issue 9: january march, 2017 - ghana health service · issue 9: january – march, 2017 national...
TRANSCRIPT
1 | P a g e
Issue 9: January – March, 2017
National Malaria Control Programme (NMCP) Box KB 493│Korle - Bu│Accra│Ghana
Contents Page
Editorial and Report Highlights 1
Malaria Burden 2
Key activities undertaken in First Quarter of 2017 2
Malaria Statistics 4
Indicator Definition 11
References 11
Editorial
This is the 9th issue of the Ghana Malaria Control Programme Periodic Bulletin.
The aim of this bulletin is to inform all stakeholders on progress achieved and challenges
encountered in malaria control in Ghana. Most importantly, it is to encourage use of this
information at all levels in order to foster improvement of our efforts, highlight achievements and
create awareness for increased resource mobilization and allocation in order to maintain the gains
we have achieved.
In this issue, we present DHIMS data, representing malaria burden, case management and
coverage of malaria interventions for first quarter 2017.
We would be pleased to receive comments from you regarding this publication, and we welcome
your contributions to subsequent issues.
Thank you. We hope this will inform decision making at all levels.
ACKNOWLEDGEMENT
Programme Manager and staff of NMCP
GHS: Regional and District Directors of Health Services
Policy Planning Monitoring and Evaluation Division (PPMED)

2 | P a g e
Regional Malaria Focal Persons
Partners (WHO, Global Fund, USAID/PMI, DFID, CDC, and Noguchi etc.)
Malaria Burden
In the quarter under review, the country recorded 2.3 million suspected malaria cases at the OPD.
This represents a 1.18% increase over cases reported during the same period in 2016. Averagely,
24,885 suspected malaria cases were recorded daily. The number of malaria admissions reduced
from 79,822 in 2016 to 69,467. The number of deaths also reduced from 379 to 143 in 2017. This
represents a percentage decrease of 22.86% and 165.03% in admissions and deaths respectively.
Out of the 143 malaria deaths recorded in 2017, 74 deaths occurred among children under5 years
compared to 152 in2016. Malaria under five Case Fatality Rate (CFR) also decreased from 0.39 in
2016 to 0.22 in 2017.
Key Activities Undertaken in the First Quarter of 2017
NMCP undertook the following activities in 2017 to help achieve the targets set for the year with
the ultimate aim of reducing malaria morbidity and mortality by 75% (using 2012 as baseline) by
the year 2020.
Case Management
The unit participated in the Malaria Operational Plan (MOP) for the 2018 financial year. NMCP
conducted 510,484home visits through CHPs within the period under review.
SHOPS USAID in collaboration with NMCP coached 720 Over the Counter Medicine Sellers
(OTCMS) attendance who purchased malaria RDTs from SHOPs on practical RDT principles and
testing. The programme in collaboration with Institutional Care Division (ICD) oriented 30
Regional Malaria Lab OTSS Supervisors on proficiency Testing Scheme. Proficiency testing of
medical laboratory scientists was conducted for 40 facilities nationwide. A survey on the
availability and pricing of co-paid or green leaf ACTs was conducted in all the 10 regions.
Integrated Vector Control
Activities of the vector control unit within the period under review were mainly on planning for

3 | P a g e
the 2017 Schools LLIN distribution campaign. The first ITN sub-committee meeting for the year
was held in February 2017.Continuous distribution of LLINs in health facilities for Antenatal
clinics (ANC) registrants and children 18 months and above due for measles 2 (two) continued in
all regions. DHIMs data for the period under review showed that 128,540 LLINs were distributed
in health facilities to ANC registrants and children 18 months and above given measles 2.
Social and Behaviours Change Communication (SBCC)
The Programme used mass media campaigns to advocate and intensify education on test, treat and
track (T3); compliance, use and improve provider confidence in RDT, Intermittent preventive
treatment in pregnancy (IPTp) and proper care and use of LLIN. A total number of 54 TV and
1,817 radio adverts were aired across the country in the quarter under review.
In addition, 33 NGOs were funded to implement community sensitization in 9 regions, except
Ashanti.
Surveillance, Monitoring and Evaluation (SM&E)
In the quarter under review, the SM&E unit organized three monthly data verification and
validation exercise of routine data in all the 10 Regions. The programme populated a Principal
Recipient (PR) dashboard for submission to Country Coordination Mechanism (CCM).
Other activities undertaken include; preparation of annual statistics for the 2016 malaria report,
participation in the Malaria Operational Plan (MOP) for the 2018 financial year, classification of
DHIMS indicators, preparation of 2016 progress update and disbursement to The Global Fund
(TGF), production of quarterly malaria bulletin (annual bulletin), participation in Malaria/RSSH
Global Fund grant application, planning for Outreach Training and Supportive Supervision
(OTSS) and Participated in the harmonization of DHIMS indicators organized by PPMED.
Research
The following research has either being conducted or is still ongoing; Malaria Indicator Survey,
ATM Mortality Trend Analysis, Durability and viability studies on LifeNets (LLIN), Impact
evaluation of BCC interventions among others.
Finance and Administration

4 | P a g e
As at the end of first quarter 2017, the programme had absorbed 91% of total funds released. A
huge proportion of this disbursement was for procurement of commodities; (RDTs and ACTs
including private sector co - payment).
MALARIA STATISTICS FOR JANUARY – MARCH, 2017
Reporting Rates
DHIMS2 reporting rate completeness on the monthly OPD morbidity form increased from 70.8%
in the first quarter of 2016 to 80.5% in 2017.The Monthly Anti-Malaria reporting form also
increased from 86.6% in2016 to 97.5% in 2017.
Table 4: Number and Proportion of Malaria OPD Cases, Admissions and Deaths in Ghana, Jan
– Mar 2017
Indicator Number
Reported
Proportion Of
Cases Attributable
To Malaria
OUT PATIENT
DEPARTMENT
(OPD)
Total OPD Cases 6,066,431
Suspected Malaria Cases 2,270,774 37.4
Tested Malaria Cases 1,904,183 83.9
Confirmed Malaria Cases 956,123 42.1
Pregnant Women 28,793 0.5
ADMISSION
Total Admissions (All ages) 349,949
Malaria admissions (All ages) 69,467 19.9
Under 5 malaria admissions 33,402 48.1
DEATHS
Total deaths (All ages) 7,966
Total malaria deaths (All ages) 143 1.8
Under 5 malaria deaths 74 51.7
Under 5 Malaria CFR 0.22
Source: DHIMS2, May, 2017
MALARIA MORBIDITY AND MORTALITY

5 | P a g e
The country recorded a reduction in under-five CFR from 152 (0.39%) in the first quarter of 2016
to 74(0.22%) in 2017. This represents 105.4% reduction in malaria deaths. In the period under
review, Brong Ahafo and Upper East Regions recorded the highest under 5 malaria CFR of 0.41%
and 0.54%respectively whilst Eastern Region had the lowest CFR of (0.04%). Figure 1.
Figure 1: Malaria Case Fatality Rate for children under 5 years by Region, Jan - Mar 2016
&2017
Source: DHIMS2, May, 2017
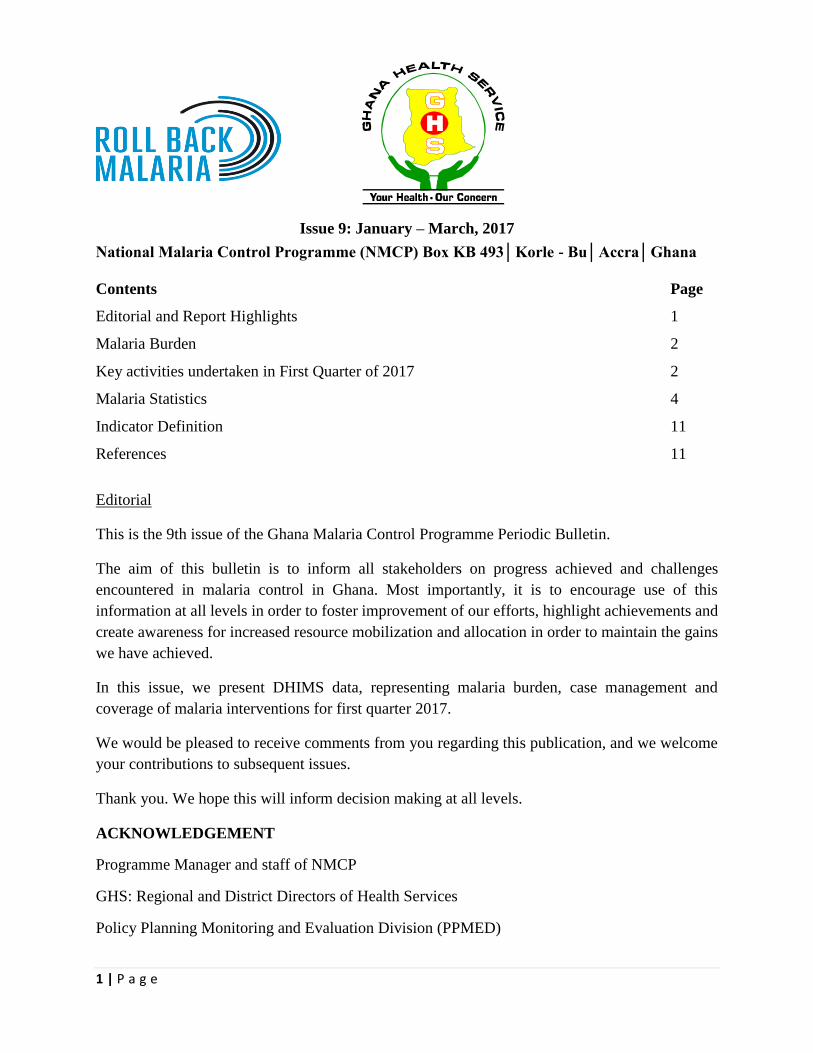
The country recorded a decrease in malaria CFR amongst persons above five years from 227
(0.55%) in the first quarter of 2016 to 69 (0.19%) in 2017.This represents a 228.9% reduction in
malaria deaths. Northern Regions recorded the highest above five malaria CFR of 21(0.67%).
Comparatively, there has been an improvement in case management in all the 10 Regions. Upper
East Region recorded the lowest malaria above five CFR of 0.06 with one (1) malaria deaths out
of 1,787 malaria admissions. (Figure 2).
AshantiBrongAhafo
Central EasternGreaterAccra
NorthernUpperEast
UpperWest
Volta Western Ghana
Jan - Mar 2016 0.16 0.21 0.47 0.26 0.32 0.68 0.12 0.69 0.52 0.32 0.39
Jan - Mar 2017 0.05 0.41 0.14 0.04 0.08 0.32 0.54 0.39 0.27 0.25 0.22
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
Cas
e F
atal
ity
Rat
e
6 | P a g e
Figure 2: Malaria Case Fatality Rate for persons above five years by Region, Jan - Mar 2016
& 2017
Source: DHIMS2, May, 2017
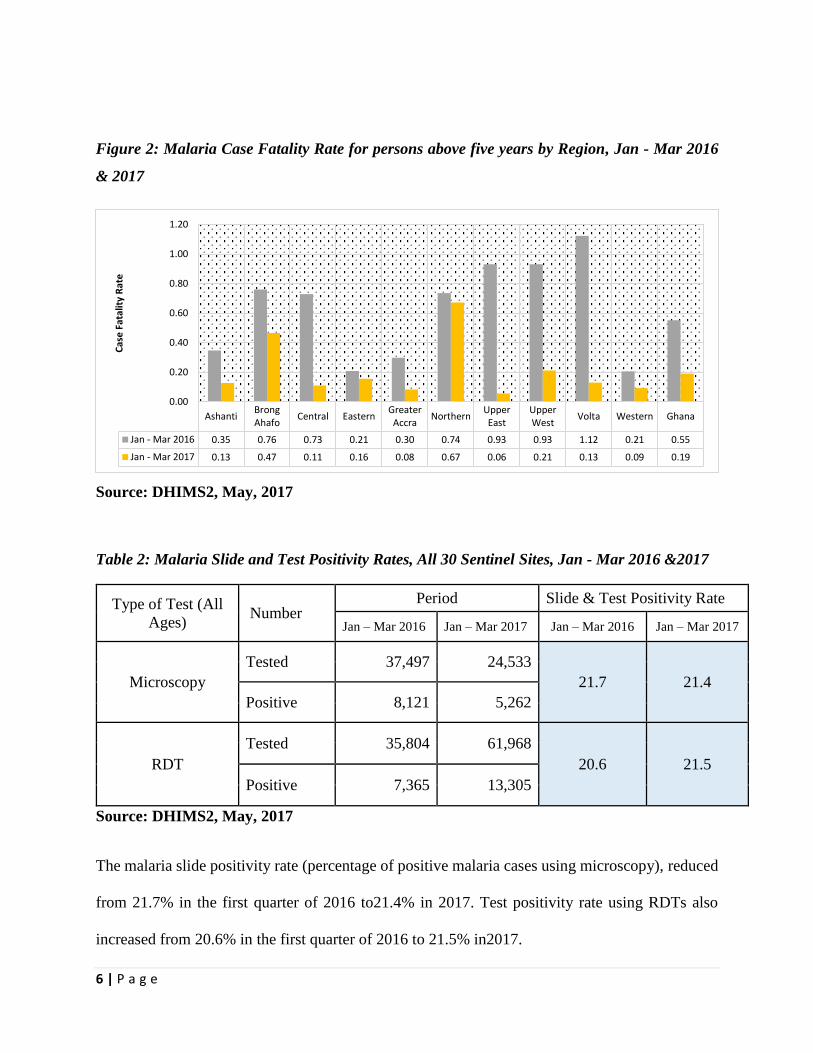
Table 2: Malaria Slide and Test Positivity Rates, All 30 Sentinel Sites, Jan - Mar 2016 &2017
Type of Test (All
Ages) Number
Period Slide & Test Positivity Rate
Jan – Mar 2016 Jan – Mar 2017 Jan – Mar 2016 Jan – Mar 2017
Microscopy
Tested 37,497 24,533
21.7 21.4
Positive 8,121 5,262
RDT
Tested 35,804 61,968
20.6 21.5
Positive 7,365 13,305
Source: DHIMS2, May, 2017
The malaria slide positivity rate (percentage of positive malaria cases using microscopy), reduced
from 21.7% in the first quarter of 2016 to21.4% in 2017. Test positivity rate using RDTs also
increased from 20.6% in the first quarter of 2016 to 21.5% in2017.
AshantiBrongAhafo
Central EasternGreaterAccra
NorthernUpperEast
UpperWest
Volta Western Ghana
Jan - Mar 2016 0.35 0.76 0.73 0.21 0.30 0.74 0.93 0.93 1.12 0.21 0.55
Jan - Mar 2017 0.13 0.47 0.11 0.16 0.08 0.67 0.06 0.21 0.13 0.09 0.19
0.00
0.20
0.40
0.60
0.80
1.00
1.20
Cas
e F
atal
ity
Rat
e

7 | P a g e
For the period under review, the number of suspected malaria cases put on ACTs reduced from
1,206,237 in the first quarter of 2016 to 1,145,062 in 2017. This could be attributed to the
improvement in adherence to the T3 policy. (Table 2)
Figure 3: Number of Malaria Suspected Cases, Malaria Cases Tested, Malaria Cases Test
Positive and Cases Put On ACTs in Ghana, Jan - Mar 2016 &2017
Source: DHIMS2, May, 2017
The country recorded an increase in malaria testing rate from 75.3% in the first quarter of 2016 to
83.9% in 2017. All the ten (10) Regions recorded an increase in testing compared to that of 2016.
Brong Ahafo Region recorded the highest testing rate of 91.6% whilst Northern Region recorded
the lowest rate of 64.7%. Refer to Figure 4.
UncomplicatedSuspected malaria
cases
Tested Malariacases
Confirmed MalariaCases
Malaria casestreated with ACTs
Jan - Mar 2016 2,243,950 1,689,532 853,031 1,206,237
Jan - Mar 2017 2,270,774 1,904,183 956,123 1,145,062
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
Nu
mb
er
of
case
s
Jan - Mar 2016 Jan - Mar 2017

8 | P a g e
Figure 4: Testing Rate of all Health Facilities by Region, Jan - Mar 2016 &2017
Source: DHIMS2, May, 2017
INTERMITTENT PREVENTIVE TREATMENT IN PREGNANCY (IPTp)
There was a steady supply of Sulphadoxine Pyrimethamine (SP) for IPTp throughout the country
in the first quarter of 2017. This had a positive impact on the uptake of IPTp. The proportion of
IPTp 1 uptake increased from 62.1% to 66.5% in 2017.The country recorded an increase in all the
stages of IPTp uptake (IPT 1 – 5) compared to that of last year. Refer to Figure 5.
AshantiBrongAhafo
Central EasternGreaterAccra
NorthernUpperEast
UpperWest
Volta Western Ghana
Jan - Mar 2016 68.6 77.9 78.6 79.0 76.8 57.1 84.3 54.8 78.1 81.7 75.3
Jan - Mar 2017 77.4 91.6 87.6 87.6 82.9 64.7 89.4 90.2 81.5 83.9 83.9
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Pro
po
rtio
n

9 | P a g e
Figure 5: Proportion of Pregnant Women Taking IPT 1-5, Ghana, Jan - Mar 2016 - 2017
Source: DHIMS2, May, 2017
LONG LASTING INSECTICIDAL NETS (LLINs)
Continuous distribution of LLINs for ANC registrants was carried out in all the 10 Regions. The
coverage of LLIN given to pregnant women increased from 22.9% in the first quarter of 2016 to
74.3% in 2017. Brong Ahafo Region had the highest coverage; 94.0% whiles Central Region
recorded the lowest coverage of 51.1% (Figure 6).
Figure 6: Proportion of ANC Registrants given LLIN by Region, Jan - Mar 2016 &2017
62.1
52.3
36.6
15.6
5.6
66.6
57.3
41.3
19.5
7.2
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
% IPTp 1 % IPTp 2 % IPTp 3 % IPTp 4 % IPTp 5
Pro
po
rtio
n
Period
Jan - Mar 2016 Jan - Mar 2017

10 | P a g e
Source: DHIMS2, May, 2017
LLIN coverage for children due for measles 2 Child Welfare Clinic (CWC) increased from 36.8%
in 2016 to 80.2% in 2017. In the quarter under review, all the 10 Regions recorded an increase
over that of 2016. Upper West Region had the highest coverage with94.2% whilst Ashanti Region
recorded the least coverage; 61.5% (Figure 7).
Figure 7: Proportion of under five children given LLIN through CWC by Region, Jan - Mar
2016 &2017
Source: DHIMS2, May, 2017
AshantiBrongAhafo
Central EasternGreaterAccra
Northern
UpperEast
UpperWest
Volta Western Ghana
Jan - Mar 2016 14.0 35.2 7.5 12.9 15.1 41.7 80.7 28.2 24.8 15.2 22.9
Jan - Mar 2017 56.7 94.6 51.7 85.1 73.6 74.4 88.2 79.8 85.4 83.4 74.3
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0P
rop
ort
ion
AshantiBrongAhafo
Central EasternGreaterAccra
Northern
UpperEast
UpperWest
VoltaWester
nGhana
Jan - Mar 2016 20.9 47.8 12.0 19.6 47.2 58.9 90.3 39.7 43.0 31.0 36.8
Jan - Mar 2017 61.5 90.4 66.7 92.8 86.1 68.2 91.3 94.2 90.9 86.7 80.2
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Pro
po
rtio
n

11 | P a g e
INDICATOR DEFINITIONS
Reporting completeness: Percentage of monthly reports received from health facilities in
relation to the number of monthly reports expected.
Malaria Case Fatality Rate: Proportion of deaths attributable to malaria out of all malaria
admissions.
Malaria slide positivity rate: percentage of total malaria microscopy positive test out of all
malaria microscopy tests conducted.
Malaria Test positivity rate: percentage of total malaria RDT positive test out of all malaria
RDT test done.
Testing Rate: Proportion of suspected malaria cases that received a parasitological test at a
facility (RDT and microscopy).
IPTp1 – 5 coverage: Percentage of pregnant mothers who received appropriate dose of SP
REFERENCES
GHS. District Health Information Management System II. Ghana Health Service, Ghana, Jan –
Mar, 2017.
GHS.NMCP – NMCP Surveillance data, Ghana, Jan – Mar, 2017.
GHS.NMCP - PSM Malaria drugs and commodities stock level, Ghana, Jan – Mar, 2017.

12 | P a g e