at pre-hospital stage is
accompanied by a pronounced
sympathicotonia, which should be taken
into account during antiarrhythmic
therapy. The combination of diazepam
with antiarrhythmic preparations
provides a faster relief of the AF
paroxysm.
3. In the case of uncomplicated episodes
of atrial fibrillation lasting up to 24
hours, medical care tactics at pre-
hospital stage should be aimed primarily
at normalizing the heart’s ventricular
rate and vegetative imbalance.
4. In the case of primary appeal to acute
medical care, the tactics of mandatory
hospitalization of patients with
uncomplicated atrial fibrillation episode
that lasts up to 24 hours and is not
relieved by pre-hospital treatment are
invalid.
References
1. Vegetative Disorders: Clinical Picture,
Diagnostics and Treatment. Ed. Vein
AM. Moscow: Medical Information
Agency, 2003, 752 p.
2. Pogosova GV: Psychological stress and
acknowledgement of its value as a first
order cardiovascular risk factor.
Kardiologiya (Cardiology) 2, 65-72
(2007)
3. Popov SV, Batalov RE, Antonchenko IV:
Current aspects of atrial fibrillation
treatment. Bolezni Serdtsa I Sosudov
(Cardiovascular Diseases) 1, 30-34
(2009)
4. Prokhorovich EA, Talibov OB,
Topolyansky AV: Treatment of the
rhythm and conduction disturbances at
pre-hospital stage. Lechaschiy Vrach
(Hospital Doctor) 3, 56-60 (2002)
5. Guidelines for Acute Care Doctors. Eds.
Bagnenko SF, Vertkin AL,
Miroshnichenko AG, Khubutiya MSh.
Moscow: GEOTAR-Media, 91-99 (2009)
6. Skurikhina ON, Miller ON: Anxiety and
depression in patients with paroxysmal
and persistent atrial fibrillation. Vestnik
Aritmologii (Arrhythmology Bulletin)
55, 14-18 (2009)
7. Syrkin AL, Kopylov FYu, Popova EA et
al.: Mental disorders at different stages
of atrial fibrillation. Psikhicheskie
ISJM
30 Issue 01 / September 2013 isjm.kaznmu.kz
Rasstroistva v Obschei Meditsyne
(Mental Disorders in General Medicine)
2(4), 10-14 (2007)
8. Amar D, Zhang H, Miodownik S:
Competing autonomic mechanisms
precede the onset of postoperative atrial
fibrillation. J Am Coll Cardiol 42, 1262-
1268 (2003)
9. Bettoni M, Zimmermann M: Autonomic
tone variations before the onset of
paroxysmal atrial fibrillation,
Circulation 105, 2753-59 (2002)
10. Friberg J, Buch P, Scharling H et al.:
Rising rates of hospital admissions for
atrial fibrillation. Epidemiology 14, 666-
672 (2003)
Table I. Effect of antiarrhythmic therapy on the heartbeat rate, arterial pressure
level, respiratory rate and vegetative status of patients (M±σ)
Parameter Stage of
examination
1st group
(n = 903)
2nd group
(n = 106)
Mann-
WhitneyTes
t p1-2
HBR, min–1 before therapy 135.5±27.13 135.1±22.87 0.8104 after therapy 94.3±19.91 87.8±14.45 0.001
WilcoxonTest p1-2 <0.001 <0.001 − APsystol,
Mm Hg
before therapy 147.4±27.84 149.1±25.27 0.565 after therapy 133.4±15.47 131.4±16.01 0.146
WilcoxonTest p1-2 <0.001 <0.001 − APdiast,
Mm Hg
before therapy 89.6±13.76 90.3±12.81 0.830 after therapy 81.7±7.72 80.6±6.96 0.173
WilcoxonTest p1-2 <0.001 <0.001 −
RR, min–1 before therapy 17.4±2.78 17.2±2.07 0.565
after therapy 15.8±1.83 15.2±1.35 0.001 WilcoxonTest p1-2 <0.001 <0.001 − VI
(LQ-Me-UQ)
before therapy 22.2-33.3-42.7 23.1-32.0-42.8 0.782 after therapy 0.0-11.1-22.2 –3.6-4.7-19.5 0.013
WilcoxonTest p1-2 <0.001 <0.001 −
Q before therapy 7.9±1.84 7.9±1.33 0.947 after therapy 6.0±1.39 5.8±1.09 0.318
WilcoxonTest p1-2 <0.001 <0.001 −
MV (ml) before therapy 6518.5±1890.24 6587.7±1793.78 0.525 after therapy 4495.9±1200.66 4204.5±937.48 0.009
WilcoxonTest p1-2 < 0.0001 < 0.0001 −
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 31
Table II. Effect of antiarrhythmic therapy on the relief time of atrial fibrillation
paroxysm
Rhythm is restored Group up to 1 h
by 12th h
by 24th h
Mean time LQ-Me-UQ
1st group (n = 903) 189 736 875 2.0-6.0-10.0
% 20.9% 81.5% 96.9% − − 2nd group (n = 106) 43 94 102 1.0-2.0-7.0
% 40.6% 88.7% 96.2% − − Fisher's Exact Test (2-tailed P)
p1-2
0.0011 0.5986 0.9999 −
Cox's F-test p1-2 <0.0001
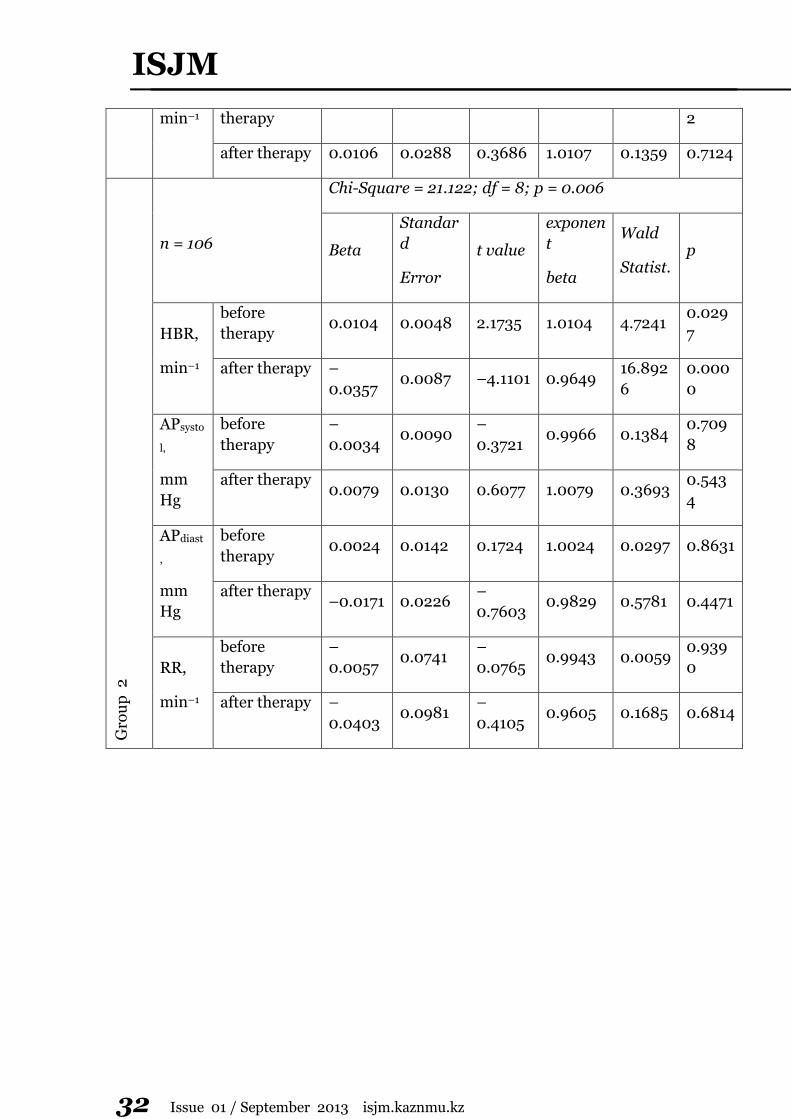
Table III. The Cox’s regression model of proportional intensities in the tested groups
of atrial fibrillation patients
Gro
up
1
n = 903
Chi-Square = 9.619; df = 8; p = 0.292
Beta
Standar
d
Error
t value
exponen
t
beta
Wald
Statist. p
HBR,
min–1
before
therapy 0.0031 0.0013 2.3515 1.0031 5.5299 0.0187
after therapy –
0.0039 0.0019
–
1.9729 0.9961 3.8927
0.048
5
APsysto
l,
mm
Hg
before
therapy
–
0.0018 0.0027
–
0.6861 0.9982 0.4707
0.492
6
after therapy 0.0014 0.0038 0.3676 1.0014 0.1352 0.7131
APdiast
,
mm
Hg
before
therapy 0.0058 0.0049 1.1699 1.0058 1.3688
0.242
0
after therapy –
0.0042 0.0068
–
0.6156 0.9958 0.3791 0.5381
RR, before 0.0032 0.0191 0.1659 1.0032 0.0275 0.868
ISJM
32 Issue 01 / September 2013 isjm.kaznmu.kz
min–1 therapy 2
after therapy 0.0106 0.0288 0.3686 1.0107 0.1359 0.7124
Gro
up
2
n = 106
Chi-Square = 21.122; df = 8; p = 0.006
Beta
Standar
d
Error
t value
exponen
t
beta
Wald
Statist. p
HBR,
min–1
before
therapy 0.0104 0.0048 2.1735 1.0104 4.7241
0.029
7
after therapy –
0.0357 0.0087 –4.1101 0.9649
16.892
6
0.000
0
APsysto
l,
mm
Hg
before
therapy
–
0.0034 0.0090
–
0.3721 0.9966 0.1384
0.709
8
after therapy 0.0079 0.0130 0.6077 1.0079 0.3693
0.543
4
APdiast
,
mm
Hg
before
therapy 0.0024 0.0142 0.1724 1.0024 0.0297 0.8631
after therapy –0.0171 0.0226
–
0.7603 0.9829 0.5781 0.4471
RR,
min–1
before
therapy
–
0.0057 0.0741
–
0.0765 0.9943 0.0059
0.939
0
after therapy –
0.0403 0.0981
–
0.4105 0.9605 0.1685 0.6814
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 33
INVESTIGATION OF STOMATITIS CAUSES AMONG THE STUDENTS AND DEVELOPMENT OF "PHYTOMEDICATION" FOR THE PREVENTION AND TREATMENT D. Sharipov E-mail: [email protected] S.D. Asfendiyarov Kazakh National Medical University, Almaty, Republic of Kazakhstan
Actuality
In the Republic of Kazakhstan among the children aged from 6 months to 16 years who applied to the dental clinic, the cases of stomatitis 90%, with 80% of acute herpetic stomatitis. Therefore, the development of effective pharmacon for the prevention and treatment of stomatitis is an urgent.
The aim of this work
To investigate the causes of stomatitis among students and its influence on their attendance and performance, as well as to provide them an effective "Phytomedication" for the prevention and treatment, handy in using and in mobile formation.
Results
The results showed that the cause factor of stomatitis is various: mechanical trauma, infections, allergies, etc., but always stomatitis causes pain, discomfort and suffering. Also revealed that one of the common reasons for the development of stomatitis and recrudescence in adolescents feedings in the times of recreation, caused no personal hygiene, lack of capability to neutralize food particles and their degradation products, leading subsequently to pathological disorders of the gastrointestinal tract.
Designed composition comprises a substance derived from medicinal plants, which have a wide range of pharmacological effects, and applicatory no side effects. The compositions include extracts of chamomile flower, which has an antibacterial, anti-
inflammatory, soothing and recovering effect. Glycyram - water-soluble salt of monoammonium of glycyrrhizic acid, a derivative of licorice root which has an anti-inflammatory, antiviral activity and has a sweet taste, also serves as a flavoring component. An extract of oak bark, contains tannin, used as an astringent. Peppermint oil was introduced to impart a pleasant odor, as well as all essential oils have antiseptic activity. Rosehip extract and oil is used in the treatment of ulcers and fissures in the oral cavity, to promote healing.
At the laboratory of Santo, Member of Polpharma Group received extractive substance and extracts from plant material, select the rational structure of auxiliary substances and developed the technology of the "Phytostom" drug. The new pharmacon is designed in optimal dosage form for students: in granular form which packed in sachets and in the plates.
The main advantages of the granular formulation and plates are high bioavailability, rapid onset of therapeutic effect, portability, an accuracy of dosing, storage stability and the possibility of correction of unpleasant sensory properties of drugs.
Conclusion
In summary, as a result of the study:
- ostended the basic reasons for the development of stomatitis among students and its negative impact on their academic performance and attendance;
- derived biologically active substances from endemic medicinal plants;

ISJM
34 Issue 01 / September 2013 isjm.kaznmu.kz
- developed the technology of the new domestic pharmacon of oral using for the prevention and treatment of stomatitis (obtained the Innovation patent of the Republic of Kazakhstan for the drug "Phytostom» № 23948).
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 35
CHANGING OF SUCCINATE DEHYDROGENASE’S (SDH’S) ACTIVITY IN
HYPOTHYROIDISM OF NEWBORN AND PREGNANT WOMEN
Kulmaganbetov M.A.
E-mail: [email protected]
Scientific supervisor: d.m.s., prof. Pleshkova S.M., Department of biochemistry
S.D Asfendiyarov Kazakh National Medical University, Almaty, Kazakhstan
Actuality
Kazakhstan is a country in which the
problem of iodine deficiency is
extremely relevant. Iodine deficiency is
the reason of hypothyroidism - a serious
illness caused by the decrease in
functional activity of the thyroid gland.
Prenatal hormonal status’ correction of
pregnant reduces the risk of having
children with the disease and reduces
the impact of the disease to the
newborn. Syndrome (thyroid failure) is
formed in utero and manifested after
birth. This pathological condition may
be due to disembriogenesis (due to
anatomical defect producing the thyroid
gland, thyroid bud migration or fetal
injury) or due to functional immaturity
of enzyme systems involved in the
synthesis of hormones. Among the
reasons for its release of deficiency
iodine in the environment, the use of
supraphysiological doses of iodine in
pregnant women and infants, thyroid
disease the mother, adverse perinatal
factors. [1,2,3]
The purpose of the study
The study of the relationship between
SDH’s activity and levels of hormones
triiodothyronine (T3) and thyroid-
stimulating hormone (TSH) in pregnant
women and newborns.
Materials and methods
The object of the study was taken total of
40 pairs of "mother-child", 25 of who
had been diagnosed hypothyroidism -
the main group. The control group,
which was not detected hypothyroidism,
was 15 pairs of "mother-child
relationship." We studied the
concentration of TSH in newborns in the
peripheral blood.
Results
3-fold excess of TSH from the main
group as compared with the control
group represents increase of
hypothyroidism in the main group (table
1). During the 3 days the concentration
of TSH in the control group decreased
by 43%, which is normal for babies(table
1).
The enzyme SDH is a key enzyme of the
Krebs cycle, which represents activity of
the cell energy potential, so it is
important to consider its activity
(diagram 1).
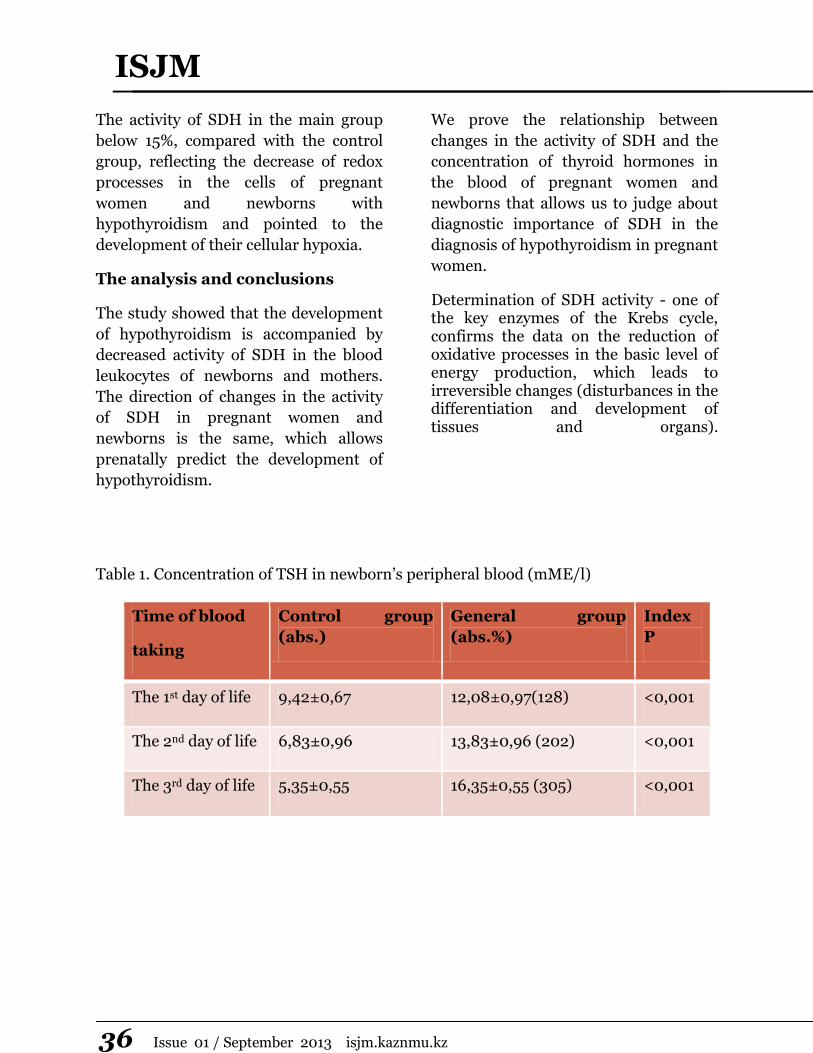
ISJM
36 Issue 01 / September 2013 isjm.kaznmu.kz
The activity of SDH in the main group
below 15%, compared with the control
group, reflecting the decrease of redox
processes in the cells of pregnant
women and newborns with
hypothyroidism and pointed to the
development of their cellular hypoxia.
The analysis and conclusions
The study showed that the development
of hypothyroidism is accompanied by
decreased activity of SDH in the blood
leukocytes of newborns and mothers.
The direction of changes in the activity
of SDH in pregnant women and
newborns is the same, which allows
prenatally predict the development of
hypothyroidism.
We prove the relationship between
changes in the activity of SDH and the
concentration of thyroid hormones in
the blood of pregnant women and
newborns that allows us to judge about
diagnostic importance of SDH in the
diagnosis of hypothyroidism in pregnant
women.
Determination of SDH activity - one of the key enzymes of the Krebs cycle, confirms the data on the reduction of oxidative processes in the basic level of energy production, which leads to irreversible changes (disturbances in the differentiation and development of tissues and organs).
Table 1. Concentration of TSH in newborn’s peripheral blood (mME/l)
Time of blood
taking
Control group
(abs.)
General group
(abs.%)
Index
P
The 1st day of life 9,42±0,67 12,08±0,97(128) <0,001
The 2nd day of life 6,83±0,96 13,83±0,96 (202) <0,001
The 3rd day of life 5,35±0,55 16,35±0,55 (305) <0,001
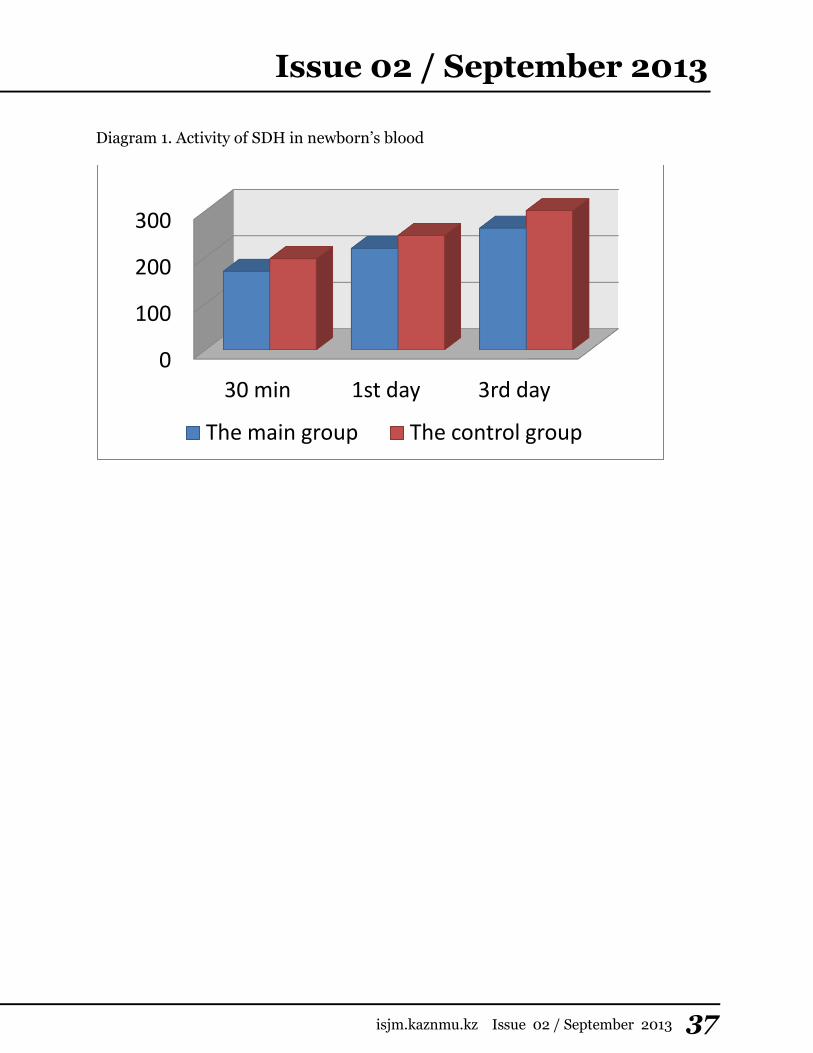
Issue 02 / September 2013
isjm.kaznmu.kz Issue 02 / September 2013 37
Diagram 1. Activity of SDH in newborn’s blood
0
100
200
300
30 min 1st day 3rd day
The main group The control group

New rubric is for sharing
information about Health Care
System of countries. Here you can
find Country Profile, Brief History,
basic information about Health
Situation, Health Determinants,
Health issues and others.
The first trip will be to the Heart of
Eurasia – Kazakhstan! So, let’s get
started...
Kazakhstan is a country in Central Asia.
The 9th largest country in the world by land area
(territory of 2,727,300 square kilometres);
The world's largest landlocked country;
Capital is Astana, the largest city is Almaty
(former Alma Ata);
Population is 16,6 million (2011);
The climate is continental, with warm summers
and colder winters
The Kazakh ethnomedicine
An ancient ethnomedicine of Kazakhstan arose up on
the basis of practical experience of many generations. So,
for example, a hunt and stock-raising gave knowledge of
structure and functions of internal organs of animals, that
assisted knowledge of anatomy of man.
The Kazakh doctors gave a large value a prophylaxis
and timeliness of treatment. They systematized diseases in
two groups: external and internal. By the way, in the
Kazakh traditional medicine is much in common with the
methods applied by the Arab and Persian infirmarians.
Kamlaniye – the treatment, carried out dollars or the
healer, was accompanied, like a spiritualistic session,
calling of ancestral spirits by means of music, singing,
dances and rituals with fire. The essence of all these magic
rituals was reduced to one: the healer stole or tried to get
the soul selected at the patient at evil ghosts. The use of
musical instruments in treatment was explained by that
spirits that was used in a ritual flew on the sound of melody
of kobiz.
With arrival of islam on territory of ancient
Kazakhstan treatment began to be practiced with sanctified
stones, amulets, that was brought from Mecca.
Treatment by herbs on the basis of which there was a
traditional Kazakh medicine was one more direction of
ancient Kazakh medicine. Also after bathing of newborns
smeared with a fat tail, which has heated them.
In curative aims Kazakhs were use a kumiss until now
remaining excellent means at treatment of row of diseases.
Folk doctors could well treat a syphilis. For this aim
they prepared from different medical plants, roots and
arboreal bark strong infusion composition of that was kept
under a hat. Gave infusion two times in a day inside.
The most effective methods of treatment were different
surgical receptions.
The art of the Kazakh bone-setters is well-known.
Many researchers wrote about them. Bone-setters easily
and faultlessly could set any breaks of extremities, collar-
bones and even thighs, and also various arthral
dislocations. A tire was held to fixing of breaks, and it
depended on character of breaks and from age of man.
Currency is Tenge (1 USD = 157 Tenge);
The Kazakh, Russian & English languages;
Religious and language freedoms were
guaranteed by Kazakhstan’s Constitution;
Leader of KZ – president N.A. Nazarbaev
In Kazakhstan there are editions sanctified to history
and practice of the Kazakh ethnomedicine. The first books
were produced in soviet time. In a manual "Essays are on
history of ethnomedicine of Kazakhstan", going out in light
in 1978 edited by Toregeldy Sharmanov, it is talked that
Kazakhs "had necessary anatomic knowledge, a
comparative anatomy" was not bad developed.
Map of Kazakhstan Coat of Arms of KZ Flag of KZ
The history of our medicine is very cognitive. It is a
philosophy. Relationships of nature, people, animals, plants
are the basis of all. Everything is important - from the
physical cooperating with the surrounding world to the
manner of thoughts of man. Now we study diagnostics
methods, it too is interesting.. The Kazakh doctors
diagnosed, feeling a pulse. They paid attention to eyes.
“Salamatty Kazakhstan” State Program resultsfor 2012
The Government of Kazakhstan has been implementing the State Program of
Healthcare Development “Salamatty Kazakhstan” aimed at improving the people’s
health for ensuring the country’s stable socio-demographic development.
The main demographic indices following the results of 2012 per 1000 population are:
natural increase - 14.51; birth rate - 23.07; mortality - 8.56.
Upcoming events & Health Days
September-November 2013
2 September–30 October 2013 – Annual meetings of WHO
Regional Committees
23 September 2013 – UN High-level Meeting on Disability
and Development
24 – 29September 2013 – United Nations General Assembly
(UNGA)
6 – 11 October 2013 – 6th MIM Pan-African Malaria
Conference
17 – 18 October 2013 – UHC Annual Conference
20-26 October 2013 – International Lead Poisoning
Prevention Week of Action
30 October - 3 November 2013 – The 44th Union World
Conference on Lung Health
2 – 6 November 2013 – American Public Health Association
(APHA)
12 – 15 November 2013 – International Conference on Family
Planning
13 – 17 November 2013 – American Society for Tropical
Medicine and Hygiene (ASTMH)

S.D.Asfendiyarov Kazakh National Medical University
International Students Journal of Medicine (ISJM)
Issue 02 / September 2013
http://www.isjm.kaznmu.kz
Editorial Board is not responsible for the content of publications.
Authors of the works are responsible for the content of the articles.
