iterative user centered design for development of a ... · iterative user centered design for...
TRANSCRIPT

lable at ScienceDirect
Applied Ergonomics 56 (2016) 117e126
Contents lists avai
Applied Ergonomics
journal homepage: www.elsevier .com/locate/apergo
Iterative user centered design for development of a patient-centeredfall prevention toolkit
Zachary Katsulis a, *, Awatef Ergai a, Wai Yin Leung b, Laura Schenkel d, Amisha Rai d,Jason Adelman d, James Benneyan a, David W. Bates b, c, Patricia C. Dykes b, c
a Healthcare Systems Engineering Institute at Northeastern University, Boston, MA, USAb Brigham and Women's Hospital, Boston, MA, USAc Harvard Medical School, Boston, MA, USAd Montefiore Medical Center, Bronx, NY, USA
a r t i c l e i n f o
Article history:Received 27 October 2015Received in revised form21 March 2016Accepted 22 March 2016Available online 8 April 2016
Keywords:Evidence-based fall preventionPatient-centered designPatient safetyRE-AIMUsability
* Corresponding author.E-mail address: [email protected] (Z. Katsulis
http://dx.doi.org/10.1016/j.apergo.2016.03.0110003-6870/© 2016 Elsevier Ltd. All rights reserved.
a b s t r a c t
Due to the large number of falls that occur in hospital settings, inpatient fall prevention is a topic of greatinterest to patients and health care providers. The use of electronic decision support that tailors fallprevention strategy to patient-specific risk factors, known as Fall T.I.P.S (Tailoring Interventions for Pa-tient Safety), has proven to be an effective approach for decreasing hospital falls. A paper version of theFall T.I.P.S toolkit was developed primarily for hospitals that do not have the resources to implement theelectronic solution; however, more work is needed to optimize the effectiveness of the paper version ofthis tool. We examined the use of human factors techniques in the redesign of the existing paper fallprevention tool with the goal of increasing ease of use and decreasing inpatient falls. The inclusion ofpatients and clinical staff in the redesign of the existing tool was done to increase adoption of the tooland fall prevention best practices. The redesigned paper Fall T.I.P.S toolkit showcased a built in clinicaldecision support system and increased ease of use over the existing version.
© 2016 Elsevier Ltd. All rights reserved.
1. Introduction
Falls are a serious public health problem both within andoutside healthcare settings (Chen et al., 2009; Kannus et al., 2005).As a leading cause of injury and death, falls can lead to painful andcostly injuries such as fractures, lacerations, or internal bleeding(Sondik, 2009; Ganz et al., 2013). Hospitalization can increase therisk for falls and fall related injuries (Evans et al., 2001) due to theunfamiliar environment, illnesses, or treatments. While falls havelong been recognized as an important patient safety issue, theCenters for Medicare and Medicaid Services (CMS) added anadditional incentive to prevent fall injuries when they announcedin 2009 that treatment for injuries from falls occurring duringhospitalizationwould no longer be reimbursable (Ganz et al., 2013).Approximately 700,000 to 1,000,000 inpatient falls occur annuallyin the U.S, and the associated healthcare utilization costs make falls
).
an important patient safety issue nationwide (Ganz et al., 2013). Fallrisk assessment is currently required by The Joint Commission, withfall prevention interventions targeting a multitude of patientproblems or root causes including toileting, mobility, and impairedcognition (The Joint Commission, 2015). Prior research suggeststhat about 92% of hospital-based falls are “preventable” (Morse,2008). The Fall T.I.P.S (Tailoring Interventions for Patient Safety)toolkit was developed and tested to address barriers to fall pre-vention in hospital settings. Fall T.I.P.S used health IT to link routinenursing fall risk assessment with evidence-based interventions.The Fall T.I.P.S toolkit integrated electronic fall prevention decisionsupport into the clinical workflow by generating tailored fall pre-vention plans, patient education handouts, and bed posters withintervention icons based on patient-specific fall risk factors (Dykeset al., 1912e1918). Because the evidence-based fall risk in-terventions were automatically selected by Fall T.I.P.S software as

Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126118
the nurse completed the fall risk assessment, the chance of humanerror in the selection of fall interventions was minimized. Fall rateswere 22% lower in the Fall T.I.P.S intervention units than in thecontrol units. The Fall T.I.P.S intervention was particularly effectivewith patients 65 and older; the patients at greatest risk for falls(Dykes et al., 1912e1918). The Fall T.I.P.S toolkit was the firstintervention to demonstrate a significant reduction in patient fallsin acute care hospitals (Dykes et al., 1912e1918). While this studydemonstrated a significant reduction in falls, further work isneeded to integrate fall prevention decision support into settingswithout access to sophisticated electronic systems.
Recently an extension project, known as Developing a Patient-centered Fall Prevention Toolkit, was funded by the Agency forHealthcare Research and Quality (AHRQ). The goal of the project isto develop a suite of tools to support patient engagement in fallprevention practices in hospitals. One aspect of the project aims torevise a paper version of the Fall T.I.P.S toolkit. Since the original FallT.I.P.S solution required electronic decision support and compli-cated informatics expertise, a redesigned paper Fall T.I.P.S toolkitwith decision support will allow for broader adoption amonghospitals that cannot implement the electronic solution. In addi-tion, with the Joint Commission citing three of the most commoncontributing factors pertaining to patient falls - inadequateassessment, communication failures, and inadequate staff orien-tation e the redesigned paper Fall T.I.P.S toolkit must address thesefactors and not increase workload (The Joint Commission, 2015).
The paper version of the Fall T.I.P.S toolkit was revised usingMicrosoft's conventional user-centered design cycle. User-centereddesign (UCD) can be defined as “design processes in which end-users influence how a design takes shape.” (Abras et al., 2004)With the development of any application or tool, the design processshould be user-centered. As seen in Fig. 1, the user-centered designcycle consists of four main components: study, design, build, andevaluate (Harper, 2008). The extent towhich end users are involvedcan vary based on the scenario; however, it is critical that end-usersare involved to at least some extent. In addition, universal princi-ples of design including symmetrical alignment, use of distinctlyseparate colors, and prototyping were applied throughout thestudy (Lidwell et al., 2010).
For this study, paper versions of the Fall T.I.P.S toolkit
Fig. 1. Microsoft's conventional user-centered design cycle served as the underlyingapproach for this project.
intervention were developed and refined at Brigham and Women'sHospital (BWH) in Boston, MA and Montefiore Medical Center(MMC) in Bronx, NY. Prior to arriving at the final version of thepaper Fall T.I.P.S toolkit, multiple iterations were required, keepinguniversal principles of design in mind. The purpose of this manu-script is to describe the production of the final version of the paperFall T.I.P.S toolkit through the use of the user-centered design cycle.
2. Materials and methods
2.1. Study: nursing workflow observations
The institutional review boards at BWH and MMC reviewed thestudy protocol and due to minimal risk for patients and staff, it wasdeemed exempt status. The first step in our user-centered designcycle was the observation of nursing staff at both BWH and MMC.The purpose of these workflow observations was to study thecurrent state related to how nurses do fall risk assessment, how afall prevention plan was established, and if the patient or familymembers were involved in the process. At baseline there was a lotof variation between the fall prevention practices at BWH andMMC. BWH used an existing paper version of the Fall T.I.P.S toolkitthat was implemented after the original Fall T.I.P.S study, whereasMMC lacked an established tailored fall prevention tool. Workflowobservations were conducted by members of the research teamwith designated nursing staff at each hospital. The research teamtook note of any fall-related workflow, while also probing nursingstaff with questions related to fall risk assessment and tailored fallprevention plans.
2.2. Design: gathering user requirements
Prior to any physical redesign, initial user requirements wereidentified. Specifically, the elements that the users would like to seein the application or tool were gathered. In this study, our end userswere nursing staff and patients from all adult oncology units atBWH. Ideally nursing staff complete the entire fall risk assessmentand prevention plan with the patient; however, each end usershould be able to understand the completed risk assessment andplan individually. Patient feedback at times was difficult to receivedue to their acute illness or treatment schedule. Nursing re-quirements were gathered during informal interviews of staff onthe patient care units, as well as at three nursing practice com-mittee meetings. Interviews with nursing staff were conductedwith varying group sizes, ranging from 1 to 20 nurses; whereasinterviews with patients were always held with a single patient. Inorder to gain an appropriate amount of feedback from all nursingstaff interviewed, the existing paper version of the Fall T.I.P.S toolkitwas demonstrated (Fig. 2) to solicit feedback during the interview.Complete informal interview guides for gathering user re-quirements from both nurses and patients are included inAppendix A. Nursing and patient interviews were voluntary andkept to less than 10 min in length. All participants providedinformal verbal consent to participate.
2.3. Design: icon content validity index (CVI) testing
In addition to gathering user requirements regarding thephysical design of the prototype, user feedback was also gatheredregarding the icons used to represent the risk factors and fall pre-vention interventions. The icons used in the original paper FallT.I.P.S toolkit were developed by a commercial illustrator and weretested and validated by nurses and nursing assistants in four

Fig. 2. The existing paper version of the Fall T.I.P.S toolkit developed at BWH.
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126 119
Partners HealthCare (PHS) hospitals using content validity index(CVI) testing as part of a prior study (Lidwell et al., 2010). In thisstudy we performed CVI testing to validate the icons with patientsand families to ensure that they were understandable by thisimportant group of end users. This approach incorporated the useof icon validity and ranking forms, with each icon being ranked on a4 point Likert scale (1 ¼ strongly disagree, 4 ¼ strongly agree thatthe icon represents the concept). Multiple iterations of the iconswere conducted until each icon received a mean CVI score of atleast 3.0 by patients and families. For icons that received a scoreequal to or less than 3.0, patients and families were asked to pro-vide feedback on how to improve the icon. This feedback wasgathered, discussed by team members, and then relayed to theillustrator to iteratively refine the icons. CVI testing was thencompleted on the revised icons with nurses. Patient rankings weregiven a greater emphasis than nursing rankings due to the patients’lower health literacy levels. Additional details about the icon vali-dation methods have been described previously (Hurley et al.,2009).
2.4. Build: prototype comparison interviews
Prior to beginning another round of nursing staff and patientinterviews at BWH, multiple versions of the paper Fall T.I.P.Stoolkit were discussed among the research team. After coming to aconsensus on a specific prototype, members of the team thenconducted interviews with patients, families, and nurses to gainfeedback on ways to improve. If a consensus was not reached onone specific prototype among the team, multiple prototypeswould be referenced in the interviews. Fig. 3 showcases four mainversions of the prototype, each of which was developed based on
patient and nursing feedback. Members of the research teamgathered all feedback in order to discuss the potential changes,giving higher priority to recurring improvement ideas. Theseprototype comparison interviews were typically conducted inconjunction with icon CVI testing, as the new prototypes wouldfeature the updated icons. This paper Fall T.I.P.S toolkit will serve asa care team communication tool and a patient education tool.Therefore, patient and family feedback was considered highlyvaluable. Patient and family feedback was important in evaluatingif the toolkit could be seen from the bedside, as well as howeffective the color mapping of risks and interventions was forhelping end users understand which interventions would mitigateeach individual risk factor. Additional patient and family feedbackis included in Fig. 3. Root causes of inpatient falls include thatpatients do not believe they are at risk for falls and they do notknow their fall prevention plan. To be most effective, the toolkithad to be easily understood by all team members, including pa-tients and their family members.
2.5. Evaluate: usability testing
The final stage of the user-centered design cycle includesevaluation of what has been built. This evaluation should becompleted by the targeted end users and in as realistic of anenvironment as possible (Abras et al., 2004). Ideally each proto-type developed should incorporate some level of usability testing.For the purpose of this study, structured usability testing occurredonly on the final paper Fall T.I.P.S toolkit at BWH due to limitedavailability of patients and nurses. While no structured usabilitytesting occurred on the final paper Fall T.I.P.S toolkit at MMC,informal nursing and patient feedback was still gathered. The
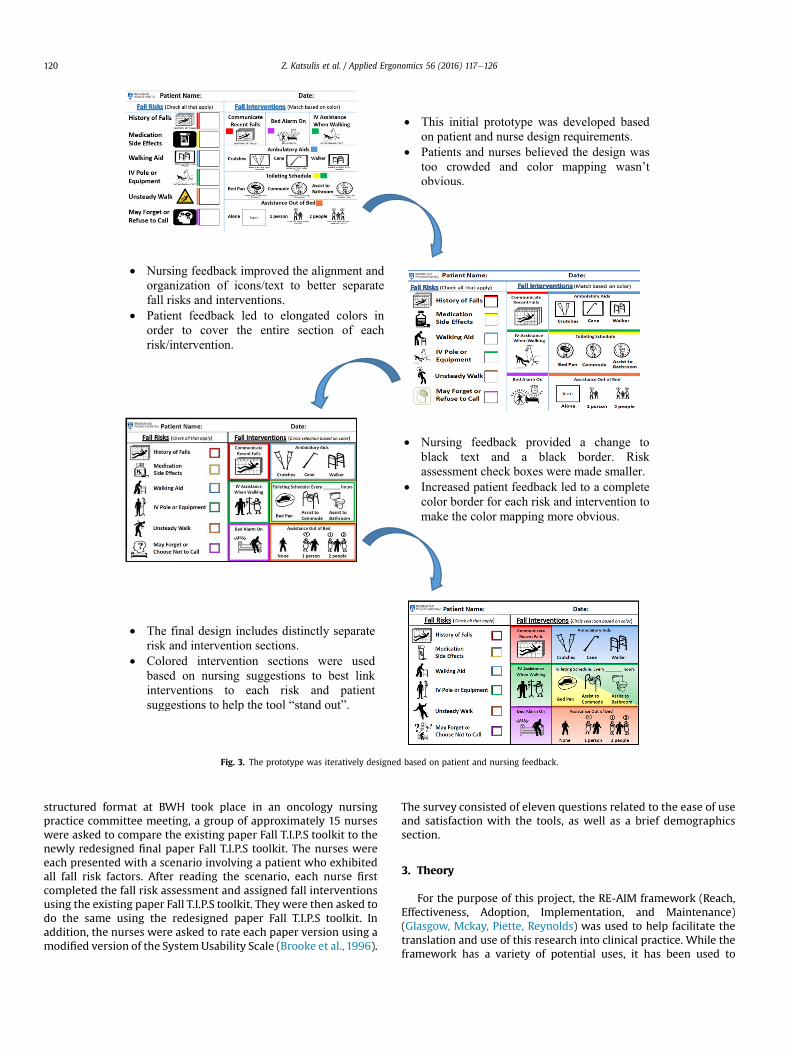
Fig. 3. The prototype was iteratively designed based on patient and nursing feedback.
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126120
structured format at BWH took place in an oncology nursingpractice committee meeting, a group of approximately 15 nurseswere asked to compare the existing paper Fall T.I.P.S toolkit to thenewly redesigned final paper Fall T.I.P.S toolkit. The nurses wereeach presented with a scenario involving a patient who exhibitedall fall risk factors. After reading the scenario, each nurse firstcompleted the fall risk assessment and assigned fall interventionsusing the existing paper Fall T.I.P.S toolkit. They were then asked todo the same using the redesigned paper Fall T.I.P.S toolkit. Inaddition, the nurses were asked to rate each paper version using amodified version of the System Usability Scale (Brooke et al., 1996).
The survey consisted of eleven questions related to the ease of useand satisfaction with the tools, as well as a brief demographicssection.
3. Theory
For the purpose of this project, the RE-AIM framework (Reach,Effectiveness, Adoption, Implementation, and Maintenance)(Glasgow, Mckay, Piette, Reynolds) was used to help facilitate thetranslation and use of this research into clinical practice. While theframework has a variety of potential uses, it has been used to

Table 1RE-AIM measures for assessing the applicability of Fall T.I.P.S
Measure Project phase Data source
Reach�Overall use of toolkit by patients Evaluation � Patient interviews�Use of toolkit by various demographicsEffectiveness�Positive and negative unanticipated consequences Evaluation � Patient interviews�Patient falls Evaluation � Event reporting system�Patient falls with injury�Effectiveness in older vs. younger patientsAdoption�Type of settings the toolkit is used in Evaluation � Patient interviews�Type of organizations the toolkit is used in � Study databaseImplementation�“Bugs” noted within the toolkit Implementation � Workflow observations�Development of “workarounds” � Patient, RN interviews�Consistency and frequency of use�Barriers and enabling factors�Resources used during implementation�Changes related to communication and collaboration related to fall prevention�Unintended consequences notedMaintenance�Strategies used for sustainability Evaluation � Workflow observations�The continued use of the intervention � Patient, RN interviews
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126 121
support evaluation of healthcare informatics projects (Glasgow).Although this study does not deal directly with the electronicversion of the Fall T.I.P.S toolkit, we determined this framework tostill be acceptable. Table 1 illustrates the various measures exam-ined for each component of the framework. For this publication,measures relating to implementation and maintenance will beexamined after the redesigned paper Fall T.I.P.S toolkit is imple-mented on the clinical units.
4. Results
4.1. Study: nursing workflow
According to hospital policy, fall risk assessment is completedupon admission and during every shift at BWH and MMC. As notedearlier, there was no previous paper version of the Fall T.I.P.S toolkitin place at MMC. At MMC, nurses documented the fall risk assess-ments and fall interventions in their electronic health record sys-tem. At BWH, the previous paper version of Fall T.I.P.S toolkit was inplace for patient education purposes, but nurses reported that itwas rarely used with patients. Nurses at BWH would insteadcomplete the fall risk assessment on the patient's paper flowsheets.Through observations, nurses at both sites rarely communicatedthe patients' risk factors, and often neglected to provide patientswith a tailored fall prevention plan.
4.2. Design: gathering user requirements
The majority of nurses communicated reservations related tothe original paper version of the Fall T.I.P.S toolkit due to a varietyof factors including the following: 1) difficult to read due to smallicons and font size, 2) an excessive amount of text used, 3) thestrong yellow background, and 4) lack of patient centeredness. Asseen previously in Fig. 2, the existing paper Fall T.I.P.S toolkitpresents detailed information regarding both patient fall risksand interventions, commonly displaying this information incomplete sentences directed at the patient. Nursing staff, as wellas a few patients, noted that a patient must be able to read the
sign on the wall while sitting in bed. In addition, the sign shouldattract visitors' attention allowing anyone who enters the room tobe aware of the patient's risk status and their tailored fall pre-vention plan. Nursing staff requested the sign be quick andintuitive to fill out in interest of time management. Nurses alsoreported that with the original paper Fall T.I.P.S toolkit, they haddifficulty identifying which interventions should be selected foreach area of fall risk. This led to variation in the fall preventionplans and lack of confidence that the plan selected was evidence-based.
4.3. Design: CVI testing
The icons which received the highest ratings generally refer-enced only a single concept (e.g cane, walker); whereas icons whichrepresented multiple concepts (e.g bed alarm on, medication sideeffects) received the lowest ratings. Additional information aboutthe CVI testing performed in this study is described and under re-view for publication elsewhere. The final version of the paper FallT.I.P.S toolkit, along with the patient and nurse validated icons canbe seen in Fig. 4.
4.4. Build: final paper fall T.I.P.S
As seen in Fig. 4, the final version of the paper Fall T.I.P.S toolkitfeatures two distinctly separate sections: fall risks and fall in-terventions. For each fall risk is a specific iconwith a fewwords in aconsumer level of health literacy describing the risk factor and theaccompanying icon. Each fall risk also contains a colored check box,with distinct directions next to the section heading “check all thatapply”. The colors of these check boxes directly correspond to thecolors of the fall intervention boxes. Based on our previous study,and as stated previously, each fall risk factor has at least oneevidence-based fall intervention associated with it. Therefore thecolor code system utilized is an example of a low level decisionsupport system, allowing any user to complete the fall in-terventions piece based on the selected risk factors by simplymatching colors. This decision support system should ideally
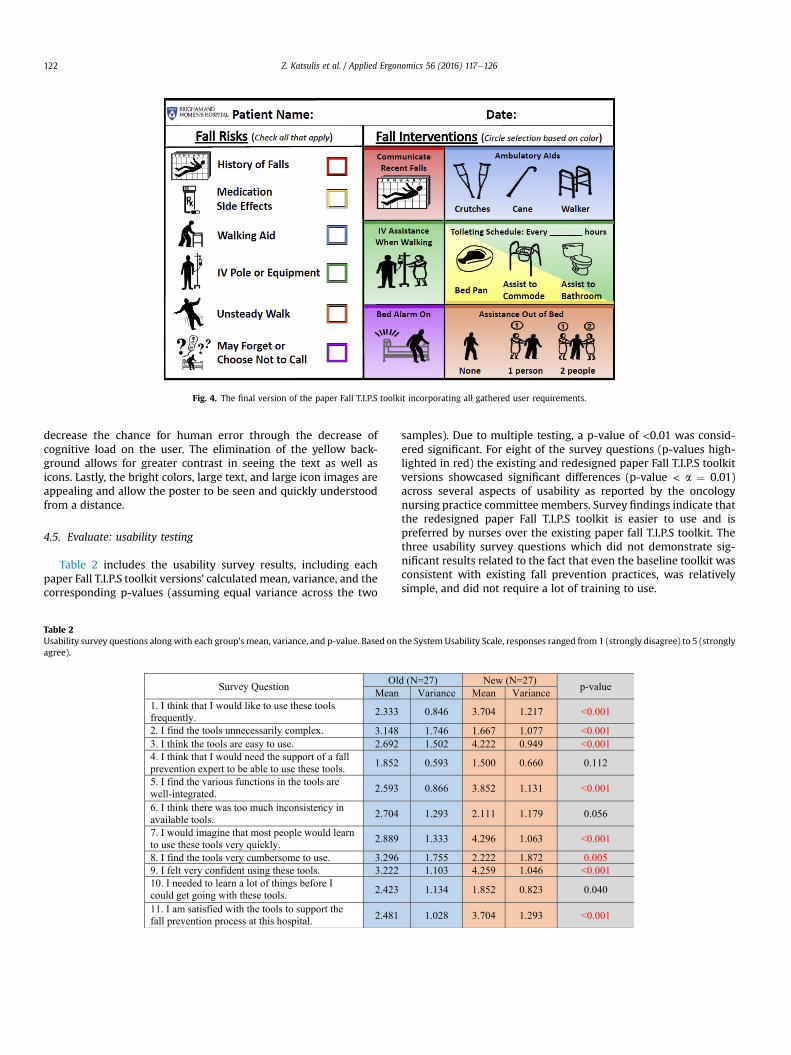
Fig. 4. The final version of the paper Fall T.I.P.S toolkit incorporating all gathered user requirements.
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126122
decrease the chance for human error through the decrease ofcognitive load on the user. The elimination of the yellow back-ground allows for greater contrast in seeing the text as well asicons. Lastly, the bright colors, large text, and large icon images areappealing and allow the poster to be seen and quickly understoodfrom a distance.
4.5. Evaluate: usability testing
Table 2 includes the usability survey results, including eachpaper Fall T.I.P.S toolkit versions’ calculatedmean, variance, and thecorresponding p-values (assuming equal variance across the two
Table 2Usability survey questions along with each group's mean, variance, and p-value. Based onagree).
Survey Question OlMean
1. I think that I would like to use these tools frequently. 2.333
2. I find the tools unnecessarily complex. 3.1483. I think the tools are easy to use. 2.6924. I think that I would need the support of a fall prevention expert to be able to use these tools. 1.852
5. I find the various functions in the tools are well-integrated. 2.593
6. I think there was too much inconsistency in available tools. 2.704
7. I would imagine that most people would learn to use these tools very quickly. 2.889
8. I find the tools very cumbersome to use. 3.2969. I felt very confident using these tools. 3.22210. I needed to learn a lot of things before I could get going with these tools. 2.423
11. I am satisfied with the tools to support the fall prevention process at this hospital. 2.481
samples). Due to multiple testing, a p-value of <0.01 was consid-ered significant. For eight of the survey questions (p-values high-lighted in red) the existing and redesigned paper Fall T.I.P.S toolkitversions showcased significant differences (p-value < a ¼ 0.01)across several aspects of usability as reported by the oncologynursing practice committee members. Survey findings indicate thatthe redesigned paper Fall T.I.P.S toolkit is easier to use and ispreferred by nurses over the existing paper fall T.I.P.S toolkit. Thethree usability survey questions which did not demonstrate sig-nificant results related to the fact that even the baseline toolkit wasconsistent with existing fall prevention practices, was relativelysimple, and did not require a lot of training to use.
the System Usability Scale, responses ranged from 1 (strongly disagree) to 5 (strongly
d (N=27) New (N=27) p-valueVariance Mean Variance
0.846 3.704 1.217 <0.001
1.746 1.667 1.077 <0.0011.502 4.222 0.949 <0.001
0.593 1.500 0.660 0.112
0.866 3.852 1.131 <0.001
1.293 2.111 1.179 0.056
1.333 4.296 1.063 <0.001
1.755 2.222 1.872 0.0051.103 4.259 1.046 <0.001
1.134 1.852 0.823 0.040
1.028 3.704 1.293 <0.001

Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126 123
5. Discussion and conclusion
At BWH, the redesigned version of the paper Fall T.I.P.S toolkitexhibited improved usability and ease of use over the existingpaper Fall T.I.P.S toolkit. Going forward, the team will evaluate theconsistency of use by nurses as they complete the redesignedpaper Fall T.I.P.S toolkit. As mentioned previously, nurses statedthat the existing paper toolkit was rarely used; therefore bycollecting how consistently the redesigned paper Fall T.I.P.Stoolkit is completed, the team will be able to evaluate the effec-tiveness of the iterative design cycle. Nurses from the oncologypractice committee stated that they thought the redesignedversion was more aesthetically pleasing, simpler to use, andeasier to gain an understanding of a patient's fall prevention planover the existing paper Fall T.I.P.S toolkit. Similar success withuser-centered design work has been seen in the field of personalhealth records (PHRs) (Brennan and Hajopoulos, 2008). WithPHRs emerging as a primary pathway for patients to maintaintheir health information outside of a healthcare setting, user-centered design is necessary to ensure the success of thesetools. As was conducted in our study, primary users of these toolsare incorporated into the iterative design process, ultimatelyleading to tools with greater usability and acceptance. Some ofthe challenges seen in user-centered design with PHRs can alsobe seen in the work conducted in this study due to the verydiverse group of users within a healthcare setting, from patientswith varying illness degree to busy clinical staff (Brennan andHajopoulos, 2008).
In relation to the RE-AIM framework, the team addressedvarious measures related to reach, effectiveness, and adoption ofthe redesigned paper Fall T.I.P.S toolkit. Reach of the redesignedFall T.I.P.S toolkit was achieved through BWH's partnership withMMC and the inclusion of their patient population. This providedtoolkit exposure to a more diverse and larger patient and clinicalpopulation than what would have been possible at BWH alone.The inclusion of the redesigned paper Fall T.I.P.S toolkit at anothermedical center enhances the likelihood of adoption of evidence-based fall prevention best practices in diverse settings. Agreater absolute number of clinical staff exposed to this newlydesigned tool, may translate to improved adoption and spread(Bakken and Ruland). In terms of effectiveness, the team attendedmultiple Patient Family Advisory Council meetings to gain patientand patient family perspectives on the use of the newly designedFall T.I.P.S toolkit. The feedback from these meetings wasconsidered during the redesign. Implementation and mainte-nance measures will be tracked following full implementation ofthe redesigned paper Fall T.I.P.S toolkit in the pilot phases at BWHand MMC.
5.1. Limitations
While almost all user requirements were satisfied with theappearance of the paper Fall T.I.P.S toolkit, one user requirementwas omitted due to a conflict with maintaining the integrity ofthe Morse Fall scale and the order of its risk factors and thepreferred order of the risk factors on the paper Fall T.I.P.S toolfrom a usability perspective. As seen in Fig. 4, the fall risks shownon the left side are in consistent order, from top to bottom, that isconsistent with the order in which they appear in the Morse FallScale risk assessment. Two users recommended that this order be
adjusted to increase the ease of use of the tool by decreasing thedistance between where a risk factor is checked off and where thecorresponding fall intervention is circled. It was decided thatkeeping the risk factor order consistent with the Morse Fall Scaleis crucial, given the fact it is a standardized scale for registerednurses and the order of risk factors was established during scaledevelopment. In addition, keeping the original order of risk fac-tors increases ease of completion by the nursing staff that isfamiliar with the validated order of the Morse Fall Scale riskfactors.
A second limitation of this study deals with the co-designprocess and evaluation of the prototypes throughout the user-centered design cycle. For future studies usability testingshould be conducted on prototypes throughout the cycle, ratherthan just on the final version. In addition, the co-design processshould consist of a more structured approach in order to bettercollect informal and formal feedback, as well as design ideasfrom both patients and nurses. One possible method which ourteam could follow can be seen in Lang, AR et al. (2014) (Langet al., 2014). The co-design process could also incorporate a“contextual inquiry method” as seen in Viitanen, J (2011) in orderto allow the team to better understand the working environmentand how the toolkit is used by nurses, patients, and familymembers (Viitanen, 2011).
A third limitation is that we did not formally evaluate the us-ability of the existing and redesigned paper Fall T.I.P.S toolkit withpatients or nurses at Montefiore Medical Center. We howevercollected qualitative feedback fromMMC nurses on the appearanceof the redesigned tool. We anticipate piloting the redesigned tool atMMC and will collect feedback regarding the implementation ofthe tool within this diverse hospital setting.
5.2. Future work
As previously stated, the paper version of the Fall T.I.P.S toolkitis only one component of a suite of tools that our team is devel-oping in the Patient-Centered Fall Prevention Toolkit project fun-ded by AHRQ. Our team is also working on developing electronictools to engage patients and the care team members in buildingevidenced-based fall prevention plans tailored to individual pa-tients' determinants of risk. This suite of tools will be available forall patients in the study units, regardless of their comfort levelwith technology and devices. The tools will provide access toevidence-based fall prevention practices facilitated either throughthe paper or electronic Fall T.I.P.S tools. An improved user-centereddesign approach, addressing the stated limitations, will be used forthe development of the electronic Fall T.I.P.S tools with Microsoft'sconventional user-centered design cycle as the underlyingconcept.
Acknowledgments
Wewould like to thank the nursing staff from all adult oncologyunits at BWH and MMC for their cooperation and insightful feed-back throughout the design process. This project was supported bygrant number P30HS023535 from the Agency for HealthcareResearch and Quality. The content is solely the responsibility of theauthors and does not necessarily represent the official views of theAgency for Healthcare Research and Quality.
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126124
Appendix A
Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126 125
References
Abras, C., Maloney-Krichmar, D., Preece, J., 2004. User-centered design. In:Bainbridge, W. (Ed.), Encyclopedia of Human-Computer Interaction. Sage Pub-lications, Thousand Oaks.
Bakken, S., & Ruland, C.. (n.d.). Translating clinical informatics interventions intoroutine clinical care: how can the RE-AIM framework Help? Journal of the
American Medical Informatics Association, 889e897.Brennan, P., Hajopoulos, K., 2008, May 8. Practical Solutions for Engaging Con-
sumers in the Design and Use of PHRs: beyond User Centered Design (Lecture).Brooke, John, 1996. SUS: a “quick and dirty” usability scale. In: Jordan, P.W.,
Thomas, B., Weerdmeester, B.A., McClelland, I.L. (Eds.), Usability Evaluation inIndustry. Taylor & Francis, London, pp. 189e194.
Chen, L.H., Warner, M., Fingerhut, L., Makuc, D., 2009. Injury episodes and cir-cumstances: National health interview survey, 1997-2007. Vital Health Stat. 10

Z. Katsulis et al. / Applied Ergonomics 56 (2016) 117e126126
10 (241), 1e55.Dykes, P., Carroll, D., Hurley, A., Lipsitz, S., Benoit, A., Chang, F., Middleton, B.,
1912e1918. Fall prevention. In: Acute Care Hospitals: a Randomized Trial.JAMA: The Journal of the American Medical Association.
Evans, D., Hodgkinson, B., Lambert, L., Wood, J., 2001. Falls risk factors in the hos-pital setting: a systematic review. Int. J. Nurs. Pract. 7 (1), 38e45.
Ganz, D.A., Huang, C., Saliba, D., et al., January 2013. Preventing Falls in Hospitals: aToolkit for Improving Quality of Care (Prepared by RAND Corporation, BostonUniversity School of Public Health, and ECRI Institute under Contract No.HHSA290201000017I TO #1.). Agency for Healthcare Research and Quality,Rockville, MD. AHRQ Publication No. 13-0015-EF.
Glasgow, R. (n.d.). EHealth Evaluation and Dissemination Research. Am. J. Prev.Med..
Glasgow, R., Mckay, H., Piette, J., & Reynolds, K. (n.d.). The RE-AIM framework forevaluating interventions: what can it tell us about approaches to chronic illnessmanagement? Patient Educ. Couns., 119e127.
Harper, R., 2008. Being Human: HumaneComputer Interaction in the Year 2020.Microsoft Research, Cambridge, England.
Hurley, A.C., Dykes, P.C., Carroll, D.L., Dykes, J.S., Middleton, B., 2009. Fall TIP:
validation of icons to communicate fall risk status and tailored interventions toprevent patient falls. Stud. Health Technol. Inf. 146, 455e459.
Kannus, P., Siev€anen, H., Palvanen, M., J€arvinen, T., Parkkari, J., 2005. Prevention offalls and consequent injuries in elderly people. Lancet 366 (9500), 1885e1893.
Lang, A.R., Kwok, T.C., Fioratou, E., LeJeune, I., Sharples, S., 2014. User-centred designof patient information for hospital admissions and patient experience.Contemporary Ergonomics and Human Factors 2014. Taylor Francis Group203e210.
Lidwell, W., Holden, K., Butler, J., 2010. Universal Principles of Design, second ed.Rockport Publishers, Beverly, Massachusetts.
Morse, J.M., 2008. Preventing Patient Falls: Establishing a Fall Intervention Program,vol. 2. Springer, , New York, p. 192.
Sondik, E., 2009. Injury episodes and circumstances: national health interviewsurvey, 1997e2007. Vital Health Statistics 10 (241). Retrieved September 21,2015.
The Joint Commission, 2015. Preventing falls and fall-related injuries in health carefacilities. Sentinel Event Alert 55, 1e5.
Viitanen, J.. (2011). Contextual inquiry Method for UserCentred Clinical IT SystemDesign. Eur. Fed. Med. Inf., 965e969.