j. clin. microbiol. doi:10.1128/jcm.01974-12 t...
TRANSCRIPT

1
TITLE: Pneumocystis jirovecii colonization among cystic fibrosis patients: A French prospective 1
multicenter study. 2
3 RUNNING HEAD: Pneumocystis carriage in cystic fibrosis 4
5 AUTHORS: Francisca Hernández-Hernández1-5, Emilie Fréalle1-4, Patrick Caneiro1-4, Julia 6
Salleron6, Isabelle Durand-Joly4,7, Isabelle Accoceberry8, Jean-Philippe Bouchara9,10, Benoit 7
Wallaert11, Eduardo Dei-Cas1-4, Laurence Delhaes1-4# 8
9 AUTHORS’AFFILATIONS:
1Center for Infection and Immunity of Lille (CIIL), Institut Pasteur de 10
Lille, Biology and Diversity of Emerging Eukaryotic Pathogens (BDEEP, EA4547), BP 245, 11
59019 Lille cedex, France; 2INSERM U1019, 59000 Lille cedex, France; 3UMR CNRS 8204, 12
59021 Lille cedex, France; 4Department of Microbiology, Lille Hospital, Faculty of Medicine, 13
59000 Lille cedex, France; 5Microbiology and Parasitology Department, Faculty of Medicine, 14
Universidad Nacional Autónoma de México, México D.F., México. 6Department of 15
Biostatistics, Lille Hospital, Faculty of Medicine, 59000 Lille cedex, France; 7Department of 16
Hygiene, Hospital of Dunkerque, Dunkerque, France; 8Department of Parasitology and 17
Mycology, Saint André Hospital, CHU of Bordeaux, Bordeaux, France; 9Department of 18
Parasitology-Mycology, CHU, Angers, France, 10GEIHP – UPRES, EA 3132, University of 19
Angers, France; 11Department of Pneumology and Immuno-Allergology, Calmette Hospital, 20
59000 Lille, France. 21
# CORRESPONDENT FOOTNOTE: Laurence Delhaes: Center for Infection and Immunity of Lille 22
(CIIL), Institut Pasteur de Lille, INSERM U1019, UMR CNRS 8204, University Lille Nord de 23
France, Biology and Diversity of Emerging Eukaryotic Pathogens (BDEEP), EA4547, 1 rue du 24
Pr Calmette, BP 245, 59019 Lille Cedex, France. Tel.: +33 3 2087 7156; fax: +33 3 2044 4895. 25
E-mail address: [email protected] 26
Copyright © 2012, American Society for Microbiology. All Rights Reserved.J. Clin. Microbiol. doi:10.1128/JCM.01974-12 JCM Accepts, published online ahead of print on 26 September 2012
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

2
ABSTRACT 27
Pneumocystis carriage was detected in 12.5% of 104 cystic fibrosis (CF) patients during a 28
prospective multicenter French study, with a prevalence of genotype 85C/248C and geographic 29
variations. It was significantly associated with the absence of P. aeruginosa colonization and 30
better FEV1 values. Results are discussed considering the natural history of CF. 31
32
Key-words: Pneumocystis jirovecii, PCR, Real-Time PCR, Genotype, mtLSU, Cystic fibrosis. 33
34
While Pneumocystis jirovecii is a well-known cause of pneumonia (PcP) in severely 35
immunocompromised patients, Pneumocystis carriage has drawn increasing interest. Several 36
works support a significant association of P. jirovecii colonization with diverse chronic 37
pulmonary diseases (6, 12, 21). In cystic fibrosis (CF), few severe PcP have been reported (23, 38
25), and only some studies reported Pneumocystis carriage for which the clinical significance 39
remains practically unexplored (14, 18-20, 22-26). The aim of the present study was therefore to 40
evaluate the prevalence of P. jirovecii colonization during a prospective multicenter 41
observational study, to provide information regarding the distribution of Pneumocystis 42
genotypes, and to explore the clinical relevance of Pneumocystis colonization among CF 43
patients from France. 44
One hundred and four CF patients of median age 24.0 years (interquartile ranges Q1:18 y - Q3: 45
29.5y; 50 males and 54 females) were included by physicians according to the same criterion 46
(an annual check-up or exacerbation situation that required an expectorated sputum), and were 47
screened for P. jirovecii carriage (Reference number of the institutional ethics committees of 48
Lille Hospital: CPP 06/84). All patients had a well-documented diagnosis of CF with either the 49
two known mutations in the CFTR gene (35.6% were homozygous and 45.2% heterozygous for 50
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
3
the F508del mutation) or an abnormally high sweat chloride test (median: 102, Q1-Q3: 90-128 51
mmol/L). Clinical data including spirometry, therapeutic, radiological and biological data were 52
collected by clinic staff at each time of the visit and used for the statistical analysis under SAS 53
software (version 9.2; SAS Institute-USA). Sputum specimens (n=146) were collected from 54
hospitals in Lille (93 samples, 58 patients), Dunkerque (27 samples, 20 patients), Angers (18 55
samples, 18 patients), and Bordeaux (8 samples, 8 patients) between October 2006 and March 56
2009. Each specimen examined was considered as independent event since the delay between 2 57
sputa was at least 6 months (18). Samples were collected and analyzed according to a 58
standardized protocol as previously described (3, 8). 59
After DNA extraction (8), the presence of P. jirovecii was detected by combining an initial 60
conventional PCR with a real-time PCR reaction (rt-PCR). Briefly, rt-PCRs were performed in a 61
final volume of 20 µl, consisting of 18 µl of LightCycler-FastStart Taq (Roche), reaction buffer 62
containing 2.4 mM MgCl2, 0.5 µM of each of the primers (pAZ 102 X and pAZ 102 Y), 0,2 µM 63
of the fluorescein (5’-CAG ACT ATG TGC GAT AAG GTA GAT AGT CGA [Flc]-3’) and LC 64
Red-640 (5’-[LC640] GGA AAC AGC CCA GAA CAG TAA TTA AA-3’) FRET-probes, and 65
2 µl DNA template obtained from the first round PCR. Initial preheating and touch-down 66
procedures were performed on LightCycler 2.0 System as previously described (13). Samples 67
were handled under a laminar flow cabinet. Extraction, mix preparation, and LightCycler 68
carousel loading were performed in different rooms. Negative and positive controls were 69
included in each extraction step and each PCR reaction. PCR inhibitions were identified when 70
DNA samples were diluted 1/10. A sample was considered positive for P. jirovecii DNA 71
detection when at least one combined PCR assay (with pure or 1/10 diluted DNA) yielded a 72
positive result. Purified amplicons from positive samples were sequenced directly (18), to detect 73
mtLSU polymorphisms (10, 14, 16-20, 22, 24). Pneumocystis colonization (or asymptomatic, 74
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
4
subclinical carriage) was defined as a molecular detection (positive PCR) without positive direct 75
examination, clinical signs of PcP, nor progression to PcP infection (4, 5). 76
P. jirovecii DNA was detected in 13/104 (12.5%) of patients, corresponding to a total of 17 77
positive samples. In 5 samples, PCR inhibitions were observed and avoided using 1/10 diluted 78
DNA. Patients colonized with Pneumocystis were distributed as follow: 4 patients from Angers, 79
2 from Bordeaux, 4 from Dunkerque and 3 from Lille. The colonization rate reported in Lille (3 80
patients out of 58 followed-up in Lille hospital: 5.2%) was significantly lower than in the other 81
centres (p = 0.036, using Fisher’s exact test). Fourteen out of the 17 PCR-positive samples were 82
successfully sequenced. Only mutations at position 45 were recorded, leading to a predominance 83
of genotypes 1 and 2 (genotype 2 was sequentially isolated from two samples of one patient in 84
Lille - Fig. 1). Their distributions varied according to CF patients’ place of diagnosis (Fig. 1). 85
When we compared characteristics collected at each sampling time of CF patients with or 86
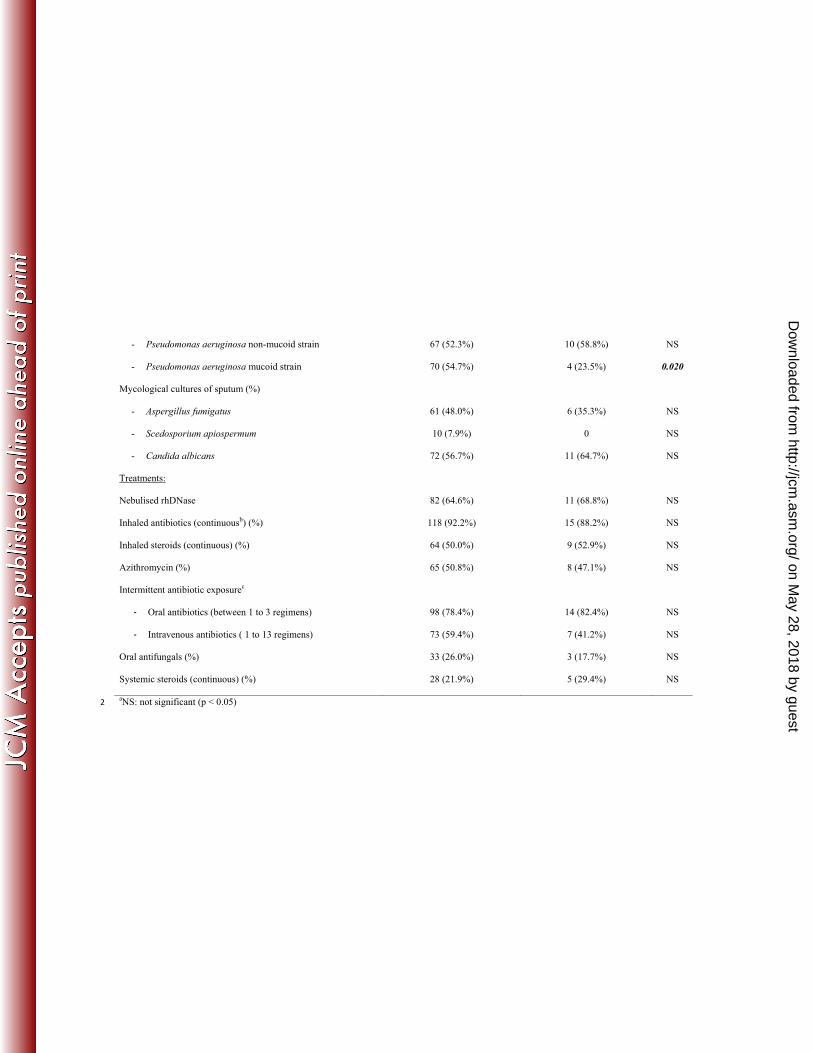
without indication of P. jirovecii carriage (Table 1), Pneumocystis colonization was significantly 87
associated with the absence of colonization by Pseudomonas aeruginosa mucoide strain (p = 88
0.020, Fisher’s exact test). Moreover, forced expiratory volume in 1 s values (% of predicted 89
FEV1) were significantly higher in patients colonized with P. jirovecii (80% versus 53.0 % of 90
FEV1 median, p = 0.032 using Kruskal-Wallis Test), suggesting a better pulmonary function in 91
Pneumocystis colonized P. aeruginosa-positive patients. The present population of CF patients 92
colonized with Pneumocystis was not considered as having severe airway disease, since the 93
median (Q1-Q3) values of Shwachman-Kulczycki score (S-K score), body mass index (BMI) 94
and forced vital capacity (% of predicted FVC) were respectively 80 (60-90), 19.2 (18.0-20.9), 95
and 90 (61-109 %) in Table 1; S-K score being under 50%, BMI under 16 and FVC under 50% 96
in severe disease. No association between therapeutics, including systemic corticotherapy, and 97
Pneumocystis colonization was significant. Since the overall numbers of subjects in subgroups 98
were small, univariate methods were used here, requiring larger studies to confirm these results, 99
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

5
the use of multivariate analysis to select variable subsets and to determine relative worth of the 100
variables. Clinical and microbiological features of our population were in agreement with recent 101
published data (2, 3). 102
P. jirovecii is now classified as an atypical fungus, unable to grow in vitro in current fungal 103
culture media, and exhibiting pulmonary tropism with strict human host-specificity. While PCR 104
assays have represented a significant advance in Pneumocystosis diagnosis, they also revealed 105
Pneumocystis colonization occurring in immunocompromised and non-immunocompromised 106
patients, and allowed exploration of the corresponding P. jirovecii circulation between Humans, 107
including non-immunocompromised patients (5, 6, 10, 12-15, 17-22, 24, 26-29, 32). Here, we 108
combined conventional PCR and rt-PCR methods targeting the mtLSU gene in order to increase 109
the detection rate whilst maintaining the specificity of detection by using FRET-probes. Both, 110
diluted and non-diluted DNA samples are suggested to be used: diluted DNA overcomes 111
potential inhibitors, and non-diluted DNA overcomes amplification failures due to scarce 112
amounts of Pneumocystis DNA in the specimen. According to our observations, it is a reliable 113
technique that allowed us to detect Pneumocystis colonization in 12.5% of patients. This 114
percentage is in agreement with data reported in CF patients from European and Brazilian areas 115
(7.4, 21.5, and 38.2%) (22, 24, 26), but higher than the value of 1.3% reported by Le Gal et al. 116
in a serie of 76 CF patients from French Brittany (14). As previously reported (1, 17), such 117
geographic differences in Pneumocystis carriage prevalence might be linked with the local 118
Pneumocystis circulation, which may be lower in the North of France (14, our results in Lille). 119
The low prevalence of Pneumocystis carriage we observed in the Lille population could be 120
related to a colder climate than in Angers or Bordeaux (average yearly temperature of 10.4°C, 121
11.8°C or 13.3°C, respectively), as previously suggested (16, 22). Using mtLSU rRNA (a highly 122
informative marker for discerning associations between specific genotypes and geographical or 123
clinical data (1, 10, 13-20, 22, 24, 26-29, 32)), we identified genotypes 1 and 2 as predominant, 124
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
6
in agreement with data from most European and American studies in non-CF or CF patients (1, 125
16, 17). Taking into account all these studies including Spanish and Brazilian ones that have 126
reported genotypes 1 and 3 as predominant in CF patients, genotype 1 polymorphism might be 127
the best adapted to patients with CF (1, 16-18, 20, 22, 24). 128
Despite technical factors that can influence the reported prevalence of Pneumocystis 129
colonization, and according to the above cited studies (including our results), it appears that CF 130
is mainly associated with lower Pneumocystis colonization rates than are other chronic 131
pulmonary diseases (14, 20, 22, 24, 26, 27, 32). Three studies have reported the association of P. 132
jirovecii and P. aeruginosa in CF patients (14, 22, 25), but whether Pneumocystis 133
infection/colonization complicated CF-associated lung disease remained unclear. In fact, little is 134
known regarding the in vivo interactions between species, especially considering the bacterial 135
and fungal community as a unique entity (lung microbiota) (8, 11, 31). In our study, 136
Pneumocystis carriage was associated with the absence of P. aeruginosa and with less severe 137
lung disease, a result in agreement with the role of Pneumocystis microorganisms in stimulating 138
pulmonary inflammation, being involved in the initial development of lung diseases, and in this 139
manner encouraging other, subsequent infections, as recently proposed (6, 7, 9, 12, 21, 30). 140
While high amounts of immunosuppressors, including steroids, seem to be a crucial factor 141
allowing PcP to occur (4, 6, 21, 32), we did not find any association between P. jirovecii 142
colonization in CF patients and systemic steroid therapy (Table 1). 143
To conclude, we have reported the prevalence of Pneumocystis carriage in CF patients from four 144
different French areas. Whether Pneumocystis colonization could have a role in the natural 145
course of CF lung disease has not been demonstrated so far, but the role of CF-patients 146
colonized by P. jirovecii as reservoir and as infective sources of this microorganism for other 147
susceptible individuals can be strongly suspected (28, 29), which is consistent with the 148
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

7
continuous infection/clearance cycle involving P. jirovecii recently reported in CF patients by 149
Montes-Cano et al. (18). 150
151
ACKNOWLEDGMENTS. Francisca Hernández-Hernández was supported by the Programa de 152
Apoyos para la Superación del Personal Académico (DGAPA- UNAM University, Mexico). 153
The authors thank all the clinicians for their cooperation in collecting sputum samples and 154
clinical data, and PHRC 1902 - Vaincre la mucoviscidose - Pfizer® for their financial support. L 155
Delhaes and J-P Bouchara are members of the ECMM/ISHAM Working Group Fungal 156
respiratory infections in CF. The authors thank Dr. R.J. Pierce for his attentive critical reading of 157
the manuscript, and declare having no conflict of interest. 158
159
REFERENCES 160
1. Beard CB, Carter JL, Keely SP, Huang L, Pieniazek NJ, Moura IN, Roberts JM, 161
Hightower AW, Bens MS, Freeman AR, Lee S, Stringer JR, Duchin JS, del Rio C, 162
Rimland D, Baughman RP, Levy DA, Dietz VJ, Simon P, Navin TR. 2000. Genetic variation 163
in Pneumocystis carinii isolates from different geographic regions: implications for 164
transmission. Emerg. Infect. Dis. 6:265-272. 165
2. Blyth CC, Middleton PG, Harun A, Sorrell TC, Meyer W, Chen SC. 2010. Clinical 166
associations and prevalence of Scedosporium spp. in Australian cystic fibrosis patients: 167
identification of novel risk factors? Med. Mycol. 48(Suppl. 1): S37–S44. 168
3. Borman AM, Palmer MD, Delhaes L, Carrère J, Favennec L, Ranque S, Gangneux 169
JP, Horré R, Bouchara JP. 2010. Lack of standardization in the procedures for mycological 170
examination of sputum samples from CF patients: a possible cause for variations in the 171
prevalence of filamentous fungi. Med. Mycol. 48 (Suppl 1):S88-S97. 172
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

8
4. Botterel F, Cabaret O, Foulet F, Cordonnier C, Costa JM, Bretagne S. 2012. Clinical 173
significance of quantifying Pneumocystis jirovecii DNA by using real-time PCR in 174
bronchoalveolar lavage fluid from immunocompromised patients. J. Clin. Microbiol. 50:227-175
231. 176
5. Calderón EJ, Friaza V, Dapena FJ, de La Horra C. 2010. Pneumocystis jirovecii and 177
cystic fibrosis. Med. Mycol. 48 (Suppl. 1), S17-S21. 178
6. Calderón EJ, Gutiérrez-Rivero S, Durand-Joly I, Dei-Cas E. 2010. Pneumocystis 179
infection in humans: diagnosis and treatment. Expert. Rev. Anti. Infect. Ther. 8:683-701. 180
7. Calderón EJ, Rivero L, Respaldiza N, Morilla R, Montes-Cano MA, Friaza V, Muñoz-181
Lobato F, Varela JM, Medrano FJ, Horra C de L. 2007. Systemic inflammation in patients 182
with chronic obstructive pulmonary disease who are colonized with Pneumocystis jirovecii. 183
Clin. Infect. Dis. 45:e17-e19. 184
8. Delhaes L, Monchy S, Fréalle E, Hubans C, Salleron J, Leroy S, Prevotat A, Wallet F, 185
Wallaert B, Dei-Cas E, Sime-Ngando T, Chabé M, Viscogliosi E. The airway microbiota in 186
cystic fibrosis: a complex fungal and bacterial community-implication for therapeutic 187
management. PLoS One. 2012;7:e36313. 188
9. Döring G, Parameswaran IG, Murphy TF. 2011 Differential adaptation of microbial 189
pathogens to airways of patients with cystic fibrosis and chronic obstructive pulmonary disease. 190
FEMS Microbiol. Rev. 35:124-146. 191
10. Esteves F, Gaspar J, de Sousa B, Antunes F, Mansinho K, Matos O. 2012. 192
Pneumocystis jirovecii multilocus genotyping in pooled DNA samples: a new approach for 193
clinical and epidemiological studies. Clin Microbiol Infect. 18: E177-E184. 194
11. Guss AM, Roeselers G, Newton IL, Young CR, Klepac-Ceraj V. Lory S, Cavanaugh 195
CM. 2011. Phylogenetic and metabolic diversity of bacteria associated with cystic fibrosis. 196
ISME J. 5:20-29. 197
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
9
12. Gutiérrez S, Respaldiza N, Campano E, Martínez-Risquez MT, Calderón EJ, De La 198
Horra C. 2011. Pneumocystis jirovecii colonization in chronic pulmonary disease. Parasite. 199
18:121-126. 200
13. Larsen HH, Masur H, Kovacs JA, Gill VJ, Silcott VA, Kogulan P, Maenza J, Smith M, 201
Lucey DR, Fischer SH. 2002. Development and evaluation of a quantitative, touch-down, real-202
time PCR assay for diagnosing Pneumocystis carinii pneumonia. J. Clin. Microbiol. 40:490-494. 203
14. Le Gal S, Héry-Arnaud G, Ramel S, Virmaux M, Damiani C, Totet A, Nevez G. 2010. 204
Pneumocystis jirovecii and cystic fibrosis in France. Scand. J. Infect. Dis. 42: 225–227. 205
15. Lu Y, Ling G, Qiang C, Ming Q, Wu C, Wang K, Ying Z. 2011. PCR diagnosis of 206
Pneumocystis pneumonia: a bivariate meta-analysis. J Clin Microbiol. 49: 4361-4363. 207
16. Miller RF, Evans HE, Copas AJ, Cassell JA. 2007. Climate and genotypes of Pneumocystis 208
jirovecii. Clin Microbiol Infect. 13: 445-448. 209
17. Miller RF, Lindley AR, Copas A, Ambrose HE, Davies RJ, Wakefield AE. 2005. Genotypic 210
variation in Pneumocystis jirovecii isolates in Britain. Thorax. 60: 679-682. 211
18. Montes-Cano MA, de la Horra C, Dapena FJ, Mateos I, Friaza V, Respaldiza N, 212
Muñoz-Lobato F, Medrano FJ, Calderon EJ, Varela JM. 2007. Dynamic colonisation by 213
different Pneumocystis jirovecii genotypes in cystic fibrosis patients. Clin. Microbiol. Infect. 13: 214
1008-11. 215
19. Montes-Cano MA, de la Horra C, Martín-Juan J, Varela JM, Torronteras R, 216
Respaldiza N, Medrano FJ, Calderón EJ. 2004. Pneumocystis jirovecii genotypes in the 217
Spanish population. Clin. Infect. Dis.39:123-128. 218
20. Montes-Cano MA, de la Horra C, Respaldiza N, Medrano FJ, Varela JM, Calderón 219
EJ. 2006. Polymorphisms in Pneumocystis jirovecii Strains in Spanish children with cystic 220
fibrosis. J. Infect. Dis. 193: 1332-1333. 221
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from

10
21. Morris A, Norris KA. 2012. Colonization by Pneumocystis jirovecii and its role in disease. 222
Clin Microbiol Rev. 25:297-317. 223
22. Pederiva MA, Wissmann G, Friaza V, Morilla R, de La Horra C, Montes-Cano MA, 224
Goldani LZ, Calderón EJ, Prolla JC. 2012. High prevalence of Pneumocystis jirovecii 225
colonization in Brazilian cystic fibrosis patients. Med. Mycol. 50: 556-560. 226
23. Quattrucci S, Rolla M, Cimino G, Bertasi S, Cingolani S, Scalercio F, Venuta F, 227
Midulla F. 2005. Lung transplantation for cystic fibrosis: 6-year follow-up. J Cyst Fibros. 228
4:107-114. 229
24. Respaldiza N, Montes-Cano MA, Dapena FJ, de la Horra C, Mateos I, Medrano FJ, 230
Calderon E, Varela JM. 2005. Prevalence of colonisation and genotypic characterisation of 231
Pneumocystis jirovecii among cystic fibrosis patients in Spain. Clin. Microbiol. Infect. 11:1012-232
1015. 233
25. Royce FH, Blumberg DA. 2000. Pneumocystis carinii isolated from lung lavage fluid in an 234
infant with cystic fibrosis. Pediatr. Pulmonol. 29:235-238. 235
26. Sing A, Geiger MA, Hogardt M, Heesemann J. 2001. Pneumocystis carinii carriage 236
among cystic fibrosis patients, as detected by nested PCR. J. Clin. Microbiol. 39:2717–2718. 237
27. Sivam S, Sciurba FC, Lucht LA, Shang Y, Duncan SR, Norris KA, Morris A. 2011. 238
Distribution of Pneumocystis jirovecii in lungs from colonized COPD patients. Diagn. 239
Microbiol. Infect. Dis. 71:24-248. 240
28. Totet A, Duwat H, Magois E, Jounieaux V, Roux P, Raccurt C, Nevez G. 2004. Similar 241
genotypes of Pneumocystis jirovecii in different forms of Pneumocystis infection. Microbiology. 242
150: 1173-1178. 243
29. Totet A, Latouche S, Lacube P, Pautard JC, Jounieaux V, Raccurt C, Roux P, Nevez 244
G. 2004. Pneumocystis jirovecii dihydropteroate synthase genotypes in immunocompetent 245
infants and immunosuppressed adults, Amiens, France. Emerg Infect Dis. 10: 667-673. 246
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
11
30. Ulrich M, Worlitzsch D, Viglio S, Siegmann N, Iadarola P, Shute JK, Geiser M, Pier 247
GB, Friedel G, Barr ML, Schuster A, Meyer KC, Ratjen F, Bjarnsholt T, Gulbins E, 248
Döring G. 2010. Alveolar inflammation in cystic fibrosis. J. Cyst. Fibros.9:217-227. 249
31. van der Gast CJ, Walker AW, Stressmann FA, Rogers GB, Scott P, Daniels TW, 250
Carroll MP, Parkhill J, Bruce KD.2011 Partitioning core and satellite taxa from within cystic 251
fibrosis lung bacterial communities. ISME J. 5:780-791. 252
32. Visconti E, Marinaci S, Zolfo M, Mencarini P, Tamburrini E, Pagliari G, Ortona E, 253
Siracusano A. 2000. Very low frequence of Pneumocystis carinii DNA detection by PCR in 254
specimens from patients with lung damage. J. Clin. Microbiol. 38:1307–1308. 255
256
FIGURE LEGEND 257
Figure 1. Distribution of P. jirovecii mt LSU r RNA genotypes in French CF patients according 258
to the geographic origin of CF patients. 259
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
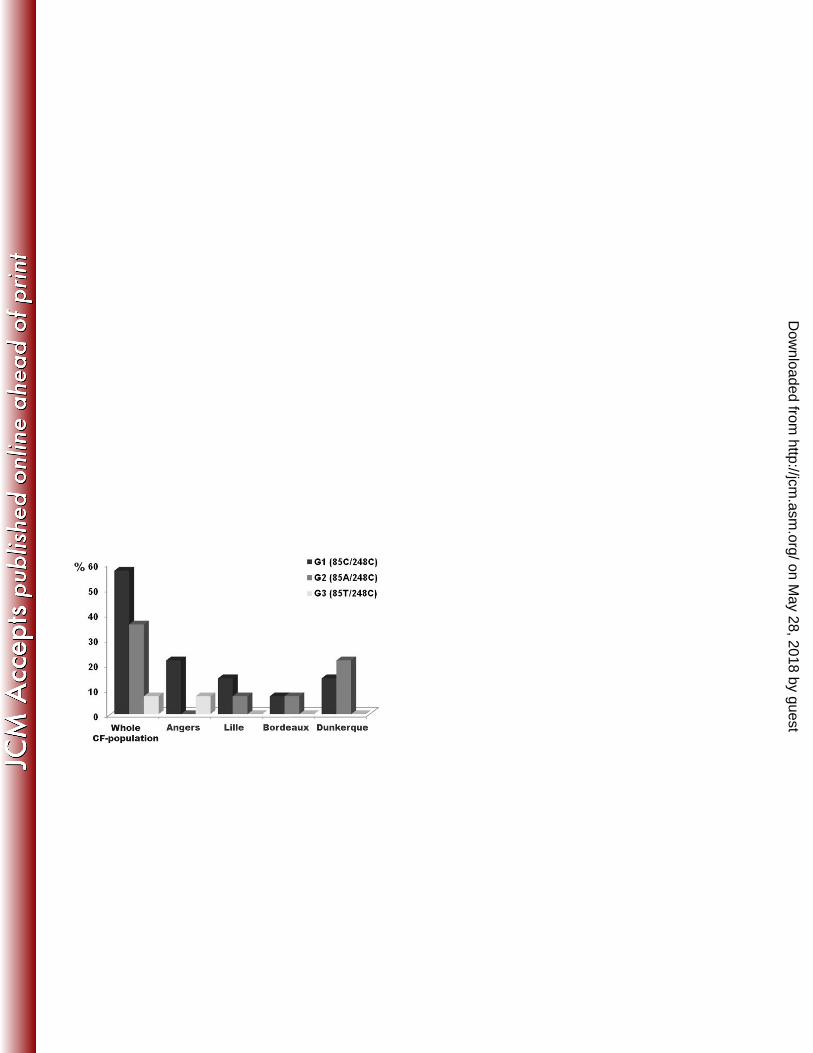

TABLE 1: Comparison of subjects with and without detectable P jiroveci DNA in sputum samples: Characteristics at each sputum sampling time. 1
P jiroveci DNA not detected in
sputum samples (n=129)
P jiroveci DNA detected in
sputum samples (n=17)
p valuea
General data:
Sex (Male – Female) 44 - 47 (48.4% - 51.7%) 6 – 7 (46.2% - 53.9%) NS
Age 24 (18 – 32) 23 (15 – 28) NS
CF clinical status:
S-K Score (median, and Q1 - Q3) 75 (60 - 83) 80 (60 - 90) NS
BMI (median, and Q1 - Q3) 19.1 (17.2 – 21.1) 19.2 (18.0 – 20.9) NS
FEV1 (median, and Q1 - Q3 in % of predicted value) 53.0 (36.0 – 77.0) 80.0 (46.0 – 100) 0.032
FVC (median, and Q1 - Q3 in % of predicted value) 68.5 (54.0 – 89.7) 90.0 (61.0 - 109) NS
Microbiological data
Bacterial colonization (at least one over the preceding year, %) by
- Haemophilus influenzae
- Methicillin-sensitive Staphylococcus aureus
- Methicillin-resistant Staphylococcus aureus
24 (18.8%)
51 (39.8%)
24 (18.8%)
3 (17.7%)
7 (41.2%)
0
NS
NS
NS
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
- Pseudomonas aeruginosa non-mucoid strain
- Pseudomonas aeruginosa mucoid strain
67 (52.3%)
70 (54.7%)
10 (58.8%)
4 (23.5%)
NS
0.020
Mycological cultures of sputum (%)
- Aspergillus fumigatus
- Scedosporium apiospermum
- Candida albicans
61 (48.0%)
10 (7.9%)
72 (56.7%)
6 (35.3%)
0
11 (64.7%)
NS
NS
NS
Treatments:
Nebulised rhDNase 82 (64.6%) 11 (68.8%) NS
Inhaled antibiotics (continuousb) (%) 118 (92.2%) 15 (88.2%) NS
Inhaled steroids (continuous) (%) 64 (50.0%) 9 (52.9%) NS
Azithromycin (%) 65 (50.8%) 8 (47.1%) NS
Intermittent antibiotic exposurec
- Oral antibiotics (between 1 to 3 regimens)
98 (78.4%)
14 (82.4%)
NS
- Intravenous antibiotics ( 1 to 13 regimens) 73 (59.4%) 7 (41.2%) NS
Oral antifungals (%) 33 (26.0%) 3 (17.7%) NS
Systemic steroids (continuous) (%) 28 (21.9%) 5 (29.4%) NS
aNS: not significant (p < 0.05) 2
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from
bContinuous drug exposure is defined as daily administration over the previous 6 months (3). 3
cIntermittent antibiotic exposure does not include TMP-SMX. 4
on May 28, 2018 by guest
http://jcm.asm
.org/D
ownloaded from