izben c. williams, md, mph instructor. substance abuse the abuse of alcohol and other psychoactive...
TRANSCRIPT

BEHAVIORAL SCIENCE
IzBen C. Williams, MD, MPHInstructor

SUBSTANCE ABUSE
The Abuse of Alcohol and other
Psychoactive Substances

Overview
Definitions:Substance use disorders are divided
into…….1. Substance abuse – 2. Substance dependence:
1. Abuse plus withdrawal symptoms, tolerance or a pattern of repetitive use
2. Concept of cross tolerance

OverviewDefinitions:
Substance abuse is the use of a psychoactive substance (drug) to such an extent that it seriously interferes with health or occupational and social functioning (obligations, interpersonal and legal problems, risks, )This definition is objective and non-judgmental.
The emphasis is on dysfunction rather than on social or cultural norms, or on the enhancement of pleasure or performance
OverviewSubstance abuse is a major public
health problem globallyAlcoholism is the most common
substance use disorderIn the USA, deaths associated with
alcohol abuse and alcoholism now rank third behind heart disease and cancer
Certain basic principles of diagnosis and treatment apply to all psychoactive substance use disorders

OverviewDefinitions:
Substance dependence is a pathologic pattern of substance use that results in impairment or distress. Characterized by:Withdrawal: physiological and/or psychological
symptoms after reduction or cessation of intake of a substance
Tolerance: decreased effect with continued use of the same amount of the substance
Other characteristics: CAGE features, time spent, physical or mental problems, compromises commitments

OverviewDefinitions:
Physiologic dependence
Refers to the presence of either tolerance or withdrawal
OverviewObservation:
Although the focus in this lecture is on “recreational” drugs, it should be noted that prescribed psychoactive medications can also be abused
Physicians who prescribe such drugs have a responsibility to monitor their effects on a patient and to ensure that dependence or toxicity are not developing

Illicit drug use profile
The use of Illicit drugs in the USA has been increasing.In 2002, an estimated 8.3% of the population aged
12 or older had used an illicit drug or abused a psychotherapeutic medication (such as a pain reliever, stimulant, or tranquilizer) in the past month.
In 2012, that figure stood at 9.2 % of the population.
The increase mostly reflects a recent rise in the use of marijuana, the most commonly used illicit drug.
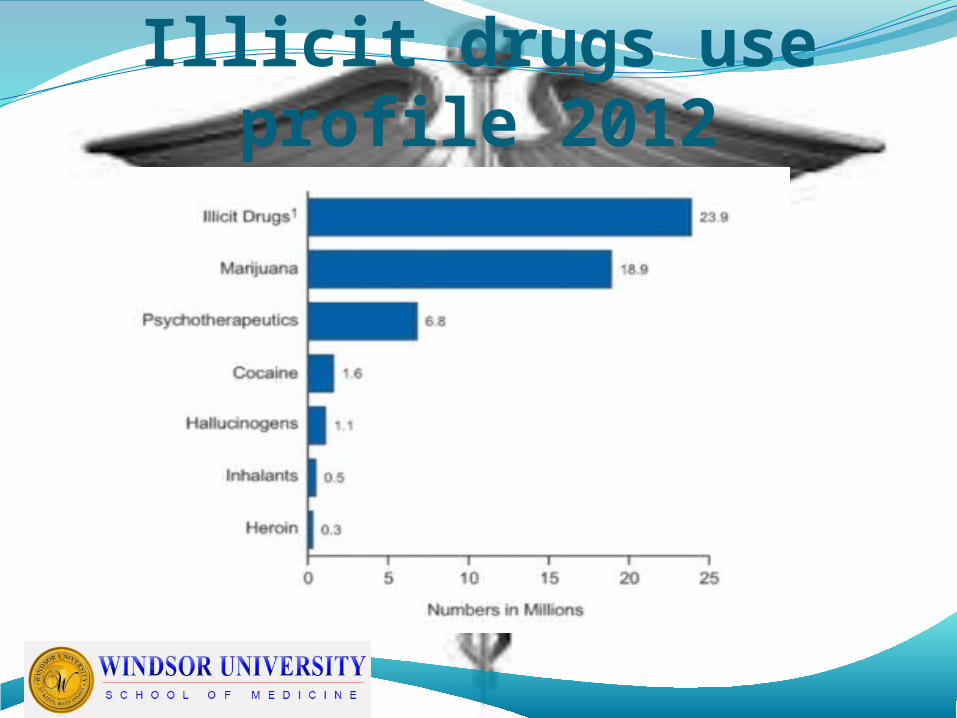
Illicit drugs use profile 2012

Illicit drug use trends
Illicit drug use profile
The use of Illicit substances is more common among young adults, ages 18-25And it is twice as common in males
Most abused substances can be administered by a number of routes
Routes that provide quick access to the bloodstream, and hence the brain, are often preferred by abusers

Specific-substance use
ClassificationA. CNS StimulantsB. Sedatives, Hypnotics and AnxiolyticsC. OpioidsD. Hallucinogens and PhencyclidineE. CannabisF. Inhalants

Specific-substance use
A. CNS StimulantsThey include:
Caffeine, Nicotine Amphetamines and related compoundsCocaineMethamphetamine Phenmetrazine

Specific-substance use
A. CNS StimulantsIncrease the availability of
dopamine:Amphetamines cause the release of
dopamineCocaine blocks the reuptake of dopamineIncreased availability of dopamine at the
synapse is believed to be involved in the euphoric effects of stimulants and opioids
Specific-substance use
A. CNS StimulantsUse of Amphetamines
Depression in the elderly and in the medically ill who cannot tolerate antidepressants,
Augmentation of antidepressants in treatment-resistant depression
NarcolepsyADD in children & Adult (residual) ADD
The most common clinically used amphetamine is methylphenidate (Ritalin)

Specific-substance use
A. CNS StimulantsCocaine
Clinically used for nosebleed and in local anesthetic of the ENT
NicotineToxic to all systems and decreases life
expectancy more than the use of any other substance
Specific-substance use
A. CNS StimulantsCocaine
Intoxication: euphoria, fighting, grandiosity, confused speech impaired judgment, high » crash » withdrawal
Withdrawal: dysphoric mood, irritability, anxiety, fatigue, agitation, occurs within 24 hrs after cessation of last use
Delirium: within 24 hoursDelusional Disorder: usually persecutory, distorted
body images and faces » aggression and violence

Specific-substance use
B. Sedatives, Hypnotics and Anxiolytics
These are CNS depressants; they include:(Alcohol)Barbiturates and related drugsBenzodiazepines (tranquilizers and
hypnotics)Chloral compounds (eg chloral hydrate)

Specific-substance use
B. Sedatives, Hypnotics and AnxiolyticsThis group of drugs work primarily by
increasing the activity of the inhibitory neurotransmitter GABA
Withdrawal effects could be life threatening (include seizures, and CVS compromise) so inpatient care for withdrawal is often necessary and advisable

Specific-substance use B. Sedatives, Hypnotics and AnxiolyticsAlcohol associated problems:
Acute: relational, suicide, abuse, rape, various indiscretions and infarctions
Chronic: Thiamine deficiency, GI, fetal, liver, CNS including DTs,
IntoxicationLegal intoxication .08%-.15% bacComa usually above .50% dependent on use
history

Specific-substance use B. Sedatives, Hypnotics and
AnxiolyticsBarbiturates:
Uses: sleeping pills, sedatives, tranquilizers, anticonvulsants, anesthetic
Clinically: respiratory depression, low safety margin (suicide), risk of death from withdrawal

Specific-substance use B. Sedatives, Hypnotics and
AnxiolyticsBenzodiazepines:
Uses: tranquilizers, sedatives, muscle relaxants, treats alcohol withdrawal,
Clinically: by itself high safety marginBenzodiazepine receptor antagonists such as
s Flumazeni can reverse benzodiazepine effects in cases of overdose

Specific-substance use
C. OPIOIDS - These include
Morphine Alphaprodine
Hydromorphone Oxycodone
Oxymorphone Levophanol
Heroin Meperidine
Methadone Propoxyphene
Codine Hydrocodone
Specific-substance use
C. OpioidsUses:
Analgesia (morphine), drugs of abuse (heroin),
Clinically:Abused opioids cross bbb, have a faster
onset of action, and are more euphoric than medically used opioids, death from withdrawal rare

Specific-substance use
C. OpioidsMethadone is a synthetic opioid
Others are LAMM and Buprenorphine (Temgesic) Uses: treatment of heroin addiction but can itself
cause physical dependence and tolerance. ‘legal’ opioids can be substituted for illegal opioids to prevent withdrawal symptoms
Advantages over heroin: can be taken orally, have a longer duration of action, and can block both the withdrawal and euphoric actions of heroin (temgesic); they also cause less euphoria and drowsiness

Specific-substance use
D. Hallucinogens and Phencyclidine
They include:Lysergic acid diethylamide (LSD)MescalinePhencyclidinePsilocybin
Specific-substance use D. Hallucinogens and Phencyclidine
These drugs produce altered states of consciousness, mediated by increased availability of serotonin
LSD is ingested and PCP is smoked in marijuana (*) or cigarette
Both cause altered perception (bad trip) with intoxication
PCP causes more episodes of violent behavior, hypothermia and nystagmus, and consumption of more than 20 mg may cause convulsion, coma and death

Specific-substance use
E. Cannabis -1Specific substances include:
MarijuanaHashish∆-tetrahydrocannabinol (THC)

Specific-substance use E. Cannabis -2Intoxication by marijuana and related
substances rarely produces hallucinations More common side effects are Euphoria, anxiety, increased suggestibility,
distortion of time and space, increased appetite
Red conjunctivae, dry mouth, tachycardia, no change in pupils
Specific-substance use E. Cannabis -3
In low doses, marijuana increases appetite and relaxation and causes conjunctival reddening
Chronic users experience lung problems associated with smoking and a decrease in motivation ‘the amotivational syndrome’ characterized by apathy and lack of desire to work
Treatment: like most hallucinogens, the psychological effects are eased by reassurance in a quiet setting

Specific-substance use F. Inhalants -1 They include:
GasolineGluePaint thinner solvents

Specific-substance use F. Inhalants -2
Sniffing of inhalants is increasing among children and adolescents.
Brain damage may occur with repeated use, and no antidote or specific treatment exists
Intoxication may cause CNS depression, confusion and delirium
Chronic use may result in dementia
Principles of treatment of Substance-related Disorders
Certain approaches are useful for treatment of abuse and dependence of all substances:i. Detoxification - the first goal of
treatmentii. Insistence on abstinence – few
individuals can use addiction substances in moderation after successful treatment but they cannot be identified, hence complete abstinence is advised

Principles of treatment of Substance-related Disorders
Approaches to treatment for all substances:
iii. Avoidance of other substances associated with dependence (beware of tranquilizers)
iv. Involvement of family – the family can be important allies in insisting that the patient’s drug abuse problem be dealt with, however substance abuse may also provide the family with a convenient distraction from a less palatable family problem
Principles of treatment of Substance-related Disorders
Approaches to treatment for all substances:
v. Toxicology screens – periodic urine screens are often essential in identifying relapse and non- compliance
vi. Self-help groups – Peer support groups provide credibility and encouragement from individuals who have had similar problems and who are adept at dealing with common resistances to treatment. Twelve step programs have been developed for most substances
Principles of treatment of Substance-related Disorders
Approaches to treatment for all substances:
vii. Sanctioned treatment: When an patient is forced to remain in therapy by a le gal sanction, the outcome is better individual is better than when free will is at play
viii.Contingency contracting – powerful negative and positive contingencies tied to treatment. Pre-signed letter of patient is mailed by therapist if failures evident. Especially effective in medical licensure

Principles of treatment of Substance-related Disorders