issues regarding the structure of the south african health market
DESCRIPTION
Issues regarding the Structure of the South African Health Market. Prof Alex van den Heever Chair in the Field of Social Security [email protected]. Source for Content. - PowerPoint PPT PresentationTRANSCRIPT

Issues regarding the Structure of the South African Health Market
Prof Alex van den HeeverChair in the Field of Social Security

Source for Content
The contents of this presentation reflect a high level summary of the analysis in a report provided to the Competition Commission in 2012
http://www.compcom.co.za/assets/Healthcare-Inquiry/Review-of-Competition-in-the-South-African-Health-System.pdf
What makes markets work?
• Basis for exchange – Individuals produce products and are able to exchange
them for other products• Consumers– Understand the product (price/quality)– Have a choice of alternatives– Able to exercise choice

When do markets fail?
• Basis for exchange – Individuals produce products and are unable to exchange
them for other products (absence of efficient systems of exchange – money)
• Consumers– Do not understand the product (price/quality)– Have limited or no choice of alternatives– Unable to exercise choice
How do consumers lose control of demand?
• Product complexity– Price, cost and quality comparisons not possible in real
time– Market problems possible despite competition
• Market concentration– Structural reduction in products choice– National or geographic markets
• Market manipulation– Collusion to exclude competition from the market• Agreements between market participants, including the sharing
of information (e.g. prices/costs)• Punishment for non-compliance
– Payment of kickbacks to intermediaries able to determine demand (agents)
– Market segmentation• Forcing consumers into market segments on the basis of their
ability to pay
Correcting dysfunctional/failing markets
• Ensure an efficient basis for exchange• Put consumers rather than product suppliers in
control of demand– Effective market signalling• Price• Quality
– Product simplicity – remove need for advice• Correcting markets is more than just about price
What about efficiency?
• Allocative efficiency - static• Technical efficiency - static• Dynamic efficiency - innovation

ANALYSIS OF THE SOUTH AFRICAN MARKET

Two key “products”
• Insurance• Healthcare
• What about consumers?– Don’t understand what they’re buying– Don’t understand the pricing or the cost– Have no idea about product quality– Key strategic product purchases are channelled through
conflicted intermediaries

3rd Party Managed Care
Diagnostic Specialists
SurgicalSpecialists
3rd Party Administration
Hos
pita
l-bas
ed
and
subs
titut
e se
rvic
es
Medicines and other medical products and services
Financing and Risk Pooling
Health goods and services
Health insurance - unregulated
General PractitionerConsumer
Information asymmetry
Information asymmetry
Health insurance - regulated
Holding companies
Brokers

3rd Party Managed Care
Diagnostic Specialists
SurgicalSpecialists
Hos
pita
l-bas
ed
and
subs
titut
e se
rvic
es
Medicines and other medical products and services
Financing and Risk Pooling
Information asymmetry
Information asymmetry
Health goods and services
Gate keeperConsumer agentsPossible conflicts of interestMoral hazardAnti-selectionRisk-selectionCommercial relationships
Health insurance - unregulated
Financial sector holding companies
General Practitioner
Brokers Health insurance - regulated
Consumer
3rd Party Administration
WHAT’S IN THE CONTRACT TODAY
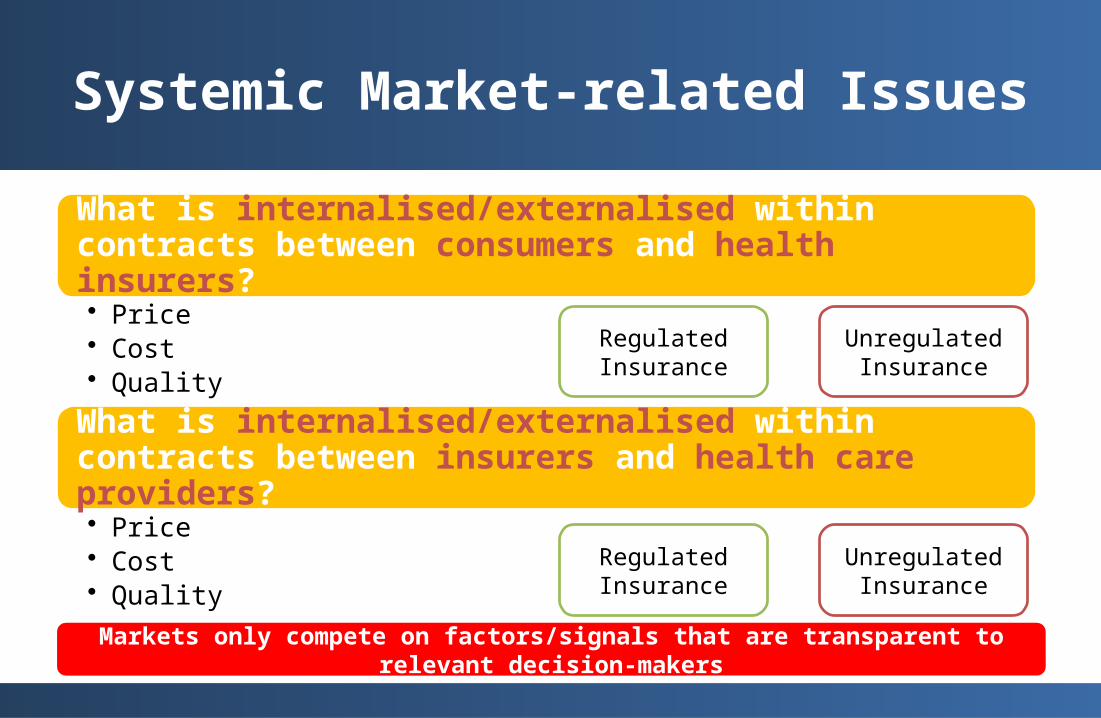
Systemic Market-related Issues
What is internalised/externalised within contracts between consumers and health insurers?• Price• Cost• Quality
What is internalised/externalised within contracts between insurers and health care providers?• Price• Cost• Quality
Regulated Insurance
Unregulated Insurance
Regulated Insurance
Unregulated Insurance
Markets only compete on factors/signals that are transparent to relevant decision-makers

Internalised into Insurance contract – medical schemes
• Risk Medium• Price Medium• Quality of coverage Medium• Quality of health care services Medium/Weak• Quality of healthcare products Medium/Weak
• Regulations prevent some risks from being transferred arbitrarily back to consumers
Insurance contract – other
• Risk Weak• Price Weak• Quality of coverage Very weak• Quality of health care services Very weak• Quality of healthcare products Very weak
Internalised into insurance contract with HC service providers
• Derived from the contract between consumers and insurers
• Risk Weak• Price Very weak• Quality of coverage n/a• Quality of health care services Weak• Quality of healthcare products Weak

MARKET OUTCOMES
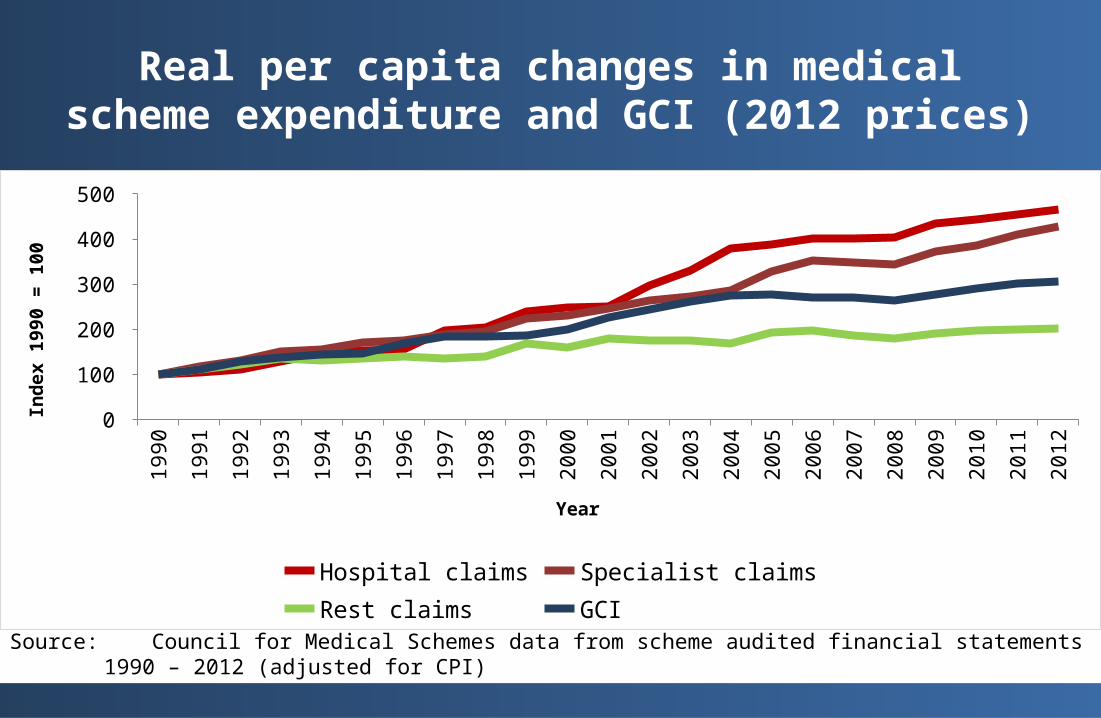
Real per capita changes in medical scheme expenditure and GCI (2012 prices)
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
0 50
100 150 200 250 300 350 400 450 500
Hospital claims Specialist claims Rest claims GCI
Year
Inde
x 19
90 =
100
Source: Council for Medical Schemes data from scheme audited financial statements 1990 – 2012 (adjusted for CPI)
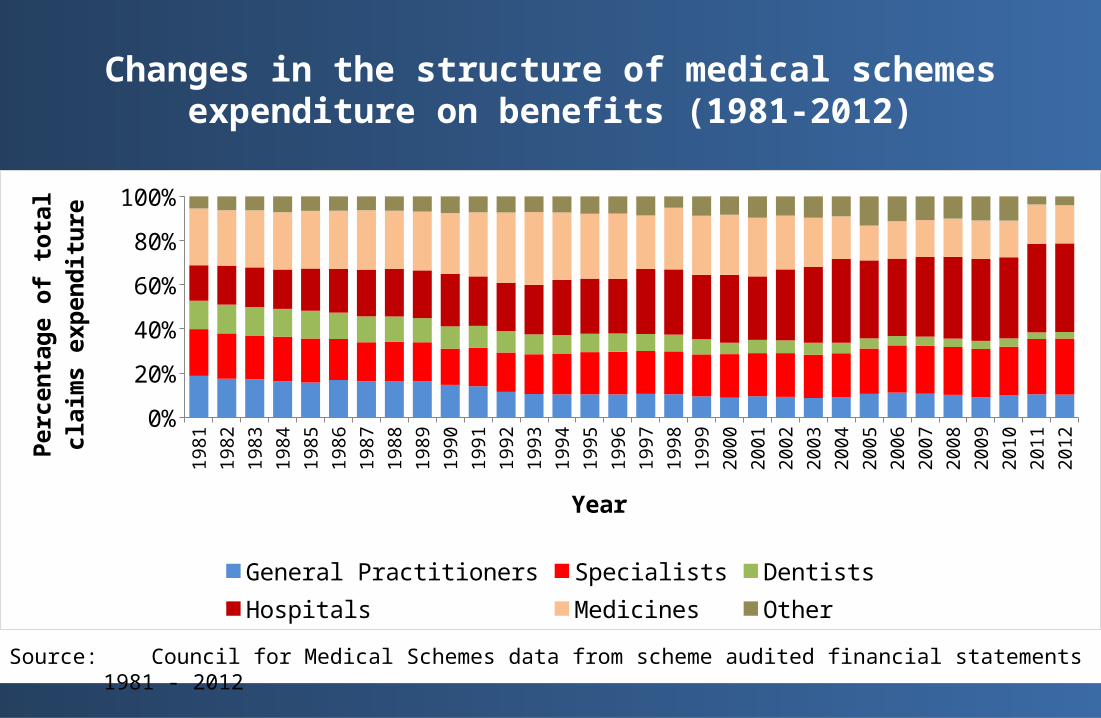
Changes in the structure of medical schemes expenditure on benefits (1981-2012)
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
2011
2012
0%10%20%30%40%50%60%70%80%90%
100%
General Practitioners Specialists DentistsHospitals Medicines Other
Year
Perc
enta
ge o
f tot
al c
laim
s ex
pend
iture
Source: Council for Medical Schemes data from scheme audited financial statements 1981 - 2012

Hospital claims (real pbpa) compared to beds per 1,000 and market concentration (HHI) (for private
beds)19
97
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0.0
50.0
100.0
150.0
200.0
250.0
300.0
Hosp claims Beds/Pop HHI (lag 1 yr)
Inde
x w
ith 1
997
= 10
0
Point at which beds per 1,000 is roughly equal to the US and UK (noting that they have vastly older populations)
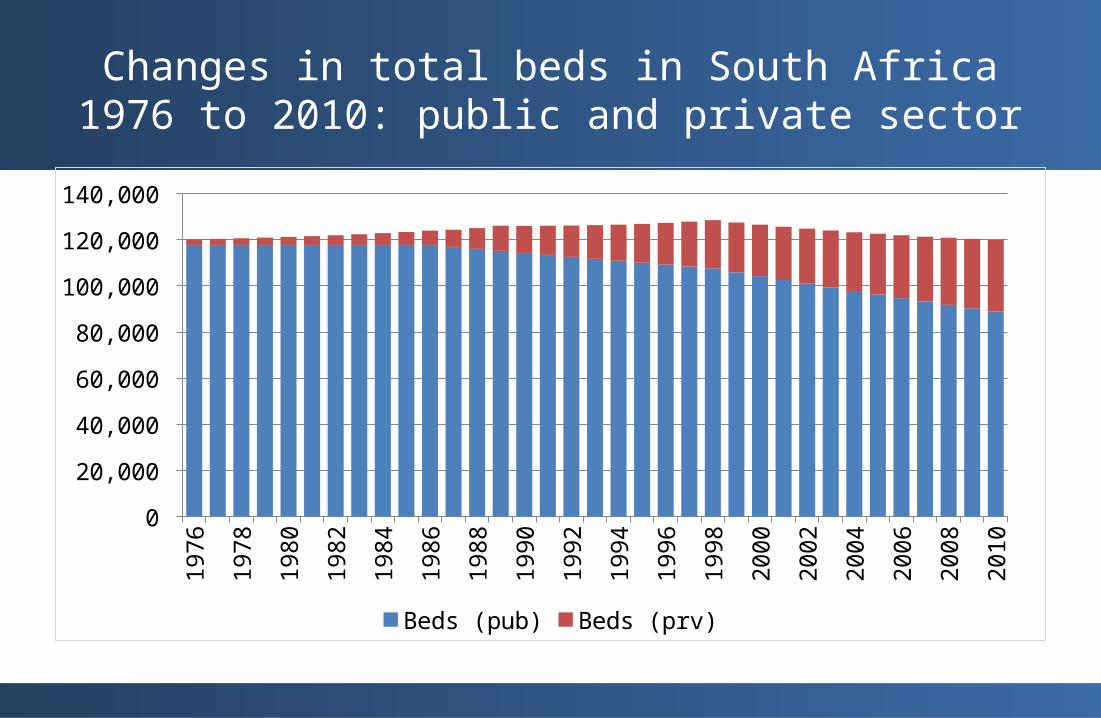
Changes in total beds in South Africa 1976 to 2010: public and private sector
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Beds (pub) Beds (prv)

Return on Capital Employed (Mediclinic and Netcare)
Source: Anthony Felet, Duncan Lishman and Fatima Fiandeiro, “Do hospital mergers lead to healthy profits?”, 2012, p.11
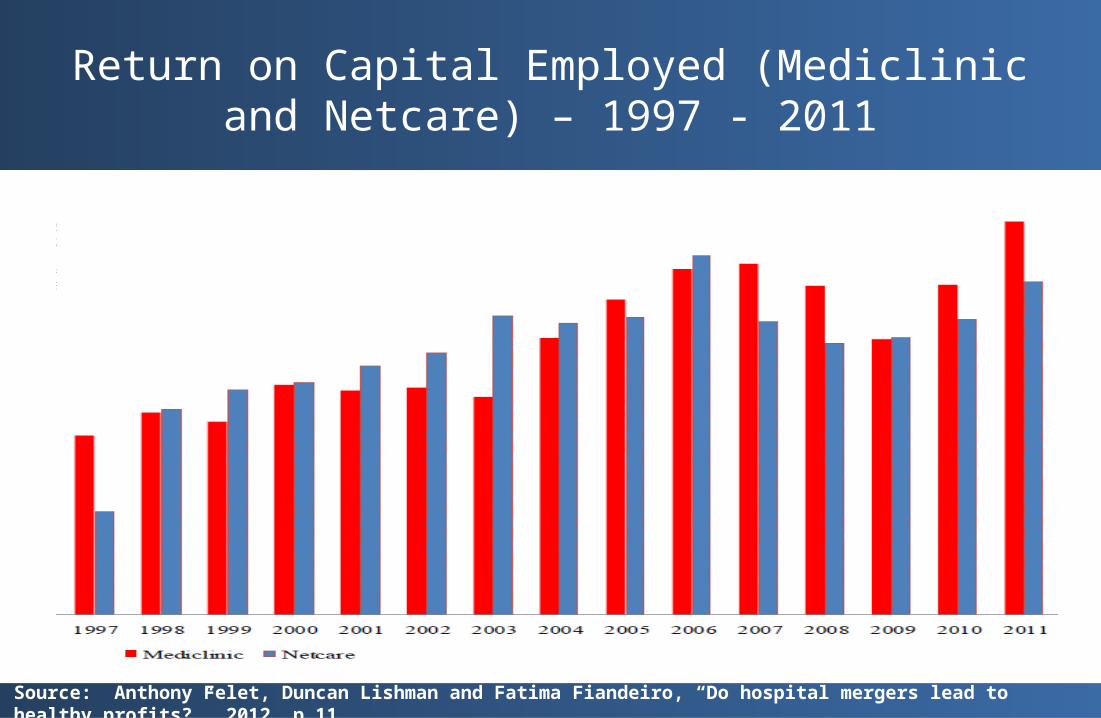
Return on Capital Employed (Mediclinic and Netcare) – 1997 - 2011
Source: Anthony Felet, Duncan Lishman and Fatima Fiandeiro, “Do hospital mergers lead to healthy profits?”, 2012, p.11
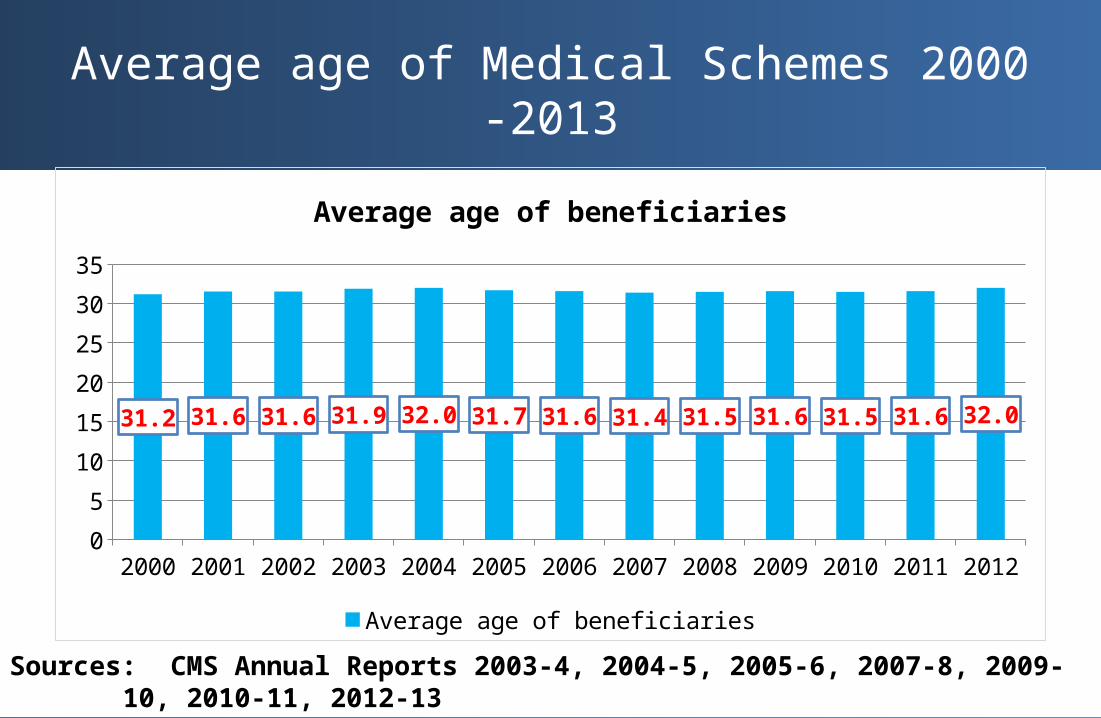
Average age of Medical Schemes 2000 -2013
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
5
10
15
20
25
30
35
31.2 31.6 31.6 31.9 32.0 31.7 31.6 31.4 31.5 31.6 31.5 31.6 32.0
Average age of beneficiaries
Average age of beneficiaries
Sources: CMS Annual Reports 2003-4, 2004-5, 2005-6, 2007-8, 2009-10, 2010-11, 2012-13
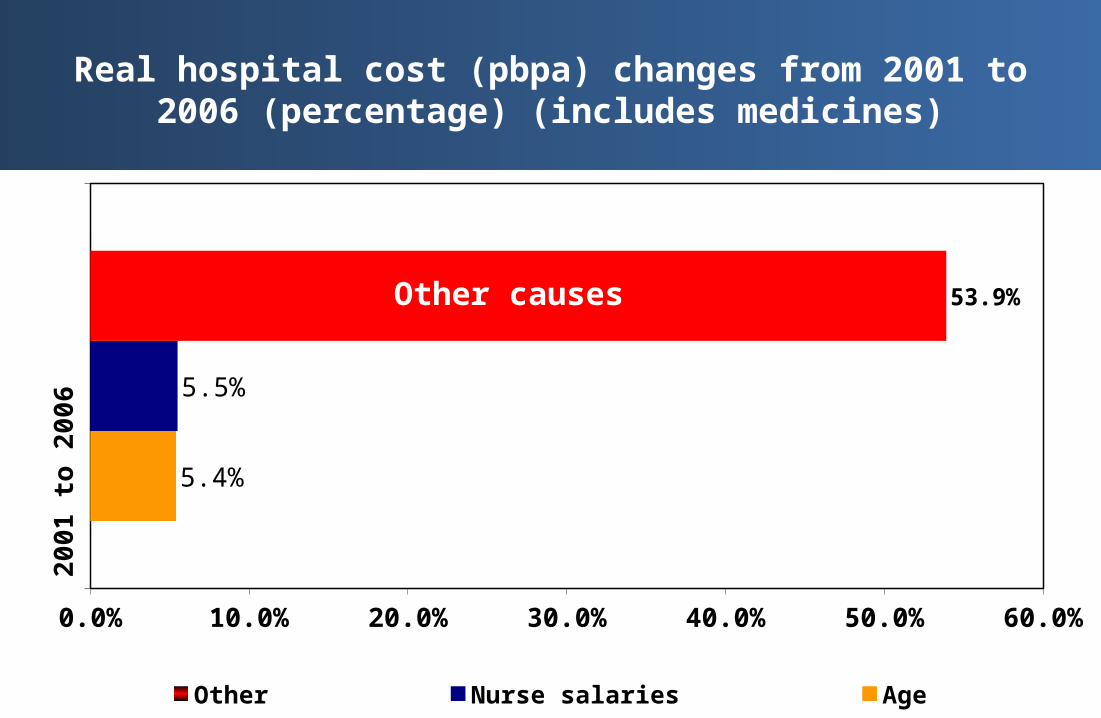
Real hospital cost (pbpa) changes from 2001 to 2006 (percentage) (includes medicines)2
00
1 t
o 2
00
6
0.0% 10.0% 20.0% 30.0% 40.0% 50.0% 60.0%
5.4%
5.5%
53.9%
Other Nurse salaries Age
Other causes
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Total Non-health Administration
Perc
enta
ge o
f GCI
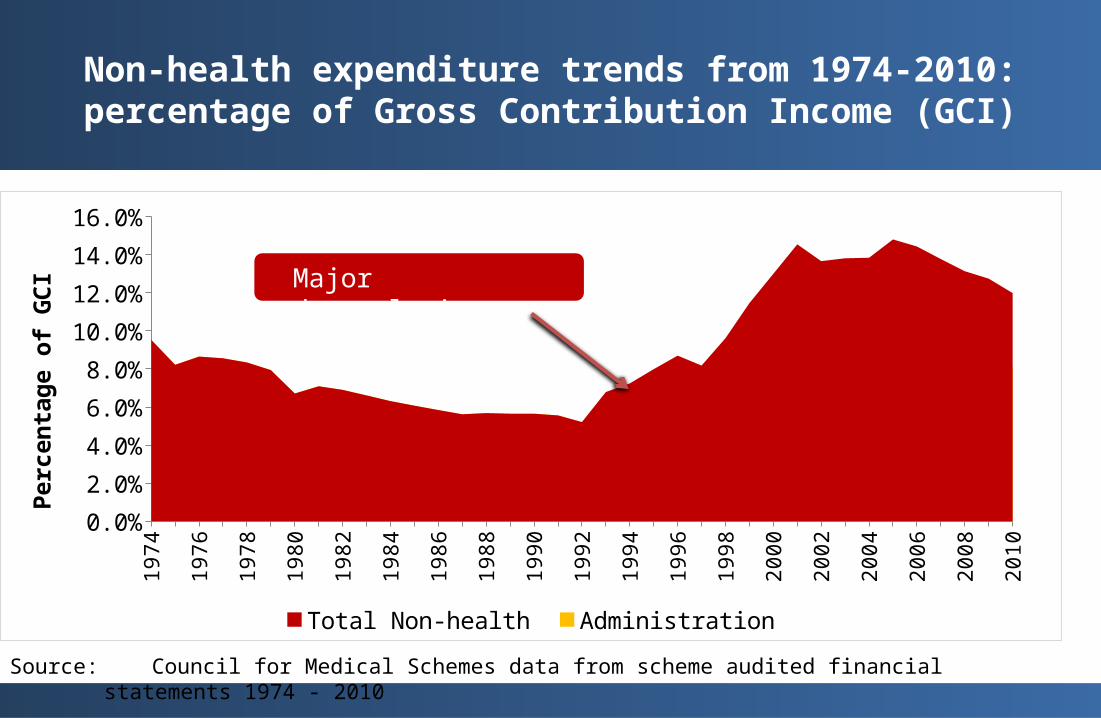
Non-health expenditure trends from 1974-2010: percentage of Gross Contribution Income (GCI)
Source: Council for Medical Schemes data from scheme audited financial statements 1974 - 2010
Major deregulation
CONCLUDING REMARKS
• Ensure that health insurers have the incentive to purchase efficiently– Remove conflicts of interest in markets for advice– Simplify and standardise products– Market transparency on key indicators central to consumer
choice– Internalising price and quality into the contract– Deal with regulatory arbitrage– Ensure governance arrangements correctly locate the
commercial imperative in the scheme
• Ensure that insurer incentives cannot be undermined by anti-competitive structures and conduct on the supply side– Market transparency (price/cost/quality)– Conflicts of interest• Separate doctors from other products
– Accumulation and abuse of market power• Market diversification• Penalise abuse
– Collusion
END