iv anaesthetics
TRANSCRIPT

Intravenous Anesthetic Agents

Introduction
Used IV anesthetic drugs are:
1. Propofol ,Fospropofol
2.Thiopentone, Methohexital
3.Ketamine
4.Etomidate
5.Benzodiazepines (Diazepam, midazolam, lorazepam)
6.Dexmeditomidine
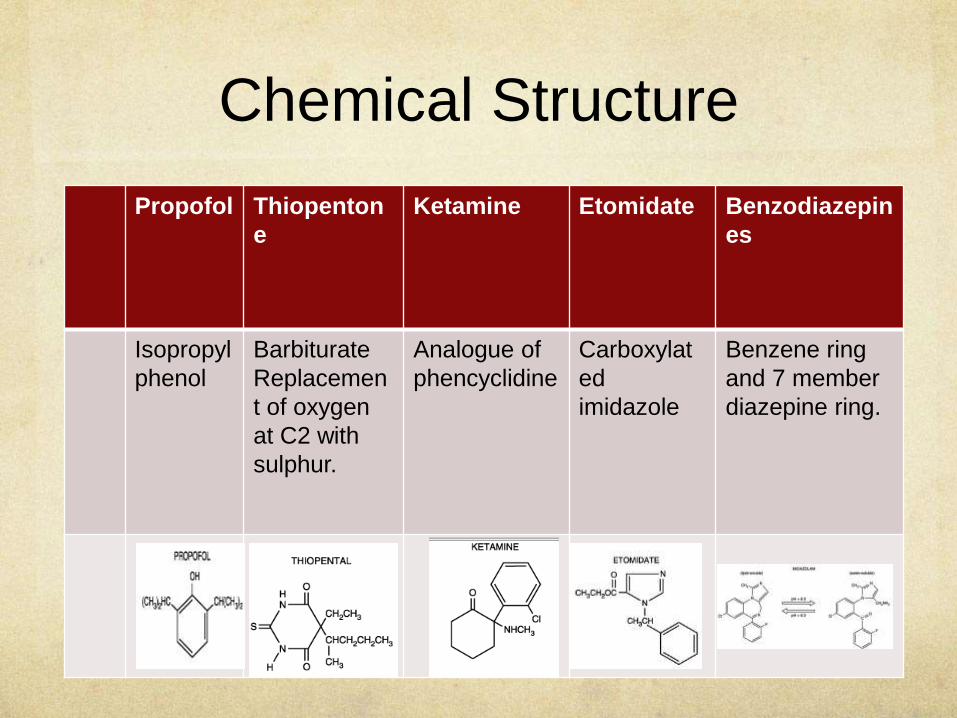
Chemical Structure
Propofol Thiopenton
e
Ketamine Etomidate Benzodiazepin
es
Isopropyl
phenol
Barbiturate
Replacemen
t of oxygen
at C2 with
sulphur.
Analogue of
phencyclidine
Carboxylat
ed
imidazole
Benzene ring
and 7 member
diazepine ring.

Physio chemical propertiesPRPOFO
L
THIOPENTONE KETAMINE ETOMIDATE BENZO-
DIAZEPINE
Colour Emulsion
*, milky
white
Sodium salts Clear
aqueous
solution
Clear solution Midazolam-
Clear aqueous
solution.
Conc. 1%, 2%
soln.
Medium,
long chain
triglycerides
Yellow amorphous
powder.
500mg, 1g
1%, 2%,10%
solution
2mg/ml in
35%
propylene
glycol
Lipid
Solubility
Only in
emulsion
form
Highly soluble Very Lipid
soluble
Acidic pH lipid
soluble
Lipid soluble
midazolam
Water
solubility
Insoluble Readily soluble Soluble Poorly water
soluble.
Water soluble
ph 4.5-6.4 10.5 3.5-5.5 6.9 3.5
pKa 11 7.6 7.5 4.2 6.15
Chirality Not chiral Racemic mixture Racemic Single isomer
R+

PROPOFOL
Neeeds an emulsifying agent: 1% (w/v) propofol10% soyabean oil 2.25% glycerol 1.2%purified egg phosphatide Di-sodum edetate (0.005%)
Supports bacterial growth. E.Coli and Pseudomonas.
Aseptic technique should be used during administration.
KETAMINE
Racemic mixture S+
isomer.
THIOPENTONE
Cannot be mixed with catecholamines, opioids and NMB drugs.
Powder form stable at room temp indefinately. Refrigerated- 2weeks Room temp reconstituted- 6 days
BENZODIAZEPINES:
Have a reversible ring
structure that opens at a pH
<6 and closes at pH>6.

METABOLISM
PROPOFOL THIOPENTONE KETAMINE ETOMIDATE BENZO-
DIAZEPINE
S
Liver
Ring
hydroxylation
by CytP450
4-hydroxy
propofol.
CONJUGATION
Glucuronidation
and sulfation
EXCRETED
Kidney
Inactive
metabolite
Liver
Oxidation, N-
dealkylation,
desulfration and
destruction of
barbituric acid ring.
EXCRETED
Kidneys and bile
Inactive metabolite
Liver
Demethylatio
n of ketamine
by P-450
Nor-
KetamineACTIVE
METABOLITE
Hydroxylated
and
conjugated
Water
soluble
glucuronide
metabloite.
EXCRETED
Kidney
Liver and
plasma
esterase.
Hydrolysis of
ethyl ester side
chain.
Carboxylic acid
ester.
EXCRETED
Kidney
Inactive
metabolite
Liver
1-hydroxy
midazolam.
N-dealkylation
and aliphatic
hydroxylation/
glucuronide
conjugation.
EXCRETED
Kidney
Phase I
metabolite is
active.

PharmacokineticsPROPOFOL THIO-
PENTONE
KETAMINE ETOMIDATE BENZO-
DIAZEPINES
ONSET 15-45s <30s 45-60s 15-45s 30-90s
AWAKENING 5-10mins 5-10mins 10-20mins
Full orientation
60-90mins
3-12 mins 15-30mins
RATE OF
FALL IN
PLASMA
CONC.
Redistribution
and elimination
redistribution redistribution
CONTEXT
SENSITIVE
HALF LIFE
<40mins <150mins
EXTRACTION
RATIO
low high high
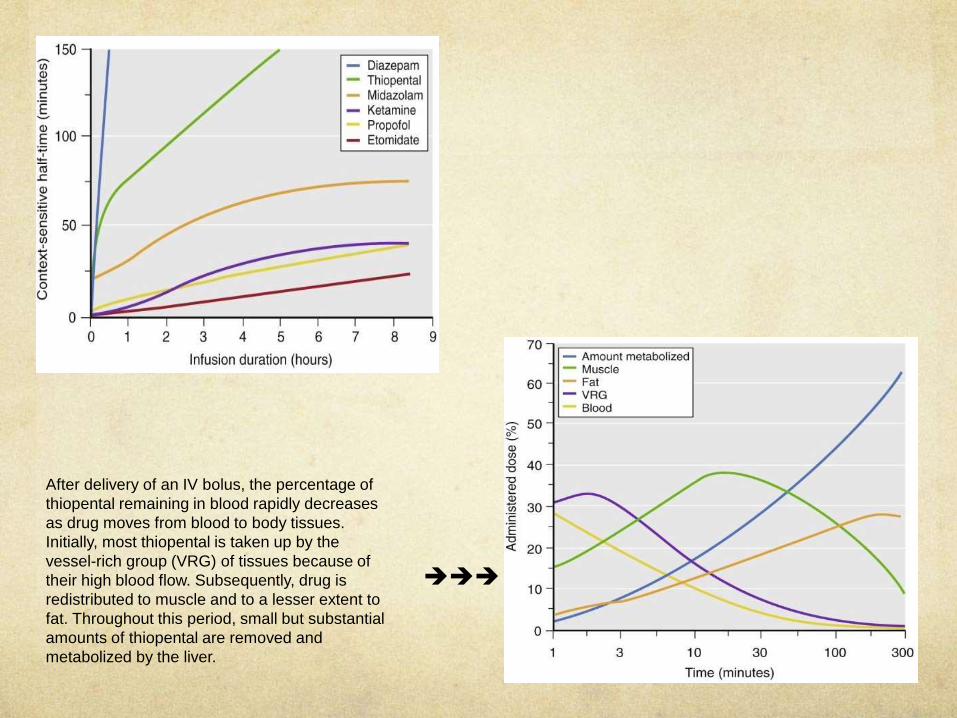
After delivery of an IV bolus, the percentage of
thiopental remaining in blood rapidly decreases
as drug moves from blood to body tissues.
Initially, most thiopental is taken up by the
vessel-rich group (VRG) of tissues because of
their high blood flow. Subsequently, drug is
redistributed to muscle and to a lesser extent to
fat. Throughout this period, small but substantial
amounts of thiopental are removed and
metabolized by the liver.

Mechanism of action
PROPOFOL THIOPENTONE KETAMINE ETOMIDATE BENZO-
DIAZEPINES
Selective
modulator of
GABAa
increasing
affinity for
GABA.
Depress RAS in
brain stem.
Action via GABAa
receptor, increases
the duration of
opening of chloride
channels.
Non
competitive
binding to
phencyclidine
site on NMDA
receptors.
Weak action
at GABA.
Dissociates
THALAMUS
from LIMBIC
CORTEX.
Depresses RAS
in the brain
stem.
Binds to a
subunit of the
GABAa receptor
increasing
affinity for
GABA.
Bind to GABAa
receptor but
different site.
Increase the
frequency of
opening of the
chloride ion
channel.

SYSTEMIC EFFECTS

CENTRAL NERVOUS
SYSTEMPROPOFO
L
THIOPENTONE KETAMNE ETOMIDATE MIDAZOLAM
CMRO2
CBF
ICP
IOP − − −
DISSOCIATIVE
ANESTHESIA
✕ ✗ ✔ ✕ ✗
EMERGENCE
REACTION
✕ ✗ ✔ ✕ ✗
NYSTAGMUS ✕ ✗ ✔ ✕ ✗
SKELETAL MUSCLE
TONE
− − − −
SALIVATION
LACRIMATION
− − − −

PROPOFOL THIOPENTONE KETAMINE
NEURO-
PROTECTIV
E
• Anti oxidant
properties.
• Reduced infarct
size when
administered
immediately or 1hr
after ischemic
insult
• Decreases oxygen
demand
• Preserves CPP
(cerebral perfusion
pressure)
• Robin Hood
phenomenon
• Free radical
scavenging
• Improves
perfusion in
incomplete
cerebral
ischemia
THIOPENTONE KETAMINE ETOMIDATE
EEG
changes
• Small dose-low voltage
fast wave activity
• High dose-high voltage
slow wave activity
• Continuous infusion-
isoelectric EEG
• Abolotion of alpha
rhythm and
dominance of
theta activity.
• Onset of delta
activity co incides
with loss of
consciousness.
• Produces burst
supression at high
dose.
• Similar to
thiopentone but
frequency of
excitatory spikes
is more

CVS
PROPOFOL THIOPENTONE KETAMINE ETOMIDATE BENZO
DIAZEPINES
BP 25-40% −
unchange
d
HR Inhibits
tachycardic
response to
hypotension
.
May cause
bradycardia
−
unchange
d
CO −
unchange
d

Respiratory System
PROPOFO
L
THIOPENTONE KETAMINE ETOMIDATE BENZODIAZEPINE
S
APNEA ++ ++ + LARGE
DOSE
+ RAPID
INJECTION+
VENTILATOR
Y DRIVE
BHRONCODIL
ATATION✔ ✗ ✔✔ ✗ ✗
AIRWAY
REFLEXES intact intact intact intact

DOSESPROPOFOL THIOPENTO
NE
KETAMINE ETOMIDATE BENZO-
DIAZEPINE
S
Induction 1-2.5 mg/kg IV 3-4mg/kg 0.5-2 mg/kg
IV4-6 mg/kg IM
0.2-0.6 mg/kg
IV
0.05-
0.15 mg/kg
Maintainence 50-
150 µg/kg/min
IV combined
with N2O or an
opiate
50-100mg
every 10-20
mins
0.5-1 mg/kg IV
with N2O 50%
in O2 15-
45 µg/kg/min
IV with N2O
50-70% in O2
10 µg/kg/min
IV with N2O
and an opiate
0.05 mg/kg prn
1 µg/kg/min
Sedation 25-
75 µg/kg/min
IV
0.2-0.8 mg/kg
IV over 2-3 min
2-4 mg/kg IM
0.5-1 mg
repeated
0.07 mg/kg IM
Analgesia 0.15-
0.25 mg/kg IV.
Preventive/pre
emptive.
Anti-emetic 10-20 mg IV,
repeat every 5-
10 min or start
infusion
10 µg/kg/min

Drug interactions
PROPOFOL THIOPENTON
E
KETAMINE ETOMIDATE BENZODIAZE
PINE
• Fentanyl and
Alfentanyl
concentration
s may be
increased
with
concurrent
administratio
n.
• Contrast
media and
drugs that
occupy the
same protein
binding sites
can displace
drug.
• Ethanol,
opioids and
anti
histamines
potentiate
the CNS
depressant
effect.
• Interacts
synergisticall
y with volatile
anesthetics
• Midazolam
attenuate
ketamines
cardio-
stimulatory
effect.
• Fentanyl
increases its
plasma level
• Opioids
decrease the
myoclonusch
aracteristic.
• Eryhtromycin
inhibits
metabolism
of midazolam
• In
combination
with opioids
BP falls.
• Reduce the
MAC of
volatile
anesthetics
as much as
30%

USES
POPOFOL THIOPENTON
E
KETAMINE ETOMIDATE BENZODIAZE
PINE
INDUCTION ✔ ✔ ✔ ✔ ✔
SEDATION ✔ − ✔ ✔ ✔
MAINTAINENC
E
✔✔ ✔ ✔ ✔ ✔
ANALGESIA ✗ ✗ ✔✔ ✗ ✗
PRE-EMPTIVE
ANALGESIA
✗ ✗ ✔✔ ✗ ✗
ANTI EMETIC ✔✔ ✗ ✗ ✗ ✗
ANTI
PRURITIC
✔ ✗ ✗ ✗ ✗
ANTI
CONVULSANT
✔ ✔ ✗ − ✔
CHR.
HEADACHE
✔ ✗ ✗ ✗ ✗
AMNESTIC ✔ − ✔✔ − ✔

Side EffectsPROPOFOL THIOPENTO
NE
KETAMINE ETOMIDATE BENZODIAZ
EPINE
Pain on
injection
✔✔ ✔ ✗ ✔ ✗
Hypotension ✔✔ ✔ ✗ ✔ ✗
Bronchospas
m
✗ ✔ ✗ ✗ ✗
Allergic rxn ✔ ✔ ✗ ✗ ✗
Emergence
rxn
✗ ✗ ✔ ✗ ✗
Thrombophle
bitis
✔ ✔✔ ✗ ✗ ✗
Hangover
effect
✗ ✓ ✔ ✗ ✗
Tolerance and
dependence
✔ ✔ ✔ − −
Immunosuppr
ession
✔ − − ✔
Neutrophil
func.
✗ −

Other side effects
PROPOFOL: Risk of bacterial infection
Hypertriglyceridemia
Pulmonary Embolism
Propofol infusion syndrome: Lactic acidosis
>75mcg/kg/min for >24hrs
Unexpected tachycardia with increased anion gap
MOA- Poisoning of ETC
D/D: Hyperchloremic metabolic acidosis
Diabetic Ketoacidosis

ETOMIDATE:
Adrenocortical suppression, inhibition of 11-beta
hydroxylase.
Lasts for 4-8hrs after induction.
KETAMINE:
Emergence delirium
Symptoms: Visual auditory proprioceptive and confusional
illusions. Transient
cortical blindness.
Dreams (morbid) Hallucinations.
Mechanism: Ketamine induced depression of inferior colliculus
and medial geniculate body
Incidence: Age>15, Female, Dose>2mg/kg, H/O personality
problems
Prevention: Benzodiazepines pre-operatively 5mins before
induction.

DEXMEDITOMIDINE
Highly selective α2 adrenergic agonist.
Physicochemical properties: Active S enantiomer of meditomidine.
Water soluble.
Pharmacokinetics:
Rapid hepatic metabolism.
Conjugation.
Metabolites excreted through urine and bile.
Clearance high, elimination half life short.
Significant increase in context sensitive half time from 4mins after
10min infusion to 250 mins after 8hr infusion

Pharmacodynamics:Activation of CNS α2 receptors. Hypnosis is due to this activation in locus cerulus. Analgesia at the level of spinal cord. Sedation resembles physiologic sleep state. Decreases CBF no significant change in ICP.
CVS: HR & SVR BP Heart block asystole or sever bradycardia may occur.
RS: Mod decrease in tidal volume. Upper airway obstruction due to sedation possible.
Uses: Short term sedation of ICU patients. Adjunct to GA. Sedation during fiberoptic intubation/ regional anesthesia.
DOSE: 0.5-1mcg/kg over 10-15mins followed by infusion of 0.2-0.7mcg/kg/hr.

References
Millers 7th edition
Clinical Anesthesiology- Morgan 5th edition
Stoeltings handbook of pharmacology and
physiology in anesthetic practice. 4th edition
Clinical Anesthesia Barash 7th edition