it’s more than checklists - open | home · scrub nurse/tech resident, pa, perfusionist, others...
TRANSCRIPT

Teamwork and
Communication for
Quality & Safety:
James P. Bagian, MD, PE
Director
Center for Healthcare Engineering and Patient Safety
University of Michigan
It’s More Than Checklists

Overview
Problem
Background
Strategy
Interventions

VA – 2001-2006

Root Cause Analyses (RCA)
Database*
~70% to 80% of RCAs cited COMMUNICATION FAILURE as, at least one of the root causes/contributing factors for an adverse event or close call report.
*SPOT Database: VA National Center for Patient Safety, April, 2008 Completed RCAs, Number = 8661.


Assumptions
Current OR situation was unacceptable
Communication was factor
Improvement was possible
The risk from intervening was less than
the status quo
Didn’t require absolute evidence base,
evaluate on the fly

Communication Skills
In medical school and nursing
school, the focus is on
successful communication
with the patient.

Aviation Safety
&
Crew Resource Management
(CRM)

Tenerife – March 1977
Pan Am KLM

Fatalities - 583

Crew Resource Management
(CRM)*
Origin: 1979-80 NASA workshops examining the role of human error in airline crashes Research into aviation accidents in 1970s
Definition: “Using all available sources – information, equipment, and people – to achieve safe and efficient operations.”
Focus: safety, efficiency, and morale of humans working together
LOFT: “Line Oriented Flight Training” Work in flight simulators and measurement of airline crew
performance
Briefings and Debriefings * Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future
directions. Harvard Health Policy Review. 2004; 5(1): 25-35.

CRM Training*
Required by FAA and worldwide – “the way of doing business”
Aircrew performance measured by materials, organization, individual, and group variables
Expanded aviation training from technical focus to human factors dimensions – stress, fatigue, communication, shared awareness, and teamwork
Outcomes: efficiency, safety, customer satisfaction
Airline crew surveys: CRM relevant, useful, and effective in changing attitudes and behavior to improve safety
CRM accepted by industry on face validity
* Musson D, Helmreich RL. Team training and resource management in health care: Current issues and future
directions. Harvard Health Policy Review. 2004; 5(1): 25-35.

Corrigan J, Kohn LT, Donaldson MS. To Err Is Human. Washington, DC: National Academy
Press; 2000.
“…establish team training
programs for personnel in critical
care areas using proven methods
such as the crew resource
management training techniques
employed in aviation.”
Institute of Medicine

Teamwork

What are the characteristics of a
TEAM?

Characteristics of a Powerful
Team
Common Purpose
Clear Roles
Accepted Leadership
Effective Processes
Solid Relationships
Excellent Communications
Exceptional Results

18
VHA NCPS Medical Team Training Program
2005 -2010
Mean = 74 Attendees Per Learning Session
Largest One Day Session = 208 (Baltimore, MD Jan 14, 2010)
Largest Facility Attendance = 356 (Dallas, TX December 9-11, 2008)

MTT Plan
Identify and guide implementation
team at site
Define responsibilities, goals, and
tools (e.g., checklist content)
Baseline data – e.g., SAQ
OR-wide training on communication,
briefings and debriefings
Follow-up, measure and assist/advise
Months Prior
Weeks/Days Prior
Implement
Months

Culture Measurement
Survey open to all MDs, RNs, Techs in OR
and PACU
SAQ (Safety Attitude Questionnaire)
Nationally accepted, validated, normed
Short (~35 questions)
Online
Anonymous
Shorter and more focused than AHRQ

Briefings
Dialogue among principals using
concise, relevant information to
promote clear and effective
communication
- Real time
- Face-to-face
- All team members present
- All team members participate

Why Do a Briefing?
Establish a platform for common
understanding
Gives people permission to be frank & honest
Gets everyone on the same page
Provides a structure for collaborative
planning
Creates a shared mental model

23

Situational Awareness
Definition: The continuous perception of
self and team in relation to the dynamic
environment and the ability to make
adjustments.
The one most important aid in maintaining
Situational Awareness is a common
understanding of the briefed plan.

Pre-Op Briefing
Entire Surgical Team
Attending surgeon
Anesthesiologist/CRNA
Circulator
Scrub nurse/tech
Resident, PA, perfusionist, others
Guided by checklist
OR suite prior to anesthetic induction
Does not replace pre-op planning
Complements the TIMEOUT

Supporting Long Term
Memory Checklists
Put knowledge in the world vs. in the head
Recognition is better than recall
Tool to Guide and Improve Communication
Checklist Philosophy
“Read and Verify” checklists
“Read and Do” checklists

Read and Verify

Read and Do

IV Insertion Checklist
Before Insertion
• Patient Identification……………………………..CONFIRMED
• Correct Side………………………………………CONFIRMED
• Catheter Size……………………………………..CONFIRMED
• Equipment…………………………………………AT BEDSIDE
• Patient……………………………………………..BRIEFED
After Insertion
• Tourniquet…………………………………………REMOVED
• Line………………………………………………...FLUSHED
• Pump……………………………………………….SET (with fluids)
• Sharps………………………………………………DISPOSED
• Site…………………………………………………..LABELED
• Documentation…………………………………….COMPLETE

Checklist-Driven Preoperative Briefing

Checklist-Driven Preoperative Briefing

Post-op Debriefing
Entire Surgical Team Attending surgeon Anesthesiologist/CRNA Circulator Scrub nurse/tech Resident, PA, perfusionist, others
Guided by checklist
What went well? What did not go well? What can we do to improve our processes? What did we learn?
Timing – when patient is stable before attending leaves (update prior to patient leaving OR)
Method to track debrief items and follow-up:
Leadership Group




The Checklist is the Tool that
Provides the Framework for
Communication

Communication Techniques
Communication techniques
Call out/transparent thinking
Directed communication
Closed-loop communication / Feedback
Read back / Repeat back
Teamwork, communication protocols
Dynamic Skepticism
Assertive statements / wording
3 W’s, SBAR, 4 steps

Dynamic Skepticism
Attitude of constantly questioning and
evaluating the patient care environment
Avoid trusting what appears to be obvious
Do not assume!
Seek facts
Verification is NOT a mistrust of others
Questioning and verifying is safe practice

Asking the Right Question
“Any questions?”
VS
“What is your biggest concern for today?”

Clarity
Communication should be
Specific
Direct
Concise
DO NOT “Hint and Hope”

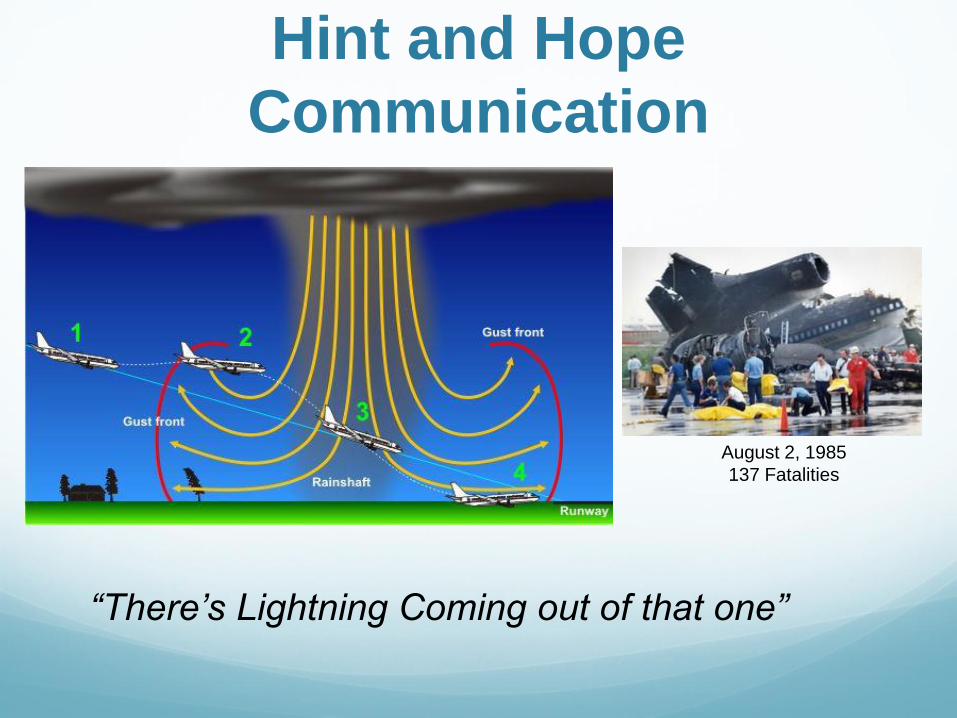
Hint and Hope
Communication
“Boy that grass is really getting tall out there!”
Hint and Hope
Communication
“There’s Lightning Coming out of that one”
August 2, 1985
137 Fatalities

3 “W”s
1. What I see
2. What I’m concerned about
3. What I want

SBAR
Situation What is the problem?
Background Brief background information
Assessment What is your assessment of the patient?
Recommendations
What do you recommend?
Response Close the loop
R

Assertive Statements
Direct and clearly communicated statements that facilitate patient advocacy in decision-making.
• Not a license to be rude
• Use “I” statements, rather than “You” statements
• “I” statements describe your experience rather than another’s shortcomings
• Give people options

4 Step Assertive Communication Tool 1. Get Attention - State name/position - Strip away title
2. State concern - Preface with “I’m uncomfortable” 3. Offer Alternative - …….
4. Pose question - to get resolution
Assertive Communication Standardized Communication Tools
“Assertiveness with Respect”

When all else fails?
Chain of Command

Avoid Hint and Hope
1. Specific 2. Direct 3. Concise
3 W’s
1. What I see
2. What I’m concerned about
3. What I want
4 Step Assertive Tool
1. Get Attention
2. State Concern
“I’m uncomfortable with…”
3.Offer Solution
4.Pose Question
Use Chain of Command
SBARR
TAKE ACTION
OR
STEP BACK
Engage Team

Results

**
Carney, et al, Differences in Nurse and Surgeon Perceptions of Teamwork.
AORN J. 2010Jun;91(6):722-9
Are they working in the same OR?

Medical Team Training Safety Attitudes Questionnaire
* *
* P < 0.05 paired, Students t-test N = 3138 Questionnaires
In this clinical area, it is easy to speak up. I would feel safe being a patient here.

0
2
4
6
8
10
% T
urn
ov
er
Pe
r Y
ea
r
Pre Post
Operating Room
Nursing Turnover
P = 0.02
45 Operating Rooms and 35 Intensive Care Units
Pre = 12 Months Prior to Learning Session
Post = 12 Months Following Learning Session

Leadership Participation Matters

0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
TeamClimate SafetyClimateJobSa sfac on StressRecogni on
Percep onofmanagemnent
WorkingCondi ons
Diiferencebetw
eenM
axandM
inresponse(byroleave.)
SAQDimension
TeamConsensus:DisparitybetweenPhysiciansandNurses
(Smallnumbersarebe er)
2011disparity
2012disparity

Positive Consensus, Before and After MTT
0%
10%
20%
30%
40%
50%
60%
Team Climate Safety Climate Job Satisfaction Stress Recognition Perception of
management
Working Conditions
SAQ Dimension
% c
on
sen
su
s
PreMTT
PostMTT

Improved Results after One Year

MTT – Facility Level Impact
67% High Impact on OR Staff
73% High Impact on OR Patients
69% of OR Teams Improved Teamwork
66% of OR Teams Report Improved Efficiency
Eqpt Util (61%), Starts (35%), Duration (19%)
Safety Attitudes Questionnaire (SAQ) Significant Improvement (p<0.001):
Working Conditions, Perception of Mgmt, Job Satisfaction, Safety Climate, & Teamwork

Neily et al. Assoc. Between MTT and Surg Mortality. JAMA. 2010;304(15):1693-1700.



MTT Impact - VA
N=108; 74 MTT, 34 Control
MTT 50% greater decrease in mortality &
morbidity than Control, 18% & 17% respectively
Dose-response –
0.5 deaths/1000 procedures less per quarter
p=0.001
0.6 deaths/1000 procedures per increase in
briefing/debriefing p=0.001
70% reduction in reported OR related harm

Debriefings
Provide near real-time feedback
Must be prepared to handle reports
Prioritization
Action
Feedback must prompt to prevent cynicism
The engine for continuous improvement



Obstacles to Performing the
Debrief - Summary
Transparency and Feedback are the key


60%
44%
75%
27%
100%
36%
73%
100%
60%
0%
20%
55% 47%
71%
17%
0%10%20%30%40%50%60%70%80%90%
100%
Ora
l(10)
Oto
lary
ngolo
gy(1
8)
Neuro
(16)
Pla
stic
s(2
6)
Oph
thalm
olo
gy(1
)
Orth
op
aed
ics(1
4)
End
ocrin
e(1
1)
Tra
nspla
nt(1
)
Hepa
tobilia
ry(5
)
Co
lore
cta
l(0)
Gyne
colo
gy(1
0)
Uro
logy(1
1)
Min
imally
Invasiv
e(1
5)
Onco
log
y(7
)
Tra
um
a B
urn
(12)
Pod 1 Pod 2 Pod 3
Debrief Participation For the week of Dec. 23
Se
rvic
e (#
Ca
se
s)
Increase from last week
No change from last week
Decrease from last week






Observational Data



MTT Summary
Systems Approach – Surgical issues must be
dealt with in the extended peri-operative period,
not solely in the OR Entire System of care must be Examined and
Engineered with desired results in mind – avoid
unintended consequences
Team Training – start in initial training & sustain
More than SBAR – Leadership Must Be Involved
Checklist-guided briefings and debriefings Can’t rely on individuals being careful (vigilant)
Compliance – Trust But Verify Consequences for Deliberate Non-Compliance

Beyond the Operating Room


Slide Title
Text here
Creating a
Shared
Mental
Model

If patients know what to
expect… they are
more likely to identify
and question an
unexpected or
unplanned event

• Providers Orders extracted from the electronic medical record
• Limited to current date
• Printed for each patient

Straightforward
Implementation
Nurses Review the Daily Plan with patients to:
Identify potential errors
Explain the day’s activity
Encourage questions
Provide patient education

17.6% of
the nurses
found at
least one
error as the
result of
The Daily
Plan

Improves the patient satisfaction
Strengthens communication
Provides patient education
Facilitates continuity of care

Conclusions Need to Provide Recurrent Teamwork Training
– Not ‘One and Done’ for OR and Floor
Data show that people more likely to be “on
the on same page” post implementation
MTT process (Debriefing) highlights issues
that need attention Must continue to improve system in place to deal
with debrief comments – Avoid BLACK HOLE
EFFECT
Ongoing Process – Requires Leadership

Move From:
Resistance
Pro forma Compliance