it’s broke, so let’s fix it: anatomy of an injury, fallacy of body mechanics valerie beecher,...
TRANSCRIPT

It’s broke, so let’s fix it: Anatomy of an Injury, Fallacy of Body Mechanics
Valerie Beecher, MS, AEPErgonomics – Employee Health
Danielle Wheeler-Vickery, PTAcute Rehabilitation SUNY Upstate Medical University

History of Patient Handling

History of Patient Handling
Quotes from nursing texts:
“Occasionally the complaint is made that a nurse has injured her back or strained herself in some way in moving a patient. This will generally be because she has failed to do the lifting properly.” (Hampton, 1898, p.102)
“It is very good for strength To know that someone needs you to be strong”(Committee of the Connecticut Training-School for Nurses, 1906, preface verso).
“Lifting does not always require strength. It takes skill which the nurse can readily develop once she has made good body mechanics a habit” (Gill, 1958, p.299).
Taken from: Safe Patient Handling and Movement: A Practical Guide for Health Care Professionals, Nelson, A. Ed. (2006).

Awkward Handling
“Compared to objects manually lifted or moved in industrial settings, the body is heavier, more delicate and awkward to handle”
Source: A Back Injury Prevention Guide for Healthcare Workers; Cal/OSHA
“The adult human form is an awkward burden to lift or carry. Weighing up to 100 kg or more, it has no handles, it is not rigid, and it is liable to severe damage if mishandled or dropped. In bed a patient is placed inconveniently for lifting, and the placing of a load in such a situation would be tolerated by few industrial workers” (“The Nurse’s Load”, 1965, p.422).
Taken from: Safe Patient Handling and Movement: A Practical Guide for Health Care Professionals, Nelson, A. Ed. (2006).

National Problem of Ergonomic Injury in Healthcare Services
Top Ten Occupations for MSDs
6) Truck drivers, light and
delivery
7) Janitors and cleaners
8) Stock clerks and order
fillers
9) Construction laborers
10) Maintenance and repair
workers
1) Laborers and freight, stock, and material movers
2) Nursing aides, orderlies, and attendants
3) Truck drivers, heavy and tractor-trailer
4) Retail salesperson
5) Registered nurses
Source: US Department of Labor, Bureau of Labor Statistics, News Release, “Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work, 2006,” November 8, 2007. Accessible at www.bls.gov/iif/

National Problem of Ergonomic Injury in Healthcare Services
In 2006, nursing aides, orderlies and attendants had:
49,480 days away from work cases
An incidence rate of 526 per 10,000 workers, which was more than four times the total for all occupations.
Source: US Department of Labor, Bureau of Labor Statistics, News Release, “Nonfatal Occupational Injuries and Illnesses Requiring Days Away from Work, 2006,” November 8, 2007. Accessible at www.bls.gov/iif/

National Problem of Ergonomic Injury in Healthcare Services
In 2000, ANA reported that compared to the general workforce, nurses used 30% more sick leave annually due to back pain.
38% of the nursing workforce had been affected by back injury.
68% of disabling injuries reported by nurses were attributable to over-exertion injuries from lifting patients.
98% of patient lifting was still done manually.
Source: American Nurses Association Website, NursingWorld, Jan.-Feb. 2000

National Problem of Ergonomic Injury in Healthcare Services
ANA estimates that 12% of nurses leave the profession annually due to back injuries.
>52% complain of chronic back pain.
More than 1/3 of back injuries among nursing personnel is associated with patient handling and the frequency with which nurses are required to manually move patients.
Source: American Nurses Association Website, NursingWorld, July 2008

Cost Factors
In 1990, the annual cost of back injury ranged from $50 to $100 billion in the US
One low back injury: $40,000
Indirect costs outweigh direct costs 5:1
$20 billion per year is spent annually on workers compensation costs associated with musculoskeletal disorders (MSDs)
$100 billion per year is spent on indirect costs
Source: US Department of Labor, Occupational Safety and Health Administration
National Problem of Ergonomic Injury in Healthcare Services

National Problem of Ergonomic Injury in Healthcare Services
Reporting
In 2006 there were over 350,000 musculoskeletal disorders (MSDs) reported that required days away from work.
Many experts believe this figure represents significant under-reporting of cases.
MSDs account for 30% of all lost-workday injuries and illnesses.
Source: US Department of Labor, Occupational Safety and Health Administration

Low Back Pain Prevalence
Back injury is the #2 work-related injury in the US
Back pain is the most common reason for filing workers comp claims
Low back pain (LBP) is the #2 reason why patients are seen by an MD.
80% of adults will experience LBP.
Most of the time injury to the low back happens at work.
Source: National Institute of Occupational Safety and Health (NIOSH)

What is Low Back Pain?
Pain that originates from the spine, muscles, nerves or other structures in the back that can radiate into the lower extremities, such as tingling, burning sensation, dull or sharp ache.
Causes weakness/imbalance in strength and flexibility in the lower back and abdominal areas.

Low Back Pain Statistics
15-20% of US adult population experience back pain every year. Out of that number, another 15-20% require medical care for a minimum of 3 years. 90% LBP resolve in 6 weeks 5% LBP resolve in 12 weeks <1% LBP serious spinal disease <5% LBP true nerve root pain
Source: American Academy of Orthopaedic Surgeons

Anatomy of Lumbar Spine
1) Intervertebral disc
2) Facet joints
3) Vertebral body
4) Ligaments
5) Spinous process
6) Transverse process
7) Muscles
8) Spinal cord

Causes of Low Back Pain
Lifting of heavy objectsProlonged sittingInjury/accidentQuick movementsOther Causes:
Muscle spasms Decreasing alignment Herniated Disc (HNP) Small fractures Degenerative Disc Disease (DDD)
StenosisMuscle strains/tearsCurvature of spineFibromyalgia

Low Back Pain Disorders

Herniated Disc (HNP)
Nucleus pulposus (center of disc which is a fibrogelatinous pulp) acts as a shock absorber.
Disc protrudes outside of the center (annulus fibrosis), i.e. jelly donut when squeezed.
95% occur at L4L5 or L5S1 (center of gravity) 75% recover within 6 months Sudden onset of LBP and radicular symptoms
in leg(s).

Facet Joints
Occur in 40%; mainly extension and rotation Symptoms increase with lumbar extension “compression” Symptoms decrease with lumbar flexion “separates” Sudden attacks No radicular symptoms to buttocks or below knee.
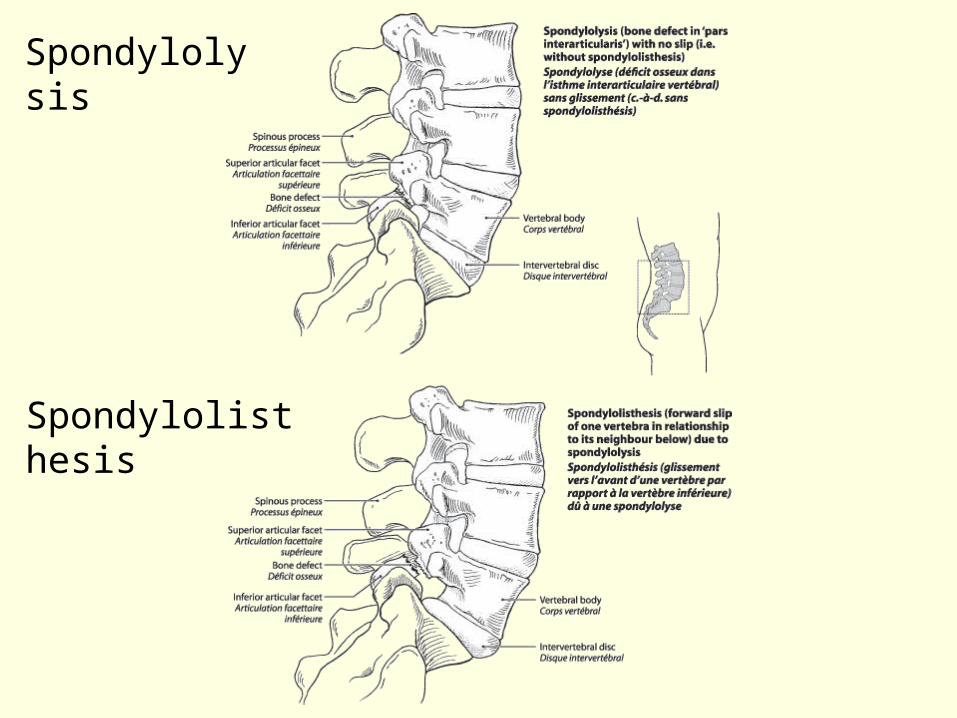
Spondylolysis
Spondylolisthesis

Spondylolysis
Stress fracture of pars interarticularisRepetitive flexion/extensionLBP with occasional
radicular symptoms past buttocks and thighs, no neurologic deficits

Spondylolisthesis
“Slipping of vertebrae”75% have LBPRestrictive ROM


DDD/Spinal Stenosis
Neurogenic claudications Pain/symptoms increase with
standing/walking (buttock and lower extremity symptoms)
Pain decreases with flexion

LBP Risk Factors
Heavy manual lifting Repetitive movement: lifting/twisting Constant vibration Poor posture Continuous work Poor physical fitness Low pain threshold Weak trunk musculature Smoking Stressed/depressed Pregnancy Arthritis

Biomechanics
How does it work together?

“It’s broke…”
Past Approaches to Reducing Injury in Healthcare
Training in body mechanics and appropriate lifting techniques, i.e. “bend your knees, not your back”.
Lectures addressing human anatomy and function of the musculoskeletal system.
Promotion of healthcare worker physical fitness.
Promotion of healthcare worker proper nutrition.
Modified from: Ergonomics, How to Contain On-The-Job Injuries in Health Care by Guy Fragala, PhD. Reprinted
with permission from Joint Commission on Accreditation of Healthcare Organizations.

Dispelling the Myth
Education on lifting techniques and training in body mechanics are not effective in reducing injuries.
Research over past 35 years reveals that these efforts by themselves have failed to reduce injury.
Most common factor contributing to ergonomic injury in healthcare is the caregiver’s tendency to exceed one’s own safe lifting capacity when handling patients, putting excess force on the spine.
Sources: Patient Safety Center of Inquiry of the Veterans Administration Medical Center (www.visn8.med.va.gov/patientsafetycenter/) and Back Injury Prevention (www.premierinc.com)

Facts
Early studies on body mechanics focused on men and nursing still consists primarily of women.
Early body mechanics studies were performed in controlled settings with boxes with handles (patients are bulky and don’t have handles!)
Patients can be combative, experience muscle spasms, or lose their balance.
A patient’s ability to assist varies.
The environment is complex.
Sources: Patient Safety Center of Inquiry of the Veterans Administration Medical Center (www.visn8.med.va.gov/patientsafetycenter/)

Facts
When the lifting capacity is exceeded, there is no way to “lift properly” or use “proper body mechanics”.
Forces exerted on the musculoskeletal system when caregivers perform patient-handling tasks are beyond reasonable limits and capabilities, regardless of technique to perform the task manually.
Training programs fail to consider that lifting, turning, and repositioning patients are frequently performed on a horizontal plane, such as a bed or stretcher, requiring the nurse to use the weaker muscles of the arms and shoulders, rather than the stronger muscles of the legs.
Sources: Patient Safety Center of Inquiry of the Veterans Administration Medical Center (www.visn8.med.va.gov/patientsafetycenter/)

Patient Handling Risk Factors Personnel Factors:
Staff shortage Healthcare worker general
health factors Poor patient handling
techniques Repetitive tasks End-of-shift fatigue Lack of equipment training Lack of time Resistance to change
Patient Related Factors: Decreased consciousness Decreased strength and
ability to cooperate Mental status and
combativeness Patient size and weight No handles Progression for patient Patient/family resistance to
equipment use
Modified from Ergonomics, How to Contain On-The-Job Injuries in Health Care by Guy Fragala, PhD.
Reprinted with permission from Joint Commission on Accreditation of Healthcare Organizations.

Patient Handling Risk Factors
Environmental Factors: Confined space of patient room and bathroom Wet and slippery floors Multiple monitors, IV poles, equipment, etc. in rooms
Equipment Factors: Lack of proper equipment (lateral transfer equipment,
bariatric equipment) Broken and poorly maintained equipment Low height of patient chairs, toilets, or high height of patient
bed
Modified from Ergonomics, How to Contain On-The-Job Injuries in Health Care by Guy Fragala, PhD.
Reprinted with permission from Joint Commission on Accreditation of Healthcare Organizations.

NIOSH Lifting Equation
Can be used to calculate a weight limit for a lifting task under ideal conditions.
Based on biomechanics, psychophysics, physiology, and epidemiology.
Recommended weight limit is 35 pounds for most patient-lifting tasks, but less when conditions are not ideal.
Reasonable to use this maximum limit to assess patient handling when equation isn’t feasible.
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.

NIOSH Lifting Equation
Not originally used for assessing the lifting of patients due to limitations: Patient unpredictability and combativeness Patient movements while lifting can create additional
loads
Can be used under ideal conditions as a guide Patient can follow directions, non-combative Weight a caregiver handles can be estimated Lifting is smooth and slow “Geometry” of the lift doesn’t change
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.

What does this mean?
Many patient-handling tasks that caregivers perform are unacceptable based on a 35-pound limit.
Few patients weigh less than 35 pounds (except in pediatrics).
Recommended weight limit (RWL) can assist with identifying tasks/situations for which the use of equipment is necessary.
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.

Patient Handling Scenarios
2 nurses helping patient to stand from chair
Patient weighs 180lbs Can assist partially
(about ½ his weight) 2 nurses need to lift 90lbs 45lbs > 35lb RWL
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.
Use lift or a sit-to-stand device

Patient Handling Scenarios
1 nurse needs to raise a patient’s leg off the bed for wound care
Patient weighs 300lbs (leg is ~16% of total body weight)
47lbs > 35lb RWL
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.
Use lift with limb sling or limb positioner

Patient Handling Scenarios
4 nurses about to move a fully dependent patient from bed to chair
Patient weighs 250lbs 4 nurses need to lift
250lbs 62.5lbs > 35lb RWL
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.
Use lift

Patient Handling Scenarios
1 nurse about to move a fully dependent patient from bed to chair
Patient weighs 100lbs 1 nurse needs to lift
100lbs 100lbs > 35lb RWL
Source: Waters, T. When is it Safe to Manually Lift a Patient? AJN 2007; 107(8): 53-58.
USE LIFT!

“…So, let’s fix it”
Change in philosophy:
Modify the job to fit the worker rather than changing the worker to fit the job.
Lifting techniques are still important but no longer the only key elements.
Elimination or modification of lifting activities is more effective. Use task analysis and patient assessment.
Use engineering solutions (such as patient lifts, friction-reducing devices, or transfer belts to reduce risk of injury).
Standardized processes for equipment, sling and staff selection.

Questions?